
Bencana dan peperangan akhir zaman - Ibnu katsir - penerbit ummul qura
Upload
marjory-wrightCategory
view
225download
1
Arterial and Venous Occlusive Disease
of the Retina
Dr.M NAQEEB
Assistant professor Um Al-Qura university

Objective
1. Central retinal artery occlusion
2. Branch retinal artery occlusion
3. Branch retinal vein occlusion
4. Central retinal vein occlusion

retinal artery obstructions
57% of obstructions involved the central retinal artery
38% involved one of the branch retinal arteries
5% involved the cilioretinal artery

Central Artery Obstruction
Characteristics Sudden severe visual loss Painless Retinal appearance
» Opaque and edematous Most prominent in posterior pole
– Thickest ganglion cell layer
» Cherry-red spot Visible intact choroidal
vasculature beneath the foveola
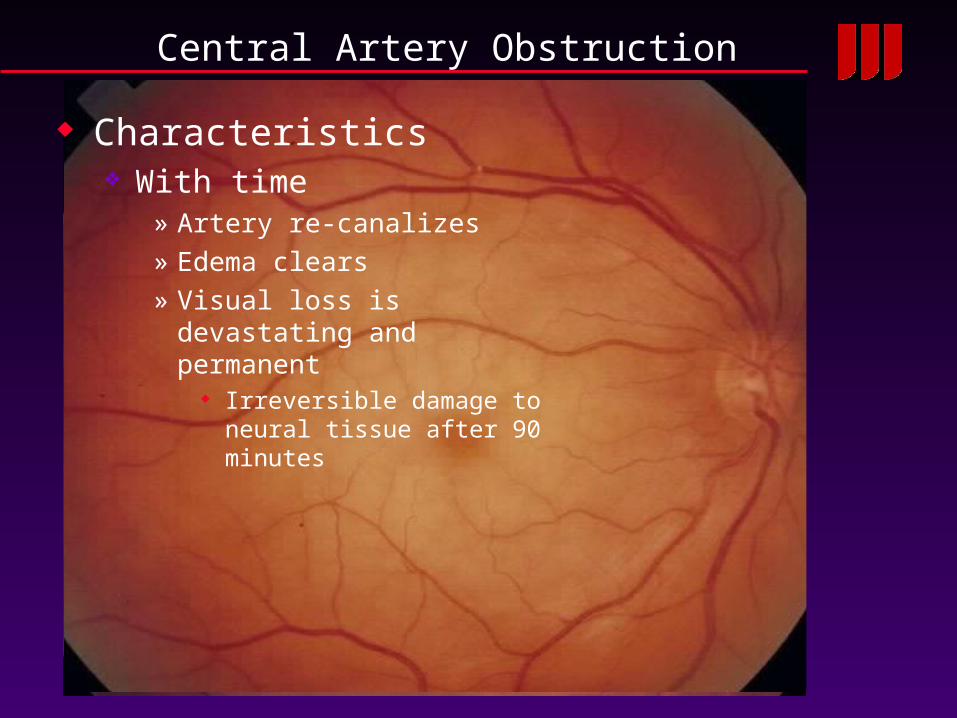
Central Artery Obstruction
Characteristics With time
» Artery re-canalizes» Edema clears» Visual loss is devastating and
permanent Irreversible damage to neural
tissue after 90 minutes

Intravenous fluorescein angiography

Central Artery Obstruction
Prognosis 20/400 or worse: 2/3 of eyes 20/40 or better: 1/6 eyes
» Intact cilioretinal artery
Vision of NLP» Implies ophthalmic artery
occlusion Choroidal ischemia as well

Central Artery Obstruction
Pathogenesis Majority
» atherosclerosis-related thrombosis
At the level of the lamina cribrosa
Other causes» Arterial spasm» Dissecting aneurysm» GIANT CELL ARTERITIS
1% of cases– Check ESR in elderly
patients!– Start high does steroids if
suspicious

Central Artery Obstruction
Management No good therapy exists, all
treatments questionable» Ocular message» Anterior chamber paracentesis
Attempt to acutely reduce IOP Dislodge thrombosis
» Inhalation therapy 95%O2, 5%CO2
– Stimulate vasodilatation
Iris neovascularization» Occurs in 18% of eyes
1-12 weeks later (usually 3-4 weeks later)
» Full PRP treatment required

Branch Retinal Artery Obstruction
Characteristics Vision loss Visual filed defect Within hours/days
» Edematous opacification of the retina
In the distribution of the affected vessel

Branch Retinal Artery Obstruction
Pathogenesis Embolization or thrombosis of vessel Three types of emboli
» Cholesterol Hollenhorst plaques Arise from carotid
» Platelet-fibrin Associated with arteriosclerosis
» Calcific Diseased cardiac valves

Retinal Embolization
Hollenhorst plaque Glistening cholesterol emboli Found within retinal arteriole
» Typically lodge at bifurcations
Arise in carotid arteries

Retinal Embolization
Hollenhorst plaque Glistening cholesterol emboli Found within retinal arteriole
» Typically lodge at bifurcations
Arise in carotid arteries

Branch Retinal Artery Obstruction
Other causes of BRVO Migraine
» Particularly in smokers Trauma Coagulation disorders Sickle cell disease Oral contraceptive use
» Smoking, older women Mitral valve prolapse Infections
» Toxoplasmosis, syphilis Giant cell arteritis
» Check ESR in elderly patients
Good prognosis

Workup
ESR,CBC and C-reactive protein Fasting blood sugar Glycosylated hemoglobin Doppler US for carotid artery ECG, echocardiogram Refer for haematology

Mortality/Morbidity
Further emboli to the brain resulting in CVA 55% death over 10 years 27% age matched population
Further emboli to same or contralateral eye resulting in further visual loss
Progression of temporal arteritis

Venous Occlusive Disease

Central Retinal Vein Occlusion
Findings Dilated and tortuous
retinal veins Swollen optic disc Intra-retinal hemorrhages Retinal edema
All four quadrants

Central Retinal Vein Occlusion
Classification Based on amount of non-profusion on fluorescein
angiography» Ischemic
≥10 disk areas
» Non-ischemic < 10 disk areas
» Indeterminate Too much hemorrhage to tell 80% progress to ischemic

Central Retinal Vein Occlusion
Pathogenesis Thrombosis of the central retinal vein
» At or posterior to the lamina cribrosa
Atherosclerotic central retinal artery » Impinges on central retinal vein
Turbulent flow → thrombus

Central Retinal Vein Occlusion
Non-ischemic CRVO Less dilation and vascular
tortuosity Dot and flame hemorrhages
in all quadrants Less or no disk swelling
Angiogram shows» Delayed A-V transit time» Leakage» Minimal capillary dropout
Neovascularization is rare
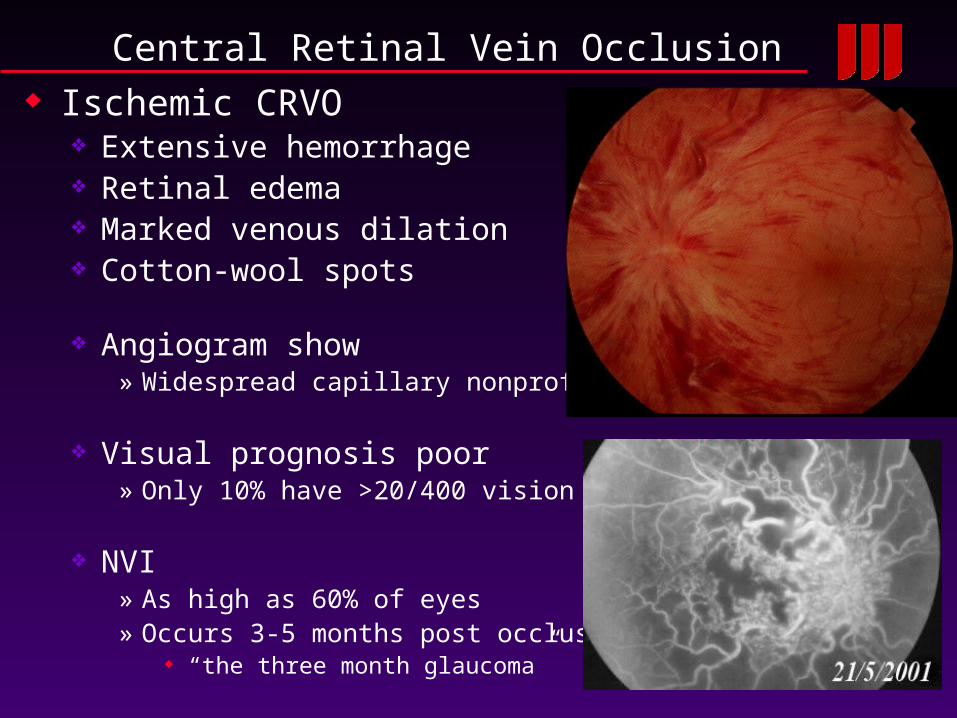
Central Retinal Vein Occlusion Ischemic CRVO
Extensive hemorrhage Retinal edema Marked venous dilation Cotton-wool spots
Angiogram show» Widespread capillary nonprofusion
Visual prognosis poor» Only 10% have >20/400 vision
NVI» As high as 60% of eyes» Occurs 3-5 months post occlusion
“the three month glaucoma”

Central Retinal Vein Occlusion
Risk Factors Eye Disease Case-Control
Study» Hypertension» Diabetes
Unlike BRVO
» Glaucoma Check and treat IOP!
CRVO in young patients requires more extensive workup for cause

CRVO In Young Patients – Causes
Systemic vascular disease Hypertension Diabetes mellitus Cardiovascular disease
Blood dyscrasias Polycythemia vera Lymphoma Leukemia
Clotting disorders Activated protein C resistance Lupus anticoagulant Anticardiolipin antibodies Protein C Protein S Antithrombin III
Paraproteinemia and dysproteinemias Multiple myeloma Cryoglobulinemia
Vasculitis Syphilis Sarcoidosis
Autoimmune disease Systemic lupus erythematosus
Oral contraceptive use in women Other rare associations
Closed-head trauma Optic disc drusen Arteriovenous malformations of retina

Central Retinal Vein Occlusion
Management Family medical doctor to
manage» Hypertension» Diabetes» Elevated cholesterol

Central Retinal Vein Occlusion
Management Macular edema
» Central Vein Occlusion Study Group
Grid laser treatment in the macula
– DOES reduce angiographic evidence of edema
– DOES NOT improve vision

Central Retinal Vein Occlusion
Management Macular edema
» Intravitreal trimcinolone/Avastin » Capable of transiently
improving vision Risks
– Glaucoma– RD– Cataract– Endopthalmitis

Central Retinal Vein Occlusion
Management Iris neovascularization
PRP to eyes prior to NVI» NO benefit
Even if very ischemic
Once neovascularization detected
» Prompt PRP

Central Retinal Vein Occlusion
Outcome Most important predictor is
initial visual acuity:» 20/40 or better
Likely to remain unchanged
» 20/400 or less Likely to remain worse than
20/400
» 20/50-20/200 1/3 unchanged 1/3 improve 1/3 worse

Branch Retinal Vein Occlusion
Findings Within one sector of the
retina» Superficial hemorrhages» Retinal edema» Cotton-wool spots» Dilated and tortuous vein» Corresponding artery narrowed
and sheathed

Branch Retinal Vein Occlusion
Findings Superotemporal quadrant
most common» 63%
Occurs at arteriovenous crossing
» Artery and vein bound together in a common sheath
» Arterial thickening compresses vein
Turbulent flow → thrombus formation

Branch Retinal Vein Occlusion
Risk factors Identified by the Eye Disease
Case-Control Study» Hypertension» Cardiovascular disease» Increased BMI at age 20» Glaucoma
Note : Diabetes not an independent risk factor

Branch Retinal Vein Occlusion
Visual Loss Acute
» Macular hemorrhage» Macular edema» Capillary occlusion
Chronic» Macular ischemia» CME» Macular pigmentary changes» Epiretinal membrane formation» Subretinal fibrosis

Branch Retinal Vein Occlusion
Photocoagulation Used to treat:
» Macular edema Requires intact foveal perfusion
» Neovascularization
Macular edema» Allow three months for
improvement» Vision 20/40 or worse» Light grid pattern of laser spots to
involved sector of retina
» Branch vein occlusion study Treated eyes more likely to gain
2 lines of vision– Treated 65%, untreated 37%


Branch Retinal Vein Occlusion
Photocoagulation Neovascularization
» BVOS defined ischemic BRVO Area of non-profusion > 5 disk
diameters
» Large areas of non-profusion increase risk of neovascularization
Apply scatter PRP to areas of retinal ischemia
» Only when neovascular complications develop
NVI, NVE, NVD

Branch Retinal Vein Occlusion
Vascular Remodeling
Photocoagulation» Must differentiate
Neovascular tissue– Leaks on fluorscein angiogram
Collateral vessels– Help to reduce vascular tissue– Do not treat

Thank you xoxo


















