
Chapter 48 Care of the Patient with a Cardiovascular or a Peripheral Vascular Disorder
Upload
alannah-simonCategory
view
216download
0
Assessment of the Cardiovascular System
The Heart and Peripheral Vasculature

Cardiovascular System
Health HistoryInspectionPalpationPercussionAuscultation

Health History Chest pain Dyspnea, Orthopnea, Cough, Fatigue Edema, Swollen joints, Nocturia HTN, DM, CAD, CHD, Hyperlipidemia, Bleeding
disorders Cardiac surgery or related hospitalization within last 5
years Personal and Social Hx. Family History
CHD – once a defect occurs in a family, the likelihood of recurrence is 3-5 times the general population, especially with left sided lesions
Sudden death in young and middle-aged relatives Cardiac History/Race-related considerations
Cardiac History/Race-Related Considerations Rheumatic fever (5-15yrs.) Mitral valve prolapse (20-50yrs.) HTN (20-70yrs.) Valve stenosis or regurgitation (30-50yrs.) Coronary artery dx. (40-60yrs.) MI (40-60 yrs.) Arteriosclerosis (50-70 yrs.) CVA (50-70 yrs.) Abdominal aortic aneurysm (60-70 yrs.)
Race-related Considerations: African American (CVA, CAD, HTN, Diabetes) Hispanic and Filipino (HTN) American Indian (CVA, CAD)
Age-related Considerations Children
Prenatal Hx. Cyanosis with feedings Growth and activity FTT Developmental milestones
Elderly Current medications Environment ADL’s
Inspection Note chest configuration Color of nailbeds, M/M Capillary refill, < 3 seconds Respiratory pattern and effort – any
dyspnea, etc. Lifts or heaves Inspect for any pulsations
Neck Jugular Vein Distention
Anterior Chest – eye should be at chest level Mild pulsation – normal Strong pulsation - abnormal

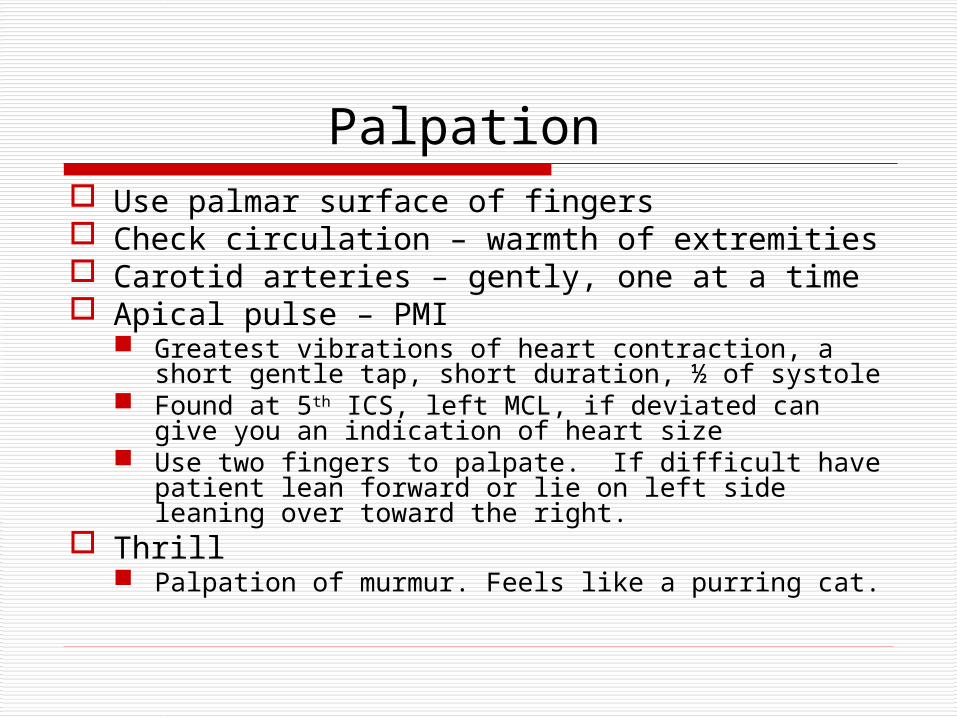
Palpation Use palmar surface of fingers Check circulation – warmth of extremities Carotid arteries – gently, one at a time Apical pulse – PMI
Greatest vibrations of heart contraction, a short gentle tap, short duration, ½ of systole
Found at 5th ICS, left MCL, if deviated can give you an indication of heart size
Use two fingers to palpate. If difficult have patient lean forward or lie on left side leaning over toward the right.
Thrill Palpation of murmur. Feels like a purring cat.

Percussion
Generally a poor indicator, rarely used
Used to outline heart’s borders, dullness
Difficult to perform with breast tissue CXR
Auscultation
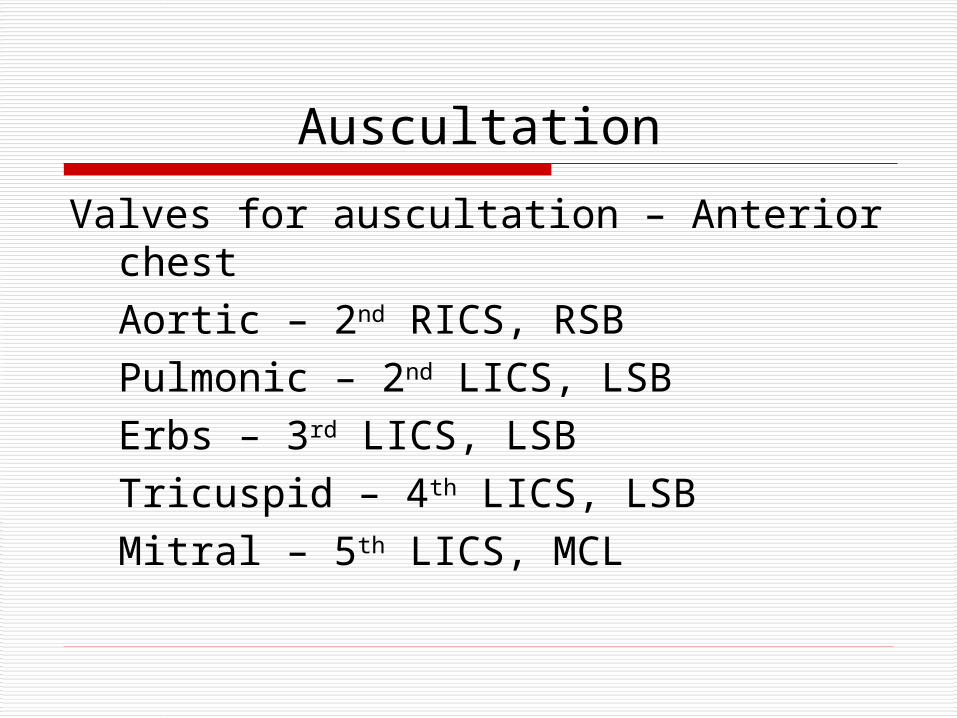
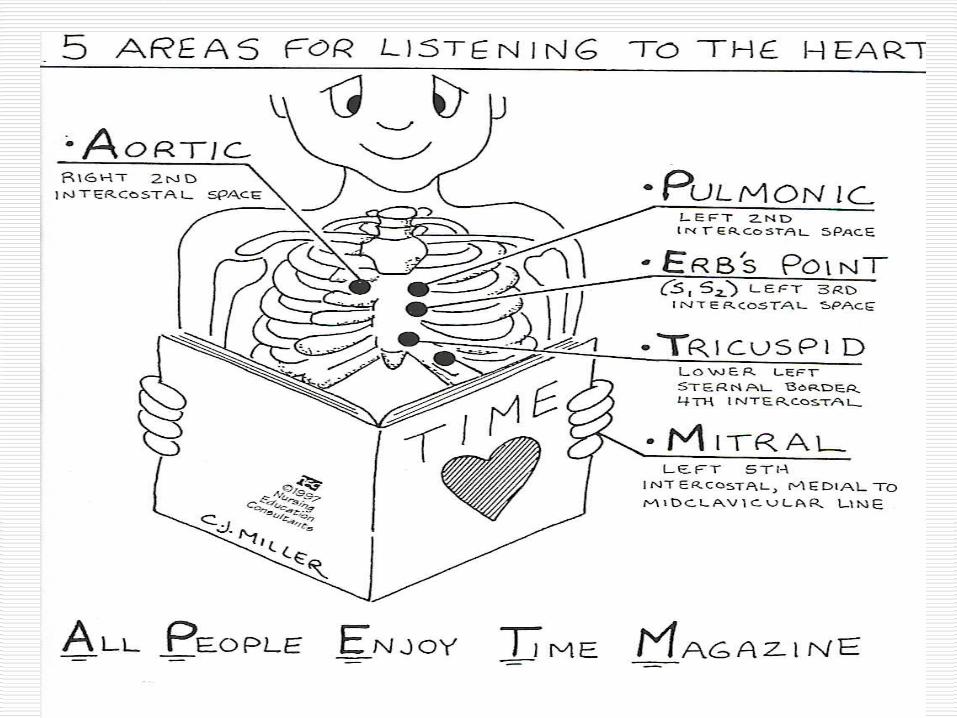
Valves for auscultation – Anterior chestAortic – 2nd RICS, RSBPulmonic – 2nd LICS, LSBErbs – 3rd LICS, LSBTricuspid – 4th LICS, LSBMitral – 5th LICS, MCL

Auscultation – Heart Sounds Auscultate the heart in the sitting and lying
down positions. Use both the diaphragm and the bell. Diaphragm – high pitched Bell – low pitched
Note rate and rhythm 60-100 BPM Sinus arrhythmia Irregularities (apical), Count one full minute
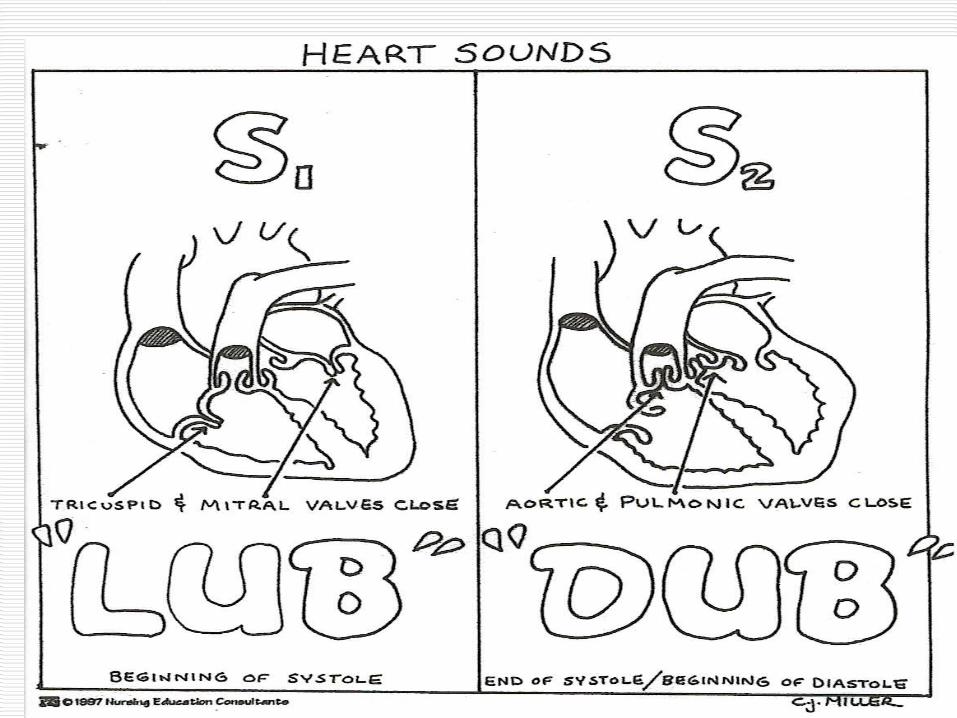
Identify heart sounds S1 S2

S1 Closure of the mitral and tricuspid valves,
AV valves First heart sound – LUB Louder at the apex, heard best with
diaphragm Heard at the beginning of systole It is the R wave on EKG and the carotid
artery pulse Split S1 (normal)
Hear closure of mitral and tricuspid valves separately

S2 Closure of the aortic and pulmonic valves,
semilunar valves Second heart sound – DUB Louder at the base, heard best with
diaphragm Heard at the end of systole, beginning of
diastole Physiologic split of S2 (normal in children)
Two sounds heard – A2, P2 Pressures in the R heart are lower than the L,
producing two heart sound. The L side first A2, then the R side, P2.
Split heard best in pulmonic area

Auscultate for Extra Heart Sounds
Auscultate with diaphragm, then bell Heard during diastole
Ventricular filling
Lower pitch, heard at apex Extra heart sounds
S3 S4
S3 Heard at the beginning of diastole, after S2
Lub-dubba Ken/tuck/(Y) S1 – S2 – S3
Heard best with bell Sound is produced by blood hitting a non-
pliable ventricle wall during diastole. Normal in infants and young children d/t firm
heart muscle In adults can be d/t increased blood volume or
indicative of heart dx.CHFRegurgitation
S4 Also known as an Atrial Gallup Heard at the end of diastole, before S1
daLub-Dub (Ten)/ness/ee S4 – S1 –S2
Heard best with bell It is caused by a turbulence of flow against pressure.
(Resistance of flow). Heard with: Pulmonary hypertension Aortic and pulmonic stenosis Cardiomyopathy, valve dx. MI’s
Always abnormal
Adventitious Heart Sounds
Clicks Murmurs
Clicks Heard early in systole. More pronounced with pt.
sitting up Associated with valve dx. Aortic click
Most common D/T coarcation, aortic stenosis, anuerysm Sound does not change with respiration
Mitral click D/T prolapsed mitral valve
Pulmonic click Associated with pulmonic valve stenosis and
pulmonary hypertension Heard throughout respiratory cycle, more intense in
expiration
Murmurs Extra sound superimposed on normal heart sounds
caused by a disruption of flow into, through, or out of heart
Causes of Murmurs Anatomic valve disorder Diseased valves Hi output demands that increase speed of flow
Anemia, pregnancy Diminished strength of myocardial contraction Altered blood flow in vessels near heart
Newborn - PDA 7 Assessments Grading of Murmur

Murmurs – 7 Assessments Pitch
High, medium, low Pattern
Crescendo Decrescendo Crescendo-Decrescendo Diamond shaped
Quality Describe, generally a blowing, rubbing sound
Location Where is it loudest
Radiation Does it transmit to other areas
Posture Does it change with position change
Timing in cardiac cycle

Grading of Murmurs (Loudness) Grade 1
Barely audible Grade 2
Readily heard Grade 3
Moderately loud Grade 4
Loud with associated thrill – fine, palpable, rushing sensation
Grade 5 Very loud with thrill
Grade 6 Loudest with thrill, may be audible with diaphragm
off the chest
Physiologic Murmur
Normal in children Heard as a systolic flow murmur that
varies with position change Generally a G1 or G2 Pregnant women



![ARTERIAL PERIPHERAL VASCULAR DISEASES.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000113-cardiovascular-system/… · arterial peripheral vascular diseases acute arterial occlusion](https://static.fdocuments.net/doc/165x107/604e83caf1418f71db611c5a/arterial-peripheral-vascular-read-onlyocwusuacidcoursedownload1110000113-cardiovascular-system.jpg)














