Association of religiosity and spirituality with quality ...promote a holistic approach in managing...
21
Vol.:(0123456789) 1 3 Quality of Life Research (2018) 27:2777–2797 https://doi.org/10.1007/s11136-018-1906-4 REVIEW Association of religiosity and spirituality with quality of life in patients with cardiovascular disease: a systematic review Hawa O. Abu 1 · Christine Ulbricht 1 · Eric Ding 1 · Jeroan J. Allison 1 · Elena Salmoirago‑Blotcher 2,3,4 · Robert J. Goldberg 1 · Catarina I. Kiefe 1 Accepted: 5 June 2018 / Published online: 11 June 2018 © The Author(s) 2018 Abstract Purpose This review systematically identified and critically appraised the available literature that has examined the associa- tion between religiosity and/or spirituality (R/S) and quality of life (QOL) in patients with cardiovascular disease (CVD). Methods We searched several electronic online databases (PubMed, SCOPUS, PsycINFO, and CINAHL) from database inception until October 2017. Included articles were peer-reviewed, published in English, and quantitatively examined the association between R/S and QOL. We assessed the methodological quality of each included study. Results The 15 articles included were published between 2002 and 2017. Most studies were conducted in the US and enrolled patients with heart failure. Sixteen dimensions of R/S were assessed with a variety of instruments. QOL domains examined were global, health-related, and disease-specific QOL. Ten studies reported a significant positive association between R/S and QOL, with higher spiritual well-being, intrinsic religiousness, and frequency of church attendance positively related with mental and emotional well-being. Approximately half of the included studies reported negative or null associations. Conclusions Our findings suggest that higher levels of R/S may be related to better QOL among patients with CVD, with varying associations depending on the R/S dimension and QOL domain assessed. Future longitudinal studies in large patient samples with different CVDs and designs are needed to better understand how R/S may influence QOL. More uniformity in assessing R/S would enhance the comparability of results across studies. Understanding the influence of R/S on QOL would promote a holistic approach in managing patients with CVD. Keywords Religiosity · Spirituality · Quality of life · Global QOL · Health-related QOL · Cardiovascular disease Introduction Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide, with an estimated 17.7 million deaths from CVD in 2015 [1]. Patients with CVD experience numerous physical symptoms including fatigue, dyspnea, or chest pain, which affects their physical, emotional, and social well-being with significant impair- ment in quality of life (QOL) [2]. While current strategies for the management of patients with CVD are designed to reduce morbidity and prolong survival, treatment should also be focused on improving patient’s QOL by reducing their symptoms, optimizing life’s daily functions, and overall well-being [2, 3]. Cardiac rehabilitation programs involving lifestyle modification, psychological interventions, educa- tion, and counseling have been shown to limit the adverse physiologic and psychologic effects associated with cardiac illness and enhance patient’s QOL [4]. Electronic supplementary material The online version of this article (https://doi.org/10.1007/s11136-018-1906-4) contains supplementary material, which is available to authorized users. * Hawa O. Abu [email protected] 1 Department of Quantitative Health Sciences, University of Massachusetts Medical School, 368 Plantation Street, Worcester, MA 01605, USA 2 Centers for Behavioral and Preventive Medicine, The Miriam Hospital, Providence, RI 02903, USA 3 Department of Epidemiology, Brown School of Public Health, Providence, RI 02903, USA 4 Warren Alpert School of Medicine & School of Public Health, Brown University, Providence, RI 02903, USA
Transcript of Association of religiosity and spirituality with quality ...promote a holistic approach in managing...

Vol.:(0123456789)1 3
Quality of Life Research (2018) 27:2777–2797 https://doi.org/10.1007/s11136-018-1906-4
REVIEW
Association of religiosity and spirituality with quality of life in patients with cardiovascular disease: a systematic review
Hawa O. Abu1 · Christine Ulbricht1 · Eric Ding1 · Jeroan J. Allison1 · Elena Salmoirago‑Blotcher2,3,4 · Robert J. Goldberg1 · Catarina I. Kiefe1
Accepted: 5 June 2018 / Published online: 11 June 2018 © The Author(s) 2018
AbstractPurpose This review systematically identified and critically appraised the available literature that has examined the associa-tion between religiosity and/or spirituality (R/S) and quality of life (QOL) in patients with cardiovascular disease (CVD).Methods We searched several electronic online databases (PubMed, SCOPUS, PsycINFO, and CINAHL) from database inception until October 2017. Included articles were peer-reviewed, published in English, and quantitatively examined the association between R/S and QOL. We assessed the methodological quality of each included study.Results The 15 articles included were published between 2002 and 2017. Most studies were conducted in the US and enrolled patients with heart failure. Sixteen dimensions of R/S were assessed with a variety of instruments. QOL domains examined were global, health-related, and disease-specific QOL. Ten studies reported a significant positive association between R/S and QOL, with higher spiritual well-being, intrinsic religiousness, and frequency of church attendance positively related with mental and emotional well-being. Approximately half of the included studies reported negative or null associations.Conclusions Our findings suggest that higher levels of R/S may be related to better QOL among patients with CVD, with varying associations depending on the R/S dimension and QOL domain assessed. Future longitudinal studies in large patient samples with different CVDs and designs are needed to better understand how R/S may influence QOL. More uniformity in assessing R/S would enhance the comparability of results across studies. Understanding the influence of R/S on QOL would promote a holistic approach in managing patients with CVD.
Keywords Religiosity · Spirituality · Quality of life · Global QOL · Health-related QOL · Cardiovascular disease
Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide, with an estimated 17.7 million deaths from CVD in 2015 [1]. Patients with CVD experience numerous physical symptoms including fatigue, dyspnea, or chest pain, which affects their physical, emotional, and social well-being with significant impair-ment in quality of life (QOL) [2]. While current strategies for the management of patients with CVD are designed to reduce morbidity and prolong survival, treatment should also be focused on improving patient’s QOL by reducing their symptoms, optimizing life’s daily functions, and overall well-being [2, 3]. Cardiac rehabilitation programs involving lifestyle modification, psychological interventions, educa-tion, and counseling have been shown to limit the adverse physiologic and psychologic effects associated with cardiac illness and enhance patient’s QOL [4].
Electronic supplementary material The online version of this article (https ://doi.org/10.1007/s1113 6-018-1906-4) contains supplementary material, which is available to authorized users.
* Hawa O. Abu [email protected]
1 Department of Quantitative Health Sciences, University of Massachusetts Medical School, 368 Plantation Street, Worcester, MA 01605, USA
2 Centers for Behavioral and Preventive Medicine, The Miriam Hospital, Providence, RI 02903, USA
3 Department of Epidemiology, Brown School of Public Health, Providence, RI 02903, USA
4 Warren Alpert School of Medicine & School of Public Health, Brown University, Providence, RI 02903, USA

2778 Quality of Life Research (2018) 27:2777–2797
1 3
The World Health Organization defines QOL as ‘a broad ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships and their relationship to salient features of their environment’ [5]. Global QOL broadly assesses the overall impact of disease on an individual’s life, while health-related QOL (HRQOL) focuses on the impact of health conditions and their symptoms on patients’ well-being [6]. Prior studies in patients with CVD have identified QOL as a sensitive patient-reported outcome measure of various intervention strategies [7], as an independent determinant of survival among patients with CVD [8, 9], and have reported a gradual decline in QOL with increasing number of CVD risk factors present [10, 11].
There is no consensus as to the definitions of “religiosity” or “spirituality.” For purposes of this systematic review, we have utilized working definitions of religiosity/spirituality (R/S) used in the prior literature [12, 13]. Religious practices and spiritual beliefs influence coping mechanisms in deal-ing with various chronic illnesses [14–16]. In many patients with CVD, R/S are important and highly personal aspects of their disease experience and provide vital strategies for cop-ing [17]. Studies on the relationship between R/S and QOL among patients with various forms of CVD have, however, demonstrated mixed results. While several reviews have examined factors associated with QOL in patients with CVD [18, 19], the association between R/S and global or HRQOL among patients with CVD has received limited attention.
The objective of this systematic review is to summarize and critically appraise available evidence on the association between R/S and QOL in patients with CVD. Understanding this relationship may help in developing intervention strate-gies to promote spiritual well-being and to optimize QOL in patients with chronic CVD.
Methods
This review was registered in the international prospective registry of systematic reviews PROSPERO (identification #: CRD42017076970) and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20].
Search strategy
We searched four electronic databases (PubMed, SCO-PUS, PsycINFO, and Cumulative Index to Nursing and Allied Health Literature (CINAHL)) from database incep-tion with no constraints on publication year. All searches were conducted between September 15, 2017 and Octo-ber 20, 2017. Two reviewers (H.O.A and C.U) worked in conjunction with two medical research librarians to create
a search algorithm that used Medical Subject Headings (MeSH) terms and key words related to “religiosity” and “spirituality” (including related terms religious, religious-ness, and spiritual) in combination with “quality of life” (and its associated synonyms HRQOL and well-being), and “cardiovascular disease” (with related terms acute myocardial infarction, acute coronary syndrome, congen-ital heart disease, rheumatic heart disease, heart failure, and cardiac surgery). The reference sections of eligible full-text articles were examined to identify additional studies suitable for inclusion. The full search algorithm is presented in an electronic supplementary material (Online Resource 1).
Eligibility criteria
We included only full-text peer-reviewed articles pub-lished in English that provided quantitative data with no restriction on study design (observational, randomized controlled trials). Qualitative studies, case reports, and reviews were excluded. Studies of patients with various forms of CVD including heart failure, acute myocardial infarction, coronary heart disease, atrial fibrillation, and congenital heart disease were included. The study popu-lation included patients of all ages, at different stages of their care (in-hospital, community dwelling, rehabilita-tion), and those who received any form of cardiac treat-ment (medical or surgical). Studies were included if they specifically assessed patient’s R/S and assessed either patient’s HRQOL, global QOL, or disease-specific QOL as the primary study outcome. The included studies had to assess the direct relationships between R/S and QOL, and studies that examined R/S and QOL as potential mediators were excluded from further evaluation.
Review process
Study eligibility was assessed by an initial review of the arti-cle title followed by a review of the abstract. Full-text publi-cations were subsequently retrieved of eligible articles and those that met our inclusion criteria were retained for data abstraction. One reviewer (H.O.A) independently conducted the reviews, while another reviewer (E.D) determined the appropriateness of final article inclusion. The two review-ers (H.O.A and E.D) met weekly to discuss the eligibility of included studies, and the inter-rater agreement between both reviewers was calculated using Cohen’s Kappa statistic [21]. Any discrepancies related to article eligibility were dis-cussed and resolved with reference to the explicit eligibility criteria. If no consensus was reached, a co-author (C.U) pro-vided final judgement about article inclusion or exclusion.

2779Quality of Life Research (2018) 27:2777–2797
1 3
Data extraction
A standardized form was used to obtain relevant information from eligible articles including publication date, authors, coun-try of origin, study design, recruitment, completion rates, sam-ple size, and baseline characteristics of the study population. Detailed information was obtained regarding the measures of QOL and R/S including the scale used, number of items, dimensions captured, and the scoring system. The statistical measure(s) of association between R/S and the respective QOL measures were obtained. Two authors (H.O.A and E.D) com-pleted the data extraction process independently.
Study quality assessment
The methodological quality of identified studies was criti-cally appraised using a revised version of the Downs and Black quality rating scale [22]. The Downs and Black scale was originally developed to assess quality in clinical trials with a checklist consisting of 27 items and a maximum score of 32 points. Similar to prior systematic reviews [23, 24], we revised the scale to allow for the assessment of observational studies. The modified checklist comprised 13 items with a maximum score of 14 for assessing cross-sectional studies, and 18 items with a maximum score of 19 for longitudi-nal studies. For each study, a quality score (in percentages) was obtained by dividing the number of points earned by the total number the study was eligible to receive based on appropriate reporting of study objectives, methods, results, and validity. Given the limited number of studies identi-fied in this review, no exclusions were based on the quality assessment. Results of the methodological quality assess-ment are available in an electronic supplementary material (Online Resource 2).
Data synthesis
The included studies were too heterogeneous for a meta-analysis to be conducted. Heterogeneity between studies was observed in the varying approaches used to assess R/S, ranging from the different instruments used across studies to multiple dimensions of R/S examined; these issues have been acknowledged in prior systematic reviews [25, 26]. We provide a qualitative synthesis of the results obtained from the studies identified in our review.
Results
Study selection
Our database search retrieved 623 potentially relevant stud-ies, from which 229 duplicates were removed. Following
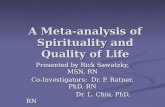
title and abstract review, 360 articles were excluded leav-ing 34 full-text articles to be screened for eligibility. We excluded 19 full-text articles that did not measure QOL or R/S, did not statistically assess the association between R/S and QOL, or treated R/S or QOL as mediators. The remaining 15 articles were included in this review. Agree-ment between the two reviewers on the selection of full-text articles was high (Cohen’s κ 0.90). No eligible articles were identified from the reference lists of included studies. Of the 15 publications in this review, four used data derived from a single cohort study [27–30], while two articles used data from another cohort investigation [31, 32]. Publications using data from the same cohort study were considered indi-vidually due to their varying study objectives and findings. Detailed results of our screening process are presented in Fig. 1.
Description of included studies
Study design and setting
The fifteen studies included in this review were published between 2002 and 2017; most were conducted in the US (n = 12, [27–38]) while others were carried out in Greece (n = 1, [39]), Iran (n = 1, [40]), and Korea (n = 1, [41]). All identified studies were observational; two-thirds used a cross-sectional design (n = 9, [30, 33–35, 37–41]), while six studies used a longitudinal design [27–32]. Study follow-up periods ranged from 3 months [27–29, 32] to 2 years [31]. Study sample sizes ranged from 58 to 163 patients with varying manifestations of CVD.
Patient characteristics
In all studies except for one, patients were typically mid-dle aged or older with the mean age at the time of study enrollment ranging from 53 to 67 years. The patient popu-lations were predominantly male (range 48–79%) and mar-ried (range 50–91%). The only exception was a study that included adult patients with congenital heart disease [41]; the mean age of these patients at study enrollment was 26.5 years and only 10.6% were married. Patient’s racial distribution was reported only in US-based studies with a predominance of non-Hispanic Whites (range 47–100%). Nine publications [27–33, 39, 40] reported religious affilia-tion. In the Greek study [39], all participants were Orthodox Christians; while in the Iranian study [40], all participants were Muslims. In the seven US-based studies that provided data on religious affiliation [27–33], most participants were Protestants (range 62–72%) or Catholics (range 16–29%). Eleven of the fifteen studies enrolled patients with heart fail-ure [27–30, 33–38, 40]), and the average time since diag-nosis varied between 6 months and 6.5 years. One study

2780 Quality of Life Research (2018) 27:2777–2797
1 3
[39] enrolled patients with varying diagnoses of CVD. Other studies included patients with a diagnosis of myocardial infarction [31, 32] and congenital heart disease [41]. Table 1 provides a detailed description of studies included in this systematic review.
Measures of R/S
The dimensions of R/S assessed in the identified studies included religious attitudes [40], religious, existential, and spiritual well-being [33, 37, 38], religious support [28], spiritual perspectives [34], strength and comfort from
religion [35], religious coping [28, 31, 32, 36], church ser-vice attendance [39], intrinsic religiousness [39], religious identification and religious struggle [27, 28], spiritual desires and constraints [30], spiritual and religious con-cerns [32], belief in the afterlife [28], forgiveness [28], and daily spiritual experience [27, 28, 30]. A variety of instru-ments were used to assess R/S (Table 2) ranging from a simple validated one-item scale [39] to a more complex 29-item scale [42]. Three instruments that assessed R/S were used in more than one study: the 12-item Functional Assessment of Chronic Illness Therapy (FACIT-Sp-12), a validated self-reported measure of overall spiritual
Records iden�fied through database searching(n = 623)
PubMed = 249Scopus = 212CINAHL = 87PsycInfo = 75
Scre
enin
gIn
clud
edEl
igib
ility
Iden
�fica
�on
Addi�onal records iden�fied through other sources
(n = 0)
Records a�er duplicates removed(n = 394)
Records screened(n = 394 )
Records excludedTitle ineligible (n =247)
Abstract ineligible (n= 113)Reasons for abstract exclusion Not published in English = 4Study popula�on not limited to CVD = 6Not peer reviewed = 7No measure of religiosity/spirituality (R/S) = 10No measure of Quality of Life (QOL) = 33No sta�s�cal measure of the associa�on between R/S and QOL=15Qualita�ve/Review studies = 38Full-text ar�cles assessed for
eligibility(n = 34) Full-text ar�cles excluded, with reasons
(n =19)QOL not assessed = 4No measure of R/S = 4R/S handled as mediators = 2No sta�s�cal measure of the associa�on between R/S and QOL= 7No separate results for pa�ents with CVD=2
Studies included in qualita�ve synthesis(n = 15)
Fig. 1 Flow diagram for systematic review methodology in accordance with PRISMA guidelines

2781Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
Sum
mar
y of
full-
text
arti
cles
incl
uded
in th
is sy
stem
atic
revi
ew
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Park
et a
l (2
011)
USA
[27]
Long
itudi
-na
l stu
dy
(3 m
onth
s du
ratio
n)
111
enro
lled;
10
1 fo
l-lo
wed
up
60.3
% m
enM
ean
age
(SD
) = 66
.7 y
ears
(1
1.0)
56%
Cau
casi
an39
% A
fric
an A
mer
ican
10%
Lat
ino
5% N
ativ
e A
mer
ican
60%
mar
ried
67%
pro
test
ant
16%
Cat
holic
1% Je
wis
h9%
no
relig
ious
affi
li-at
ion
Hea
rt fa
ilure
; mea
n le
ngth
of d
iagn
o-si
s = 6.
5 ye
ars
SD =
5.6
year
s
1. R
elig
ious
stru
ggle
mea
sure
d by
th
e re
ligio
us st
rain
scal
e2.
Rel
igio
us c
omfo
rt m
easu
red
with
th
e da
ily sp
iritu
al e
xper
ienc
e sc
ale
3. R
elig
ious
iden
tifica
tion
(mea
sure
d at
1 a
nd 3
mon
ths
resp
ectiv
ely)
1. H
RQ
OL
SF-1
22.
MLW
HFQ
(mea
sure
d at
bas
e-lin
e an
d 3
mon
ths r
espe
ctiv
ely)
1. C
orre
latio
n A
naly
sis
2. H
iera
rchi
cal
regr
essi
on
anal
ysis
1. A
t bas
elin
e, re
ligio
us
strug
gle
mea
sure
d w
as n
ot si
gnifi
cant
ly
corr
elat
ed w
ith p
hysi
cal
impa
irmen
t (r =
0.13
, p >
0.05
), as
wel
l as t
he
phys
ical
(r =
− 0.
11,
p > 0.
05) n
or m
enta
l (r
= 0.
06, p
> 0.
05) c
om-
pone
nts o
f HR
QO
L2.
Rel
igio
us st
rugg
le
mea
sure
d at
bas
elin
e w
as n
ot si
gnifi
cant
ly
corr
elat
ed w
ith p
hysi
cal
impa
irmen
t, (r
= 0.
20
p < 0.
10) a
s wel
l as t
he
phys
ical
(r =
− 0.
14,
p > 0.
05) n
or m
enta
l (r
= −
0.15
, p >
0.05
) co
mpo
nent
s of H
RQ
OL
mea
sure
d at
3 m
onth
s3.
Rel
igio
us st
rugg
le
at b
asel
ine
did
not
pred
ict c
hang
e in
QO
L co
mpa
ring
3 m
onth
s to
base
line
Park
et a
l (2
014)
USA
[28]
Long
itudi
-na
l stu
dy
(3 m
onth
s du
ratio
n)
111
enro
lled;
10
1 fo
l-lo
wed
up
60.3
% m
enM
ean
age
(SD
) = 66
.7 y
ears
(1
1.0)
56%
Cau
casi
an39
% A
fric
an A
mer
ican
10%
Lat
ino
5% N
ativ
e A
mer
ican
67%
Pro
test
ant
16%
Cat
holic
1% Je
wis
h9%
no
relig
ious
affi
li-at
ion
Mar
ital s
tatu
s not
re
porte
d
Hea
rt fa
ilure
; mea
n le
ngth
of d
iagn
o-si
s = 6.
5 ye
ars
SD =
5.6
year
s
1. R
elig
ious
stra
in sc
ale
2. B
MM
R/S
(mea
sure
d at
1 a
nd
3 m
onth
s, re
spec
tivel
y)
1. M
LWH
FQ2.
HR
QO
L-SF
12 (m
easu
red
at 1
an
d 3
mon
ths,
resp
ectiv
ely)
1. C
orre
latio
n an
alys
is2.
Hie
rarc
hica
l lo
ngitu
dina
l re
gres
sion
1. O
nly
one
dim
ensi
on o
f R
/S (i
.e.,
daily
spiri
tual
ex
perie
nce)
at 1
mon
th
was
sign
ifica
ntly
cor
-re
late
d w
ith p
hysi
cal
wel
l-bei
ng a
t 3 m
onth
s. (r
= −
0.29
, p <
0.05
)2.
Bel
ief i
n af
terli
fe a
t 1
mon
th w
as n
egat
ivel
y co
rrel
ated
with
men
tal
HR
QO
L at
3 m
onth
s (r
= −
0.21
, p <
0.05
)3.
In lo
ngitu
dina
l hi
erar
chic
al m
odel
s, no
dim
ensi
ons o
f R/S
pr
edic
ted
phys
ical
w
ell-b
eing

2782 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Sacc
o et
al
(201
4)U
SA [2
9]
Long
itudi
-na
l stu
dy
(3 m
onth
s du
ratio
n)
111
enro
lled
103
follo
wed
up
60.3
% m
enM
ean
age
(SD
) = 66
.7 y
ears
(1
1.0)
56%
Cau
casi
an39
% A
fric
an A
mer
ican
10%
Lat
ino
5% N
ativ
e A
mer
ican
67%
Pro
test
ant
16%
Cat
holic
1% Je
wis
h9%
no
relig
ious
affi
li-at
ion
Mar
ital s
tatu
s not
re
porte
d
Hea
rt fa
ilure
; mea
n le
ngth
of d
iagn
o-si
s = 6.
5 ye
ars
SD =
5.6
year
s
Ope
n-en
ded
ques
tions
on
copi
ng
with
illn
ess
HR
QO
L-SF
12C
orre
latio
n A
naly
sis
1. R
elig
ion/
Spiri
tual
ity
was
not
sign
ifica
ntly
co
rrel
ated
with
the
men
tal (
r = 0.
14,
p > 0.
05) n
or p
hysi
cal
(r =
-0.1
1, p
> 0.
05)
com
pone
nts o
f HR
QO
L m
easu
red
at b
asel
ine
2. R
elig
ion/
Spiri
tual
ity
mea
sure
d at
bas
elin
e w
as si
gnifi
cant
ly c
or-
rela
ted
with
onl
y th
e ph
ysic
al c
ompo
nent
of
HR
QO
L m
easu
red
3 m
onth
s afte
r enr
oll-
men
t (r =
0.20
, p <
0.05
)Pa
rk &
Sa
cco
(201
7)U
SA [3
0]
Cro
ss-s
ectio
nal
study
111
60.3
% m
enM
ean
age
(SD
) = 67
yea
rs (1
1.4)
56%
Cau
casi
an39
% A
fric
an A
mer
ican
10%
Lat
ino
5% N
ativ
e A
mer
ican
61%
mar
ried
67%
pro
test
ant
17%
Cat
holic
9% n
o re
ligio
us a
ffili-
atio
n<
1% Je
wis
h
Hea
rt fa
ilure
; mea
n le
ngth
of d
iagn
o-si
s = 6.
5 ye
ars
SD =
5.6
year
s
1. S
pirit
ual d
esire
s, co
nstra
ints
, and
ne
eds q
uesti
onna
ire2.
The
Dai
lySp
iritu
al E
xper
ienc
e su
bsca
le
of th
eB
MM
R/S
HR
QO
L-SF
12Su
bgro
up
regr
essi
on
anal
ysis
ac
cord
ing
to p
atie
nts
who
des
ired
spiri
tual
at
tend
ance
or
not
1. In
pat
ient
s who
des
ired
spiri
tual
atte
ndan
ce,
spiri
tual
con
strai
nt w
as
asso
ciat
ed w
ith p
oore
r ph
ysic
al q
ualit
y of
life
(β
= −
0.39
, p <
0.01
)2.
In p
atie
nts w
ho d
id
not d
esire
spiri
tual
at
tend
ance
, hav
ing
thei
r sp
iritu
al n
eeds
met
w
as a
ssoc
iate
d w
ith
high
er m
enta
l (β =
0.24
p <
0.10
) and
phy
sica
l qu
ality
of l
ife (β
= 0.
29,
p < 0.
05)

2783Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Trev
ino
et a
l (2
014)
USA
[31]
Long
itudi
nal
study
(2 y
ears
du
ratio
n)
Full
sam
-pl
e = 10
5A
naly
tic sa
m-
ple =
43
79%
men
Mea
n ag
e (S
D) =
60.2
yea
rs
(10.
9)10
0% W
hite
91%
mar
ried
72%
pro
test
ant
Firs
t tim
e M
yoca
rdia
l Inf
arct
ion
patie
nts o
r Pos
t-Cor
onar
y A
rtery
by
pass
Sur
gica
l
1. T
he R
elig
ious
Cop
ing
Act
iviti
es
Scal
e2.
The
Rel
igio
sity
Mea
sure
(mea
sure
d at
bas
elin
e, 1
yea
r, an
d 2
year
s)
QLM
I (m
easu
red
at b
asel
ine,
1
year
, and
2 y
ears
)Pe
arso
n co
rrel
atio
n an
alys
is
1. G
reat
er in
crea
se in
con
-se
quen
tial r
elig
iosi
ty
(r =
0.32
, p <
0.05
) and
ex
perie
ntia
l rel
igio
sity
(r
= 0.
34, p
< 0.
05) w
as
sign
ifica
ntly
cor
rela
ted
with
gre
ater
incr
ease
in
QO
L Li
m fr
om b
asel
ine
to 2
-yea
r fol
low
-up
2. G
reat
er in
crea
se in
re
ligio
us av
oida
nce
copi
ng (r
= 0.
35,
p < 0.
05) a
nd re
ligio
us
copi
ng to
tal s
core
s (r
= 0.
34, p
< 0.
05) w
as
sign
ifica
ntly
cor
rela
ted
with
gre
ater
incr
ease
in
QO
L Em
from
bas
elin
e to
2-y
ear f
ollo
w-u
pTr
evin
o et
al
(201
5)U
SA [3
2]
Long
itudi
nal
study
(12
wee
ks o
f ca
rdia
c re
ha-
bilit
atio
n)
105
77%
men
Mea
n ag
e (S
D) =
60.6
yea
rs
(11.
5)10
0% W
hite
91%
mar
ried
72%
pro
test
ant
Firs
t tim
e M
yoca
rdia
l Inf
arct
ion
patie
nts o
r Pos
t-Cor
onar
y A
rtery
by
pass
Sur
gica
l pat
ient
s
1. S
RQ
C2.
The
Rel
igio
sity
Mea
sure
3. T
he R
elig
ious
Cop
ing
Act
iviti
es
Scal
e
QLM
I (m
easu
red
at b
asel
ine
and
12 w
eeks
)Sp
earm
an
Ran
k co
rrel
atio
n an
alys
is o
f th
e ba
selin
e re
latio
nshi
p be
twee
n R
/S a
nd
QO
L; a
nd
betw
een
the
base
line
R/S
an
d Q
OL
chan
ges
1. N
o si
gnifi
cant
cor
-re
latio
ns b
etw
een
the
dim
ensi
ons o
f R/S
and
Q
OL
at b
asel
ine
2. N
o si
gnifi
cant
cor
-re
latio
n be
twee
n R
/S
mea
sure
d at
bas
elin
e an
d ch
ange
d va
lue
of
QO
L (1
2-w
eek
QO
L M
easu
re m
inus
bas
elin
e Q
OL
mea
sure
)

2784 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Bee
ry e
t al
(200
2)U
SA [3
3]
Cro
ss-s
ectio
nal
study
(fina
l pa
rt of
a
long
itudi
nal
study
)
5860
% m
enM
ean
age =
57 y
ears
90%
Eur
opea
n A
mer
ican
10%
Afr
ican
Am
eric
anRe
ligio
us A
ffilia
tion
62%
pro
test
ant
29%
Cat
holic
9% o
ther
Mar
ital s
tatu
s not
re
porte
d
Hea
rt Fa
ilure
No
indi
catio
n of
tim
e si
nce
diag
-no
sis
Spiri
tual
Wel
l-Bei
ng S
cale
1. In
dex
of W
ell-
Bei
ng2.
HR
QO
L-SF
363.
MLW
HFQ
Cor
rela
tion
Ana
lysi
s1.
Spi
ritua
l wel
l-bei
ng
was
cor
rela
ted
with
m
easu
res o
f glo
bal
QO
L (r
= 0.
49,
p ≤ 0.
001)
, hea
lth-
rela
ted
QO
L (M
CS:
r =
0.34
, p ≤
0.05
), an
d di
seas
e-sp
ecifi
c Q
OL
(phy
sica
l sym
ptom
s:
r = −
0.37
, p ≤
0.01
; em
otio
nal s
ympt
oms:
r =
− 0.
47, p
≤ 0.
001)
2. C
ombi
ned
spiri
tual
ity
scor
e pr
edic
ted
24%
of
the
varia
nce
in g
loba
l qu
ality
of l
ifeW
estla
ke
et a
l (2
002)
U
SA
[34]
Cro
ss-s
ectio
nal
study
6174
% m
enM
ean
age
(SD
) = 56
.8 y
ears
(1
3.8)
84%
Whi
te15
% H
ispa
nic
2% B
lack
72%
mar
ried
No
relig
ious
affi
liatio
n re
porte
d
Hea
rt Fa
ilure
At l
east
6 m
onth
s sin
ce d
iagn
osis
Spiri
tual
Per
spec
tive
Scal
eH
RQ
OL-
SF36
1. C
orre
latio
n A
naly
sis
2. M
ultip
le
linea
r re
gres
sion
1. S
pirit
ualit
y w
as n
ot
sign
ifica
ntly
cor
rela
ted
with
the
phys
ical
(r
= 0.
03, p
= 0.
81)
nor m
enta
l com
pone
nt
of H
RQ
OL
(r =
0.04
, p =
0.75
)2.
In th
e m
ultiv
aria
ble
anal
ysis
, spi
ritua
lity
was
not
ass
ocia
ted
with
th
e ph
ysic
al (β
= 0.
17,
p = 0.
28) n
or m
enta
l co
mpo
nent
of H
RQ
OL
mea
sure
(β =
0.08
, p =
0.54
)B
linde
r-m
an
et a
l (2
008)
USA
[35]
Cro
ss-s
ectio
nal
data
obt
aine
d at
bas
elin
e fro
m lo
ngitu
-di
nal s
tudy
103
71.8
% m
enM
ean
age
(SD
) = 67
.1 y
ears
(1
2.1)
73%
Whi
te13
% B
lack
10%
His
pani
c53
% m
arrie
dN
o re
ligio
us a
ffilia
tion
repo
rted
Con
gesti
ve h
eart
failu
re; t
ime
sinc
e di
agno
sis n
ot re
porte
dFA
CIT
-Sp-
4M
ILQ
Cor
rela
tion
Ana
lysi
sTh
e FA
CIT
-Sp
mea
sure
of
spiri
tual
ity w
as n
ot
sign
ifica
ntly
cor
rela
ted
with
MIL
Q (r
= 0.
16,
p = 0.
11)

2785Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Park
et a
l (2
008)
USA
[36]
Long
itudi
-na
l stu
dy
(6 m
onth
s du
ratio
n)
202
enro
lled
163
fol-
low
ed u
p
60.3
% m
enM
ean
age =
65.6
yea
rs67
% C
auca
sian
30%
Afr
ican
Am
eric
an3%
Lat
ino
and
othe
r ra
cial
cat
egor
ies
Mar
ital s
tatu
s not
re
porte
dRe
ligio
us a
ffilia
tion
not
repo
rted
Left-
side
d sy
stolic
con
gesti
ve h
eart
failu
re; d
iagn
osed
with
in o
ne y
ear
prio
r to
study
enr
ollm
ent
Relig
ious
cop
ing—
COPE
mea
sure
HR
QO
L-SF
36(m
easu
red
at b
asel
ine
and
6 m
onth
s of
follo
w-u
p)
Cor
rela
tion
Ana
lysi
sRe
ligio
us c
opin
g m
eas-
ured
at b
asel
ine
was
not
si
gnifi
cant
ly c
orre
late
d w
ith th
e ph
ysic
al
(r =
− 0.
11, p
> 0.
05)
nor m
enta
l (r =
− 0.
05,
p > 0.
05) c
ompo
nent
s of
HR
QO
L m
easu
red
at
6 m
onth
s
Bea
n et
al
(200
9)U
SA [3
7]
Cro
ss-s
ectio
nal
study
100
67%
men
Mea
n ag
e (S
D) =
53 y
ears
(14)
49.5
% A
fric
an A
mer
ican
47.4
% C
auca
sian
3.1%
His
pani
c51
.6%
mar
ried
No
relig
ious
affi
liatio
n re
porte
d
Hea
rt fa
ilure
; tim
e si
nce
diag
nosi
s no
t rep
orte
dFA
CIT
-Sp-
12M
LWH
FQC
orre
latio
n A
naly
sis
1. T
he m
eani
ng/p
eace
su
bsca
le o
f the
FA
CIT
-Sp
was
sign
ifica
ntly
co
rrel
ated
with
QO
L (r
= −
0.43
, p <
0.01
)2.
The
faith
subs
cale
of
the
FAC
IT-S
p w
as n
ot
sign
ifica
ntly
cor
rela
ted
with
QO
L (r
= −
0.06
, p >
0.05
)3.
The
tota
l sco
re o
f th
e FA
CIT
-Sp
was
si
gnifi
cant
ly c
orre
late
d w
ith Q
OL
(r =
− 0.
32,
p < 0.
01)
Bek
elm
an
et a
l (2
010)
USA
[38]
Cro
ss-s
ectio
nal
study
6063
.3%
men
Med
ian
age
[IQ
R] =
75 y
ears
[7
0.81
]11
.7%
Afr
ican
Am
eric
an50
.9%
mar
ried
No
relig
ious
affi
liatio
n re
porte
d
Hea
rt fa
ilure
; no
time
sinc
e di
agno
-si
s rep
orte
d1.
FA
CIT
-Sp-
122.
IWK
CC
Q-Q
OL
Pear
son
Cor
rela
tion
Ana
lysi
s
1. T
he m
eani
ng/p
eace
(r
= 0.
41, p
= 0.
001)
an
d fa
ith (r
= 0.
38,
p = 0.
003)
subs
cale
s of
the
FAC
IT-S
p w
ere
sign
ifica
ntly
cor
rela
ted
with
KC
CQ
-QO
L2.
The
faith
in G
od
subs
cale
of t
he IW
was
si
gnifi
cant
ly c
orre
late
d w
ith K
CC
Q-Q
OL
(r =
0.25
, p =
0.05
)3.
The
sens
e of
pea
ce
(r =
0.21
, p =
0.10
), re
ligio
us b
ehav
ior
(r =
0.09
, p =
0.52
), an
d co
mpa
ssio
nate
vie
w
(r =
− 0.
05, p
= 0.
73)
subs
cale
s of t
he IW
w
ere
not s
igni
fican
tly
corr
elat
ed w
ith K
CC
Q-
QO
L

2786 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Kar
ade-
mas
(2
010)
Gre
ece
[39]
Cro
ss-s
ectio
nal
study
135
67.4
% m
enM
ean
age
(SD
) = 60
.4 y
ears
(1
2.5)
83%
mar
ried
No
raci
al d
istrib
utio
nA
ll affi
liate
d to
the
Orth
odox
Chr
istia
n C
hurc
h
75.5
% M
yoca
rdia
l inf
arct
ion
14.1
%
Seve
re a
ngin
a pe
ctor
is6.
7% A
rrhy
thm
ias
3.7%
hea
rt fa
ilure
; mea
n tim
e (S
D)
sinc
e di
agno
sis =
10.7
yea
rs (6
.4)
1. In
trins
ic re
ligio
usne
ss2.
Fre
quen
cy o
f chu
rch
serv
ice
atte
ndan
ceR
AN
D H
ealth
Su
rvey
-Phy
sica
l fu
nctio
ning
and
Em
otio
nal w
ell-
bein
g sc
ales
1. P
ears
on
Cor
rela
tion
Ana
lysi
s2.
Hie
rarc
hica
l re
gres
sion
an
alys
es
1. In
trins
ic re
ligio
us-
ness
was
sign
ifica
ntly
co
rrel
ated
with
phy
sica
l fu
nctio
ning
(r =
0.26
, p <
0.01
) and
em
otio
nal
wel
l-bei
ng (r
= 0.
32,
p < 0.
001)
2. F
requ
ency
of c
hurc
h se
rvic
e at
tend
ance
w
as si
gnifi
cant
ly c
or-
rela
ted
with
em
otio
nal
wel
l-bei
ng (r
= 0.
20,
p < 0.
05) b
ut n
ot w
ith
phys
ical
func
tioni
ng
(r =
0.06
, p >
0.05
)3.
Intri
nsic
relig
ious
-ne
ss w
as a
sign
ifica
nt
pred
icto
r of p
hysi
cal
func
tioni
ng (β
= 0.
29,
t = 3.
08p <
0.01
) and
em
otio
nal
wel
l-bei
ng (β
= 0.
28,
t = 3.
05, p
< 0.
001)
4. F
requ
ency
of c
hurc
h se
rvic
e at
tend
ance
w
as o
nly
a si
gnifi
cant
pr
edic
tor o
f em
otio
nal
wel
l-bei
ng (β
= 0.
20,
t = 2.
02, p
< 0.
05)
Has
an
et a
l (2
017)
Ir
an [4
0]
Cro
ss- s
ectio
nal
study
130
47.7
% m
enM
ean
age
(SD
) = 59
.5 y
ears
(1
2.5)
76.9
% M
arrie
dRe
ligio
us a
ffilia
tion:
all
Mus
lims
No
raci
al d
istrib
utio
n pr
ovid
ed
Hea
rt Fa
ilure
At l
east
one
year
sinc
e di
agno
sis
Isla
mic
relig
ious
atti
tude
que
stion
naire
HR
QO
L-SF
361.
Pea
rson
C
orre
latio
n2.
Mul
tiple
lin
ear
regr
essi
on
1. S
igni
fican
t cor
rela
-tio
n be
twee
n re
ligio
us
attit
udes
and
QO
L in
th
e m
enta
l (Pe
arso
n’s
r = 0.
19, p
= 0.
03)
and
gene
ral h
ealth
di
men
sion
s (Pe
arso
n’s
r = 0.
19, p
= 0.
04)
2. N
o si
gnifi
cant
cor
rela
-tio
n be
twee
n re
ligio
us
attit
udes
and
phy
sica
l as
pect
of Q
OL
(Pea
r-so
n’s r
= 0.
04, p
= 0.
66);
nor t
otal
QO
L sc
ores
(P
ears
on’s
r =
0.10
, p =
0.30
)

2787Quality of Life Research (2018) 27:2777–2797
1 3
well-being that assesses “Meaning/Peace” and “Faith” [43], the Brief Multidimensional Measure of Religion/Spirituality (BMMR/S) [44], and the Religious strain scale [45]. Table 2 provides a description of the R/S instruments and scoring systems used in the included studies.
QOL outcomes
In contrast to the different measures of R/S, the QOL out-comes were more homogenous across studies (Table 3). Commonly reported outcomes were global QOL, mental or physical HRQOL, disease-related QOL, and dimensions of functional, emotional, or social well-being. Global QOL was assessed in three studies [33, 35, 41] with a different instrument used in each study: The Index of Well-Being [54], Short-version of The World Health Organization QoL assessment (WHOQOL-BREF) [55], and the Multidimen-sional Index of Life Quality (MILQ) [56]. Nine studies evaluated patients’ HRQOL using three instruments: The 36-item Medical Outcomes Study Questionnaire (SF-36) [57] was used in four studies [33, 34, 36, 40], the 12-item Short Form of the Medical Outcomes Study Questionnaire (SF-12) [58] was used in four studies [27–30], and the RAND 36-item Health Survey [59], a validated instru-ment adapted from the SF-36 that uses a simpler scor-ing system, was utilized in one study [39]. Five studies assessed disease-specific QOL with three instruments: The Minnesota Living with Heart Failure (MLHF) Question-naire [60] in two studies [33, 37], the Quality of Life after Acute Myocardial Infarction (QLMI) [61] in two studies [31, 32], and the Kansas City Cardiomyopathy Question-naire (KCCQ)-QOL subscale [62] in a single study [38].
Statistical analysis
Eight studies conducted a correlational analysis only [29, 31–33, 35–38], three studies conducted both correlation and hierarchical regression analyses [27, 28, 39], two stud-ies conducted both correlation and multiple linear regres-sion analyses [34, 40], one study utilized only multiple regression analysis [30], and another study used t tests to assess between group differences [41]. Correlation analysis was conducted between R/S and QOL measured at a single time point in cross-sectional studies [33–35, 37–40]. In studies using a longitudinal design, researchers examined the association between R/S measured at base-line and QOL during the course of follow-up [27–29, 31, 32, 36]. Socio-demographic variables commonly adjusted for in the regression analyses included age, gender, race, marital status, and education.
Tabl
e 1
(con
tinue
d)
Aut
hors
(p
ub.
year
)C
ount
ry
[ref
er-
ence
]
Stud
y de
sign
Sam
ple
size
Parti
cipa
nts
Type
of c
ardi
ovas
cula
r dis
ease
; tim
e si
nce
diag
nosi
sRe
ligio
sity
and
/or s
pirit
ualit
y m
easu
reQ
ualit
y-of
-life
mea
sure
Stat
istic
al
anal
ysis
Maj
or fi
ndin
gs
Ban
g et
al
(201
3)K
orea
[41]
Cro
ss-s
ectio
nal
study
8558
.5%
men
Med
ian
age
(SD
) = 26
.5 y
ears
(5.9
)10
.6%
Mar
ried
No
relig
ious
affi
liatio
n no
r rac
ial d
istrib
utio
n re
porte
d
Con
geni
tal H
eart
Dis
ease
Self-
repo
rted
as re
ligio
us (Y
es/N
o)W
HO
QO
L-B
REF
Stud
ent’s
t te
stPa
tient
s who
iden
tified
as
bei
ng re
ligio
us h
ad
high
er p
hysi
cal h
ealth
Q
OL
(60.
09 ±
12.7
4 vs
52
.64 ±
11.5
8; t =
2.71
9;
p va
lue <
0.01
) and
En
viro
nmen
t QO
L sc
ores
com
pare
d to
th
ose
who
did
not
iden
-tif
y as
bei
ng re
ligio
us
BMM
R/S
brie
f mul
tidim
ensi
onal
mea
sure
of r
elig
ion/
spiri
tual
ity, F
ACIT
-Sp
(FAC
IT-S
p-12
; FAC
IT-S
p-4)
the
func
tiona
l ass
essm
ent o
f chr
onic
illn
ess
ther
apy-
spiri
tual
wel
l-bei
ng (1
2-ite
m s
cale
; 4-
item
sca
le),
HRQ
OL
(SF3
6; S
F12)
Hea
lth-R
elat
ed Q
ualit
y-of
-Life
(the
36-
item
of t
he M
edic
al O
utco
mes
Stu
dy Q
uesti
onna
ire; t
he 1
2-ite
m s
hort
form
of t
he M
edic
al O
utco
mes
Stu
dy Q
ues-
tionn
aire
), IW
Iron
son–
Woo
ds S
pirit
ualit
y/Re
ligio
usne
ss In
dex,
KC
CQ
-QO
L Q
ualit
y-of
-life
Sub
scal
e of
the
self-
repo
rted
Kan
sas
City
Car
diom
yopa
thy
Que
stion
naire
, MC
S M
enta
l Com
pone
nt
Scor
e, M
ILQ
Mul
tidim
ensi
onal
Ind
ex o
f Li
fe Q
ualit
y, M
LWH
FQ M
inne
sota
Liv
ing
with
Hea
rt Fa
ilure
Que
stion
naire
, QLM
I Q
ualit
y of
life
afte
r A
cute
Myo
card
ial I
nfar
ctio
n Q
uesti
onna
ire,
QO
L Li
m Q
ualit
y-of
-life
Lim
itatio
ns, Q
OL
Em Q
ualit
y-of
-life
Em
otio
ns, S
RCQ
The
Spi
ritua
l and
Rel
igio
us C
once
rns
Que
stion
naire
, WH
O-B
REF
shor
t-ver
sion
of t
he W
orld
Hea
lth O
rgan
iza-
tion
QoL
ass
essm
ent

2788 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 2
Rel
igio
sity
and
/ or
spiri
tual
ity m
easu
res u
sed
in th
e in
clud
ed st
udie
s
Relig
iosi
ty a
nd/o
r spi
ritua
lity
mea
sure
[ref
eren
ce]
Num
ber
of it
ems
Instr
umen
t des
crip
tion
Scor
ing
syste
mSt
udie
s tha
t use
d m
easu
re in
this
re
view
Spiri
tual
des
ires,
cons
train
ts, a
nd n
eeds
que
stion
-na
ire [3
0]3
Instr
umen
t dev
elop
ed fo
r thi
s spe
cific
stud
y ba
sed
on p
rior q
ualit
ativ
e stu
dy fi
ndin
gs o
n sp
iritu
al
need
s. Ite
ms w
ere
“‘D
o yo
u w
ant y
our d
octo
r an
d ot
her h
ealth
care
pro
vide
rs to
atte
nd to
you
r sp
iritu
al n
eeds
?,’ ‘H
ow m
uch
do y
ou fe
el li
mite
d or
con
strai
ned
in d
iscu
ssin
g yo
ur sp
iritu
al is
sues
w
ith y
our d
octo
r and
oth
er h
ealth
car
e pr
ovid
ers?
,’ an
d ‘H
ow w
ell a
re y
our s
pirit
ual n
eeds
get
ting
met
rig
ht n
ow?.’
” N
o ps
ycho
met
ric p
rope
rties
of t
he
scal
e or
val
idat
ion
proc
edur
e w
ere
repo
rted
Resp
onse
s for
eac
h ite
m ra
nged
from
1 (n
ot a
t all)
to
4 (v
ery
muc
h/a
grea
t dea
l)[3
0]
Chu
rch
serv
ice
atte
ndan
ce [3
9]1
Sing
le it
em a
sses
sing
the
freq
uenc
y of
chu
rch
ser-
vice
atte
ndan
ce in
the
prev
ious
6 m
onth
sIte
m re
spon
se is
scor
ed u
sing
a fi
ve-p
oint
Lik
ert-
type
scal
e ra
ngin
g fro
m 1
(lea
st fr
eque
ncy
of
atte
ndan
ce) t
o 5
(mos
t fre
quen
t ser
vice
atte
nd-
ance
)
[39]
Isla
mic
relig
ious
atti
tude
que
stion
naire
[40]
25A
self-
repo
rt sc
ale
with
6 d
imen
sion
s on
lear
ning
an
d re
adin
g th
e Q
uran
; Kno
wle
dge
of G
od a
nd
faith
in G
od; b
elie
f in
afte
rlife
; atti
tude
to Is
lam
ic
relig
ious
ritu
als;
pos
itive
attr
ibut
es; d
evot
ion
to
relig
ious
wor
ship
; and
pra
ying
. The
instr
umen
t w
as d
evel
oped
for t
he p
urpo
se o
f the
stud
y [1
1].
Psyc
hom
etric
val
idat
ion
of th
e in
strum
ent w
as
cond
ucte
d w
ith te
st–re
test
corr
elat
ion
coeffi
cien
t of
0.8
6 an
d in
tern
al c
onsi
stenc
y C
ronb
ach’
s α
= 0.
89
4-po
int L
iker
t Sca
le w
ith re
spon
se it
ems r
angi
ng
from
1 =
stro
ngly
dis
agre
e to
4 =
stro
ngly
agr
ee[4
0]
The
Relig
ious
Cop
ing
Act
iviti
es S
cale
[42]
29A
val
idat
ed in
strum
ent w
hich
ass
esse
s the
deg
ree
to
whi
ch p
eopl
e us
e re
ligio
n to
cop
e w
ith st
ress
-fu
l life
eve
nts.
Six
type
s of r
elig
ious
cop
ing
are
asse
ssed
: spi
ritua
lly b
ased
act
iviti
es (1
2 ite
ms)
, go
od d
eeds
(6 it
ems)
, dis
cont
entm
ent (
3 ite
ms)
, in
terp
erso
nal r
elig
ious
supp
ort (
2 ite
ms)
, ple
adin
g an
d ba
rgai
ning
with
a S
upre
me
Bei
ng (3
item
s),
and
relig
ious
avoi
danc
e (3
item
s)
A 4
-poi
nt L
iker
t sca
le is
use
d to
ass
ess h
ow p
ar-
ticip
ants
rely
on
each
relig
ious
cop
ing
strat
egy.
H
ighe
r sco
res i
mpl
y gr
eate
r rel
ianc
e on
relig
ion
for c
opin
g. S
ubsc
ale
and
tota
l sco
res a
re d
eriv
ed
from
the
mea
n of
the
indi
vidu
al it
ems
[31,
32]
Func
tiona
l Ass
essm
ent o
f Chr
onic
Illn
ess T
hera
py
FAC
IT-S
p-12
[43]
12A
val
idat
ed se
lf-re
port
mea
sure
of o
vera
ll sp
iritu
al
wel
l-bei
ng. T
wo
subs
cale
s are
ass
esse
d: “
Mea
n-in
g/Pe
ace”
(8 it
ems)
and
Fai
th (4
item
s). T
he
mea
ning
/pea
ce su
bsca
le a
sses
ses o
ne’s
sens
e of
m
eani
ng, p
eace
, har
mon
y, a
nd li
fe’s
pur
pose
. The
fa
ith su
bsca
le m
easu
res t
he re
latio
nshi
p be
twee
n fa
ith, s
pirit
ual b
elie
fs, a
nd il
lnes
s, an
d se
ekin
g so
lace
in o
ne’s
faith
The
resp
onse
to e
ach
item
rang
es fr
om 0
(not
at a
ll)
to 4
(ver
y m
uch)
. A c
ompo
site
scor
e ra
ngin
g fro
m
0 to
48
is d
eriv
ed fr
om th
e su
bsca
les w
ith h
ighe
r sc
ores
indi
catin
g gr
eate
r spi
ritua
l wel
l-bei
ng
[37,
38]
Relig
ious
iden
tifica
tion
[44]
1A
val
idat
ed m
easu
re o
f the
ext
ent t
o w
hich
an
indi
-vi
dual
con
side
red
them
selv
es re
ligio
usSc
ored
from
0 (n
ot a
t all)
to 4
(ext
rem
ely)
. Dic
hoto
-m
ized
in th
e stu
dy a
s low
and
hig
h[2
7]

2789Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 2
(con
tinue
d)
Relig
iosi
ty a
nd/o
r spi
ritua
lity
mea
sure
[ref
eren
ce]
Num
ber
of it
ems
Instr
umen
t des
crip
tion
Scor
ing
syste
mSt
udie
s tha
t use
d m
easu
re in
this
re
view
Relig
ious
com
fort—
Dai
ly sp
iritu
al e
xper
ienc
e sc
ale
[44]
3Re
ligio
us c
omfo
rt as
sess
ed fr
om th
e D
aily
spiri
tual
ex
perie
nce
scal
e. R
espo
nden
ts ra
te h
ow th
ey fe
el
abou
t the
pre
senc
e of
God
, der
ived
com
fort
or
stren
gth
in th
eir r
elig
ion
or sp
iritu
ality
, and
exp
e-rie
nced
God
’s lo
ve d
irect
ly o
r via
oth
ers
Resp
onse
s ran
ge fr
om 0
(nev
er o
r alm
ost n
ever
to 6
(m
any
times
a d
ay),
with
hig
her s
core
s refl
ectin
g gr
eate
r rel
igio
us c
omfo
rt
[27]
Brie
f Mul
tidim
ensi
onal
Mea
sure
of R
elig
ion/
Spir-
itual
ity (B
MM
R/S
) [44
]23
The
follo
win
g di
men
sion
s of r
elig
ious
ness
/spi
ritua
l-ity
is a
sses
sed
with
the
BM
MM
R/S
: For
give
ness
(3
item
s), d
aily
spiri
tual
exp
erie
nces
(8 it
ems)
, be
lief i
n lif
e af
ter d
eath
(1 it
em),
relig
ious
iden
tity
(1 it
em),
relig
ious
supp
ort (
2 ite
ms)
, pub
lic re
li-gi
ous p
ract
ices
(2 it
ems)
, and
pos
itive
relig
ious
/sp
iritu
al c
opin
g (4
item
s)
Each
dim
ensi
on is
scor
ed se
para
tely
: For
give
ness
(1
–4),
daily
spiri
tual
exp
erie
nce
(1—
neve
r to
8—m
any
times
a d
ay),
belie
f in
life
afte
r dea
th (0
—no
, 1—
unde
cide
d, 2
—ye
s), r
elig
ious
iden
tity
(0—
not c
onsi
dere
d a
relig
ious
per
son
to 4
—ex
trem
ely
relig
ious
), re
ligio
us su
ppor
t (1—
none
to 4
—a
grea
t dea
l), p
ublic
relig
ious
pra
ctic
es (1
—ne
ver
to 8
—se
vera
l tim
es a
wee
k), p
ositi
ve R
/S c
opin
g (1
—no
t at a
ll to
4—
a gr
eat d
eal)
[28,
30]
Relig
ious
stru
ggle
—Re
ligio
us st
rain
scal
e [4
5]6
Instr
umen
t der
ived
from
the
brie
f ver
sion
of t
he
relig
ious
stra
in sc
ale.
Res
pond
ents
rate
thei
r ag
reem
ent w
ith th
e ite
ms o
n th
eir f
eelin
g of
ang
er
or a
liena
tion
from
God
Resp
onse
s ran
ge fr
om 0
(not
at a
ll) to
10
(ext
rem
ely)
. Sum
med
scor
es ra
nge
from
0 to
60,
w
ith h
ighe
r sco
res i
mpl
ying
gre
ater
relig
ious
str
uggl
e
[27,
28]
Spiri
tual
Wel
l-Bei
ng S
cale
[46]
20A
val
idat
ed 1
0-ite
m su
bsca
les a
sses
sing
relig
ious
w
ell-b
eing
(RW
B) a
nd e
xiste
ntia
l wel
l-bei
ng
(EW
B),
resp
ectiv
ely.
Item
s on
the
RWB
mak
e di
rect
refe
renc
e to
God
whi
le it
ems o
n th
e EW
B
mea
sure
a se
nse
of p
urpo
se o
r mea
ning
to li
fe
with
dire
ct re
fere
nce
to G
od
6-po
int L
iker
t sca
le w
here
hig
her n
umbe
rs in
dica
te
grea
ter e
ndor
sem
ent o
f the
stat
emen
t. N
ega-
tive
item
s are
reve
rsel
y sc
ored
. The
10
item
s are
sc
ored
from
10
to 6
0 an
d th
e sc
ores
from
the
two
subs
cale
s can
be
adde
d to
der
ive
an o
vera
ll sp
ir-itu
al w
ell-b
eing
scor
e ra
ngin
g fro
m 2
0 to
120
with
hi
gher
scor
es in
dica
ting
bette
r spi
ritua
l wel
l-bei
ng
[33]
The
Spiri
tual
Per
spec
tive
Scal
e [4
7]10
A v
alid
ated
mea
sure
of s
pirit
ualit
y w
ith a
dequ
ate
psyc
hom
etric
pro
perti
es. T
he it
ems m
easu
re th
e ex
tent
to w
hich
spiri
tual
ity p
erm
eate
s one
’s li
fe,
one’
s eng
agem
ent i
n sp
iritu
ally
rela
ted
inte
rac-
tions
, per
ceiv
ed sp
iritu
al p
ersp
ectiv
es, a
nd a
n in
divi
dual
s’ p
ract
ice
and
belie
f sys
tem
Ther
e ar
e 5
resp
onse
opt
ions
scor
ed fr
om 1
(not
at
all/
stron
gly
disa
gree
) to
6 (a
bout
onc
e a
day/
stron
gly
agre
e). T
he to
tal s
core
rang
es fr
om 1
0 to
60,
hig
her s
core
s ind
icat
e gr
eate
r spi
ritua
l per
-sp
ectiv
e an
d hi
gher
leve
ls o
f sel
f-tra
nsce
nden
ce
[34]
Func
tiona
l Ass
essm
ent o
f Chr
onic
Illn
ess T
hera
py
FAC
IT-S
p-4
[48]
4D
eriv
ed fr
om th
e FA
CIT
-Sp-
12. M
easu
res t
he
exte
nt o
f stre
ngth
and
com
fort
deriv
ed fr
om o
ne’s
fa
ith
Scor
es ra
nge
from
0 to
4, w
ith h
ighe
r sco
res i
ndic
at-
ing
grea
ter s
pirit
ualit
y[3
5]

2790 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 2
(con
tinue
d)
Relig
iosi
ty a
nd/o
r spi
ritua
lity
mea
sure
[ref
eren
ce]
Num
ber
of it
ems
Instr
umen
t des
crip
tion
Scor
ing
syste
mSt
udie
s tha
t use
d m
easu
re in
this
re
view
Relig
ious
cop
ing—
COPE
mea
sure
[49]
4Th
e CO
PE m
easu
re is
a v
alid
ated
60-
item
instr
u-m
ent w
ith 1
5 su
bsca
les t
hat m
easu
res h
ow
indi
vidu
als c
ope
with
stre
ssfu
l life
situ
atio
ns. T
he
Relig
ious
subs
cale
(4 it
ems)
ass
esse
s how
peo
ple
turn
to re
ligio
n by
seek
ing
God
’s h
elp,
put
ting
thei
r tru
st in
God
, find
ing
com
fort
in th
eir r
eli-
gion
, and
pra
ying
mor
e th
an u
sual
dur
ing
stres
sful
pe
riods
The
resp
onse
to e
ach
item
is sc
ored
from
1 (I
us
ually
do
not d
o th
is a
t all)
–4 (I
usu
ally
do
this
a
lot),
indi
catin
g th
e fr
eque
ncy
with
whi
ch a
n in
divi
dual
car
ries o
ut re
ligio
us c
opin
g. S
ubsc
ales
ar
e as
sess
ed in
divi
dual
ly w
ith sc
ores
rang
ing
from
4
to 1
6. H
ighe
r sco
res i
mpl
y gr
eate
r rel
igio
us
copi
ng
[36]
Irons
on–W
oods
Spi
ritua
lity/
Relig
ious
ness
Inde
x (I
W) [
50]
25A
val
idat
ed se
lf-re
port
instr
umen
t tha
t mea
sure
s sp
iritu
ality
in tw
o di
men
sion
s: tr
aditi
onal
reli-
giou
snes
s and
priv
ate
spiri
tual
ity. F
our s
ubsc
ales
as
sess
an
indi
vidu
als’
“se
nse
of p
eace
” (9
item
s),
“fai
th in
God
” (6
item
s), “
relig
ious
beh
avio
r” (5
ite
ms)
, and
“co
mpa
ssio
n vi
ew o
f oth
ers”
(5 it
ems)
Resp
onse
s ind
icat
e ho
w st
rong
ly o
ne a
gree
s with
ea
ch it
em w
ith sc
ores
from
1 (s
trong
ly d
isag
ree)
to
5 (s
trong
ly a
gree
)
[38]
Intri
nsic
relig
ious
ness
[51]
9Th
e In
trins
ic re
ligio
usne
ss su
bsca
le is
der
ived
from
th
e Re
ligio
us O
rient
atio
n Sc
ale
Resp
onse
s are
scor
ed u
sing
a fi
ve-p
oint
Lik
ert-t
ype
scal
e, w
ith lo
wer
scor
es in
dica
ting
high
er in
trins
ic
relig
ious
ness
[39]
The
Relig
iosi
ty M
easu
re [5
2]8
A v
alid
ated
instr
umen
t whi
ch a
sses
ses t
he im
pact
of
relig
ion
on a
n in
divi
dual
’s d
aily
life
. Com
pris
es
four
subs
cale
s with
two
item
s eac
h: ri
tual
relig
ios-
ity, c
onse
quen
tial r
elig
iosi
ty, i
deol
ogic
al re
ligio
s-ity
, and
exp
erie
ntia
l rel
igio
sity
. Ritu
al re
ligio
sity
as
sess
es th
e fr
eque
ncy
of a
ttend
ance
in re
ligio
us
serv
ices
, and
the
prac
tice
of m
edita
tion
or p
raye
r. C
onse
quen
tial r
elig
iosi
ty m
easu
res t
he e
xten
t to
whi
ch re
ligio
n aff
ects
resp
onde
nt’s
dec
isio
n an
d da
ily li
fe. I
deol
ogic
al re
ligio
sity
ass
esse
s bel
ief i
n a
Supr
eme
Bei
ng a
nd li
fe a
fter d
eath
. Exp
erie
ntia
l re
ligio
sity
ass
esse
s the
resp
onde
nt’s
relig
ious
de
votio
n an
d co
mfo
rt fro
m re
ligio
n
Each
item
is sc
ored
on
a 5-
poin
t Lik
ert s
cale
from
0
(leas
t rel
igio
sity
) to
4 (g
reat
est r
elig
iosi
ty) e
xcep
t th
e ite
m o
n re
ligio
us se
rvic
e at
tend
ance
that
is
scor
ed fr
om 1
to 4
with
incr
easi
ng fr
eque
ncy
of
serv
ice
atte
ndan
ce. E
ach
subs
cale
has
a m
axim
um
scor
e of
8 a
nd th
e ov
eral
l sco
re fo
r the
relig
iosi
ty
mea
sure
is 3
2
[31,
32]
The
Spiri
tual
and
Rel
igio
us C
once
rns Q
uesti
onna
ire
(SR
QC
) [53
]11
A v
alid
ated
instr
umen
t whi
ch a
sses
ses t
he st
reng
th
of sp
iritu
al b
elie
fs (7
item
s) a
nd re
ligio
us p
rac-
tices
(4 it
ems)
. Orig
inal
ly d
esig
ned
to a
sses
s spi
r-itu
al c
once
rns i
n ad
oles
cent
s who
wer
e ho
spita
l-iz
ed. A
dapt
ed fo
r use
in a
dult
popu
latio
n to
ass
ess
spiri
tual
con
cern
s bro
adly
and
in k
eepi
ng w
ith th
e re
spon
dent
’s il
lnes
s
Each
resp
onse
is sc
ored
from
1 (l
east
spiri
tual
/reli-
giou
s) to
9 (m
ost s
pirit
ual/r
elig
ious
). Th
e ov
eral
l sc
ore
is d
eriv
ed fr
om th
e m
ean
of th
e 11
item
s
[32]

2791Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 3
Qua
lity-
of-li
fe (Q
OL)
mea
sure
s use
d in
the
incl
uded
stud
ies
Qua
lity-
of-li
fe m
easu
rem
ent [
refe
renc
e]N
umbe
r of
item
sIn
strum
ent d
escr
iptio
nSc
orin
g sy
stem
Stud
ies w
hich
use
d m
easu
re in
this
re
view
Glo
bal q
ualit
y-of
-life
mea
sure
Inde
x of
Wel
l-Bei
ng [5
4]9
A v
alid
ated
mea
sure
of w
ell-b
eing
. Com
pris
es 8
sp
ecifi
c ite
ms a
bout
the
indi
vidu
al’s
per
cept
ion
of th
eir l
ife. T
he fi
nal i
tem
mea
sure
s the
ir ov
eral
l sa
tisfa
ctio
n w
ith li
fe. E
ach
item
is ra
ted
on a
7-
poin
t rat
ing
syste
m w
ith a
pos
itive
asp
ect o
n on
e en
d an
d a
nega
tive
aspe
ct a
t the
oth
er e
nd
The
first
8 ite
ms h
ave
a m
ean
wei
ghte
d at
1.0
whi
ch
is a
dded
to th
e sc
ore
for t
he la
st ite
m w
eigh
ted
at 1
.1. T
he to
tal p
ossi
ble
scor
es ra
nge
from
2.1
(lo
wes
t life
satis
fact
ion)
to 1
4.7
(hig
hest
life
satis
fact
ion)
[33]
Sho
rt-ve
rsio
n of
The
Wor
ld H
ealth
Org
aniz
atio
n Q
oL a
sses
smen
t (W
HO
QO
L-B
REF
) [55
]26
The
WH
OQ
OL-
BR
EF is
a sh
orte
ned
vers
ion
of th
e W
HO
QO
L-10
0 w
hich
pro
vide
s a d
etai
led
asse
ss-
men
t of Q
OL
but m
ay b
e to
o le
ngth
y fo
r pra
ctic
al
use.
24
item
s der
ived
from
the
WH
OQ
OL-
100
are
used
to a
sses
s fou
r dom
ains
incl
udin
g an
in
divi
dual
s’ p
erce
ptio
n of
thei
r phy
sica
l hea
lth
(7 it
ems)
, psy
chol
ogic
al h
ealth
(4 it
ems)
, soc
ial
rela
tions
hips
(3 it
ems)
, and
thei
r env
ironm
ent
(8 it
ems)
. Tw
o ad
ditio
nal q
uesti
ons a
sses
s the
ov
eral
l QO
L an
d ge
nera
l hea
lth
The
item
s are
use
d to
der
ive
a m
ean
scor
e fo
r the
ir re
spec
tive
dom
ain.
The
add
ition
al it
ems a
re ra
ted
on a
5-p
oint
Lik
ert s
cale
(1- l
east
scor
e to
5-h
igh-
est s
core
). Th
e m
ean
scor
e fo
r eac
h do
mai
n is
tra
nsfo
rmed
in tw
o st
ages
. Firs
t, th
e m
ean
scor
e is
mul
tiplie
d by
4 to
der
ive
a sc
ore
rang
ing
from
4
to 2
0 w
hich
is c
ompa
rabl
e w
ith th
e W
HO
-Q
OL-
100
scor
e. S
econ
d, th
e do
mai
n sc
ores
are
co
nver
ted
to a
0-1
00 sc
ale
with
hig
her s
core
s im
plyi
ng b
ette
r QO
L
[41]
Mul
tidim
ensi
onal
Inde
x of
Life
Qua
lity
(MIL
Q)
[56]
35Th
e M
ILQ
is a
val
idat
ed, p
atie
nt se
lf-re
porte
d in
strum
ent t
hat a
sses
ses 9
dom
ains
, nam
ely,
ph
ysic
al, c
ogni
tive,
and
soci
al fu
nctio
ning
; phy
si-
cal a
nd m
enta
l hea
lth; p
rodu
ctiv
ity, fi
nanc
ial
stat
us, i
ntim
acy,
and
rela
tions
hip
with
hea
lth
prof
essi
onal
s
Each
item
is sc
ored
on
a 7-
poin
t Lik
ert s
cale
from
1
(ver
y di
ssat
isfie
d) to
7 (v
ery
satis
fied)
. All
sub-
scor
es o
f the
MIL
Q a
re sc
ored
with
a ra
nge
from
4
to 2
8. T
he c
ompo
site
scor
e ra
nges
from
8 to
24,
an
d is
der
ived
as a
wei
ghte
d su
m o
f an
indi
vidu
-al
s’ g
loba
l QO
L
[35]
Hea
lth-r
elat
ed q
ualit
y-of
-life
mea
sure
The
36-
item
Med
ical
Out
com
es S
tudy
Que
stion
-na
ire (S
F-36
) [57
]36
A st
anda
rdiz
ed m
easu
re o
f gen
eric
hea
lth-r
elat
ed
QO
L w
ith c
lose
-end
ed st
ruct
ured
que
stion
s. Th
ere
are
8 di
men
sion
s, 4
of w
hich
com
pris
e th
e Ph
ysic
al C
ompo
nent
Sco
re (P
CS)
incl
udin
g m
eas-
ures
of l
imita
tion
in p
hysi
cal f
unct
ioni
ng, p
hysi
cal
heal
th p
robl
ems w
ith re
sulta
nt ro
le li
mita
tions
, bo
dily
pai
n, a
nd g
ener
al h
ealth
per
cept
ions
. The
ot
her 4
dim
ensi
ons w
hich
com
pris
e th
e M
enta
l C
ompo
nent
Sco
re (M
CS)
incl
ude
vita
lity,
soci
al
func
tioni
ng, e
mot
iona
l pro
blem
s with
resu
ltant
ro
le li
mita
tions
, and
gen
eral
men
tal h
ealth
Each
resp
ectiv
e di
men
sion
tran
sfor
med
into
0–1
00
scal
e. H
ighe
r sco
res i
ndic
ate
bette
r QO
L[3
3, 3
4, 3
6, 4
0]
The
12-
item
Sho
rt Fo
rm o
f the
Med
ical
Out
com
es
Stud
y Q
uesti
onna
ire (S
F-12
) [58
]12
Valid
mea
sure
whi
ch a
sses
ses t
wo
dim
ensi
ons o
f Q
OL:
phy
sica
l hea
lth c
ompo
nent
(mea
sure
s of
gene
ral h
ealth
, pai
n as
sess
men
t, fa
tigue
, phy
sica
l fu
nctio
ning
, and
inte
rfere
nce
of ro
le p
erfo
r-m
ance
due
to p
hysi
cal h
ealth
lim
itatio
ns),
and
a m
enta
l hea
lth c
ompo
nent
(mea
sure
s of e
mot
iona
l w
ell-b
eing
, vita
lity,
soci
al fu
nctio
ning
, and
role
in
terfe
renc
e du
e to
em
otio
nal h
ealth
lim
itatio
ns)
Item
s are
mea
sure
d on
diff
eren
t sca
les i
nclu
ding
‘y
es’/’
no,’
‘not
at a
ll’/‘v
ery
muc
h.’ A
mea
n sc
ore
is g
ener
ated
for e
ach
com
pone
nt ra
ngin
g fro
m 0
to
100
. The
subs
cale
s are
nor
med
on
the
gene
ral
adul
t US
popu
latio
n w
ith a
mea
n (S
D) o
f 50
(10)
. H
ighe
r sco
res i
ndic
ates
bet
ter H
RQ
OL
[27–
30]

2792 Quality of Life Research (2018) 27:2777–2797
1 3
Tabl
e 3
(con
tinue
d)
Qua
lity-
of-li
fe m
easu
rem
ent [
refe
renc
e]N
umbe
r of
item
sIn
strum
ent d
escr
iptio
nSc
orin
g sy
stem
Stud
ies w
hich
use
d m
easu
re in
this
re
view
RA
ND
36-
item
hea
lth su
rvey
[59]
36Th
e ite
ms i
n th
e R
AN
D H
ealth
surv
ey w
ere
adap
ted
from
the
36-it
em M
edic
al O
utco
mes
St
udy
Que
stion
naire
(SF-
36),
alth
ough
hav
ing
a si
mpl
er sc
orin
g sy
stem
. Eig
ht d
omai
ns a
re
asse
ssed
, nam
ely,
bod
ily p
ain
(2 it
ems)
, ene
rgy/
fatig
ue (4
item
s), p
hysi
cal f
unct
ioni
ng (1
0 ite
ms)
, ro
le li
mita
tions
from
phy
sica
l hea
lth p
robl
ems
(4 it
ems)
, em
otio
nal w
ell-b
eing
(5 it
ems)
, rol
e lim
itatio
ns d
ue to
em
otio
nal p
robl
ems (
3 ite
ms)
, so
cial
func
tioni
ng (2
item
s), a
nd g
ener
al h
ealth
pe
rcep
tions
(5 it
ems)
. A si
ngle
item
mea
sure
s pe
rcei
ved
chan
ge in
hea
lth
Each
item
is sc
ored
from
0 to
100
(hig
her s
core
s in
dica
te m
ore
favo
rabl
e he
alth
). Th
e ite
ms i
n ea
ch
dom
ain
are
aver
aged
to c
reat
e 8-
scal
e sc
ores
[39]
Dis
ease
-spe
cific
qua
lity-
of-li
fe m
easu
re M
inne
sota
Liv
ing
with
Hea
rt Fa
ilure
Que
stion
-na
ire (M
LHF)
[60]
21A
val
idat
ed L
iker
t-typ
e in
strum
ent c
reat
ed fo
r as
sess
ing
heal
th-r
elat
ed Q
OL
amon
g pa
tient
s di
agno
sed
with
hea
rt fa
ilure
. Mea
sure
s the
eff
ect o
f hea
rt fa
ilure
on
phys
ical
and
em
otio
nal
dim
ensi
ons o
f life
. The
phy
sica
l ite
ms i
nclu
de
sym
ptom
s suc
h as
fatig
ue, s
wel
ling,
shor
tnes
s of
brea
th, r
ole
func
tioni
ng w
ith d
ifficu
lty p
erfo
rm-
ing
wor
k or
soci
al a
ctiv
ities
. The
em
otio
nal i
tem
s as
sess
wor
ry, d
epre
ssio
n, a
nd lo
sing
self-
cont
rol
Each
item
is ra
ted
from
0 (d
id n
ot) t
o 5
(ver
y m
uch
prev
ente
d m
e fro
m li
ving
as I
wan
ted)
. Hig
her
scor
es o
n th
e ph
ysic
al a
nd e
mot
iona
l sub
scal
es
impl
y lo
wer
qua
lity
of li
fe
[33,
37]
Qua
lity
of L
ife a
fter A
cute
Myo
card
ial I
nfar
ctio
n (Q
LMI)
[61]
25Va
lidat
ed a
nd re
liabl
e di
seas
e-sp
ecifi
c in
strum
ent
whi
ch c
onsi
sts o
f tw
o su
bsca
les:
The
Lim
ita-
tions
(QO
L Li
m) s
ubsc
ale
whi
ch a
sses
ses t
he
freq
uenc
y of
phy
sica
l sym
ptom
s and
how
muc
h it
inte
rfere
s with
dai
ly li
fe, a
nd th
e Em
otio
nal
subs
cale
(QO
L Em
) whi
ch a
sses
ses p
atie
nts’
se
lf-es
teem
, em
otio
nal w
ell-b
eing
, and
abi
lity
to
man
age
thei
r illn
ess
The
scor
es ra
nge
from
1 (a
ll of
the
time)
to 7
(non
e of
the
time)
with
a m
ean
resp
onse
to a
ll 25
item
s. H
ighe
r sco
res i
ndic
ate
bette
r QO
L
[31,
32]
Kan
sas C
ity C
ardi
omyo
path
y Q
uesti
onna
ire
(KC
CQ
)-Q
OL
subs
cale
[62]
3Th
e Q
OL
subs
cale
of t
he se
lf-re
porte
d K
CC
Q is
a
valid
ated
mea
sure
whi
ch a
sses
ses h
ow h
eart
failu
re im
pact
s pat
ient
’s o
vera
ll Q
OL.
Tw
o ite
ms
addr
ess Q
OL,
whi
le th
e th
ird it
em a
sses
ses
depr
essi
on
Scor
ed fr
om 0
to 1
00 w
ith a
hig
her s
core
indi
catin
g be
tter Q
OL
[38]

2793Quality of Life Research (2018) 27:2777–2797
1 3
Association between R/S and QOL
The association between R/S and QOL differed according to the dimension of R/S and QOL domain assessed. We have summarized the principal study findings based on the association between R/S and QOL domain examined (global QOL, HRQOL, and disease-specific QOL), and according to the type of CVD. Results from included studies are detailed in Table 1.
Association between R/S and QOL in patients with heart failure
Eleven studies examined the association between R/S and QOL in patients with heart failure. Four publications used longitudinal data [27–29, 36], and seven used a cross-sec-tional design [30, 33–35, 37, 38, 40]. A significant positive association between R/S and QOL was reported in six of the eleven studies [28–30, 33, 38, 40]. The association between R/S and QOL domains in patients with heart failure is as follows:
R/S and Global QOL: Spiritual well-being was positively correlated with global QOL measures (r = 0.49, p ≤ 0.001) [33], while spirituality, as assessed with the FACIT-Sp measure, was not significantly related to global QOL [35].
R/S and HRQOL: Higher daily spiritual experience and having one’s spiritual needs met were positively associated with higher physical well-being [28, 30]. Attending to one’s spiritual needs, spiritual well-being, and a more religious attitude were positively associated with better mental or emotional well-being [30, 33, 40]. However, belief in the afterlife at 1 month was negatively associated with mental HRQOL at 3 months [28], while spiritual constraint was associated with poorer physical QOL [30]. Spirituality was not associated with the physical or mental components of HRQOL [34]. Neither religious struggle nor religious cop-ing were significantly associated with the mental or physi-cal components of HRQOL at study baseline and during a subsequent follow-up evaluation [27, 36].
R/S and disease-specific QOL: A cross-sectional study assessed patient’s spirituality with the FACIT-Sp and Iron-son–Woods Spirituality/Religiousness Index (IW) [38]; the meaning/peace and faith subscales of the FACIT-Sp, and the faith in God subscale of the IW were positively corre-lated with QOL, as assessed with the KCCQ. In contrast, the sense of peace, religious behavior, and compassionate view subscales of the IW were not significantly associated with KCCQ-QOL. Another study found no significant associa-tion between the meaning/peace and faith subscales of the FACIT-Sp and QOL as assessed with the MLHF question-naire [37]. Lower spiritual well-being was negatively asso-ciated with poorer physical and emotional symptoms [33].
Association between R/S and QOL in patients with acute myocardial infarction (AMI)
Two longitudinal studies examined the association between R/S and disease-specific QOL in patients with AMI [31, 32]. The findings from a study of 105 patients with a first time AMI [31], showed that higher consequential religios-ity, experiential religiosity, and religious avoidance coping were significantly associated with increases in QOL from baseline to the 2-year follow-up. In this cohort, no sig-nificant association was found between the dimensions of R/S and QOL at baseline, and the baseline measure of R/S was not associated with changes in QOL after 12-weeks of cardiac rehabilitation [32].
Association between R/S and QOL in congenital heart disease
One cross-sectional study examined the association between R/S and global QOL in patients with congenital heart disease [41]. Those who identified as being religious had higher physical and environmental QOL scores (60.1 vs 52.6; p value < 0.01) compared with those who did not identify as being religious.
Association between R/S and QOL in a study with multiple CVD diagnoses
A cross-sectional study that enrolled patients (n = 135) with varying CVD diagnoses (75.5% myocardial infarc-tion, 14.1% severe angina pectoris, 6.7% arrhythmias, and 3.7% heart failure) examined the association between R/S and HRQOL [39]. Intrinsic religiousness was positively associated with higher emotional and physical well-being, and a higher frequency of church attendance was positively associated with better mental or emotional well-being.
Study quality assessment
The quality scores of the included studies ranged from 73.7 to 94.7%. All studies clearly reported their objective(s), described study participant characteristics, and their key exposure and outcome variables. With respect to internal validity, only a few studies sufficiently adjusted for poten-tial confounders in the form of a multivariable regression analysis [27, 28, 34, 39, 40]. Five longitudinal studies [27–29, 31, 36] adequately reported the number of par-ticipants recruited, those lost to follow-up, and reasons for attrition. Most studies addressed the representative-ness of their study sample and the generalizability of their

2794 Quality of Life Research (2018) 27:2777–2797
1 3
findings to the population from which the study subjects were selected.
Discussion
In this systematic review, we found evidence for an asso-ciation between R/S and QOL among patients with CVD. This association varied depending on the dimension of R/S and QOL domain assessed. Ten of the fifteen studies identi-fied in this review reported a significant positive association between R/S and QOL, and approximately half of the stud-ies reported negative or null associations. The majority of included studies were conducted among patients with heart failure.
Prior studies have posited a variety of mechanisms by which R/S influences QOL in patients with chronic condi-tions. Religiousness has been shown to enhance self-esteem, generate positive emotions, and promote positive self-care practices by encouraging individuals to refrain from unhealthy lifestyle practices, which in turn fosters well-being [63–65]. R/S may favorably influence an individual’s QOL by fostering a deeper sense of meaning when faced with life-threatening or chronic debilitating conditions [66]. Our findings suggest that R/S is associated with QOL, as intrinsic religiousness, spiritual well-being, and attending to one’s spiritual needs were related to better physical, mental, and emotional functioning. On the other hand, spiritual con-straint and lower spiritual well-being were associated with poorer physical and emotional well-being.
R/S and QOL
We observed considerable heterogeneity in the R/S measures utilized, reflective of the varying dimensions of R/S assessed in research and the general lack of consensus in defining R/S [67]. Most of the included studies utilized already existing validated scales, whereas one recent study designed their R/S questionnaire for purposes of assessing religious atti-tudes [40]. This latter study provided a detailed description of their instrument validation process and had a high-quality rating in our methodological assessment.
Upwards of sixteen dimensions of R/S were assessed across studies with religious coping being the most com-monly assessed aspect. In patients diagnosed with an initial AMI or after coronary artery bypass surgery, higher reli-gious coping was associated with better emotional QOL over a 2-year follow-up period. In contrast, no association was observed between religious coping and physical/mental well-being in patients living with heart failure at 6 months of follow-up. These findings reflect how R/S may differ-entially influence QOL depending on the domain assessed, patient’s clinical diagnosis, and the duration of follow-up
in assessing the impact of one’s R/S on their QOL since shorter follow-up periods may not sufficiently allow for R/S to influence health outcomes. Furthermore, reverse causa-tion and residual confounding may explain these differences observed in the various studies included in this review. In a study [28] that examined seven dimensions of R/S (forgive-ness, daily spiritual experiences, belief in afterlife, religious identity, religious support, public practices, and positive RS coping), only moderate correlations were found between the dimensions suggesting that they each represent a unique aspect of one’s religious/spiritual experience, and that each R/S dimension may have a distinct role in the relationship between R/S and patient’s QOL domains.
We observed considerably greater uniformity in the QOL outcome measures examined in this review, with the three major domains of global, health-related, and disease-specific QOL assessed.
Summary of the Literature
A majority of studies included in this review [n = 11] were conducted between 2010 and 2017, indicative of an increas-ing awareness of the relationship between R/S and patient’s QOL. Most of the identified studies [n = 11] enrolled patients with heart failure, which may be attributable to the worldwide rise in the magnitude of heart failure and its con-siderable morbidity and mortality, and impact on patient’s QOL due to its physical and emotional symptoms [68, 69]. However, future research is needed among patients with varying manifestations of underlying CVD, including acute and chronic forms of heart disease, which may have a con-siderable impact on patient’s QOL.
Most of the included studies [n = 12] were conducted in the US, and the study participants were predominantly non-Hispanic Whites and middle-older aged persons, which limits the generalizability of the study findings to ethnic minority groups and younger individuals. There was an overrepresentation of studies with small sample sizes, short follow-up duration, or the use of a cross-sectional design, which limits the conclusiveness of our review. Results from the methodological quality assessment revealed that included studies had moderate- to high-quality ratings, which lends some credence to the reliability of our findings.
Strengths and limitations of the current systematic review
To our knowledge, this is the first systematic review to examine the association between R/S and QOL in patients with CVD. From a self-evaluation of our review using the AMSTAR tool for assessing systematic review quality [70], we obtained a score of 10 out of a maximum of 11

2795Quality of Life Research (2018) 27:2777–2797
1 3
points. The one point not credited to this review was due to our inability to investigate possible publication bias with a funnel plot as we would have required a uniform measure of effect, which was impossible due to heterogeneity in the assessment of R/S across the included studies.
Several limitations of our review exist. First, we excluded non-English articles, likely leading to publica-tion bias. Our initial search of the electronic databases did not exclude studies based on publication language; however, only four studies in foreign languages were identified. Second, we suggest caution in interpreting the synthesized results from this review, as causal inferences on the association between R/S and QOL cannot be made from observational studies which are susceptible to poten-tial confounding by unmeasured or inadequately measured variables, and cross-sectional studies do not account for temporality. Most included studies were conducted among patients with heart failure, which may have limited the generalizability of our findings. Lastly, most identified studies were conducted in the US, which may not ade-quately capture R/S and cultural impact on QOL from a global perspective.
Research and clinical implications
Future research should be conducted in patients with different CVD conditions to better understand how R/S may influence their QOL. Longitudinal studies in larger patient samples are needed to better understand how R/S may affect QOL over varying follow-up periods, as it is unclear whether any associations observed over the short-term persist on a longer-term basis. Future studies should evaluate how patients may turn to or away from R/S in periods of illness and stress, how this might influence their QOL, and identify those in need of clerical intervention for a more holistic approach in patient management. In addition, there is a need for uniformity in assessing R/S to ensure more reliable and comparable results across stud-ies. Furthermore, advanced analytic techniques, such as propensity scoring and instrumental variables to address confounding in observational studies should be explored.
The findings from this review reveal that certain dimen-sions of R/S are likely associated with patient’s QOL. Healthcare providers need to consider the influence of R/S on patient’s QOL, as this may also influence patient engagement with their treatment and long-term outcomes.
Acknowledgements We thank Catherine Carr and Victoria Rossetti for their assistance in developing the search strategy for the electronic databases used in this systematic review.
Funding This study did not receive any funding.
Compliance with ethical standards
Conflict of interest The authors have no conflict of interest to disclose.
Ethical approval This article does not contain any studies with human participants performed by any of the authors.
Open Access This article is distributed under the terms of the Crea-tive Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribu-tion, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
References
1. World Health Organization. (2017). Cardiovascular diseases. [Fact Sheet]. Retrieved September 27, 2017, from http://www.who.int/media centr e/facts heets /fs317 /en/.
2. Moryś, J. M., Bellwon, J., Höfer, S., Rynkiewicz, A., & Gruchała, M. (2016). Quality of life in patients with coronary heart dis-ease after myocardial infarction and with ischemic heart failure. Archives of Medical Science, 12(2), 326–333.
3. Wenger, N. K., Mattson, M. E., Furberg, C. D., & Elinson, J. (1984). Assessment of quality of life in clinical trials of cardiovas-cular therapies. American Journal of Cardiology, 54(7), 908–913.
4. Shepherd, C. W., & Alison, E. W. (2012). Cardiac rehabilitation and quality of life: A systematic review. International Journal of Nursing Studies, 49(6), 755–771.
5. World Health Organization. (1987). WHOQOL: Measur-ing quality of life. Geneva: WHO. Retrieved September 27, 2017, from http://apps.who.int/iris/bitst ream/10665 /63482 /1/WHO_MSA_MNH_PSF_97.4.pdf.
6. Burns, T. M., Graham, C. D., Rose, M. R., & Simmons, Z. (2012). Quality of life and measures of quality of life in patients with neuromuscular disorders. Muscle and Nerve, 46, 9–25.
7. Cepeda-Valery, B., Cheong, A. P., Lee, A., & Yan, B. P. (2011). Measuring health related quality of life in coronary heart disease: the importance of feeling well. International Journal of Cardiol-ogy, 149, 4–9.
8. Kato, N., Kinugawa, K., Seki, S., Shiga, T., Hatano, M., Yao, A., et al. (2011). Quality of life as an independent predictor for cardiac events and death in patients with heart failure. Circulation Journal, 75, 1661–1669.
9. Issa, S. M., Hoeks, S. E., Scholte op Reimer, W. J. M., Van Gestel, Y. R., Lenzen, M. J., Verhagen, H. J., et al. (2010). Health-related quality of life predicts long-term survival in patients with periph-eral artery disease. Vascular Medicine, 15, 163–169.
10. Xie, J., Wu, E. Q., Zheng, Z. J., Sullivan, P. W., Zhan, L., & Labarthe, D. R. (2008). Patient-reported health status in coronary heart disease in the United States: Age, sex, racial, and ethnic dif-ferences. Circulation, 118, 491–497.
11. De Smedt, D., Clays, E., Annemans, L., Doyle, F., Kotseva, K., Pająk, A., et al. (2013). Health related quality of life in coronary patients and its association with their cardiovascular risk profile: Results from the EUROASPIRE III survey. International Journal of Cardiology, 168, 898–903.
12. Ross, L. (1995). The spiritual dimension: Its importance to patients’ health, well-being and quality of life and its implications for nursing practice. International Journal of Nursing Studies, 32, 457–468.

2796 Quality of Life Research (2018) 27:2777–2797
1 3
13. Koenig, H. G., McCullough, M., & Larson, D. (2001). Handbook of religion and health. New York: Oxford University Press.
14. Van Groenestijn, A. C., Kruitwagen-van Reenen, E. T., Visser-Meily, J. M. A., van den Berg, L. H., & Schröder, C. D. (2016). Associations between psychological factors and health-related quality of life and global quality of life in patients with ALS: A systematic review. Health and Quality of Life Outcomes, 14, 107.
15. Yamout, B., Issa, Z., Herlopian, A., El Bejjani, M., Khalifa, A., Ghadieh, A. S., et al. (2013). Predictors of quality of life among multiple sclerosis patients: A comprehensive analysis. European Journal of Neurology, 20, 756–764.
16. Paiva, C. E., Paiva, B. S., de Castro, R. A., de Pádua Souza, C., de Paiva Maia, Y. C., Ayres, J. A., et al. (2013). A pilot study addressing the impact of religious practice on quality of life of breast cancer patients during chemotherapy. Journal of Religion and Health, 52, 184–193.
17. Najafi Ghezeljeh, T., & Emami, A. (2014). Strategies for recre-ating normal life: Iranian coronary heart disease patients’ per-spectives on coping strategies. Journal of Clinical Nursing, 23, 2151–2160.
18. Yaghoubi, A., Tabrizi, J. S., Mirinazhad, M. M., Azami, S., Naghavi-Behzad, M., & Ghojazadeh, M. (2012). Quality of life in cardiovascular patients in iran and factors affecting it: A system-atic review. Journal of Cardiovascular and Thoracic Research, 4(4), 95–101.
19. Muhammad, I., He, H. G., Kowitlawakul, Y., & Wang, W. (2016). Narrative review of health-related quality of life and its predictors among patients with coronary heart disease. International Journal of Nursing Practice, 22, 4–14.
20. Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ, 339, b2535.
21. Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd edn.). Hove: Lawrence Erlbaum Associates.
22. Downs, S. H., & Black, N. (1998). The feasibility of creating a checklist for the assessment of the methodological quality both of randomized and non-randomized studies of health care interven-tions. J Epidemiol Community Health, 52(6), 377–384.
23. Hajduk, A. M., Kiefe, C. I., Person, S. D., Gore, J. G., & Saczyn-ski, J. S. (2013). Cognitive change in heart failure: A systematic review. Circulation Cardiovascular Quality and Outcomes, 6(4), 451–460.
24. Pimentel, C. B., Lapane, K. L., & Briesacher, B. A. (2013). Medi-care part D and long-term care: A systematic review of quantita-tive and qualitative evidence. Drugs and Aging, 30(9), 701–720.
25. Hosseini, S., Chaurasia, A., & Oremus, M. (2017). The effect of religion and spirituality on cognitive function: A systematic review. The Gerontologist. https ://doi.org/10.1093/geron t/gnx02 4.
26. Agli, O., Bailly, N., & Ferrand, C. (2015). Spirituality and religion in older adults with dementia: A systematic review. International Psychogeriatrics, 27, 715–725.
27. Park, C. L., Wortmann, J. H., & Edmondson, D. (2011). Religious struggle as a predictor of subsequent mental and physical well-being in advanced heart failure patients. Journal of Behavioral Medicine, 34(6), 426–436.
28. Park, C. L., Lim, H., Newlon, M., Suresh, D. P., & Bliss, D. E. (2014). Dimensions of religiousness and spirituality as predictors of well-being in advanced chronic heart failure patients. Journal of Religion and Health, 53(2), 579–590.
29. Sacco, S. J., Park, C. L., Suresh, D. P., & Bliss, D. (2014). Living with heart failure: Psychosocial resources, meaning, gratitude and well-being. Heart and Lung, 43(3), 213–218.
30. Park, C. L., & Sacco, S. J. (2017). Heart failure patients’ desires for spiritual care, perceived constraints, and unmet spiritual needs:
relations with well-being and health-related quality of life. Psy-chology, Health & Medicine, 22(9), 1011–1020.
31. Trevino, K. M., & McConnell, T. R. (2014). Religiosity and reli-gious coping in patients with cardiovascular disease: Change over time and associations with illness adjustment. Journal of Religion and Health, 53(6), 1907–1917.
32. Trevino, K. M., & McConnell, T. R. (2015). Religiosity and spir-ituality during cardiac rehabilitation: A longitudinal evaluation of patient-reported outcomes and exercise capacity. Journal of Cardiopulmonary Rehabilitation and Prevention, 35(4), 246–254.
33. Beery, T. A., Baas, L. S., Fowler, C., & Allen, G. (2002). Spir-ituality in persons with heart failure. Journal of Holistic Nursing, 20(1), 5–25.
34. Westlake, C., Dracup, K., Creaser, J., et al. (2002). Correlates of health-related quality of life in patients with heart failure. Heart and Lung, 31(2), 85–93.
35. Blinderman, C. D., Homel, P., Billings, J. A., Portenoy, R. K., & Tennstedt, S. L. (2008). Symptom distress and quality of life in patients with advanced congestive heart failure. Journal of Pain and Symptom Management, 35(6), 594–603.
36. Park, C. L., Malone, M. R., Suresh, D. P., Bliss, D., & Rosen, R. I. (2008). Coping, meaning in life, and quality of life in congestive heart failure patients. Qual Life Res, 17(1), 21–26.
37. Bean, M. K., Gibson, D., Flattery, M., Duncan, A., & Hess, M. (2009). Psychosocial factors, quality of life, and psychological distress: ethnic differences in patients with heart failure. Progress in Cardiovascular Nursing, 24(4), 131–140.
38. Bekelman, D. B., Parry, C., Curlin, F. A., Yamashita, T. E., Fair-clough, D. L., & Wamboldt, F. S. (2010). A comparison of two spirituality instruments and their relationship with depression and quality of life in chronic heart failure. Journal of Pain and Symp-tom Management, 39(3), 515–526.
39. Karademas, E. C. (2010). Illness cognitions as a pathway between religiousness and subjective health in chronic cardiac patients. Journal of Health Psychology, 15(2), 239–247.
40. Abolghasem-Gorji, H., Bathaei, S. A., Shakeri, K., Heidari, M., & Asayesh, H. (2017). The effect of religiosity on quality of life in Muslim patients with heart failure: A study in Qom, the religious capital of Iran. Mental Health, Religion and Culture, 20, 217–228.
41. Bang, J. S., Jo, S., Kim, G. B., Kwon, B. S., Bae, E. J., Noh, C. I., & Choi, J. Y. (2013). The mental health and quality of life of adult patients with congenital heart disease. International Journal of Cardiology, 170(1), 49–53.
42. Pargament, K. I., Ensing, D. S., Falgout, K., et al. (1990). God help me: I. Religious coping efforts as predictors of the outcomes to significant negative life events. American Journal of Commu-nity Psychology, 18(6), 793–824.
43. Peterman, A. H., Fitchett, G., Brady, M. J., et al. (2002). Meas-uring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy–Spiritual Well-being Scale (FACIT-Sp). Annals of Behavioral Medicine, 24, 49–58.
44. Abeles, R., Ellison, C. G., George, L. K., et al. (1999). Multidi-mensional measurement of religiousness/spirituality for use in health research. Kalamazoo, MI: John E. Fetzer Institute.
45. Exline, J. J., Yali, A. M., & Sanderson, W. C. (2000). Guilt, dis-cord, and alienation: The role of religious strain in depression and suicidality. Journal of Clinical Psychology, 56, 1481–1496.
46. Ellison, C. W. (1983). Spiritual well-being conceptualization and measurement. Journal of Psychology Theology, 11, 330–340.
47. Reed, P. G. (1986). Religiousness among terminally ill adults and healthy adults. Research in Nursing & Health, 9, 35–41.
48. Cella, D. (1997). Manual of the Functional Assessment of Chronic Illness Therapy (FACIT) measurement system, version 4. Evan-ston, IL: Center on Outcomes, Research and Education (CORE), Evanston Northwestern Healthcare and Northwestern University.

2797Quality of Life Research (2018) 27:2777–2797
1 3
49. Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assess-ing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56, 267–283.
50. Ironson, G., Solomon, G. F., Balbin, E. G., et al. (2002). The Ironson-woods Spirituality/Religiousness Index is associated with long survival, health behaviors, less distress, and low cortisol in people with HIV/AIDS. Annals of Behavioral Medicine, 24(1), 34–48.
51. Allport, G. W., & Ross, J. M. (1967). Personal religious orienta-tion and prejudice. Journal of Personality and Social Psychology, 5, 432–443.
52. Rohrbaugh, J., & Jessor, R. (1975). Religiosity in youth: A per-sonal control against deviant behavior. Journal of Personality, 43(1), 136–155.
53. Silber, T. J., & Reilly, M. (1985). Spiritual and religious concerns of the hospitalized adolescent. Adolescence, 20, 217–224.
54. Campbell, A., Converse, P. E., & Rodgers, W. L. (1976). The qual-ity of American life: Perceptions, evaluations, and satisfactions. New York: Russell Sage.
55. What quality of life? The WHOQOL Group. (1996). World Health Organization quality of life assessment. World Health Forum, 17, 354–356.
56. Avis, N. E., Smith, K. W., Hambleton, R. K., Feldman, H. A., Selwyn, A., & Jacobs, A. (1996). Development of the multidi-mensional index of life quality: A quality of life measure for car-diovascular disease. Med Care, 34(11), 1102–1120.
57. Ware, J. E., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36): A conceptual framework and item selection. Med Care, 30, 473–483.
58. Ware, J. E., Kosinski, M., & Keller, S. D. (1996). SF-12: An even shorter health survey. Medical Outcomes Trust Bulletin, 4, 2.
59. RAND Health (2007) Medical outcomes study: 36-item short form. Retrieved November 11, 2017, from http://www.rand.org/healt h/surve ys_tools /mos/mos_core_36ite m.html.
60. Rector, T. S., & Banks, A. J. (1996). Use of prognostic variables in the care of patients with chronic heart failure. Cardiology in Review, 4, 254–262.
61. Foster, C., Oldridge, N. B., Dion, W., Forsyth, G., Grevenow, P., Hansen, M., et al. (1995). Time course of recovery during cardiac
rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention, 15(3), 209–215.
62. Green, C. P., Porter, C. B., Bresnahan, D. R., & Spertus, J. A. (2000). Development and evaluation of the Kansas City Cardio-myopathy Questionnaire: A new health status measure for heart failure. Journal of the American College of Cardiology, 35(5), 1245–1255.
63. Oman, D., & Thoresen, C. E. (2005). Do religion and spirituality influence health? In R. F. Paloutzian & C. L. Park (Eds.), Hand-book of the psychology of religion and spirituality (pp. 435–459). New York: Guilford.
64. Powell, L. H., Shahabi, L., & Thoresen, C. E. (2003). Religion and spirituality. Linkages to physical health. American Psychologist, 58, 36–52.
65. Lucchese, F. A., & Koenig, H. G. (2013). Religion, spirituality and cardiovascular disease: Research, clinical implications, and opportunities in Brazil. Revista Brasileira De Cirurgia Cardio-vascular, 28, 103–128.
66. Zinnbauer, B. J., Pargament, K. I., & Scott, A. B. (1999). The emerging meanings of religiousness and spirituality: Problems and prospects. Journal of Personality, 67(6), 889–919.
67. Dal Bello-Haas, V., Andrews-Hinders, D., Bocian, J., Mascha, E., Wheeler, T., & Mitsumoto, H. (2000). Spiritual well-being of the individual with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord, 1, 337–341.
68. Galbreath, A., Krasuski, R., Smith, B., Stajduhar, K., Kwan, M., Ellis, R., et al. (2004). Long-term healthcare and cost outcomes of disease management in a large, randomized, community-based population with heart failure. Circulation, 110, 3518–3526.
69. Rector, T. S., Anand, I. S., & Cohn, J. N. (2006). Relationships between clinical assessments and patients’ perceptions of the effects of heart failure on their quality of life. Journal of Cardiac Failure, 12, 87–92.
70. Shea, B. J., Grimshaw, J. M., Wells, G. A., Boers, M., Anders-son, N., Hamel, C., & Bouter, L. M. (2007). Development of AMSTAR: A measurement tool to assess the methodological qual-ity of systematic reviews. BMC Medical Research Methodology, 7, 10. https ://doi.org/10.1186/1471-2288-7-10.