
Article Control and function of uterine peristalsis during...
14
)iiliiic - Vol 13. No 4. 2006 528-540 Reproductive BioMedicine Online: www.rbmonline.com/Article/2352 on web 20 July 2006 Article Control and function of uterine peristalsis during the huinan luteal phase Georg Kunz worked from 1986 to 2003 at the department of Obstetrics and Gynaecology of the Klinikum Darmstadt, Academic Teaching Hospital, with special interests in the physiology and pathophysiology of human reproduction. Based on immunohistochemical, anatomical, sonographical and MR-imaging studies, he developed the concept of the archimetra and its diseases with Prof. Gerhard Leyendecker. in 1991 he completed his doctorate and in 2001 his residancy, both at the University of Bonn. Since 2003 Dr Kunz has been Head of the Department of Obstetrics and Gynaecology of the St Johannes Hospital in Dortmund, Germany. Dr Georg Kunz G Kunz'\ D Beii^ P Huppert^ G Leyendecker^ 'Department of Obstetrics and Gynaecology of St Johannes Hospital Dortmund, Dortmund; ^Department of Obstetrics and Gynaecology, Academic Teaching Hospital to the Universities of Frankfurt and Heidelberg/Mannheim, Klinikum Darmstadt. Darmstadt, Germany; ^Radiology I, Academic Teaching Hospital to the Universities of Frankfurt and Heidelberg/Mannheim. Klinikum Darmstadt, Darmstadt, Germany ''Correspondence: e-mail: [email protected] Abstract Rhythmic peristaltic contractions of the muscular wall of the non-pregnant uterus can be demonstrated throughout the menstrual eycle. with a maximum just before ovulalion. However, not only during the follicular phase but also during the luteal phase, the utenjs shows remarkable contractile activity. The present study was conducted in order to examine uterine peristaltic activity and its function during the luteal pha,ses of the human menstrual cycle. The results of vaginal sonography of uterine peristalsis, of hysterosalpingoscintigraphy and ofthe documentation ofthe sites of embryo implantation in natural and artificial cycles have shown that uterine peristalsis during the luteal phase is controlled by systemic and probably even more by local hormonal seeretion from the fresh corpus luteum. and facilitates the fundal implantation ofthe blastocyst predominantly ipsilateral to the site of the dominant ovarian structure. Furthermore, this study suggests that the defence against the infiltration and inflammation of the upper genital tract, and thus the degradation of the implanted embryo, represents a further and phylogcnetically old and genuine function of the archimetra. which in placentalia was modified in order to participate in the control of invasion of the endomctrium by the trophoblast. Keywords: embryo transport, implanralion. titerine peristalsis Introduction The non-pregnant uterus is far from a quiescent organ with functions only confined to the preparation ofthe endometrium for blastocyst implantation. It has gained wide acceptance that uterine peristaltic activity, visualized by means of vaginal sonography of uterine peristalsis (VSUP) during the follicuUir phases of the menstrual eyele, provides sustained and directed sperm transport, since radiolabelled albumin macrospheres of sperm size migrated from the vaginal depot through the uterus predominantly into the Fallopian tube ipsilateral to the dominant follicle (Kunz et al.. 1996. 1997; Leyendecker et ai. 1996; Wildt ei al.. 1998). Uterine peristalsis, and thus directed sperm transport during the follicular phases, are controlled by the oestradiol secretion of the dominant follicle systemically and into the utero-ovarian countercurrent system and is enhanced by oxytocin (Kunz et al.. 1998b.c: Wiidt et al.. 1998). Beyond ovulation the uterine peristaltic activity decreases in frequency and intensity, mainly as a eonsequenee ofthe rising progesterone secretion as an inhibitor of uterine contractility, but does not disappear (Lyons ef al., 1991: Leyendecker et ul., 1996; Ayoubi ei al.. 2(X1I; Fanchin et While uterine peristalsis serves directed sperm transport during the mid- and late foil icular phases, the function of luteal phase uterine contractions remains almost unknown. It seems conceivable that in hunKuis uterine peristaltic activity during the luteal phase of the menstrual cycle controls embryo implantation (Kunz et al., 1998a,b). Knowledge is still scanty about how the orientation of the human blastcKyst towards the site of implantation within the uterine cavity is brought about (Harper, 1994). After entering
Transcript of Article Control and function of uterine peristalsis during...

)iiliiic - Vol 13. No 4. 2006 528-540 Reproductive BioMedicine Online: www.rbmonline.com/Article/2352 on web 20 July 2006
Article
Control and function of uterine peristalsisduring the huinan luteal phase
Georg Kunz worked from 1986 to 2003 at the department of Obstetrics and Gynaecology ofthe Klinikum Darmstadt, Academic Teaching Hospital, with special interests in the physiologyand pathophysiology of human reproduction. Based on immunohistochemical, anatomical,sonographical and MR-imaging studies, he developed the concept of the archimetra andits diseases with Prof. Gerhard Leyendecker. in 1991 he completed his doctorate and in2001 his residancy, both at the University of Bonn. Since 2003 Dr Kunz has been Head ofthe Department of Obstetrics and Gynaecology of the St Johannes Hospital in Dortmund,Germany.
Dr Georg Kunz
G Kunz'\ D Beii^ P Huppert^ G Leyendecker^'Department of Obstetrics and Gynaecology of St Johannes Hospital Dortmund, Dortmund; ̂ Department of Obstetricsand Gynaecology, Academic Teaching Hospital to the Universities of Frankfurt and Heidelberg/Mannheim, KlinikumDarmstadt. Darmstadt, Germany; ^Radiology I, Academic Teaching Hospital to the Universities of Frankfurt andHeidelberg/Mannheim. Klinikum Darmstadt, Darmstadt, Germany''Correspondence: e-mail: [email protected]
Abstract
Rhythmic peristaltic contractions of the muscular wall of the non-pregnant uterus can be demonstrated throughout themenstrual eycle. with a maximum just before ovulalion. However, not only during the follicular phase but also during theluteal phase, the utenjs shows remarkable contractile activity. The present study was conducted in order to examine uterineperistaltic activity and its function during the luteal pha,ses of the human menstrual cycle. The results of vaginal sonographyof uterine peristalsis, of hysterosalpingoscintigraphy and ofthe documentation ofthe sites of embryo implantation in naturaland artificial cycles have shown that uterine peristalsis during the luteal phase is controlled by systemic and probably evenmore by local hormonal seeretion from the fresh corpus luteum. and facilitates the fundal implantation ofthe blastocystpredominantly ipsilateral to the site of the dominant ovarian structure. Furthermore, this study suggests that the defenceagainst the infiltration and inflammation of the upper genital tract, and thus the degradation of the implanted embryo,represents a further and phylogcnetically old and genuine function of the archimetra. which in placentalia was modified inorder to participate in the control of invasion of the endomctrium by the trophoblast.
Keywords: embryo transport, implanralion. titerine peristalsis
Introduction
The non-pregnant uterus is far from a quiescent organ withfunctions only confined to the preparation ofthe endometrium forblastocyst implantation. It has gained wide acceptance that uterineperistaltic activity, visualized by means of vaginal sonographyof uterine peristalsis (VSUP) during the follicuUir phases of themenstrual eyele, provides sustained and directed sperm transport,since radiolabelled albumin macrospheres of sperm size migratedfrom the vaginal depot through the uterus predominantly intothe Fallopian tube ipsilateral to the dominant follicle (Kunz etal.. 1996. 1997; Leyendecker et ai. 1996; Wildt ei al.. 1998).Uterine peristalsis, and thus directed sperm transport duringthe follicular phases, are controlled by the oestradiol secretionof the dominant follicle systemically and into the utero-ovarian
countercurrent system and is enhanced by oxytocin (Kunz etal.. 1998b.c: Wiidt et al.. 1998). Beyond ovulation the uterineperistaltic activity decreases in frequency and intensity, mainly asa eonsequenee ofthe rising progesterone secretion as an inhibitorof uterine contractility, but does not disappear (Lyons ef al.,1991: Leyendecker et ul., 1996; Ayoubi ei al.. 2(X1I; Fanchin et
While uterine peristalsis serves directed sperm transport during themid- and late foil icular phases, the function of luteal phase uterinecontractions remains almost unknown. It seems conceivable thatin hunKuis uterine peristaltic activity during the luteal phase ofthe menstrual cycle controls embryo implantation (Kunz et al.,1998a,b). Knowledge is still scanty about how the orientationof the human blastcKyst towards the site of implantation withinthe uterine cavity is brought about (Harper, 1994). After entering

Article - Uterine peristalsis during the human luteal phase - C Kunz et al.
the uterine cavity around 4 days following ovulation, the humanblasttx:yst remains in the high fundal part of the uterus withoutany close contact with the endomctrium for about 2 days (Harper.1994). In many mammals, the orientation ofthe blastocyst is notrandom but species-specific (Lee et al., 1977; Thorbert et al..1978; Stuckhardt ('/«/.. 1981. Pope e/a/,, 1982a,b, 1986; Rogers('/ at.. 1983; Baird and Bimey, 1985; Dziuk. 1985: Rahima andBruce. 1986: von Domarus el al.. 1986: Ugrand et at.. 1987.1989: Wiebold and Becker. 1987: Louton et al.. 1988: Nephewetal.. 1989, 1992).
By means of VSUP. hysterosalpingoscintigraphy fHSSG) andwith the determination ofthe sites of embryo implantation usingvaginal sonography (VS), control and function of luteal phaseuterine peristalsis have been examined. Tlie data provide strongevidence that luteal phase uterine contraction waves are controlledby the dominant corpus luteum and play an important role in thecontrol of hum;in embryo implantation.
Materials and methods .
Patients
A total of 490 healthy women aged 21-46 years (mean 31)with proven fertility (i.e. parous women) or suffering fromandi-ological sterility including 61 women suffering from mostlylow grade endometdosis and infertility (studies 1. 2. 3.4. 7. 8) orwith spontaneously conceived ongoing early pregnancies (study5) or suffering from missed abortions following sptmtaneousconceptions (study 6) entered the studies after giving informedconsent. In all patients in studies 1-4, 7 and 8. lapiiroscopieshad been performed previously and all 490 patients experiencedregular and ovulatory cycles. By means of vaginal sonography,the present menstrual cycle of all patients in studies I, 2, 4, 7and 8 was observed during the follicuku' phases in order todocument normal follicular development and localization as wellas ovulation preceding the luteal phase. The assignment to therespective phases of the menstrual cycles occurred according tothe results of hormone measurements and to the sonographicaldocumentation of the dominant ovarian structure. Furthermore.the site ofthe corpus luteum was documented by means of vaginalsonography (Logiq 3(X): Kranzbiihler, Solingen, Gennany).Women with a history of ovariectomy, uterine fibroids (Gianaroliet al.. 2(X)5). malformations, ectopic pregnancies or irregularmenstrual cycles were excluded from the studies.
Aims of studies
Studies 1-3 examined the patterns of uterine peristalsis underdifferent endocHnologicai situations, especially during the lutealphases of the human menstrual cycle in order to documentdifferences.
The mucus of the uterine cervix during the luteal phase is widelyconsidered as a barrier against the ascension of spermatozoa orother particles ofthe same size. Furthermore, the uterine peristalticactivity subsequent to ovulation appears rather weak. By meansof HSSG as shown in study 4. new insights were gained into thedirected transport capacity provided by uterine peristalsis duringthe luteal phase.
Studies 5S were performed to examine the physiology andpathophysiology of intrauterine migration ofthe human embryoprior to implantation.
Study 1: VSUP in normal cycles
By means of VSUP in 77 healthy women and in 61 womensutTering from mostly low grade endometriosis and infertility,the frequency and pattern ofthe uterine peristaltic activity duringthe menstrual, early-, mid- and late- follicular as well as in themidluteal phases of their cycles (span: day 18 to day 22 of thecycles, mean: day 20) were examined and published by the studygroup (Leyendecker et al.. 1996; Kunz et al.. 1997). The videodiKumentations of uterine peristalsis in this subgroup of patientswere reanalysed. Furthennore. VSUP was performed in fivehealthy women during the late-luteal phases (span: day 25 to day27 of the cycles, mean: day 26) of their regular cycles.
Study 2: VSUP in artificial cycles
Thirteen women received daily, orally administeredvalerate (Progynova ": Sehering AG. Berlin, Gennany) followingpituitary down-regulation with triptorelin (Decapeptyl-Depot'"';Ferring Arzneimittel GmbH. Kiel. Germany) administered duringthe midluteal phase ofthe preceding cycle. Oestradiol valerate wasadministeredat dosesof 4mg for days 1-3. of 6 mg for days 4-9and of 8 mg for days 10-15 in order to prepare the endometriumfor embryo transfer following cryopreservation of pronuclearstage oocytes. Oestradiol valerate administration was reducedto 4 mg for days 16-30. Starting with 2(K) mg of progesterone(Utrogestan*"'; Dr Kade/Besins Phamia GmBH, Berlin, Gennany)in the evening of day 15, 6C)() mg of progesterone per day wasadministered intravaginally on days 16-30.
Vaginal sonography of uterine peristalsis (VSUP) wasperformed on day 22, representing the midluteal phase, and onday 28, representing the late-luteal phase of the artificial cycle,respectively.
The results of the VSUP obtained from the follicular phase havebeen published (Kunz e! al.. 1998c). but the video records werere-analysed.
Study 3: VSUP in stimulated cycles
Twenty women achieved supraphysiological concentrations ofendogenous oestradiol in ovarian stimulation cycles for assistedreproductive technology. These women were treated with humanmcnopausal gonadotrophins (Menogon"; Ferring ArzneimittelGmbH) at mean daily doses of 225 lU of FSH and 225 IU of LHrespectively, following pituitary down-regulation with triptorelin(Decapeptyi-Depot*: Ferring Arzneimitte! GmbH) accordingto the long protocol (Leyendecker et al., 1990), VSUP wasperformed on days +9 and +15 days following the administrationof human chorionic gonadotrophin (HCG. Choragon": FerringGmBH). corresponding to the mid and late-luteal phase in nomialcyeles, respectively. The results of follicular phase uterine activityhave been published (Kunz et at.. 1998c). but the video recordswere reanalysed.

Article - Uterine peristalsis during the human iuteal phase - G Kunz et at.
study 4; hysterosalpingoscintigraphy(HSSG)
Between 1994 and 1996, HSSG was performed in nine womenduring the luteal phases of the regular cycles (between day 18 andday 26 ofthe menstrual cycle, mean day 21 of cycle) accordingto the methods described (Kunz et al., 1996). In addition. HSSGwas performed in 64 women during their follicuiar phases. Theresults of the HSSG obtained from women during the follicuiarphases of the menstrual cycles have been published (Kunz etal.. 1996; Leyendecker ci al.. 1996). For the present study, theHSSG documents obtained from women in the luteal phase werereanalysed.
The ascension ofthe aliquot of labelled albumin macrospheres ofsperm size from the site of application in the dorsal fomix of thevagina through the uterine cavity up to the Fallopian tubes wasdocumented by a gamma camera (Orbiter: Siemens. Eriangen.Germany), providing serial anterior-posterior scintigrams untilthe 32nd minute after application. For assessment of ascension,the genital tract was subdivided into three compartments. Thesite of application was compartment I, the uterine cavity wascompartment 2 and the Fallopian tubes were compartment 3.Regions of interest within compartments were determined and thecounts within each compartment were measured and calculated aspercentage of the total measured radioactivity (for further details,sec Kunz et al., 1996), The patients were advised not to conceiveduring an HSSG cycle and thus no conceptions occurred.
Study 5: early gestational sacs inspontaneous ongoing pregnancies
In 30 healthy women with ongoing single pregnanciesfollowing spontaneous conceptions the localization of the earlygestational sacs within the uterine horns of the high fundal partof the uterus were determined by means of high resolutionvaginal sonography. The localization was then related to the siteof the corpus luteum of pregnancy and described as localizedipsilaterally. centrally or contralaterally. The investigationswere performed between gestational weeks 5 and 7.
Study 6: early gestational sacs inspontaneous missed abortions
By means according to study 5, the localization of thegestational sac in relation to the site of the corpus luteum ofpregnancy was evaluated in 23 healthy women suffering frommissed abortions following spontaneous conceptions. Vaginalscans were performed during weeks 5-8 of gestation. Subjectsexhibiting vaginal bleeding, pelvic pain or opening of theexternal cervical os. or demonstrating myometrial contractionsas obtained by VSUP, were excluded from the study, as well aswomen with multiple pregnancies.
Study 7: early gestational sacs in assistedreproduction cycles with fresh embryotransfer
A total of 118 healthy women entered this prospectively designedstudy. All subjects achieved supraphysiological concentrations
of endogenous oestradio! in ovarian stimulation cycles forartificial reproductive technology as described in study 3. Theembryo transfers were performed 2 days subsequent to (XK'yteretrieval. One to three embryos were transferred into the uterinecavity according to the German Embryo Protection Law. Suipluspronuclei stage oocytes were eryopreserved.
A curved catheter guide (Labotect GmbH, Goningen, Germany)was used for ET. This type of catheter was originally used forperforming transvaginal embryo transfer into the isthmical partof the Fallopian tube (embryonal intra-Fallopian tube transfer,EIFT). TTie curved shape, its markings and its llexibility as wellas the way of insertion allowed placing of the tip of the guidewithin one selected uterine hom. The transfer catheter itself wasintroduced into the guide and surpassed the tip of the guide byabout 5 mm.
The transfer catheter was adjusted and all embryos of eachpatient were transferred alternately either into the left or rightcomuat section of the uterine cavity. In ca.ses of ongoing earlypregnancies between weeks 5 and 7 of gestation with respect tothe day of oocyte retrieval, the localization of the gestational sacswere documented sonographically and related to the left or rightcomual section of the uterine cavity or described as being locatedcentrally by a second investigator, who had had no previousinformation about the primary site of embryo deposition duringembryo transfer.
Study 8: early gestational sacs followingdirected transfer of frozen-thawedembryos in artificial cycles withexogenous steroids
Applying the same means as in study 7, the localization of thegestational sacs following directed transfer of frozen-thawedembryos in artificial cycles with exogenous steroids and withouta dominant ovarian structure in 135 healthy women weredocumented. The sequential administration of oestrogens andgestagens following hypophyseal down-regulation was f)erformedas described in study 2. TTie eryopreserved pronuclei stageoocytes were thawed on day 16 of the cycle and were transterredas described in study 7 on day 17 of the artificial cycle.
Vaginal sonography of uterine peristalsis(VSUP)
VSUP was performed with a 7.5 Mhz probe (Logiq 500;Kranzbiihler. Solingen. Germany) as previously published (Kunz('/ al. 1996; Leyendecker et al., 1996). The probe was placed ina position to yield a sagittal section ofthe whole uterus and waskept in a fixed position over a period of 5 min. The whole scanwas videotaped for quantitative assessment of uterine peristalsis.In order to obtain a gotxl estimation of the frequency of thecontraction waves the tape was replayed at 5 times regular speed.This also allowed the direction of the waves to be determined.Waves starting in the isthmical part ofthe utems and continuouslymigrating to the upper fundal myometriuin wen; described ascervico-fundal or type A contractions, while tyjje B contractionswere fundi>-cervical in direction. If a contraction wave started inthe isthmical part of the uterus but did not surpass the isthmicalregion or lower fundal myometrium it was characterized as

Article - Uterine peristalsis during the human luteal phase • G Kunz et al.
isthmical or type C contraction wave.
Hormone measurements
From each woman, a venous blood sample was drawn for themeasurement of the serum oestradiot. progesterone and LHconcentrations, using acommercially available radioimmunoassaykit (Serono Diagnostics GmBH, Freiburg, Gennany).
Statistical analysis
Statistical analysis was performed using Student's Mest. chi-squared test and determination of the coefficient of correlationand significance was assumed when P < 0.05.
Results
Patients
In all patients in studies 1 and 4, an ovulatory menstrtial cyclecould be documented. The women in studies 3 and 7 experiencedtransvaginal follicular aspiration 36 h after the administration of10,(XX) IU HCG, No follicular development, and thus formationof a corpus luteum, could be observed in the women in studies 2and 8.
The results of studies 1-3 are presented graphically and in tabularform below. Figure I presents serial scintigrams obtained byHSSG from a woman on day 22 of her regular menstrual cycle.Figure 2 depicts the distribution of the percentage of total counts,
Figure 1. Representativescintigrams obtained byh y s t e r o s a l p i n g o s c i n t i -graphy in a single patientduring the midluteal phase.Scintigrams obtained 1 (a),16 (b) and 32 (c) min aftervaginal application of theradioiabelled macrospheresare shown. The fresh corpusluteum was located in theright ovary.
Woman wtth HSSG duringmidluteal phase, n = 9
comp, 1
comp,2
comp. 3 ipsilat.
comp, 3 conlralat.
Time afler application o' labelled albumin macroapheres (min)
Figure 2. The distribution of the percentage of total counts, representing the labelled albumin macrospheres. within the femalegenital tract (compartments 1, 2 and 3 being the upper vagina, the uterine cavity and the isthmical part ofthe tubes, respectively)following 1, 16 and 32 min after vaginal application during the midfollicular (left half) and the midluteal (right halll phases ofthe nomial cycles. With respect to compartment 3, the right and left tubes were differentiated. While the amount of radioactivitytransported into the tubes ipsilateral to the dominant ovarian structure as compared with the contralateral tube was significantlyhigher during the mid-fotlicular phases (P < 0.05), the respective differences just failed significance during the mid-luteal phases.However, an apparent similarity ofthe relative distribution ofthe macrospheres within the uterine compartments between bothgroups of patients can be seen, with an orientation of the inert particles towards the tube ipsilateral to the localization of thedominant ovarian structure also during the mid-luteal phases of the cycles, HSSG = hysterosalpingoscintigraphy.

Article - Uterine peristalsis during the human luteal phase - G Kunz et al.
representing the labelled albumin macrospheres within the femalegenital tract during the midluteal phases ofthe cycles as comparedwith the corresponding results obtained from healthy womenduring the midfollicuiar phases as dtxumented previou.sly (Kunzetal.. 1996; Leyendeckert'/«/.. 1996).
Study 1
The reanalysis of the VSUP during the foilicular phases ofthe menstrual cycles of healthy women and of women withendometriosis confirmed the previously published results (Kunzet al., 1996, 1997; Leyendecker et al., 1996). Uterine peristalsisduring the foliicular phases comprised type A and B contractionwaves, while no type C contractions could be observed. Patientssuffering from endometriosis exhibited significantly increasedperistaltic activity as compared with the healthy controls (patientscharacteristics, apart from the endometriosis, were comparable tothe controls; for details, see Leyendecker et al., 1996). Duringthe late-follicular phase the increased peristaltic activity inwomen suffering from endometriosis attained the character ofdysperistalsis as compared with the healthy women.
However, during the mid- and late-luteal phases, a differentpattern of uterine peristalsis was obtained as compared with theuterine peristaltic activity during the follicular phases, as well ascompared with the results of midluteal phase VSUP as previouslypublished (Figure 3) (Leyendecker et al., 1996; Kunz et al..1997).
Beyond ovulation, type B contractions almost disappeared whileisthmical or type C contractions appeared as a new pattern ofperistaltic activity. During the midluteal phases of the healthywomen, the frequency of type C contractions was significantlyhigher with 2.1 contractions/min (SEM: 0.16) compiired witht.l contractions/min (SEM: 0.14) of type A contractions (P <0.05). Hence the ratio of type C to type A frequency (CA ratio)of contraction waves was 1.9:1. Since almost every contractionobserved during the midluteal phases started in the isthmicalpacemaker region and not in the high fundal myometrium,the relation of 1.9:1 means that roughly every second wavegenerated in the isthmus migrated towards the uterine fundus.During the late luteal phases type C wave frequency was 1.6contractions/min (SEM: 0.17) and type A wave frequency was0.44 contractions/min (SEM: 0.24), therefore increasing the CAratio to a value of 3.6:1. While the decrease in type A activity fromthe mid- to the late-luteal phases was statistically significant (P <0,05), type C uterine peristalsis did not change significantly withthe progression ofthe luteal phases. Further statistic calculationsrevealed a highly significant negative coefficient of correlation oftype C with -0.77 (P < O.(XX)5) and type A contraction frequencieswith -0,6 (P < O.(M)5) with the corresponding oestradiol serumconcentrations during the midluteal phases ofthe healthy women(Table 1). A positive coefficient of correlation existed duringthe late-luteal phases between type C and type A uterine activityand the serum concentrations of oestradiol and progesterone.respectively. While the correlation between serum progesteroneand type C activity was statistically significant (coefficient: 0.93;P < 0.005), the correlation between type C wave frequency andoestradiol concentrations just failed significance (coefficient:0,75, P = 0.06). No significant correlation between type A activityand the serum concentrations of the sex steroids could be obtainedduring the late luteai phases of healthy women.
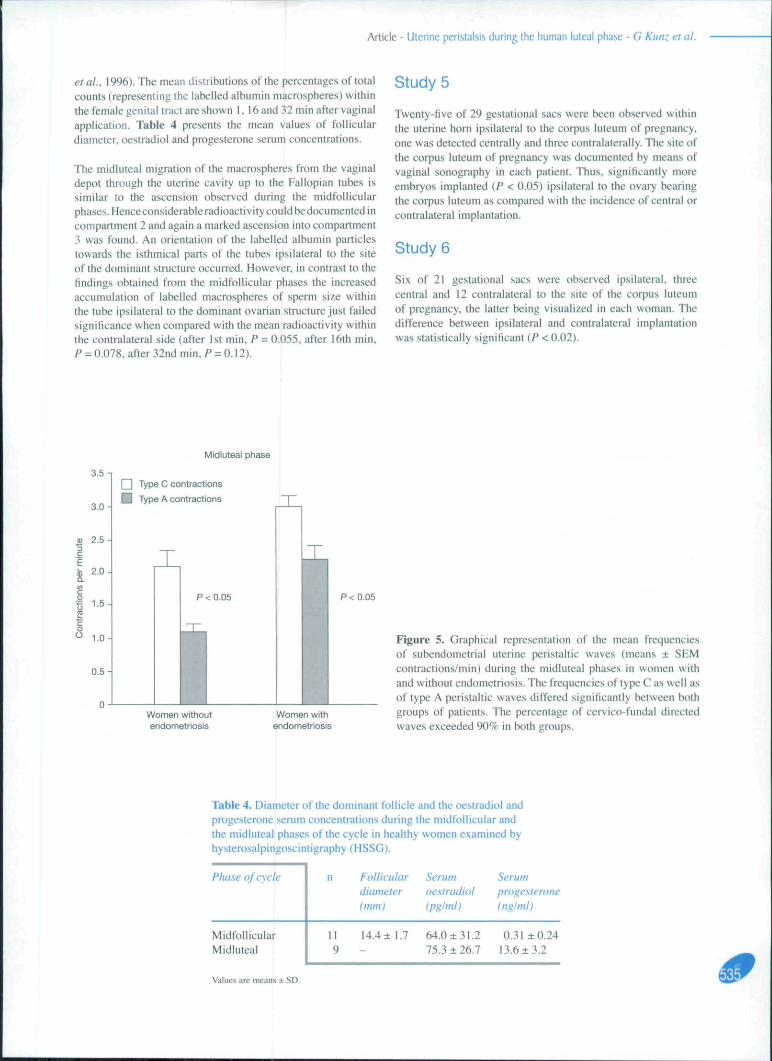
Patients with endometriosis showed a type C frequency of 3,04contractions/min (SEM: 0.16) and a type A frequency of 2.17contractions/min (SEM: 0,21) during the midluteal phases, witha calculated CA ratio of 1.4: I (Figure 4). Furthermore, themean isthmical as well as the mean fundat frequency of uterinecontractile activity differed significantly from the resp>ectivevalues obtained from the healthy control group (P < O.(XK)2).Type A and C contractions prevailed with more than 90% of allwaves. No significant correlations between the particular uterinefrequencies and the serum concentrations of oestradict! andprogesterone could be obtained.
Study 2
Oestradiol valerate and progesterone administration resulted inoestradiol and progesterone serum concentrations similar to thoseofthe normal follicular (Kunz etal.. 1998c) and midlutea! phasesof the menstmal cycle respectively. However, during the late-luteal pha.ses. sex steroid concentrations were mon." than doubledin women receiving exogenous sex steroids as compared with thecontrol (Tabie 2).
Re-analysis of uterine peristaltic activity during the first half ofthe artificial cycles with oestradiol valerate administration only,thus mimicking the follicular phase, showed no differences ascompared with published results (Kunz pr^//.. 1998c).
The frequency of peristaltic waves during the midluteal phasesparalleled those in nonnal cycles with a mean of 2.2 contractions/min (SEM: 0,25) in the isthmicai part (type C) and a mean of Llcontractions/min (SEM: 0.2) in the high fundal part (type A) oftheuterus. The CA ratio could be calculated as 2:1. However, fromthe mid- to the late-luteal phase type C wave frequency decreasednon-signilicantty to 1,9 contractions/min (SEM: 0.16), while typeA activity decreased highly significantly to 0.2 contractions/min(SEM: 0.07) (P < 0.0001). changing the CA ratio to a value of9.7:1.
The only significant coefficient of correlation could be observedduring the midluteal phase with 0.62 between the serximconcentrations of oestradiol and typK C wave activity (P < 0.05).The percentage of type A and C contractions exceeded 95%.
Study 3
The stimulation of ovarian function with human menopausalgonadotrophin (HMG) resulted in supraphysiologicalconcentrations of serum oestradiol and progesterone during thefollicular (Kunz et al., 1998c) and luteal phases of the cycles(Table 3). which differed significantly from those of normalcycles, on the basis of the day of cycle (in study 1) and oi the dayspreceding or following HCG administration (in HMG cycles)respectively.
The reanalysis of uterine peristaltic activity during the follicularphases demonstrated no differences as compared with the resultspublished (Kunz era/., 1998c).
During the midluteal phases of the stimulation cycles, the meanisthmical or type C frequency of uterine contractions was 1.6contractions/min (SEM: 0.26) and 0.7 contractions/min (SEM:0.18) for type A activity revealing a CA ratio of 2.4:1. With

Article - Uterine peristalsis during the human luteal phase - G Kunz et ai
Midluteal phase
3.0-1
2.5-
.= 2.0
2 1.5-
1.0-
0,5-
T
P < 0,05
Type C contractions
Type A contractions
P < 0.05
VSUP ofregular cycles
VSUP oestradiolvalerate andprogesteroneapplication
VSUPHMG application
Figure 3. Graphical representation of the frequency of thesubendometrial uterine peristaltic waves (means ± SEMcontractions/min) during the midluteal phases of normalmenstrual cycles and in women receiving a daily oral doseof oestradiol valerate and progesterone following down-regulation with a gonadotrophin-releasing hormone analogueand in women treated with human menopausal gonadotrophin(HMG) for ovulation induction. The frequency of type A aswell as of type C contractions, the latter comprising uterinecontractions confined to the isthmical and lower fundalpacemaker region of the uterus, was not significantly differentbetween the investigated groups of subjects. The percentage ofcervico-fundal directed waves exceeded 90%. VSUP= vagina!sonography of uterine peristalsis.
Table 1. Diameter of the dominant follicle and oestradiol and progesterone serum concentrations during the menstrualperiod, the early-, mid- and late- follicular phases, and the mid- and late luteal phases ofthe eycle in women with andwithout endometriosis examined by vaginal sonography of uterine peristalsis (VSUP).
Phase of cycle
MenstrualE;yly follicularMidfoliicularLate lbllicularMidlutealLate luteal
No ofwomen
1 814 1322 1710 914 145
Folliculardiameter (mm.)
_ —
<1I.O <ll.O13.9±1.6 14.1 ±1 .218.3 ±1 .4 19.3 ±3 .5- -
-
Serum oestradiol(pg/ml)
36.0 ±31,928,0 ± 12.863.0 ±31.1175,0 ± 106.587.0 ±48.750.0 ± 34.7
40.0 ± 33.836.0 ±21.279.0 ± 38.5180.0 ± 115.9104.0 ±93.0-
Serum progesterone(ng/ml)
0.51 ±0.550.45 ±0.460.35 ± 0.290.89 ± 1.0914.7 ± 3.66.0 ± 2.2
0.31 ±0.230.43 ± 0.120.57 ±0.810,80 ±0.9711.3 ± 6.6-
Values are means ± SD; - and + indicate patieots without and with endometriosis.
t-3te luteal phase
3.0 n
2.5-
E 2.0-
1,5
O1,0-
Type C contractions
Type A contractions
T
P<0.05 P < 0.05 P < 0.05
VSUP otregular cycles
VSUP oestradiolvalerate andprogesteroneapplication
VSUPHMG application
Figure 4. Graphical representation of the frequencies ofthe subendometrial uterine peristaltic waves (means ± SEMcontractions/min) during the late-luteal phases of nonnalmenstrual cycles and in women receiving a daily oral doseof oestradiol vaierate and progesterone following down-regulation with a gonadotrophin-releasing hormone analogueand in women treated with human menopausal gonadotrophin(HMG) for ovulation induction. The mean frequencies of type Ccontractions did not differ statistically from the corresptindingfrequencies observed during the midluteal phases. However,in all groups studied the mean frequencies of type A uterinecontraction waves decreased significantly from the mid- to thelate-luteal phase and were significantly different between theseparate groups of women during the late-luteal phases. Thepercentage of cervico-fundal directed waves exceeded 90%.VSUP= vaginal sonography of uterine peristalsis.

Article - Uterine peristalsis during the human luteal phase - G Kunz et ai
Table 2. Oestradiol and progesterone serum concentrations during the early,mid- and late-follicular phases and during the mid- and late-tuteal phases ofthe cycles in patients investigated with vaginal sonography of uterineperistalsis (VSUP) following oestradiol valerate and progesteroneapplication.
Phaseof cycle
Early follicularVlidfollicularLate follicularVlidlutealLate luteal
No. ofwomen(mm)
1313139
13
Follicular Serumdiameler oestradiol
(pghni)
83 ± 37142 ± 59229 ±188
74 ± 59131 ±95
Serumprogesterone(ng/mt)
0.3 ± 0.30.4 ± 0.350.3 ± 0.25
15.8 ±4.813.5 ±6.3
Values arc means ± SD,
3. Diameter of the dominant follicle and the oestradiol and progesteroneserum concentrations during the early, mid- and late-follicular phases and duringthe mid- and late-luteal phases of the cycles in patients investigated with vaginalsonography of uterine peristalsis (VSUP) following gonadotrophin application.
Phaseof cycle
Early follicularVlidfollicularLate follicularVlidlutealLate luteal
No. ofwomen
2020201212
Folliculardiameter(mm)
<ll13 ± 1.2I9± 1.8
--
Serumoestradiolipg/ml)
119 ±43571±485
1435 ± 11561519± 11711113 ±990
Serumprogesterone(ng/ml)
Not measuredNot measuredNot measured96 ± 1736 ± 30
Values arc means ± SD,
progression to the late-luteal phase, the type C wave frequencydecreased non-significantly to a mean of 1.4 contractions/min(SEM: 0.2). but the frequency of type A contractions decreasedsignificantly to a mean of 0,1 contractions/min (SEM: 0.05, P<0.003) and thus changing the a CA ratio to 20.3:1 (Figure 5).
The only significant coefficient of correlation could be observedduring the midluteal phase, with 0.5 between the serumconcentrations of oestradiol and the type A wave activity (P <0.05). The percentage of type A and C contractions exceeded95%.
Studies 1-3
Only during the late-lutea! phase were the mean frequencies oftype A uterine contraction waves significantly different betweenthe study groups.
However, no significant differences could be observed for themean frequencies of type A waves during the inidluteal phases
and for type C contractile activities during the mid- and late-luteal phases between the study groups 1-3,
In all women studied, the investigators gained the impressionthat each peristaltic contraction lost intensity when approachingthe fundus of the uterine myometrium. as with a wave runningout on a beach. In addition, the intensity of the high fundalor type A contraction waves decreased with the progressionof the luteal phase, as judged subjectively from the extent ofbending of the approximately oval shaped endometrial liningby a contraction wave.
Study 4: HSSG
While Figure 1 presents serial scintigrams obtained by HSSGfrom a woman on day 22 of her regular menstrual cycle. Figure2 depicts the findings of the present study provided by HSSGobtained from the midluteal phases ofthe cycles in comparisonwith the corresponding results previously obtained from HSSGperformed during the midfollicular pha.ses of the cycles (Kunz
Article - Uterine peristalsis during the human luteal phase - G Kunz et al.
et al., 1996). The mean distributions of the percentages of totalcounts (representing the labelled albumin macrospheres) withinthe female genital tract are shown 1. 16 and 32 min after vaginalapplication. Table 4 presents the mean values of follieulardiameter, oestradiol and progesterone serum concentrations.
The midluteal migration of the maerospheres from the vaginaldepot through the uterine cavity up to the Fallopian tubes issimilar to the ascension observed during the tnidfollicularphases. Henceconsiderable radioactivity could be documented incompartment 2 and again a marked ascension into compartment3 was found. An orientation of the labelled albumin particlestowards the isthmical parts of the tubes ipsilateral U) the siteof the dominant structure occurred. However, in contrast to thefindings obtained from the midfolliculjir phases the increasedaccumulation of labelled maerospheres of sperm size withinthe tube ipsilateral to the dominant ovarian structure just failedsignificance when compared with the mean radioactivity withinthe contralateral side (after 1st min, P = 0.055, after !6th min.P = 0.078, after 32nd min, P = 0.12).
I
Study 5
Twenty-five of 29 gestational sacs were been observed withinthe uterine horn ipsilaterai to the corpus luteum of pregnaney,one was detected centrally and three contralaterally. The site ofthe corpus luteum of pregnancy was documented by means ofvaginal sonography In each patient. Thus, significantly moreembryos implanted (P < 0.05) ipsilateral to the ovary bearingthe corpus luteum as eompared with the incidence of central orcontralateral implantation.
Study 6
Six of 21 gestational sacs were observed ipsilateral. threecentral and 12 contralateral to the site of the corpus luteumof pregnancy, the latter being visualized in each woman. Thedifference between ipsilateral and contralateral implantationwas statistically significant (P < 0.02).
Midluteal phase
3.5 n
3.0-
2,5-
2,0-
1-5-
1,0-
0.5-
Type C contractions
Type A contractions
T
P < 0,05
T
T
P < 0.05
Women withoutendometriosis
Women withendometriosis
Figure 5. Graphical representation of the mean frequeneiesof subendometrial uterine peristaltic waves (means ± SEMcontractions/min) during the midluteal phases in women withand without endometriosis. The frequeneies of type C as well asof type A peristaltic waves differed significantly between bothgroups of patients. The percentage of cervico-fundal directedwaves exceeded 90% in both groups.
Table 4. Diameter of the dominant follicle and the oestradiol andprogesterone serum concentrations during the midfollicular andthe midluteal phases of the cycle in healthy women examined byhysterosalpingoscintigraphy (HSSG).
Phase of cycle
MidfollicularMidiuteal
Values are rneyns ± SD,
Folliculardiameter(mm)
Serumoestradiol
Serumprogesteroneinglml)
14.4 ± 1.7 64.0 ±31.275,3 ± 26.7
0.31 ±0.2413.6 ±3.2

Article - Uterine peristalsis during the human luteal phase - G Kunz et al.
study 7
In general, three embryos were transferred (mean 2.8, SD ± 0.5)at the 2-8-cell stage (mean 4.3, SD ± 1.5). Twenty-four of 38gestational sacs in 29 women developed within the uterine horninto which the embryos were transferred primarily. Seven sacswere located centrally and seven contrakiteraily. Signiiicantlymore embryos implanted within the uterine hom into which theywere transferred primarily as compared with the contralateralside (/*< 0.001). All women in this study demonstrated multiplecorpora lutea in both ovaries during the time of embryo transferand the determination of the early gestational sacs.
Study 8
As in study 7, usually three embryos were transferred (mean2.8, SD ± 0.4) at the 2-8-cell stage (mean 2.8, SD ± 1.1). Sevenof 18 gestational sacs were found ipsilaterally, two centrallyand nine contralaterally. There were no statistically sigiiificantdifferences. None of the subjects in study 8 demonstrated afresh corpus luteum.
In all women in studies 5-8. no gestational sacs within the loweror isthmical region of the uterine cavity were observed.
Discussion
Video sonography of uterine peristalsis (VSUP) (Bimholz.1984; Oike et al., 1988; Abramovicz and Archer. 1990; DeVries et al.. 1990; Lyons ei al.. 1991; ijland et at.. 1996;Kunz et al.. 1996; Leyendecker et at.. 1996; Bulletti et ai.2000. 2002; Ayoubi et at., 2(X)I. 2003; de Ziegler et at., 2001;Fanchin et at.. 2(X) I; Ayoubi and Fanchin. 2002; Van Gestcl etai. 2003; Nakai et ai. 2004; Bulletti and dc Ziegler. 2005) andHSSG ([tturalde and Venter, 1981; Becker et ai. 1988; Stecketat.. 1991; Kunz f/a/.. 1996; Leyendecker e/a/., 1996; Wildtet ai. 1998) allow the study of uterine peristaltic activity andutero-tubal transport in Wiv» without stress and injury. Resultsfrom VSUP and HSSG indicated that the non pregnant uterusis far from a quiescent organ and that during the mid- and late-follicular phases of the menstrual cycles the uterine peristalticpump provides directed sperm transport with the preferentialaccumulation of the spermatozoa within the tube ipsilateral toIhc dominant follicle (Kunz et ai. 1996; Leyendecker et ai.1996; Wildt ('/o/., 1998).
Luteal phase subendometrial contraction waves have beendescribed as decreasing in frequency and intensity withthe progression of the secretory phase and as being directedpredominantly from the cervical canal to ihc fundal part of theuterus (Araki. 1982; De Vries et ai. 1990; Oike et ai, 1990;Crane and Martin, 1991; Lyons et ai, 1991; Leyendecker etai. 1996; Bulletti ('( ai. 2000; Van Gestcl el ai. 2003; Nakaiet ai, 2004). However, only scant information exists aboutthe control and function of uterine peristalsis during ihe lutealpha.ses of the human menstrual cycle. With regard to follicularphase uterine peristalsis providing rapid and directed spermtransport {Kunz et ai. 1996), it seems conceivable that uterineperistalsis during the luteal phase might control intrauterinemigration of the preimplantation embryo and eventually thesite of implantation. However, in contrast to the mechanismsof directed sperm transport, luteal phase uterine contractions
encounter additional problems such as tubal regurgitation of theblastocyst or the implantation within lower uterine segmentsof the uterus resulting in placenta praevia or malnutrition ofthe conceptus. Therefore, it .seems very likely that uterineperistaltic activity during the secretory phases differs in manyrespects from follicular phase uterine contractions.
Foilicular phase uterine peristalsis comprises cervico-fundalor type A and fundo-cervical or type B contractiiins (Kunzet ai. 1996; Leyendecker et ai, 1996). This means that eachcontraction wave initially starting in the fundal or istbmical partof the uterus migrates towards the opposite end. The presentstudy has shown ihat in addition to type A and B contractileactivities, a new type of uterine peristaltic contraction appearsduring the luteal phase. It starts like a type A contraction wavebut does not surpass the isthmical and lower fundal part oftheuterus, and is characterized as isthmical or type C contraction.
Although the number of type C contractions per minute did notdecrease significantly from the mid- to the late-lutea! phase inall groups of subjects, the mean frequency of type A contractionssignificantly (P < 0.05) decreased with the progression of thetutcal phase, resembling recent data (l-esny et ai, I998a,b;Fanchin etal.. 2001). This increasingly renders the fundal partofthe uterus a region of relative peristaltic quiescence with theprogression ofthe luteai phase. Since oestradiol stimulates typeA contractile activities (Kunz ('/«/., 1998c). it seems reasonableto assume that progesterone constitutes the preliminary signalfor the inhibition of fundal wave frequency during the lutea!phase ofthe cycle (Ayoubi et ai, 2001). Progesterone has beenshown to reduce myometrial contractility via gcnomic and non-genomic mechanisms (Graham and Clarke, 1997; Revelli c/ti/.,1998), while the application ofthe progesterone antagonist RU486 stimulated uterine contractility during the lutea! phase inthe human (Gemzclt-Danielsson et ai. 1993). Thus the patternof luteal pha.sc uterine peristalsis could be principally mimickedby the sequential exogenous administration of (Estrogen andprogesterone to hypogonadal women.
During the mid- as well as during the late-luteal phases, theprogesterone .serum concentrations in women following HMGadministration were highly significantly increased as comparedwith the women with normal cycles and those hypogonadalwomen with solely exogenous steroid application. In contrast, notuntil the late secretory phase did the comparably high-elevatedprogesterone serum concentrations of those women administeredHMG induce a significantly greater inhibition of type A peristalticactivity as compared with both the other groups of women. Itmight be assumed that a direct inhibition by systemic progesteroneconcentrations on type A peristaltic activity does not developuntil the late-luteal phase presumably due to a delayed and cycle-dependant progesterone receptor formation and activation wiihinthe fundal myometrium. Furthermore, the influence of the utcro-ovarian vascular eountercurrent system on the control of fundaiwave activity should also be emphasized (Einer-Jensen, 1988;Kunz ('/ (//., 1998b). Sex steroids secreted from the fresh corpusluteum into the countercurrent vascular system were found insignificantly higher concentrations in the upper third of the fundalmyometrium as compared with the systemic concentrations (Einer-Jensen. 1988; Hiner-Jensen et ai. 1989; Krzymowski, 1992). Itseems conceivable that in women receiving HMG application(resulting in the development of multiple corpwra lutea in bothovaries) the highly elevated secretion of progesterone into the
Article - Uterine peristalsis during the human luteal phase - G Kunz et ai
countercurrent vascular system as compared with normal cyclesand cycles undergoing exogenous progesterone applicationsignificantly intensified the inhibition of type A peristalsis duringthe late-luteal phase. Vagina to uterus transport by progressivediffusion might also be u.sed for the artificial control of uterineperistaltic activity (Bulletti et al.. 2001). [
Type A as well as type C contractions start within the isthmicalregion, rendering this part of the uterus the prevailingpacemaker during the menstrual cycle. In the present.study, the correlation coefficients between steroid hormoneconcentrations and the uterine peristaltic activities revealedcontroversial data for the difierent groups of subjects as weltas for the phases of the menstrual cycle. However, recentstudies have described oestrogens as the preliminary stimulatorof isthmical pacemaker activity, with the induction of at leasttype A contractions (Rexroad. 1980; Kunz ct ai. 1998c).Since the menstrual period concurs with low serum oestradiolconcentrations, the activity of the isthmical pacemaker duringthe early phases of the menstrual cycle might be temporarilyreduced and partly surpassed by alternative pacemakers ofmainly fundal localization, which are probably governed bydifferent endocrine signals confined to the menstrual period.Presumably, with the development ofthe dominant follicle theincreasing oestradiol concentrations activate the pacetnakerlocalized in the isthmical region of the womb, consequentlyrendering the isthmica! region the prevailing pacemaker of atleast type A myometrial contractions with the progression ofthefbllieular phase. Because the serum oestradiol concentrationsduring the luteai phase still remain elevated as compared withthe serum concentrations obtained during the menstrual period(Table 1), the isthmical region furthermore represents thedomitiant pacemaker region for the induction of type C and Auterine peristaltic contractions. i
As during the pre-ovulatory period (Kunz et at.. 1998c). theisthmical pacemaker during the tuteal phase is characterized bya refractoriness that cannot be surpassed even by the high serumconcentrations of t>estradiol observed in HMG cycles. Thus,type C wave frequency did not differ between the investigatedgroups. However, since in contrast to type A peristalsis type Ccontractions did not decrease significantly with the progressionofthe luteal phase, the activity of the isthmical pacemaker seemsto be only marginally influenced by the serum concentrationsof progesterone. However, as shown by the present study,progesterone-gaining access to the uterus either systemicallyor via the utero-ovarian countercurrent vascular system inhibitscontractility and irritability of the fundal myometrium. As aconsequence, with the progression ofthe luteal phase, contractionwaves continually starting in the isthmical region cannot surpassthe lower fundal myometrium due to the progesterone-inducedrefractoriness of the fundal myometrium.
Videosonography revealed that uterine peristaltic waves of thenon-pregnant uterus are usually confined to the subendometrialmyometrium or archiniyometrium(De \r\esetai. 1990; Lyonsetai. 199l;Kunz£V«/.. 1996; Leyendecker cr((/,. 1996; Fanchinet at., 2001; Van Gestel et ai, 2003). The archimyometrium, asthe innermost of three myometrial layers, surrounds the wholeendometrium and is characterized by a predominantly circulararrangement ofthe muscle fibres (Werth and Grusdcw, 1898;Wetzstein. 1965; Noe et ai, 1999; Kunz et ai. 2000). Unlikethe two outer layers of the myometrium that develop late during
ontogeny and are therefore termed neomyometrium (Werthand Grusdew, 1898). the aniage of the archimyometrium canalready be identified during the first trimester of gestation(hence its denomination). The ontogenetically early formationofthe archimyometrium is pertinent to its function that resultsfrom the fusion of the two paramesonephric ducts and theirmesenchymal elements to form the primordial uterus (Werthand Grusdcw, 1898; Noc et ai. 1999). The bipartition of thecircular subendometrial myomotriuni in the upper part of theuterine corpus and its separate continuation through the cornuainto the respective tubes is the morphological basis of directedsperm transport into the tube ipsilateral to the dominant follicle(Kunz et ai. 1996, 1998b; Noc et ai. 1999). Thus directedpassive transport of sperm (macrospheres) into the 'dominant'tube constitutes a genuine uterine function and results from both,the specific structure of the arcbimyometrium with its fundo-cornual bipartition of the circular fibres (Werth and Grusdew,1898; Noe ei at.. 1999) and the effects of the utero-ovariancounter-current system providing an ipsilaterally increasedinput of hormones from the dominant ovarian structure into theuterine cornual region (Kunz et ai. 1998b).
During the luteal phase, the archimyometrium is still active anddirected, in that inert particles are preferentially transportedinto the tubes ipsilateral to the fresh corpus luteum. However,because the human embryo has a volume and weight manyfold higher than the albumin macrospheres of sperm size usedin HSSG. and due \o the relative quiescence of the fundalmyometrium with the progression of the luteal phase, it hasto be assumed that uterine peristalsis during the secretoryphases does not have the same capacity to transport an embryointo the isthmical parts ofthe tubes as it has to transport inertparticles of sperm size (Kunz et ai. 1996; Leyendecker et at..1996). Nevertheless, the HSSG underlines that the principaldirectionality of the uteritie peristaltic pump as observed duringthe mid- and late-follicular phases (Kunz et ai. 1996) is stillpreserved at least during the midluteal phase of the menstrualcycle.
In animal studies, beads of different sizes were used to examinethe control ofembryo implantation (Pope fTc//., 1986). However,so far as is known, similar studies have never been pedbnnedin humans. The present study gained intriguing insights into thecontrol of human embryo implantation provided by the uterineperistaltic pump.
About 4 days following ovulation. the human embryo entersthe uterine cavity and remains for 2 days without implantation(Harper. 1994), During this time with no adhesive contact withthe underlying endomctrium. the uterus determines the final siteof implantation, which is not random (Harper. 1994), and asobserved in other tnammals. appears to be species-specific (Leeetai. 1977; Thorbert f/«/.. 1978; Stuckhardt <-/«/.. !98l;Popeet ai, I982a.b; Rogers et at.. 1983; Baird and Bimey. 1985;Dziuk, 1985; Pope etat., 1986; Rahima and Bruce, 1986; vonDomarus et at., 1986; Legrand et at.. 1987. 1989; Wieboldand Becker. 1987; Louton ei ai. 1988; Nephew et ai. 1989,1992; Tsutsui et ai. 2002). The present study revealed that inspontaneous singleton pregnancies, the gestational sacs werealmost always located within the uterine horn ipsilaterai to thesite ofthe corpus luteum of pregnancy. These results correspondto previous ob.scrvations (Kawakanii ct ai. 1993). This meansthat after entering the uterine cavity the human preimplantation

Article - Uterine peristalsis during the human luteal phase - G Kunz et al.
embryo usually does not migrate.
The clinical significance of ipsilateral implantation correspondswith the observation that in women suffering from missedabortions following spontaneous conceptions, significantlymore embryos implanted centrally or contralateral to the siteof the corpus luteum of pregnancy, and hence did migrate. Onthe one hand, it might be assumed that failure of luteal phaseuterine peristalsis leads to contralateral implantation resultingin missed abortions. On the other hand, it has been shown thatdelayed implantation subsequent to ovulation and fertilizationincrea,sed the risk of miscarriage in the human (Wilcox ei ai.1999). Since chromosomal anomalies have been describedfrequently in human embryos derived from missed abortions(Qouc etai, \915.Rchder etat.. 1989) it seems conceivable thatchromosomal aberrations in the btastocyst delay implantationand thus increase the rate of migration and consequently theprobability of central or contralateral implantation.
Furthermore, there is compelling evidence that the decreaseof type A contraction waves with the progression of theluteal phase protects the embryo from tubal regurgitation.However, preliminary data have shown that presumably dueto a dysfunction of the uterine peristaltic pump transuterinemigration ofthe primarily intrauterine arrived blastocyst intothe tube contralateral to the site of the corpus luteum mightcontribute to the aetiology of tubal pregnancy in spontaneousconception cycles (Kunz and Leyendecker, unpublished).On the other hand, it has to be assumed that the few type Acontractions also protect the embryo from implantation withinlower uterine regions, which would result in placenta praevia.
However, the corpus luteum controls the site of ipsilateralembryo implantation in the same way as the dominant follicledireets sperm transport into tbe ipsilateral tube (Kunz et at..1996. 1997, 1998b). The fact that following fresh IVF-embryotransport, the embryos again usually do not migrate butdo so following cryopreservation cycles, demonstrates theinfluence of the corpus luteum via the utero-ovarian vascularcountercurrent system (Einer-Jensen, 1988; Kunz et ai, 1998b)on the directional activity of the archimyometrium providingembryo migration and implantation. In cryopreservationcycles, no direct access of endocrine signals from the ovary tothe uterus could cause a gradient of signal expression withinthe fundal myometrium and thus be responsible for directeduterine functions such as providing ipsilateral high fundalembryo implantation. As a consequence, the preimplantalionembryo following embryo transport in cryopreservation cyclesmigrates more frequently than following fresh IVF-embryotransport with multiple corpora lutea in both ovaries providingendocrine signals towards each ipsilateral uterine horn. Howfar increased embryo migration in assisted reproduction cyclesinfluences the rates of conceptions remains to be furtherelucidated. Other studies did not show any correiation betweenthe frequency of mid- and late-luteal phase peristalsis foliowingIVF-embryo transfer and the pregnancy rates as emphasized byothers (Fanchin f/fl/., 1998,2001; Lesnye/(;/., 1998; Ayoubi c-rai. 2003; Kunz and Leyendecker. unpublished). Implantationrates following IVF are also influenced by the type of transfercatheters (Abou-Setta et ai. 2006).
HSSG has further shown that cervical mucus during the lutealphase d(K:s not act as a barrier against the transport of inert
particles, corresponding to a recent study which has shownspermatozoa to be present in the uterine cavity followingvaginal insemination during the luteal phase (Faundes et ai,1981). Therefore, bacteria may be aspirated from the vaginainto the uterine cavity, especially during intercourse, by theperistaltic pump. Thus, a strong antibacterial defence systemmust exist within the upper genital tract in addition to thevaginal defence systetn involving vaginal lactobacilli. MUClis expressed within the uterine and tubal epithelium (Gipsonet ai, 1997) and. following ovulation, there is an influxof bone marrow-derived white cells into the endometrium(Loke and King, 1996; Herbertz. Kunz and Leyendecker,unpublished). The latter is primarily viewed to be involvedin the immunological control of implantation, In view of thepresent results and of those reported in the literature, it may beregarded as a phylogenetically old antibacterial defence systemthat in placental species was modified during the phylogcny ofthe reproductive system in order to control the invasion of theendometriutn by the trophoblast (Hunt and Robertson, 1996;BarratandPockley. 1998).
It has been demonstrated that women suffering fromendometriosis developed uterine hyper- and dysperistalsisthroughout the menstrual cycle (Leyendecker et ai, 1996). Withrespect to the analysis of uterine contractility as peribrmed inthe present study, differentiating into three types of contractionwaves (A. B and C) the VSUP records of those women published(Leyendecker et ai, 1996) were reviewed. The reanalysisof uterine peristalsis confirmed previously obtained data(Leyendecker et ai, 1996). Uterine hyper- and dysperistalsisis a common finding in women suffering from endometriosisand sterility, which could be observed throughout the menstrualcycle. Endometriosis constitutes a disease of the archimetra andhas been described recently in great detail (Leyendecker et ai,1996. 1998. 2006; Kunz ct ai, 2000. 2(K)5),
In conclusion, this study provides insights into the functionand control of uterine peristaltic activity during the lutealphase of the menstrual cycle. The uterine peristaltic pump issignificantly active during the luteal phase of the cycle as shownby HSSG in order to sustain embryo implantation within theuterine honi. Presumably, progesterone secretion from the freshcorpus luteum systemically and into the utero-ovarian vascularcountercurrent system renders the fundo-comual region azone of relative peristaltic quiescence with the progression ofthe luteal phase thus minimizing mechanical irritation of theprocess of implantation and early embryonal growth. However,the data indicate that fundo-cornua! implantation on the sideof the dominant structure as provided by early and midlutealphase uterine peristalsis might be fundamental with respect to asuccessful pregnancy. Hormone secretion from the fresh corpusluteum into the utero-ovarian vascular countercurrent systemconstitutes the preliminary mechanism providing ipsilateralhigh fundal embryo implantation. Increased migration of thepreimplantation embryo tnight result in early pregnancy loss.Furthermore, luteal phase cervical mucus does not act as abarrier against the ascension of spennatozoa and alternativekind of debris such as bacteria; hence an anti-inflammatorydefence system appears to be crucial. There is evidence thatthe antibacterial defence system in piacentalian species wasmodified during the phylogeny of the reproductive systemin order to control the invasion of the endometrium by thetrophoblast.

Article - Uterine peristalsis during the human luteal phase • G Kunz et at.
References
Abou-Setta AM, Mansour RT. Al-Inany HG et al. 2006 Intrauterineinsemination catheters for assisted reproduction: a systematicreview and inoia analysis. Human Reprnduetion (e-pub ahead ofprint on 4 May 2006|.
Abramovicz JS, Areher DF 1990 Uterine endometrial peristalsis - atransvaginal ultrasound study. Fertility ami Steriliry 54. 451—454.
Araki J 1982 Contraction of non-gravid human uterus in variotismenstrual phases. /Nippon Sanka Fujinka Gakkai 7M.\.shi 34,
Ayoubi JM. Fanchin R 2002 Ultrasonographic observation of uterinecontractility. New perspectives. Journal of Reproduction andFertility 41. 204~2\0.
Ayoubi JM. Epiney M, Brioschi M et al. 2003 Comparison of changesin uterine contraction frequency after ovulation in the menstrua!cycle and in in vitro fertilization cycles. Fertility and Sterility- 79.110l-n05.
Ayoubi JM. Fanchin R, Kaddouz D et al. 2(H)I Uterorelaxing effectsof vaginal progesterone: comparison of two methodologies forassessing uterine coniraction frequency on ultrasound scans.Fertility ami Srerility 76, 736-740.
Baird DD. Biniey EC 1985 Bilateral distribution of implantationsites in small mammals of 22 North American species. Journal ofReproduerion ami FenilirylS. 381-392.
Barratt LR. Pockley AG 1998 New {lerspectives onimmunorccognition of gametes and embryos. Sperm survival in thefemale genital tract: presence of immunosuppression or absence ofrecognition? Molecular Hiutmn Reproduetinn 4. 309-317.
Becker W. Steck T. Alber P er«/. 1988 Hystcro-salpingo-scintigraphy:a simple and accurate method of evaluating fallopian tube patency.Niiklcarmedizin 27. 252-257.
Bimholz J 1984 Ultrasonic visualisation of endometrial movements.Fertility ami Srerility 41. 157-158.
Boue J, Bou A, Lazar P 1975 Retrospective and prospectiveepidcmiological studies of 1500 karyotyped spontaneous humanabortions. Teratnloi;y 12. I i-26.
Bulletti C. deZiegler D 2005 Uterine contractility and embryoimplantation. Current Opinion in Obstetrics and Gynecology 17.265-276.
Bulletti C. de Ziegler D. Polli V el al. 2002 Characteristics of uterinecontractility during menses in women with mild to moderateendometriosis. Ferrility mid Sterility 77. IIS6-1161.
Bulletti C. de Ziegler D, dc Moustier B et al. 2001 Uterinecontractility: vaginal administration of the beta-adrenergic agonist.terbutaline. Evidence of direct vagina-to-uterus transport. Annualsof the New York Academy of Sciences 943. 163-171.
Bulletti C. de Ziegler D. Polli V et al. 2000 Uterine contractilityduring the menstrual eycle. Human Reproduelion 15 (suppl. I).81-89.
Crane LH, Martin L 1991 Pace-maker activity in the myometriumof the oestrous rat: in vivo studies using video-Iaparoscopy.Reproducrion Feriility and Development i. 519-527.
De Vries K. Lyons EA. Ballard G ff«/. 1990 Contractions of the innerthird of the myometrium. American Journal of Obstetrics andGynecology 162. 679-682.
DeZieglerD.BuIiettiC. Fanchin Rcf«/. 2001 Contractility of thenon-pregnant uterus: the follicutar phase. Annals of the New YorkAcademy of Science 943, 172-184.
Dziuk P 1985 Effect of migration, distribution and spacing of pigembryos on pregnancy and fetal survival. Journal of Reproduetionand Fertility. Suppl 33. 57-63.
Einer Jensen N 1988 Countercurrent transfer in the ovarian pedicleand its physiological implications. Oxford Reviews of ReproductiveS/o/ofiv 10. 348-381.
Einer-Jensen N. McCracken JA. Schram W et al. 1989 Countercurrent transfer in the female adnex. Acta Fhysiologica Polonica40,3-11.
Fanchin R. Ayoubi JM. Righini C et at. 2001 Uterine contractilitydecreases at the lime of blastocyst transfers. Hunutn Reproduction
16, II15-1119.Fanchin R. Righini C. Oiivennes ? etal. 1998 Uterine contractions
at the time of embryo transfer alter pregnancy rates afier in-vitrofertilization. Human Reproduction 13, 1968-1974.
Faundes A. Montes dc Oca V. Brache V et at. 1981 Sperm migrationat different stages of the menstrual cycle. International Journal ofGynaecology and Obsterrics 19. 361-366.
Gianaroli L. Gordts S. D" Angelo A et at. 2005 Effect of innermynmetrium fibroid on reproductive outcome after IVF.Rcprodiicrive BioMedicine Online 10. 473-^77.
Gemzell Danielsson K, Swahn ML, Bygdeman M 1993 Effect ofantiprogestin. hCG and a prostaglandin analogue on human uterinecontractility. Contraception 47, 295-301.
Gipson IK. Ho SB. Spur Michaud SJ et al. 1997 Mucin genesexpresses by human female reproductive tract epithelia. Biology ofReproduerion 56. 999-1011.
Graham JD. Clarke CL 1997 Physiological action of progesterone intarget tissues. Fndocrine Reviews 18. 502-519.
Harper MJK 1994 Gamete and zygote transport.: In Knobil E. NeillJD (eds). The Physiology of Reproduction. Raven Press. NewYork. pp. 123-187.
Hunt JS. Robertson SA 1996 Uterine ttiacrophages and environmentalprogramming for pregnancy success. Joumal of Reproduction andImmunology a. 1-25.
Ijland MM. Evers JLH. Diniselman GAJ et al. 1996 Endometrialwaveiike movements during the menstrual cycle. Ferlitiry andSteritiry 65. 746-749.
Iturralde M. Venter PP 1981 Hysterosalpingo-radionuclidescintigraphy. Seminars in Nuctear Medicine 11. 301-314.
Kawakami Y. Andoh K. Mizunuma H et al. 1993 Assessment of theimplantation site by transvagina! ultrasonography. Ferrititv andSterility 59. 1003-1006.
Kr7.ymowski T 1992 New pathways in animal reproductivephysiology frontiers and perspectives. Journal of Physiology andPharmacology 43(Supp\. I). 5 - 1 9 .
Kunz G. Beil D. Huppert P et al. 2005 Adenomyosis in endometriosis- prevalence and impact on fertility. Evidence from magneticresonance imaging. Human Reproduction 20. 2309-2316.
Kunz G. Beil D. Huppert P. Leyendecker G 2(HK) Structuralabnormalities of the uterine wall in women with endometriosisand infertility visualized by vaginal sonography and magneticresonance imaging. Human Reproduction 15. 76-82.
Kunz G. Beil D. Leyendecker G 1998a Cervical mucus does not act asa barrier during the lureal phase of the menstrual cycle. Evidencefrom hysterosalpingoscintigraphy (HSSG). Hunum Reproduction13.R-165.
Kunz G. Herbertz M. Noe M. Leyendecker G 1998b Sonographicevidence of a direct impact of the ovarian dominant structure onuterine function during the menstrual cycle. Human ReproductionUpdate 4. 667-672.
Kunz G. Noe M. Herbertz M er al. 1998c Uterine peristalsis during themenstrual cycle. Eftects of oestrogen, antioestrogen and o\yt<x"in.Human Reproducrion Update 4. 647-654.
Kunz G. Beil D. Deininger H et al. 1997 The uterine peristaltic pump.Normal and impeded sperm transptirt within the female genitaltract. In: Well R. Holstein A-F (eds) The fate of the male germ cell.Advances in Experimental. Medicine and Biology 424. 267-277.
Kunz G. Beil D. Deininger H etal. 1996 The dynamics of rapid spermtransport through the female genital tract. Evidence from vaginalsonography of uterine peristalsis (VSUP) and hysterosalpingoscintigraphy (HSSG). Human Reproduction 11. 627-632.
LeeSY. Mossman HW, Mossman AS. del PinoG 1977 Evidence of aspecific nidation site in niminants. American Journat of Anatomy150,631-639.
Legrand C. Banuelos-Nevarez A. Maltier JP 1989 Changes ineleetrical activity of myometrium during intrauterine distributionof rat blastocysts and after prazosin administration. Journal ofReproducrion ami Fertiliry 86. 39-49.
Legrand C. Banueios Nevarez A. Rigolol C. Maltier JP 1987Comparative effects of 6-hydroxydopiimine and alpha-adremxeptorantagonists on intrauterine migration and spacing of blastix:ysts in

Article - Uterine peristalsis during the human luleal phase - G Kiin~. ct al.
the rat. Journal of Reproduction and Fertility ̂ \. 51-58.Usny P. Kiiiicii SR. Tetlow RL etal. t998a Embryo transfer - can
we icarn anything new from the observation of junctionai zonecontraciions? Huniati Reimnlmtiim 13. 1340-1546.
Lesny P, Kiiiick SR, Tellow RL et al. 1998b Uterine junctionai/one contraciions during assisted reproduction cycles. HumanRepniductioii Upctute 4. 440-445.
Leyendecker G, Kunz G. Kissler S. Wildt L 2006 Adenomyosis andreproduction. Be.sl Practice and Research Clitjical Ohstetetric.sand Gynaecology, in press.
Leyendecker G. Kunz G, Noe M et al. 1998 Endomelriosis: adysfunction and disea.se of the archimelra. Human ReproductionUpdate 4. 752-762.
Leyendecker G, Kunz G, Wildt L et al. 1996 Uterine hyperperistalsisand dysperistalsis as dysfunclions of the mechanism of rapidspemi transport in patients with endomelriosis and inlertility.Human Reproduction II, 1542-1551.
Leyendecker G, Bernart W. Bremen T ct al. 1990 Influence oftiic duration of tiie estradiol rise nn the success rate in GnRHanalogue/HMG stimulated IVF cycles. Human Reproduction 5.52-55.
Loke YW, King A 1996 Immunology of human implantation; anevolutionary perspective. Human Reproduction II, 283-286.
Louton T, Domarus H, Hartmann P 1988 The position effect in miceon day 19. Teratology 38,67-74.
Lyons EA. Taylor PJ. Zbeng XH et al. 1991 Cbaraeterisation ofsubendometriai myomeirial contractions throughout the menstrualcyele in normal fertile women. Fertility and Sterility 55. 771 -775.
Nakui A, Togashi K. Kosaka K ct id. 2(X)4 Uterine peristalsis:comparison of transvaginal ultrasound and two different sequencesof cine MR imaging. Journal of Magnetic Resonance Imaging 20.463-169.
Nephew KP, Xie S. Broermann-Ridder DM et al. 1992 Influence ofthe embryo on intrauterine migration in sheep. Journal ofAnitmd.SciemeHt. 1911-1915.
Nephew KP. McClure KE. Pope WF 1989 Embryonic migrationrelative to maternal recognition of pregnajicy in sheep. Journal ofAnimal Science 67. 999-m)5.
NoeM, KunzG, Herberiz M et al. 1999 The cyclic panem of theimmunocytochemical expression of oestrogen and progesteronereceptors in human myometrial and endometrial layers:characterization of the endometrial-subcndometrial unit. HumanReproduction 14. 101-110.
Oike K. Ishihara K. Kikiichi S 1990 A study on the endometrialmovement and senim honnonal level in connection with uterinecontraction, Nippon .Sanka Fujinka Gakkai Zas.shi. 42, 86-92.
Pope WF. Lawyer MS, First NL 1986 Intrauterine migration of theporcine embryo: coordination of bead migration with estradiol.Journal of Animal .Science 63. 848-853.
Pope WF. Maurer RR, Stormshak F 1982a Intrauterine migration ofthe porcine embryo interaction of embryo, uterine iiushings andindomethacin on myometrial function in vitro. Journal of Animal.SrienceSS. 1169-. 1178.
Pope WF. Maurer RR, Stormshak F 1982b Intrauterine migration ofthe porcine embryo: influence of estradiol-17 beta and histamine.Biology of Reproduction 27. .575-579.
Rahima A. Bruce NW 1986 Spacing of conceptuses in the uterinehorn and local effects on fetal and plaeental weights throughoutgestation in the rat. Journal of Reproduction and Fertility 78,741-747.
Rehder H. Coerdt W, Eggers R et al. 1989 Is there a correlationbetween morphological and cytogenetic findings in plaeental tissuefrom early missed abortions? Human Genetics 82. 377-385.
Revelli A, Massobrio M. Tesarik J 1998 Nongenomic iictions ofsteroid hormones in reproductive tissues. Frulorrine ffmews 19,3-17.
Rcxroad CE Jr 1980 Estradiol regulation of the frequency and site oforigin of uterine contractions in ewes. Journal of Animal Science51,1139-1147.
Rogers PA, Murphy CR. Squires KR, MacLennan AH 1983 Effectsof" relaxin on the inlrauterine distribution and antimesometrial
positioning and orientation of rat blast(x:yst.s before implantation.Journal of Reproduction and Fertility 68,431-435.
SteckT.Wurfcl W.Becker W, Albert PJ 1991 Serial scintigraphicimaging for visualization of passive transport pnx:esses in thehuman Fallopian tube. Human Reproduction 6, 1186-1191.
StuckhardtJL, Brunden MN, Harris SB 1981 Influence of intrauterineposition on fetal weight in Dutch belted rabbits. Journal ofToxicology and Environmental Health 8. 777-786.
Thorbert G. Aim P. Owman C et al. 1978 Regional changes instructural and functional integrity of myometrial adrenergie nervesin pregnant guinea-pig, and their relationship to the localisation oft h e c o n c e p t u s . Acta Physiologica Scandinavica 1 0 3 , 1 2 0 - 1 3 1 .
Tsutsui T, Shimizu T, Hori T, Kawakami E 2002 Factors affectingtransuterine migration of canine embryos. Journal of Veterinarianand Medical Science 64. 1117-1121.
Van Gestel I. Ijland MM, Htx>gland HJ, Evers JLH 2003 Endometrialwave-like activity in the non-pregnant uterus. HumanReproduction Update 9. 131-138.
Von Domarus H, Louton T. Lange Wuhlisch F 1986 The positioneffect in mice on day 14. Teratology 34, 73-80.
Wenh R.Grusdew W 1898 Llntersuchungen (iberdie Entwieklungund Morphologie der menschlichen Uterusmuskulaliir. Archiv derGynakologie 55. 325-HJ9.
Wetzstein R 1965 Der Uleru.smuskel: Morphologie. Archives ofGynecology 1^2. 1-13.
Wiebold JL, Becker w e 1987 Inequality in function of the rightand ieft ovaries and uterine hums of the mouse. Journal ofReproduction and Ferlility 79, 125-134.
Wilcox AJ, Baird DD. Weinbcrg CR 1999 Time of implantation ofthe conceptus and loss of pregnancy. New England Journal ofMedicinei4a. 1796-1799.
Wildt L, Kissler S, Licht P et al. 1998 Transpon in the human femalegenital tract and its mtxiulation by oxytocin as assessed by hysterosalpingoscintigraphy, hysiemtonography, electrohysterography andDoppler sonography. Human Reproduction Update 4, 655-666.
Received I? March 2006: refereed 3 April 20()6: accepted 2 Jtme
2(H)6.



















