
Atrial Fibrillation Detection in the Community and … Fibrillation Detection in the Community and...
42
Atrial Fibrillation Detection in the Community and Hospital settings Shuja Punekar Consultant Cerebrovascular Physician Hon Senior Lecturer, Manchester Medical School
Transcript of Atrial Fibrillation Detection in the Community and … Fibrillation Detection in the Community and...

Atrial FibrillationDetection in the Community and
Hospital settingsShuja Punekar
Consultant Cerebrovascular Physician Hon Senior Lecturer, Manchester
Medical School

• How common is AF in the population• Permanent vs Paroxysmal AF• Subclinical forms of AF and risk of stroke• Are there certain groups of patients or
certain areas where we may find more than the usual number of AF patients?
• How can we improve identifying all patients with AF?

•What do the 3 slides show
•What is the unifying pathology

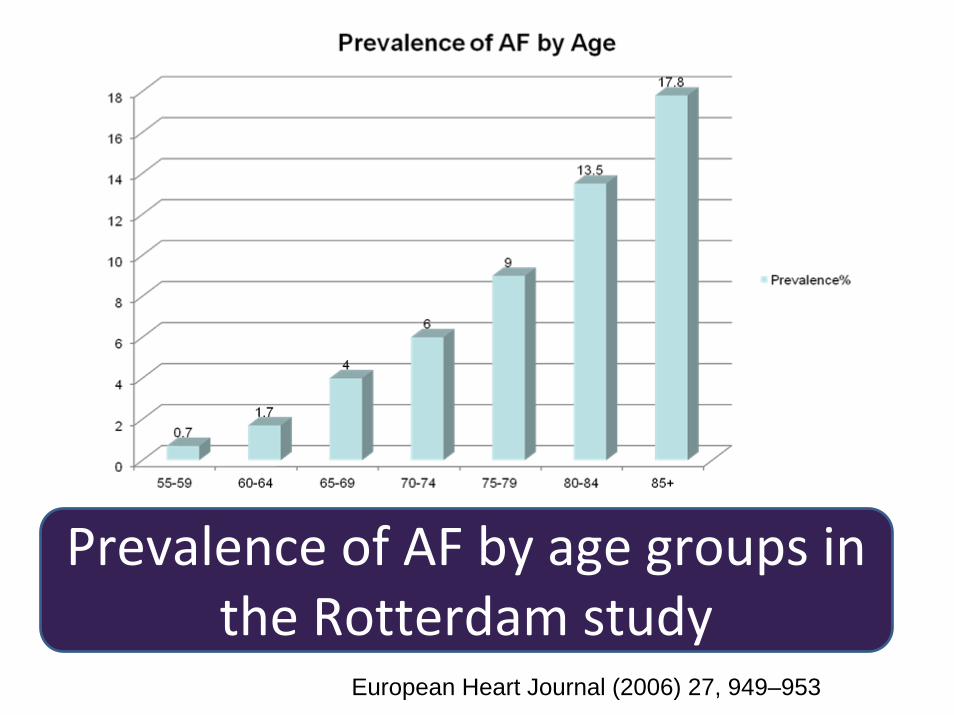
Prevalence of AF by age groups in the Rotterdam study
European Heart Journal (2006) 27, 949–953

Prevalence of AF in ScotlandAge and sex specific figures from the Renfrew‐
Paisley study from the West of Scotland. Note this study does not include patients 65 years of age or
older
Heart 2001;86:516–521

Approximate Prevalence of AF by age groups

Life Time Risk of AF at age 55Is approx
European Heart Journal (2006) 27, 949–953
Men
23.8%
Women
22.2%
1 in 4

Clinical Predictors for AF from the Renfrew‐Paisley study
Systolic BPOdds ratio 2.1 for SBP >/= 169 mm Hg
CardiomegalyOn CXR; Odds ratio 14
Heart 2001;86:516–521

Permanent AF
Paroxysmal AF
Subclinical AF

NICE recommends anticoagulation for eligible patients whether they have permanent or paroxysmal AF
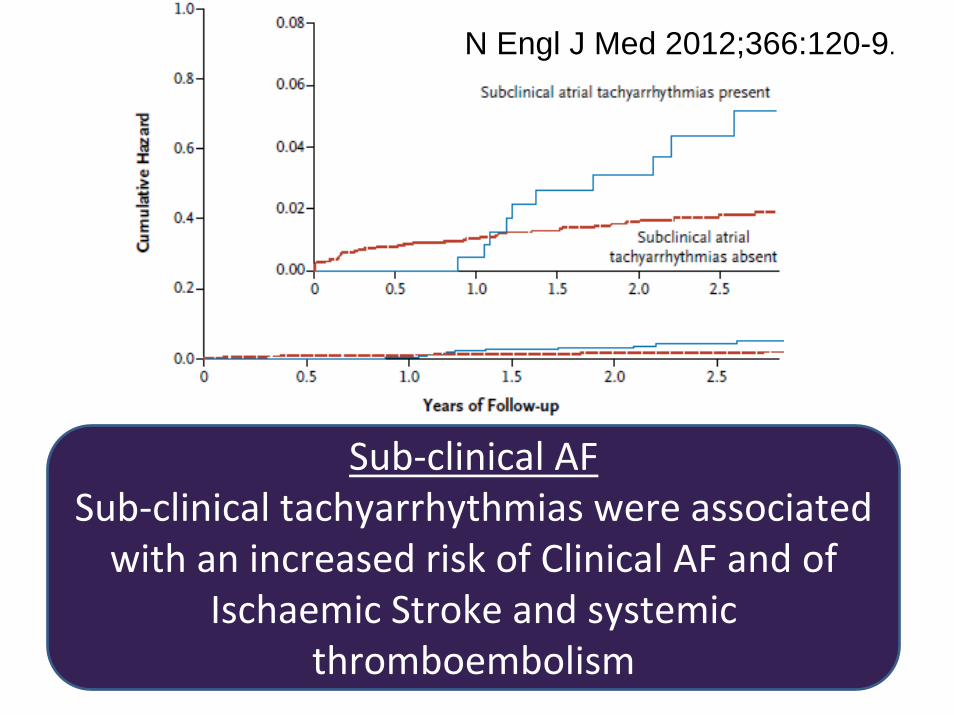
Sub‐clinical AFSub‐clinical tachyarrhythmias were associated with an increased risk of Clinical AF and of
Ischaemic Stroke and systemic thromboembolism
N Engl J Med 2012;366:120-9.

Warfarinreduces Stroke risk by
62%Aspirin
reduces Stroke risk by
22%

NNT• NNT to prevent 1 stroke per year of anticoagulation therapy in
secondary prevention (ARR: 8.5%) = 12
• NNT in primary prevention = 37
HEARTJNL/2005/066944
NNT for Secondary Prevention
= 12
NNT for Primary
Prevention = 37

How good are we in achieving target INR in patients on warfarin

In most RCTs we see ‘Time in Therapeutic Range’ (TTR) to be between 60 – 70 % as demonstrated here for AF patients on oral
anticoagulation.
Circ Cardiovasc Qual Outcomes 2008;1;84-91;

Time in therapeutic range (TTR) predicts adverse outcomes – both thromboembolic and haemorrhagic in AF patients on oral anticoagulation (weighted sample sizes); p values were significant for retrospective studies and not RCTs; Graph shows all studies - big circles are mostly RCTs
Circ Cardiovasc Qual Outcomes 2008;1;84-91;

Risk of Intracranial haemorrhage rises steeply for INRs over thetherapeutic range (Q J Med 2011; 104:747–760)

Improving Detection of AF in Hospitals
Acute Hospitals offer a great opportunity to detect almost all patients with AF and commence
adequate antithrombotic/anticoagulant
therapy

PrevalencePrevalence of AF in Acute Medical admissions in Preston500 consecutive acute medical admissions at RPH were screened for AF
50 years of age or over between 11 May and 1 June 2010
102 had AF; Prevalence = 20.4%59% were F and 41% MMean age was 78
Lucy Freeman, Shuja Punekar. 2010Awarded best student oral presentation at the UK Stroke Conference Nov/Dec 2010
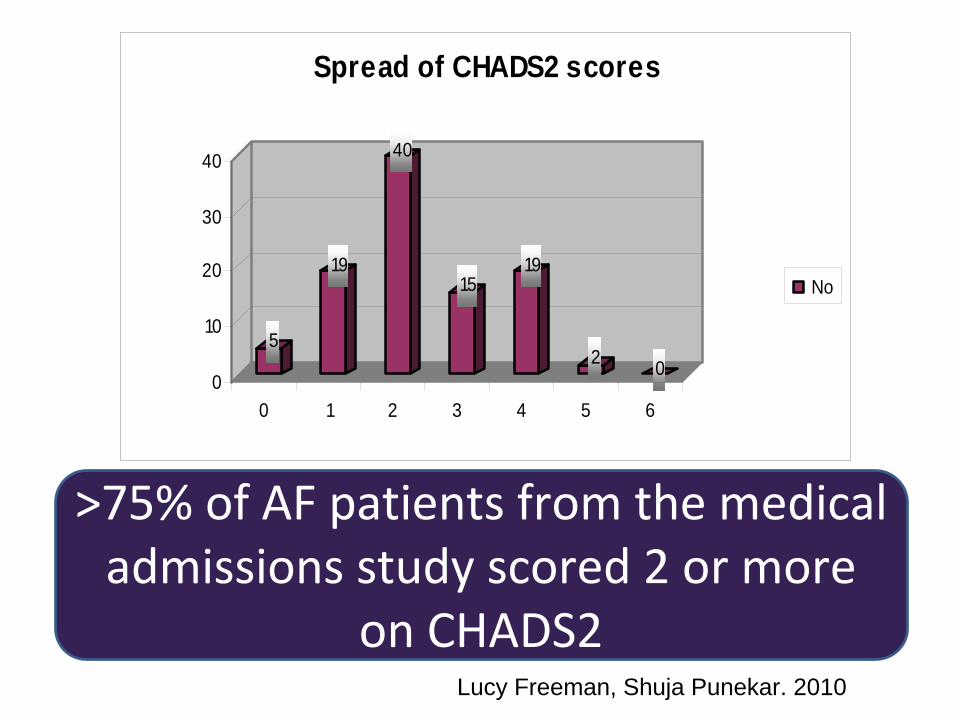
5
19
40
1519
2 00
10
20
30
40
0 1 2 3 4 5 6
Spread of CHADS2 scores
No
>75% of AF patients from the medical admissions study scored 2 or more
on CHADS2Lucy Freeman, Shuja Punekar. 2010

Type of AF Number of patients
New onset 26
Permanent 57
Paroxysmal 16
Persistent 1
Lucy Freeman, Shuja Punekar. 2010

5040
1005
101520253035404550
Warfarin Aspirin+ None
As many as 50% of patients were discharged only on Aspirin or no antithrombotic therapy at all
Lucy Freeman, Shuja Punekar. 2010

Improving Detection of AF the Community

Opportunistic Screening
• Take a pulse– For eg on all patients attending Flu
vaccinations at your practice and then confirm AF with an ECG if the pulse is irregular

• Colchester PBC Group incentivised 37 practices out of 43 to carry out screening of patients at Flu clinics for AF.
• These 37 practices screened 34,201 patients in six weeks, detecting 189 new patients with AF. The project prevented an estimated five strokes, representing an annual saving of £220,000 – a 322 per cent return on investment in addition to improved quality outcomes.
5 August 2010 Health Service Journal 25

AF in Care Homes

AF in Care HomesStudy Carried out in Care homes in Preston(May-June 2011)
McCrory S, Punekar SN; 2011

0
13.33 12.7718.58
26
66.66
0
10
20
30
40
50
60
70
51-60 61-70 71-80 81-90 91-100 100-110
Prevalence of AF in RH/NH homes by age groups
AF%
AF in Nursing/Care Homes StudyPrevalence of AF was similar to that found in other studies on the general population.
McCrory Simon, Punekar Shuja. Unpublished data

AF in the hospitalised elderly
A cross sectional survey was carried out at RPH on the 30th Jan 2012 and all elderly patients 75 years of age or over admitted in 4 medical wards were assessed for presence of AF
and their CHADS2 scores

Total No of patients 55
Mean age 85 years
Male/Female 25/30 45%/55%
Patients with AF 22 40%
Patients with AF & CHADS2 score of 2 or more
19 86.4%
40% of hospitalised elderly(75+yrs) were in AF and nearly 90% of those had a CHADS2 score
of 2 or above
Learning points
Hospitalised elderly (75+) have a very high risk of being in AF – 40%
Hospitalised elderly patients with AF invariably have high CHADS2 scores

Turning the CHADS2 on it’s head and using it to detect AF instead

Those who had a CHADS2 score of 2 or more were more likely to have AF vs those whose CHADS2 was <2
(48.72% vs 18.75% )
Is there evidence that we can improve outcomes by managing
the risk factors

Lancet 2004; 363: 1925–33
•Age-specific incidence rates of non-minor Stroke in the OCSP(1981) and the Oxvasc(2004) studies in Oxford showing a significant decline•As shown here the incidence of Stroke is improving in the general population

Age-standardized mortality rates in the Oxford region 1979 to 2004 (with 95% confidence intervals) and England 1996 to 2004,comparing underlying cause and mentions.‘Underlying cause’ as mentioned in the death certificate; ‘Mentions’ = any mention on the death certificate
Stroke. 2008;39:2197-2203.
Stroke Mortality is Falling in England

CVD Mortality - rate /000 popn - All persons under 75
0
50
100
150
200
250
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Chorley
Preston
South Ribble
West Lancashire
Central Lancashire
England
Source: Central Lancs PCT Data includes Stroke, IHD and all cardiovascular causesPer 100,000 population
Cardiovascular and Stroke Mortality in Lancashire

Why is the incidence of Stroke (and CV disease) improving

Premorbid medication inIncident first-ever TIA or Stroke in the OCSC and OxVasc studies – Note the rise in allMedications.(Primary prevention is in patients with no previous evidence of vascular disease.)
Lancet 2004; 363: 1925–33
We are managing risk factors much better now

Thank you









![Acoustic Emission Partial Discharge Detection Technique ... · T. Bhavanishanker, H.N. Nagamani,G.S. Punekar 191 [14 – 16]. The team has conducted more than 200 such tests at utility](https://static.fdocuments.net/doc/165x107/5f0520077e708231d4116454/acoustic-emission-partial-discharge-detection-technique-t-bhavanishanker-hn.jpg)








