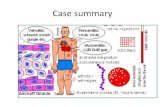
Arthropathyof Wilson's disease - Annals of the Rheumatic Diseases · Wilson's disease, wasfoundin 9...
13
Annals of the Rheumatic Diseases, 1977, 36, 99-111 Arthropathy of Wilson's disease Study of clinical and radiological features in 32 patients D. N. GOLDING AND J. M. WALSHE From Princess Alexandra Hospital, Harlow, and Department ofMedicine, University of Cambridge SUMMARY The principal clinical features and radiological findings relating to the locomotor system have been studied in 32 consecutive hospital admissions of patients with Wilson's disease. 5 of these patients were recently diagnosed and had as yet received no treatment, while 27 were routine admis- sions for follow-up and biochemical supervision of their illness. No patient was specifically included or excluded from the series because of the presence or absence of locomotor symptoms. The most common radiological abnormality was a generalized increase of radiolucency, interpreted as skeletal demineralization (21 cases), followed by premature osteoarthrosis (8 cases). Changes in the spine were common and included osteochondritis, reduction of intervertebral joint spaces, osteoarthrosis, and a tendency to squaring of vertebral bodies. Other bony changes included fluffy irregularity of femoral trochanters, osteochondritis dissecans of the knees, osteophytic protrusions at bone ends, and bunches of tongue-like osteophytes at joint margins. The symptoms associated with these radiological abnormalities comprised back pain and stiffness with restricted movement, pain and stiffness of knees, hips, and wrists, and tenderness to pressure over margins of affected joints. Joint hypermobility was also observed in 9 patients. Episodes of acute polyarthritis with serological changes were seen in 5 cases; all these episodes appeared to be related directly to treatment with penicillamine. Since Warnock (1952) first observed osteoporosis and spontaneous fractures in a patient suffering from Wilson's disease (hepatolenticular degeneration) there have been a number of reports describing various osteoarticular lesions in this condition (Finby and Beam, 1958; Rosenoer and Michell, 1959; Walshe, 1962; Mindelzun et al., 1970; Feller and Schumacher, 1972; Kaklamanis and Spengos, 1973). While certain features such as premature osteoarthrosis with periarticular fragmentation of bone and generalized osteoporosis are recognized as being common in this disease there is marked lack of agreement as to the frequency of other equally distinctive lesions such as osteochondritis, accessory bone ossicles, spontaneous fractures, and vertebral degeneration. To take a particular example, severe rickets was a presenting feature of Wilson's disease years before the onset of neurological symptoms in a case reported by Morgan et al. (1962). Other cases associated with rickets or osteomalacia have been Accepted for publication June 14, 1976 Correspondence to Dr. J. M. Walshe, Department of Medicine, Level 5, Addenbrooke's Hospital, Hills Road, Cambridge CB2 2QQ described by Mehta and Shinde (1965) and by Cavallino and Grossman (1968). One further possible example was reported by Stowers and Dent (1947). The original diagnosis was 'adult Fanconi syndrome with cirrhosis of the liver', Wilson's disease was diagnosed retrospectively by Dent and Stowers (1965) on somewhat tenuous evidence. In an attempt to clarify further the picture of osteoarticular lesions in Wilson's disease it was decided to make a routine study of all cases seen in the course of a year at Addenbrooke's Hospital, Cambridge. Particular attention was paid to the correlation between clinical findings and radio- logical changes, if any, observed either at the time of study or earlier when the patient was first seen. Patients and methods The study comprises 32 patients (16 male and 16 female) seen during the course of a year at Adden- brooke's Hospital, Cambridge. 5 were seen on their first admission for confirmation of diagnosis and management and the remaining 27 during the course 99 on July 23, 2020 by guest. Protected by copyright. http://ard.bmj.com/ Ann Rheum Dis: first published as 10.1136/ard.36.2.99 on 1 April 1977. Downloaded from
Transcript of Arthropathyof Wilson's disease - Annals of the Rheumatic Diseases · Wilson's disease, wasfoundin 9...

Annals of the Rheumatic Diseases, 1977, 36, 99-111
Arthropathy of Wilson's diseaseStudy of clinical and radiological features in 32 patients
D. N. GOLDING AND J. M. WALSHE
From Princess Alexandra Hospital, Harlow, and Department ofMedicine, University ofCambridge
SUMMARY The principal clinical features and radiological findings relating to the locomotor systemhave been studied in 32 consecutive hospital admissions of patients with Wilson's disease. 5 of thesepatients were recently diagnosed and had as yet received no treatment, while 27 were routine admis-sions for follow-up and biochemical supervision of their illness. No patient was specifically includedor excluded from the series because of the presence or absence oflocomotor symptoms.The most common radiological abnormality was a generalized increase ofradiolucency, interpreted
as skeletal demineralization (21 cases), followed by premature osteoarthrosis (8 cases). Changes inthe spine were common and included osteochondritis, reduction of intervertebral joint spaces,osteoarthrosis, and a tendency to squaring of vertebral bodies. Other bony changes included fluffyirregularity of femoral trochanters, osteochondritis dissecans of the knees, osteophytic protrusionsat bone ends, and bunches of tongue-like osteophytes at joint margins.The symptoms associated with these radiological abnormalities comprised back pain and stiffness
with restricted movement, pain and stiffness of knees, hips, and wrists, and tenderness to pressureover margins of affected joints. Joint hypermobility was also observed in 9 patients. Episodes ofacute polyarthritis with serological changes were seen in 5 cases; all these episodes appeared to berelated directly to treatment with penicillamine.
Since Warnock (1952) first observed osteoporosisand spontaneous fractures in a patient suffering fromWilson's disease (hepatolenticular degeneration)there have been a number of reports describingvarious osteoarticular lesions in this condition(Finby and Beam, 1958; Rosenoer and Michell,1959; Walshe, 1962; Mindelzun et al., 1970; Fellerand Schumacher, 1972; Kaklamanis and Spengos,1973). While certain features such as prematureosteoarthrosis with periarticular fragmentation ofbone and generalized osteoporosis are recognizedas being common in this disease there is marked lackof agreement as to the frequency of other equallydistinctive lesions such as osteochondritis, accessorybone ossicles, spontaneous fractures, and vertebraldegeneration. To take a particular example, severerickets was a presenting feature of Wilson's diseaseyears before the onset of neurological symptoms in acase reported by Morgan et al. (1962). Other casesassociated with rickets or osteomalacia have been
Accepted for publication June 14, 1976Correspondence to Dr. J. M. Walshe, Department ofMedicine, Level 5, Addenbrooke's Hospital, Hills Road,Cambridge CB2 2QQ
described by Mehta and Shinde (1965) and byCavallino and Grossman (1968). One furtherpossible example was reported by Stowers andDent (1947). The original diagnosis was 'adultFanconi syndrome with cirrhosis of the liver',Wilson's disease was diagnosed retrospectively byDent and Stowers (1965) on somewhat tenuousevidence.
In an attempt to clarify further the picture ofosteoarticular lesions in Wilson's disease it wasdecided to make a routine study of all cases seen inthe course of a year at Addenbrooke's Hospital,Cambridge. Particular attention was paid to thecorrelation between clinical findings and radio-logical changes, if any, observed either at the time ofstudy or earlier when the patient was first seen.
Patients and methods
The study comprises 32 patients (16 male and 16female) seen during the course of a year at Adden-brooke's Hospital, Cambridge. 5 were seen on theirfirst admission for confirmation of diagnosis andmanagement and the remaining 27 during the course
99
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

100 Golding, Walshe
of follow-up admission for assessment of progressand for biochemical control. No patient was selec-tively included or excluded from the study becauseof the presence or absence of rheumatic symptoms.The patients were examined both clinically andradiologically. Ages ranged from 7 to 45 years(Table 1). Specific questions were asked relating tolocomotor abnormalities, joint stiffness (includingboth morning stiffness and gelling*), pain, swelling,cramps, paraesthesiae, and a family history ofarthritis. In the examination of the locomotor systemattention was paid to abnormal postures andmovements, to the muscles, and to the synovialjoints.
Joint hypermobility was assessed according to thefollowing criteria: dorsiflexion of the wrist to 900,opposition of the thumb to the forearm, hyper-extension of the knee beyond 100, dorsiflexion of theankle >15 degrees beyond the right angle. We alsolooked for abnormalities of the palate, heart, lens,metacarpal index (normal 8), and for homocystine inthe urine.The radiological survey included views of the
spine, hands, wrists, elbows, shoulders, pelvis, knees,ankles, and feet in every case on first visit and, ifdeemed necessary, at the time of assessment. To thisextent the study must be considered retrospective.Thus in assessing osteoporosis we were not able tomeasure bone density systematically as the filmswere taken at different times and with varying viewsand techniques. In our findings we refer to 'loss ofbone density' rather than to the more precise termof osteoporosis.
Other investigations were the latex and Rose-Waaler tests, antinuclear factor, and LE cells,serum proteins and, in a limited number of cases,immunoglobulins. Also serum calcium, phosphorus,and alkaline phosphatase, and 24-hour urinarycalcium excretion. At the earlier visits alkalinephosphatase was estimated in King-Armstrongunits/100 ml, but were later measured in IU/l. InTable 4 results of earlier findings have been convertedto IU but, in view of the difference in technique, noattempt has been made to submit this investigationto statistical analysis.
Results
The principal clinical, rheumatic, serological, andradiological findings for all patients are summarizedin Table 1. Cases 15 and 16 (sibs), 24, 30, and 32were assessed on first referral, all the others werereadmissions.
*By 'gelling' we mean stiffness after immobility in degenera-tive joint disease; this is by no means synonymous with themorning stiffness of active inflammatory joint disease.
CLINICAL FEATURESSymptoms or signs relating to the locomotor systemoccurred in 24 of the 32 patients (75 Y.). The com-monest symptoms were those suggesting mild ormoderate (occasionally severe) premature osteo-arthrosis, that is pain, stiffness, and gelling of theaffected joints. Pain was most frequent in the knees(9 patients) and spine (6 patients). In patients withsymptoms relating to the knees examination usuallyshowed tenderness at the joint margins or on patello-femoral compression and this was associated withcrepitus in 2 cases; occasionally stiffness on passiveflexion and extension was also noted. In the spineextension was the movement most often limited andin 2 patients stiffness of the elbows was associatedwith inability to fully extend the joints. 8 patientshad never complained of joint pains and in these nolocomotor abnormality was found. A correlationbetween these clinical findings and the radiologicalabnormalities is given in Table 2.
Joint hypermobility, not previously recorded inWilson's disease, was found in 9 patients accordingto the criteria listed earlier, but other evidencesuggesting either arachnodactyly or homocystinuriawas not found. Attacks of acute polyarthritis, inmany ways resembling rheumatic fever or acuterheumatoid arthritis, and associated with positiveserological tests for rheumatoid or antinuclearfactor, were seen. These episodes appeared to berelated directly to penicillamine therapy and wereobserved in 5 female patients (Cases 3, 9, 12, 18, 23;Table 1) in this series. As this is not strictly a featureof Wilson's disease it is mentioned here onlybriefly. In 4 of these patients it was possible tocontinue with penicillamine, albeit in a reduced dose,but one (Case 9) suffered a severe recurrence after arest period.No clinical evidence of rickets or osteomalacia
was observed and the plasma calcium, phosphorus,and phosphatase values in no case suggested such adiagnosis, nor did the radiological changes.
RADIOLOGICAL FEATURES (TABLE 3)Bone densityGeneralized loss of bone density was observed intwo-thirds of the patients. It was usually of moderateseverity, being most evident in the hands, feet, andspine and was characterized by radiolucency, corticalthinning, and prominence of the trabecular pattern.There were no radiological features which suggestedosteomalacia (such as concave vertebrae or Looser'slines) nor did we observe changes suggestive of eitheractive or healed rickets. 5 patients had suffered afracture either before or after the diagnosis ofWilson's disease had been made (Cases 12, 13, 17,28, 31); in only one (Case 28) did the history of
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

so02 > > >E > > 9 0
+ >0u 0N 0W 0uZ04 --
tP4 < 4< A ;<0E
a:
_E
C:0 la
E . ea
J)d a
m 11
00._
(7 vD O O ON0C4 en 4 a en
t_ N __ t eq0
_ N en ,I in ID t 00 a,
00 Cd
4) 0- cjla
0 rA.- 0 .. - '- >, .: 0 0 0 0
00 O 0 tlo,4 C.4An -z: O A0 0 O O 02 0 tko .0U2 U) U24.. 02 0 U2 rA0 0 0 Cd 0 ea< 0 4) O 0 00 0 ce I
4) to -W 10> id = 0 U2 04) . 9 N N5 0 0 .=: cdea rAI? ..
..C: E O w =ed E 0 04) > rA 0 rA
cr 1.0) A4
.; o,rA g0w (t:0 4)0 t.4.)rA0 0
-a 20 0N '....- cci4 E
8 2 88 a0 0 0z 0 z
+ ++ 11 11Q; 0; 0 ~~o 0sn *7 0 +A e 7 Z04 04 04 04 0-E>-282= 0=j2^!! I1N'S2;3J2282~0
UV) coQ
>r 4,;> X, O>% 0 ,,2 e~
4) 4 i- u
R8 M i 5 5 Le0 E EU2 ~ ~ ~ ~~ 7a cis
X,Ze 2 EQ2]X xnrA °00.U CdU2 Ut
02X w
&40
.4 1-.. a 11
.- 0 9. . -
rA .- = 0 u
*.- .: Za 0 0 0E - " 0 C'46. to 7-- r. <o ".2C: 4., 0 .
... F...
.0 ol 0 '. w0Cd 4.. a co oN E-4
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

z z0
'0
t;oN
*U-' 0oMt (0
U)a 5 (
CQ ) -
4)
-flU0O
--
4 >
O44
0,
04
>0~ ~~~~
4 0
0\0 75 o c
. -.
a. 0SO00o 0
4)0(U) E
VIOm0" o
0
0,V)
0~~~ ~ ~ ~~~~~)O0 4)D - 4)2
4) o Co
Y 0aIa
0~~~~~~~~>
4)0be la
0
04)
+0vL4)LUc; ;
Xoz z
woz XZXt0 a 'OZ oZ oZ
04 0
>(zU
~~~~~~~~~4)
0 0 0 0
,(a28, a g o d 3g wY 2 Y y i; i y ° 2
I~~~~t Z%fl - r
0. - N
0n ~~Iall
LU,
c-
0
0
0
0
0)0
o..0
00
4)0'0
00.. 04. 0.0 *0.. 4)
.0
.
x
04)
I'l,L.
. IN.9 *t0
_
Q
;ut.0
<5E :2rVu -
:3X0)
4,)I.1.0CHEv
cl.
xc
oooo.
00
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

00N
- 8+ +,Sa P6 4i02 z004 < .
0 0
-Hw I
9
~~~~~~~~-o
*Z1 * ji W Y S j|ti1
inA -
en
-4
V
_ _
t- 00
t-N
1- tl- C14 0 onC4 C4 -4 V -4
in %Ot t- co42S 0 -4 C144 C14 cli C14
tiz,
UA0 OA 0tib 0 o
02 GO00 VA E O v.
0 0a .00 0'002
0
. .:
so .0 $4
oSSXo Xo A W~0 a 0 Sg
i.0q3 eA ie
t-3
:2C3'k.2(3
I-C04
8: 03
.2. s2 11;3 .-Iq "Iol
't. .2ti
A -S
.. Illl.
A~~ ~ ~ ~ ~ ~ ~ ~ A F_ A _ z W > " n 4
na & U3a7 lDj sES E
Sa*-y,garOQlaD lBa}tsc}tl a 3 aE~~~~~~~~~~~~~~~~~~~L
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

> > ;8~~~~~~~~~~~~:
cr r
S , = , >Q~~~>V
ouot z o~~~~~~~tcd
N C . 4
k ~ ~ ~ ~~~~~~~~~~~E 0
t3 0
-, Gz 0D > In 0
l~~~~~~~~~~~X
n~~~~~~~~~~~~~~~~~~~~~ 4)
EvC ° o~~~C o Cd 0
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

Arthropathy of Wilson's disease 105
Fig. 1 Prominent growth lines in the knees ofa13-year-old boy (Case 16).
trauma seem to correspond with the severity of theinjury thus giving further evidence to support thediagnosis of osteoporosis. The patient with perhapsthe most severe loss of bone density, when assessedradiologically (Case 22) had bilateral staghorn renalcalculi and a nonfunctioning right kidney, a state oraffairs suggesting a very severe hypercalciuria atanearlier stage of her illness. Prominent growth lines,bands representing period of arrested growth, were aprominent feature of 3 cases (Fig. 1).
Articular changesPremature osteoarthrosis of the peripheral joints wasnoted in 8 cases, but in only one were the handsinvolved. In Case 10 there was narrowing of thejoint spaces and irregularity of the cortices of themedial metacarpophalangeal joints, changes closelyresembling those seen in haemachromatosis (Fig. 2).Changes involving the hips (Fig. 3) were seen in Cases4, 5, and 8. Osteoarthrosis of the knees was seen in3 patients and osteochondritis dissecans of the samejoints in a further 3. A particularly well markedexample was seen in Case 10 (Fig. 4), an Indian malewho complained of severe pain in the knees severalyears before neurological symptoms indicated thetrue nature of his disease. An appearance radio-logically indistinguishable from Sudeck's (post-traumatic) bone atrophy was seen in one knee jointin Case 24, a 22-year-old male suffering fromadvanced Wilson's disease with severe dystonia andflexion contractures of the arms and legs.
Changes in the spineSix patients complained of spinal stiffness orbackache. Changes resembling those of spinalosteochondritis, well marked Schmorl's nodes withan occasional tendency to wedging of the vertebralbodies, or irregularity of the contiguous surfaces,were seen in 5 patients. In Case 17 several radio-graphs taken in childhood had shown Schmorl'snodes (Fig. 5) before the diagnosis of Wilson'sdisease was established. Premature spinal osteo.arthrosis was striking in a 32-year-old man who hadwidespread anterior spondylosis though he had no
Fig. 2 Premature degenerative changesin the metacarpophalangeal joints, mostmarked distally (Case 10).
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

106 Golding, Walshe
Table 2 Correlation of rheumatic symptoms and radiologicalfeatures
Rheumatic features Radiological features Case no.
Pain/stiffness of knees Premature osteoarthrosis 4, 5, 12(9 patients) Osteochondritis dissecans 10, 26, 31
Normal x-ray 14, 19, 20Pain/stiffness of spine Vertebral squaring 4
(6 patients) Osteochondritis 7, 12, 17, 19Normal x-ray 3
Pain/stiffness of hips Premature osteoarthrosis 2(2 patients) Fluffy periostitis of trochanter 5
Wrist pain Chondrocalcinosis/bone fragmentation 5(2 patients) Normal x-ray 21
Pain in feet/ankles Normal x-ray 8(1 patient)
Hypermobility 1, 9, 11, 12, 14, 16,(9 patients) 20, 26, 30
Table 3 Radiological features in 32 patients withWilson's disease
No. ofpatients
Generalized osteoporosis 21Prominent growth (Harris's )lines 3Premature osteoarthrosis (peripheral joints) 8Osteochondritis of spine 5Reduction of intervertebral disc spaces 4Osteoarthrosis of spine 3Fluffy irregularities of femoral trochanters 4Osteochondritis dissecans of knees 3Tendency to squaring of vertebrae 4Tongue-like osteophytic protrusions at bone ends 2
Fig. 3 Loss of medial joint space of hips, earlyosteoarthrotic changes (Case 8).
corresponding symptoms. A tendency to squaring ofthe vertebral bodies (that is, increase in the height ofthe vertebrae without a corresponding increase inthe anteroposterior diameter and with loss of theanterior concavity) was seen in some patients. This
Fig. 4 Large erosions (osteochondritis dissecans in themedial tibial condyles ofboth knees (Case 10).
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

Arthropathy of Wilson's disease 107
Table 4 Plasma calcium, inorganic phosphorus, alkaline phosphatase, and 24-hour urine calcium excretion(mean±SE)
Mean age Plasma Ca Plasma P Alkaline phosphatase Urine Ca(years) (nmol/l) (nmol/l) (lU/i) (nmol/24 h)
1st visit (32 patients*) 17-1 2-40±0-04 1-20±0-05 35±14 74-7±8-7Time of assessment (32 patients*) 23-1 2-35±0 02 1-20±0-05 74±8 50-1 ±8-0Significance <0-05 <0-05 <0.05
*As the 5 new patients were seen only once their findings are included in both sets of findings.
Table 5 Frequency of radiographic abnormalities in phosphorus, and alkaline phosphatase difficult asvarious joints higher levels for these parameters would be expected
No. of instances during periods of active growth. Values suggestingrickets or osteomalacia were not recorded but
Hands and wristsIrregularity of articular surfaces ofMCP joints 1? chondrocalcinosis, ? subchondral bone 1fragmentations
ElbowsTongue-like osteophytic protrusions 1SpineOsteochondritis 5Anterior spondylosis 3Reduction of intervertebral disc spaces 4Vertebral squaring 4....HipsDegenerative changes 4Fluffy irregularity of trochanters 4KneesDegenerative changes 3Osteochondritisdissecans3Erosion of lateral borders of patellae 1Appearances resembling Sudeck's atrophy 1Ankles, heels, and feetTongue-like osteophytic protrusions 1Fluffy (compound) calcaneal spurs I
appearance closely resembles the vertebral squaringseen in ankylosing spondylitis. Another occasionalfinding was narrowing of the intervertebral discspaces, here illustrated in a 12-year-old girl (Fig. 6).
Other changesA distinctive radiological change seen in 4 patientswas a fluffy appearance of the femoral trochanters,probably representing periosteal reactions at tendoninsertions (Fig. 7).
Tongue-like osteophytic protrusions from bonyprominences were seen at the elbows in one patient(Case 5) (Fig. 8) and at the ankles in another (Case25). This patient also had bilateral fluffy calcanealplantar spurs of the compound variety (Fig. 9). Thechanges at the elbows in Case 5 resembled a bunch ofbananas growing from the lateral humeral epicondyleand olecranon. It is uncertain whether the opacitiesseen in the wrists of this patient represent chondro-calcinosis or subchondral bone fragmentation, noother similar examplewas seen (Fig. 10). The findingsare summarized in Table 5.
BIOCHEMICAL FINDINGSThe widespread age range, from 7 to 45 years, makes Fig. 5 Multiple Schmorl's nodes in thoracic and lumbarinterpretation of the plasma levels of calcium, spine in a 13-year-old boy (Case 17).
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

108 Golding, Walshe
Fig. 7 Fluffy irregularities (periostitis ?) of lessertrochanters in a 30-year-old man (Case 8).
Fig. 6 Narrowing ofL5-SJ intervertebraldisc space in a12-year-old girl (Case18).
urinary calcium values, on a normal ward diet,tended to be high on the initial visit and lower whenseen for reassessment, but the difference was notsignificant (Table 4).
SEROLOGICAL CHANGESThe Rose-Waaler test was strongly positive in 3patients and antinuclear factor positive (titre >1/80)in 5 patients at some time. These serological abnor-malities were thought to be related to penicillaminetherapy and were not seen in any patients beforetreatment was given. Immunoelectrophoresis ofserum proteins, carried out on sera from 6 patients,was normal.
Discussion
As in earlier reports we found premature osteo-arthrosis to be a frequent feature in our patients.Usually of mild or moderate degree, the degenera-tive changes were on occasions severe and could be
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

Arthropathy of Wilson's disease 109
Fig. 8 Small tongue-like osteophytesprotruding from lateral epidondyle andolecranon (right elbow) (Case 5).
Fig. 9 Bilateral fluffy calcaneal spurs of 'compound'appearance (Case 25).
associated with disabling symptoms. Unlike thearthropathy of haemochromatosis, the larger jointsand spine are mainly affected in Wilson's disease.It is interesting though that in one of our patientsdegenerative changes were found involving themedial metacarpophalangeal joints similar to thechanges reported by Hamilton et al. (1968) in
haemochromatosis. Effusions of the knee joints, asreported by Kaklamanis and Spengos (1973) werenot seen in this series. These workers reported findinga noninflammatory exudate on aspiration of thejoint but punch biopsies of the knee in 7 casesshowed microvillus formation, vascular changes,and infiltration with chronic inflammatory cells.Chondrocalcinosis of the joints (Boudin and Pepin,1959; Feller and Schumacher, 1972) was seen in thewrist joints of one of our patients though it ispossible that the changes represented bone fragmen-tation as previously described (Finby and Bearn,1958).There seems little doubt that of the other radio-
logical abnormalities found in patients with Wilson'sdisease, generalized loss of bone density, mostobvious in the hands, feet, and spine, does occur inthe majority of patients and is further testified to bythe high incidence of fractures noted in the presentseries, 5 in 32 cases. The loss of bone densityprobably results from the loss of calcium andphosphorus in the urine (Bearn et al., 1957; Lancet,1962). Rickets or osteomalacia was described byFinby and Bearn in a quarter of their patients (7 outof 27), though the evidence for the diagnosis seemsless than complete in 4. The Fanconi syndrome hasalso been reported in Wilson's disease by Morganet al. (1962) and, in a less well documented case byDent and Stowers (1965). We have not seen thisclinical syndrome which must be a rare accompani-ment of this disease.
U
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

110 Golding, Walshe
Fig. 10 Opacities in the right wrist joint: ? chondrocal-cinosis, ? subchondral bone fragmentation (Case 5).
It also appears that Schmorl's nodes and otherchanges of osteochrondritis of the spine are arelatively common feature of Wilson's disease,although it must be remembered that these arechanges frequently seen in the spines of adolescentsand men and women in their twenties. However, asRosenoer and Michell (1959) pointed out, the usualregions of the spine affected in Wilson's disease,mid-dorsal and lumbar, are not those typical ofScheuermann's disease. Osteochondritis dissecanshas also been described previously (Rosenoer andMichell, 1959; Walshe, 1962; Mindelzun et al.,1970; Kalkamanis and Spengos, 1973). Althoughusually in the knees, this condition affected themedial aspect of the talus in one of Rosenoer andMichell's patients. The finding of periostitis attendon attachments causing a fluffy irregular appear-ance of the trochanters does not seem to have beenmentioned previously in the literature. This may be aperiosteal reaction of a type similar to that occurringin some cases of psoriatic arthritis and Reiter'sdisease, with which may be associated localizedepisodes ofpain (Case 5).
Other features we have noted are small groups oftongue-like osteophytes protruding from bone endsand squaring of the vertebral bodies giving anappearance similar to that seen in ankylosingspondylitis. It is possible that some of these abnor-malities may result from a direct toxic action ofcopper on the chondroblasts at the epiphyses and in
the intra-articular cartilages. In this connection it isof interest that the urinary peptides of Wilson'sdisease, the significance of which has long been astanding source of controversy, have recently beencharacterized and shown to be proline-containingpeptides derived from the skeleton and indicative ofexcess breakdown in this tissue (Asatoor et al., 1976).
It appears, from our observations, that Wilson'sdisease can now be added to the list of conditionsknown to be associated with joint hypermobility(hypermobility syndrome). Whether this is due tometabolic changes affecting the ligaments such asoccurs in homocystinuria, or else perhaps a featureby patients with the Wilson's disease gene in doubledose, is a matter for conjecture. One possibility isthat hypermobility may be induced by penicillaminetherapy, as collagen formed under the influence ofthis drug lacks normal tensile strength due todisruption of cross linkages (Morris et al., 1969).However, hypermobility was present in 2 patientsbefore penicillamine therapy was started. Ashypermobile joints predispose to early osteoarthrosis,this may represent one of the mechanisms leading tothe degenerative joint changes commonly seen inpatients with this disease.There have been anumber of reports of acute poly-
arthritis or a lupus-like syndrome occurring as a resultof penicillamine therapy (Harpey et al., 1974) andreversed by drug withdrawal. In 1968 one of us(J.M.W.) reported 2 such cases, one of which is in-cluded in the present series (Case 18). Arthralgia,fever, pericarditis, pleurisy, and nephritis with LE cellsin the blood and a positive test for antinuclear factorhave been recorded in patients given penicillamine forWilson's disease and for cystinuria (Boudin et al.,1971; Rassmussen, 1971; Oliver et al., 1972). Poly-arthritis, apparently related to treatment with penicil-lamine has been observed in 5 female patients in thepresent series, but as these changes are secondary totreatment and do not result directly in Wilson'sdisease, they will not be discussed further.
ReferencesAsatoor, A. M., Milne, M. D., and Walshe, J. M. (1976).
Urinary excretion of peptides and hydroxyproline inWilson's disease. Clinical Science and Molecular Medicine,51, 369-378.
Beam, A. G., Yu, T. F., and Gutman, A. B. Y. (1957). Renalfunction in Wilson's disease. Journal of Clinical Investiga-tion, 36, 1107-1114.
Boudin, G., and Ppin, B. (1959). DeJgeJn6rescence Hepato-Lenticulare. Masson, Paris.
Boudin, G., Pepin, B., Godeau, P., Vernant, J-C., andGoueron, H. (1971). Lupus 6ryth6mateux induit par lap6nicillamine au cours d'une maladie de Wilson. Annalesde Medecine Interne, 122, 269-273.
Cavallino, R., and Grossman, H. (1968). Wilson's diseasepresenting with rickets. Radiology, 90, 493-494.
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from

Arthropathy of Wilson's disease 111
Dent, C. E., and Stowers, J. M. (1965). Adult Fanconisyndrome and cirrhosis. (Letter.) British Medical Journal,1,520.
Feller, E. R., and Schumacher, H. R. (1972). Osteoarticularchanges in Wilson's disease. Arthritis and Rheumatism, 15,259-266.
Finby, N., and Beam, A. G. (1958). Roentgenographicabnormalities of the skeletal system in Wilson's disease(hepatolenticular degeneration). American Journal ofRoentgenology, Radium Therapy, and Nuclear Medicine,79,603-611.
Hamilton, E., Williams, R., Barlow, K. A., and Smith, P. M.(1968). The arthropathy of idiopathic haemochromatosis.Quarterly Journal of Medicine, 37, 171-182.
Harpey, J. P., Caille, B., Moulias, R., and Goust, J. M. (1971).Lupus-like syndrome induced by D-penicillamine inWilson's disease. (Letter.) Lancet, 1, 292.
Kaklamanis, P., and Spengos, M. (1973). Osteoarticularchanges and synovial biopsy findings in Wilson's disease.Annals ofthe Rheumatic Diseases, 32,422-427.
Lancet (1962). Copper, kidneys and calcium. (Leadingarticle),2,866-868.
Mehta, R. S., and Shinde, V. A. (1965). Wilson's disease withrickets. Neurology (Bombay), 13, 67-73.
Mindelzun, R., Elkin, M., Scheinberg, I. H., and Stemlieb, I.(1970). Skeletal changes in Wilson's disease: a radiologicalstudy. Radiology, 94, 127-132.
Morgan, H. G., Stewart, W. K., Lowe, K. G., Stowers, J. M.,
and Johnstone, J. H. (1962). Wilson's disease and theFanconi syndrome. Quarterly Journal of Medicine, 31,361-384.
Morris, J. J., Seifter, E., Rettura, G., Geever, E. F., andLevenson, S. M. (1969). Effect of penicillamine uponhealing of wounds. Journal of Surgical Research, 9,142-149.
Oliver, I., Liberman, U. A., de Vries, A., and Tikva, P. (1972).Lupus-like syndrome induced by penicillamine. Journal ofthe American Medical Association, 220, 588.
Rasmussen, K. (1971). Observations during treatment ofcystinuria with D-penicillamine. Acta Medica Scandinavica,189,367-372.
Rosenoer, V. M., and Michell, R. C. (1959). Skeletal changesin Wilson's disease (hepatolenticular degeneration).British Journal ofRadiology, 32, 805-809.
Stowers, J. M., and Dent, C. E. (1947). Studies on themechanism of the Fanconi syndrome. Quarterly Journal ofMedicine, 16,275-290.
Walshe, J. M. (1962). Wilson's disease: the presentingsymptoms. Archives of Disease in Childhood, 37, 253-255.
Walshe, J. M. (1968). Toxic reactions to penicillamine inpatients with Wilson's disease. Postgraduate MedicalJournal, 44, Suppl., 6-8.
Wamnock, C. G. (1952). Hepatolenticular degeneration(Wilson's disease); report of 5 cases, with commentary.Ulster MedicalJournal, 21, 155-171.
on July 23, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.36.2.99 on 1 A
pril 1977. Dow
nloaded from