Augmented Capillary Leak during Isolated Hepatic Perfusion ... · and perfusate was temperature...
6
Vol. 4, 2357-2362, October 1998 Clinical Cancer Research 2357 Augmented Capillary Leak during Isolated Hepatic Perfusion (IHP) Occurs via Tumor Necrosis Factor-independent Mechanisms H. Richard Alexander,’ Charles K. Brown, David L. Bartlett, Steven K. Libutti, William D. Figg, Sangeeta Raje, and Ewa Turner Surgical Metabolism Section, Surgery Branch, and the Clinical Pharmacokinetics Section, Medicine Branch, Division of Clinical Sciences, National Cancer Institute, Bethesda, Maryland 20892 ABSTRACT Isolated organ perfusion of the liver or extremity with tumor necrosis factor (TNF) and melphalan results in re- gression of bulky tumors in the majority of patients. The efficacy of TNF in this setting is not known, although data suggest that it may exert antitumor effects primarily on tumor-associated neovasculature. We studied the effects of TNF on capillary leak in liver and tumor tissue during isolated hepatic perfusion (IHP) with melphalan. Twenty- seven patients with unresectable cancer confined to the liver underwent a 60-mm hyperthermic 11W using 1.5 mg/kg melphalan alone (n = 7) or with 1.0 mg of TNF (n = 20). Complete vascular isolation was confirmed in all patients using an intraoperative leak monitoring 1-131 radiolabeled albumin technique. Samples of tumor and liver were col- lected just prior to and immediately after IIIP. There was no difference in 1-131 radiolabeled cpm/g of tissue (cpm) in liver versus tumor at baseline (P2 0.44). After DIP, 1-131 albumin cpm were higher in tumor versus liver (10,999 ± 1,976 versus 3,821 ± 780, respectively; P2 < 0.005). How- ever, 1-131 albumin cpm in tumor were not effected by TNF (11,636 ± 2,518 with TNF versus 9,180 ± 2,674 without TNF; P2 = 0.59). TNF did not affect melphalan concentra- tions in tumor (1,883 ± 540 ng/g versus 1,854 ± 861 nglg without TNF; P2 0.9). Capillary leak, as reflected by diffusion of 1-131 radiolabeled albumin into the interstitial space, is comparable in liver and tumor before IHP but is significantly higher in tumor after IHP. The increased dif- fusion in the capillary tumor bed must occur through TNF- independent mechanisms such as intrinsic features of tumor neovasculature, hyperthermia, or other unrecognized perfu- sion-related factors. These data indicate that TNF must continue to be critically evaluated in clinical trials before it is routinely used with melphalan in isolated organ perfusion. Received 4/29/98; revised 6/22/98; accepted 7/6/98. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. I To whom requests for reprints should be addressed, at Surgery Branch, National Cancer Institute, NIH, Building 10, Room 2B07, Bethesda, Maryland 20892. Phone: (301) 496-2195; Fax: (301) 402-1788; E-mail: [email protected]. INTRODUCTION Isolated organ perfusion with TNF2 and melphalan has resulted in remarkably high response rates in patients with intransit melanoma or unresectable high-grade sarcoma of the extremity or unresectable cancers confined to the liver (1-4). In 1992, Li#{233}nard et a!. (1) published their initial results of ILP with TNF, melphalan, and IFN-y for patients with intransit mela- noma or extremity sarcoma. They reported an 89% complete response rate and an overall response rate of 100% ( 1). These results were interpreted to be superior to those obtained in previous reports of ILP using melphalan alone (2, 5), and based on these data, a number of centers initiated ILP clinical trials using TNF and melphalan administered via ILP to critically evaluate the potential therapeutic efficacy of this regimen. Sub- sequent series have reported complete response rates between 75 and 90% for patients with intransit melanoma and a limb salvage rate of over 80% in patients with unresectable high- grade extremity sarcoma (6-8). A Phase II trial of IHP using TNF and melphalan resulted in an overall response rate of 74% in patients with unresectable hepatic malignancies, including those with numerous metastases, bulky sites of disease, or patients who had failed extensive prior treatment (9). When TNF is used with melphalan, there is a characteristic tumor response distinct to that observed following ILP with melphalan alone. There is often rapid necrosis of tumors with eschar formation of bulky cutaneous lesions and abrupt cystic changes in deeper lesions on computed tomography or contrast- enhanced magnetic resonance imaging. There are considerable experimental data ( 10-12) and clinical observations (1 3, 14) that indicate that the primary antitumor effects of TNF admin- istered via isolated organ perfusion are on the tumor-associated neovasculature. In experimental models, TNF administration systemically results in rapid necrosis of tumors, and on histo- logical evaluation, there is primarily endothelial cell injury with intravascular erythrostasis and fibrin deposition (10). Turnors resistant to direct TNF cytotoxic effects in vitro may be sensi- tive to TNF effects in vivo, particularly when > 1 cm in diam- eter, a size at which the tumor neovasculature has been estab- lished (15). In ILP with TNF-based regimens, there is cornplete obliteration of the tumor-associated neovasculature after treat- ment (14). Despite considerable clinical evaluation, the exact contri- bution of TNF to the antitumor effects during hyperthermic isolated organ perfusion with melphalan are not known. Phase III random assignment trials are under way in Europe and the United States comparing these two treatment regimens admin- istered via ILP for extremity melanoma. In a preliminary anal- 2 The abbreviations used are: TNF, tumor necrosis factor; ILP, isolated limb perfusion; IHP, isolated hepatic perfusion; IVC, inferior vena cava; GDA, gastroduodenal artery.
Transcript of Augmented Capillary Leak during Isolated Hepatic Perfusion ... · and perfusate was temperature...

Vol. 4, 2357-2362, October 1998 Clinical Cancer Research 2357
Augmented Capillary Leak during Isolated Hepatic Perfusion (IHP)
Occurs via Tumor Necrosis Factor-independent Mechanisms
H. Richard Alexander,’ Charles K. Brown,
David L. Bartlett, Steven K. Libutti,
William D. Figg, Sangeeta Raje, and Ewa TurnerSurgical Metabolism Section, Surgery Branch, and the Clinical
Pharmacokinetics Section, Medicine Branch, Division of Clinical
Sciences, National Cancer Institute, Bethesda, Maryland 20892
ABSTRACTIsolated organ perfusion of the liver or extremity with
tumor necrosis factor (TNF) and melphalan results in re-
gression of bulky tumors in the majority of patients. The
efficacy of TNF in this setting is not known, although data
suggest that it may exert antitumor effects primarily on
tumor-associated neovasculature. We studied the effects of
TNF on capillary leak in liver and tumor tissue during
isolated hepatic perfusion (IHP) with melphalan. Twenty-
seven patients with unresectable cancer confined to the liver
underwent a 60-mm hyperthermic 11W using 1.5 mg/kg
melphalan alone (n = 7) or with 1.0 mg of TNF (n = 20).
Complete vascular isolation was confirmed in all patients
using an intraoperative leak monitoring 1-131 radiolabeled
albumin technique. Samples of tumor and liver were col-
lected just prior to and immediately after IIIP. There was no
difference in 1-131 radiolabeled cpm/g of tissue (cpm) in
liver versus tumor at baseline (P2 0.44). After DIP, 1-131
albumin cpm were higher in tumor versus liver (10,999 ±
1,976 versus 3,821 ± 780, respectively; P2 < 0.005). How-
ever, 1-131 albumin cpm in tumor were not effected by TNF
(11,636 ± 2,518 with TNF versus 9,180 ± 2,674 without
TNF; P2 = 0.59). TNF did not affect melphalan concentra-
tions in tumor (1,883 ± 540 ng/g versus 1,854 ± 861 nglg
without TNF; P2 0.9). Capillary leak, as reflected by
diffusion of 1-131 radiolabeled albumin into the interstitial
space, is comparable in liver and tumor before IHP but is
significantly higher in tumor after IHP. The increased dif-
fusion in the capillary tumor bed must occur through TNF-
independent mechanisms such as intrinsic features of tumor
neovasculature, hyperthermia, or other unrecognized perfu-
sion-related factors. These data indicate that TNF must
continue to be critically evaluated in clinical trials before it
is routinely used with melphalan in isolated organ perfusion.
Received 4/29/98; revised 6/22/98; accepted 7/6/98.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
I To whom requests for reprints should be addressed, at Surgery Branch,
National Cancer Institute, NIH, Building 10, Room 2B07, Bethesda,
Maryland 20892. Phone: (301) 496-2195; Fax: (301) 402-1788; E-mail:
INTRODUCTIONIsolated organ perfusion with TNF2 and melphalan has
resulted in remarkably high response rates in patients with
intransit melanoma or unresectable high-grade sarcoma of the
extremity or unresectable cancers confined to the liver (1-4). In
1992, Li#{233}nard et a!. ( 1 ) published their initial results of ILP with
TNF, melphalan, and IFN-�y for patients with intransit mela-
noma or extremity sarcoma. They reported an 89% complete
response rate and an overall response rate of 100% ( 1). Theseresults were interpreted to be superior to those obtained in
previous reports of ILP using melphalan alone (2, 5), and based
on these data, a number of centers initiated ILP clinical trials
using TNF and melphalan administered via ILP to critically
evaluate the potential therapeutic efficacy of this regimen. Sub-
sequent series have reported complete response rates between
75 and 90% for patients with intransit melanoma and a limb
salvage rate of over 80% in patients with unresectable high-
grade extremity sarcoma (6-8). A Phase II trial of IHP using
TNF and melphalan resulted in an overall response rate of 74%
in patients with unresectable hepatic malignancies, including
those with numerous metastases, bulky sites of disease, or
patients who had failed extensive prior treatment (9).
When TNF is used with melphalan, there is a characteristic
tumor response distinct to that observed following ILP with
melphalan alone. There is often rapid necrosis of tumors with
eschar formation of bulky cutaneous lesions and abrupt cystic
changes in deeper lesions on computed tomography or contrast-
enhanced magnetic resonance imaging. There are considerable
experimental data ( 10-12) and clinical observations ( 13, 14)
that indicate that the primary antitumor effects of TNF admin-
istered via isolated organ perfusion are on the tumor-associated
neovasculature. In experimental models, TNF administration
systemically results in rapid necrosis of tumors, and on histo-
logical evaluation, there is primarily endothelial cell injury with
intravascular erythrostasis and fibrin deposition (10). Turnors
resistant to direct TNF cytotoxic effects in vitro may be sensi-
tive to TNF effects in vivo, particularly when > 1 cm in diam-
eter, a size at which the tumor neovasculature has been estab-
lished (15). In ILP with TNF-based regimens, there is cornplete
obliteration of the tumor-associated neovasculature after treat-
ment (14).
Despite considerable clinical evaluation, the exact contri-
bution of TNF to the antitumor effects during hyperthermic
isolated organ perfusion with melphalan are not known. Phase
III random assignment trials are under way in Europe and the
United States comparing these two treatment regimens admin-
istered via ILP for extremity melanoma. In a preliminary anal-
2 The abbreviations used are: TNF, tumor necrosis factor; ILP, isolated
limb perfusion; IHP, isolated hepatic perfusion; IVC, inferior vena cava;
GDA, gastroduodenal artery.

2358 IHP and Capillary Leak
ysis of a random assignment trial comparing these regimens in
patients with stage lilA or IIIAB intransit melanoma, the corn-
plete response and overall response rate between groups were
not significantly different, although patients with bulky disease
or large lesions may have had a better response to TNF and
melphalan compared with melphalan alone.3 Although TNF has
potential effects on the tumor-associated neovasculature, when
it is given alone via hyperthermic isolated organ perfusion of the
limb or liver, there are no significant antitumor effects (16). In
addition, leak of perfusate containing TNF can result in poten-
tially significant systemic toxicity (5). Insight into the mecha-
nisms of the effects of TNF in isolated organ perfusion will be
important to use it most efficaciously in this setting. The present
study was undertaken to determine the effects of TNF on endo-
thelial cell permeability as measured by diffusion of radiola-
beled 1-131 albumin in normal and tumor tissue before and after
hyperthermic IHP with rnelphalan.
PATIENTS AND METHODSPatient Population. Between August 1996 and May
1997, 27 patients with primary or metastatic unresectable can-
cers confined to the liver were treated with a 60-mm hyperther-
mic IHP using 1.5 mg/kg of melphalan with (n = 20) or without
(n 7) tumor necrosis factor. The treatment protocols were
approved by Institutional Review Board and the Cancer Ther-
apeutics Evaluation Program of the National Cancer Institute.
Patients were treated on two consecutive Phase II protocols
using identical IHP treatment parameters; the latter without
TNF. All patients had multiple bibobar hepatic tumors. All
patients who had tumors accessible for biopsy were included in
the study. All patients had measurable, unresectable, biopsy-
proven primary metastatic cancers confined to the liver. Patients
underwent standard staging studies including computed tomog-
raphy scan of the chest, abdomen, and pelvis and, as clinically
indicated, brain magnetic resonance imaging or bone scan.
Eligibility criteria included Eastern Cooperative Oncology
Group performance status of 0 or 1 , a serum bilirubin <2.0
mg/dl, a platelet count > l50,000/ml, and a serum creatinine
�l.5 mg/dl.
IHP. The treatment technique of IHP was performed as
described previously (4). Briefly, via a laparotomy the liver is
extensively mobilized by dividing the falciform ligament and
the right and left triangular ligaments. The duodenum is exten-
sively mobilized and reflected medially. The right lobe of the
liver is retracted anteriorly and medially and the IVC from the
level of the renal veins to the diaphragm is completely dissected
from the retroperitoneum. The portahepatis structures are com-
pletely dissected and skeletonized, and a cholecystectomy is
performed. A 2-cm segment of GDA is dissected and serves as
the arterial cannulation site during IHP. The portal vein and
common bile duct are mobilized from the head of the pancreas
3 D. L. Fraker, H. R. Alexander, D. L. Bartlett, and S. A. Rosenberg. Aprospective randomized trial oftherapeutic isolated limb perfusion (ILP)
comparing melphalan (M) versus melphalan, tumor necrosis factor(TNF) and interferon-rny (IFN): an initial report, submitted for publica-
tion.
to the inferior border of the liver. All lymph node-bearing
tissues around the portahepatis structures are resected. A saphe-
nous vein and left axillary cutdown are performed. The patient
is systemically heparimzed with 200 units/kg, and after -5 mm,
a cannula is inserted into the saphenous vein and advanced into
the inferior vena cava just below the renal veins. A second
venous cannula is inserted into the axillary vein, and these are
connected to a veno-veno bypass circuit. The IVC is occluded
above the renal veins, and infrahepatic IVC blood flow is
shunted to the axillary vein using a centrifugal pump. A short
segment of infrahepatic IVC is isolated between vascular oc-
cluding clamps, and a 20-24 French venous cannula is inserted
through a venotomy and positioned behind the retrohepatic IVC
just beneath the hepatic veins. This cannula is connected to the
venous outflow line of the extracorporeal bypass circuit. The
portal vein blood flow is shunted by inserting a cannula distally
and incorporating it into the veno-veno bypass circuit. The GDA
is ligated, the common hepatic artery is occluded, and a
3-4-mm GDA cannula is positioned at the orifice of the corn-
mon hepatic artery. Finally, the suprahepatic IVC is cross-
clamped just below the diaphragm and isolated hepatic perfu-
sion is initiated.
The extracorporeal bypass circuit consists of a roller pump,
membrane oxygenator, and heat exchanger. The perfusate con-
sists of 700 ml of balanced salt solution primed with 300 ml of
packed RBCs and 2000 units of heparin. Arterial and venous
perfusate blood gases are obtained at regular intervals, and
sodium bicarbonate was added to the perfusion circuit to main-
tam an arterial perfusate pH between 7.2 and 7.3. Hepatic
parenchymal temperature probes are placed at various positions,
and perfusate was temperature controlled using a Hemotherm
cooler heated model #4 (Cincinnati SubZero Products, Cincin-
nati, Ohio). Flow rates are adjusted upward while monitoring for
a stable reservoir volume and acceptable line pressures. Usually,
stable perfusion parameters are achieved almost immediately,
and there is rapid and uniform heating of the liver to target
temperatures of 39.5-40#{176}C. Melphalan at a dose of 1.5 mg/kg
(Glaxo-Wellcome, Research Triangle Park, NC) and 1.0 mg
TNF (Knoll Pharmaceuticals, Whippany, NJ) are added sequen-
tially to the arterial inflow line of the perfusion circuit at time 0,
and the perfusion continued for 60 mm. At the conclusion of the
perfusion, the liver is flushed through the arterial inflow cannula
with 1500 ml of crystalloid, followed by 1500 ml of colloid, and
the proximal portal vein is flushed with 1 liter of normal saline.
After decannulation and repair of the P/C and portal venoto-
mies, normal physiological blood flow is reestablished promptly
to the liver.
Continuous Intraoperative Leak Monitoring with 1-131
Radiolabeled Human Serum Albumin. A continuous intra-
operative leak monitoring system as described previously for
isolated limb and liver perfusion with TNF and melphalan was
used in all patients. In addition, because the 1-131 radiolabeled
albumin was being used to assess capillary endothelial leak in
the liver and tumor vascular beds just before and after IHP,
tissue samples were obtained at consistent predetermined points.
Once stable perfusion parameters were established, a gamma
detection camera was positioned over the centrifugal pump
housing, which served as a stable reservoir of systemic blood
flow for the purposes of calculating leak rates. A 20 pCi dose of

Clinical Cancer Research 2359
Table 1 Patient demographics
Total TNF No TNF
n 27 20 7Male:female 18:9 13:7 5:2
AgeMean (range) 50 ± 2.2 49.6 ± 2.7 52.4 ± 3.5Range (yr) 24-71 24-7 1 37-65
Previous treatment (%) 13 (49%) 9 (45%) 4 (56%)Diagnoses
Colon adenocarcinoma 17 13 4Ocular melanoma 5 4 1
Hepatocellular carcinoma 2 2 0Carcinoid 2 0 2Leiomyosarcoma 1 1 0
radiolabeled 1-131 human serum albumin (Merck-Frosst, Que-
bec, Canada) was administered via a central vein, and a baseline
level of radioactive cpm (cpm) was determined on a stripchart
recorder. Subsequently, a 10-fold higher dose of 1-131 radiola-
beled albumin was then injected into the perfusion circuit. If any
increase in cpm were detected on the stripchart recorder, this
would indicate a leak from the perfusion circuit into the sys-
temic circuit circulation.
Tissue Samples. Between 3 and 5 mm after the perfusate
dose of radiolabeled I- 13 1 albumin had been administered, liver
and tumor biopsy samples were obtained, maintained on ice, and
immediately transported to the laboratory. At the completion of
IHP, after the flush of perfusate from the circuit and prior to
reestablishing native liver blood flow, a second biopsy of liver
and tumor tissue was obtained and transported immediately to
the laboratory on ice. If sufficient tissue had been obtained, a
portion of each sample was immediately frozen at - 80#{176}Cfor
subsequent melphalan tissue concentrations. The remaining
samples were immediately weighed and placed in scintillation
vials. 1-131 albumin was quantitated as cpm/g of tissue (cpm)
using a gamma counter.
Melphalan Assay. The melphalan tissue samples were
analyzed using an acid precipitation method, and reverse-phase
HPLC assay was used for quantification of melphalan. The
standard curve preparation procedure involved weighing 0.3 g
of blank liver tissue, adding 300 �l of water, and adding known
amounts of melphalan using a stock that was prepared in 0. 12 N
HC1. The tissue was then homogenized, and 300 p.1 of the
homogenate were transferred to a cold 1 .5-ml centrifugation
tube. The precipitation of proteins was facilitated by the addition
of 75 ml of ice-cold 4.6 N perchloric solution. The solution was
then vortexed and refrigerated at 4#{176}Cfor 20-30 mm to aid in
further protein precipitation. The homogenate was then centri-
fuged for 4-5 rain at 13,500 rpm, and 200 �i.l of the supernatant
were transferred into injector vials. A total of 170 pA was
injected into the reverse phase-HPLC system composed of a � 8
column and a isocratic mobile phase consisting of 0.24 N HC1:methanol (53:47% v/v) with a flow rate of 1 mI/mm. Fluores-
cence detection was used to detect melphalan, which had an
excitation wavelength of 260 nm and an emission wavelength of
365 nm. The patient samples were weighed, and 300 pA of water
added and the samples were processed with the same method as
the standard curve. The equation produced using the standard
TabI e 2 IHP parameters
Total TNF No TNF
n
Melphalan dose
Mean (mg)
Range (mg)
Duration (mm)
Flow rateMean (mL/min)
Range (mL/min)
Mean central hepatic
temperature (#{176}C)
Mean perfusion pressure
(mm Hg)
Perfusion pressure range(mm Hg)
Mean change reservoir
volume (ml)
%leak
27
117 ± 4.1
75-160
60
853 ± 25600-1350
40.0 ± 0.06
176 ± 5.7
105-240
98 ± 14
0
20
115 ± 4.375-144
60
840 ± 21600-1050
40. 1 ± 0.07
177 ± 6.3
1 10-240
1 10 ± 17
0
7
124 ± 9.4
95-160
60
889 ± 75720-1350
39.9 ± 0.07
171 ± 12.9
105-223
64 ± 23
0
curve was used to calculate the mass of melphalan present in
each sample. The mass of melphalan was then divided by the
weight of the tissue to give the final concentration in ng/g tissue.
Statistics. Data are presented as mean ± SE. Data were
analyzed using Student’s t test, and significance of differences
between data was determined by using the Bonferoni correction
for multiple comparisons.
RESULTSPatient demographics are shown in Table 1 . There was a
similar mean age, a 2: 1 male:female ratio, and a predominance
of colon adenocarcinoma diagnoses in both groups. Twenty-
seven patients were treated with a 60-mm hyperthermic IHP
using 1.5 mg/kg melphalan; 20 were treated with TNF, and 7
without. The perfusion parameters are shown in Table 2. The
mean flow rate, central hepatic temperature, line pressure, and
other parameters were comparable between groups. Using the
radiolabeled 1-131 albumin continuous leak monitoring system,
there was no identifiable leak of perfusate into the systemic
circulation in any patient. Conversely, the mean change in
reservoir volume in each group was < 100 ml, indicating no leak
of systemic blood into the perfusion circuit. Small changes in
reservoir volume are typically observed during the 60-mm IHP
and usually reflect small changes in passive filling or emptying
of the hepatic vascular bed.
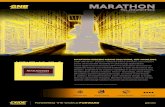
Fig. 1 illustrates the protocol for administration of radio-
labeled 1-131 albumin and biopsies of liver and tumor just
before and immediately after Il-IF. After establishing a stable
hepatic perfusion circuit, the systemic dose of I- 13 1 albumin
was administered through a central vein. Biopsies of liver and
tumor were obtained 3-5 mm after administration of the circuit
dose of 1-131 radiolabeled albumin. On the basis of mean flow
rates of almost 850 mi/mn and a circuit volume of 1 liter, this
allowed the perfusion circuit containing 1-131 albumin to recir-
culate through the hepatic vascular bed -4 times. Melphalan,
with or without TNF, was then added via the arterial line of the
perfusion circuit. After 60 mm, the circuit was flushed to re-
move melphalan and TNF from the intravascular space and also
served to remove any intravascular I- 1 3 1 radiolabeled albumin.

Establish IHP circuit
15000 -
0�.2� �oooo
E
�
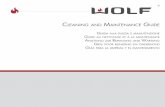
Fig. 3 1-131 albumin cpm in tumor samples post-IHP with or without
TNF (P1 = 0.59). Bars, SE.
1 .) Biopsy liver and tumor
2.) Add melphalan± TNF�
C)
a)� 2000 -
-�
0.. �
4)
0�
= Liver
- TumorFig. 4 Melphalan concentrations (ng/gm) in tumor samples after IHPwith n = 14 and without TNF (n 5, P2 0.96). Bars, SE.
___ 15000a)
�C
E
g�Pre-IHP Post-IHP
Fig. 2 Mean 1-131 albumin cpm in liver and tumor samples obtainedimmediately before and after IHP. Post-IHP 1-131 albumin was signif-icantly greater than post-IHP liver levels (*, P2 0.005) and pretreat-
ment tumor levels (*, P2 = 0.006). There was no difference in 1-131
albumin cpm in liver compared with tumor at baseline and a marginal
increase in 1-131 albumin cpm in post- compared with pre-IHP liver(P2 = 0.06). Bars. SE.
Therefore, all 1-131 albumin detected in these samples is in the
interstitial space.
Overall, there was no difference in 1-131 albumin cprn in
liver compared with tumor at baseline (P2 = 0.44; Fig. 2). There
was a marginal increase in I- 1 3 1 albumin cpm in post- corn-
pared to pre-IHP liver tissue (P2 = 0.06). I- 13 1 albumin cpm
were significantly higher in tumor after IHP compared with
pre-IHP tumor (P2 = 0.006) and post-IHP liver (P2 = 0.005;
Fig. 2). Interestingly, the 1-13 1 albumin in tumor was not
2360 IHP and Capillary Leak
1T3 to 5 mm
20 uCi 1-131 albumin�
� systemically
3to5min
200 uCi 1-131 albumin intoIHP circuit
5mm
60 mm 3000 ----�-�--
I .) Flush HP circuit
2.) Biopsy liver and tumorj
Fig. 1 Protocol for obtaining liver and tumor samples before and
immediately after isolated hepatic perfusion.
TNF NoTNF
TNF NoTNF
statistically different between patients treated with or without
TNF (P, = 0.59; Fig. 3). Furthermore, TNF did not affect
melphalan tumor concentrations after IHP when compared with
melphalan alone (P2 = 0.97; Fig. 4). These last data are based
on sample analyses of 14 patients treated with TNF and 5
without. One other patient treated without TNF had a melphalan
concentration in tumor that was >2-fold higher than any other
value, almost 10-fold higher than the mean of either group and,
therefore, was excluded from the statistical analysis. However,
the outcome of the statistical analysis between the groups re-
mained nonsignificant when the value was included in the data.
DISCUSSION
Because of the significant effects on tumor neovasculature
that have been observed after hyperthermic isolated limb per-
fusion with TNF and melphalan (13, 14) and the experimental
data suggesting that the primary antitumor effects of TNF may
be exerted on the tumor neovasculature ( 1 1 , 14), this study was
performed to determine whether hyperthermic isolated hepatic
perfusion may cause augmentation in tumor-associated micro-
vascular permeability, thereby facilitating the selective delivery
of chemotherapeutics to the tumor.
The data presented here show that comparable amounts of

Clinical Cancer Research 2361
4 H. R. Alexander, unpublished observations.
radiolabeled 1-131 albumin are present in liver and tumor tissue
just prior to treatment with isolated hepatic perfusion. However,
after a 60-mm hyperthermic hepatic perfusion using rnelphalan
with or without TNF, there is a significant and selective increase
in interstitial 1-13 1 albumin in tumor compared with both pre-
treatment tumor levels and posttreatrnent liver tissue. The pre-
treatment 1-131 albumin cprn in liver and tumor also reflect
some I- 13 1 albumin contained in the intravascular space in the
tissue biopsies obtained. However, posttreatrnent values reflect
true interstitial amounts of 1-131 albumin because the circuit is
flushed with 3 liters of crystalloid and colloid solution, which
effectively removes the 1-131-containing perfusate from the
intravascular space. The 27 patients analyzed in this report
underwent an identical hepatic perfusion treatment protocol.
This cohort represents consecutively treated patients who had
tumor that could be easily biopsied before and after treatment.
All but two patients had metastatic cancers to the liver, and
two-thirds of those were colorectal tumors. All identifiable
perfusion-related parameters that may have influenced micro-
vascular permeability were comparable between the 20 patients
treated with TNF and the 7 who received no TNF. Remarkably,
using the maximum safe tolerated dose of TNF when combined
with 1.5 mg/kg rnelphalan, there was no significant difference in
interstitial 1-131 albumin in patients treated with TNF compared
with those who received no TNF. This suggests that other
unrecognized perfusion-related factors must be accounting for
the augmented capillary leak in the tumor bed during isolated
perfusion. The number of possibilities are considerable and
would include the artificial flow dynamics of the extracorporeal
bypass circuit, local pH changes potentially related to nonphysi-
ological flow rates, or local production of cytokines or other
factors that may render the tumor-associated neovasculature
selectively sensitive to hyperthermia or melphalan. Interest-
ingly, the initial overall response rates between the groups are
similar.4
The comparable levels of rnelphalan in liver tissue after
IHP in patients treated with or without TNF may be related to
the increased diffusability of 1-131 albumin. The larger macro-
rnolecule, I- 13 1 albumin, has a molecular weight of 66,000,
whereas melphalan is a considerably smaller molecule with a
molecular weight of 305. Therefore, its delivery into the inter-
stitial space may not be as dependent on changes in endothelial
permeability as 1-131 albumin. Although mean melphalan con-
centrations were similar in patients treated with TNF compared
with those who were not, because there was only a single time
point available for analysis, there are limited conclusions that
can be drawn from these data. The tissue concentrations of
melphalan over time or the possible cellular or molecular effects
of rnelphalan with or without TNF have not been addressed in
this study.
A large number of institutions are evaluating the use of
TNF in isolated limb perfusion for intransit melanoma or unre-
sectable high grade extremity sarcoma, and a smaller number of
centers are evaluating its use in IHP for unresectable cancers
confined to the liver. In both limb and liver perfusion TNF is
associated with considerable regional and systemic toxicities
(9, 17, 1 8) and has not been conclusively demonstrated to
improve response rates.3 On the basis of presently available
data, it appears that TNF causes a very characteristic pattern of
tumor regression manifested by rapid tumor necrosis with es-
char formation of cutaneous lesions, significant angiographic
and radiographic changes of large extremity sarcomas, and a
more rapid time course of response compared with patients
treated with melphalan alone (2, 14, 19). Taken together, these
points highlight the fact that the use of TNF in isolated perfusion
must be critically evaluated in appropriately designed clinical
trials to determine efficacy and mechanisms of its antitumor
effects, optimal dosing schedules, and appropriate patient selec-
tion.
We have recently reported results of a Phase II trial of IHP
with melphalan and TNF for patients with unresectable cancers
confined to the liver (9). The 60-mm perfusion interval has been
used based upon previously conducted studies, and there are no
data indicating that a longer or shorter interval would be supe-
nor. The overall response rate in 33 evaluable patients was 74%
including patients with large or numerous lesions as well as
those who had undergone extensive previous treatment. Seventy-
five percent of all patients experienced transient grade 3 or 4
(National Cancer Institute common toxicity criteria) hepatic
toxicity, and one patient developed fatal hepatic veno-occlusive
disease. Complete vascular isolation was achieved during IHP
on the basis of the results of continuous intraoperative leak
monitoring and the fact that systemic levels of TNF could not be
detected, except for low transient levels in two patients who had
a correctable small (<4%) leak of perfusate during treatment.
However, there are significant hernodynamic changes associated
with this procedure, and circulating levels of interleukin 6 and
interleukin 8 between 2 and 12 h after the procedure are as high
as those reported in patients with life-threatening septic shock
(20-22). These secondary cytokines are presumably released by
the liver in response to the perfusion. In patients undergoing
isolated limb perfusion with TNF and melphalan, systemic
toxicity is associated with the presence of a perfusate leak
during treatment, and leak rates of 5% or greater occur in -15%
of patients (23, 24). The question as to whether the routine use
of TNF is justified in isolated organ perfusion has not yet been
determined.
In summary, the data presented in this report show that
hyperthermic IHP results in a selective and significant increase
in capillary endothelial permeability in tumor-associated neo-
vasculature. This has important implications for the use of
isolated organ perfusion with various therapeutic agents. Al-
though the exact mechanisms for this increase in microvascular
permeability are not known, it does not appear that TNF con-
tributes significantly to this effect.
REFERENCES
1. Li#{233}nard,D., Ewalenko, P., Delmotti, J. J., Renard, N., and Lejeune.
F. J. High-dose recombinant tumor necrosis factor a in combinationwith interferon y and melphalan in isolation perfusion of the limbs formelanoma and sarcoma. J. Clin. Oncol., 10: 52-60, 1992.
2. Alexander, H. R., Fraker, D. L., and Bartlett, D. L. Isolated limbperfusion for malignant melanoma. Semin. Surg. Oncol., 12: 4 16-428,
1996.

2362 IHP and Capillary Leak
3. Eggermont, A. M. M., Koops, H. S., Klausner, J. M., Kroon,
B. B. R., Schlag, P. M., Li#{233}nard,D. v. G. A. N., Hoekstra, H. J., Meller,
I., Nieweg, 0. E., Kettelhack, C., Ben-Ari, G., Pector, J-C., and Lejeune,F. J. Isolated limb perfusion with tumor necrosis factor and melphalanfor limb salvage in 186 patients with locally advanced soft tissueextremity sarcomas. Ann. Surg., 224: 756-765, 1996.
4. Alexander, H. R., Bartlett, D. L., and Libutti, S. K. Isolated hepaticperfusion: a potentially effective treatment for patients with metastatic or
primary cancers confined to the liver. Cancer J. Sci. Am., 4: 2-11, 1998.
5. Fraker. D. L., and Alexander, H. R. Isolated limb perfusion with high-dose tumor necrosis factor for extremity melanoma and sarcoma. In: V. I.DeVita, Jr., S. Heilman, and S. A. Rosenberg (eds.), Important Advances inOncology. pp. 179-192. Philadelphia: J. B. Lippincott, 1994.
6. Vaglini, M., Belli, F., Ammatuna, M., Inglese, M. G., Manzi, R.,Prada, A., Persiani, L., Santinami, M., Santoro, N., and Cascinelli, N.Treatment of primary or relapsing limb cancer by isolation perfusionwith high-dose a-tumor necrosis factor. �y-interferon, and melphalan.
Cancer (Phila.), 73: 483-492, 1994.
7. Li#{233}nard,D., Aggermont, A., Koops, H. S., Kroon, B., and Lejeune,F. J. The use of TNF in isolated limb perfusion for treatment of locallyadvanced melanoma: an update. Cambridge Symp., 1: 12, 1996.
8. Eggermont, A. M. M., Koops, H. S., Li#{233}nard,D., Kroon, B. B. R.,
van Geel, A. N., and Hoekstra, H. J. Isolated limb perfusion with highdose tumor necrosis factor-a in combination with interferon--y andmelphalan for irresectable extremity soft tissue sarcomas: a multicenter
trial. J. Clin. Oncol., /4: 2653-2665, 1996.
9. Alexander, C., Bartlett, D. L., Libutti, S. K., Fraker, D. L., Moser, I.,and Rosenberg, S. A. Isolated hepatic perfusion with tumor necrosis
factor and melphalan for unresectable cancers confined to the liver.
J. Clin. Oncol., 16: 1479-1489, 1998.
10. Nawroth. P. P., and Stern, D. M. Modulation of endothelial cellhemostasis properties by tumor necrosis factor. J. Exp. Med., 163:
740-745, 1986.
1 1. Nawroth, P., Handley, D., Matsueda, G., de Waal, R.. Gerlach, H.,
Blohm, D., and Stern, D. Tumor necrosis factor/cachectin-induced in-
travascular fibrin formation in meth A fibrosarcomas. J. Exp. Med., 168:
637-647, 1988.
12. Nooijen, P., Manusama, E. R., Eggermont, A. M., Schalkwijk, L.,
Stavast, J., Marquet, R. L., de Waal, R. M., and Ruiter, D. J. Synergisticeffects of TNF-a and meiphalan in an isolated limb perfusion model of
rat sarcoma: a histopathological, immunohistochemical and electron
microscopical study. Br. J. Cancer, 74: 1908-1915, 1996.
13. Renard, N., Nooijen, P. 1., Schalkwijk, L., de Waal, R. M., Egg-
ermont, A. M., Li#{233}nard,D., Kroon, B. B., Lejeune, F. J.. and Ruiter.D. J. VWF release and platelet aggregation in human melanoma afterperfusion with TNF a. J. Pathol., 176: 279-287, 1995.
14. Olieman, A. F. I., van Ginkel, R. J., Hoekstra, H. J., Mooyaart,
E. L., Molenaar, W. M., and Koops, H. S. Angiographic response oflocally advanced soft-tissue sarcoma following hyperthermic isolatedlimb perfusion with tumor necrosis factor. Ann. Surg. Oncol., 4: 64-69,1997.
15. Asher, A. L., Mule, J. J., Reichert, C. M., Shiloni, E., and Rosen-
berg, S. A. Studies on the anti-tumor efficacy of systemically adminis-tered recombinant tumor necrosis factor against several murine tumorsin vivo. J. Immunol., /38: 963-974, 1987.
16. Posner, M. C.. Li#{233}nard,D., Lejeune, F. J., Rosenfelder, D., andKirkwood, J. Hyperthermic isolated limb perfusion with tumor necrosisfactor alone for melanoma. Cancer J. Sci. Am., 1: 274-280, 1995.
17. Fraker, D. L., Alexander, H. R., Andrich, M., and Rosenberg, S. A.Treatment of patients with melanoma of the extremity using hyperther-mic isolated limb perfusion with melphalan, tumor necrosis factor, and
interferon-gamma: results of a TNF dose escalation study. J. Clin.Oncol., 14: 479-489, 1996.
18. Eggimann, P. C. R., Chassot P-G,, Li#{233}nard, D., Gerain, J., and
Lejeune, F. Systemic and hemodynamic effects of recombinant tumor
necrosis factor a in isolation perfusion of the limbs. Chest. 107: 1074-
1082, 1995.
19. Eggermont, A. M., Schraffordt, K. H., Klausner, J. M., Li#{233}nard,D.,Kroon, B. B., Schlag, P. M., Ben-Air, G., and Lejeune, F. J. Isolationlimb perfusion with tumor necrosis factor a and chemotherapy for
advanced extremity soft tissue sarcomas. Semin. Oncol., 24: 547-555,
1997.
20. Damas, P., Ledoux, D., Nys, M., Vrindts, Y., de Groote, D.,
Franchimont, P., and Lamy, M. Cytokine serum level during severesepsis in human IL-6 as a marker of severity. Ann. Surg., 215: 356-362,
1992.
21. Hack, C. E., Dc Groot, E. R., Felt-Bersma, J. F., Huijens, J. H., vanSchijndel, R. J. M. S., Eerenberg-Belmer, A. J. M., Thijs, L. G., and
Aarden, L. A. Increased plasma levels of interleukin-6 in sepsis. Blood,74: 1704-1710, 1989.
22. Endo, S., Inada, K., Inoue, Y., Kuwata, Y., Suzuki, M., Yamashita,H., Hoshi, S., and Yoshida, M. Iwo types of septic shock classified bythe plasma levels ofcytokines and endotoxin. Circ. Shock, 38: 264-274,1992.
23. Fraker, D. L., and Alexander, H. R. Use of high-dose tumor necrosisfactor in isolation perfusion of the limbs and liver. Reg. Cancer Treat.,8: 37-41, 1995.
24. Klaase, J. M., Kroon, B. B. R., van Geel, A. N., Eggermont,A. M. M., and Franklin, H. R. Systemic leakage during isolated limbperfusion for melanoma. Br. J. Surg., 80: 1 124-1 126, 1993.