Assessment of Coronary Artery Disease Severity...
12
825 Assessment of Coronary Artery Disease Severity by Positron Emission Tomography Comparison With Quantitative Arteriography in 193 Patients Linda L. Demer, MD, PhD, K. Lance Gould, MD, Richard A. Goldstein, MD, Richard L. Kirkeeide, PhD, Nizar A. Mullani, Richard W. Smalling, MD, PhD, Akira Nishikawa, MD, and Michael E. Merhige, MD With the technical assistance of Mary Haynie, RN, and Richard L. Holmes, RT To assess the accuracy of positron emission tomography (PET) for evaluation of coronary artery disease (CAD), cardiac PET perfusion images were obtained at rest and with dipyridamole- handgrip stress in 193 patients undergoing coronary arteriography. PET images were reviewed by two independent readers blinded to clinical data. Subjective defect severity scores were assigned to each myocardial region on a 0 (normal) to 5 (severe) scale. Results were compared with arteriographic stenosis severity expressed as stenosis flow reserve (SFR), with continuous values ranging from 0 (total occlusion) to 5 (normal), calculated from quantitative arterio- graphic dimensions using automated detection of the vessel borders. There were 115 patients with significant CAD (SFR<3), 37 patients with mild CAD (3.SFR<4), and 41 patients with essentially normal coronaries (SFR.4). With increasingly severe impairment of stenosis flow reserve, subjective PET defect severity increased. Despite wide scatter, a PET score of 2 or more was highly predictive of significant flow reserve impairment (SFR <3). For each patient, the score of the most severe PET defect correlated with the SFR of that patient's most severe stenosis (r,=0.77±0.06). For each of 243 stenoses, PET defect score correlated with the SFR of the corresponding artery (r,=0.63±0.08). PET defect location closely matched the region supplied by the diseased artery, and readers agreed whether the most severe PET defect was less than or more than 2 for 89% of patients. (Circulation 1989;79:825-835) M y yocardial perfusion imaging is widely used for noninvasive assessment of stenosis V severity. Knowledge of the diagnostic accuracy of these tests is important for proper clinical application and interpretation. Most previ- ous reports of the diagnostic accuracy of myocar- dial perfusion imaging1-4 have used sensitivity- From the Division of Cardiology, Department of Medicine, and Positron Diagnostic and Research Center, University of Texas Medical School, Houston, Texas. Presented in part as an abstract at the American College of Cardiology Scientific Session, March 28, 1988. Supported in part by Grants RO1-HL-26862 and R01-HL-26885 from the National Institutes of Health; DE-FG05-84ER60210 from the Department of Energy; and as a joint collaborative research project with the Clayton Foundation for Research, Houston, Texas. Address for correspondence: Linda L. Demer, MD, PhD, Division of Cardiology, UCLA School of Medicine, 47-123 CHS, 10833 LeConte Avenue, Los Angeles, CA 90024-1679. Address for reprints: K. Lance Gould, MD, Division of Cardiology, University of Texas Medical School, P.O. Box 20708, Houston, TX 77225. Received June 7, 1988; revision accepted December 6, 1988. specificity analysis to describe the relation between image defects and arteriographic disease. This method requires binary (positive or negative) clas- sification of both imaging and arteriographic results. Arteriographic results have usually been described in terms of percent diameter narrowing, with a threshold value of 50% as the criterion for presence of coronary disease. There are three limitations to this use of sensitivity- specificity analysis for assessing accuracy of nonin- vasive tests for coronary disease. First, coronary disease is not an all-or-none condition; binary clas- sification requires arbitrary threshold criteria and creates artificial distinctions in coronary artery dis- ease that, in actuality, has a continuous spectrum of severity. Threshold values that yield optimal sensitivity and specificity values for one test may yield falsely lower values for a different but more accurate test if its detection threshold is different. For example, an imaging test capable of detecting 40% stenoses may have low specificity according to a 50% stenosis by guest on July 15, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Assessment of Coronary Artery Disease Severity...
825
Assessment of Coronary Artery DiseaseSeverity by Positron Emission Tomography
Comparison With Quantitative Arteriography in 193 Patients
Linda L. Demer, MD, PhD, K. Lance Gould, MD, Richard A. Goldstein, MD,
Richard L. Kirkeeide, PhD, Nizar A. Mullani, Richard W. Smalling, MD, PhD,
Akira Nishikawa, MD, and Michael E. Merhige, MD
With the technical assistance ofMary Haynie, RN, and Richard L. Holmes, RT
To assess the accuracy of positron emission tomography (PET) for evaluation of coronary arterydisease (CAD), cardiac PET perfusion images were obtained at rest and with dipyridamole-handgrip stress in 193 patients undergoing coronary arteriography. PET images were reviewedby two independent readers blinded to clinical data. Subjective defect severity scores were
assigned to each myocardial region on a 0 (normal) to 5 (severe) scale. Results were comparedwith arteriographic stenosis severity expressed as stenosis flow reserve (SFR), with continuousvalues ranging from 0 (total occlusion) to 5 (normal), calculated from quantitative arterio-graphic dimensions using automated detection of the vessel borders. There were 115 patientswith significant CAD (SFR<3), 37 patients with mild CAD (3.SFR<4), and 41 patients withessentially normal coronaries (SFR.4). With increasingly severe impairment of stenosis flowreserve, subjective PET defect severity increased. Despite wide scatter, a PET score of 2 or morewas highly predictive of significant flow reserve impairment (SFR <3). For each patient, thescore of the most severe PET defect correlated with the SFR of that patient's most severestenosis (r,=0.77±0.06). For each of 243 stenoses, PET defect score correlated with the SFR ofthe corresponding artery (r,=0.63±0.08). PET defect location closely matched the regionsupplied by the diseased artery, and readers agreed whether the most severe PET defect was lessthan or more than 2 for 89% of patients. (Circulation 1989;79:825-835)
My yocardial perfusion imaging is widely usedfor noninvasive assessment of stenosis
V severity. Knowledge of the diagnosticaccuracy of these tests is important for properclinical application and interpretation. Most previ-ous reports of the diagnostic accuracy of myocar-dial perfusion imaging1-4 have used sensitivity-
From the Division of Cardiology, Department of Medicine,and Positron Diagnostic and Research Center, University ofTexas Medical School, Houston, Texas.
Presented in part as an abstract at the American College ofCardiology Scientific Session, March 28, 1988.
Supported in part by Grants RO1-HL-26862 and R01-HL-26885from the National Institutes of Health; DE-FG05-84ER60210from the Department of Energy; and as a joint collaborativeresearch project with the Clayton Foundation for Research,Houston, Texas.Address for correspondence: Linda L. Demer, MD, PhD,
Division of Cardiology, UCLA School of Medicine, 47-123 CHS,10833 LeConte Avenue, Los Angeles, CA 90024-1679.Address for reprints: K. Lance Gould, MD, Division of
Cardiology, University of Texas Medical School, P.O. Box20708, Houston, TX 77225.Received June 7, 1988; revision accepted December 6, 1988.
specificity analysis to describe the relation betweenimage defects and arteriographic disease. Thismethod requires binary (positive or negative) clas-sification of both imaging and arteriographic results.Arteriographic results have usually been describedin terms of percent diameter narrowing, with athreshold value of 50% as the criterion for presenceof coronary disease.There are three limitations to this use of sensitivity-
specificity analysis for assessing accuracy of nonin-vasive tests for coronary disease. First, coronarydisease is not an all-or-none condition; binary clas-sification requires arbitrary threshold criteria andcreates artificial distinctions in coronary artery dis-ease that, in actuality, has a continuous spectrum ofseverity.Threshold values that yield optimal sensitivity
and specificity values for one test may yield falselylower values for a different but more accurate test ifits detection threshold is different. For example, animaging test capable of detecting 40% stenoses mayhave low specificity according to a 50% stenosis
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

826 Circulation Vol 79, No 4, Aptil 1989
criterion but high specificity according a 40% ste-nosis criterion.
Second, sensitivity and specificity values are alsodetermined by the disease distribution of the studypopulation.5 A sample population with a high fre-quency of mild disease will be distributed centrallynear the threshold values where scatter is morelikely to lower sensitivity and specificity. The sen-sitivity and specificity found in one population maynot apply to a different population. To overcomethese limitations, analysis of test results as contin-uous variables has been proposed.6
Finally, recent reports by Marcus and others7,8have indicated that percent diameter narrowing isnot an adequate standard for quantifying stenosisseverity in clinical studies. It does not account forthe effects of diffuse disease, inherent eccentricity,stenosis length, viscosity, cross-sectional area,entrance and exit angles, and absolute dimensionson flow impedance; and it is limited by substantialinterobserver and intraobserver variability.9-11 Pro-posed alternative approaches include quantitativearteriographic methods based on the Brown-Dodgemethod12 to calculate stenosis flow reserve13 anddirect measurement of coronary flow velocity byDoppler catheter.14
In an earlier study, Wijns and colleagues15 usedquantitative arteriographic and direct physiologicmeasurements to assess the accuracy of planar 201T1imaging, but they retained the conventional thresh-old criteria to classify arteriographic severity andperfusion defect severity as positive or negative.The feasibility of clinical PET perfusion imaging hasalso been addressed in previous work by Schelbertand colleagues16 and, with quantitative arterio-graphic flow reserve, by our group.17 These studiesalso retained the binary classification system andinvolved small numbers of patients.The purpose of the present study was to reeval-
uate the accuracy of positron perfusion imaging inassessment of coronary disease severity with scalescovering the range of disease severity rather thanbinary classification, direct correlation rather thansensitivity-specificity analysis, and quantitative arte-riographic flow reserve rather than percent diame-ter narrowing, in a large series of patients.
MethodsStudy Patients
Subjects consisted of 193 patients (143 men, 50women) undergoing diagnostic cardiac catheteriza-tion. The patient sample included 50 patients previ-ously reported in a study where binary classificationand sensitivity-specificity analysis were used.17 Clin-ical indications for arteriography included chestpain syndromes, myocardial infarction, abnormalstress tests, coronary angioplasty, thrombolytic ther-apy for acute infarction, evaluation before renaltransplant, before and after cholesterol loweringprograms, or as part of screening feasibility studies.
Sixty-six patients were clinically diagnosed as hav-ing a previous myocardial infarction. From an initialgroup of 209 patients, 12 early patients were excludedbecause part of the heart was not imaged due topositioning error, and four PET images were notinterpretable due to camera or computer malfunc-tion. Patients were not enrolled if there was evidenceof unstable angina or active bronchospasm withtheophylline bronchodilator therapy, which are con-traindications to intravenous dipyridamole. Afterinformed consent was obtained, coronary arteriogra-phy and PET imaging were performed according toprotocols approved by the University of Texas Com-mittee for Protection of Human Subjects.
Quantitative ArteriographyCineangiographic frames of orthogonal views were
digitized for each stenosis involving a major artery,including diagonal, obtuse marginal, ramus interme-dius, and acute marginal branches. Absolute andrelative stenosis dimensions were measured with acomputer program providing automatic detection ofvessel borders (Figure 1), with an accuracy of ± 0.1mm. The theory and equations for predicting steno-sis flow reserve from these dimensions have beendescribed previously.13"18 In brief, the coronary per-fusion pressure distal to each stenosis was calculatedas a function of flow'9'20 according to the equation:
Pcor = PAO-(fQ + sQ2)where Pcor is distal coronary pressure, PAO is aorticpressure, Q is flow, f is 8piTL/As2, s is p((1/A)- (1/A0))2, A, is minimum absolute area, An is absolutearea of normal adjacent artery, ,L is blood viscosity,p is blood density, and L is stenosis length.
This relation, shown as the curved line in Figure 1,lower panel, was compared with the known pressure-flow relation for conditions of maximal coronaryvasodilation, shown as the diagonal line. Stenosisflow reserve (SFR) was defined as the intersection ofthese two relations (i.e., flow at maximum coronaryvasodilation) relative to rest flow, under standardizedhemodynamic conditions. In comparison with directmeasurements by electromagnetic flow meter, the95% confidence interval was ±0.66 with a reproduc-ibility of 2-3%.13 The advantages of SFR over othermethods of describing stenosis severity have beendiscussed in detail in a recent editorial.21Coronary arteries were considered normal ifpatent
bypass grafts supplied the arterial bed (two patients).Five patients having their PET study after acutemyocardial infarction, with normal coronary arteri-ography after revascularization of chronic occlu-sions, were considered to have total occlusions forthe purposes of patient-by-patient analysis. Infarct-related stenoses of 19 patients who had undergoneacute revascularization were excluded from this analy-sis because the residual stenosis severity would notbe comparable to the variable degree of resultantperfusion defect; the remaining stenoses in thesepatients were included in the regional analysis.
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

Demer et al Cardiac PET and Quantitative Arteriography 827
FIGURE 1. Top panel: Automated edge-detection analysis of a coronary arterio-gram. Bottom panel: Quantitative arterio-graphic dataforanotherpatient includingplots of diameter and cross-sectionallumen area as functions of axial position(lower left); parameters calculated fromdimensions including minimal, proximal,distal, andpercent diameter in each view
p (D1,,D2J, minimal, proximal, distal, andpercent cross-sectional area, volume,
tT ilength, and relative length ofthe stenosedsegment, entrance and e-xit angles (av and£l), predicted rest flow (Q,), and viscousand expansion loss coefficients (Cv, Ce,Kv, Ke) (upper left); and the derivedpressure-flow relation and stenosis flowreserve (upper right). The diugunad linecrossing the pressure-flow curve repre-sents the condition of maximal arteriolar
&Xmm2) $ 5*$&vasodilation. As flow increases, pressuredistal to the stenosis decreases, until it
L,, n reaches a minimum at the point of maxi-mal vasodilation. Stenosis flow reserve isdefined as that maximum value of flowrelative to restingflow (Q/Q,) under standardized hemodynamic conditions, wherenormal stenosis flow reserve is S.
Quantitative Orteriography 1-SEP-83RCO UTHSCH/Cardiology 0PT00217723-PPR-88UCIN #310
Prox Min Dist '%Redh Norm
D1lmm) 2.63 0.27 3.02 711 3.02D2(mm) 2.79 1.29 3.33 611 3.33 PoorPrdmm2) 5.30 0.39 7.91 389 7.91 (rnmHg)L(mm) 17.0 L/Dn %.4 U(mm3) 69.3Hipha -l 3. 8 Omneg 13.7Pn(mm2) 7.9 Ky 2053 Ke 1.40GT 20Qr(cc/a) 1.6 Cv 2.13 Ce 5.36
S
5r_
4XJhPLHOSQ[TON(5I[PU6
0/Orest 5
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

828 Circulation Vol 79, No 4, April 1989
FIGURE 2. Positron emission tomographic 82Rb images acquiredfrom apatient withproximal disease ofthe left anteriordescending artery before (top row of upper and lower images) and after (bottom row) intravenous dipyridamole withhandgrtip stress. The views are oriented in the oblique semi-long axis and arranged in vertical orderfrom base (upper left)to inferior wall (lower right). Each slice is viewed from above so that the apex is at the top, the lateralfree wall on theleft, the valve ring at the bottom, and the interventricular septum at the upper right of the horseshoe-shaped leftventricular slices. In the color coding, white is the highest, red next highest, yellow intermediate, and green and bluelowest uptake. There is a large anterior, septal, and apical defect. The right ventricular wall is not normally visualizedon PET imaging due to its thin walls.
Positron Emission TomographyPatients were fasted for 4 hours, and caffeine and
theophylline were withheld for 8 hours before imag-ing to prevent interference with the hyperemiceffect of dipyridamole. Fluoroscopy was used tomark the cardiac borders for proper patient posi-tioning. Scans were performed with the Universityof Texas multislice tomograph17,22 with a recon-structed resolution of 14 mm full-width half-maximum. Transmission images were performed tocorrect for photon attenuation. Emission imageswere obtained with 82Rb produced by a portablegenerator23 or, when 82Rb was not available, 13Nammonia.17,2425 Eighty-two patients received 82Rband 111 received 13N ammonia. The tracer wasinjected through a 20-gauge catheter inserted intoan antecubital vein. To allow for blood pool clear-ance, there was a 1-minute delay after 82Rb and a
3-minute delay after ammonia administration. Afterthis delay, data were acquired for 5-8 minutes for82Rb and 15-20 minutes for 13N ammonia. Afterisotope decay, 10 minutes after administration ofthe first dose of 82Rb or 40 minutes after 13Nammonia, dipyridamole (0.142 mg/kg/min) wasinfused for 4 minutes. Two minutes after the infu-sion was completed, 25% of the predeterminedmaximal handgrip was begun as described byBrown.26At 8 minutes from onset of the infusion, a
second dose of the same amount of the same tracerwas injected, and imaging was repeated. Datawere acquired over the same period. Radiationdoses involved in these procedures have beendescribed previously.27-29For those patients devel-oping significant angina, aminophylline (125 mg)was given intravenously.
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
Demer et al Cardiac PET and Quantitative Arteriography 829
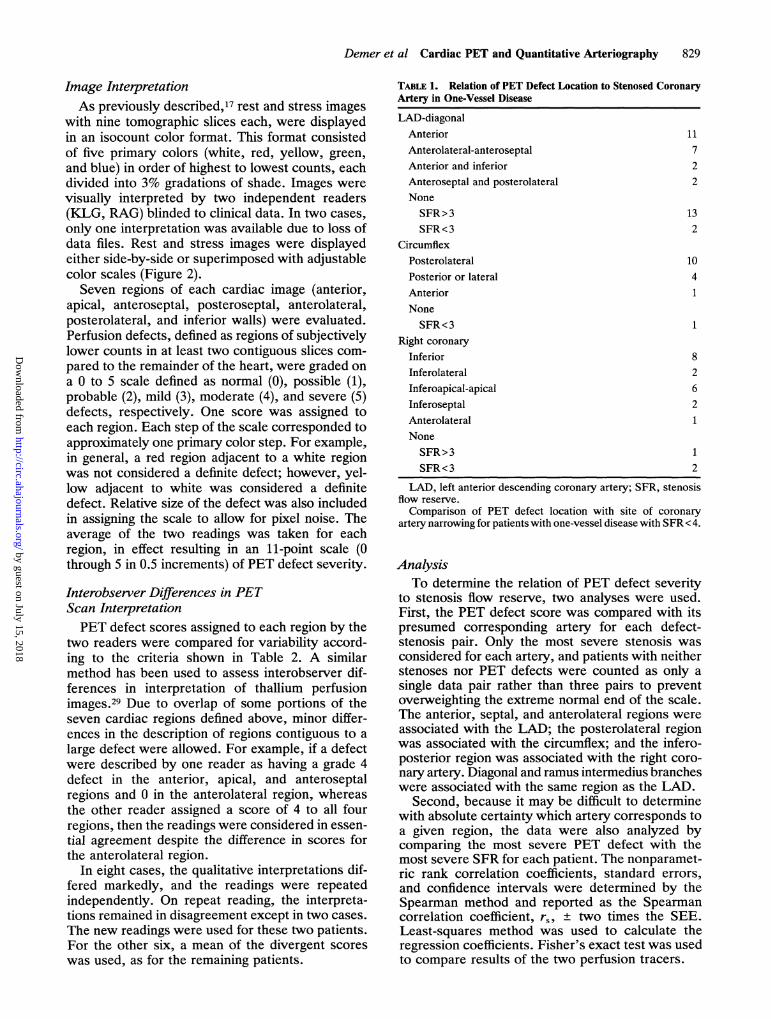
Image InterpretationAs previously described,17 rest and stress images
with nine tomographic slices each, were displayedin an isocount color format. This format consistedof five primary colors (white, red, yellow, green,
and blue) in order of highest to lowest counts, eachdivided into 3% gradations of shade. Images were
visually interpreted by two independent readers(KLG, RAG) blinded to clinical data. In two cases,
only one interpretation was available due to loss ofdata files. Rest and stress images were displayedeither side-by-side or superimposed with adjustablecolor scales (Figure 2).Seven regions of each cardiac image (anterior,
apical, anteroseptal, posteroseptal, anterolateral,posterolateral, and inferior walls) were evaluated.Perfusion defects, defined as regions of subjectivelylower counts in at least two contiguous slices com-
pared to the remainder of the heart, were graded on
a 0 to 5 scale defined as normal (0), possible (1),probable (2), mild (3), moderate (4), and severe (5)defects, respectively. One score was assigned toeach region. Each step of the scale corresponded toapproximately one primary color step. For example,in general, a red region adjacent to a white regionwas not considered a definite defect; however, yel-low adjacent to white was considered a definitedefect. Relative size of the defect was also includedin assigning the scale to allow for pixel noise. Theaverage of the two readings was taken for eachregion, in effect resulting in an 11-point scale (0through 5 in 0.5 increments) of PET defect severity.
Interobserver Differences in PETScan InterpretationPET defect scores assigned to each region by the
two readers were compared for variability accord-ing to the criteria shown in Table 2. A similarmethod has been used to assess interobserver dif-ferences in interpretation of thallium perfusionimages.29 Due to overlap of some portions of theseven cardiac regions defined above, minor differ-ences in the description of regions contiguous to a
large defect were allowed. For example, if a defectwere described by one reader as having a grade 4defect in the anterior, apical, and anteroseptalregions and 0 in the anterolateral region, whereasthe other reader assigned a score of 4 to all fourregions, then the readings were considered in essen-tial agreement despite the difference in scores forthe anterolateral region.
In eight cases, the qualitative interpretations dif-fered markedly, and the readings were repeatedindependently. On repeat reading, the interpreta-tions remained in disagreement except in two cases.
The new readings were used for these two patients.For the other six, a mean of the divergent scores
was used, as for the remaining patients.
TABLE 1. Relation of PET Defect Location to Stenosed CoronaryArtery in One-Vessel Disease
LAD-diagonalAnteriorAnterolateral-anteroseptalAnterior and inferiorAnteroseptal and posterolateralNoneSFR>3SFR<3
CircumflexPosterolateralPosterior or lateralAnteriorNoneSFR<3
Right coronary
InferiorInferolateralInferoapical-apicalInferoseptalAnterolateralNoneSFR>3SFR<3
117
22
132
1041
1
82621
12
LAD, left anterior descending coronary artery; SFR, stenosisflow reserve.Comparison of PET defect location with site of coronary
artery narrowing for patients with one-vessel disease with SFR < 4.
AnalysisTo determine the relation of PET defect severity
to stenosis flow reserve, two analyses were used.First, the PET defect score was compared with itspresumed corresponding artery for each defect-stenosis pair. Only the most severe stenosis wasconsidered for each artery, and patients with neitherstenoses nor PET defects were counted as only asingle data pair rather than three pairs to preventoverweighting the extreme normal end of the scale.The anterior, septal, and anterolateral regions wereassociated with the LAD; the posterolateral regionwas associated with the circumflex; and the infero-posterior region was associated with the right coro-nary artery. Diagonal and ramus intermedius brancheswere associated with the same region as the LAD.
Second, because it may be difficult to determinewith absolute certainty which artery corresponds toa given region, the data were also analyzed bycomparing the most severe PET defect with themost severe SFR for each patient. The nonparamet-ric rank correlation coefficients, standard errors,and confidence intervals were determined by theSpearman method and reported as the Spearmancorrelation coefficient. rs_ + two times the SEE.Least-squares method was used to calculate theregression coefficients. Fisher's exact test was usedto compare results of the two perfusion tracers.
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

830 Circulation Vol 79, No 4, April 1989
-Normol
0 2 3 4
SUBJECTIVE PET DEFECT SEVERITY
5
638 1
_ 1___
0 2 3 4SUBJECTIVE PET DEFECT SEVERITY
5
N
48
09 1315
24
25
32
_35
N
40
12
14
9
1 1
22
15
16
25
FIGURE 3. Top panel: Plot of the relation betweenarteriographic stenosis flow reserve and subjective PETdefect severity in the corresponding anatomic region for243 stenoses. Mean value ofSFR is plotted as a functionofPET defect severity. The horizontal dashed lines iden-tify the ranges of normal, mildly reduced, and signifi-cantly reduced stenosis flow reserve. The vertical dashedline indicates that PET defect scores of2 or more predictthe presence of mild or significant stenoses. The error
bars represent 90% confidence intervals. The number ofpatients represented is shown adjacent to each point.Right-hand column lists the numbers ofpatients found ineach interval of SFR, to illustrate the distribution ofcoronary disease in this population. SFR is plotted on a
reverse scale (5 to 0) to parallel stenosis severity. Noerror bars are shown for the point representing a singlestenosis. Bottom panel: Plot of the relation betweenarteriographic stenosis flow reserve and subjective PETdefect severity in 174 patients. The most severe stenosiswas compared with the most severe PET defect for eachpatient. Nineteen patients with revascularization duringacute infarction were excluded because the residualstenosis severity would not be comparable to the severityof the fixed perfusion defect. As for the top panel, thehorizontal dashed lines identify the ranges of normal,mildly reduced, and significantly reduced stenosis flowreserve. The vertical dashed line indicates that PETdefect scores of2 or more predict thepresence ofmild orsignificant stenoses.
ResultsCoronary ArterographyCoronary artery stenoses with flow reserve val-
ues less than 4 were found in 137 patients. Thirty-seven of these patients had stenosis flow reservevalues between 3 and 4, consistent with milddisease. Fifteen had myocardial infarction withrevascularization. Occlusive disease was presentin 34, involving 42 vessels.
PET Defect Severity Versus Stenosis Severity forEach Artery
For the 243 stenosis-defect pairs among the 193patients, PET defect score was compared with arte-riographic severity of the corresponding coronarystenosis (Figure 3, top). With increasing impairmentof flow reserve, subjective PET defective severityincreases. Although there is wide scatter, a PETdefect score of 2 or more, indicated by the verticalline in Figure 3, top, is highly predictive of significantflow reserve impairment (SFR<3). PET score rankcorrelated significantly with SFR (r =0.63±0.08).Linear regression yielded the equation:
predicted SFR = 3.91 -0.55 (PET defect rank)
with standard errors for the coefficients of 1.4 and0.04, respectively. This regression equation is pro-vided for description rather than for calculations;because of the scatter in the relation, direct calcula-tion of any individual value of SFR from PET defectscore would not be accurate. Mean values are shownfor clarity because of overlap of the large number ofdata points; regression was performed with the rawdata. Although the correlation coefficient is negative,the slope is positive in Figure 3, top, because thevertical scale was reversed in the figure for conve-nience so that SFR would parallel stenosis severity.
PET Defects Compared With ArteriographicSeverity for Each PatientTo determine whether PET defects identify
patients with coronary disease, irrespective of loca-tion, the SFR of the most severe stenosis wascompared to the score of the most severe PETdefect for each patient over the entire range ofdisease severity (Figure 3, bottom).As in the preceding figure, increasing impairment
of flow reserve corresponds to increasing PETdefect severity. Although there is wide scatter, aPET defect score of 2 or more (indicated by thevertical line in Figure 3, bottom) is predictive ofsignificant flow impairment (SFR<3). The SEMsare larger for the middle range of stenosis severity(from 2 to 4) than for the extremes. This is attrib-utable in part to the smaller numbers ofPET defectsin this range. In addition, several of these defectscorrespond to lesions in diagonal arteries or in distalportions of the larger arteries, affecting small regionsof myocardium. The severity of such small defects
0r
W> 1W-U)
0.-J(0 3n,0
W
zU),
5
O0
W Itr_WUnWcc 2
- 3in-0zW
U)n d
l-L
T
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
Demer et al Cardiac PET and Quantitative Arteriography 831
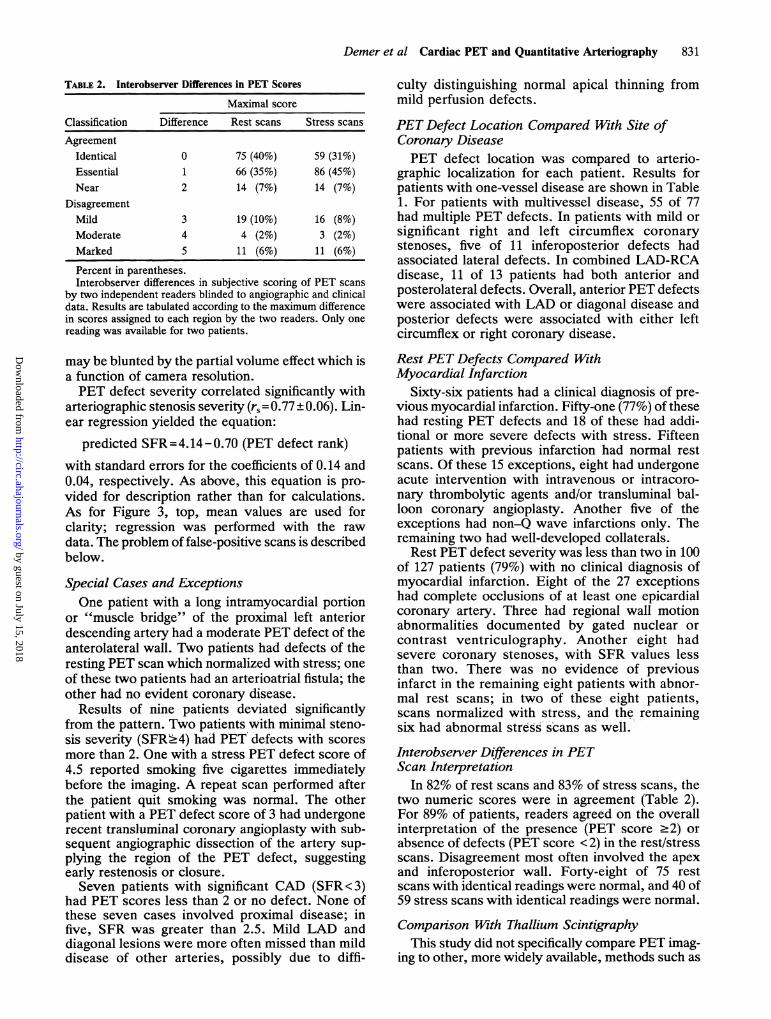
TABLE 2. Interobserver Differences in PET Scores
Maximal score
Classification Difference Rest scans Stress scans
AgreementIdentical 0 75 (40%) 59 (31%)Essential 1 66 (35%) 86 (45%)Near 2 14 (7%) 14 (7%)
DisagreementMild 3 19 (10%) 16 (8%)Moderate 4 4 (2%) 3 (2%)Marked 5 11 (6%) 11 (6%)
Percent in parentheses.Interobserver differences in subjective scoring of PET scans
by two independent readers blinded to angiographic and clinicaldata. Results are tabulated according to the maximum differencein scores assigned to each region by the two readers. Only onereading was available for two patients.
may be blunted by the partial volume effect which isa function of camera resolution.PET defect severity correlated significantly with
arteriographic stenosis severity (rs = 0.77 + 0.06). Lin-ear regression yielded the equation:
predicted SFR = 4.14- 0.70 (PET defect rank)with standard errors for the coefficients of 0.14 and0.04, respectively. As above, this equation is pro-vided for description rather than for calculations.As for Figure 3, top, mean values are used forclarity; regression was performed with the rawdata. The problem of false-positive scans is describedbelow.
Special Cases and ExceptionsOne patient with a long intramyocardial portion
or "muscle bridge" of the proximal left anteriordescending artery had a moderate PET defect of theanterolateral wall. Two patients had defects of theresting PET scan which normalized with stress; oneof these two patients had an arterioatrial fistula; theother had no evident coronary disease.
Results of nine patients deviated significantlyfrom the pattern. Two patients with minimal steno-sis severity (SFR.4) had PET defects with scores
more than 2. One with a stress PET defect score of4.5 reported smoking five cigarettes immediatelybefore the imaging. A repeat scan performed afterthe patient quit smoking was normal. The otherpatient with a PET defect score of 3 had undergonerecent transluminal coronary angioplasty with sub-sequent angiographic dissection of the artery sup-plying the region of the PET defect, suggestingearly restenosis or closure.Seven patients with significant CAD (SFR <3)
had PET scores less than 2 or no defect. None ofthese seven cases involved proximal disease; infive, SFR was greater than 2.5. Mild LAD anddiagonal lesions were more often missed than milddisease of other arteries, possibly due to diffi-
culty distinguishing normal apical thinning frommild perfusion defects.
PET Defect Location Compared With Site ofCoronary DiseasePET defect location was compared to arterio-
graphic localization for each patient. Results forpatients with one-vessel disease are shown in Table1. For patients with multivessel disease, 55 of 77had multiple PET defects. In patients with mild orsignificant right and left circumflex coronarystenoses, five of 11 inferoposterior defects hadassociated lateral defects. In combined LAD-RCAdisease, 11 of 13 patients had both anterior andposterolateral defects. Overall, anterior PET defectswere associated with LAD or diagonal disease andposterior defects were associated with either leftcircumflex or right coronary disease.
Rest PET Defects Compared WithMyocardial Infarction
Sixty-six patients had a clinical diagnosis of pre-vious myocardial infarction. Fifty-one (77%) of thesehad resting PET defects and 18 of these had addi-tional or more severe defects with stress. Fifteenpatients with previous infarction had normal restscans. Of these 15 exceptions, eight had undergoneacute intervention with intravenous or intracoro-nary thrombolytic agents and/or transluminal bal-loon coronary angioplasty. Another five of theexceptions had non-Q wave infarctions only. Theremaining two had well-developed collaterals.
Rest PET defect severity was less than two in 100of 127 patients (79%) with no clinical diagnosis ofmyocardial infarction. Eight of the 27 exceptionshad complete occlusions of at least one epicardialcoronary artery. Three had regional wall motionabnormalities documented by gated nuclear orcontrast ventriculography. Another eight hadsevere coronary stenoses, with SFR values lessthan two. There was no evidence of previousinfarct in the remaining eight patients with abnor-mal rest scans; in two of these eight patients,scans normalized with stress, and the remainingsix had abnormal stress scans as well.
Interobserver Differences in PETScan Interpretation
In 82% of rest scans and 83% of stress scans, thetwo numeric scores were in agreement (Table 2).For 89% of patients, readers agreed on the overallinterpretation of the presence (PET score >2) orabsence of defects (PET score < 2) in the rest/stressscans. Disagreement most often involved the apexand inferoposterior wall. Forty-eight of 75 restscans with identical readings were normal, and 40 of59 stress scans with identical readings were normal.
Comparison With Thallium ScintigraphyThis study did not specifically compare PET imag-
ing to other, more widely available, methods such as
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

832 Circulation Vol 79, No 4, April 1989
`01TI scintigraphy. Available data are not directlycomparable because of the limitations of sensitivity/specificity analysis described in the introduction.One recent study, by Zijlstra and colleagues,30
reported the sensitivity and specificity of exercisethallium compared with radiographic coronary flowreserve in 38 patients with one-vessel disease. It isnot directly comparable because of major differencesin methods, including binary classification, numberand selection of patients, coronary flow reservecompared with stenosis flow reserve, and exercisecompared with dipyridamole stress. However, this isthe only previous study, to our knowledge, in whichimaging data are compared with a continuous scaleof flow reserve (FR), permitting indirect comparisonto the present results. 1) For moderate to severestenoses (FR <3), 72% (18 of 25) of thallium scanscompared with 94% (108 of 115) of PET scans werenegative. 2) For intermediate stenoses (FR=3-4),0% (0 of 9) of thallium scans compared with 49% (18of 37) of PET scans were positive. 3) For minimalstenoses (FR.4), 100% (4 of 4) of thallium scanscompared with 95% (39 of 41) of PET scans werenegative. Three categories were compared becausethe small number of patients in the thallium study didnot permit finer divisions, and correlation coeffi-cients were not available for the thallium data. Theintermediate range of 3-4 is used for simplicity, butit closely approximates the 95% confidence interval ofstenosis flow reserve at the cut-off value of 3.4-3.5established by other investigators.30,31 This compari-son is limited because of the small number of thalliumpatients, especially in the range of normal and lesssevere disease; the specificity of thallium may beoverestimated because of the small proportion ofwomen, reducing the effect of attenuation artifacts.
Comparison of 82Rb with "NAmmoniaImages obtained with 82Rb and 13N ammonia
tracers were qualitatively similar. The two falsepositive cases included one 13N ammonia and one82Rb image. Of the seven false negative scans, fivewere ammonia scans and two rubidium. Thus, 79 of82 rubidium images and 105 of 111 ammonia imageswere consistent with the arteriographic results. Theseratios were not significantly different (p = 0.73).
DiscussionThe accuracy of positron perfusion imaging of the
heart has been reported in previous studies of thefeasibility of clinical dipyridamole-PET imaging.Schelbert and colleagues16 compared PET scanresults to percent diameter narrowing and foundsensitivity and specificity values of 97% and 100%.According to standard statistical tables,32 the lowerlimits of the 95% confidence intervals for thesevalues are 84% and 75%, respectively. In a study of50 patients by Gould et al,17 PET scan results werecompared with quantitative arteriographic stenosisflow reserve, and sensitivity and specificity werefound to be 95% and 100%. The corresponding
S-
W
0CO 4-
W
00
0
z
0C
STENOSIS CFR VS. % DIAMETER
*.X* :,*
.*N
. 1
\ v
*% *.Q
*. 0*0-..
0 10 20 30 0 50 60 70 80 90 100% DIAMETER NARROWING
FIGURE 4. Plot of the relation between stenosis flowreserve andpercent diameter narrowing, both calculatedfrom quantitative arteriographic measurements, in thefirst 100 patients. Becausepercent diameter narrowing isonly one ofseveralfactors used to calculate stenosis flowreserve, the scatter in this relation indicates the impor-tance of those factors other than relative diameter thatinfluence flow impedance of a stenosis.
lower limits of the 95% confidence intervals are 77%and 66%. The lower limits of the 99% confidenceintervals are 71% and 56%. The overlap of thesewide confidence intervals with the sensitivity andspecificity values reported for planar thallium imag-ing, and even electrocardiographic exercise testing,indicate the need for larger numbers of patients forstatistical accuracy.The present study differs from earlier reports
of perfusion imaging accuracy in the combined useof quantitative arteriographic stenosis flow re-serve rather than percent diameter narrowing asthe gold standard, the large number of patients,and the use of correlation rather than binarysensitivity-specificity analysis.
Stenosis Flow Reserve Compared With CoronaryFlow Reserve
It is important to distinguish stenosis flowreserve,33 which is calculated from static quantita-tive arteriographic dimensions, compared with cor-onary flow reserve, which is derived from directmeasurement of the instantaneous ratio of hyper-emic to rest flow. Coronary flow reserve dependson perfusion pressure, coronary venous pressureand/or arteriolar tone, and strength of the hyper-emic stimulus; two stenoses of exactly the samegeometry may have entirely different values ofcoronary flow reserve in different patients, or evenin the same patient under different hemodynamicconditions. SFR, in contrast, is independent ofhemodynamic conditions. It describes the conduc-tance of the stenosis itself as if the arterial segmentwere excised and studied in vitro under controlledconditions. In the present application, this feature isadvantageous because it allows comparison betweenpatients. Neither measurement is superior; each
0lXl
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

Demer et al Cardiac PET and Quantitative Arteriography 833
measures a different aspect of the stenosis, andeach is applicable to a different clinical question.
Stenosis Flow Reserve Compared WithDiameter NarrowingThe advantages of SFR over percent diameter
narrowing, including the use of all relevant dimen-sions and absolute dimensions to allow for diffusedisease, have been described previously.21 To assessthe importance of dimensions other than percentdiameter narrowing that enter into the equation forstenosis flow reserve, calculated SFR was plottedas a function of percent diameter narrowing for thefirst 100 patients (Figure 4). Further patients werenot included because of overlap of data points. Thescatter in this relation represents the effect of fac-tors other than relative diameter, such as length,absolute cross-sectional area, and expansion angle,that determine stenosis flow reserve.These data reveal important limitations of the use
of percent diameter narrowing as the sole indicatorof stenosis severity, even when it is measuredaccurately. For arteries with 50% diameter narrow-ing, stenosis flow reserve ranges from 2.8 to 4.5.The spread is even wider for 60% narrowing. Manystenoses with more than 50% diameter narrowinghave only mild or minimal reduction in SFR. Of 107stenoses with more than 50% diameter narrowing,30% had only mild SFR reduction (SFR.3), and 8%had nearly normal coronaries (SFR.4). Thus, true-negative perfusion scans associated with such lesionswould be labeled as false-negative, if 50% diameterreduction alone were used to define significantcoronary disease. In some studies, the criterion forsignificant coronary stenoses is 75% diameter nar-rowing. This cut-off point, or even 70% diameternarrowing, classifies a large number of stenoseswith a significantly reduced SFR as negative. Onethird of stenoses with less than 75% diameter nar-rowing had significantly reduced stenosis flowreserve (SFR <3), and 16% of these were severelynarrowed (SFR < 2). As a result, true-positive scansassociated with such lesions would be labeled asfalse-positive, were 75% diameter narrowing aloneused to define significant coronary disease.
PET Defect Severity Compared WithStenosis SeverityPET defect severity correlated significantly with
arteriographic stenosis severity in both the regionaland patient-by-patient analysis. However, there wasconsiderable scatter in these relations which may beattributable to the subjective scoring of PET defectsor other limitations described below.
Rest PET Compared With Myocardial InfarctionThe relation between PET defects and myocar-
dial infarction has been previously described in asmaller group of patients.34 The present resultsconfirm that resting perfusion defects seen by PETcorrespond to clinical myocardial infarction.
Interobserver AgreementInterobserver disagreement occurred primarily
in scans of patients with mild coronary diseaseand those with small defects. The finding of 75%and 76% identical or essential agreement forrest and stress scans, respectively, is comparablewith the 79% exact or essential interobserveragreement reported for 20`TI images with a slightlydifferent analytic method.27
Potential LimitationsThe use of a subjective scoring method for PET
defect severity most likely accounts for much of thescatter in the relations in Figure 3. Quantitativemethods for describing PET defect severity havebeen described, such as measurement of relativemyocardial perfusion reserve.35 However, this tech-nique was not practical for the large number ofpatients in the present study because it requiressubjective border delineation for regional analysisand assumes the presence of a normal region ofmyocardium in each patient. Technical limitationsof quantitative PET imaging include cardiac motion,patient motion, partial volume errors, and decreasedextraction of perfusion tracers at high flows.36,37Subendocardial infarction may add to apparent errorby introducing a partial-thickness perfusion defectwithout a correspondingly severe stenosis in thesupply artery.
Stenoses in series may not have been accuratelyassessed. Only the single most severe stenosis wasused to represent each artery because stenoses inseries do not necessarily behave as additive resis-tances, due to intervening branches, and criteria forquantitative analysis of such lesions have not beenestablished.Anatomic variations in the coronary tree and
overlap of perfusion beds limited the accuracy ofmatching each stenosis to a corresponding defect.For this reason, an additional analysis was per-formed to compare results for individual patientsirrespective of defect location. This effect wouldtend toward underestimation of the relation betweenPET defect and stenosis severity by contributing toscatter. In addition, variation in perfusion bed sizemay cause arteries with equally severe stenoses tohave variable sizes of PET defect.
Stenosis flow reserve may not correspond to PETperfusion reserve in the presence of altered physio-logic conditions such as very high or low perfusionpressure and heart rate, collateral flow, increasedresting flow, ventricular hypertrophy, abnormalvenous pressure, or inadequate vasodilatory stimu-lus.38 Although direct measurement of coronary flowreserve reflects these conditions, except for collat-eral flow, it may not be advantageous because hemo-dynamic conditions are likely to change between thetimes of catheterization and PET imaging.
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
834 Circulation Vol 79, No 4, April 1989
SummaryTraditionally, noninvasive tests for the detection
of coronary artery disease have been comparedwith percent diameter stenosis using binary classi-fication and sensitivity-specificity analysis.1-4,39Recent analyses-56'8'11'40 have indicated the need forcomparison to a more accurate gold standard andthe use of continuous rather than binary outcomevariables. In the present study, subjective PETdefect severity and quantitative arteriographic ste-nosis flow reserve, a more physiologic gold stan-dard, were compared over the full spectrum ofcoronary disease severity. Results indicate thatsubjective severity of regional PET perfusion defectscorrelates significantly with the calculated stenosisflow reserve of the corresponding coronary arteries.
AcknowledgmentsWe are grateful to Jeffrey Gornbein, DrPH, for
assistance with statistical analysis; to Barry Elson,Martin Buchi, and Yvonne Stuart for technicalassistance; and to Claire Finn and Kathryn Rain-bird for assistance with the manuscript. Intra-venous dipyridamole was kindly provided byBoehringer Ingelheim, Inc.
References1. Ritchie JL, Trobaugh GB, Hamilton GW, Gould KL, Nara-
hara KA, Murray JA, Williams DL: Myocardial imagingwith thallium-201 at rest and during exercise: Comparisonwith coronary angiography and resting and stress electrocar-diography. Circulation 1977;56:66-71
2. Hamilton GW, Trobaugh GB, Ritchie JL, Williams DL,Weaver DW, Gould KL: Myocardial imaging with intrave-nously injected thallium-201 in patients with suspected cor-onary artery disease: Analysis of technique and correlationwith electrocardiographic coronary anatomic and ventricu-lographic findings. Am J Cardiol 1977;39:347-354
3. VanTrain K, Berman D, Garcia EV, Berger HJ, Sands M,Freidman J, Freeman M, Pryzlak M, Ashburn W, Norris S,Green A, Maddahi J: Quantitative analysis of stress thallium-201 myocardial scintigrams: A multicenter trial. JNucl Med1986;27:17-25
4. Ritchie JL, Zaret BL, Strauss HW, Pitt B, Berman DS,Schelbert HR, Ashburn WL, Berger HJ, Hamilton GW:Myocardial imaging with thallium-201: A multicenter studyin patients with angina pectoris or acute myocardial infarc-tion. Am J Cardiol 1978;42:345-350
5. Massof R, Emmel T: Criterion-free, parameter-free,distribution-independent index of diagnostic test perfor-mance. Appl Optics 1987;26:1395-1408
6. Hlatky MA, Mark DB, Harrell FE, Lee KL, Califf RM,Pryor DB: Rethinking sensitivity and specificity. Am JCardiol 1987;59:1195-1198
7. Marcus ML, Skorton DJ, Johnson MR, Collins SM, Harri-son DG, Kerber RE: Visual estimates of percent diametercoronary stenosis: A battered gold standard. J Am CollCardiol 1988;11:882-885
8. Gould KL: Percent coronary stenosis: Battered gold stan-dard, pernicious relic, or clinical practicality? J Am CollCardiol 1988;11:886-888
9. White CW, Wright CB, Doty DB, Hiratza LF, Eastham CL,Harrison DG, Marcus ML: Does visual interpretation of thecoronary arteriogram predict the physiologic importance of acoronary stenosis? N EnglJ Med 1984;310:819-824
10. Mates RE, Gupta RL, Bell AC, Klocke FJ: Fluid dynamicsof coronary artery stenosis. Circ Res 1978;42:152-162
11. Marcus ML, White CW, Kirchner PT: Isn't it time toreevaluate the sensitivity of non-invasive approaches for thediagnosis of coronary artery disease? J Am Coll Cardiol1986;8:1033-1034
12. Brown BG, Bolson E, Frimer M, Dodge HT: Quantitativecoronary arteriography: Estimation of dimensions, hemody-namic resistance, and atheroma mass of coronary arterylesions using the arteriogram and digital computation. Cir-culation 1977;55:329-337
13. Kirkeeide RL, Gould KL, Parsel L: Assessment of coronarystenoses by myocardial perfusion imaging during pharmaco-logic coronary vasodilation: VII. Validation of coronary flowreserve as a single integrated functional measure of stenosisseverity reflecting all its geometric dimensions. JAm CollCardiol 1986;7:103-113
14. Wilson RF, Laughlin DE, Ackell PH, Chilian WM, HolidaMD, Hartley CJ, Armstrong ML, Marcus ML, White CW:Transluminal subselective measurement of coronary arteryblood flow velocity and vasodilator reserve in man. Circu-lation 1985;72:82-92
15. Wijns W, Serruys PW, Reiber JHC, VandenBrand M, Sim-oons ML, Kooijman CJ, Balakumaran K, Hugenholtz PG:Quantitative angiography of the left anterior descendingcoronary artery: Correlations with pressure gradient andresults of exercise thallium scintigraphy. Circulation 1985;71:273-279
16. Schelbert HR, Wisenberg G, Phelps ME, Gould KL, HenzeE, Hoffman EJ, Gomez A, Kuhl DE: Noninvasive assess-ment of coronary stenoses by myocardial imaging duringpharmacologic coronary vasodilation: VI. Detection of cor-onary artery disease in man with intravenous 13-NH3 andpositron computed tomography. Am I Cardiol 1982;49:1197-1207
17. Gould KL, Goldstein RA, Mullani NA, Kirkeeide RL, WongWH, Tewson TJ, Berridge MS, Bolomey LA, Hartz RK,Smalling RW, Fuentes F, Nishikawa A: Noninvasive assess-ment of coronary stenoses by myocardial perfusion imagingduring pharmacologic coronary vasodilation: VIII. Clinicalfeasibility of positron cardiac imaging without a cyclotronusing generator-produced rubidium-82. JAm Coll Cardiol1986;7:775-789
18. Kirkeeide RL, Fung P, Smalling RW, Gould KL: Automatedevaluation of vessel diameter from arteriograms, in Comput-ers in Cardiology: Proceedings ofIEEE Computer Society.New York, IEEE, 1982, pp 215-219
19. Gould KL, Kelley KO: Experimental validation of quantita-tive coronary arteriography for determining pressure-flowcharacteristics of coronary stenoses. Circulation 1982;66:930-937
20. Gould KL, Kelley KO: Physiological significance of coro-nary flow velocity and changing stenosis geometry duringcoronary vasodilation in awake dogs. Circ Res 1982;50:695-704
21. Gould KL: Identifying and measuring severity of coronaryartery stenosis: Quantitative coronary arteriography andpositron emission tomography. Circulation 1988;78:237-245
22. Mullani NA, Ficke DC, Hartz R, Markham J, Wong WH:System design of fast PET scanners utilizing time-of-flight.IEEE Trans Nucl Sci 1981;28:104-108
23. Yano Y, Cahoon JL, Budinger TF: A precision flow-controlled Rb-82 generator for bolus or constant-infusionstudies of the heart and brain.JNuclMed 1981;22:1006-1010
24. Schelbert HR, Phelps ME, Huang SC, MacDonald NS,Hansen H, Selin C, Kuhl DE: N3 ammonia as an indicatorof myocardial blood flow. Circulation 1981;63:1259-1272
25. Tamaki N, Yonekura Y, Senda M, Kureshi SA, Saji H,Kodama S, Konishi Y, Ban T, Kambara H, Kawai C,Torizuka K: Myocardial positron computed tomographywith N-13 ammonia at rest and during exercise. Eur JNucMed 1985;11:246-251
26. Brown BG, Josephson MA, Petersen RB, Pierce CD, WongM, Hecht HS, Bolson E, Dodge HT: Intravenous dipyridam-ole combined with isometric handgrip for near maximal
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

Demer et al Cardiac PET and Quantitative Arteriography 835
acute increase in coronary flow in patients with coronaryartery disease. Am J Cardiol 1981;48:1077-1085
27. Ter-Pogossian MM, Klein MS, Markham J, Roberts R,Sobel BE: Regional assessment of myocardial metabolicintegrity in vivo by positron-emission tomography withC-11-labeled palmitate. Circulation 1980;61:242-255
28. Budinger TF, Rolio D: Physics and instrumentation. ProgCVDis 1977;20:19-53
29. Trobaugh GB, Wackers FJTh, Sokole EB, DeRouen TA,Ritchie JL, Hamilton GW: Thallium-201 myocardial imag-ing: An interinstitutional study of observer variability. JNucl Med 1978;19:359-363
30. Zijlstra F, Fioretti P, Reiber JHC, Serruys PW: Whichcineangiographically assessed anatomic variable correlatesbest with functional measurements of stenosis severity? Acomparison of quantitative analysis of the coronary cinean-giogram with measured coronary flow reserve and exercise/redistribution thallium-201 scintigraphy. JAm Coil Cardiol1988;12:686-691
31. Harrison DG, White CW, Hiratza LF, Doty DB, Barnes DG,Eastham CL, Marcus ML: The value of lesion cross-sectional area determined by quantitative coronary angiog-raphy in assessing the physiologic significance of proximalleft anterior descending coronary arterial stenoses. Circula-tion 1984;69:1111-1119
32. Diem K (ed): Documenta Geigy: Scientific Tables, ed 6.Ardsley, New York, Geigy Pharmaceuticals, 1962, p 88
33. Demer LL, Gould KL, Kirkeeide R: Assessing stenosisseverity: Coronary flow reserve, collateral function, quanti-tative coronary arteriography, positron imaging, and digitalsubtraction angiography. A review and analysis. Prog CVDis 1988;30:307-322
34. Goldstein RA, Mullani NA, Wong WH, Hartz RK, HicksCH, Fuentes F, Smalling RW, Gould KL: Positron imagingof myocardial infarction with rubidium-82. JNucl Med 1986;27:1824-1829
35. Goldstein RA, Kirkeeide RL, Demer LL, Merhige M, Nishi-kawa A, Smalling RW, Mullani NA, Gould KL: Relationbetween geometric dimensions of coronary artery stenosesand myocardial perfusion reserve in man. J Clin Invest 1987;79:1473-1478
36. Mullani NA, Gould KL: First pass regional blood flowmeasurements with external detectors. J Nucl Med 1983;24:577-581
37. Mullani NA, Goldstein RA, Gould KL, Fisher DJ, MaraniSK, O'Brien HA: Myocardial perfusion with rubidium- 82: I.
Measurement of extraction fraction and flow with externaldetectors. J Nucl Med 1983;24:898-906
38. Klocke FJ: Measurements of coronary flow reserve: Definingpathophysiology versus making decisions about patient care.Circulation 1987;76:1183-1189
39. DePasquale EE, Nody AC, DePuey EG, Garcia EV, PilcherG, Bredlau C, Roubin G, Gober A, Gruentzig A, D'Amato P,Berger H: Quantitative rotational thallium-201 tomographyfor identifying and localizing coronary artery disease. Circu-lation 1988;77:316-327
40. Diamond GA, Rozanski A, Forrester JS, Morris D, PollockBH, Staniloff HM, Berman DS, Swan HJC: A model forassessing the sensitivity and specificity of tests subject toselection bias: Application to exercise radionuclide ventric-ulography for diagnosis of coronary artery disease.J ChronicDis 1986;39:343-355
KEYWoRDs * cardiac PET * quantitative coronary arteriography* coronaiy stenosis * perfusion imaging
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

Nishikawa and M E MerhigeL L Demer, K L Gould, R A Goldstein, R L Kirkeeide, N A Mullani, R W Smalling, A
Comparison with quantitative arteriography in 193 patients.Assessment of coronary artery disease severity by positron emission tomography.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.79.4.825
1989;79:825-835Circulation.
http://circ.ahajournals.org/content/79/4/825the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from