Assessment of Iatrogenic Damage to Teeth Adjacent to … · Adjacent to Crown and Bridge...
44
1 Assessment of Iatrogenic Damage to Teeth Adjacent to Crown and Bridge Preparations at Kuwait University Dental Center Elective Project Study - Course No. 703 Student: Rana Lababidi Supervisors: Prof. Hien Ngo Dr. Jaber Akbar Faculty of Dentistry, Health sciences Center Kuwait University 2013
Transcript of Assessment of Iatrogenic Damage to Teeth Adjacent to … · Adjacent to Crown and Bridge...

1
Assessment of Iatrogenic Damage to Teeth
Adjacent to Crown and Bridge Preparations
at Kuwait University Dental Center
Elective Project Study - Course No. 703
Student:
Rana Lababidi
Supervisors:
Prof. Hien Ngo
Dr. Jaber Akbar
Faculty of Dentistry, Health sciences Center
Kuwait University
2013

2
Abstract
Objectives: This study aimed to investigate the prevalence and extent of iatrogenic damages
associated with crown and bridge preparations done at Kuwait University Dental Centre (KUDC)
as well as trying to find associations, if any, between damage and different variables.
Methods: Dental stone casts reproduced from PVS final impressions of crown/FPD
preparations performed at KUDC (n=160) were collected and coded to de-identify them by an
independent person. Mesial and distal surfaces (n=270) adjacent to crown preparations, when
present, were included in the study. These surfaces were examined by the student investigator
with the use of 2.5x magnifying dental loupes. Examination criteria were degree, location, and
pattern of damage. Four variables, namely operator category, prepared tooth location,
preparation side (in relation to the operator’s dominant side), and type of restoration were then
related to these different types of damage.
Results: A very high (97.8%) prevalence of damage was observed, with the majority belonging
to the most severe categories. No statistically significant relations were found between damage
and the different studied variables. However, there was a trend for more severe damages to occur
in posterior tooth preparations as compared to anteriors and in more experienced operators as
compared to less experienced ones.
Conclusions: The prevalence of iatrogenic damage reported in this study is similar to those
which were reported in the literature. More attention should be directed towards protection of
adjacent proximal surfaces during crown preparations. It is also highly recommended to review
these surfaces afterwards and treat them if needed.
3
Introduction
Literature review:
This literature review aims to discuss the topic of iatrogenic damage to teeth adjacent to crown
and bridge preparations from a wide perspective. Since this important topic hasn’t been
sufficiently studied in literature, it was of an utmost importance to include close topics and go
further to discuss the effects of such damages and their consequences. Accordingly, this
literature review will be divided into four sections: (I) Iatrogenic damage in dentistry, (II) Rough
surfaces and plaque accumulation, (III) Consequences of iatrogenic damage, (IV) The effect of
magnification
I. Iatrogenic damage
There appears to have been no investigation of the practicalities of achieving the four aims of
crown preparation (optimum taper, margin angle, minimum reduction and avoidance of damage
to the adjacent tooth) simultaneously in the same tooth when there are adjacent teeth in contact.
Many of the investigations of this topic have been conducted on individual extracted teeth or
artefacts. Indeed the problem of combining these four aims is often ignored in textbooks where
drawings of 'ideal' preparations are shown unencumbered by adjacent teeth or gingival tissues
[1]. Moopnar & Faulkner were among the earlier investigators who studied iatrogenic damage to
teeth adjacent to crown-prepared abutments. They also discussed the possible ways to prevent
and manage possibilities. The examiners used dental stone working casts of full crown

4
preparations reproduced with silicone/polysulfide/polyether impressions. Examiners accepted
preparations that had at least one adjacent tooth surface. Both undergraduate and experienced
postgraduate dentists participated in the study. An overall number of 652 tooth surfaces were
inspected. The incidence of tooth surface damage was found to be 73.8%, which is considered to
be high [2]. An older study was published by Long and Smith (1988) which illustrated the effect
of contact area morphology on both crown preparations and MOD cavity preparations. This
study used 45 extracted teeth were grouped into 7 sets, each containing 5 teeth in the form of a
quadrant. Silicone impressions were taken before and after the preparations and poured in
plaster. Three different groups of dentists performed the preparations. The study showed that all
surfaces adjacent to the complete crown preparations were damaged. The authors classified the
damage into 3 categories (nicks, abrasions, and score lines). Many cases had a combination of
the categories of damage. The highest number of abrasions only was related to crown
preparations. This investigation highlighted the need for greater consideration of proximal tooth
surfaces during preparations and questioned the practicality of achieving traditional features of
complete crown preparation design [1].
Unexpectedly, iatrogenic damage to adjacent teeth during Class II cavity preparations was more
discussed in literature than that of crown preparations. This was unexpected since impressions
are a routine part of crown procedures while they are not in Class II preparations. In the
previously discussed study by Long and Smith, 94% of tooth surfaces adjacent to the MOD
cavities were damaged by burs. The highest number (57.4%) of nicks only was related to these
MOD preparations [1]. Meideros (2000) conducted a retrospective study on 28 patients who had
previous Class II restorations and compared them to contralateral control teeth in the same
5
patients. The examiners used elastic separators to gain access to tooth surfaces adjacent to Class
II restorations. Light body impressions were taken for these surfaces after separation and
examined by light microscope and scanning electron microscope for iatrogenic damage.
Impressions that had iatrogenic damage got further examined with scanning electron microscopy.
The results of the study showed that 49-60% of the studied surfaces presented signs of iatrogenic
damage. Damage was 3 times more prevalent in permanent teeth compared to primary teeth. The
study also specified the types of damage and their percentages, with grooves being the most
common type [3]. Another study, conducted by Lussi and Gygax, compared the occurrence of
iatrogenic damage to tooth surfaces adjacent to Class II preparations when using conventional
rotary instruments to that caused by a new method and instrumentation (a combination of the file
system with a specially designed bur). A total of 134 first-intervention preparations were studied.
Silicone impressions were taken before and after cavity preparation and Stereomicroscopic
examination of the poured models was conducted to evaluate the damage. Results of the study
showed that using conventional methods, all adjacent tooth surfaces showed deep damage
compared to less incidence & severity of damage in the test group (a file system combined with a
special bur) [4]. Qvist et al (1992) conducted a study to evaluate the effect of iatrogenic damage
to neighboring teeth during Class II preparation on the need for subsequent operative caries
treatment. Primary as well as permanent teeth were included in this study. The examiners studied
190 unfilled proximal surfaces adjacent to first-time Class II preparations. Stereomicroscopic
examination of the models reproduced from alginate impressions was conducted to evaluate the
damage. The results showed an incidence rate of 64% in primary teeth compared to 69% in
permanent teeth. Bur trauma was observed in about two thirds of untreated surfaces, with
scratches and grooves being the most common findings. Patients were followed-up for 7 years to

6
check for the occurrence of caries at the affected sites. The study came up with a conclusion that
affected surfaces needed later operative procedures more (3.5 folds for primary, 2.5 folds for
permanent) than those that were not affected [5]. In 2002, Niek et al published a study that
compared the effect of 2 finishing techniques of class II adhesive preparations on micro leakage
& damage to adjacent teeth. 30 class II preparations on extracted teeth fixed in phantom heads
were beveled with a bur (control group); while a sonic preparation device (experimental group)
was used to finish another 30 restorations. Teeth were then restored with composite. Damage to
adjacent teeth was assessed using light microscopy. The results of the study showed 80% of
damage in the control group opposed to 30% in the experimental group [6].
Iatrogenic damage can also occur during the finishing procedures of Class V composite
restorations. This topic was studied by Mitchell et al (2002). Finishing was performed using 3
different systems: aluminum oxide disks, tungsten carbide burs, or ultrafine finishing diamond
burs. All 3 finishing systems tested resulted in iatrogenic damage to enamel and dentine, with
aluminum oxide disks being more destructive to dentine than enamel. Two types of composites
were also tested and showed no difference in loss of surrounding tooth structure [7].
Rubber dam clamps, which are routinely used for isolation during operative procedures, were
looked-into from another angle by Jeffery and Woolford (1989). The examiners collected a
number of teeth that had been extracted surgically, rather than by forceps, to study damage
caused by metal rubber dam clamps. They used a special apparatus to load the teeth with clamps
and then examined them by scanning electron microscopy. The results showed that damage
occurred in the form of depressive disruption of cementum or dentine surfaces [8].

7
Although interdental stripping is done intentionally, mostly for orthodontic purposes, its final
result can be comparable to that of iatrogenic damage during crown preparation which causes
loss of tooth structure and some degree of surface roughness. In this part of literature review, we
aim to discuss the effects of interdental stripping, which is a more controlled process, to have an
insight on how even planned procedures can cause harm, which leads us to seriously think about
un-intentional stripping as per during preparation on adjacent teeth. Air-rotor stripping is a
commonly used method to alleviate crowding in the permanent dentition that usually results in
50% enamel reduction. In this study, 40 patients were treated with ARS and examined a
minimum of 1 year after the procedure. A fine tapered diamond bur was used for enamel
reduction, and a diamond-coated strip was subsequently used for polishing. No fluoride or
sealant application followed the procedure. The results showed that ARS does not result in an
increase in enamel caries in fixed orthodontic patients [9]. Arman et al (2006) investigated
ultramorphology, surface roughness, and micro hardness of permanent and deciduous tooth
enamel after various stripping methods. They also used scanning electron microscopy (SEM) for
quantitative evaluation after stripping. Stripping methods studied included: stripping disks,
diamond coated metal strip, stripping disk plus fine Sof-Lex discs, diamond coated metal strip
plus Sof-Lex discs, chemical stripping, and a control group. The results showed that all stripping
protocols resulted in roughness and grooving of enamel surfaces regardless of enamel type. No
morphological difference was noted between primary and permanent teeth. Surface roughness
values of stripped enamel were significantly greater than unstrapped enamel. Sof-Lex discs were
found to produce smoother surfaces when used after stripping [10]. In their paper, Zachrisson et
al (2007) assessed dental health in mandibular incisors more than 10 years after enamel
reduction. The study examined a number of patients who have had mesiodistal enamel reduction
8
in all 6 anterior mandibular teeth more than 10 years previously. The enamel reduction was
performed with fine or medium grit diamond disks at medium speed with careful air-cooling
during the grinding. The control group included students who haven’t had enamel reduction in
their mandibular anterior teeth. Caries diagnosis was done by 3 methods: traditional explorer
catch, radiographic examination, and trans illumination. The results showed no new caries
lesions in the patients of the experimental group. The examiners came up with the conclusion
that interdental enamel reduction according to the protocol used did not result in iatrogenic
damage [11]. In 2011, Zachrisson conducted another study to assess caries risk in posterior teeth
after interproximal enamel reduction. The sample included all patients in a consecutive series of
80 who had stripping at least 4 years before examination. The stripping was performed using
perforated diamond-coated stripping disks. On examination, bitewings of the involved teeth were
taken and interproximal caries on each surface were recorded according to a 5-level scale.
Contralateral, unstrapped teeth were used as a control group. The results agreed with
Zachirrson’s previous study and showed no significant difference in caries development between
stripped and control teeth, and no evidence of harm to teeth and supporting structures when
mesiodistal enamel reduction is done within recognized limits and in appropriate situations [12].
An in vitro study by Twesme et al sought to evaluate the effect of air-rotor stripping on the
susceptibility of human enamel to demineralization. 22 extracted mandibular first molars with
sound proximal surfaces underwent proximal enamel reduction with a 699L tapered fissure bur
on one side. No more than 0.5 of enamel thickness was removed, and the enamel walls were
finished with an ultrafine diamond bur. The other proximal sides (un-stripped) were used as
control. Lesion depth and mineral content on the abraded and intact surfaces was measured with
contact microradiography and computerized image analysis. The results showed that air-rotor

9
stripping increases the susceptibility of human proximal enamel demineralization. The authors
came with a recommendation that the caries potential (DMF scores) of each patient to be
evaluated before removing proximal enamel [13]. A scanning electron microscopy (SEM) study
was carried by Piacentini and Sfondrini to compare enamel polishing methods proposed in the
literature after air-rotor stripping. The examiners collected 48 healthy extracted human teeth and
mounted them in typodonts to simulate clinical conditions. 7 different methods of stripping then
polishing were used. The teeth were then examined by SEM. The results of the SEM
demonstrated that it is not possible to eliminate, with normal polishing and cleaning methods, the
furrows left on enamel by diamond burs, diamond disks, and tungsten carbide burs. In agreement
with previously mentioned studies, the results showed that by polishing with Sof-Lex disks after
stripping with tungsten carbide burs, it is possible to obtain a well-polished enamel surface that
many times appears smoother than intact enamel [14]. Zhong et al performed another SEM study
that investigated in vivo the interproximal surface roughness and the patients’ subjective ratings
of treatment with a 3-step method for interdental enamel reduction. 32 patients undergoing
orthodontic treatment that requires interdental stripping were enrolled. A total of 296 sound tooth
surfaces underwent the enamel reduction. Enamel reduction was first undertaken with a
perforated diamond-coated disk, and then polished with Sof-Lex XT fine and ultrafine disks. The
maximum amount of enamel removed was 0.3 mm for anterior teeth, and 0.5 mm for posterior
teeth. Impressions were then taken by an injection-type vinyl polysiloxane material then casted
in epoxy resin to fabricate replicas that were later examined by SEM. The SEM evaluation
showed that more than 90% of all surfaces were polished either well or very well. There was no
significant difference between roughness of anterior teeth and that of posterior teeth. The vast
majority of patients felt very little discomfort, if any. The clinical conclusion came with

10
agreement with the previously mentioned study by Piacentini and Sfondrini showing that using
the previously mentioned technique produced enamel surfaces that are smoother than untreated
enamel [15].
II. Plaque accumulation on rough surfaces
Since tooth preparation is usually initially done with coarse diamond burs, it is expected to cause
surface roughness if it touches the adjacent tooth surface. This roughness is not likely to get
smoothed later by finer diamond burs because by then, the contact would have already been
relieved and these burs have a lesser chance to touch these surfaces. Many articles in literature
related plaque accumulation to tooth surface roughness, regardless of the procedure which
caused the roughness. As in many of the previously discussed studies in this review, SEM was
used to measure surface roughness caused by interdental stripping and its effect on bacterial
adhesion. An interproximal enamel reduction of 0.5 mm was performed on 2 groups of sound
premolars (in vitro and in vivo) by means of a coarse diamond-coated bur. It was found that fine
diamond burr left furrows of almost the same size as those caused by the coarse bur. In the in
vivo part of the study, Sof-Lex strips (3M, St Paul, USA) were used and lead on one hand to a
considerable smoothness (in coherence with other studies discussed), but on the other hand deep
furrows caused by coarser strips cut across the prepared surface, which got filled with plaque.
Flossing every night in these areas did not succeed in preventing plaque accumulation at the
bottom of the furrows [16]. A recent paper published by Mei et al studied the influence of
surface roughness on streptococcal adhesion forces to composite resins. 2 types of light-cured
orthodontic composites were formed into disks and used in the study. These were polished and
11
grinded to obtain smooth, moderately rough, and rough surfaces. Atomic force microscopy
(AFM) was used to measure the surface roughness of composites as well as adhesion forces of
Streptococcus Sanguinis and Streptococcus Mutans. The results showed a significant linear
correlation between bacterial adhesion forces and roughness of the composite surfaces. Bacterial
adhesion forces and their strengthening over time were proofed to be dependent on the surface
roughness of the composites. The researchers, however, found that composite surface roughness
affects adhesion forces with S.mutans less than that with S.sanguinis [17]. In their study titled
“The influence of abutment surface roughness on plaque accumulation and peri-implant
mucositis”, Bollen et al (1996) performed microbiological examinations on 6 patient having 2
types of implant abutments (standard and ultrapolished) after 3 and 12 months of implant
insertion. The results showed that the reduction of roughness of intra oral hard surfaces below
the threshold Ra of 0.2 µm will result in a retardation of the supra- and sub gingival plaque
maturation [18]. Bollen et al also published a literature review (1997) that compared surface
roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention.
This review analyzed the initial surface roughness of different dental materials and the effect of
different treatment modalities on this initial surface roughness and compared them to the
threshold surface roughness of 0.2 µm. The results showed that an increase in surface roughness
above a threshold (Ra=0.2 µm) resulted in a simultaneous increase in plaque accumulation,
thereby increasing the risk for both caries and periodontal inflammation. As for finishing
procedures to achieve a smooth surface, this review recommended SnO2 or pumice finishing for
amalgam, rouge polishing for gold surfaces, Sof-Lex disks or carbide burs for ceramics. As for
resin composites, acrylic resins, and glass ionomer cements, the review suggested compressing
them against a polyester strip, polishing them with alumina disks, Sof-Lex disks, rubber wheels,

12
or diamond paste [19]. To study the influence of surface roughness on plaque formation,
Quirynen et al (1990) did a clinical trial on 16 volunteers in whom 2 strips (one made of
fluorethylenepropylene and the other made of cellulose acetate) were stuck to the labial surface
of central incisors. Half of the surface of each strip was smooth while the other was rough. After
3 then 6 days, samples were taken from each half as well as from control surfaces and examined
under a light microscope to detect bacterial growth. The results showed a more mature plaque on
rough surfaces compared to others, indicated by fewer cocci and a higher proportion of rod-
shaped bacteria. It was concluded that a surface with a low roughness clearly can delay plaque
accumulation in vivo [20]. The effect of different surface finishing and polishing methods for 3
types of composite resins and 1 ceramic material on surface roughness and adhesion of S.mutans
bacteria. Specimens of these materials were put into 4 groups, each of which received a one of
these finishing techniques: ( diamond rotary cutting instruments, Sof-Lex disks, silicone-carbide
rubber points- Shofu, or a felt wheel with diamond paste). Surface roughness was measured with
a profliometer. Surface roughness varied depending on surface treatment and composition of the
restorative materials tested. In agreement with previously discussed publications, Sof-Lex and
Shofu polishing systems produced the smoothest surfaces. The lowest bacterial adhesion was
also found with Sof-Lex and Shofu polishing kits. Maximum vital bacterial adhesion was found
on surfaces finished with the diamond rotary cutting instrument. In conclusion, a significant and
positive correlation was found between surface roughness and vital bacterial adhesion [21].
Plaque accumulation and gingival inflammation investigated by Rosenberg and Ash in relation to
root roughness. In this study, 58 teeth from 20 prospective denture patients were randomly
assigned into curette, Cavitron, or control groups. 1-8 months after instrumentations, plaque
scores and gingival biopsies were taken. They concluded that root surface roughness was not

13
related significantly to the mean inflammatory index of the adjacent gingival tissues, nor to the
supra-gingival plaque accumulation [22].
III. Consequences of iatrogenic damage
Since teeth that are to be prepared for crowns usually have had severe damage and large
proximal caries, it is interesting to know that tooth surfaces adjacent to them already have a
higher chance of caries, which raises the question about iatrogenic preparation damage adding to
the harm of these surfaces. Vanderas et al (2004) conducted a 4-year prospective study on
permanent first molars adjacent to primary second molars with interproximal caries that showed
that this situation increases the risk of developing mesial surface caries lesions on the permanent
first molars [23]. In their paper titled: “In vitro demineralization of human enamel natural and
abraded surfaces: A micromechanical and SEM investigation”, Xue et al were able to postulate
that the existence of natural surface enamel will influence and reduce in vitro enamel rod
demineralization. In particular this study has shown that abraded samples exposed to in vitro
demineralization form deeper lesion depths and greater loss of mechanical properties than un-
abraded samples subjected to the same demineralization. Un-abraded samples in vitro
demineralization were found to form characteristic subsurface demineralization while the surface
remains intact. This was not found in abraded samples with the experimental demineralization
solution. It was also concluded that natural enamel surface acts as a caries resistant barrier to
protect deep enamel from acid dissolution. The in vitro demineralization pattern of un-abraded
samples was also found to more closely resemble the pattern of a natural white spot lesion [24].

14
IV. Effect of magnification
It is a fact that magnification has an important role in dentistry. As for our topic, magnification
was used both for some crown preparations, and for the assessment of damage to adjacent
surfaces, which makes us question whether or not magnification has an effect on both damage
and assessment of damage. Lussi et al reported on the effect of magnification on the iatrogenic
damage to tooth surfaces adjacent to Class II preparations. A group of dentists performed Class
II cavity preparations on phantom heads without the use of magnification, then after 2 months
did similar preparations utilizing a surgical telescope system. Damage was assessed using a light
microscope that was equipped with a video camera. The results indicated no reduction of
iatrogenic preparation trauma to surfaces adjacent to approximal preparation sites when a
surgical telescope system was used. The study came with a conclusion that surgical telescopes do
not decrease damage to adjacent tooth surfaces [25]. Kielbassa et al performed an in vitro study
to evaluate cavitation in proximal caries lesions at various magnification levels. A number of
extracted teeth were assessed radiographically and then using naked eye, 4.3x magnification
eyeglasses, a 10x stereo microscope, or a 200x scanning electron microscope. The results
showed that the use of magnification aids significantly increased the detected cavitations. The
study came with a recommendation to use magnification in clinical observation of directly
accessible lesion sites [26]. Another in vitro study was conducted by Forgie et al on the effect of
magnification in restoration removal. Class I composite restorations were formed on extracted
teeth, measured, and then set in phantom heads. The restorations were then removed with the
same diamond bur either using unaided vision or 2.6x magnification. In this study, magnification
has been shown to decrease the cavity size change by about 5% compared with unaided vision

15
and whilst it is difficult to predict the importance of this reduction, it is clear that over the course
of a practicing career, the effect will be positive [27].
Overview on the importance of this study:
Fixed prosthodontics is a major component of restorative dentistry. As stated by Shillingburg
[28]: “the indications for full coverage have increased because of the preservation of teeth that
may have been removed in the past”. This trend is likely to increase over the immediate and long
term future as the population is getting largely older and teeth are being retained in function for
much longer. By searching different literature sources in fixed prosthodontics, it was obvious
that the focus is mainly on technical aspects of preparation, designs, and dental materials while
the effect on neighboring teeth was mostly ignored and rarely discussed. The guiding principle in
medical ethics is “to cause no harm”, which raises a controversial question on crown
preparations when we consider iatrogenic damage to adjacent tooth surfaces. The Oxford
dictionary defines iatrogenic damage to be those that are “caused by examination or
treatment”. This topic is not commonly discussed as it is difficult for health care
professionals to accept that unnecessary harm can happen to patients during a routine
procedure such as a cavity or crown preparations. In dentistry, the risk of iatrogenic
damage during restorative procedures is high due to the fact that high speed cutting
instruments are used with indirect vision and teeth are in close contact. Breaking through
the contact points is when iatrogenic damage is most likely to happen.

16
Aims/ Objectives:
The aim of this pilot study is to determine the prevalence and extent of iatrogenic damages
associated with crown and bridge preparations, which were done at Kuwait University Dental
Centre (KUDC). This was further related to variables that could be associated with operator and
tooth.
Materials and Methods
After getting the ethical clearance from the Ethical Committee of the Health Sciences Centre of
Kuwait University, dental stone casts reproduced from PVS final impressions of crown/FPD
preparations were collected from Kuwait University Dental Clinic laboratory during a period of
7 months (from 29/11/2012 to 27/6/2013).
The study casts were examined after being removed from the impressions. No further
manipulation was done, so any damage to the proximal surface of the adjacent tooth could only
be associated with the clinical procedures. Only casts with fixed prosthodontic preparations
involving the proximal area with at least one adjacent surface were accepted.
A total of 160 casts were collected. Of which, 152 casts with 207 preparations and 270
registrable surfaces were included. The crown preparations were undertaken by four groups of
operators:

17
(1) Junior students (second semester of fifth year and first semester of sixth year)
(2) Senior students (second semester of sixth year and first semester of seventh year)
(3) General dental practitioners
(4) Prosthodontists
A special sheet was used to register information about the study casts by the laboratory chief
technician (appendix A). Casts were then coded by an independent person and de-identified
before the examination. Examination of casts and recording of damage according to the
classifications to be mentioned were performed by the student investigator. For ease of recording
and to make later comparison possible, mesial and distal tooth surfaces adjacent to each
preparation were recorded separately. (Figure 1)
The casts were examined in the pre-clinical simulation laboratory under an adjustable light, using
2.5x magnifying loupes. Damage to surfaces adjacent to crown-prepared abutments was the
classified as follows:
-Degree of damage (adapted from Moopnar and Faulkner, 1999):
0: no damage visible to the naked eye or under magnifying glass (x2.5).
Figure 1: mesial and distal surfaces a
Mesial
surface (M) Distal
surface (D)
18
1: slight damage visible to the naked eye and identifiable with a magnifying glass.
2: obvious damage.
**For statistical reasons, 0 and 1 categories were combined during analysis into 1 category
called “slight damage”.
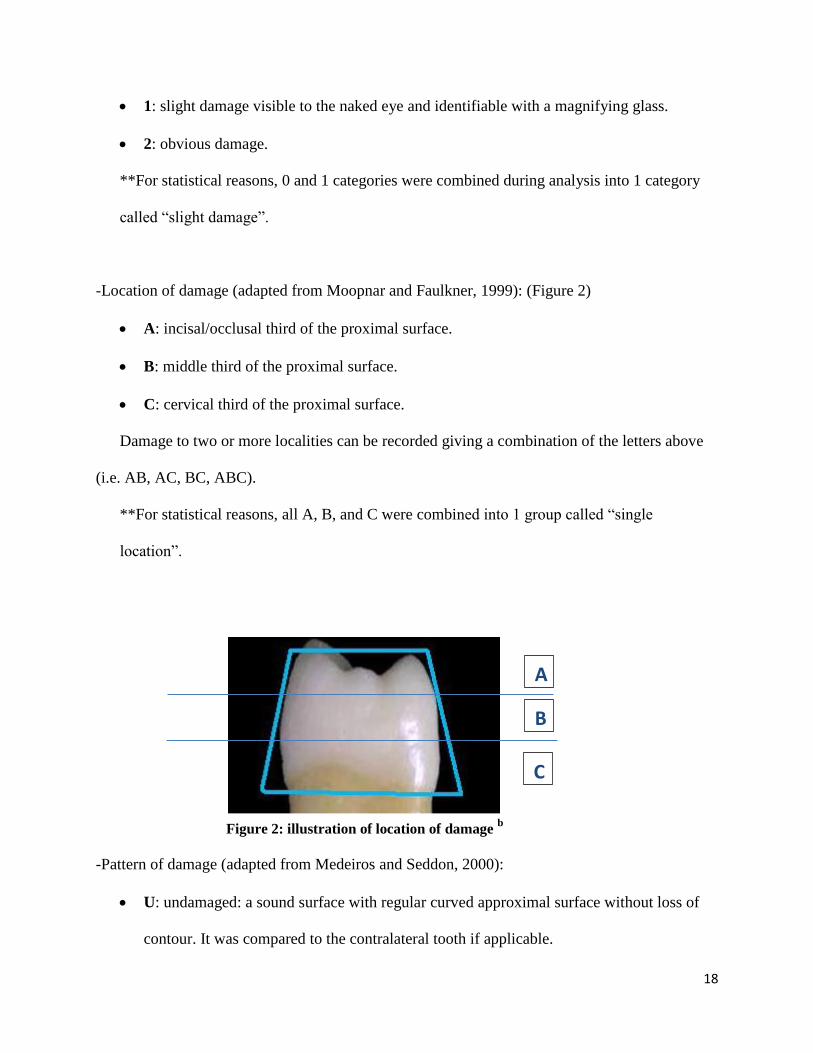
-Location of damage (adapted from Moopnar and Faulkner, 1999): (Figure 2)
A: incisal/occlusal third of the proximal surface.
B: middle third of the proximal surface.
C: cervical third of the proximal surface.
Damage to two or more localities can be recorded giving a combination of the letters above
(i.e. AB, AC, BC, ABC).
**For statistical reasons, all A, B, and C were combined into 1 group called “single
location”.
-Pattern of damage (adapted from Medeiros and Seddon, 2000):
U: undamaged: a sound surface with regular curved approximal surface without loss of
contour. It was compared to the contralateral tooth if applicable.
A
B
C
Figure 2: illustration of location of damage b

19
I: indentation: a regular defect without an orientation, roughly circular or irregular in
shape. (picture 1)
S: scratches: narrow, shallow scorelines, usually multiple with a consistent orientation.
(picture 2)
G: groove: a deeper defect, length greater than width with a vertical or horizontal
orientation. (picture 3)
X: extensive damage: damage involving a large area of the approximal surface bucco-
lingually or a combination of more than 2 types of damage. (picture 4)
**For statistical reasons, the pattern of damage was collapsed to 3 main groups: “Single
type- included S,G,I”, “Combination of 2 types- included S+G,S+I,G+I”, “Extensive
damage-X”.
Picture 1:
indentations
Picture 2:
scratches
Picture 3: groove
Picture 4: extensive
damage

20
Examination results for each cast were recorded into an individual card (appendix B). After
examining all casts, data was entered into computer software (SPSS), and codes were broken to
obtain the following information about each cast and preparation:
-Operator’s category: junior student, senior student, general dentist, prosthodontist.
-Type of restoration: single crown all ceramic, single crown all metal, single crown porcelain
fused to metal (PFM), inlay, onlay, veneer, all ceramic fixed partial denture (FPD), PFM FPD.
For statistical reasons, these were grouped into 3 categories: single PFM, single other, and FPD.
-Tooth identification: upper right posterior (#18-#14), upper right anterior (#13-#11), upper left
anterior (#21-#23), upper left posterior (#24-#28), lower left posterior (#38-#34), lower left
anterior (#33-#31), lower right anterior (#41-#43), lower right posterior (#44-#48). To allow later
comparison between upper and lower teeth and for statistical reasons, these groups were
collapsed into upper posterior, upper anterior, lower posterior, lower anterior.
-Operator’s dominant hand-side: this was, where the side to which the prepared tooth belongs,
linked to the operator. A list of left-handed operators was obtained, and matching between the
teeth and operators gave either a ‘coinciding’ for matching dominant hand side and tooth side,
and a ‘non-coinciding’ for non-matching ones.
Around two months after the first examination, 20 casts (~12.5% of the sample), with 25
surfaces, were chosen randomly for re-examination by the same initial examiner. Repeat
observations were made on these surfaces to determine the intra-examiner reliability. The result
was an agreement occurrence of 84.7% (intra-examiner reliability). The agreement between the 2
examinations was significant (Kappa= 0.712, p<0.001).

21
Statistical analysis: Data recorded for the categorical variables: Operator’s category,
dominant hand side, tooth number, restoration type; degree, location and pattern of damage with
surface type; were entered and analyzed using computer software, “Statistical Package for
Social Sciences (SPSS version 21, IBM Corp., Armonk, NY,USA). Frequency analysis was
carried out to review the data, and some variables were coded and recoded for statistical analysis.
Descriptive statistics has been presented as number and percentages, and Chi-square or Fisher’s
test was performed to detect any association or significant difference between the variables. A
normal Z-test was used to find any significant difference between two proportions. Cohen’s
Kappa was applied to measure the agreement between two set of observations for reliability. A
probability value ‘p’ < 0.05 was considered statistically significant.
Results
In total there were 207 tooth preparations with 270 adjacent tooth surfaces present. Out of the
207 tooth preparations included in this study, the majority (73.9 %) were done by students and
the remaining (26.1%) by dentists. 56% of the prepared teeth were located on the operators’
dominant hand side, while 44% occurred on the opposite side. The maximum preparations
(80.7%) were for posterior teeth, with maxillary preparations being more than mandibular in
total. Almost two third (67.1%) of the preparations were for single PFM crowns. (Table 1)
Of the 270 units (tooth surfaces) inspected, only 6 (2.2%) surfaces showed no damage from
cutting burs or diamonds, while all the other surfaces showed damage. As for the degree of
damage, 44 surfaces were found to have slight damage, while 220 with obvious damage.

22
Regarding location of damage, it was observed that all damaged surfaces but three shared
damage in “location B”, with almost ¾ (74.6%) of the surfaces having damage in all locations
occluso-gingivally “ABC”. The most common pattern of damage found was “extensive-56%”
with “scratches -16.3%” being the second common. (Table 2), (Figures 3,4, 5)
ABC 75%
AB 12%
BC 8%
Single location 5%
Figure 4:Location of Damage
Obvious damage 81.5%
Slight damage visible to the
naked eye and identifiable
with a magnifying
glass 16.3%
Damage not visible to
naked eye or under
magnifying glass (x2.5)
2.2%
Figure 3: Degree of damage

23
As regards the degree of damage in relation to different variables, the results showed that the
obvious damage was higher (88.7%) in preparations done by general dentists and prosthodontists
as compared to students (78.4%). No association was found between degree of damage and the
operator’s dominant side. Also for tooth location, the preparations of upper posterior teeth
seemed to cause the most obvious damage (83.8%) to adjacent surfaces as compared to lower
posterior teeth (78.7%). The type of restoration showed slightly higher association with obvious
damage for FPD abutments’ preparations (84%) than either of the single restoration (Table 3).
Regarding location of damage, the preparations by general practitioners and prosthodontists were
found to have more damage to adjacent surfaces in all three locations together ‘ABC’ (80.8%)
compared to students (72%). The dominant hand side again showed no relation to the location of
damage. No significant differences were found in the location of damage and tooth location,
though preparations of posterior teeth in general caused the maximum damage in the three
locations together ‘ABC’. FPDs and single PFM crowns were found to have more damage in all
three locations ‘ABC’ (76% & 75.6% respectively) than single others (66.7%). (Table 4)
In case of the pattern of damage, preparations by general practitioners showed maximum
extensive damage (78.6%) compared to any other operator, especially students (53.8%,
p=0.023). It was also observed that the highest percentage of extensive damage was that of the
Extensive damage
57%
Scratches 17%
Scratches & indentations
7%
Grooves 6%
Scratches & grooves
5% Indentations
4%
Grooves & indentations
4%
Figure 5:Pattern of Damage

24
general practitioners who also had the least percentage of single type. Same as for ‘degree’ and
‘location’, no relation was seen between the operator’s dominant hand side and the pattern of
damage. A significant associations was, however, found between pattern of damage and tooth
location (p=0.014).The most extensive damage occurred in the upper posterior teeth group
(67.3%) compared to any other teeth location. As for the type of restoration, FPD preparations
were found to cause the least extensive damage in the pattern compared to either of the two types
(Table 5). Overall, upper teeth showed higher tendency to have obvious and extensive damage as
compared to lower teeth (Table 6).
Figure 6 above shows the relation between mesial and distal tooth surfaces vs. upper and lower
teeth to the most severe categories of damage. An association was observed between mesial and
lower as well as distal and upper.
79.7
87.3
69.2
78.2
60 62.8
73.7
87
74.7 76.1
49.3
56.5
0
10
20
30
40
50
60
70
80
90
100
Mesial Distal Mesial Distal Mesial Distal
Figure 6:Percent Damage in Upper & Lower for Mesial and
Distal according to Degree, Location and Pattern
Upper
Lower
Pattern:
Extensive
Degree:
Obvious
Location:
ABC

25
Table 1: General Characteristics of the Study Sample
Characteristic No. of Preparations
(N=207)
Percent
(%) Operator: Junior Student
71
34.3
Senior Student 82 39.6
General Practitioner 19 9.2
Prosthodontist 35 16.9
Operator’s Dominant side
Coincide 91 44.0
Non-Coincide 116 56.0
Tooth Identification
URP 33 15.9
ULP 49 23.7
URA 18 8.7
ULA 15 7.2
LRP 37 17.9
LLP 48 23.2
LRA 4 1.9
LLA 3 1.4
Restoration Type
Single PFM 20 9.7
Single Other* 139 67.1
FPD 48 23.2
* Includes: Single all ceramic, single all metal, on lay & in lay

26
Table 2: Degree, Location and Pattern of Damage in Mesial and Distal Surfaces.
Level of Damage Mesial (n=145) Distal (n=125) Total (n=270)
Degree No % No % No %
No damage visible to the
naked eye or under
Magnifying glass (x2.5).
5 3.4 1 0.8 6 2.2
Slight damage visible to the
naked eye and identifiable
with a magnifying glass
29 20.0 15 12.0 44 16.3
Obvious damage 111 76.6 109 87.2 220 81.5
Location
AB 18 12.9 15 12.1 33 12.5
BC 15 10.7 7 5.6 22 8.3
ABC 101 72.1 96 77.4 197 74.6
Single location* 6 4.3 6 4.8 12 4.6
Pattern
Undamaged 5 3.4 1 0.8 6 2.2
Scratches 26 17.9 18 14.4 44 16.3
Grooves 7 4.8 9 7.2 16 5.9
Indentations 7 4.8 4 3.2 11 4.1
Extensive damage 76 62.4 75 60.0 151 55.9
Scratches & grooves 7 4.8 7 5.6 14 5.2
Scratches & indentations 11 7.6 8 6.4 19 7.1
Grooves & indentations 6 4.1 3 2.4 9 3.3
* Mesial (2A, 3B & 1C) and Distal (1A, 4B & 1C)

27
Table 3: Degree of damage in relation to different characteristics
Characteristic
N
Slight damage visible to
the naked eye and
identifiable with a
magnifying glass
Obvious
damage
p-value
N (%) N (%)
Operator:
Junior student 89 22 (24.7) 67 (75.3)
0.135 Senior student 101 19 (18.8) 82 (81.2)
General Practitioner 28 2 (7.1) 26 (92.9)
Prosthodontist 52 7 (13.4) 45 (86.6)
Operator’s dominant
hand side:
Coincide 118 21 (18.5) 97 (81.5) 0.788
Non-Coincide 152 29 (19.1) 123 (80.9)
Tooth location:
UP 109 14 (12.8) 95 (87.2)
0.226 UA 39 10 (25.6) 29 (74.4)
LP 114 24 (21.1) 90 (78.9)
LA 8 2 (25.0) 6 (75.0)
Type of restoration:
Single PFM 187 33(17.6) 154 (82.4)
0.372 Single other 33 9 (27.3) 24 (72.7)
FPD 50 8 (16.0) 42 (84.0)
*GP vs Students (92.9% vs 75.3%, p=0.082), ** UP vs UA (87.2% vs 74.4%, p=0.065)

28
Table 4: Location of damage in relation to different characteristics
Characteristic N Single
location
AB BC ABC p-value
N (%) N (%) N (%) N (%)
Operator:
Junior student 85 7 (8.2) 7 (8.2) 9 (10.6) 62 (73.0)
0.199 Senior student 101 4 (4.0) 14 (13.8) 11 (10.9) 72 (71.3)
General Practitioner 28 1 (3.6) 4 (14.3) 0 (0.0) 23 (82.1)
Prosthodontist 50 0 (0.0) 8 (16.0) 2 (4.0) 40 (80.0)
Operator’s
dominant hand side:
Coincide 115 5 (4.3) 14 (12.2) 9 (7.8) 87 (75.7) 0.988
Non-Coincide 149 7 (4.7) 19 (12.8) 13 (8.7) 110 (73.8)
Tooth location:
UP 107 4 (3.7) 12 (11.2) 10 (9.3) 81 (75.8)
0.770 UA 36 2 (5.6) 4 (11.1) 5 (13.9) 25 (69.4)
LP 113 5 (4.4) 15 (13.3) 7 (6.2) 86 (76.1)
LA 8 1 (12.5) 2 (25.0) 0 (0.0) 5 (62.5)
Type of restoration:
Single PFM 184 8 (4.3) 21 (11.4) 16 (8.7) 139 (75.6)
0.854 Single other 30 1 (3.3) 6 (20.0) 3 (10.0) 20 (66.7)
FPD 50 3 (6.0) 6 (12.0) 3 (6.0) 38 (76.0)

29
Table 5: Pattern of damage in relation to different characteristics
Characteristic N Single type Two types Extensive p-value
N (%) N (%) N (%)
Operator:
Junior student 85 28 (32.9) 10 (11.8) 47 (55.3)
0.130 Senior student 101 28 (27.7) 20 (19.8) 53 (52.5)
General Practitioner* 28 2 (7.1) 4 (14.3) 22 (78.6)
Prosthodontist 50 13 (26.0) 8 (16.0) 29 (58.0)
Operator’s
dominant hand side:
Coincide 115 31 (27.0) 17 (14.8) 67 (58.2) 0.903
Non-Coincide 149 40 (26.8) 25 (16.8) 84 (56.4)
Tooth location:
UP** 107 20 (18.7) 15 (14.0) 72 (67.3)
0.014 UA 36 14 (38.9) 6 (16.7) 16 (44.4)
LP 113 35 (31.0) 17 (15.0) 61 (54.0)
LA 8 2 (25.0) 4 (50.0) 2 (25.0)
Type of restoration:
Single PFM 184 44 (23.9) 33 (17.9) 107 (58.2)
0.383 Single other 30 9 (30.0) 3 (10.0) 18 (60.0)
FPD 50 18(36.0) 6 (12.0) 26 (52.0)
*GP vs Students (78.6% vs 53.8%, p=0.023), ** UP vs UA (67.3% vs 44.4%, p=0.025)
Table 6: Degree, Location and Pattern of Damage (%) in upper and lower
teeth
Damage Upper Lower Both p-value
Degree Slight 16.2 21.3 18.5 0.283 Obvious 83.8 78.7 81.5
Location Others 25.9 24.8 25.4 0.841 ABC 74.1 75.2 74.6
Pattern Others 38.5 47.9 42.8 0.121
Extensive 61.5 52.1 57.2

30
Discussion
The results of this study showed a very high incidence of iatrogenic damage to teeth adjacent to
prepared abutments for fixed prosthesis. A review of the literature showed that there were few
papers that discussed this topic or even related ones. The high incidence of iatrogenic damage
reported in this study (97.8%) agrees with the previous studies on this topic: (100%) by Long
and Smith [1] and (73.8%) by Moopnar and Faulkner
[2]. High incidence of iatrogenic damage
was also reported in studies on class II cavity preparations and it ranged from 60% (Medeiros
and Seddon) [3] to 100% (Lussi and Gygax)
[4].
Regarding the “degree” of damage, 81.5% of our sample had obvious damage as compared to
49.2% by Moopnar and Faulkner [2]. Both results showed that the majority of surfaces were
damaged obviously, but the prevalence in our study was relatively higher.
Similar pattern was observed for the “location” of damage, where we found that 95.4% of
damage was on multiple locations, 74.6% of which was involving all 3 locations “ABC”, as
compared to Moopnar and Faulkner’s study (65.7 % and 42.2% respectively) [2].
We found in our study that the most prevalent “pattern” of damage was extensive (55.9%), and
that most types of damage occur in combination, which was also concluded by Long and Smith
[1]. However, other studies found grooves and/or scratches to be the most common [1, 3, 5].
In our results, it was observed that less severe damage happened in students’ preparations as
opposed to those done by doctors, but this difference was not statistically significant. The results
of another study supported this trend that we observed and found a statistically significant
relation where the group of graduate operators was found to have more iatrogenic damage

31
happening than that of undergraduate students (64% vs. 23%) [3]. On the other hand, some other
studies found no difference between different operator groups when classified based on clinical
experience and qualification [1, 2, 4, 25]. Our result can be explained by the fact that students
usually get assistance during their prosthodontic work especially during their first preparations
where a big part of the work is done by the supervisors. This explanation was also suggested by
Medeiros and Seddon who stated that this “might be an indication of more cautious and careful
approach to operative procedures by less experienced but supervised personnel” [3].
Our results showed that damage is more prevalent and severe in the maxillary teeth than
mandibular, with a more tendency of posterior teeth to be damaged than anteriors (82.9% and
74.5% respectively). The results of the study by Medeiros and Seddon concede with our finding
that upper teeth are more damaged than lowers (61% vs. 25%) [3]. While the results of the study
by Moopnar and Faulkner agreed with our findings that posterior teeth are more damaged than
anteriors (83.1% and 62.9% respectively), they disagree with the uppers being more damaged
than the lowers since they found no difference between both groups (73.1% vs. 75.5%) [2].
Another study found a small relationship between the difficulty of access and the tooth structure
removed during preparation procedures [1]. A good explanation for more damage in the
maxillary arch was attributed to the more difficult visual access to the maxillary teeth as opposed
to the mandibular [3]. More need for the use of indirect vision during preparation of upper teeth
is also a possible reason. More damage to posterior teeth than anteriors can be attributed to more
difficult physical and visual accessibility to posterior teeth, especially with the tongue, cheeks,
and coronoid process coming in our way.
In our study, we aimed to be more reasonable in relating right and left sides to damage, so we
looked at them in relation to the operator’s dominant hand side since it wouldn’t be reasonable to

32
look at a tooth preparation on the right side performed by a right handed operator as being the
same to the one performed by a left handed operator. Our results showed no difference between
preparations on dominant and non-dominant sides, which supports the results by Medeiros and
Seddon who found no differences in the distribution of damage between right and left sides [3].
However, Moopnar and Faulkner found a tendency for a higher incidence of iatrogenic
preparation damage on the right side [2]. Our results can be explained by the fact that since a
crown preparation usually involves working on all tooth surfaces in a 360 degree orientation, the
operator always faces surfaces that are towards him and surfaces that are away from him
regardless of the side, which eventually means that there will be surfaces even if on the patients
dominant side that are not directly visible or accessible.
We found no significant relation between the type of preparation (restoration) and damage,
which comes in coherence with the results by Long and Smith who found that damage occurred
adjacent to prepared surfaces regardless of the marginal configuration whether it was a shoulder,
chamfer, or knife edge [1].
Our results showed a slightly higher prevalence, of no statistical significance, between obvious
damage in surfaces facing the distal side of preparations as compared to mesial surfaces.
Medeiros and Seddon also found no significant difference in the distribution of damage between
mesial and distal surfaces [3].
Since this study showed a very high prevalence of iatrogenic damage with the majority
belonging to the severe categories, it is of utmost importance to discuss possible preventive as
well as management measures.

33
Prevention was well-discussed in previous papers related to this topic. Some of the
recommendations were to use metal matrix bands to protect adjacent surfaces during preparation
2, 3, 25], the use of tapering diamond instruments that have a small diameter [1, 28], leaving a
small enamel fin on the prepared tooth surface near the proximal contact and breaking it later
with hand instruments [2, 3, 4], the use of elastic tooth separators [3], and most importantly
taking a higher level of care [2].
At the end this discussion, we will focus the light on how to manage/treat such damages after
they have already occurred. Suggested treatments discussed in literature varied from topical
fluoride application to extensive restorations, depending on the amount of lost tooth structure.
When the roughness is limited to superficial enamel, polishing the surface with Sof-Lex discs is
an option to reduce surface roughness and thus plaque accumulation and to allow for better
access for oral hygiene measures. Some articles showed that a better result can be obtained if this
process is followed by fluoride application. It has even been argued that the surface produced by
this method can be smoother than untouched enamel surfaces [4, 5, 10, 14, 15]. If the damage
occurred on an already restored surface, there are the options of either re-polishing the
restoration if the damage is small, or replacing it if the damage is severe [2].
The use of smooth surface resin sealants (similar to pit and fissure sealants), di-methacrylate
sealants with incorporated fluoride, and polyurethane tapes was recommended by many authors
to protect roughened enamel surfaces [4, 5, 25, 29-32].
Phosphopeptide amorphous calcium fluoride phosphate (CPP-ACFP) paste application to
abraded enamel surfaces is another innovative option to treat such surfaces, which has shown
promising results so far [33-37].

34
When the stripped/damaged tooth surface already has enamel caries/cavitation, the situation
becomes more challenging. A new conservative method for managing such cases is by the
application of special low viscosity resins, which are known as caries infiltrants [38, 39].
If the surface damage is severe and already reaching to dentine, the best management approach
would be by placement of a restoration. As for the choice of restorative material, many studies
have shown a better longevity for amalgams, while some other studies reported a comparably
good survival of composite restorations [40-44]. However, we think that amalgam is the least
likely to be used to restore surfaces that were iatrogenically damaged by crown preparations
because no matter how extensive the damage is, it is not likely to reach to a level where it fulfils
the criteria for amalgam.
Management of these cases is never easy because it should be a multi-disciplinary approach,
considering repairing the iatrogenic damage in consistence with the plan to crown the prepared
tooth (i.e. it should be done before the crown final impression and should take into consideration
anatomy, contact, and accessibility to oral hygiene methods after placement of the planned
crown on the adjacent tooth).

35
Limitations of the study:
For our study to be more specific and representative, the sample was supposed to include only
first-intervention crown preparations, which excludes second hand preparations and surfaces
adjacent to previous Class II restorations. This was not possible because of shortage of time due
to the delay in ethical clearance, without which we didn’t have authorization to access patients’
files and data.
Another limitation of this study is that the student was the only examiner, while it is always
better to have more than one examiner and to do calibration and assess inter-examiner reliability.
Conclusions:
Two hundred and seventy proximal tooth surfaces adjacent to fixed prosthodontic preparations
were examined and assessed. An alarming very high incidence of iatrogenic damage to these
surfaces was observed- 97.8%. No relations of statistical significance were found between
damage categories and different variables studied, but there was a trend for more severe damage
occurring in preparations done by more experienced operators and in posterior teeth.
It is recommended to take extra care to adjacent teeth during crown preparations and to use extra
protective measures like interproximal metal matrix bands. It is also highly recommended to dry
and review the surfaces adjacent to crown preparations after being done with the preparations to
assess them for any damage and decide on the suitable management from topical fluoride
application to placement of restoration if indicated.

36
Acknowledgements
I am most grateful to Dr. Prem Sharma for his great help and guidance in the statistical analysis
as well as giving me valuable advice and support all the way throughout the project. Thanks
from the heart to my great parents who always believed in me and gave me endless support. I
would also like to thank: the clinical and lab directors in our faculty for facilitating our data
collection, Prof. Eino Honkala for his guidance, and the chief technician Mrs Haneen and
technician Allan for handling our samples and records in the lab. Thanks also go to Mrs Zahra
Al-Nasser who did the coding and de-identification procedures.

37
References
1 Long TD, Smith BGN: The effect of contact area morphology on operative dental
procedures. Journal of Oral Rehabilitation 1988;15:593-598.
2 Moopnar M, Faulkner KDB: Accidental damage to teeth adjacent to crown-prepared
abutment teeth. Australian Dental Journal 1991;36:136-140.
3 Medeiros VAF, Seddon RP: Iatrogenic damage to approximal surfaces in contact with
Class II restorations. Journal of dentistry 2000;28:103-110.
4 Lussi A, Gygax M: Iatrogenic damage to adjacent teeth during classical approximal box
preparation. Journal of Dentistry 1998;26:435-441.
5 Qvist V, Johannessen L, Bruun M: Progression of approximal caries in relation to
iatrogenic preparation damage. J. Dent. Res 1992;71:1370-1373.
6 Opdam NJM, Roeters JJM, Berghem EV, Eljsvogels E, Bronkhorst E: Microleakage and
damage to adjacent teeth when finishing Class II adhesive preparations using either a
sonic device or bur. American Journal of dentistry 2002;15:317-320.
7 Mitchell CA, Pintado MR, Douglas WH: Iatrogenic tooth abrasion comparisons among
composite materials and finishing techniques. J Prosthet Dent 2002;88:320-328.
8 Jeffery IWM, Woolford MJ: An investigation of possible iatrogenic damage caused by
metal rubber dam clamps. International Endodontic Journal 1989;22:85-91.
9 Jarjoura K, Gagnon G, Niebergc L: Caries risk after interproximal enamel reduction. Am
J Orthod Dentofacial Orthop 2006;130:26-30.
38
10 Arman A, Cehreli SB, Ozel E, Arhun N, Cetinsahin A, Soyman M: Qualitative and
quantitative evaluation of enamel after various stripping methods. Am J Orthod
Dentofacial Orthop 2006;130:131.e7-131.e14.
11 Zachrisson BU, Nyøygaard L, Mobarak K: Dental health assessed more than 10 years
after interproximal enamel reduction of mandibular anterior teeth. Am J Orthod
Dentofacial Orthop 2007;131:162-169.
12 Zachirsson BU, Minster L, Ogaard B, Birkhed D: Dental health assessed after
interproximal enamel reduction: Caries risk in posterior teeth. Am J Orthod Dentofacial
Orthop 2011;139:90-98.
13 Twesme DA, Firestone AR, Heaven TJ, Feagin FF: Air-rotor stripping and enamel
demineralization in vitro. Am J Orthod Dentofac Orthop 1994;105:142-152.
14 Piacentini C, Sfondrini G: A scanning electron microscopy comparison of enamel
polishing methods after air-rotor stripping. Am J Orthod Dentofac Orthop 1996;109:57-
63.
15 Zhong M, Jost-Brinkmann P, Zellmann M, Zellmann S, Radlanski RJ: Clinical
Evaluation of a New Technique for Interdental Enamel Reduction. J Orofac
Orthop/Fortschr Kieferorthop 2000;61:432–439.
16 Radlanski RJ, Jager A, Schwestka R, Bertzbach F: Plaque accumulations caused by
interdental stripping. Am J Orthod Dentofac Orthop 1988;94:416-420.
17 Mei L, Busscher HJ, Mei HC, Ren Y: Influence of surface roughness on streptococcal
adhesion forces to composite resins. Dental materials 2011;27:770-778.

39
18 Bollen CML, Papaioannou W, Van Eldere J, Schepers E, Quirynen M, Van Steenberghe
D: The influence of abutment surface roughness on plaque accumulation and peri-implant
mucositis. Clin Oral Impl Res 1996;7:201-211.
19 Bollen CML, Lambrechts P, QuirynenM: Comparison of surface roughness of oral hard
materials to the threshold surface roughness for bacterial plaque retention: A review of
the literature. Dent Mater 1997;13:258-269.
20 Quirynen M, Marechal M, Busscher HJ, Weerkamp AH, Darius PL, Van Steenberghe D:
The influence of surface free energy and surface roughness on early plaque formation. An
in vivo study in man. J Cli Periodontol 1990; 17: 138-144.
21 Aykent F, Yondem I, Ozyesil AG, Gunal SK, Avunduk MC, Ozkan S: Effect of different
finishing techniques for restorative materials on surface roughness and bacterial
adhesion. J Prosthet Dent 2010;103:221-227.
22 Rosenberg RM, Ash MM: The Effect of Root Roughness on Plaque Accumulation and
Gingival Inflammation. J Periodontol 1974;45:146-150.
23 Vanderas AP, Kavvadia K, Papagiannoulis L: Development of Caries in Permanent First
Molars Adjacent to Primary Second Molars With Interproximal Caries: Four-year
Prospective Radiographic Study. Pediatr Dent 2004;26:362-368.
24 Xue J, Li W, Swain MV: In vitro demineralization of human enamel natural and abraded
surfaces: A micromechanical and SEM investigation. Journal of dentistry 2009;37:264-
272.
25 Lussi A, Kronenberg O, Megert B: The effect of magnification on the iatrogenic damage
to adjacent tooth surfaces during class II preparation. Journal of Dentistry 2003;31: 291-
296.

40
26 Kielbassa AM, Paris S, Lussi A, Meyer-Lueckel H: Evaluation of cavitations in proximal
caries lesions at various magnification levels in vitro. Journal of dentistry 2006;34:817-
822.
27 Forgie AH, Pine CM, Pitts NB: Restoration removal with and without the aid of
magnification. Journal of Oral Rehabilitation 2001;28:309-313.
28 Shillingburg HT, Sather DA, Wilson EL, Cain JR, Mitchell DL, Blanco LJ, Kessler JC:
Fundementals of fixed prosthodontics. 4th
edn. Chicago, Quintessence, 2012.
29 Schmidlin PR, Zehnder M, Zimmermann MA, Zimmermann J, Roos M, Roulet J: Sealing
smooth enamel surfaces with a newly devised adhesive patch: a radiochemical in vitro
analysis. Dental Materials 2005;21:545–550.
30 Gomez SS, Basili CP, Emilson CG: A 2-year clinical evaluation of sealed noncavitated
approximal posterior carious lesions in adolescents. Clin Oral Invest 2005;9:239–243.
31 Korbmacher-Steiner HM, Schilling AF, Huck LG, Kahl-Nieke B, Amling M: Laboratory
evaluation of toothbrush/toothpaste abrasion resistance after smooth enamel surface
sealing. Clin Oral Invest 2013;17:765–774.
32 Alkilzy M, Berndt C, Splieth CH: Sealing proximal surfaces with polyurethane tape:
three-year evaluation. Clin Oral Invest 2011;15:879–884.
33 Mayne RJ, Cochrane NJ, Cai F, Woods MG, Reynolds EC: In-vitro study of the effect of
casein phosphopeptide amorphous calcium fluoride phosphate on iatrogenic damage to
enamel during orthodontic adhesive removal. Am J Orthod Dentofacial Orthop
2011;139:543-551.

41
34 Ranjitkar S, Rodriguez JM, Kaidonis JA, Richards LC, Townsend GC, Bartlett DW: The
effect of casein phosphopeptide–amorphous calcium phosphate on erosive enamel and
dentine wear by toothbrush abrasion. Journal of dentistry 2009;37:250-154.
35 Srinivasan N, Kavitha M, Loganathan SC: Comparison of the remineralization potential
of CPP–ACP and CPP–ACP with 900 ppm fluoride on eroded human enamel: An in situ
study. Archieves of oral biology 2010;55:541-544.
36 Giulio AB, Matteo Z, Serena IP, Silvia M, Luigi C: In vitro evaluation of casein
phosphopeptide-amorphous calcium phosphate (CPP-ACP) effect on stripped enamel
surfaces. A SEM investigation. Journal of dentistry 2009;37:228-232.
37 Neto FCR, Maeda FA, Turssi CP, Serra MC: Potential agents to control enamel caries-
like lesions. Journal of dentistry 2009;37:786-790.
38 Meyer-Lueckel H, Chatzidakis A, Naumann M, Dorfer CE, Paris S:. Influence of
application time on penetration of an infiltrant into natural enamel caries. Journal of
dentistry 2011;39:465-469.
39 Schmidlin PR, Sener B, Attin T, Wiegand A: Protection of sound enamel and artificial
enamel lesions against demineralisation: Caries infiltrant versus adhesive. Journal of
dentistry 2012;40:851-856.
40 Sunnegardh-Gronberg K, Dijken JWV, Funegard U, Lindberg A, Nilsson M: Selection of
dental materials and longevity of replaced restorations in Public Dental Health clinics in
northern Sweden. Journal of dentistry 2009;37:673-678.
41 Pallesen U, Dijken JWV, Halken J, Hallonsten AL, Hoigaard R: Longevity of posterior
resin composite restorations in permanent teeth in Public Dental Health Service: A
prospective 8 years follow up. Journal of dentistry 2013;41:297-306.

42
42 Ferracane JL: Resin-based composite performance: Are there some things we can’t
predict? Dental materials 2013;29:51-58.
43 Nieuwenhuysen JPV, D’Hoore W, Carvalho J, Qvist V: Long-term evaluation of
extensive restorations in permanent teeth. Journal of Dentistry 2003;31:395–405.
44 Rodolpho PAR, Cenci MS, Donassollo TA, Loguercio AD, Demarco FF: A clinical
evaluation of posterior composite restorations: 17-year findings. Journal of dentistry
2006;34:427-435.
a Figure 1 was taken from: http://www.dentaljuce.com/fruit/page.asp?pid=103 and
modified.
b Figure 2 was taken from: http://dentallecnotes.blogspot.com/2011/09/tecture-note-on-
dental-anatomy.html and modified.
43
Appendix A
Technician File
number
Operator’s
name
Patient’s
name
Date Work
description

44
Appendix B
Code
Tooth:
Mesial surface Distal surface
Degree of damage
Location of damage
Pattern of damage
Tooth:
Mesial surface Distal surface
Degree of damage
Location of damage
Pattern of damage



![Marginal quality of ceramic inlays after three different ... · especially in the enamel [1]; and iatrogenic damage to adjacent teeth [11–13], may occur. This mechanical damage](https://static.fdocuments.net/doc/165x107/5f238c86189dba68bb57aa52/marginal-quality-of-ceramic-inlays-after-three-different-especially-in-the-enamel.jpg)