Associations between Kidney Function and Subclinical Cardiac Abnormalities in CKD Park M et al. JASN...
24
Associations between Kidney Function and Subclinical Cardiac Abnormalities in CKD Park M et al. JASN September 2012 Renal Journal Club Oct 2012 BHH Matthew Graham-Brown
-
Upload
ericka-cavill -
Category
Documents
-
view
214 -
download
0
Transcript of Associations between Kidney Function and Subclinical Cardiac Abnormalities in CKD Park M et al. JASN...

Associations between Kidney Function and Subclinical Cardiac Abnormalities in CKD
Park M et al. JASN September 2012
Renal Journal Club Oct 2012 BHHMatthew Graham-Brown

Introduction
• CKD is associated with increased CVS risk and mortality, with an increased incidence of heart failure…….this is well known!!
• More recent studies have demonstrated cardiac abnormalities develop much sooner than previously anticipated [1,2]

Previous studies
• Several studies have evaluated associations between kidney function and LVH in patients with advanced disease, and in those requiring dialysis, [3,4] and there are some looking at associations in earlier disease, as well as some small studies looking at diastolic dysfunction and CKD.
• Study premise: Among patients without known HF, the associations at different stages of eGFR with changes in cardiac structure and function are not well described

What’s different about this study?
• ‘No study has characterised the associations of different stages of eGFR with the range of changes in cardiac structure and function in a large cohort of patients with established CKD’
• ‘It is testing the hypothesis that cardiac structural changes are a key factor in the pathogenesis leading from reduced kidney function to accelerating HF risk’
• Hypothesis: Subclinical cardiac changes start early in CKD, and the associations strengthen as CKD progresses

Study design
• The Chronic Renal Insufficieny Cohort (CRIC) study was established in 2001
• Observational study to evaluate the determinants of progression to ESRD and of CVS disease in patients with CKD
• Participants recruited from 7 centres from 2003 – 2008.

Inclusion Criteria
• eGFR : 20 – 70 for patients aged 21 – 44• eGFR : 20 – 60 for patients aged 45 – 64• eGFR : 20 – 50 for patients aged 65 – 74

Exclusion Criteria
• Prior Transplant• APKD• Multiple Myeloma• Use of immunosuppression• ‘Severe co-morbid illness’ (cirrhosis, HIV)• Severe HF (NYHA III – IV)
• Of the 3939 initially found in CRIC, a further 443 were excluded as they had a ‘physician’ diagnosis of HF at baseline

Methods
• Echocardiogram was performed at 1 year after recruitment into study – structural and functional data recorded and sent to a central lab for analysis
• 2% of all ECHOs checked for reproducibility
• Primary predictor of kidney function was eGFR using cystatin C

Cystatin-C
• A protein produced by all body cells with a nucleus.
• It’s physiological function is to inhibit breakdown of lysosomal proteinases.
• Major advantage is that it’s levels do not vary depending on muscle mass or protein in diet (unlike creatinine)
• May also be useful in predicting early onset CVS disease

Methods
• Primary measures:1. LVH and geometry (+LV Mass)2. LV systolic function3. LV diastolic function

Results – basic demographic details
• 3487 participants in total with appropriate eGFRs and without HF
• Mean age – 59 +/- 11 years• 45% female• 40% were black• Mean eGFRcys was 50 +/- 20• Mean eGFRcr was 41 +/- 15

Results – Kidney Function and Structural Heart Abnormalities
• A linear association between decline kidney function and increase in LV mass
• Linear regression and multi-variant analyses showed a strong association for all categories between eGFR and LV mass
– Only 21% of patients had normal LV geometry (dimensions)– 30% had concentric remodelling– 13% had eccentric hypertrophy– 36% had concentric hypertrophy

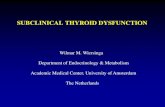
Mean LV mass (g/m2.7) increases across categories of declining eGFR by cystatin C.
Park M et al. JASN 2012;23:1725-1734
©2012 by American Society of Nephrology

Results – Kidney Function and Structural Heart Abnormalities
• 50% of whole cohort found to have LVH:– 32% of patients with eGFR >60– 49% of patients with eGFR 45-59– 57% of patients with eGFR 30-44– 75% of patients with eGFR <30
Results similar for white and black patients

Results – Kidney Function and Functional Heart Abnormalities
• Diastolic function was normal in (only) 29% of total cohort
The majority (62%) had ‘mildly abnormal’ relaxation8% had moderately impaired diastolic function1% (only) had severely abnormal diastolic function
All levels of eGFR were associated with LV diastolic dysfunction, but after multi-variant adjustment, this only reached statistical significance in the category eGFR 45-59

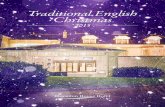
Categories of diastolic function by level of eGFRcys.
Park M et al. JASN 2012;23:1725-1734
©2012 by American Society of Nephrology

Results – Kidney Function and Functional Heart Abnormalities
• Systolic dysfunction (defined as EF < 45%) was present in 8% of the cohort.
• 82% had an EF > 50%• Only 2% had an EF < 35%
• There was no association between between decline in kidney function and systolic dysfunction

Summary
• Prevalence of LVH increases from 32% in patients with eGFR >60 to 75% in patients with eGFR < 30 …… this is the same as previous studies
• Strong association between declining kidney function and LV mass (adjusting for demographic bias) and the association progressed linearly in association with declining renal function

Summary
• Association between diastolic dysfunction and eGFR < 30 is strong, but linear decline with renal function is not present.
• As with previous studies, there is no association between reduced (or reducing) eGFR and systolic dysfunction

Discussion
• Suggestion is abnormalities in LV structure, and not function, precede the onset of clinical HF
• Strikingly high prevalence of abnormalities in LV mass (and geometry) in patients with CKD who have no signs or symptoms of HF
• ?May well represent the precursors of clinical HF, as patients with CKD are more likely to have HF in the absence of decreased LVEF

Discussion
• The high prevalence of patients with ‘mild’ diastolic dysfunction in this cohort, may have impeded the ability to detect graded association with decline in eGFR
• Absence of association with systolic dysfunction was predictable as patients with clinical HF were excluded by study design….

Discussion• Limitations
1. Lack of healthy control group2. Numbers not large enough to accurately demonstrate any differences
between ethnic groups3. Some ECHO data incomplete4. Cardiac MRI may be more cost-effective and give greater (and more
accurate) structural information5. Study is cross-sectional (and no controls), so causality and mechanisms for
proposed pathogenesis of HF cannot be proposed6. Duration of co-morbid illnesses could not be ascertained (important given
the relationship between BP and LVH)7. CRIC does not provide information about underlying cause for CKD, which
may have independent impact on LV structure and function8. Exclusion of patients with known HF means this study is NOT representative
of all patients with CKD

Conclusion(s)• Changes to practice??• Changes to understanding??
• ‘It is testing the hypothesis that cardiac structural changes are a key factor in the pathogenesis leading from reduced kidney function to accelerating HF risk’….
Hypothesis: Subclinical cardiac changes start early in CKD, and the associations strengthen as CKD progresses
• ‘As your kidney mass gets smaller your heart mass gets bigger’ – a good enough summary?!?

The end
• Thankyou