ASD Surgical Anatomy
15
The Surgical Anatomy of Atrial Septal Defects: Experiences with Repair Under Direct Vision' F. JoHN LEWIS, M.D., MANSUR TAUFIC, M.D., RIcHARD L. VARco, M.D., AND SUAD NiAZI, M.D. Minneapolis, Minnesota From the Department of Surgery, University of Minnesota, MlIinneapolis INTRODUCTION THROUGH USE OF an open repair technic we have become keenly aware of the com- plex anatomy of atrial septal defects. They vary in form, in size, in position, and even in number-two or more may exist in one heart. Other important anomalies may occur in association with them. Yet, atrial septal de- fects conform to a logical pattern. Their anatomical nature and development is un- derstandable if it is explained as an embry- ological growth failure of the complex atrial septal complex25' 28, 31 and the pulmonary veins.7' 9 The classification presented here is based on embryological knowledge but the classi- fication as well as the ideas of surgical anat- omy to be described are a result, primarily, of our experience at the operating table. During operation we have not only palpated these defects; we have seen them in the liv- ing heart as well. To record this experience, some defects were photographed during op- eration, and sketches were made of all im- mediately after the operation. An examina- tion of some rather unsatisfactory fixed specimens from the pathological museum yielded supplementary information. There is nothing new concerning pathological an- atomy in this material. We hope merely to * Presented before the American Surgical Asso- ciation, Philadelphia, Pa., April 27, 1955. This work was supported by Grant Number H-1374 of the U. S. Public Health Service and by grants from the Minnesota Heart Association and the Graduate School of the University of Minnesota. present a rational classification of the de- fects, and to call attention to several impor- tant anatomical features not yet clearly described in the surgical literature. Further- more, we plan to show how most of these defects may be repaired under direct vision, by simple technics. TECHNIC OF HYPOTHERMIA The operations have all been done during hypothermia. The method we have used has been described elsewhere,2-23 so only a brief review of the technic will be given here. After anesthetic induction, the body tem- perature is lowered over a period of one and one-quarter to three and one-half hours by surface cooling. When the body tempera- ture has reached approximately 300 C. the operation is started but the temperature con- tinues to drop, falling to a low point of between 24.50 and 29.5° C. The chest is open with a transverse, sternal splitting inci- sion made through the fourth interspaces bilaterally. Before the cardiac inflow is in- terrupted the heart is explored digitally through the right auricular appendage. Then the cardiac inflow and outflow are occluded, and the right atrium is opened widely to ex- pose the defect. After the defect has been repaired, both the right and left heart are filled with saline and the atrium is closed with a clamp. Circulation is resumed before the atrial wound is sutured. The length of inflow occlusion has ranged from three to seven and three-quarters minutes (median of four and three-quarters minutes). Re- 401
-
Upload
nakatsugawa -
Category
Documents
-
view
41 -
download
2
Transcript of ASD Surgical Anatomy

The Surgical Anatomy of Atrial Septal Defects:Experiences with Repair Under Direct Vision'
F. JoHN LEWIS, M.D., MANSUR TAUFIC, M.D.,RIcHARD L. VARco, M.D., AND SUAD NiAZI, M.D.
Minneapolis, Minnesota
From the Department of Surgery, University of Minnesota, MlIinneapolis
INTRODUCTION
THROUGH USE OF an open repair technicwe have become keenly aware of the com-plex anatomy of atrial septal defects. Theyvary in form, in size, in position, and even innumber-two or more may exist in one heart.Other important anomalies may occur inassociation with them. Yet, atrial septal de-fects conform to a logical pattern. Theiranatomical nature and development is un-derstandable if it is explained as an embry-ological growth failure of the complex atrialseptal complex25' 28, 31 and the pulmonaryveins.7' 9The classification presented here is based
on embryological knowledge but the classi-fication as well as the ideas of surgical anat-omy to be described are a result, primarily,of our experience at the operating table.During operation we have not only palpatedthese defects; we have seen them in the liv-ing heart as well. To record this experience,some defects were photographed during op-eration, and sketches were made of all im-mediately after the operation. An examina-tion of some rather unsatisfactory fixedspecimens from the pathological museumyielded supplementary information. Thereis nothing new concerning pathological an-atomy in this material. We hope merely to
* Presented before the American Surgical Asso-ciation, Philadelphia, Pa., April 27, 1955.
This work was supported by Grant NumberH-1374 of the U. S. Public Health Service and bygrants from the Minnesota Heart Association andthe Graduate School of the University of Minnesota.
present a rational classification of the de-fects, and to call attention to several impor-tant anatomical features not yet clearlydescribed in the surgical literature. Further-more, we plan to show how most of thesedefects may be repaired under direct vision,by simple technics.
TECHNIC OF HYPOTHERMIA
The operations have all been done duringhypothermia. The method we have usedhas been described elsewhere,2-23 so onlya brief review of the technic will be givenhere.
After anesthetic induction, the body tem-perature is lowered over a period of oneand one-quarter to three and one-half hoursby surface cooling. When the body tempera-ture has reached approximately 300 C. theoperation is started but the temperature con-tinues to drop, falling to a low point ofbetween 24.50 and 29.5° C. The chest isopen with a transverse, sternal splitting inci-sion made through the fourth interspacesbilaterally. Before the cardiac inflow is in-terrupted the heart is explored digitallythrough the right auricular appendage. Thenthe cardiac inflow and outflow are occluded,and the right atrium is opened widely to ex-pose the defect. After the defect has beenrepaired, both the right and left heart arefilled with saline and the atrium is closedwith a clamp. Circulation is resumed beforethe atrial wound is sutured. The length ofinflow occlusion has ranged from three toseven and three-quarters minutes (medianof four and three-quarters minutes). Re-
401

LEWIS, TAUFIC, VARCO AND NIAZI
sant..m ItRight Atrium r"
Left Atrium SuperiorVena Cava _
~~~~~~~~~~~~~~~~~~a -'
EndocardialCushion' Inferior. Veno Cava
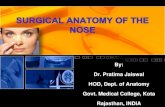
FIG. 1. Semi-diagrammatic illustrations modified after Patten (Am. J. Path., 14: 135, 1938),showing the embryological development of the atrial septum. (A) The septum primum hasalmost reached the endocardial cushion and the ostium secundum has appeared. (B) A later stageillustrating how the septum primum forms the valve of the foramen ovale.
warming is started while the opeiation is inprogress, but after the chest has been closed,it is usually completed by immersing thepatient in hot wvater.
ANATOMY OF THE DEFECTS AND TECHNICS
OF REPAIR
The discussion will follow the classifica-tion of atrial septal defects which is given inTable I. We have operated upon 35 patientswith atrial septal defects, including the per-
sistent common atrioventricular canal, andone patient who doubtless had an atrial sep-
tal defect but whose heart was not opened.Though this is a relatively small number ofcases, we have seen defects of each typelisted in the table.
TABLE I. Defects of the Atrial Septum.
I Foramen Ovale DefectsII High Defects
III Continuous defects of both Foramen Ovale and HighSeptum
IV Low Defects
In every case the atrial septal defect wasthe major anomaly. A number of the defectshave been complicated by mitral valve dis-ease or partial anomalous pulmonary venous
drainage, but none were found in combina-
tion with anatomical pulmonary stenosis,tricuspid atresia, total anomalous pulmonarydrainage, etc. Of course, from a purely ana-tomical point of view the atrial septal com-
ponent of these latter anomalies would prob-ably fit into the classification as well.Though they are important associated de-
formities, the classification holds no specialplace for mitral valve disease or partialanomalous pulmonary venous drainage. Pre-sumably mitral stenosis or insufficiencycould occur with any of the defects. As a
matter of fact, however, we have encoun-
tered mitral valve disease, presumed to berheumatic in origin, only with the Type Idefects, while a congenitally deformedmitral cusp, on the other hand, is appar-
ently a constant feature of the Type IVanomaly. Associated partial anomalous pul-monary venous drainage has been foundwith the first three types, and it seems to bean integral part of the high defect (TypesII and III).
This classification is similar to that ofEdwards and associates,.10 19 but in our
classification non-surgical probe patency ofthe foramen ovale has been omitted, and thehigh defects are listed as a major type ratherthan as part of a poorly defined group called"atrial septal defects in unusual location."
402
Annals of SurgerySeptember, 19 5 5
Septum 1r
1d6

THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTS
Right pulm1l*veins
(Inferior)/
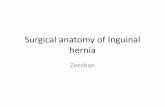
FIG. 2. Figures 2 through 8 depict atrial septal defects from the surgeon's point of view ashe stands on the right side of the supine patient with the patient's head to the left. This is aforamen ovale defect in which the valvula foraminis ovalis is absent. (A) A variation of theforamen ovale defect in which part of the valve remains as a fenestrated membrane.
A. FORAMEN OVALE DEFECTS
Morphologically these defects are basi-cally similar to one another. The structureof this commonest type of atrial septal de-fect-can best be understood by a study ofthe embryological development of the sep-tum. This has been particularly well ex-plained by Patten28 (Fig. 1). The marginsof the clinical defect superiorly, anteriorly,and usually posteriorly are formed by therelatively thick edge of the septum secun-dum, which-normally forms the limbus fora-minis ovalis (Fig. 2). This defect may becaused by a developmental arrest of theseptum secundum, which results in an open-ing too big to be closed by the septum pri-mum. Or the septum primum, which nor-mally forms the valvula foraminis ovaliswithin the oval limits of the limbus, mayhave reabsorbed too far in the process that
creates the normal ostium secundum. Thus,by excessive reabsorption, the septum pri-mum will no longer-form a valve adequateto close the foramen ovalis. This latter proc-ess-excessive reabsorption-seems to be themore important one, for the valvula fora-minis ovalis (septum primum) usually ap-pears to be inadequate. Part of the septumprimum may remain, and when it does itmay form the lower edge of the defect, orin some cases the remaining septum primummay be found as a membrane with numerousperforations (sub-type A, Table II, andFig. 2A). In still other cases it may be pres-ent only as a few thin strands. Finally, theseptum primum may be totally absent in thisarea (sub-type B, Table II, and Fig. 2).When this occurs there is no clear lowermargin of the defect above the orifice ofthe inferior vena cava, and the caudal-wall
403
Volume 142Number 3

LEWIS, TAUFIC, VARCO AND NIAZI Aiuials of SurgerySeptember, 1 9 5 5
- Septal leaflet oftricuspid valve
~-- Coronary- Sinus
alve of l.V.C.INCV.C.
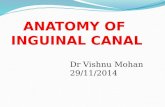
A BFIG. 3. In this foramen ovale defect the valvula foraminis ovalis is absent and the prominentvalve of the inferior vena cava creates a false lower margin. (A) First repair stitch in place. (B)
First repair stitch tied.
of the left atrium then blends imperceptiblyinto the wall -of the right atrium, or into themedial wall of the inferior vena cava at thelower part of the defect.An important variation of this type of
defect-the foramen ovale defect with ab-sence of the septum primum-at least to sur-geons, occurs when a prominent valve ofthe inferior vena cava forms a confusingfalse margin (sub-type C, Table II, andFig. 3). Here the anterior and posterior ex-tremities of the caval valve blend into thetrue edges of the defect. The excellent illus-trations of Licata, which show the appear-ance of the septum in the embryo,25 clarifythe origin of this variation. During a certainperiod of embryonic life the right venousvalve, which ultimately becomes the valveof the inferior vena cava, is so large thatit almost covers the foramen ovale on theright. This valve doubtless regresses incom-
pletely in some cases to produce the varia-tion just described.What this all means to the surgeon is evi-
dent in the illustrations. In the simple fora-men ovale defect, with or without a lowermargin, repair is easy. We have usually em-ployed a continuous stitch of 2-0 silk. If
TABLE II. Foramen Ovale Defects.
No. ofPatients
A. Part of the valvula foraminis ovalis present as afenestrated membrane or caudal margin ..... 14*
B. Valvula foraminis ovalis absent; no lower margin 3C. Valvula foraminis ovalis absent; true margins
continuous with valve of inferior vena cava. . 6t
Total .................................. 23:(3 deaths)
*One patient had a separate anomalous pulmonary veinentering the superior vena cava and another patient had adouble superior vena cava.
tOne patient had an anomalous pulmonary vein enteringthe right atrium.
$Four patients had mitral stenosis.404

Volume 142Number 3
THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTS
Anomalous rightsuperior pulmonary vein
Right inferior pulmonary
AFIG. 4. Usually anomalous pulmonary veins are closely related to the septal defect (Fig. 5),
but in this case the right superior pulmonary vein enters the superior vena cava at a distance fromthe foramen valve defect. (A) The anomalous vein has been transferred to the left side of theheart by means of an end-to-side anastomosis to the inferior pulmonary vein.
there are a number of small holes in a mem-brane at the lower part of the defect (Fig.2A), the whole thing should be closed asone defect. When there is no lower margin,the lowest stitch, consisting of several bites,is placed first. Some of the bites are takenin the lowest part of the left atrial wall. Thisstitch is tied before closing the rest of thedefect. Similarly, the more difficult defect,characterized by a prominent and confusing
caval valve, is closed by first placing thelowermost stitch to the left of the cavalorifice, with some of its bites in the left atrialwall, as is illustrated in Figures 3 A and B.It is obviously quite possible to err and usethe valve of the vena cava in the repair, thusdiverting the inferior vena cava into the leftatrium. This has been done with a blindtechnic of repair,5 but it is an error thatcould be made with an open technic, too.
405

LEWIS, TAUFIC, VARCO AND NIAZI Annals of SurgerySeptember, 19 5 5
"' Foramen ovale defect
A BFIG. 5. High defect in association with a separate, small foramen ovale defect. (A) The firstrepair stitch is placed above the anomalous pulmonary vein. (B) First repair stitch tied.
The right inferior pulmonary vein maydrain directly into the right atrium if theposterior margin of the defect is poorlyformed. In correcting this it is a relativelysimple matter to place the stitches to theright of the vein orifice, and thus direct thepulmonary vein to its proper termination inthe left atrium.
In one case the right superior pulmonaryvein entered the superior vena cava at a dis-tance from the septal defect. Repair of thedefect, and an end-to-side anastomosis, rem-edied the condition (Fig. 4).When mitral valve disease coexists, as it
did in four of the foramen ovale defects, acommissurotomy may be done with the fin-ger inserted through the atrial septal defectinto the left atrium. The degree of mitralstenosis in these cases has been less than
that ordinarily found in uncomplicatedmitral stenosis.
B. HIGH DEFECTS-LOCATED ABOVETHE FOSSA OVALIS
High defects are not a type of foramenovale defect, yet the distinction is not clearlymade in the surgical literature. It is obviousfrom descriptions and illustrations that othersurgeons have encountered these defectsjust as we have.5 14, 15, 26 They have failed,however, to delineate them as a distinct,relatively uniform type with an embryologi-cal origin which must be entirely differentfrom that of either the foramen ovale or thelow defect. We came to an understandingof these defects with a sense of discoveryonly to find that they have been describedby a number of pathologists, anatomists, and
406

THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEV14CTS
NVaIve of I.V.C.
AB
FIG. 6. Large defect which has the characteristics of both a high defect and a foramen ovaledefect. (A) The upper stitch is the same as the first repair stitch of a high defect. The lowerstitch is identical to the first repair stitch of a Type C, foramen ovale defect (Fig. 3). (B) Upperand lower stitches tied.
clinicians whose work dates back as far as1868.1, 2, 8, 12, 13, 17, 18, 35, 36 Usually thesedefects have been set forth as an extremelyrare anomaly, but in our relatively smallseries three were definitely of this type andtwo probably were. It has been at least ascommon as the persistent ostium primum.Located just below the superior vena cava
the high defect has three important charac-teristics. First of all, the defect is above thefossa ovalis and separate from it. Before weknew this we failed to search for the fossaovalis, and therefore failed to identify it intwo patients who doubtless had this defect.
Then, in a third patient, an easily identifiablepatent foramen ovale, independent of thehigh defect, forced us to recognize thenature of the anomaly (Fig. 5). After thiswe looked about more carefully, and found anormal fossa ovalis in both of the last twopatients with high defects. As a second ana-tomical feature, the high defect lacks a com-plete margin. Characteristically there is nomargin superiorly, and an incomplete oneposteriorly. Finally, the defect is regularlyassociated with anomalous drainage of theright superior, and sometimes of the rightmiddle or inferior, pulmonary vein. This fea-
407
Volume 142Nutmber 3

LEWIS, TAUFIC, VARCO AND NIAZI Annals of SurgerySeptember, 1 9 5 a
Septal leaflet oftricuspid valve
-Cleft mitralleaf let
A BFIG. 7. Persistent ostium primum with closed foramen ovale. (A) Repair of this defect employ-ing the lowermost part of the left atrial wall to avoid injuring the conduction system. (B) Firststitch tied.
ture was not always noticed by earlier au-thors perhaps because the hearts they exam-ined were removed from the body withoutthe pulmonary veins and the cavae.36The embryological development of high
defects has not been clearly explained. Thedefect has sometimes been described as anabnormal entry of the superior vena cavainto both the right and left atria rather thanas a defect of the atrial septum.12' 18 Such adescription suggests, of course, that the de-fect represents an anomaly of venousdevelopment rather than an anomaly of theatrial septal complex. In its completed form,however, the defect is in the position of theostium secundum of the septum primum.Normally this ostium is covered by the upper
part of the septum secundum, the septunsperious, and the left sinus valve, so theremust be a failure of the proper attachmentsin this area. A developmental failure herewould almost certainly involve both theatrial septum and the large veins. The arti-cles of Brown and Davis on the development
TABLE III. High Defects.A. Single defects (foramen ovale closed) .......... 4*B. Combined with Separate patent foramen ovale.
Total ............................ 5(no deaths)
*The evidence that these are high defects is direct in two-the closed foramen ovale was identified during surgery. Theother two were earlier cases and we did not look for the fossaovalis.
408

THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTS
imon posterior valve
Common valves are notfused to ventricular septum
FIG. 8. Common atrioventricular canal with small foramen ovale defect. (A) Detail of dorsal,common atrioventricular valve which has been split to show how it is suspended above theventricular septum by numerous small chordae.
of the pulmonary veins help to explain thiscomplicated embryology.7 9
To repair this defect, the first, and mostdifficult, stitch is placed superiorly and thentied down before continuing (Fig. 5 A andB). Properly placed, this stitch directs theright superior pulmonary vein into the leftatrium. The rest of the closure is simple. Insome cases the atrial wall incision has beencarried up into the lower part of the superiorvena cava in order to expose the orifice ofthe superior pulmonary vein. Even with thisextension, repair of the incision has not ob-
structed the vena cava. Some high defectshave been repaired improperly, however.The anomalous pulmonary vein was not
recognized in the first high defect encoun-
tered. This error was not discovered untila catheter was passed into the vein duringpostoperative cardiac catheterization.21 Inanother case the right phrenic nerve was
accidently included in the repair stitches.Neither of these mistakes will be madeagain.The foramen ovale defect was repaired
independently in the one patient who had409
Volume 142Number 3

LEWIS, TAUFIC, VARCO AND NIAZI Annals of SurgerySeptember, 19 5 5
METRICfFIG. 9. A common atrioventricular canal with an additional foranen ovale defect. The hemo-
stat runs beneath the dorsal, common, atrioventricular valve to illustrate the ventricular componentof the defect.
this double defect. Apparently, as will bedescribed in the next section, these two de-fects may occur together as one continuous,large defect instead of two separate defects.C. CONTINUOUS DEFECT OF BOTH THE FORAMEN
OVALE AND THE HIGH SEPTUM-
ABSENT SEPTUM
The appearance and size of one defectled us to call it a continuous combined defectof both the foramen ovale and the high types(Fig. 6). Superiorly it continued into thesuperior vena cava, and posteriorly the pul-monary veins emptied anomalously. Thesefeatures characterize the high defect. In-feriorly, its margins continued into the valveof the inferior vena cava in a way typical ofsome foramen ovale defects. It is possible,of course, that this defect represents simplyan enormous foramen ovale defect, with an
almost complete growth failure of the sep-tum secundum. But the features illustrated,especially the anomalous entry of the pul-monary vein into the superior vena cava,caused us to classify it as a high defect plusa foramen ovale defect.
In any case, surgical repair must combinethe technics used in the high defect, and inone variety of the foramen ovale defect. Byplacing the first two stitches as shown inFigure 6A, a technical problem that seemedformidable at first was satisfactorily solved.Postoperative catheterization studies of thiscase demonstrated that the defect is closed.
This defect may have been called "com-plete absence of the atrial septum" byothers.3' 5, 6, 10, 16, 30 It is also possible thatvery large foramen ovale defects or largeostium primum defects have been labeled,absence of the septum. Of course, in any of
410
k 111, I.A

THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTS
TABLE IV. Low Defects.(Part of persistent, common, atrioventricular canal)
Number
A. Persistent ostium primum; Atrioventricularvalves fused to ventricular septum and mitralvalve notched ............... ............. 3*
B. Common Atrioventricular Canal; primitivevalves usually suspended above ventricularseptum .................................. 3*
*One patient in each group had a separate foramen ovaledefect in addition.
these cases some septal tissue would remain,but in the reported cases of "complete de-fects," too, a rim of septal tissue has beendescribed and so this explanation is notinvalidated.
D. LOW DEFECTS-PART OF PERSISTENT
COMMON ATRIOVENTRICULAR CANAL
Low defects offer a formidable challengeto the surgeon. Some seem at present to beirreparable. Others may be closed surgically,but the incidence of serious postoperativecomplications has been distressingly high.In short, treatment is still unsatisfactory, duein large part to the complicated surgicalanatomy (Figs. 7 and 8).
In order to describe and classify thesedefects we have referred to the terminologyand concepts of Edwards and his associ-ates.'0 11, 19, 31 In some of these defects thepatent ostium primum apparently stands outas the only important deformity, but Ed-wards has shown that all of these low defectshave in common evidence of a persistentcommon atrioventricular canal. In some thiscommon canal may remain as nothing morethan a notching of the mitral valve, but it isstill this feature that draws all of the lowdefects into one group. Within the group twomain sub-types, each presenting differentsurgical problems, can be discerned (TableIV).The defect designated "persistent ostium
primum" in Table IV has been referred to asa septum primum defect. Superficially one
term fits as well as the other, for though theorifice itself is a persistent ostium primum, itis clear that the septum primum in thesehearts fails to fuse with the endocardialcushions and the ventricular septum as itshould. The important developmental errorin the entire group of low defects, however,probably concerns the endocardial cushionsprimarily rather than the septum pri-mum.16, 29, 31 If this type of defect is notactually a defective septum primum, thenthe designation "persistent ostium primum,"which emphasizes the most obvious part ofthe defect without implication concerningits origin, should be preferred.
In the persistent ostium prinium the atrio-ventricular valves are fused to the uppercrest of the ventricular septum. The tri-cuspid valve is usually complete, while theaortic cusp of the mitral is notched or de-formed. Superiorly the two valves have acontinuous surface, but inferiorly they aredivided by the ventricular septum (Fig. 7).The edges of such defects can be stitched
together without great difficulty while theheart is open, but the repair itself oftencauses serious complications. The atrioven-tricular node which lies near the caudaledge of the defect, adjacent to the coronarysinus, may be injured. The three patientsupon whom we have operated all developedcomplete heart block with an idioventricularrhythm. One developed this arrhythmia im-mediately and died suddenly on the thirdpostoperative day. Presumably she died ofcardiac arrest, for autopsy disclosed nocause. The second patient had a temporarycomplete heart block immediately after op-eration, which became permanent one weekthereafter. The third patient did not showcomplete heart block until one month afteroperation, but in her case, too, this arrhyth-mia now seems to be permanent.
In the case of this last patient we made a
careful effort to avoid the conduction sys-tem by placing the stitches as illustrated inFigure 7 A and B. The inferior point of theleft atrium reaches approximately the same
411
Volume 142Number 3

LEWIS, TAUFIC, V
level as the inferior margin of the defect,so that the left atrial wall may easily bebrought into the repair at this dangerousangle. Perhaps this type of repair-furthermodified-will be the answer. It should bepossible to avoid injury to the conductionsystem, but there is still another danger.Both of our surviving patients may havesome mitral insufficiency which was notpresent preoperatively. After encounteringso much trouble in these three patients, weare consoled by knowing that our experi-ence is not unique.4 37The second anomaly in Table IV (illus-
trated in Fig. 8) is even more difficult torepair. Called a common atrioventricularcanal or an incomplete double heart,' itconsists of an ostium primum defect abovetwo primitive atrioventricular valves. Theseventral and dorsal common valves shouldnormally have joined together, and eachshould have developed into part of themitral and the tricuspid valve. Below oneor both of the primitive common valves afree passage between the ventricular cavi-ties is usually found, and it is this additionaldeformity, especially (a ventricular septaldefect), that distinguishes the defect fromthe persistent ostium primum. The primitivevalves of the common atrioventricular canalare suspended above the crest of the ven-tricular septum by numerous chordae (Fig.8A), creating an unusual ventricular septaldefect. To cure the anomaly the entire de-fect, including the ventricular component,must be repaired. This is an appallingproblem.Three patients with this defect have been
operated upon during hypothermia. The firsttwo, one four years old and the other sevenmonths old, were operated upon two yearsago. The preoperative diagnosis was simplyinteratrial septal defect, and we did not,unfortunately, make a correct diagnosis evenduring the operation. This error led in eachcase to a fatal attempt at repair. We did atleast learn how to recognize the defect atoperation, and when to suspect preopera-
'ARCO AND NIAZI Annals of SurgeryARGOANDNIAZI ~~~~~~September. 1955
tively that it might be present. The thirdpatient was operated upon with the correctpresumptive diagnosis and a suture repairwas done, stitching the posterior arch of theatrial component down to the valves, andthe ventricular septum beneath them.Stitches were taken deep through the valvesin order to include the ventricular septum,and thus close the ventricular defect. Nev-ertheless, the entire ventricular componentof the defect was not closed; on top of this,a significant mitral insufficiency was created,and the child did not survive the operation.Figure 9 is a photograph of this defect.
DISCUSSION
OPEN CARDIAC SURGERY
The open technic, employing hypother-mia, is a good technic for repairing atrialseptal defects of the first three types (TableI). Among 29 patients, only three died. Eventhese deaths, in the light of experience, couldhave been prevented, with the possible ex-ception of one which was due to irreversibleventricular fibrillation. This low mortalityrate has been achieved without employingan age limitation for the operation. Eightpatients were over 30, and the oldest, anapparent cure, was 52. The median age was19. If the three patients with ostium primumdefects (Table IV, sub-type A), and the onepatient who did not have a cardiotomy areadded, survival statistics are still good (fourdeaths among 33 patients) . It seems reason-able, when trying to estimate the risk of anoperation for atrial septal defects, to excludethe three patients who had common atrio-ventricular canal defects, for these defectshave a ventricular component.By objective criteria the operation has
made good in the first three types of defect.Twelve patients have had postoperative, car-diac catheterization studies to date, and thedefect was completely closed in all but two.In both of these the shunt is only a fractionof its former value. In one the remainingshunt is due to an anomalous pulmonaryvein which was associated with a high de-
412

THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTS
fect; it was unnoticed at the time of surgery(Type II defect). The other patient with asmall remaining shunt had a large forantenovale defect and mitral stenosis. Except forthe patients with low defects, the survivorshave improved clinically in every case.
VENTRICULAR FIBRILLATION
The most disturbing complication of thistechnic is ventricular fibrillation. It occurredin 11 patients, but with massage, intracardiacadrenalin and electrical shock the heartswere successfully defibrillated in every case
but one. This one was a 39-year-old man
whose heart fibrillated while the chest was
being opened. He was the only patientcooled rapidly in an ice water bath. In one
other patient ventricular fibrillation startedbefore the heart was exposed, but in thenine remaining patients it occurred justbefore, during, or just after the open cardi-otomy.Some experimental evidence has indi-
cated that the addition of C02 to the respira-
tory mixture during cooling might lower theincidence of ventricular fibrillation,27 butwe have been able to test this concept inonly one patient. Despite the fact that shewas a poor operative risk, 31 years old, withmitral stenosis, mitral insufficiency, and con-
gestive failure, ventricular fibrillation didnot occur.
Experimentally, coronary perfusion dur-ing hypothermia has extended the time limitfor inflow occlusion, and it was used in twoof the patients in this series.33 It has not,however, done away with the problem ofventricular fibrillation.
REPAIER OF LOW DEFECTS
Even with the advantages of an opentechnic we have not yet mastered low de-fects. In the persistent ostium primum, re-
pair may injure the conduction system or themitral valve. For the common atrioventricu-lar canal defect, suture repair is even more
troublesome. In all of the low defects stitches
needed for the repair may cause trouble.It would be advisable to do without them.Of course this cannot be accomplished bysimply using a graft or a plastic patch, forstitches are still necessary. We have de-veloped various plastic devices to close ven-tricular septal defects, experimentally atleast, without stitches or with only one
stitch,24' 34 but such devices do not fit intothese low defects.There is still another disconcerting com-
plication. In low defects the scarring whichfollows repair may cause late complications.In the foramen ovale defects and the highdefects there is plenty of room for a scar,but not in the low defects. In these the re-
pair scar may impede valve function, or even
cause late damage to the conduction system.Both patients who survived repair of lowdefects developed complete heart blocksome time after surgery. In one it becamepermanent one week after operation, and inthe other it did not occur until one monththereafter.
MULTIPLE DEFECTS
There is no mystery associated with multi-ple defects of the atrial septum. They do notoccur in random fashion but seem, rather,to be of two general types. The first type issimply an association of either a high or a
low defect with a patent foramen ovale. Thesecond type of multiple defect is merely a
variation of the foramen ovale defect. It isfound when the membranous valve of thefossa ovalis remains either as a perforatedmembrane, or as a number of strands cross-
ing the defect (Fig. 2A). It has been wellillustrated and described by Patten,28 andmuch earlier by Rokitansky.32 The per-
forated foramen ovale defect could, ofcourse, coexist with either a low or highdefect, and conceivably all three principaldefects could occur, isolated from one an-
other, in the same septum, but we have notyet seen or read about such a fantasticpathological cluster.
413
Volume 142Number 3

LEWIS, TAUFIC, VARCO AND NIAZI September, 1955
SUMMARY
1. The surgical anatomy of atrial septaldefects described here is based upon obser-vations made during 35 operations to repairthese defects under direct vision, duringhypothermia.
2. Defects of the atrial septum have beenclassified into four main types: foramenovale defects, high defects, continuous de-fects of both the foramen ovale and the highseptum, and low defects. Partial anomalouspulmonary venous drainage is found occa-sionally with the first type of defect, and itis invariably associated with high defects,in our experience.
3. The first three types of defect, evenwhen complicated, can be satisfactorily re-paired under direct vision by carefullydrawing the true margins together withstitches. Attempts to repair low defects, onthe other hand, have so far been unreward-ing, if not catastrophic. Nonetheless, atleast one category of low defect, the per-sistent ostium primum, should be reparableat the present time.
BIBLIOGRAPHYI Abbott, M. E.: Atlas of Congenital Cardiac Dis-
ease. American Heart Association, New York,1936, p.62.
2 Atkinson, W. J., J. L. Dean, E. H. Kennendelland C. J. Lambertsen: A Multiple Anomalyof the Human Heart and Pulmonary Veins.Anat. Rec., 78: 383, 1940.
3 Bailey, C. P., D. F. Downing, G. Geckeler,W. Likoff, H. Goldberg, J. C. Scott, 0. Jan-ton and H. P. Redondo-Ramirez: CongenitalInteratrial Communications: Clinical andSurgical Considerations With a Descriptionof a New Surgical Technic: Atrio-Septo-Pexy. Ann. Int. Med., 37: 888, 1952.
4 Bailey, C. P., H. T. Nichols, H. E. Bolton,W. L. Jamison and M. Gomez-Almeida:Surgical Treatment of Forty-six InteratrialSeptal Defects by Atrio-Septo-Pexy. Ann.Surg., 140: 805, 1954.
5 Bailey, C. P.: Surgery of the Heart. Lea &Febiger, Philadelphia, 1955, p. 1062.
6 Bedford, D. E., C. Papp and J. Parkinson:
Atrial Septal Defect. Brit. Heart J., 3: 37,1941.
7 Brown, A. J.: The Development of the Pul-monary Vein in the Domestic Cat. Anat.Rec., 7: 299, 1913.
8 Cabot, R. C.: Facts on the Heart. W. B. Saun-ders Co., Philadelphia, 1926, p. 754.
9 Davis, F., and M. A. MacConaill: Cor Bilocu-lare, With a Note on the Development ofthe Pulmonary Veins. J. Anat. 71: 437, 1937.
10 Edwards, J. E.: Congenital Malformations ofthe Heart and Great Vessels. In Gould, S. E.:Pathology of the Heart. C. C. Thomas,Springfield, 1953, p. 266.
Edwards, J. E., T. J. Dry, R. L. Parker, H. B.Burchell, E. H. Wood and A. H. Bulbulian:Congenital Anomalies of the Heart andGreat Vessels. Charles C. Thomas, Spring-field, 1954. p. 202.
12 Geddes, A. C.: Abnormal Superior Vena Cava.Anat. Anz., 41: 449, 1912.
13 Greenfield, WV. S.: A Case of Malformation ofthe Heart, with Large Deficiency in the In-terauricular Septum, Patency of the Fora-men Ovale, and Stenosis of the Aortic Orifice.J. Anat. & Physiol., 24: 423, 1890.
14 Gross, R. E.: The Surgery of Infancy and Child-hood. W. B. Saunders Co., Philadelphia,1953, p. 1000.
15 Gross, E., E. Watkins, Jr., A. Pomeranz andT. Goldsmith: A Method for Surgical Closureof Interauricular Septal Defects. Surg.,Gynec. & Obst., 96: 1, 1953.
16 Gunn, F. C., and J. M. Dieckmann: Malforma-tions of the Heart Including Two Cases WithCommon Atrioventricular Canal and SeptumDefects and One With Defect of the AtrialSeptum. Am. J. Path., 3: 595, 1927.
17 Hepburn, D.: Double Superior Vena Cava,Right Pulmonary Veins Opening Into theRight Auricle, and a Special InterauricularForamen. J. Anat. & Physiol., 21: 438, 1887.
18 Ingalls, N. W.: Report. Communication Be-tween the Right Pulmonary Veins and theSuperior Vena Cava. Anat. Rec., 1: 14, 1907.
19 Kirklin, J. W., H. J. C. Swan, E. H. Wood,H. B. Burchell and J. E. Edwards: Anatomic,Physiologic, and Surgical Considerations inRepair of Interatrial Communications inMan. J. Thoracic Surg., 29: 37, 1955.
20 Lewis, F. J., and M. Taufic: Closure of AtrialSeptal Defects With the Aid of Hypother-mia; Experimental Accomplishments and theReport of One Successful Case. Surgery, 33:52, 1953.
21 Lewis, F. J., R. L. Varco and M. Taufic: Re-pair of Atrial Septal Defects in Man Under
414

Volume 142 THE SURGICAL ANATOMY OF ATRIAL SEPTAL DEFECTSNumber 3
Direct Vision With the Aid of Hypothermia.Surgery, 36: 538, 1954.
22 Lewis, F. J.: Hypothermia in Cardiac and Gen-eral Surgery. Minnesota Med., 38: 77, 1955.
23 .-----: Repair of Atrial Septal Defects Dur-ing Hypothermia. Postgraduate Med., 17:293, 1955.
24 Lewis, F. J., and M. Taufic: The Repair of Ex-perimental Interventricular Septal Defects,During Hypothermia, with a Molded Poly-vinyl Sponge. Surg., Gynec. & Obst., 100:583, 1955.
25 Licata, R. H.: The Human Embryonic Heart inthe Ninth Week. Am. J. Anat., 94: 73, 1954.
26 Muller, W. H., Jr., S. W. Smith, J. F. Dam-mann, Jr., F. H. Adams and M. L. Darsie:Considerations and Physiologic Studies in theClosure of Interauricular Septal Defects.Surgery, 37: 1, 1955.
27 Niazi, S. A., and F. J. Lewis: The Effect ofCarbon Dioxide on Heart-Block and Ven-tricular Fibrillation During Hypothermia inRats and Dogs. Surg. Forum Am. Coll. ofSurg., 1954. In press.
28 Patten, B. M.: Developmental Defects at theForamen Ovale. Am. J. Path., 14: 135, 1938.
29 Robson, G. M.: Congenital Heart Disease. APersistent Ostium Atrioventriculare Com-mune With Septal Defects in a MongolianIdiot. Am. J. Path. 7: 229, 1931.
30 Roesler, H.: Interatrial Septal Defect. Arch.Int. Med., 54: 339, 1934.
31 Rogers, H. M., and J. E. Edwards: IncompleteDivision of the Atrioventricular Canal WithPatent Interatrial Foramen Primum (Per-sistent Common Atrioventricular Ostium).Am. Heart J., 36: 28, 1948.
32 Rokitansky, C. F.: Die Defect der Scheidewandedes Herzens. Wilhelm Braumiiller, Vienna,1875, p. 153.
33 Shumway, N. E., and M. L. Gliedman: Cor-onary Perfusion for Longer Periods of Car-diac Occlusion Under Hypothermia. Pre-sented at Am. Assoc. for Thoracic Surg.Meeting. April, 1955.
34 Taufic, M., and F. J. Lewis: Production andRepair of Experimental Interventricular Sep-tal Defects Under Direct Vision With Aid ofHypothermia. Surg. Forum. American Col-lege of Surgeons, W. B. Saunders Co., Phlia-delphia, 4: 67, 1953.
35 Van Cleave, C. D.: A Multiple Anomaly of theGreat Veins and Interatrial Septum in aHuman Heart. Anat. Rec., 50: 45, 1931.
36 Wagstaffee, W. W.: Two Cases of Free Com-munication Between the Auricles, by Defi-ciency of the Upper Part of the SeptumAuricularum. Tr. Path. Soc. London, 19: 96,1868.
37 Watkins, E., Jr., and R. E. Gross: ExperiencesWith Surgical Repair of Atrial Septal De-fects. Presented at Am. Assoc. for ThoracicSurg. Meeting, April, 1955.
DIscUSSION.-DR. HARus B. SCHUMACKER, JR.,Indianapolis, Indiana: I would like to congratulateDr. Swan and his co-workers, and Dr. Lewis andhis group, upon their very informative and stimu-lating papers.
Dr. Lewis mentioned the problem of the pre-vention of ventricular fibrillation, and I arise pri-marily to tell you briefly of some experiences wehave had in the experimental laboratory with nor-mal dogs.
The situation may not be entirely the same withthe diseased human heart, but it has been possiblefor us to carry out without ventricular fibrillationright ventriculotomies in cooled dogs during com-plete occlusion of venous inflow provided we didone of several things. One is to block the sino-auricu-lar node with procaine. Under such circumstancesthe heart slows remarkably, becomes quite free ofirritability, and the animal seems to be well pro-tected. A second is to perform a sympathetic de-
nervation by removing the upper dorsal and lowercervical sympathetic chain. Finally, although ourwork in this respect is as yet quite preliminary, itseems that the use of the blocking agent, arfonad,accomplishes almost as much as the other methods.All the control animals undergo ventricular fibrilla-tion when right ventriculotomy is carried out in thehypothermic state.
These methods have indeed changed the picturein the experimental animal to this extent, that wehave been able to open the right ventricle andproduce and close ventricular septal defects in afairly large series of animals without mortality.
DR. HENRY T. BAHNSON, Baltimore, Maryland:I can give nothing but compliments to the two pre-ceding speakers, and hope that my comments willnot be taken as a criticism of their papers.
Knowing that Dr. Lewis and others are so wellbracketed by hypothermia, and knowing that all of
415