
Are Providers Self-Efficacy and Outcome Expectations ... · Social Cognitive Theory ... Analysis...
43
1 Are Providers’ Self-Efficacy and Outcome Expectations Related to Obesity Counseling Frequency? Lisa M. Lowenstein, MPH, RD Eliana Perrin, MD, MPH; Marci K Campbell PhD; Deborah Tate, PhD; Jianwen Cai, PhD, Alice Ammerman, DrPh, RD Gillings School of Global Public Health, School of Medicine Center for Health Promotion and Disease Prevention The University of North Carolina at Chapel Hill
Transcript of Are Providers Self-Efficacy and Outcome Expectations ... · Social Cognitive Theory ... Analysis...
1
Are Providers’ Self-Efficacy and Outcome Expectations Related to Obesity Counseling Frequency?
Lisa M. Lowenstein, MPH, RD
Eliana Perrin, MD, MPH; Marci K Campbell PhD; Deborah Tate, PhD; Jianwen Cai, PhD, Alice Ammerman, DrPh, RD
Gillings School of Global Public Health, School of MedicineCenter for Health Promotion and Disease PreventionThe University of North Carolina at Chapel Hill
2
Background

3
Childhood Overweight and Obesity
NHANES Data (2003-2006)
BMI Category 2-5 year olds 6-11 year olds
Overweight (≥ 85th percentile) 26% 33%
Obese (≥ 95th percentile) 14% 18%
Ogden JAMA 2008

4
Consequences of Childhood Overweight and Obesity
� Health Disparities� Physical
� Asthma � Sleep apnea� Diabetes� More likely to develop other chronic diseases
� Psychosocial� Low self-esteem � Decreased quality of life
� Economic� Increased health care costs� Increased lab requests
Daniels, SR Future child 2006; Dietz, W Pediatrics 1998; SchwimmerJAMA 2003; Magarey, AM Int J Obes Relat Metab Disord. 2003

5
Points of Intervention
� One point of intervention is in primary care� May be the only option for low-income
populations� Multiple levels of intervention
� Provider-patient communication� Provider

6
Obesity Prevention and Treatment in Primary Care� Primary care providers seen as a source of
health information� Clinic based interventions
� Weight loss� Improved health behaviors
� Few resources are available� USPSTF Guidelines
� 25 hours of contact
Epstein LH. Health Psychol 1994; Mellin LM J Am Diet Assoc. 1987; Sothern MS J Am Diet Assoc 2002; Patrick K Arch Pediatr Adolesc Med 2001; Savoye M JAMA 2007; Schwartz R Arch Pediatr Adolesc Med 2007

7
Preventive Counseling Frequency
� Less than 50% of providers counsel on nutrition and physical activity
� Predictors of counseling� Female providers� > 10 patients/week� Spent >20 minutes/patient� Plotting BMI� Older children� Children with a BMI ≥ 95th percentile
Frank E Am J Clin Nutr 2002; Rattay K Obesity Res 2004; Cook S Pediatrics 2005
8
Barriers to Preventive Counseling
� Lack of time� Lack of resources� Lack of reimbursement� Low parent motivation� Low perceived efficacy� Low self-efficacy
Story MT Pediatrics 2002; Douglas F BMC Public Health 2006; Perrin EM Ambul Pediatr2005

9
Providers’ Attitudes and Beliefs
� What we know� Providers
� Believe overweight and obese children and adolescents need treatment
� Believe overweight and obesity during childhood and adolescence affects chronic disease risk
� Have low self-efficacy for obesity prevention counseling� Find obesity counseling unrewarding
Story MT Pediatrics 2002; van Gerwen M Obesity Reviews 2009

10
Providers’ Attitudes and Beliefs
� What we don’t know� Outcome expectations
� One study assessed outcome expectations � "How much can you do to prevent these problems?“� Not outcome expectations
� Relationship of self-efficacy, outcome expectations, and counseling frequency
Cheng T Arch Pediatr Adolesc Med 1999

11
Objectives
� Does obesity preventive counseling differ from other preventive counseling topics?
� Do providers with higher levels of self-efficacy or outcome expectations report they counsel on obesity related topics more often?

12
Methods

13
Kids Eating Smart and Moving More (KESMM) – Phase II
� Goal: Improve providers’ ability to identify and assess children who are at risk for or already overweight
� 5-year randomized pediatric obesity intervention trial funded by NICHD

14
Participants - Providers
� Providers include:� Medical Doctors, Nurse Practitioners, and Physician
Assistants
� Can participate if their practice is enrolled into KESMM
� Provider champion lets other providers know about the study
� Consented at the first practice training � Receive continuing medical education credits at
second practice training

15
Provider Baseline Survey
� Developed� Review of the literature � Refined from the pilot study
� Pre-tested the survey to assess � Amount of time to fill out� Clarity of questions
� Administration:� Delivered at the first practice training � Picked-up at the second practice training

16
Social Cognitive Theory
Self Efficacy Goals
Sociostructural Factors
Facilitators
Barriers
Outcome Expectations
Physical
Social
Self-evaluative
Behavior
Bandura A Health Educ Behav 2004

17
Social Cognitive Theory
Self Efficacy Goals
Sociostructural Factors
Facilitators
Barriers
Outcome Expectations
Physical
Social
Self-evaluative
Behavior
Bandura A Health Educ Behav 2004

18
Social Cognitive Theory
Self Efficacy Goals
Sociostructural Factors
Facilitators
Barriers
Outcome Expectations
Physical
Social
Self-evaluative
Behavior
Bandura A Health Educ Behav 2004
19
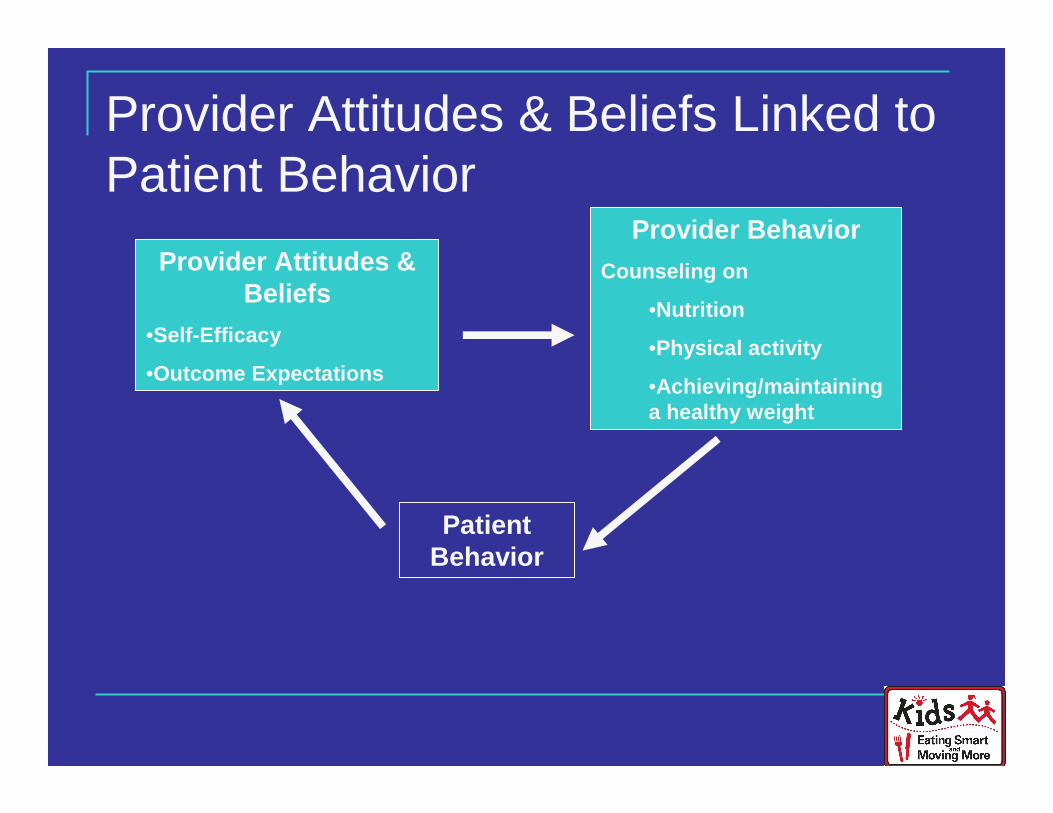
Provider Attitudes & Beliefs Linked to Patient Behavior
Provider Attitudes & Beliefs
•Self-Efficacy
•Outcome Expectations
Provider Behavior
Counseling on
•Nutrition
•Physical activity
•Achieving/maintaining a healthy weight
Patient Behavior

20
Dependent Variables – Preventive Counseling Frequency� When you see children 3-8 for well child
check, how often do you discuss the following topics:� Healthy Eating� Physical Activity� Achieving/Maintaining a Healthy Weight

21
Independent Variables – Self-Efficacy
� Please rate your confidence in your ability to effectively counsel families about � Increasing F&V� Decreasing sweetened beverage consumption� Decreasing juice consumption� Switching to lower fat milk� Decreasing junk food consumption� Reducing screen time � Increasing outdoor activity� Discuss children’s weight status

22
Independent Variables – Outcome Expectations� Please rate your agreement with the following
statement: “I believe that my counseling families will result in actual change regarding …. � Increasing F&V� Decreasing sweetened beverage consumption� Decreasing juice consumption� Switching to lower fat milk� Decreasing junk food consumption� Reducing screen time � Increasing outdoor activity� Discuss children’s weight status

23
Analysis
� STATA� Basic descriptive statistics� Proportional-Odds-Modeling
� Outcome variables are ordered and non-normal� Greater power than logistic regression� Random effect to account for clustering

24
Results

25
Participant CharacteristicsClinics (N=21)Providers (N=110)
8268Pediatrics/Med-Peds
1815Family Medicine
Provider Type/Residency
%nVariable
27
83
96
24Nurse Practitioner/Physician Assistant
75MD/DO
69Female

26
Healthy Eating Counseling FrequencyAll of the time
0
10
20
30
40
50
60
Healthy eating
Physical activity
Age-specific injuryprevention
Maintaining andachieving a healthyweight General behaviorproblems
Preschool/schoolproblems
* Single test of proportions (p<0.05)
**
* * *

27
Physical Activity Counseling FrequencyAll of the time
0
10
20
30
40
50
60Healthy eating
Physical activity
Age-specific injuryprevention
Maintaining andachieving a healthyweight General behaviorproblems
Preschool/schoolproblems
* Single test of proportions (p<0.05)
*
* * *

28
Healthy Weight Counseling FrequencyAll of the time
0
10
20
30
40
50
60Healthy eating
Physical activity
Age-specific injuryprevention
Maintaining andachieving a healthyweight General behaviorproblems
Preschool/schoolproblems
* Single test of proportions (p<0.05)
*
* *

29
Providers are confident but have low expectations
9 (8)
7 (6)
4 (4)
6 (5)
22 (20)
15 (14)
18 (16)
5 (5)
4 (4)
Outcome ExpectationsN (%)
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
p-value
44 (40)Weight status
Self-EfficacyN (%)
37 (34)Outdoor activity
35 (32)Screen time
16 (15)Behavior problems
42 (38)“Junk food”
52 (47)Lower fat milk
52 (47)Juice
50 (45)SSB
42 (38)Fruit & vegetables

30
Providers are confident but have low expectations
9 (8)
7 (6)
4 (4)
6 (5)
22 (20)
15 (14)
18 (16)
5 (5)
4 (4)
Outcome ExpectationsN (%)
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
<0.00001
p-value
44 (40)Weight status
Self-EfficacyN (%)
37 (34)Outdoor activity
35 (32)Screen time
16 (15)Behavior problems
42 (38)“Junk food”
52 (47)Lower fat milk
52 (47)Juice
50 (45)SSB
42 (38)Fruit & vegetables

31
Providers are confident but have low expectations
9 (8)
7 (6)
4 (4)
6 (5)
22 (20)
15 (14)
18 (16)
5 (5)
4 (4)
Outcome ExpectationsN (%)
<.001
<.001
<.001
<.001
<.001
<.001
<.001
<.001
<.001
p-value
44 (40)Weight status
Self-EfficacyN (%)
37 (34)Outdoor activity
35 (32)Screen time
16 (15)Behavior problems
42 (38)“Junk food”
52 (47)Lower fat milk
52 (47)Juice
50 (45)SSB
42 (38)Fruit & vegetables

32
Is Self-Efficacy Related to Counseling Frequency (CF)?
Physical Activity
1.4 (0.78, 2.7)2.3 (0.89, 5.8)Healthy weight
Healthy Eating
1.7 (1.0, 2.7)
1.5 (0.9, 2.3)
1.5 (0.9, 2.6)
1.7 (1.0, 2.9)
2.0 (1.2, 3.2)
2.3 (1.4, 3,7)
2.2 (1.3, 3.8)
Outcome ExpectationsOR (95% CI)
Self-EfficacyOR (95% CI)
2.6 (1.7, 3.9)Outdoor activity
1.8 (1.1, 2.8)Screen time
1.7 (1.0, 3.0)“Junk food”
2.5 (1.4, 4.3)Lower fat milk
2.0 (1.2, 3.4)Juice
2.2 (1.1, 4.3)SSB
1.8 (1.0, 3.1)Fruit & vegetables
33
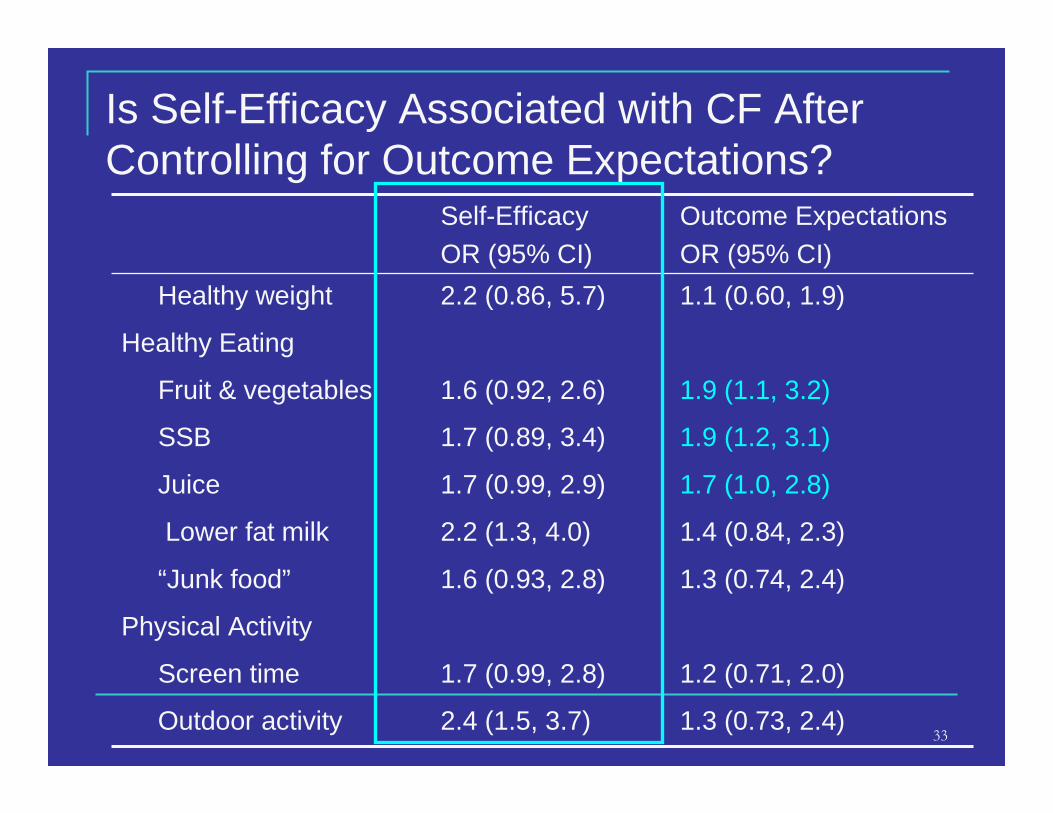
Is Self-Efficacy Associated with CF After Controlling for Outcome Expectations?
Physical Activity
1.1 (0.60, 1.9)2.2 (0.86, 5.7)Healthy weight
Healthy Eating
1.3 (0.73, 2.4)
1.2 (0.71, 2.0)
1.3 (0.74, 2.4)
1.4 (0.84, 2.3)
1.7 (1.0, 2.8)
1.9 (1.2, 3.1)
1.9 (1.1, 3.2)
Outcome ExpectationsOR (95% CI)
Self-EfficacyOR (95% CI)
2.4 (1.5, 3.7)Outdoor activity
1.7 (0.99, 2.8)Screen time
1.6 (0.93, 2.8)“Junk food”
2.2 (1.3, 4.0)Lower fat milk
1.7 (0.99, 2.9)Juice
1.7 (0.89, 3.4)SSB
1.6 (0.92, 2.6)Fruit & vegetables
34
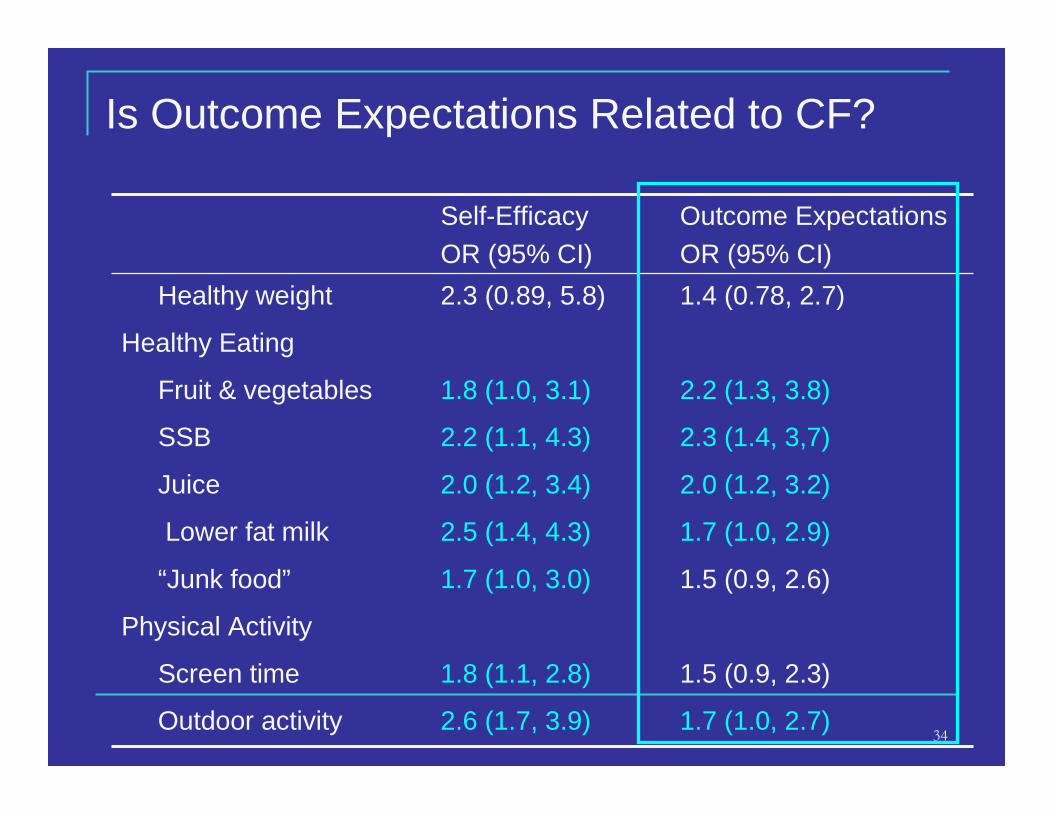
Is Outcome Expectations Related to CF?
Physical Activity
1.4 (0.78, 2.7)2.3 (0.89, 5.8)Healthy weight
Healthy Eating
1.7 (1.0, 2.7)
1.5 (0.9, 2.3)
1.5 (0.9, 2.6)
1.7 (1.0, 2.9)
2.0 (1.2, 3.2)
2.3 (1.4, 3,7)
2.2 (1.3, 3.8)
Outcome ExpectationsOR (95% CI)
Self-EfficacyOR (95% CI)
2.6 (1.7, 3.9)Outdoor activity
1.8 (1.1, 2.8)Screen time
1.7 (1.0, 3.0)“Junk food”
2.5 (1.4, 4.3)Lower fat milk
2.0 (1.2, 3.4)Juice
2.2 (1.1, 4.3)SSB
1.8 (1.0, 3.1)Fruit & vegetables
35
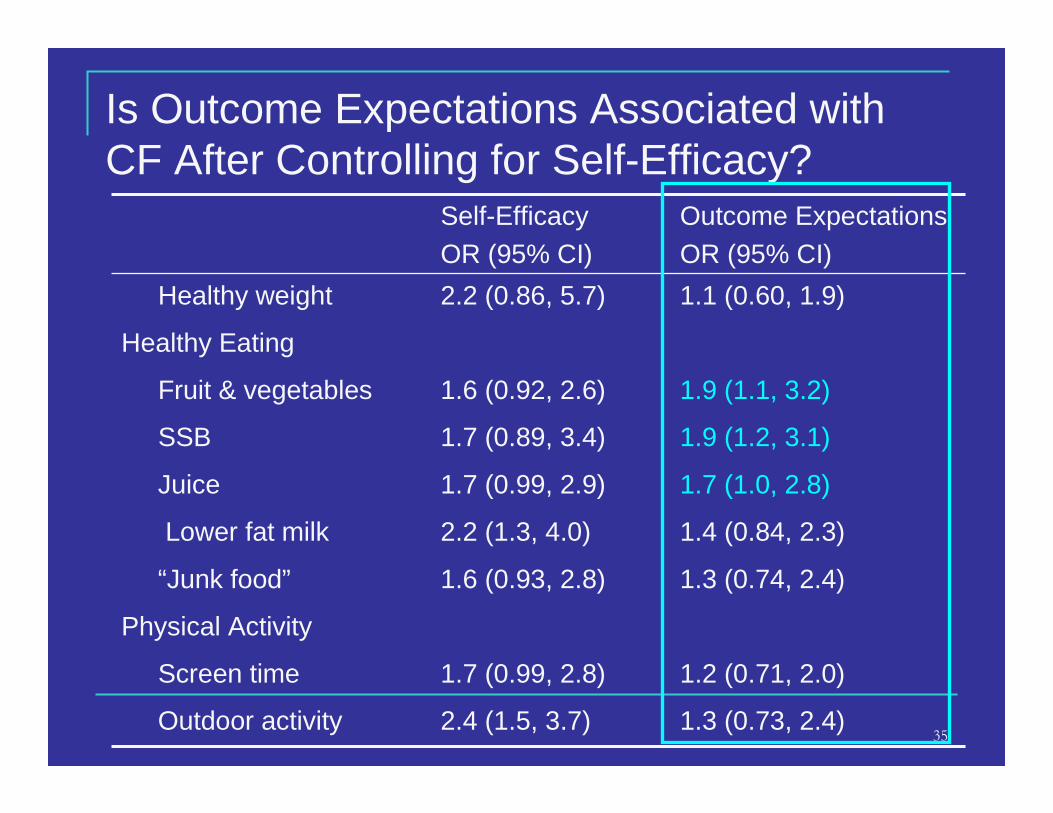
Is Outcome Expectations Associated with CF After Controlling for Self-Efficacy?
Physical Activity
1.1 (0.60, 1.9)2.2 (0.86, 5.7)Healthy weight
Healthy Eating
1.3 (0.73, 2.4)
1.2 (0.71, 2.0)
1.3 (0.74, 2.4)
1.4 (0.84, 2.3)
1.7 (1.0, 2.8)
1.9 (1.2, 3.1)
1.9 (1.1, 3.2)
Outcome ExpectationsOR (95% CI)
Self-EfficacyOR (95% CI)
2.4 (1.5, 3.7)Outdoor activity
1.7 (0.99, 2.8)Screen time
1.6 (0.93, 2.8)“Junk food”
2.2 (1.3, 4.0)Lower fat milk
1.7 (0.99, 2.9)Juice
1.7 (0.89, 3.4)SSB
1.6 (0.92, 2.6)Fruit & vegetables

36
Discussion

37
Main Points
� Providers are confident in their counseling skills but do not have high expectations
� Self-efficacy and outcome expectations were associated with counseling frequency for dietary and exercise behaviors but not counseling about healthy weight

38
Strength & Limitations
� Modeled the relationship of provider attitudes and beliefs with behavior
� Providers from clinics participating in an obesity prevention intervention
� Sample limited to mainly pediatricians� Counseling frequency was self-report

39
Summary & Discussion
� Contributes to the emerging research on pediatric overweight and obesity prevention and assessment in primary care practices
� Future research could target provider outcome expectations in addition to self-efficacy
� May help the development of other interventions to train providers in the prevention, assessment, and treatment of childhood obesity

Questions?
Funded by NICHD
Acknowledgements: Ziya Gizlice, Larry Johnson, Lisa Pullen Davis, Maihan Vu, Cecelia Gonzales
Contact: [email protected]

41
ReferencesNationalTaskForceonthePreventionandTreatmentofObesity . Overweight, obesity, and health risk. Arch Intern Med. 2000;160:898-904.Expert committee recommendations on the assessment, prevention and treatment of child and adolescent overweight and obesity. 2007.Hedley A, Ogden C, Johnson C, Carroll M, Curtin L, Flegal K. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA.
2004;291:2847-2850. Ogden et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA, 2006;295(13):1549-55.North Carolina Nutrition and Physical Activity Surveillance System (NC-PASS). Eat Smart, Move More North Carolina Website. Available at:
http://www.eatsmartmovemorenc.com/data.htm.Daniels SR. The consequences of childhood overweight and obesity. Future Child. 2006;16:47-67.Dietz W. Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatrics. 1998;101:518-525.Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289:1813-1819.Magarey AM, Daniels LA, Boulton TJ, Cockington RA. Predicting obesity in early adulthood from childhood and parental obesity. Int J Obes Relat Metab Disord. 2003;27:505-
513.Estabrooks P, Shetterly S. The prevalence and health care use of overweight children in an integrated health care system. Arch Pediatr Adolesc Med. 2007;161:222-227.Hampl SE, Carroll CA, Simon SD, Sharma V. Resource utilization and expenditures for overweight and obese children. Arch Pediatr Adolesc Med. 2007;161:11-14.Woolford SJ, Gebremariam A, Clark SJ, Davis MM. Incremental hospital charges associated with obesity as a secondary diagnosis in children. Obesity (Silver Spring).
2007;15:1895-1901.Lowenstein LM, Vu MB, Davis LP, et al. Parents prescription for providers: What fathers are saying about preventing childhood overweight. Epstein LH, Valoski A, Wing RR, McCurley J. Ten-year outcomes of behavioral family-based treatment for childhood obesity. Health Psychol. 1994;13:373-383.Mellin LM, Slinkard LA, Irwin CE,Jr. Adolescent obesity intervention: Validation of the SHAPEDOWN program. J Am Diet Assoc. 1987;87:333-338.Sothern MS, Schumacher H, von Almen TK, Carlisle LK, Udall JN. Committed to kids: An integrated, 4-level team approach to weight management in adolescents. J Am Diet
Assoc. 2002;102:S81-5.Patrick K, Sallis JF, Prochaska JJ, et al. A multicomponent program for nutrition and physical activity change in primary care: PACE+ for adolescents. Arch Pediatr Adolesc Med.
2001;155:940-946.Savoye M, Shaw M, Dziura J, et al. Effects of a weight management program on body composition and metabolic parameters in overweight children: A randomized controlled
trial. JAMA. 2007;297:2697-2704.Schwartz R, Hamre R, Dietz W, et al. Office-based motivational interviewing to prevent childhood obesity: A feasibility study. Arch Pediatr Adolesc Med. 2007;161:495-501.Perrin EM, Flower KB, Ammerman AS. Body mass index charts: Useful yet underused. J Pediatr. 2004;144:455-460.Centers for Disease Control and Prevention. ICD-9-CM. Official Guidelines for Coding and Reporting. Available at: http://www.cdc.gov/nchs/data/icd9/icdguide.pdf. Accessed
September 2007.Cook S, Weitzman M, Auinger P, Barlow SE. Screening and counseling associated with obesity diagnosis in a national survey of ambulatory pediatric visits. Pediatrics.
2005;116:112-116.Dorsey K, Wells C, Krumholz H, Concato J. Diagnosis, evaluation, and treatment of childhood obesity in pediatric practice. Arch Pediatr Adolesc Med. 2005;159:632-638.Kolagotla L, Adams W. Ambulatory management of childhood obesity. Obesity Res. 2004;12:275-283.Quiros-Tejeira RE, Rivera CA, Ziba TT, Mehta N, Smith CW, Butte NF. Risk for nonalcoholic fatty liver disease in hispanic youth with BMI > or =95th percentile. J Pediatr
Gastroenterol Nutr. 2007;44:228-236.Wang Y, Chen X, Klag MJ, Caballero B. Epidemic of childhood obesity: Implications for kidney disease. Adv Chronic Kidney Dis. 2006;13:336-351.Frank E, Wright E, Serdula M, Elon L, Baldwin G. Personal and professional nutrition-related practices of US female physicians. Am J Clin Nutr. 2002;75:326-332.Rattay K, Fulton J, Galuska D. Weight counseling patterns of U.S. pediatricians. Obesity Res. 2004;12:161-169.

42
ReferencesStory MT, Neumark-Stzainer DR, Sherwood NE, et al. Management of child and adolescent obesity: Attitudes, barriers, skills, and training needs among health care
professionals. Pediatrics. 2002;110:210.Perrin EM, Flower K, Garrett J, Ammerman A. Preventing and treating obesity: Pediatricians' self-efficacy, barriers, resources, and advocacy. Ambulatory Pediatrics. 2005;5:150-
156.Bandura A. Social cognitive theory: An agentic perspective. Annu Rev Psychol. 2001;52:1-26.Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44:1175-1184.Barlow S, Trowbridge F, Klish W, Dietz W. Treatment of child and adolescent obesity: Reports from pediatricians, pediatric nurse practitioners, and registered dietitians.
Pediatrics. 2002;110:229-235.Dunlop AL, Leroy Z, Trowbridge FL, Kibbe DL. Improving providers' assessment and management of childhood overweight: Results of an intervention. Ambul Pediatr.
2007;7:453-457.Flower KB, Perrin EM, Viadro CI, Ammerman AS. Using body mass index to identify overweight children: Barriers and facilitators in primary care. Ambul Pediatr. 2007;7:38-44.Campbell KJ, Crawford DA, Salmon J, Carver A, Garnett SP, Baur LA. Associations between the home food environment and obesity-promoting eating behaviors in adolescence.
Obesity (Silver Spring). 2007;15:719-730.Matheson DM, Robinson TN, Varady A, Killen JD. Do mexican-american mothers' food-related parenting practices influence their children's weight and dietary intake? J Am Diet
Assoc. 2006;106:1861-1865.Pugliese J, Tinsley B. Parental socialization of child and adolescent physical activity: A meta-analysis. J Fam Psychol. 2007;21:331-343.Styles JL, Meier A, Sutherland LA, Campbell MK. Parents' and caregivers' concerns about obesity in young children: A qualitative study. Fam Community Health. 2007;30:279-
295.Douglas F, Torrance N, van Teijlingen E, Meloni S, Kerr A. Primary care staff's views and experiences related to routinely advising patients about physical activity. A
questionnaire survey. BMC Public Health. 2006;6:138.Perrin EM, Flower KB, Garrett J, Ammerman AS. Preventing and treating obesity: Pediatricians' self-efficacy, barriers, resources, and advocacy. Ambul Pediatr. 2005;5:150-156.Etelson D, Brand DA, Patrick PA, Shirali A. Childhood obesity: Do parents recognize this health risk? Obes Res. 2003;11:1362-1368.Eckstein KC, Mikhail LM, Ariza AJ, et al. Parents' perceptions of their child's weight and health. Pediatrics. 2006;117:681-690.Crawford PB, Gosliner W, Anderson C, et al. Counseling latina mothers of preschool children about weight issues: Suggestions for a new framework. J Am Diet Assoc.
2004;104:387-394.Edmunds LD. Parents' perceptions of health professionals' responses when seeking help for their overweight children. Fam Pract. 2005;22:287-292.Woolford SJ, Clark SJ, Lumeng JC, Williams DR, Davis MM. Maternal perspectives on growth and nutrition counseling provided at preschool well-child visits. J Natl Med Assoc.
2007;99:153-158.A Horodynski M, Arndt MJ. "Eating-together" mealtimes with african-american fathers and their toddlers. Appl Nurs Res. 2005;18:106-109.Cabrera NJ, Tamis-LeMonda CS, Bradley RH, Hofferth S, Lamb ME. Fatherhood in the twenty-first century. Child Dev. 2000;71:127-136.Sarkadi A, Kristiansson R, Oberklaid F, Bremberg S. Fathers' involvement and children's developmental outcomes: A systematic review of longitudinal studies. Acta Paediatr.
2008;97:153-158.Coleman WL, Garfield C, American Academy of Pediatrics Committee on Psychosocial Aspects of Child and Family Health. Fathers and pediatricians: Enhancing men's roles in
the care and development of their children. Pediatrics. 2004;113:1406-1411.Garfield CF, Isacco A. Fathers and the well-child visit. Pediatrics. 2006;117:e637-45.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol.
1986;51:1173-1182.Judd, C. M. Kenny, D. A. Process analysis: Estimating mediation in treatment evaluations. Evaluation Review. 1981:602-619.Patton M. Qualitative Evaluation and Research Methods. 2nd ed. Newbury Park, CA: Sage Publications, Inc.; 1990.Ulin PR, Robinson ET, Tolley EE. Qualitative Methods in Public Health: A Field Guide Fo Applied Research. 1st ed. ed. San Francisco, CA: Family Health International; 2005.Muhr T, Friese S, Scientific Software Development. Atlas.ti. Berlin:2004;5.0.

43
Psychometric Testing of Scales(Self-efficacy, Outcome Expectations, Counseling Frequency)
� Cronbach’s alpha was calculated � Items were equally weighted
Preventive counseling
Nutrition Physical Activity
Self-Efficacy 0.9334 0.9519 0.7785
Outcome expectations 0.9414 0.9206 0.8677
Counseling Frequency 0.8524 NA NA


















