Assessment and Management of Delirium in Older Adults
49
Assessment and Management of Delirium in Older Adults Dr. Dallas Seitz and Dr. Agata Szlanta
description
Assessment and Management of Delirium in Older Adults. Dr. Dallas Seitz and Dr. Agata Szlanta. Objectives. Understand the differential diagnosis and presentation of delirium in older adults; Review the risk factors and precipitants for delirium; and - PowerPoint PPT Presentation
Transcript of Assessment and Management of Delirium in Older Adults
Slide 1
Assessment and Management of Delirium in Older AdultsDr. Dallas Seitz and Dr. Agata SzlantaObjectivesUnderstand the differential diagnosis and presentation of delirium in older adults;Review the risk factors and precipitants for delirium; and Discuss delirium prevention and management strategies.
Case 1:Mr. A: 75 y.o. male, resides with wifeRFV: wife concerned that husband is depressed
HPI:Recently discharged from KGH following 3 week admission for community acquired pneumoniaNever fully recovered physically or mentally since his KGH dischargeStarted on antidepressant in hospital for depressive symptoms in hospital, zopiclone to help with sleepSince discharge: Napping for most of the day, having some difficulties with sleep at nightSeems disinterested in environmentWife now having to assist with personal careIncontinence has worsened and gait is unsteadyOral intake poor over last weekSpeech difficult to understand at times
Past Medical History:Mild cognitive impairmentCAD with angioplastyDyslipidemiaChronic renal failureHypertensionBenign prostate hypertrophyDepression (recently diagnosed)
Medications:Citalopram 20 mg po ODZopiclone 7.5 mg po QHSMetoprolol 25 mg PO BIDRosuvastatin 20 mg PO QHSDutasteride 0.5 mg PO QHSTamsulosin 25 mg PO ODHCTZ 25 mg PO OD
Case objectivesDifferential diagnosis?How to you confirm your diagnosis?Office work-up and management
Triple DDeliriumDementiaDepressionOnsetAcuteInsidiousVariableDurationDays to weeksMonths to yearsVariableCourseFluctuatingSlowly progressiveDiurnal variationConsciousnessImpaired, fluctuatesClear until late in illnessUnimpairedAttention & MemoryInattentive,Poor memoryPoor memory without inattentionDifficulty concentrating, memory intactAffectVariableVariableDepressed, loss of interest and pleasureCCSMH, Delirium Guidelines, 2006DSM-IV criteria DeliriumDisturbance of consciousnessChange in cognition, not accounted for by pre-existing dementiaOnset over a short period of time and fluctuating presentationEvidence from history, physical exam, or lab findings that the disturbance is caused by direct physiological consequences of a general medical condition.Diagnosing DeliriumAcute Onset and Fluctuating Course+InattentionDisorganized ThinkingAltered Level of ConsciousnessORAdapted from: Inouye, et al. Ann Intern Med 1990;113:941-948Confusion Assessment Method+10Comments about the sensitivity and specificity of the CAMSubtypesHypoactiveMore lethargic, difficult to arouse, minimal speech, slowed motor responseDdx: depression or dementiaHyperactiveRestless, agitated, hallucinations, hypervigilance, delusionsDdx: hypomania mania, psychosis, anxiety disorders, akathisia
Mixed
PathophysiologyFong et al. Nat Rev Neuro. 2009 April; 5(4): 210-220
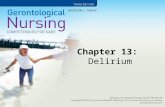
Predisposing Factors/ VulnerabilityPrecipitating Factors/ InsultsDementiaSevere illnessMulti-sensory impairmentHealthy young personHigh VulnerabilityLow VulnerabilityNoxious InsultNon-noxious insultMajor surgeryICU stayMultiple psychoactivemedicationsSleep deprivationOne dose of sleeping medicationAdapted from: Inouye and Charpentier, JAMA 1996;275:852-857Advanced ageUTI13This is Sharon Inouyes model of delirium illustrating the interplay of precipitating and predisposing factors in delirium, for example in an elderly person with dementia and perhaps other medical co-morbidities, one dose of sleeping medication or a urinary track infection may be enough to precipitate delirium,On the other hand a young healthy individual would need to be confronted with a major physiological insult such as a mutli organ trauma or major operation to stress them sufficiently to cause deliriumPredisposing FactorsAge (>65)Cognitive impairment dementia is present in up to 2/3 of cases of delirium in the elderlyMaleHistory of delirium
Sensory impairementDehydrationPoor functional status (immobility, falls)Alcohol abusePsychoactive drugsMultiple medical conditions
Precipitating FactorsIntercurrent illnessInfection, CHF, metabolic abnormality, hypoxiaProlonged sleep deprivationSurgeryEnvironmetalRestraints, catheter, pain
MEDS, MEDS, MEDSSedativesNarcoticsAnticholinergicsPsychoactivesHistamine-2 blocking agentsAntiparkinsonianOver the counter (benadryl, gravol)Chronic medspolypharmacy
DELIRIUM multifactorial!D rugsE yes, earsL ow oxygen states (MI, PE, stroke)I nfectionR etentionI ctalU nderhydration/undernutritionM etabolicS ubuduralConsequences of DeliriumOne year mortality of 35-40%.Associated with worse prognosis- risk of dementia, institutionalization and death UnderdiagnosedPrevalence in community: 1-2% in older adults, 14% in > 85 yoUp to 1/3 of cases are preventable
Persistent DeliriumSystematic review by Cole1
Substantial number of patients with in-hospital delirium not fully recovered Worse outcomes: LTC placement, cognition, function and mortalityTime to recovery is variable1Cole, M. Systematic Review. Age and Ageing 2009: 38: 19-26.Discharge1 month3 mo6 moPersistent Delirium45%33%26%21%Investigations?Delirium work upCBCCalcium, albumin, Cr, electroylytes, Liver function Tests, glucoseTSHUrine culture ECG, blood culture, Chest X-ray, blood gas
Case 2Mrs. O.P.83 year old women lives alone in own home roomFound by paramedics on floor in home after family called police due to no telephone callTripped on rug in home fell (?approximately 24 hours)Pain and bruising over L hipVitals: Pulse = 110, BP = 150/95, RR = 16Past Medical HistoryMedical ConditionsMedicationsHTNModerate aortic stenosisObesityDiabetes mellitus IIOsteoarthritisHearing ImpairmentUrinary incontinenceHCTZInsulinOxybutyninIbuprofenTylenolInvestigationsBlood WorkImagingHgb = 90Na2+ = 130K+ = 5.0Cl- = 99FBG = 12Creatinine = 95Urea = 13eGFR = 40INR = 1.1
24Hospital Course4 day delay to surgery, NPO in emergency roomLying on stretcher in hallwayFoley catheter due to limited mobilityReceives general anesthetic for surgeryUndergoes left hip pin and plateDischarged to orthopedic floor
QuestionsWhat risk factors does Mrs. E.B. have for postoperative delirium?
Postoperative DeliriumOutcomes associated with postoperative delirium:Functional decline: OR = 2.0 hospital length of stayMortality: OR = 2.4
Surgical ProcedureIncidenceOrthopedic30 50%Cardiac20 50%General surgery18%Urologic5 10%Predisposing Factors for DeliriumDemographic characteristicsAdvanced age (> 65)Male sexCognitive StatusDementiaDepressionPast History of DeliriumFunctional StatusImmobilityFunctional dependenceLow level of activityHistory of fallsSensory ImpairmentVisual impairmentHearing impairmentNutritional StatusDehydrationMalnutritionMedicationsPolypharmacyPsychoactive medicationsAlcohol abuseMedical HistoryStrokeNeurological diseaseMetabolic diseasesHepatic or renal failureSeverity of illnessFracture or trauma
Risk Factors for Postoperative DeliriumRelative RiskAge 703.4Male Gender2.0MMSE < 244.0Severity of illness4.3Visual impairment3.0Dehydration (BUN/creatinine ratio 18)2.9Alcohol abuse2.4Functional impairment2.1Abnormal Na2+, K+, or glucose2.8WBC > 122.3QuestionsWhat interventions could be utilized to prevent postoperative delirium?Hospital Elder Life ProgramPrevention of delirium through addressing common delirium risk factors:CognitionSleep deprivationImmobilityVisual impairmentHearing ImpairmentDehydrationDelirium outcomes:Incidence: 9.9 vs 15% (OR = 0.6, p=0.02)Duration and recurrence of delirium also reduced
NICE Delirium PreventionEnsure providers are familiar with patient, avoid unnecessary transfers within and between wards.Multicomponent intervention should be used for all individuals including risk assessment within 24 hours.Intervention should be delivered by multidisciplinary teamAddress cognitive impairment by orientation measures, clear signage, clock, calendar, and reassurance.Ensure adequate oral intake and prevent constipation.Assess for and treat hypoxia.Look for and treat infections, avoid catheterization.NICE Delirium PreventionAddress and minimize immobility through encouragement of walking and/or active range of motion exercises.Assess and address pain, look for non-verbal signs of pain in individuals with communication difficulties.Carry out a medication review.Address poor nutrition and ensure that dentures fit.Address sensory impairment by resolving reversible causes of impairment and ensure use of aids.Promote good sleep patterns and hygiene through scheduling of work routines and minimizing noise.Delirium Rooms4-bed room within Acute Care of Elderly (ACE) unitRationale: provide constant nursing supervision without use of sitters, restraints, and minimize use of medicationsStaffed by one RPN with shared RN coverageAll patients are visible to RPN, room close to RN stationTADA: tolerate, anticipate, and dont agitateNo increase in rates of falls, reduction in use of psychotropics to manage delirium symptomsPharmacological InterventionsAntipsychotics:Postoperative ICU patients receiving bolus (0.5 mg IV) + infusion (0.1mg/hour) haloperidol had a lower rate of postoperative delirium (15.3% vs 23.2%)Low-dose haloperidol (0.5 mg PO TID) reduced severity and duration of delirium but not incidence in hip surgerySingle dose of 1 mg risperidone reduced delirium in cardiac surgery patientsCholinesterase inhibitors:3 small RCTs have failed to show any benefitGabapentin:1 small RCT demonstrating benefit (? opioid sparing)
Case 3Mrs. A.D., 89 y.o. female, resident in LTC facility for 2 yearsNurses ask you to assess as she hasnt been herself over past two daysFlucuates between being drowsy and restless, yelling out, picking at air, falling out of bed, increasingly difficult to provide careIn Broda chair most of the day now, bed rails up at night to prevent fallsPRN lorazepam ordered by on-call physician
MedicationsDonepezil 10 mg 0dMemantine 10 mg BIDClopidogrel 75 mg po odBisoprolol 5 mg PO ODPantoprazole 40 mg po odTylenol 1 g TIDHydromorphone 0.5 mg po BID prnLorazepam 1 mg PO BID prn (given twice in last 24 hours)
Past Medical HistoryAlzheimers diseaseLast MDS-RAI: Cognitive Performance Scale score: 6Global Deterioration Scale: stage 7 (non-verbal, bed-bound, incontinent of bowel and bladder)StrokeCoronary artery diseaseCOPDGERDOsteoarthritis in both hips (L THR)
What is your differential diagnosis?Initial investigations?Delirium Superimposed on DementiaPrevalence: 22 - 89% of hospitalized and community patientsAccelerates cognitive and functional declineUnderdiagnosed as some behaviours can also occur in dementiaDifficult to diagnosis in advanced dementiaDelirium in Long-Term CarePrevalenceMMSE 10: 3.4%MMSE < 10: 33.3%Incidence:MMSE 10: 1.6/100 person weeksMMSE < 10: 7/100 person weeks
Risk FactorHazard RatioDementia2.6Dementia Severity Minimal Mild Moderate Severe1.05.110.19.5Depression2.1Behavioral Changes and Medical IllnessSymptomPredictive ValueLiklihood RatioLethargy*0.517.3Weakness*0.507.0Decreased appetite*0.466.0Agitation*0.374.2Disorientation0.313.2Dizziness0.272.5Falls*0.232.1Delusions0.211.9Depressed mood0.171.4Weight loss0.171.4Aggression0.131.0*p < 0.05Boockvar, JAGS, 2003Acute Medical Illness in LTC UTIPneumoniaGICardiacDehydrationOtherBoockvar, 200328%18%20%17%8.8%8%Hung, 201027%10%--16%5%40%Alessi, 199827%33%Management of DeliriumTreat correctable causesWithdraw all medications contributing to delirium when possibleStart antibiotics promptlyEnsure cardiovascular stability, oxygenation, and electrolyte balanceEnsure hydration and monitor fluid intake and output
Management of DeliriumAssess and monitor nutrition and skin integrityIndentify and correct sensory deficitsAssess and manage pain using safest interventionsSupport normal sleep patterns and avoid use of sedativesPharmacological InterventionsMedicationInitial Dosage(mg)Mean Daily Dose(mg)Haloperidol0.25 0.5 mg bid1.5 5 mgRisperidone0.25 0.5 mg bid1 2 mgOlanzapine2.5 5 mg5 7.5 mg Quetiapine12.5 25 mg bid50 125 mgConclusionsDelirium is common among older adults and can have a number of presentationsManagement of delirium needs to include a comprehensive review of risk factors and potential precipitantsPrevention and non-pharmacological interventions are cornerstones of delirium careRESOURCESCanadian Coalition for Seniors Mental Health. The Assessment and Treatment of Delirium. www.ccsmh.caCCSMH Pocket Card: Delirium Assessment and Treatment for Older AdultsAmerican Geriatrics Society. Geriatrics at Your Fingertips. Inouye SK. Delirium in Older Persons. N Eng J Med 2006;354:1157-1165Journal of the American Geriatrics Society. 2011; Nov Supplement: Advancing Delirium Science: Systems, Mechanisms, and Management
Questions?