Assessing Risk in Drug Development David M. Benjamin, Ph.D. Clinical Pharmacologist & Toxicologist...
55
Assessing Risk Assessing Risk in Drug Development in Drug Development David M. Benjamin, Ph.D. David M. Benjamin, Ph.D. Clinical Pharmacologist & Toxicologist Clinical Pharmacologist & Toxicologist Adjunct Assistant Professor - Tufts Medical School Adjunct Assistant Professor - Tufts Medical School Fellow, American Academy of Forensic Sciences (Toxicology) Fellow, American Society for Healthcare Risk Management Fellow, American College of Clinical Pharmacology Fellow, American College of Legal Medicine
-
date post
18-Dec-2015 -
Category
Documents
-
view
223 -
download
3
Transcript of Assessing Risk in Drug Development David M. Benjamin, Ph.D. Clinical Pharmacologist & Toxicologist...

Assessing Risk Assessing Risk in Drug Developmentin Drug Development
David M. Benjamin, Ph.D.David M. Benjamin, Ph.D.
Clinical Pharmacologist & ToxicologistClinical Pharmacologist & Toxicologist
Adjunct Assistant Professor - Tufts Medical SchoolAdjunct Assistant Professor - Tufts Medical School
Fellow, American Academy of Forensic Sciences (Toxicology)
Fellow, American Society for Healthcare Risk Management
Fellow, American College of Clinical Pharmacology
Fellow, American College of Legal Medicine

Goals of the PresentationGoals of the Presentation
Provide Criteria for Assessing Risk in Drug Development
Describe Theories of Drug Product Liability Examine Omniflox, Baycol and other Recent
Drug Withdrawals Identify Reasons for Drug Withdrawal Review Criteria for “Adequate” labeling

What Got Everything Started?What Got Everything Started?
The Institute of Medicine issued: To Err is Human which reported that 44,000 - 98,000 patients died each year as a result of “Medical Error” (e.g., medication errors, surgical errors, missed diagnoses)
At an estimated cost to the US economy of $17-$29 billion

Major Findings of the IOM StudyMajor Findings of the IOM Study
Based on two reports from three states: New York (1984), Utah and Colorado (1992)
NY study sampled 30,000 charts from 51 state hospitals and found:
3.7% of pts suffered injury severe enough to disable them or prolong hospitalization
58% of these injuries were due to error; 13.6% were fatal

Major Findings of the IOM Major Findings of the IOM Study-2Study-2
The 98,000 number was extrapolated from the NY study, based on the number of hospitalizations for 1997
Based on reports from Utah and Colorado (1992) 15,000 charts were sampled and a value of 44,000
deaths was extrapolated from these data The IOM report has been criticized by one of the
investigators, Troyen Brennan, MD, JD, MPH of the Harvard School of Public Health

Drug Product Liability:Drug Product Liability:Murphy’s Law RulesMurphy’s Law Rules
“Often, however, the benefits to the many come at a high cost to the few, for there are increasingly more opportunities for mishaps, not only in the manufacturing process, but also in the marketing and use of the finished products.” Page Keeton, Former Dean, U. Page Keeton, Former Dean, U. of Texas School of Law, (Michigan Law of Texas School of Law, (Michigan Law Review, 1966)Review, 1966)

What About Investigational What About Investigational Drugs During Development?Drugs During Development?
Chemical Animal Pharmacology Animal Toxicology Clinical Phases I-III: 2,500-
5,000 patients only detects ADRs of 1/1000 (0.1%)
Post-Marketing: hundreds of Post-Marketing: hundreds of thousands to millionsthousands to millions

Types of Adverse Drug Reactions Types of Adverse Drug Reactions (ADRs) Frequently Encountered(ADRs) Frequently Encountered Overmedication Side Effect Secondary Effect AllergicAllergic IdiosyncraticIdiosyncratic DrugDrug--DrugDrug Interaction Investigational Drugs - Fewer pts. Investigational Drugs - Fewer pts.
studied; less info available to IRBs; studied; less info available to IRBs; e.g., Investigator’s Drug Brochure e.g., Investigator’s Drug Brochure

Evaluating ADRs for Causation Evaluating ADRs for Causation Does alleged ADR: (1) follow a reasonable temporal
sequence from drug administration Does alleged ADR represent a known effect of the
drug? Could the alleged ADR be caused by: (1) the
patient’s pathophysiological (clinical) condition or (2) an intercurrent illness?
Could alleged ADR be caused by: (1) prior exposure to another agent or (2) concomitant medication?

Evaluating ADRs for Causation -2Evaluating ADRs for Causation -2 Is there a prior History of Sensitivity? What were the: Dosage, Frequency and
Route of Administration? What was the patient’s Cardiac, Pulmonary,
Hepatic and Renal Status? Was the patient receiving any Concomitant
Medications, OTC meds, herbals or alternative medical products?
Was suspect drug D/C’d? Was suspect drug restarted? With what effects on ADR?

Theories of Drug &Theories of Drug &Device Product Liability:Device Product Liability:
Defective Warning (Failure to Warn) Inadequate Testing (Animal or Human) Overpromotion (Lack of Fair Balance)Overpromotion (Lack of Fair Balance) Defectively Designed Drug or Device
(Unfit for intended (Unfit for intended purpose)purpose)
Adulterated or Contaminated DrugAdulterated or Contaminated Drug

Communication of InformationCommunication of Information
Pharmaceutical Company ---warns--> Pharmaceutical Company ---warns--> Physician of known adverse effectsPhysician of known adverse effects
Physician serves as “Learned Intermediary” for patient
Physician provides patient with Informed Physician provides patient with Informed ConsentConsent
Including Including reasonablyreasonably foreseeable, foreseeable, materialmaterial risksrisks
Once fully informed, the patient either:Once fully informed, the patient either:
accepts treatmentaccepts treatment or or states informed refusalstates informed refusal

VicariousVicarious Defendants in Drug & Defendants in Drug & Device Product Liability SuitsDevice Product Liability Suits
Pharmaceutical Manufacturer is Primary, vicarious defendants include:
Physician Prescribing Medication Distributor Pharmacist Dispensing MedicationPharmacist Dispensing Medication Nurse Administering MedicationNurse Administering Medication Hospital Employing MD, Reg.Ph., or RN Apparent or ostensible agents of entity or
medical school, e.g., IRB members

Defenses for Vicarious Defenses for Vicarious DefendantsDefendants
Not negligent, or negligence was not a “Proximate Cause” of injury to patient (e.g., Bad Outcome)
Cannot warn when not informed or misled Cross-Claim against manufacturer Subrogation claim by insurance company Claim for injury to MD’s reputation see:
Washington State Physicians Ins. Exch & Ass’n Washington State Physicians Ins. Exch & Ass’n v. Fisons Corp.v. Fisons Corp. 858 P.2d 1054 (Wash. 1993) 858 P.2d 1054 (Wash. 1993)

Legal Theories of Liability, akaLegal Theories of Liability, aka What the lawyer says to the . . . What the lawyer says to the . . .
Physician: Physician: “Shouldn’t have prescribed it” Nurse: Nurse: “Shouldn’t have administered it” Pharmacist:Pharmacist: “Shouldn’t have dispensed it” Hospital: Hospital: “Shouldn’t have had it
in your formulary ” IRB: “Should have monitored
more closely or not approved protocol”


Federal Food, Drug, and Cosmetic Federal Food, Drug, and Cosmetic Act 1938Act 1938 Replaced US Pure Food and
Drug Act of 1906 Enacted as a result of the 1937
sulfanilamide crisis Ensured that: (1) Foods were
pure and wholesome, and produced under sanitary conditions, and that (2) Drugs were safe for their intended use (i.e., not adulterated).

Chloramphenicol - Approved 1949Chloramphenicol - Approved 1949 June 1952 JAMA article describes
aplastic anemia - sometimes fatal Jan 1967 Cal Med Assoc & Dept of
Health reported an incidence of aplastic anemia of: 1:25,000 in chloramphenacol users vs 1:524,000 in the general population (21X)
Lesson to be learned: Post-Marketing Surveillance is essential to identify rare, previously unrecognized ADRs

Thalidomide 1960Thalidomide 1960 FDA’s Dr. Frances Kelsey will not FDA’s Dr. Frances Kelsey will not
approve thalidomide for US marketapprove thalidomide for US market Mass Torts on teratogenic effects
postponed till Bendectin/Daubert 1962 Harris-Kefauver Amendment
to FDCA required: (1) animal testing prior to human administration, (2) filing of an IND, and (3) manufacturer must prove efficacy (in addition to safety) - NAS/NRC DESI Studies

Post-1960s Withdrawals Post-1960s Withdrawals We Have Known and Loved We Have Known and Loved
1970s1970s DESDES IUDs DPT/MMRDPT/MMR 1980s1980s Oraflex, Zomax, Oraflex, Zomax,
SuprofenSuprofen Generic Drugs Bendectin Bendectin
1990s1990s L-Tryptophan - EMSL-Tryptophan - EMS Omniflox - 5-month lifeOmniflox - 5-month life Toradol - 5-day labelingToradol - 5-day labeling Imitrex - First-Year EffectImitrex - First-Year Effect Silicone Breast ImplantsSilicone Breast Implants Fen-Phen - “Off-Label” useFen-Phen - “Off-Label” use Duract - Where is Dr. Duract - Where is Dr.
Kelsey when we still need Kelsey when we still need her?her?

Omniflox (temofloxacin) - PMOmniflox (temofloxacin) - PM
Introduced: Jan 1992Introduced: Jan 1992 First Rx: February 24First Rx: February 24 Voluntarily withdrawn: June Voluntarily withdrawn: June
9th - 15 weeks 9th - 15 weeks US Clin Trials 4,600 ptsUS Clin Trials 4,600 pts Mkt’d in 8 countries Est. Mkt’d in 8 countries Est.
300,000 pts rec’d drug 300,000 pts rec’d drug worldwide worldwide

Pre- vs Post- Marketing Pre- vs Post- Marketing Adverse Drug Reaction ReportsAdverse Drug Reaction Reports
Post-Marketing fewer than 300,000 pts 1,700 non-fatal ADRs
reported to FDA 54 cases of Acute
Renal Failure, 113 cases of hemolytic anemia
60 deaths, 25-50 may be related; Globe 1/94
Pre-Marketing 4,261 pts Incidence > 1% N,V,D,
headache, rash, itching
Labs: Incr. BUN & creatinine
Renal Failure <0.1%


Recent Withdrawn Drugs Recent Withdrawn Drugs Posicor - too many interactionsPosicor - too many interactions Rezulin - liver toxicityRezulin - liver toxicity Raxar - cardiac arrhythmiasRaxar - cardiac arrhythmias Propulsid - too many interactionsPropulsid - too many interactions Seldane/ Seldane/ Hismanyl - drugs inhibit - drugs inhibit
metabolism--> metabolism--> - long QT syndrome RotashieldRotashield - infant bowel obstruction - infant bowel obstruction Lotronex - off Nov 2000 GI ADRs & deaths; Lotronex - off Nov 2000 GI ADRs & deaths;
Re-instituted 2002 w/pt FURe-instituted 2002 w/pt FU Baycol (are other “statins” to follow?)Baycol (are other “statins” to follow?)


Why are Drugs Withdrawn Why are Drugs Withdrawn From the Market?From the Market?
Examples: Posicor, Propulsid, Seldane, and Hismanyl
Removed because of too Removed because of too many drug-drug interactionsmany drug-drug interactions
Manufacturers & FDA tried to minimize interactions by revising labeling - BUT
How do physicians view (and How do physicians view (and use) labeling?use) labeling?

FDA Studies on Practitioners’ FDA Studies on Practitioners’ Views About Drug Labeling Views About Drug Labeling
1992 Focus Groups Oct 1993-March 1994: FDA-sponsored
phone interview surveys of office-based MDs to determine:
How physicians perceive & use drug labeling, and
How labeling could be made more useful

““Survey Said:”Survey Said:”
Office-based MDs used labeling primarily to answer specific questions, rather than as a general educational tool
Labeling is typically consulted after a prescribing decision has been made
Physicians wanted: important information summarized in the front of labeling, and
More graphs, larger print, abstracting of important data

Re: Clinical PharmacologyRe: Clinical PharmacologySection Survey Said:Section Survey Said:
Among the least useful section Information in this section is used less often
than other labeling information Physicians wanted it “moved toward the
end of labeling”, and Important data from Clinical Pharmacology
Section should be put under other sections like “Special Populations” or “Drug Interactions”

Revising Labeling Will Not Revising Labeling Will Not Reduce Drug-Drug InteractionsReduce Drug-Drug Interactions Labeling is not Labeling is not readread Dear Dr. Letters are Dear Dr. Letters are
not not readread See Yarrow v. Sterling See Yarrow v. Sterling
Drug Inc, (on a Drug Inc, (on a subsequent slide) subsequent slide) regarding Aralen regarding Aralen (chloroquine) and (chloroquine) and labeled retinal damagelabeled retinal damage

Where’s the Proof ?Where’s the Proof ? Cisapride (Propulsid) withdrawal Marketed August 1993 By 1995, 5 million OutPt Rxs and FDA
had received reports of: 34 cases of torsade de pointes 23 cases of prolonged QT interval including 4 deaths
1995 “Black Box” warning added to labeling contraindicating use in pts also receiving drugs that block the CYP 3A4 enzymes, e.g. macrolides, “conazole” antifungals, & indinavir/ritonavir for HIV

More ProofMore Proof 1998 “Black Box” warning expanded to
contraindicate concomitant use of agents that caused prolongation of QT interval due to reports of serious arrhythmias, e.g., class IA or III antiarrhythmics, tricyclic anti-depressants, and antipsychotics, or in pts with “other conditions” that predispose to cardiac arrhythmias, e.g., vent. arrhythmia, CHF, ASHD, electrolyte imbalance, renal failure and respiratory failure.

Still More ProofStill More Proof June 26, 1998 - FDA circulated “Press Release”
and manufacturer sent “Dear Healthcare Professional” letter to 800,000 MDs informing them of the changes in the labeling
July 2000 - Manufacturer terminated marketing of cisapride in US
December 20, 2000 JAMA 284:3036-3039: Smalley et al reviewed regulatory history of cisapride in Contraindicated Use of Cisapride Impact of FDA Regulatory Action

Smalley, Shatin, Wysowski, et alSmalley, Shatin, Wysowski, et al Analyzed number of pts. at three centers who
received cisapride when it was contraindicated Received cisapride July 1997 - June 1998 (pre-
warning revision) vs. Received cisapride July 1998 - June 1999 (post-
warning revision) Pre-Warning Year 7/97-6/98: 26%, 30% & 60% Post-Warning Year 7/98-6/99: 24%, 28% & 58%

Smalley, Shatin, Wysowski, et alSmalley, Shatin, Wysowski, et al Conclusions: “There was no material reduction in . . . use
at any of the study sites following FDA regulatory action, which included a black-box warning . . . and a Dear Health Care Professional letter” page 3038
“. . . no material change in contraindicated use even in the group most likely to be affected by the regulatory action” - pts. beginning new cisapride use.

Smalley, Shatin, Wysowski, et alSmalley, Shatin, Wysowski, et al Conclusions: “ . . . despite the prominent publication of
case reports, label changes, and Dear Health Care Professional letters . . .”
“ . . . need to develop more effective methods for modifying practice to reflect new information about a drug’s risks and benefits.”

Ditto for MetforminDitto for Metformin Metformin marketed for Type 2 DM in 1995 with
“black box” warning regarding lactic acidosis Contraindications included: renal dysfunction and
CHF In 2000, 25 million Rxs for metformin Horlen, Malone, Dennis et al (letter in JAMA
287:2504-5) performed retrospective chart review of pts. who received metformin at UNC outpatient pharmacy between Jan 1, 2000 - Sept 30, 2000.

Metformin (continued)Metformin (continued) Metformin was prescribed twice or more for 241
pts. - 100 charts randomly selected 22% of pts. had either CHF or renal dysfunction;
14 CHF, 5 renal dysfunction, 3 had both CHF and renal dysfunction
Only 2 pts. had documentation in the medical record considered metformin contraindications
“. . . it is difficult to determine whether clinicians are aware they are prescribing metformin against a black-box warning.”

Yarrow v. Sterling re: AralenYarrow v. Sterling re: AralenWhere the doctor is inundated with the literature and product cards of the various drug manufacturers . . . a change in the literature or an additional letter intended to present new information on drugs to the doctor is insufficient. The most effective method employed by the drug company in the promotion of new drugs is shown to be the use of detail men; thus, the Court feels that this would also present the most effective method of warning the doctor about recent developments in drugs already employed by the doctor, at no great additional expense.
Yarrow v. Sterling Drug, Inc. 263 F. Supp. 159, 1963

What ADRs will this Drug Have?What ADRs will this Drug Have?
Look to animal studies Examine other drugs of the same
pharmacologic or chemical class Review SBA of other similar drugs Toxicity is the interaction of frequency and
severity, e.g., Severe but infrequent = OK, and Mild but common = OK
True frequency cannot be determined before marketing because “n” is too small

Assessing ADRs -1Assessing ADRs -1
SeveritySeverity
MildMild ModerateModerate SevereSevere |<|<--------------------50%----------------------------------50%-------------->|>|100% Nausea, More Than 100% Nausea, More Than Life- Rash? Annoying Life- Rash? Annoying ThreateningThreatening
Red & Itchy vs. SJS/TEN Red & Itchy vs. SJS/TEN

Assessing ADRs - 2Assessing ADRs - 2
FrequencyFrequency
Rare: <1/10,000, Rare: <1/10,000, e.g.,e.g., chloramphenacol &
blood dyscrasias
Rare, but life-threateningRare, but life-threatening
Frequent: >1/100, Frequent: >1/100, e.g.,e.g., headache & dry mouth
Frequent, but not serious

Characteristics of Characteristics of IdealIdeal Drug Drug Novel pharmacologic
action or treats condition for which no acceptable alternative exists
Higher Therapeutic Index Higher Therapeutic Index than other drugs in its classthan other drugs in its class
Lower frequency & severity Lower frequency & severity of reported reactions of reported reactions
Manufactured inexpensivelyManufactured inexpensively Secondary or multiple usesSecondary or multiple uses

What are the Most Common What are the Most Common Processes Associated with Processes Associated with
Medication Errors?Medication Errors? Physician ordering: 39-49% Nursing administration: 26-38% Transcription error: 11-12% Pharmacy dispensing error: 11-14%Pharmacy dispensing error: 11-14%
Source: Bates et al JAMA Source: Bates et al JAMA 1995;274(1):29-34 & Leape et al JAMA 1995;274(1):29-34 & Leape et al JAMA 1995;274(1):35-43.1995;274(1):35-43.

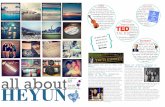
Portrait of a Poor Portrait of a Poor PrescriptionPrescription
What is the name of the first drug written on this prescription? See next slide for discussion.

The Correct Drug was . . .The Correct Drug was . . .
Final Answer: Isordil. Not Plendil, which was dispensed and caused fatal hypotension for which both the MD and RPh were held jointly liable for almost $500,000.

Why Computerize?Why Computerize?
MD computerized order entry decreased serious medication errors 55% and
Potential undetected Adverse Drug Experiences (ADE) declined 84%
Bates et al JAMA 1998;280:1311-1316

Transcription ErrorsTranscription Errors
Transcription Error Data Entry Error Verification Error
Vigilance

Transcription Errors - 2Transcription Errors - 2
ConfusionConfusion Over:Over: Drug Names Drug Names or HandwritingHandwriting
Larocin 250 vs. Lanoxin 0.250 (Larocin changed to Larotid after mix-up)
enalapril vs. Elderpryl Lamisil vs. Lamictal

The “Name Game”:The “Name Game”: Risk Management Strategies Risk Management Strategies Select drug names that are not easily
confused with other marketed products: e.g., Losec 50 mg vs. Lasix 50 mg, ultimately Losec changed to Prilosec
Packaging should ddiissttiinngguuiisshh between different dosage strengths of the same drug
Size, shape and color of different dosage strengths of the same product should make it easy to tell the difference

Writing Adequate LabelingWriting Adequate Labeling
Clear Directions for Use Use adjectives and adverbs
carefully, e.g., Rarely, occasionally vs. Frequently, commonly Mild, moderate, severe Frequencies: A few mild rashes
vs. a few cases of aplastic anemia. Can you determine the true incidence?

Use Imprecise “Stock” Use Imprecise “Stock” Statements SparinglyStatements Sparingly
The relationship to the drug The relationship to the drug has not been provenhas not been proven
What if you have a positive What if you have a positive dechallenge/rechallenge?dechallenge/rechallenge?
Use only when the expected Use only when the expected benefit outweighs the potential benefit outweighs the potential riskrisk
Caution should be exercisedCaution should be exercised Long-term & short-term useLong-term & short-term use
Graham, G. Labeling: What Should it Say, and How Should it Say it? Drug Information Journal 1991;25:211-216

Risk Management Strategies to Risk Management Strategies to Minimize the Risk of LitigationMinimize the Risk of Litigation
The Merck Paradigm: Patient took Flexeril
(cyclobenzaprine) with an MAOI and developed NMS
Patient sued for Failure to Warn
Labeling stated, “cyclobenzaprine is closely related to the TCAs, e.g., amitriptyline and imipramine”

Risk Management Strategies to Risk Management Strategies to Minimize the Risk of LitigationMinimize the Risk of Litigation
Labeling also stated, “Flexeril may interact with MAOIs.”*
“Hyperpyretic crisis … and deaths have occurred in patients receiving TCAs and MAOIs”*
Generalizing: Although this ADR has not been reported with this drug, it has been reported to occur with other drugs of the same (pharm/chemical) class.
Your Package Insert
*Benjamin, DM. Case Studies in Pharmaceutical Risk Management, Medical Sciences Bulletin, November 1995.

SummarySummary True safety of a drug usually cannot be
determined until after marketing Stay away from “me-toos” with poorer safety
profiles than already marketed drugs, e.g., bromfenac
Doctors do not read the package insert or Dear Doctor Letters, find another way to warn them (Detailpersons?) to avoid withdrawal from the market
Look for new uses of old drugs, e.g., spironolactone