ASSESSMENT OF periodontal risk factors and indicators.pptx

of 113
-
Upload
neal-torwane -
Category
Documents
-
view
218 -
download
0
Transcript of ASSESSMENT OF periodontal risk factors and indicators.pptx
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
1/113
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
2/113
INTRODUCTION
As our understanding of periodontal diseases has deepened, it
has become clear that certain risk factors are associated with
disease development.
As dental professionals seek to optimize treatment and improve
outcomes for patients, the role of risk assessment and disease
management has become increasingly important.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
3/113
RISK ASSESSMENT..
According to MeSH, risk assessment can be defined as the
Qualitative or quantitative estimation of the likelihood of
adverse effects that may result from exposure to specifiedhealth hazards or from the absence of beneficial influences.
Risk assessment involves dental care providers, identifying
patients, and populations at increased risk of developingperiodontal disease.
The assessment of patients risk to controlsignificant impact
on clinical decision making.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
4/113
Rather than concentrating on obvious pathology that requires
immediate (and typically surgical) intervention, the risk
assessment model invites dental care professionals to take a
step back and look at the potential development of dentaldisease over the long term.
To improve clinical decision making, risk assessment can
reduce the need for complex periodontal therapy, improvepatient outcomes and ultimately reduce oral health care costs.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
5/113
This presentation reviews the application of risk assessment
and disease management to the general population and to
groups at risk of developing periodontal disease.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
6/113
RISK FACTORS
A risk factor can be defined as any environmental, behavioral,
or biologic factor that, when present, increases the likelihoodthat an individual will develop the disease.
Risk factorswith a disease but..cause the disease.
However, to be identified as a risk factor, the exposure must
occur before disease onset.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
7/113
Risk factors may be modifiable or non-modifiable.
Modifiable risk factors are usually environmental or behavioralin nature whereas non-modifiable risk factors are usually
intrinsic to the individual and therefore not easily changed.
Non-modifiable risk factors are also known as determinants.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
8/113
Associations identified through longitudinal and interventional
studies are termed risk factors whereas associations, based on
the observations of cross-sectional and case controlled studies
are termed risk indicators.
Thus the term risk factor denotes a greater weight of evidence
supporting an association than does the term risk indicator.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
9/113
CRITERIA FOR CAUSAL RELATION ACCEPTANCE
Causal inference, i.e. the procedure of drawing conclusions
related to the cause of disease is a complex issue.
In the 1970s, Hill (1971) formalized the criteria that have to befulfilled in order to accept a causal relation. These included:
Strength of association
Dose-response effect
Temporal consistency
Consistency of the findings
Biological plausibility
Specificity of the association
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
10/113
1. Strength of association:
- Stronger the association between the potential risk factor and
disease, the more likely it is that the anticipated causal relationis valid.
2. Dose-response effect:
- An observation that the frequency of the disease increases with
the dose or level of exposure to a certain factor supports a causal
interpretation.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
11/113
3. Temporal consistency:
- It is important to establish that the exposure to the anticipated
causative factor occurred prior to the onset of the disease.- This may be difficult in case of diseases with long latent periods
or factors that change over time.
4. Consistency of the findings:
- If several studies investigating a given relationship generate
similar results, the causal interpretation is strengthened.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
12/113
5. Biological Plausibility:
- It is advantageous if the anticipated relationship makes sense
in the context of current biological knowledge.- Less that is known about the etiology of given disease, more
difficult it become to satisfy this criterion.
6. Specificity of the association:
- If the disease is found to be associated with only one factor
among a multitude of factors tested, the causal relationship is
strengthened.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
13/113
- it is important that the criteria described are meant as
guidelines when a causal inference is established.
- None of them, however, is either necessary or sufficient for acausal interpretation.
- Strict adherence to any of them without concomitant
consideration, may result in incorrect conclusions.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
14/113
PRINCIPLES OF RISK ASSESSMENT PROCESS
According to BECK (1994): STEPS:
Identification of factors to be associated with the disease.
In case of multiple factors, Multivariate risk assessment model
must be developed that discloses which combination of factors
does most effectively discriminate between health and disease.
Assessment: new populations are screened for this
combination of factors.
Targeting: exposure to the identified factors is modified by
prevention or intervention and the effectiveness of the approach
in suppressing the incidence of the disease is evaluated
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
15/113
Thus, according to this process,potentialorputative risk factors
are first identified and thereafter tested until their significance
as true risk factoris proven.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
16/113
PERIODONTAL RISK FACTORS
According to Borrell and Papanou (2005):
- Non amenable to intervention ( non modifiable background
factors)
- Modifiable factors (environmental, acquired andbehavioral)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
17/113
NON MODIFIABLE BACKGROUND FACTORS
AGE:
Aging.increased incidence..
- Studies on periodontal disease prevalence, extent, and severity
show more disease in older age groups compared with younger
groups.
- However it has been suggested that the increased level of
periodontal destruction observed with aging is the result of
cumulative destruction rather than a result of increased rates of
destruction, thus aging is not a risk factorper se.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
18/113
GENDER:
Periodontal disease.. men at comparable ages.
Diseases related to attachment loss and bone height are more
common.
- Men exhibit poor oral hygiene and report fewer visits to the
dentist, than women.
- Female estrogen hormone protect against destructive
periodontal bone loss.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
19/113
RACE:
Assessment related to race, socio-economic status (SES) and
poverty have been unsuccessful in making associations with
periodontal disease.
Race/ ethnicity is a social construct that determines an array of
opportunities related to access, status and resources. As a
result,
- Race and SES are strongly intertwined, suggesting that the
racial effect may partially attributed to confounding by SES due
to the unequal meaning of SES indicators across racial groups.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
20/113
In a study of risk indicators for African Americans and
Caucasian Americans, there were more indicators related to
socioeconomic status.
- For e.g. Prevotella intermedia was a risk indicator for African
Americans but not for Caucasian Americans. But when
persons from both races belong to the same socioeconomic
group, differences in periodontal disease disappeared.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
21/113
GENETIC FACTORS: affect most oral conditions.
a. Genetic aspects of localized Juvenile Periodontal disease:
- LJP has a familial aggregation and has been thought to be agenetically determined condition.
- According to Long, Beaty, Hart , Saxby; periodontitis is a
because of autosomal mode of inheritance (transmission).
- According to some studies, genetic abnormalities in neutrophil
function may also associatebecause in LJP, the nuetrophil
functions are associated with genetic polymorphisms.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
22/113
Attempts to associate human leukocyte antigens (HLA) with JP
are conflicting.
- Reinholdt and colleagues.LJP patients have higher
prevalence of HLA-AG, HLA-A28, HLA-BW15.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
23/113
b. Genetic aspects of adult periodontitis:
Three approaches have been carried out,
- Human leukocyte antigen associations
- Twin studies,
- Genetic polymorphisms
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
24/113
i. Human leukocyte antigen association:
- Early studies negative association of periodontitis with HLA-A2.
- Klouda, Amer and colleagues showed: increase in HLA-Ag in
patients with periodontitis, which was related to report
presented by Reinholdt for JP.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
25/113
ii. Twin studies:
- Carried out on 26 sets of twins aged 12-17 years, 7 pairs:
monozygotic and 19: dizygotic.
- No differences in gingival recession, gingival crevice depth,
gingival bleeding, calculus or plaque.
- Michalowicz and colleagues: alveolar bone was significantly
affected by genetic factors.
- The same group found: genetic influence on gingivitis, probing
depth, attachment loss and plaque.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
26/113
- These studies are provocative, leading to hypothesis relating to
genetic factors in periodontal disease.
- However, data must be reviewed cautiously,
- Changes in alveolar bone height may be genetic due to
anatomic variation and may or may not be related to
periodontal diseaseper se.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
27/113
iii. Genetic Polymorphisms:
- Are associated with adult periodontitis.
- For e.g. Kornman studied genetic polymorphisms in Pro-
inflammatory Cytokines IL-1. AND TN F-.
- This genotype was only responsible for PD in non smokers and
not in smokers.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
28/113
Van Schie and colleagues: relation between polymorphism
pattern & periodontitis.
Hence, it appears that candidate gene polymorphisms are a
useful approach in assessing genetic factors in both JP & AP.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
29/113
Pregnancy:
Periodontal disease has been shown to be associated with
preterm delivery and low birth weight`.
A recent study found a significant association between preterm
birth and third-molar periodontal disease in pregnant women.
Analysis of gingival crevicular fluid has demonstratedsignificantly higher levels of the inflammatory mediator
prostaglandin E2 in women who delivered preterm low-birth-
weight infants.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
30/113
However, other research has failed to demonstrate a link
between preterm low-birth-weight babies and periodontal
disease.
Although a causal connection has not been established, it is
appropriate to advise expectant mothers about the importance
of good oral health, including the use of antimicrobial rinses to
mitigate the impact of pathogenic bacteria.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
31/113
MODIFIABLE [ENVIRONMENTAL, ACQUIRED & BEHAVIORAL]
Periodontal Microflora:
- There are over 400 genera and species of micro-organisms.
- Three mainly implicated as etiogenic agents:
i. Porphyromans gingivalis,
ii. Tannerella forsythia (Bacteroides forsythus) and
iii. Actinobacillus actinomycetemcomitans.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
32/113
P. gingivalis and P. intermedia: PD in older adults.
P. gingivalis and B. forsythus: increased risk for attachment loss
and alveolar bone loss.
Presence of pathogens to is not sufficient.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
33/113
The odds ratio of developing periodontal disease in an
individual who harbors one of the putative perio. Pathognes is
not high enough to consider them a risk factor.
Presence of A. actinomycetemcomitans confrs no additional
risk of developing LAP, despite it is necessary for the disease to
develop.
It has been shown that P. intermedia, P. gingivalis and
Fusobacterium nucleatum may be risk indicators for periodontal
disease in a diverse population, though they are not riskfactors.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
34/113
Socio- economic status (SES):
- Gingivitis and poor oral hygiene can be related to lower SES.
- This can be attributed to decreased dental awareness and
decrease frequency of dental visits compared with more
educated individuals of higher SES.
- Lower SES alone does not result in increased risk for
periodontitis has to be adjusted with other risk factors, such
as smoking and poor oral hygiene.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
35/113
Stress & psychological factors:
- The incidence of NUG increases in emotional and physiologic
stress.
- Emotional stress may interfere with normal immune function
and may result in increased levels of circulating hormones
which can affect the periodontium.
- Association between psychological factors and risk behaviors (
smoking, poor oral hygiene)chronic periodontitis.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
36/113
Individuals with stress are more likely to develop clinical
attachment loss and loss of alveolar bone.
This may be due to link between stress and increase in
production of IL-6
Also the host response to P. gingivalis infection may becompromised in psychologically stressed individuals.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
37/113
Despite existing evidence from case control and cross sectional
studies, no longitudinal or interventional studies have been
published that confirm psychological stress as a risk factor forP.D.
Perhaps the relationship is due to the fact that individuals under
stress are less likely to perform regular good oral hygiene andprophylaxis.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
38/113
Tobacco Smoking:
The history of association investigated in the middle of the
last century.
Recently, many epidemiological, clinical and in vitro studies
have proven that smoking negatively impacts periodontal
health.
The incidence of CAL and ABL increases with increasedsmoking
- Heat from smoke may enhance attachment loss, and the
increased calculus deposits that often result from smoking can
enhance plaque retention.
- Nicotine can diminish collagen synthesis, protein secretion and
may inhibit bone formation.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
39/113
Former smokers (clinically 5 or more years since quitting),
experience less AL than current smokers and more than never
smokers.
The likelihood of developing periodontal disease exhibits dose
dependency.
Odds ratio for developing perio. disease:
- Current heavy smokers: 7.2
- Current light smokers: 3.2
- Former smokers: 1.6
Smoking is associated with reduced gingival bleeding.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
40/113
Smoking is associated with reduced gingival bleeding.
Smokers may experience less gingival bleeding than non
smokers.
It is suggested that,alterations of the caliber of the blood
vessels perfusing the gingival tissues.
These findings suggest.. a reduced reliance on the use of
gingival bleeding as an indicator of gingival inflammation when
assessing a smokers periodontal health.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
41/113
Some in vitro studies have shown altered gingival crevicular
fluid, inflammatory cytokine profiles, immune cell function and
altered proteolytic regulation in smokers.
Also majority of the periodontal treatments are less successful
in smokers.
Nonetheless, the results of these studies are inconsistent and
no clear mechanism has emerged to explain how smoking may
affect periodontal disease.
Smoking and genetic polymorphisms is the new area ofresearch
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
42/113
Diabetes Mellitus:
- It is modifiable factorthough it cannot be cured, it can be
controlled.
- It is clear risk factor for periodontitis.
- In general, no difference in impact has been determinedbetween type I & Type II.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
43/113
Kinane found that,.direct relationship while, Taylor et al.bi-
directional relationship.
A study on Pima Indians showed an odds ratio of 2.8 to 3.4 for
developing periodontitis in Type II diabetics to non diabetics.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
44/113
Diabetes does not cause gingivitis or periodontitis but..
- It alters the response of the periodontal tissues to local factors,
- hastening bone loss and- delaying post surgical healing of periodontal tissues.
Frequent perio. abscess is important feature of perio. disease
in diabetics.
Glucose ^es in blood and gingival fluid > ^es in bact. Activity +
polymorphonuclear leukocyte > decrease in collagen synthesis.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
45/113
OBESITY: (BMI _> 30)
Involvement of hyper-inflammatory state and aberrant lipid
metabolism as well as the pathway of insulin resistance =enhanced breakdown of periodontal tissue support.
Number of recent studies point to a positive association.
Saito et al.waist to hip ratio, BMI, and body fat .significant
risk indicators.
There are only few cross-sectional studies, so, inferences on
temporality or mechanisms are not possible.
CANCER:
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
46/113
CANCER:
Patients who have cancer and who undergo chemotherapy and
radiation therapy may experience significant deleterious oral
complications, including oral mucositis, xerostomia, radiation-
induced dental caries and even osteoradionecrosis.
Opportunistic infections such as Candida albicans have been
shown to increase in frequency with mucositis andimmunosuppression.
The antibiotics and steroids used to treat these infections can
result in secondary infections by the normal oral flora.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
47/113
DIETARY FACTORS:
i. CALCIUM:
- Nishida & co-workers evaluated the role
- The group who ingested lower levels of Ca in diet,. Increased
risk.
- Some authors showed that, women (20-30) had lower serum
calcium levels showed significantly higher risk (odds: 6.1)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
48/113
ii. VITAMIN C:
- Maintains health of gingiva.
- Severe vit. C deficiency: SCOBUTIC gingivitis.
- NHANES III (1988-1992): less intake of vit. C = increased risk ,specially among current tobacco users.
- Actual mechanism is not clear.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
49/113
MEDICATIONS:
i. PHENYTOIN:
ii. CYCLOSPORIN:iii. DIHYDROPYRIDINES:
- Overgrowth of gingiva.
- Gross increase in size: dramatic expansion of connective tissue
component.
- t/t: replacement of a drug & perio theray or surgery.
STRENGTH OF ASSOCIATION OF MODIFIABLE AND NON
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
50/113
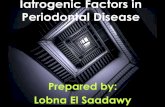
STRENGTH OF ASSOCIATION OF MODIFIABLE AND NON
MODIFIABLE FACTORS WITH DESTRUCTIVE PERIODONTAL
DISEASE.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
51/113
RISK INDICATORS FOR PERIODONTAL DISEASE
HIV/AIDS:
It has been hypothesized that, the immune dysfunction
associated increases susceptibility.
Studies revealed, HIV/AIDS patients had severe necrotizingulcerative periodontitis.
Also higher risk for periodontal pockets and CAL.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
52/113
OSTEOPOROSIS:
It is systematic factor..oral bone, (alveolar process with peri.
Infection).
From the assessment of osteoporosis in the jaws by dual
photon absorptiometry, it was found that reduction in total
skeletal mass is directly related to reduction in mandibulardensity. (Chesnut, Henrikson et al)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
53/113
INFREQUENT DENTAL VISITS:
Failure to visit the dentist regularly as a risk factor for
peridontitis is controversial.
One study demonstrated an increased risk for severe
periodontitis in patients who had not visited the dentist for 3 or
more years.
Whereas another demonstrated that there was no more loss of
attachment or bone loss in individuals who did not seek dental
care over a 6 year period.
RISK MARKERS/ PREDICTORS FOR PERIODONTAL
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
54/113
RISK MARKERS/ PREDICTORS FOR PERIODONTAL
DISEASE
POOR ORAL HYGIENE:
Since bacterial plaque is by far the most important etiologicagent for the occurrence of periodontal diseases (for review,
see Kornman and Le, 1993), it is evident that the full mouth
assessment of the bacterial load must have a pivotal impact in
the determination of the risk for disease recurrence.
Studies to date have not identified the level of plaque infection
compatible with maintenance of periodontal health.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
55/113
However, in a clinical set-up, a percentage of tooth surfaces
covered by visible plaque of 20-40% might be tolerable in most
patients.
It is important to realize that the full mouth plaque score has to
be related to the host response of the patient, i.e. compared to
inflammatory parameters.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
56/113
PREVIOUS HISTORY OF PERIODONTAL DISEASES:
History of previous periodontal disease is a good clinical
predictor of risk for future disease.
Patients with the most severe existing loss of attachment are at
the greatest risk for future loss of attachment.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
57/113
PART: II
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
58/113
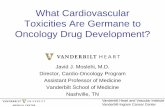
SUBJECTIVE RISK ASSESSMENT
The patient's risk assessment for periodontitis may be
evaluated on the basis of a number of clinical conditionswhereby no single parameter displays a more paramount role.
The entire spectrum of risk factors and risk indicators ought to
be evaluated simultaneously.
For this purpose, a functional diagram has been constructed
including the following aspects:
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
59/113
1. Percentage of bleeding on probing,
2. Prevalence of residual pockets greater than 4 mm (3-5 mm),
3. Loss of teeth from a total of 28 teeth,4. Loss of periodontal support in relation to the patient's age,
5. Systemic and genetic conditions, and
6. Environmental factors, such as cigarette smoking.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
60/113
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
61/113
Each parameter has its own scale for minor, moderate and
high-risk profiles.
Modifications may be made to the functional diagram if
additional factors become important according to new evidence.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
62/113
1. PERCENTAGE OF SITES WITH BLEEDING ON PROB ING
(BOP)
Bleeding on gentle probing represents an objective
inflammatory parameter which has been incorporated into index
systems for the evaluation of periodontal conditions (Le and
Silness, 1963; Mhlemann and Son, 1971).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
63/113
Although there is no established acceptable level of prevalence
of bleeding on probing in the dentition above which a higher risk
for disease recurrence has been established.
a BOP prevalence of 25% has been the cut-off point between
patients who maintained periodontal stability for 4 years and
patients with recurrent disease in the same time frame in a
prospective study in a private practice (Joss et al, 1994).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
64/113
Further evidence of BOP percentages between 20 and 30%
determining a higher risk for disease progression originates
from studies of Claffey et al (1990) and Badersten et al (1990).
In assessing the patient's risk for disease progression, BOP
percentages reflect a summary of the patient's ability to perform
proper plaque control, the patient's host response to thebacterial challenge and the patient's compliance, especially
when only few residual pockets remain after active periodontal
therapy.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
65/113
The percentage of BOP, therefore, is used as the first risk factor
in the functional diagram of risk assessment (Fig. 1).
The scale runs in a quadratic mode with 4, 9, 16, 25, 36 and >
49% being the critical values on the vector.
Individuals with low mean BOP percentages (< 10% of thesurfaces) may be regarded as patients with a low risk for
recurrent disease (Lang et al, 1990), while patients with mean
BOP percentages > 25% should be considered to be at high
risk for periodontal breakdown.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
66/113
2. PREVALENCE OF RESIDUAL POCKETS 5 MM (RESIDUAL
POCKET GREATER THAN 4 MM):
The enumeration of the residual pockets with probing depths
greater than 4 mm represents(to a certain extent) the degree of
success of periodontal treatment rendered.
Although this figureper se does not make much sense, whenconsidered as a sole parameter, the evaluation in conjunction
with other parameters such as bleeding on probing and/or
suppuration will reflect existing ecological niches from and in
which reinfection might occur.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
67/113
It is, therefore, conceivable that periodontal stability in a
dentition would be reflected in a minimal number of residual
pockets.
Presence of high frequencies of deep residual pockets and
deepening of pockets during supportive periodontal care has, in
fact, been associated with high risk for disease rogression
(Badersten et al, 1990; Claffey et al, 1990).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
68/113
In assessing the patient's risk for disease progression, the
number of residual pockets with a probing depth of5 mm is
assessed as the second risk indicator for recurrent disease in
the functional diagram of risk assessment (Fig. 1).
The scale runs in a linear mode with 2, 4, 6, 8, 10 and 12%
being the critical values on the vector.
Individuals with up to 4 residual pockets may be regarded as
patients with a relatively low risk, while patients with more than
8 residual pockets as individuals with high risk for recurrentdisease.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
69/113
3. Loss of teeth from a total of 28 teeth
Although the reason for tooth loss may not be known, the
number of remaining teeth in a dentition reflects thefunctionality of the dentition.
Mandibular stability and individual optimal function may be
assured even with a shortened dental arch of premolar topremolar occlusion, i.e. 20 teeth.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
70/113
The shortened dental arch does not seem to predispose the
individual to mandibular dysfunction (Witter et al, 1990, 1994).
However, if more than 8 teeth from a total of 28 teeth are lost,
oral function is usually impaired (Kyser, 1981, 1994, 1996).
Since tooth loss also represents a true end point outcomevariable reflecting the patient's history of oral diseases and
trauma, it is logical to incorporate this risk indicator as the third
parameter in the functional diagram of risk assessment (Fig. 1).
The number of teeth lost from the dentition without the third
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
71/113
molars (28 teeth) is counted, irrespective of their replacement.
The scale runs also in a linear mode with 2, 4, 6, 8, 10 and 12being the critical values on the vector.
Individuals with up to 4 teeth lost may be regarded as patients in
a low risk category, while patients with more than 8 teeth lostmay be considered as being in a high-risk category.
Rationale for this stems from the significance of further tooth loss
in terms of preservation of the function of the dentition.
4 Los s o f per iodon tal sup po rt in re lat ion to the pat ient 's
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
72/113
4. Los s o f per iodon tal suppo rt in relat ion to the pat ient s
age
The extent and prevalence of periodontal attachment loss (i.e.
previous disease experience and susceptibility), as evaluatedby the height of the alveolar bone on radiographs, may
represent the most obvious indicator of subject risk when
related to the patient's age.
In light of the present understanding of periodontal disease
progression, and the evidence that both onset and rate of
progression of periodontitis might vary among individuals and
during different time frames (Van der Velden, 1991), it has to berealized that previous attachment loss in relation to the patient's
age does not rule out the possibility of rapidly progressing
lesions.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
73/113
Therefore, the actual risk for further disease progression in a
given individual may occasionally be underestimated.
Hopefully, the rate of progression of disease has been
positively affected by the treatment rendered and, hence,
previous attachment loss in relation to patient's age may be a
more accurate indicator during SPT than before active
periodontal treatment.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
74/113
Given the hypothesis that a dentition may be functional for the
most likely life expectancy of the subject in the presence of a
reduced height of periodontal support (i.e. 25-50% of the root
length), the risk assessment in treated periodontal patients may
represent a reliable prognostic indicator for the stability of the
overall treatment goal of keeping a functional dentition for a
lifetime (Papapanou et al, 1988).
Th ti ti f th l f l l b i f d i th
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
75/113
The estimation of the loss of alveolar bone is performed in the
posterior region on either peri-apical radiographs, in which the
worst site affected is grossly estimated in per cent of the root
length or on bitewing radiographs in which the worst siteaffected is estimated in millimeter.
On bitewing radiographs, one millimeter is considered to be
equal to 10% bone loss.
The percentage is then divided by the patient's age.
Thi lt i f t
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
76/113
This results in a factor.
As an example, a 40-year-old patient with 20% of bone loss atthe worst affected posterior site would score BL/Age = 0.5.
Another 40-year-old patient with 50% bone loss at the worst
affected posterior site would score BL/Age = 1.25.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
77/113
In assessing the patient's risk for disease progression, the
extent of alveolar bone loss in relation to the patient's age isestimated as the fourth risk indicator for recurrent disease in the
functional diagram of risk assessment (Fig. 1).
The scale runs in increments of 0.25 of the factor BL/Age, with
0.5 being the critical value to discriminate between low and
moderate risk and 1.0 being the value for moderate and high
risk.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
78/113
This, in turn, means that a patient who has lost a higher
percentage of posterior alveolar bone than his/her own age is athigh risk regarding this vector in a multi-factorial assessment of
risk.
I b d h h i i f l h i
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
79/113
It may be argued that the incorporation of only the worst site
with bone loss in the posterior segment may overestimate an
individual's rate of periodontal destruction when only an
isolated advanced bony lesion is present due to local etiologicfactors, while an underestimation of the rate of destruction may
exist in a case of generalized advanced disease.
Nevertheless, in patients successfully treated for periodontitis it
has recently been demonstrated that the worst site with bone
loss in the posterior segment may, indeed, represent the past
history of destruction of the entire dentition (Persson et al,
2003).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
80/113
5. SYSTEMIC AND GENETIC ASPECTS:
In assessing the patient's risk for disease progression, systemic
factors, if known, are only considered as the fifth risk indicatorfor recurrent disease in the functional diagram of risk
assessment (Fig. 1).
In this case, the area of high risk is marked for this vector.
If not known or absent, systemic factors are not taken into
account for the overall evaluation of risk.
R h th i ti d/ dif i i fl i
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
81/113
Research on the association and/or modifying influence in
susceptibility and progression of periodontitis of physical or
psychological stress is sparse (Cohen-Cole et al, 1981; Green
et al, 1986; Freeman and Goss, 1993).
The hormonal changes associated with this condition, however,
are well documented (Selye, 1950).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
82/113
6. CIGARETTE SMOKING:
In assessing the patient's risk for disease progression,
environmental factors such as smoking must be considered asthe sixth risk factor for recurrent disease in the functional
diagram of risk assessment (Fig. 1).
While non-smokers (NS) and former smokers (FS; more than 5years since cessation) have a relatively low risk for recurrence
of periodontitis, the heavy smokers (HS; as defined by smoking
more than one pack per day) are definitely at high risk.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
83/113
Occasional smokers (OS; < 10 cigarettes a day) and moderate
smokers (MS; 10-19 cigarettes a day) may be considered at
moderate risk for disease progression.
CALCULATING THE PATIENT'S INDIVIDUAL PERIODONTAL RISK
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
84/113
ASSESSMENT (PRA) Based on the six parameters specified above, a multi-functional
diagram is constructed for the PRA.
In this diagram, the vectors have been formed on the basis of
the scientific evidence available.
It is obvious that ongoing validation may result in slight
modifications.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
85/113
A low PRA patient has all parameters within the low-risk
categories or - at the most - one parameter in the moderate-risk
category (Fig. 2).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
86/113
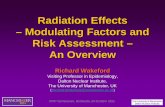
A high PRA patient has at least two parameters in high risk
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
87/113
category.
In a high-risk patient who yields high BOP percentages and
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
88/113
high numbers of residual pockets (Fig. 5), the patient's risk for
disease progression may be reduced into the moderate
category if further periodontal therapy is provided.
These two parameters (BOP and residual pockets) are easily
affected by therapy, while other parameters, such as numbers
of missing teeth or systemic and genetic factors are eitherirreversible and cannot be reduced or may only be affected with
great additional efforts (smoking cessation).
The factor determining the percentage of experienced alveolar
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
89/113
bone loss in relation to the patient's age may be reduced only
during a time period of several years.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
90/113
BIOMARKERS FOR ASSESSMENT OF PERIODONTAL
DISEASE
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
91/113
DISEASE (NEED) Traditional clinical measurements used for periodontal
diagnosis are indicators of previous periodontal disease
rather than present disease activity.
So need for development of new diagnostic tests that can
detect the presence of active disease, predict futuredisease progression and evaluate the response to
periodontal therapy.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
92/113
Advances in oral and periodontal disease diagnostic
research are moving toward methods whereby periodontal
risk can be identified and quantified by objective measuressuch as biomarkers.
Biomarkers may be defined as a substance that is
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
93/113
measured objectively and evaluated as an indicator of
normal biologic processes, pathogenic processes , and
pharmacologic responses to a therapeutic intervention.
Biomarkers, whether produced by normal healthy
individuals or by individuals affected by specific systemic
diseases, are tell-tale molecules that could be used tomonitor health status, disease onset, treatment response
and outcome.
Informative biomarkers can further serve as early sentinelsof disease.
BIOMARKERS IN GINGIVAL CREVICULAR FLUID (GCF)
AND SALIVA
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
94/113
AND SALIVA
According to Armitage (2004), more than 65 GCF constituents
have been evaluated as potential diagnostic markers ofperiodontal disease progression.
These markers can be divided into three groups: host-derived
enzymes and their inhibitors, inflammatory mediators and host-response modifiers, and byproducts of tissue breakdown.
BIOMARKERS IN GINGIVAL CREVICULAR FLUID (GCF) AND SALIVA
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
95/113
CURRENT METHODS FOR PERIODONTAL RISK
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
96/113
ASSESSMENT : In Periodontology, current methods to assess periodontal risk
factors include:
- Periodontal Risk Calculator (PRC),
- hexagonal risk diagram for Periodontal Risk Assessment
(PRA),
- PreViser Risk CalculatorTM, the periodontal risk assessment
model developed by Chandra, and
- simplified method (UniFe) (Union of European Railway
Industries) for periodontal risk assessment.
The Periodontal Risk Calculator (PRC) and the Periodontal
A t T l (PAT)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
97/113
Assessment Tool (PAT):
Page et al. developed a computer-based risk assessment tool,
the PRC, for objective, quantitative assessment of risk.
The calculation of risk using this model is based on
mathematically derived algorithms that assign relative weights
to nine factors including patient age, smoking history, diagnosisof diabetes, history of periodontal surgery, pocket depth,
furcation involvements, restorations or calculus below the
gingival margin, radiographic bone height and vertical bone
lesions.
The PRC assigns the individual a level of risk on a scale from 1
(l t i k) t 5 (hi h t i k)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
98/113
(lowest risk) to 5 (highest risk).
The Periodontal Assessment Tool (PAT) is an integral part ofthe Oral Health Information Suite (OHIS)TM (PreViser, Inc.,
Mount Vernon, WA; www.previser.com) and is considered as a
modification of the PRC method.
Following the input of only twenty-three items taken from a
ti i d t l i ti th t t li i ti
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
99/113
routine periodontal examination, the system generates linguistic
and numeric periodontal diagnoses and a risk score for future
disease, and prepares a report in two versions; one for thedentists clinical documentation and another for the patient.
The traditional documentation of six pocket depth
measurements per tooth has been reduced to the deepestpocket for each sextant. PAT also requires the greatest distance
of the bone crest to the cemento-enamel junction determined
from radiographs, again using one measurement for each
sextant and three categories: 4 mm.
The hexagonal risk diagram for Periodontal Risk Assessment
(PRA)
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
100/113
(PRA)
Lang and Tonetti28 described a functional diagram based on six
parameters for use in estimating an individuals risk for progression of
periodontitis.
The authors provided evidence supporting the inclusion of each
parameter within the diagram.
The combined assessment of each parameter allows the assessment
of the risk level for disease progression on an individual basis.
Minor modifications of the PRA model described by Lang and Tonetti
have been published later.
The periodontal risk assessment model developed by Chandra
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
101/113
In 2007, Chandra31 evaluated a novel periodontal risk assessment
model in patients presenting for dental care.
This new model based on the periodontal risk assessment model by
Lang and Tonetti where the following parameters are recorded:
- percentage of sites with bleeding on probing,
- number of sites with pocket depths 5mm,- number of teeth lost, bone loss/age ratio,
- Attachment loss/age ratio,
- diabetic and smoking status, dental status, other systemic factors and
risk determinants.
The simplified method (UniFe) for periodontal risk
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
102/113
assessment
In 2009, Trombelli and co-workers proposed a new objective
method (UniFe) (Union of European Railway Industries) in order tosimplify the risk assessment procedures.
Risk assessment according to UniFe method is based on five
parameters, derived from the patient medical history and clinicalrecordings.
parameters are as follows: smoking status, diabetic status (both
type 1 and type 2), number of sites with probing depth 5mm,bleeding on probing score, and bone loss/age records.
THE CURRENT METHODS FOR PERIODONTAL RISKASSESSMENT; ARE WE ON THE RIGHT TRACK?
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
103/113
Regarding the literature, confusing trials for setting risk
elements for periodontal disease could be found.
For instance, as reviewed by Borrel and Papapanou, a
distinction was made between putative factors (non-modifiable
background factors) and modifiable factors (environmental,acquired, and behavioral).
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
104/113
Accordingly, age, gender, and gene polymorphisms were
considered as non-modifiable background factors, whereasmicrobiota, smoking, diabetes mellitus, osteoporosis, HIV
infection, and psychosocial factors were considered as
modifiable background factors.
On the other side, some authors tended to consider smoking,
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
105/113
, g,
diabetes, pathogenic bacteria, and microbial tooth deposits as risk
factors for periodontitis, whereas age, gender, socioeconomic status,
stress, and genetic factors were considered as risk determinants, andHIV infection, osteoporosis, and infrequent dental visits were
considered as risk indicators for periodontitis.
However, it seems to be that there is a recent agreement to acceptspecific bacteria, cigarette smoking, and diabetes mellitus as the
major established risk factors for periodontitis.
The rest ofrisk elements for periodontitis still need to be confirmed
in future.
Regarding the current methods for periodontal risk assessment,
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
106/113
it seems to be that the use of risk calculators holds much
promise in the clinical practice. However, the lack of such
evidence still exists.
Chandra and Trombelli et al. tried to modify the hexagonal risk
diagram for periodontal risk assessment of Lang and Tonetti,
and found acceptable results at detecting potential risk groups.
Although the validation and accuracy of the PreViser Risk
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
107/113
g y
CalculatorTM and the information required for its use have been
reported, the whole software seems to more powerful in
demonstrating a detailed description of the patients current situation(i.e. Diagnosis), and to give several treatment options related to every
individual case.
In other words, this method is more likely to present a comprehensiveand systematic approach to clinical decision-making for periodontists.
Therefore, it is a little bit far away from being a tool that concentrates
on important and the most strong risk elements for periodontitis.
However, as is the case with the Lang/Tonetti tool, the
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
108/113
functional diagram of Chandra and of Trombelli et al. should be
only used during SPT to evaluate possible progression of the
periodontal disease and not for patients who visit the dentalclinic for the first time.
That would be more plausible.
SUMMARY
The role of risk factors and risk assessment in the prediction of
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
109/113
The role of risk factors and risk assessment in the prediction of
clinical periodontal outcomes has been a subject of much
interest.
To date, it is accepted that specific pathogenic bacteria
(Porphyromonas gingivalis, Tannerella forsythia, and
Aggregatibacter actinomycetemcomitans), cigarette smoking,
and diabetes mellitus are the major established risk factors for
periodontitis.
Although several approaches have been developed to assess
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
110/113
Although several approaches have been developed to assess
the factors which may interfere with periodontal diseases onset
and/or progression, some contradictions regarding the
classification, the definition, and the assumed implemented
factors do exist among all these methods.
REFERENCES
Chester W. Douglass. Risk assessment and management of
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
111/113
g g
periodontal disease. JADA, Vol. 137 http://jada.ada.org
November 2006.
Aous Dannan. Periodontal Risk Assessment; Are We On The
Right Track.AOSR2011;1(3):162-167.
Lei Zhang, Bradley S. Henson, Paulo M. Camargo & David T.
Wong. The Clinical Value Of Salivary Biomarkers For
Periodontal Disease. Periodontology 2000, Vol. 51, 2009, 2537.
Gun-Bak Rheu, Suk Ji, Jae-Jun Ryu. Risk assessment for
clinical attachment loss of periodontal tissue in Korean adults. J
Adv Prosthodont 2011;3:25-32.
REFERENCES
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
112/113
Raul I. Garcia, Martha E. Nunn & Thomas Dietrich. Risk
calculation and periodontal outcomes. Periodontology 2000,
Vol. 50, 2009, 6577.
A. Kazemnejad, F. Zayeri, A.R. Rokn, and M.J. Kharazifard.
Prevalence and risk indicators of periodontal disease among
highschool students in Tehran. Eastern Mediterranean Health
Journal, Vol. 14, No. 1, 2008 119.
-
7/27/2019 ASSESSMENT OF periodontal risk factors and indicators.pptx
113/113
THANK YOU