Articulating the auditory imagination: when children talk about poetry they hear

Auditory Accommodations: Can You Hear Me Now?Danielle Oakes, Emily Jurcsek, Victoria Giannone
Joanne Christodoulou, EdD. CCC-SLP & James Baer, AuD, F-AAA, CCC-A
Utilizing a personal amplification device (i.e., PockeTalker) during cognitive-linguistic testing allowed clients with a hearing loss easier access to the required auditory stimuli while maintaining the integrity and construct of the assessment.
Participants: All participants were > 18 years of age and were from diverse backgrounds and education levels. All participants were recruited from the NJ/NY area.
Materials: Ross Information Processing Assessment – SecondEdition (RIPA-2), PockeTalker Ultra, Decibel: dB sound level meter App; Trials were timed utilizing the publication application “Stopwatch%.” version 5.1
Procedures: All participants first completed a basic audiological evaluation. Based on the results, they were assigned to one of three groups: A = no hearing loss (n=10); B = hearing loss with personal amplification device (n=10); C = hearing loss provided with increased vocal intensity (n=10). Group A was given 8 subtests of RIPA-2 without any modification, Group B was given 4 subtests with personal amplification and 4 without modification, Group C was given 4 subtests with increased speaking intensity monitored by a dB sound level meter to ensure 75 dB consistency and 4 with no modification. Response time (RT) was measured by the clinician during all administrations of the RIPA-2 using a stopwatch app.
American Speech-Language-Hearing Association (ASHA), (2020). Vocal cord nodules and polyps https://www.asha.org/public/speech/disorders/Vocal-Cord-Nodules-and-Polyps/
Cunningham, L., and Tucci, D. (2017). Hearing loss in adults. The New England Journal of Medicine, 377(25), 2465-2473.
Kirschner, P. A., Sweller, J., Kirschner, F., & Zambrano R, J. (2018). From cognitive load theory to collaborative cognitive load theory. International Journal of Computer-Supported Collaborative Learning : An Official Publication of the International Society of the Learning Sciences, 13(2), 213–233
Mamo, S. K., Reed, N. S., Nieman, C. L., Oh, E. S., & Lin, F. R. (2016). Personal Sound Amplifiers for Adults with Hearing Loss. The American journal of medicine, 129(3), 245–250.
Wingfield, A., & Peelle, J. E. (2012). How does hearing loss affect the brain?. Aging health, 8(2), 107–109. doi:10.2217/AHE.12.5
Methods and Materials
Results
Conclusions
References
Introduction
The PockeTalker Ultra Personal Amplifier (model
PKT-D1 EH)
DiscussionWhile improvement was shown on all subtests, it only
rose to statistical significance on subtests 1, 5, 6 & 10. Kirschner, et al., 2018 found that subtests 5, 6, 8 & 10 were comprised of more complex linguistic material. The findings of this study support the need for personal amplification during assessment administration for individuals with hearing impairment. Without auditory accommodations, individuals may yield longer response time, inaccurate results, and are ultimately at risk for misdiagnosis.
Qualitative data obtained via questionnaire further described the increased vocal intensity modification as “distracting”, whereas the feedback related to the personal amplification device was described as “helpful” and “comfortable”. Clinician feedback additionally described the ease of use for the personal amplification device compared to the strain and ‘discomfort” caused by the raised intensity method. In line with American Speech-Language- Hearing Association (ASHA) guidelines to alleviate vocal misuse and abuse, researchers recommend the use of a personal amplification device as speaking with sustained or repeated raised volume can lead to vocal damage, such as vocal nodules (ASHA, 2020).
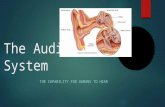
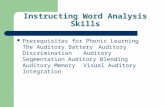
Dependent t-tests were used to determine if the response time (RT) for participants with HL using accommodations approached the average RT for participants with normal hearing. Analysis revealed that participants in Group B, when using personal amplification, approximated RT of participants in Group A (non-hearing impaired). Analysis of the results for Group C revealed no statistically significant change in RT. The increased vocal intensity was shown to have a deleterious effect.
Depicted above, no significant improvements were made with the vocal amplification accommodation.
Many speech-language and cognitive-linguistic assessments contain tasks that rely on the test-takers’ hearing abilities. The testing modifications in assessments for language disorders is typically to speak more loudly. This is difficult to standardize and may negatively impact the clinician’s ability to measure outcomes and provide an optimal diagnosis. Given the relationship between cognitive processing speeds and the difficulties recognizing speech under adverse listening conditions (Wingfield & Peelle (2012), the current investigation examined the utilization of auditory modifications (i.e. personal amplification device vs. increased speaking intensity) during speech and language evaluations.
0
20
40
60
80
100
1 2 3 4 5 6 8 10Pr
oces
sing
Tim
e (s
econ
ds)
RIPA-2 Subtests
Personal Amplfier Analysis
Normal Hearing Hearing Loss Personal Amplifier & Hearing Loss
Significant improvements seen in subtests 1, 5, 6, & 10
0
20
40
60
80
100
1 2 3 4 5 6 8 10
Proc
essi
ng T
ime
(sec
onds
)
RIPA-2 Subtests
Vocal Intensity Analysis
Modified Unmodified