
are not achieved with intravenous dosing.
28
ERWINASE- asparaginase injection, powder, lyophilized, for solution Porton Biopharma Limited Disclaimer: This drug has not been found by FDA to be safe and effective, and this labeling has not been approved by FDA. For further information about unapproved drugs, click here. ---------- HEALTH CARE PROVIDER LETTER 25 May 2021 IMPORTANT PRESCRIBING INFORMATION Subject: Temporary importation of Erwinase (crisantaspase) injection, powder, lyophilized, for solution to address a drug shortage in the United States (U.S.) Dear Healthcare Professional, In order to alleviate a critical shortage of U.S.-licensed asparaginase erwinia chrysanthemi injection, powder, lyophilized, for solution in the US market, Porton Biopharma Limited (PBL) is coordinating with the U.S. Food and Drug Administration (FDA) to make available in the U.S. the non-FDA licensed Erwinase (crisantaspase) 10,000 IU/vial powder for solution for injection/infusion. At this time, no other entity except PBL (via its distributor Clinigen Inc.) is authorized by the FDA to import and distribute Erwinase in the U.S. However, this does not represent a formal FDA approval of Erwinase in the U.S. Effective immediately, PBL (via its distributor Clinigen Inc.) will distribute the following presentation of Erwinase (Batch number: W060172) to address the critical shortage: Product Name Pack Size Description U.K. Marketing Authorization Number NDC Erwinase, 10,000 IU/vial, Powder for solution for injection/infusion. 5 vials Powder for solution for injection/infusion. W hite lyophilised powder in a vial. PL 44403/0002 NDC 81561- 413- 05* *This NDC code has been assigned by PBL. The code is presented on the carton. It should be noted that the importer and distributor in the U.S. will be Clinigen Inc. The same NDC code will be used throughout the distribution chain of the product in the U.S. It is important to note the following: Erwinase is available in the U.S. only by prescription. There is no barcode on this product for use with U.S. barcode scanning systems. Alternative procedures should be followed to assure that the correct drug product is being used and administered to individual patients. Contraindications to use of Erwinase include: Serious hypersensitivity reactions to asparaginase erwinia chrysanthemi, including anaphylaxis Serious pancreatitis with any prior asparaginase therapy Serious thrombosis with any prior asparaginase therapy Serious hemorrhagic events with any prior asparaginase therapy There are differences between the U.S.-licensed asparaginase erwinia chrysanthemi Prescribing Information and the Erwinase Summary of Product Characteristics (Appendix 2). Use the recommended dosage for U.S.-licensed asparaginase erwinia chrysanthemi To substitute for each planned dose of pegaspargase, the recommended dosage of Erwinase is 25,000 International Units/m administered intramuscularly or intravenously three times a week (Monday/Wednesday/Friday) for two consecutive weeks (total six doses). When administering Erwinase intravenously, the desired NSAA levels may not be achieved; consider monitoring nadir (pre-dose) serum asparaginase activity (NSAA) levels and switching to intramuscular administration if desired NSAA levels are not achieved with intravenous dosing. ® 2
Transcript of are not achieved with intravenous dosing.

ERWINASE- asparaginase injection, powder, lyophilized, for solution Porton Biopharma LimitedDisclaimer: This drug has not been found by FDA to be safe and effective, and thislabeling has not been approved by FDA. For further information about unapproveddrugs, click here.
----------
HEALTH CARE PROVIDER LETTER25 May 2021IMPORTANT PRESCRIBING INFORMATIONSubject: Temporary importation of Erwinase (crisantaspase) injection, powder,lyophilized, for solution to address a drug shortage in the United States (U.S.)Dear Healthcare Professional,In order to alleviate a critical shortage of U.S.-licensed asparaginase erwiniachrysanthemi injection, powder, lyophilized, for solution in the US market, PortonBiopharma Limited (PBL) is coordinating with the U.S. Food and Drug Administration(FDA) to make available in the U.S. the non-FDA licensed Erwinase (crisantaspase)10,000 IU/vial powder for solution for injection/infusion.At this time, no other entity except PBL (via its distributor Clinigen Inc.) is authorized bythe FDA to import and distribute Erwinase in the U.S. However, this does not representa formal FDA approval of Erwinase in the U.S.Effective immediately, PBL (via its distributor Clinigen Inc.) will distribute the followingpresentation of Erwinase (Batch number: W060172) to address the critical shortage:
Product Name PackSize
Description U.K.MarketingAuthorizationNumber
NDC
Erwinase,10,000 IU/vial,Powder forsolution forinjection/infusion.
5vials
Powder forsolution forinjection/infusion.White lyophilisedpowder in a vial.
PL44403/0002
NDC81561-413-05*
*This NDC code has been assigned by PBL. The code is presented on the carton. Itshould be noted that the importer and distributor in the U.S. will be Clinigen Inc. Thesame NDC code will be used throughout the distribution chain of the product in the U.S.It is important to note the following:
Erwinase is available in the U.S. only by prescription.There is no barcode on this product for use with U.S. barcode scanningsystems. Alternative procedures should be followed to assure that the correct drug product isbeing used and administered to individual patients.Contraindications to use of Erwinase include:
Serious hypersensitivity reactions to asparaginase erwinia chrysanthemi, includinganaphylaxisSerious pancreatitis with any prior asparaginase therapySerious thrombosis with any prior asparaginase therapySerious hemorrhagic events with any prior asparaginase therapy
There are differences between the U.S.-licensed asparaginase erwiniachrysanthemi Prescribing Information and the Erwinase Summary ofProduct Characteristics (Appendix 2). Use the recommended dosage forU.S.-licensed asparaginase erwinia chrysanthemi
To substitute for each planned dose of pegaspargase, the recommended dosageof Erwinase is 25,000 International Units/m administered intramuscularly orintravenously three times a week (Monday/Wednesday/Friday) for two consecutiveweeks (total six doses). When administering Erwinase intravenously, the desired NSAA levels may not beachieved; consider monitoring nadir (pre-dose) serum asparaginase activity(NSAA) levels and switching to intramuscular administration if desired NSAA levelsare not achieved with intravenous dosing.
®
2

There are differences between the U.S.-licensed product and Erwinase inthe Preparation and Handling Instructions (Appendix 2). Use therecommended handling instruction for U.S.-licensed asparaginase erwiniachrysanthemi.
Do not freeze or refrigerate reconstituted solution and administer within 4 hoursor discard.
There are differences between the U.S.-licensed product and Erwinase inthe format and content of the container and carton labelling.
The Erwinase carton includes an insert providing both the U.K. prescribinginformation (Summary of Product Characteristics) and information for the patient(package leaflet). See the bullet above regarding the recommended dosageinstructions for Erwinase.The vial label will display the text used and approved for marketing the product inU.K. Please see the product comparison tables at the end of this letter (Appendix1).The packaging of Erwinase does not include serialization information and does notmeet the product identifier requirements of section 582(b)(2) of the Federal Food,Drug and Cosmetic Act.
Ensure that your staff and others in your office and/or pharmacy who may be involvedin the prescribing and/or dispensing of Erwinase- asparaginase injection, powder,lyophilized, for solution receive a copy of this letter, review the information and instructpatients on the differences between Erwinase and U.S.-licensed asparaginase erwiniachrysanthemi.This letter and the attachments are not intended as a complete description of thebenefits and risks related to the use of Erwinase. See the full prescribing information onthe UK MHRA website at https://products.mhra.gov.uk/product/?product=ERWINASE%2010%20000%20UNITS%2FVIAL%20%20LYOPHILISATE%20FOR%20SOLUTION%20FOR%20INJECTIONContact Information:If you have any questions about the information contained in this letter, any qualityrelated problems, or questions on the use of Erwinase, please contact PortonBiopharma Limited via email [email protected] or contact directly at 1-855-209-2652.To place an order, contact McKesson Plasma and Biologics (MPB) directly at 1-877-625-2566.Adverse Events and Product Quality Complaints:Report adverse events associated with the use of Erwinase [email protected] via email or contact directly at 1-855-209-2652.Adverse events, medication errors or quality problems experienced with the use ofErwinase may also be reported to the FDA’s MedWatch Adverse Event ReportingProgram either online, regular mail, or by fax:
Complete and submit the report Online: www.fda.gov/medwatch/report.htmRegular Mail or Fax: Download form www.fda.gov/medwatch/getforms.htm or call 1-800-332-1088 to request a reporting form, then complete and return to the addresson the pre-addressed form, or submit by fax to 1-800-FDA-0178 (1-800-332-0178).
We remain at your disposal to answer any questions you may have about our productand to provide more information if needed.Yours sincerely,
Dr. Elizabeth Madichie Dr. Henno WelgemoedDirector of Regulatory Affairs &Pharmacovigilance
Director of Medical Affairs
Porton Biopharma Limited, U.K. Clinigen Group plc, U.K.
Enclosures:Appendix 1 – Product Label and Product Characteristics Side-by-Side Comparison TableAppendix 2 – Prescribing Information Side-by-Side Comparison TableAppendix 1 – Product Label and Product Characteristics Side-by-SideComparison Table
U.S. FDA Licensed Product Imported Product

Product Name Erwinaze - asparaginaseinjection, powder, lyophilized,for solution
Erwinase 10,000 IU/vialPowder for solution forinjection/infusion
Strength 10,000 International Units ina single-dose vial
10,000 IU/vial
Carton LabelImage
Vial LabelImage
Route ofAdministration
Erwinaze can be administeredintramuscularly or intravenously.
Erwinase solution can be given byintravenous infusion orintramuscular injection.
Ingredients Erwinaze is supplied as a sterile,lyophilized, white powder in vials.Each vial contains 10,000International Units ofasparaginase Erwiniachrysanthemi, and the followinginactive ingredients: glucosemonohydrate (5.0 mg), sodiumchloride (0.5 mg).
Crisantaspase (L-asparaginasefrom Erwinia chrysanthemi),10,000 International units/vial.List of excipientsSodium ChlorideGlucose Monohydrate
StorageConditions
Store unused or unopened vialsand cartons at 36°F to 46°F (2°Cto 8°C). Protect from light. Donot use Erwinaze after theexpiration date on the vial.
Store in a refrigerator (+2°C to+8°C).
Appendix 2 – Prescribing Information Side-by-Side Comparison TableA side-by-side comparison of the Erwinaze U.S. Prescribing Information (USPI) andErwinase U.K. Summary of Product Characteristics (SmPC) is provided below. It isimportant to note that there are no significant differences in the indications, dosage andadministration between the two products.Side-by-Side Comparison Table:
U.S. FDA Licensed Product Imported ProductProduct name Erwinaze®- asparaginase
injection, powder,lyophilized, for solution
Erwinase® 10,000 IU/vialPowder for solution forinjection/infusion
Indication 1 Indications and UsageERWINAZE is indicated as acomponent of a multi-agentchemotherapeutic regimen forthe treatment of patients withacute lymphoblastic leukemia(ALL) who have developedhypersensitivity to E. coliderived asparaginase.
4 Clinical Particulars4.1 Therapeutic indicationsErwinase is indicated as acomponent of achemotherapeutic regimen forthe treatment of patients withacute lymphoblastic leukaemia(ALL) who have developedhypersensitivity to E. coli-derivedasparaginase.
Erwinase is indicated in paediatricpatients from the age of
® ®

4 months and in adults.Dosage andadministration
2 Dosage andadministration2.1 Recommended DosageTo substitute for a dose ofpegaspargase:
The recommended dose foreach planned dose ofpegaspargase is 25,000International Units/madministered intramuscularly orintravenously three times aweek(Monday/Wednesday/Friday)for six doses.To substitute for a dose ofnative E. coli asparaginase:
The recommended dose is25,000 International Units/madministered intramuscularly orintravenously for eachscheduled dose of native E. coliasparaginase within atreatment.
When administering ERWINAZEintravenously, considermonitoring nadir (pre-dose)serum asparaginase activity(NSAA) levels and switching tointramuscular administration ifdesired NSAA levels are notachieved [see ClinicalPharmacology (12.3)].
4.2 Posology and method ofadministrationPosologyThe recommended dosage is20,000 or 25,000 IU/m bodysurface area administered threetimes a week (e.g.,Monday/Wednesday/Friday).
Therapy should be adjustedaccording to local treatmentprotocols.
2.2 Preparation andHandling Instructions
Visually inspect theERWINAZE powder forforeign particulate matterand discoloration prior toreconstitution. Discard vial ifpresent.Reconstitute the contents ofeach vial by slowly injecting 1or 2 mL of preservative freesterile sodium chloride(0.9%) injection (USP)against the inner vial wall.Do not forcefully injectsolution for reconstitutiondirectly onto or into thepowder. When reconstitutedwith 1 mL the resultantconcentration is 10,000International Units per mL.When reconstituted with2 mL the resultantconcentration is 5,000International Units per mL.Dissolve contents by gentlemixing or swirling. Do notshake or invert vial.When reconstituted,ERWINAZE should be aclear, colorless solution.Inspect the solution after
6.6 Special precautions fordisposal and other handlingThe contents of each vial shouldbe reconstituted in 1 mL to 2 mLof sodium chloride (0.9%)solution for injection.When reconstituted with 1 mLthe resultant concentration is10,000 IU/mL. Whenreconstituted with 2 mL theresultant concentration is 5,000IU/mL
Slowly add the sodium chloride(0.9%) solution for injection.against the inner vial wall, do notsquirt directly onto or into thepowder.
Allow the contents to dissolve bygentle mixing or swirlingmaintaining the vial in an uprightposition, avoiding contact of thesolution with the stopper. Avoidfroth formation due to excessiveor vigorous shaking.
The solution should be clearwithout any visible particles. Finecrystalline or thread-like wisps ofprotein aggregates may bevisible if shaking is excessive. Ifthere are any visible particles or
2
2
2

reconstitution and discard ifany visible particles orprotein aggregates arepresent.
there are any visible particles orprotein aggregates present thereconstituted solution should berejected.
Calculate the dose neededand the volume needed toobtain the calculated dose.Withdraw the volumecontaining the calculateddose from the vial into apolypropylene syringe within15 minutes ofreconstitution. Forintravenous use, slowlyinject the reconstitutedERWINAZE into an IVinfusion bag containing 100mL of normal salineacclimatized to roomtemperature. Do not shakeor squeeze the IV bag.If partial vial is used, do notsave or reuse the unuseddrug for later administration.Discard unused portions.Do not freeze or refrigeratereconstituted solution andadminister within 4 hours ordiscard [see HowSupplied/Storage andHandling (16)].
Erwinase is not a cytotoxicmedicinal product (such asvincristine or methotrexate) anddoes not require the specialprecautions needed formanipulating such agents. Itshould be handled in the sameway as other therapeuticenzymes such as hyaluronidase.
The solution should beadministered within 15 minutesof reconstitution. If a delay ofmore than 15 minutes betweenreconstitution and administrationis unavoidable, the solutionshould be withdrawn into a glassor polypropylene syringe for theperiod of the delay.
Any unused product or wastematerial should be disposed of inaccordance with localrequirements.The solution should be usedwithin 8 hours.
2.3 AdministrationInstructionsAdminister ERWINAZE in asetting with resuscitationequipment and other agentsnecessary to treat anaphylaxis.
ERWINAZE solution can beadministered by intramuscularinjection or by intravenousinfusion.
For intramuscular use, limitthe volume of reconstitutedERWINAZE at a singleinjection site to 2 mL; ifreconstituted dose to beadministered is greater than2 mL, use multiple injectionsites.For intravenous use, infuseERWINAZE in 100 mL ofnormal saline over 1 to 2hours. Do not infuse otherintravenous drugs throughthe same intravenous linewhile infusing ERWINAZE.
Method of administrationErwinase solution can be givenby intravenous infusion orintramuscular injection.
For IM injection the volume ofreconstituted solutionadministered at a single injectionsite should not exceed 2 mL.Multiple injection sites should beused if this volume is exceeded.
For IV infusion, the reconstitutedsolution should be further dilutedin 100 mL of normal saline andadministered over 1 to 2 hours.
For further instructions onreconstitution of the medicinalproduct before administration,see section 6.6.
Description 3 DOSAGE FORMS ANDSTRENGTHSFor injection: 10,000International Units as alyophilized powder in a single-
2 QUALITATIVE ANDQUANTITATIVECOMPOSITIONCrisantaspase (L-asparaginasefrom Erwinia chrysanthemi),

dose vial for reconstitution
11 DESCRIPTIONERWINAZE (asparaginaseErwinia chrysanthemi) containsan asparagine specific enzymederived from Erwiniachrysanthemi. L-asparaginaseis a tetrameric enzymeconsisting of four identicalsubunits, each having amolecular weight of about 35kDa. The activity of ERWINAZEis expressed in terms ofInternational Units.
ERWINAZE is supplied as asterile, lyophilized, whitepowder in vials. Each vialcontains 10,000 InternationalUnits of asparaginase Erwiniachrysanthemi, and the followinginactive ingredients: glucosemonohydrate (5.0 mg), sodiumchloride (0.5 mg).
10,000 International units/vial.For a full list of excipients, seesection 6.1.
3. PHARMACEUTICAL FORMPowder for solution forinjection/infusion.
White lyophilised powder in a vial.
6.1 List of excipientsSodium Chloride (0.5 mg)Glucose Monohydrate (5.0 mg)
Contraindications 4 CONTRAINDICATIONSERWINAZE is contraindicated inpatients with a history of:
Serious hypersensitivityreactions to ERWINAZE,including anaphylaxisSerious pancreatitis withprior L-asparaginase therapySerious thrombosis withprior L-asparaginase therapySerious hemorrhagic eventswith prior L-asparaginasetherapy
4.3 ContraindicationsHistory of severehypersensitivity to the activesubstance or to any of theexcipients listed in section 6.1Current or past severepancreatitis associated withL‑asparaginase therapyCurrent pancreatitis notassociated withL‑asparaginase therapy
Precautions 5 WARNINGS ANDPRECAUTIONS
4.4 Special warnings andprecautions for useIn order to improve traceabilityof biological medicinal products,the tradename and batchnumber of the administeredproduct should be clearlyrecorded (or stated) in thepatient file.
5.1 HypersensitivityReactionsGrade 3 and 4 hypersensitivityreactions after the use ofERWINAZE have occurred in5% of patients in clinical trials[see Adverse Reactions (6.1)].
Hypersensitivity reactionsAdministration of Erwinase cancause hypersensitivity reactions(infusion/injection reactions),including reactions presenting asanaphylaxis.Severe reactions are common.Reactions have occurredfollowing the first or subsequentadministrations.There is little or no cross-reactivity between crisantaspaseand E. coli-derived L-asparaginase.Reactions include
reactions limited to the area ator near the site of IM or IVadministration, andother reactions, including
reactions with symptoms

consistent with ananaphylactic reaction, andreactions accompanied byfever (see section 4.8).
Reactions can begin during orimmediately followingadministration. In the majority ofpatients, local and non-localreactions occur within the first24 hours. Later onset ofreactions has been reported twodays or later after IMadministration.
Administer this product in asetting with resuscitationequipment and other agentsnecessary to treat anaphylaxis.If a serious hypersensitivityreaction occurs, discontinueERWINAZE and initiateappropriate therapy.
Facilities should be madeavailable for management of ananaphylactic reaction, should itoccur, during administration. If asevere reaction occurs, Erwinasemust be discontinued (seesection 4.3).
Careful observation is requiredon re-exposure to L-asparaginase after any timeinterval (e.g. between inductionand consolidation), which mayincrease the risk of anaphylacticand hypersensitivity reactionsoccurring.
5.2 PancreatitisPancreatitis has been reportedin 4% of patients in clinical trials[see Adverse Reactions (6.1)].
Evaluate patients withsymptoms compatible withpancreatitis to establish adiagnosis. DiscontinueERWINAZE for severe orhemorrhagic pancreatitismanifested by abdominal pain >72 hours and amylase elevation≥ 2.0 x ULN. Severepancreatitis is acontraindication to additionalasparaginase administration. Inthe case of mild pancreatitis,hold ERWINAZE until the signsand symptoms subside andamylase levels return to normal.After resolution, treatment withERWINAZE may be resumed.
PancreatitisTreatment with L-asparaginase,including Erwinase, can causepancreatitis. L-asparaginase-induced pancreatitis can belimited to biochemical and/orradiologic manifestations,progress to pancreatitis withclinical symptoms, and be severe(see section 4.8).
Fatal outcome of pancreatitis dueto L-asparaginase products,including Erwinase, has beenreported.
Patients must be closelymonitored for signs andsymptoms of pancreatic toxicityand instructed to promptlyreport potential symptoms ofpancreatitis. If pancreatitis issuspected based on clinicalsymptoms, serum amylase andlipase should be determined. Inpatients treated with L-asparaginase, increases ofserum amylase and lipase maybe delayed, mild or absent.
Erwinase must be permanentlydiscontinued in case of severepancreatitis (see section 4.3).Hypertriglyceridemia, if marked,can contribute to thedevelopment of pancreatitis (seesection 4.8).
There have been isolated reports

of first onset of clinicalpancreatitis and detection ofpancreatic pseudocyst formationseveral months after the lastadministration of L-asparaginase.Patients must be monitored forlate-occurring signs ofpancreatitis.
Development of chronicpancreatitis as well as persistentpancreatic insufficiency (exocrineinsufficiency with, e.g.,malabsorption; persistentglucose intolerance/diabetesmellitus) has been reported withL- asparaginase treatment.
5.3 Glucose IntoleranceGlucose intolerance has beenreported in 5% of patientsreceiving ERWINAZE in clinicaltrials [see Adverse Reactions(6.1)]. In some cases, glucoseintolerance may be irreversible.Monitor glucose levels inpatients at baseline andperiodically during treatment.Administer insulin therapy asnecessary in patients withhyperglycemia.
Glucose IntoleranceTreatment with L-asparaginase,including Erwinase, can causeglucose intolerance andpotentially severe hyperglycemia.
In some patients, ketoacidosishas been reported.
Patients must be monitored fordeveloping hyperglycemia andpotential complications.
Administration of insulin andpossibly discontinuation ofL‑asparaginase treatment maybe necessary to managehyperglycemia.
5.4 Thrombosis andHemorrhageSerious thrombotic events,including sagittal sinusthrombosis and pulmonaryembolism have been reportedwith both E. coli and Erwinia-derived L-asparaginasetherapy. The followingcoagulation proteins weredecreased in the majority ofpatients after a 2-week courseof ERWINAZE by intramuscularadministration: fibrinogen,protein C activity, protein Sactivity, and anti-thrombin III.Discontinue ERWINAZE for athrombotic or hemorrhagicevent until symptoms resolve;after resolution, treatment withERWINAZE may be resumed.
Coagulation DisordersAdministration of L-asparaginase, includingErwinase, leads to decreasedsynthesis of coagulant,anticoagulant, and fibrinolyticproteins, abnormal coagulationtimes, and clinical coagulationabnormalities that can causeserious thromboembolic andbleeding events (see section4.8).Routine clotting screening shouldbe performed before treatmentinitiation and monitored duringtreatment. Preventive measuresmust be considered.
If significant symptomaticcoagulopathy occurs in additionto other clinically indicatedinterventions withhold Erwinasetreatment until resolved.Treatment may then continueaccording to protocol, if thebenefit of continuedadministration is considered tooutweigh the risk from re-exposure.
Adversereactions
6 ADVERSE REACTIONSThe following clinicallysignificant adverse reactionsare discussed in greater detail
4.8 Undesirable effectsa. Summary of the safety profileThe two most frequent adversereactions are:

in other sections of the label:Hypersensitivity reactions[see Warnings andPrecautions (5.1)]Pancreatitis [see Warningsand Precautions (5.2)]Glucose intolerance [seeWarnings and Precautions(5.3)]Thrombosis andhemorrhage [see Warningsand Precautions (5.4)]
• Hypersensitivity, includingurticaria, fever, arthralgiaangioedema, bronchospasm,hypotension or evenanaphylactic shock. In case ofsevere systemic hypersensitivityreaction, treatment should bediscontinued immediately andwithdrawn.• Coagulation abnormalities (e.g.thromboses), due to proteinsynthesis impairment, are thesecond most frequent class ofadverse reactions. Thrombosesof peripheral, pulmonary orcentral nervous system bloodvessels have been reported,potentially fatal or with residualdelayed affects dependent uponthe location of the occlusion.Other risk factors contributing tocoagulation abnormalities includethe disease itself, concomitantsteroid therapy and centralvenous catheters.
Undesirable effects are generallyreversible.
6.1 Clinical Trials ExperienceBecause clinical trials areconducted under controlled,but widely varying conditions,adverse reaction ratesobserved in clinical trials ofERWINAZE cannot be directlycompared to rates in the clinicaltrials of other drugs and maynot reflect the rates observedin practice.
The data presented below arebased on information collectedfrom Study 1, a single-arm,multi-center, open-label, safetyand clinical pharmacology trial(intramuscular administration),the ERWINAZE MasterTreatment Protocol (EMTP), anexpanded access program(both intramuscular,intravenous, and other orunknown administration), andStudy 2, a single-arm, multi-center, open-label,pharmacokinetic (PK) study trialof intravenous administration ofERWINAZE.
Study 1 enrolled 58 patientstreated on National CancerInstitute (NCI)-sponsoredcooperative group ALLprotocols who were unable tocontinue to receivepegaspargase due tohypersensitivity reactions.Patients received 6 doses ofERWINAZE 25,000International Units/m
b. Tabulated list of adversereactionsThe adverse reaction datapresented in Table 1 have beenidentified from 3 clinical studies(100EUSA12, ALL07P2, andErwinase Master TreatmentProtocol [EMTP]) with Erwinase in1028 patients (primarily pediatricpatients), the majority havingacute lymphoblastic leukemia, aswell as post-marketingexperience with Erwinase andother L‑asparaginasepreparations in pediatric andadult patients.
Some of the adverse reactionslisted below are known to beassociated with multi-agentchemotherapeutic regimens(e.g., reactions resulting frombone marrow depression, andinfections), and the contributoryrole of Erwinase is not clear. Inindividual cases of other adversereactions, other medicinalproducts of the regimen mayhave contributed.
Frequency definitions: verycommon (≥1/10), common(≥1/100 to <1/10), uncommon(≥1/1000 to <1/100), rare(≥1/10000 to <1/1000) and veryrare (<1/10000).When no validestimate of the incidence rate foran adverse event from availabledata can be calculated, thefrequency of such ADR has beenclassified as “Not known”.2

intramuscularly on a Monday,Wednesday, and Fridayschedule as a replacement foreach scheduled dose ofpegaspargase remaining ontheir original treatmentprotocol. The Study 1population included patientswith a median age of 11 years(2 to 18 years); 59% weremale, 78% were White, 10%were Black/African American,5% were Asian, and 7% wereother or unknown. A total of35% were Hispanic or Latino. InStudy 1, the number ofERWINAZE courses rangedfrom 1 to 9. In this study, 76%(44 of 58) completed allplanned therapy.Fourteen (24%) patientsstopped therapy prior tocompletion; seven due toallergic reactions, five due tophysician or patient choice, onedue to disease progression,and one due to discontinuationduring frontline protocol. Allother chemotherapy wascontinued according to thepatient’s prescribed treatmentregimen [see Clinical Studies(14)].
Study 2 enrolled 30 patients [29were being treated for ALL andone for lymphoblasticlymphoma (LBL)] followingallergy to native E. coliasparaginase or pegaspargase.Patients received ERWINAZE25,000 International Unit/m/dose, administered byintravenous infusion on aMonday, Wednesday, andFriday schedule (6 doses) as areplacement for dosesremaining on their originaltreatment plan. The Study 2population included patientswith a median age of 7 years (1to 17 years); 63% were male,27% were Hispanic or Latino,83% were White, 3% wereBlack/African American, 7%were Asian, and 7% were other(American Indian, Alaska Nativeor Indian) [see Clinical Studies(14)].The EMTP trial enrolled 1368patients with ALL orlymphoblastic lymphoma whoreceived ERWINAZE afterdeveloping systemichypersensitivity to an E. coli-derived asparaginase. Of these1368 patients, safety data werereceived for 940 patients with amedian age of 9 years (0 to 76years), 63% were male, 91%
Posterior reversibleencephalopathy syndromeIn rare cases, a posteriorreversible encephalopathysyndrome (PRES) has beenobserved during therapy withasparaginase-containingregimens.

with leukemia, 3% withlymphoma, and 6% withunknown disease information.Patients received ERWINAZEaccording to several schedules,and treatment centerspecifications with doses thatranged from 20,000 to 25,000International Units/m . Theroute of administration wasintramuscular n=852,intravenous n=29, other orunknown n=59. In the EMTPtrial, the planned number ofdoses of ERWINAZE rangedfrom 3 to 48 doses. Seventy-eight percent of patients (693of 893) were able to receive allplanned doses to completetheir prescribed treatmentregimen.
In Study 1 and Study 2, safetyinformation was prospectivelyand systematically collected. InStudy 1, all Grades of adverseevents were reported for thefollowing adverse events ofspecial interest: allergy,pancreatitis, coagulopathy(hemorrhage, thrombosis orinfarct), hyperbilirubinemia,hyperglycemia, hyperlipidemia,ketoacidosis, and CNS events(hemorrhage, thrombosis orinfarction, and cerebral venousthrombosis) and only Grade 3and 4 events were reported forother adverse events. In Study2 all adverse events of allGrades were prospectivelycollected. In the EMTP trial,safety data were derived fromcase report forms thatcollected adverse eventinformation. The formsspecifically requestedinformation on occurrence ofallergic reactions, thromboticevents, hemorrhagic events,hepatobiliary disorders,pancreatic disorders, andhyperglycemia.
The most common adversereactions (incidence 1% orgreater) with ERWINAZEtreatment are systemichypersensitivity, hyperglycemia,transaminases abnormal, fever,pancreatitis, local reactions,vomiting, nausea, thrombosis,hyperbilirubinemia, abdominalpain/discomfort, and diarrhea.
The incidence of non-hematologic, non-infectious,adverse events (all Grades) inStudy 1, Study 2, and the EMTPtrial is provided in Table 1.
2

trial is provided in Table 1.
The incidence of Grade 3 orgreater non-hematologic, non-infectious adverse reactionsoccurring with ERWINAZE inStudy 1, Study 2 and EMTP trialis provided in Table 2.
6.2 ImmunogenicityAs with all therapeutic proteins,there is potential forimmunogenicity. The detectionof antibody formation is highlydependent on the sensitivityand specificity of the assay.Additionally, the observedincidence of antibody (includingneutralizing antibody) positivityin an assay may be influencedby several factors includingassay methodology, samplehandling, timing of samplecollection, concomitantmedications, and underlyingdisease. For these reasons,comparison of the incidence ofantibodies in other studies or toother asparaginase Erwiniachrysanthemi products may bemisleading.
In a study with ERWINAZEtreatment by intramuscularadministration (Study 1), 6 of56 (11%) patients treated withERWINAZE developedantibodies to ERWINAZE. Ofthese 6 anti-drug antibody(ADA) positive patients, oneexperienced a hypersensitivityreaction during Study 1 (2%, 1of 56). None of these 6 patientshad neutralizing antibodies.
In a study with ERWINAZEtreatment by intravenousadministration (Study 2), 4 of30 (13.3%) patients treatedwith ERWINAZE developed anti-ERWINAZE antibodies. Of these
ImmunogenicityAs with most therapeuticproteins, patients may potentiallydevelop anti-drug antibodies(ADA) to crisantaspase.
Immunogenicity assays arehighly dependent on thesensitivity and specificity of theassay and may be influenced byseveral factors such as: assaymethodology, sample handling,timing of sample collection,concomitant medications, andunderlying disease. For thesereasons, comparison of theincidence of antibodies tocrisantaspase with the incidenceof antibodies to other productsmay be misleading.
In a study with Erwinasetreatment by IM administration(Study ALL07P2), 6 of 56 (11%)patients treated with Erwinasedeveloped antibodies tocrisantaspase. Of these 6 ADApositive patients, oneexperienced a hypersensitivityreaction (2%, 1 of 56). None ofthese 6 patients had neutralisingantibodies.
In a study with Erwinasetreatment by IV administration(Study 100EUSA12), 4 of 30(13.3%) patients treated withErwinase developed anti-crisantaspase antibodies. Ofthese 4 patients, 3 experiencedhypersensitivity reactions (10%,3 of 30). None of these 4

ERWINAZE antibodies. Of these4 patients who developed anti-ERWINAZE antibodies, 3experienced hypersensitivityreactions (10%, 3 of 30) duringthe study. None of these 4patients had neutralizingantibodies.
The presence of ADA toERWINAZE is associated with ahigher risk of hypersensitivityreactions in patients whoreceived ERWINAZE throughintravenous infusion comparedto intramuscular administrationof ERWINAZE.
3 of 30). None of these 4patients had neutralisingantibodies
Neutralising antibodiesAs with other L-asparaginasepreparations, development ofspecific neutralising antibodieshas been reported with repeateddosing and is associated withreduced L-asparaginase activity.
Reporting of suspected adversereactionsReporting suspected adversereactions after authorisation ofthe medicinal product isimportant. It allows continuedmonitoring of the benefit/riskbalance of the medicinal product.Healthcare professionals areasked to report any suspectedadverse reactions via Yellow CardScheme Website:www.mhra.gov.uk/yellowcard orsearch for MHRA Yellow Card inthe Google Play or Apple AppStore.
Druginteractions
Note: The following informationis provided in the USPI undersection 12.3 Pharmacokinetics
Drug Interaction StudiesNo formal drug interactionstudies between ERWINAZEand other drugs have beenperformed
4.5 Interaction with othermedicinal products and otherforms of interaction
No formal medicinal productinteraction studies have beenperformed.
Asparaginase must not be mixedwith any other medicinalproducts prior to administration.
In addition concomitant use of L-asparaginase and medicinalproducts affecting liver functionmay increase the risk of achange in liver parameters (e.g.increase of ASAT, ALAT,bilirubin).
Since an indirect interactionbetween components of the oralcontraception and asparaginasecannot be ruled out, oralcontraceptives are notconsidered sufficiently safe insuch clinical situation. Anothermethod than oral contraceptionshould be used in women ofchildbearing potential (seesection 4.6).
• Methotrexate, cytarabineL-asparaginase may diminish orabolish methotrexate’s andcytarabine’s effect on malignantcells; this effect persists as longas plasma asparagine levels aresuppressed. Accordingly, do notuse methotrexate or cytarabinewith, or following L-asparaginase,
while asparagine levels are belownormal.
Alternatively, administration of L-asparaginase after methotrexateor cytarabine results in asynergistic effect. The extent towhich these affect the overalleffectiveness of establishedtreatment protocols is notknown.
• PrednisoneConcomitant use of prednisoneand L-asparaginase may increasethe risk of a change in clottingparameters (e.g. a decrease infibrinogen and ATIII levels).
• VincristineAdministration of vincristineconcurrently with or immediatelybefore treatment with L-asparaginase may be associatedwith increased toxicity andincreased risk of anaphylaxis.
Specialpopulations
8 USE IN SPECIFICPOPULATIONS8.1 PregnancyRisk SummaryBased on findings from animalreproduction studies,ERWINAZE can cause fetalharm when administered to apregnant woman. In animalreproduction studies,intramuscular administration ofasparaginase Erwiniachrysanthemi to pregnant ratsand rabbits duringorganogenesis at dosesapproximately 0.005-0.5 timesthe maximum recommendedhuman dose resulted instructural abnormalities andembryo-fetal mortality (seeData). There are no availabledata on ERWINAZE use inpregnant women to evaluatethe drug-associated risk ofmajor birth defects, miscarriageor adverse maternal or fetaloutcomes. Advise pregnantwomen of the potential risk tothe fetus.
The estimated background riskof major birth defects andmiscarriage for the indicatedpopulation is unknown. Adverseoutcomes in pregnancy occurregardless of the health of themother or the use ofmedications. In the U.S. generalpopulation, the estimatedbackground risks of major birthdefects and miscarriage inclinically recognizedpregnancies are 2 to 4% and
4.6 Fertility, pregnancy andlactationPregnancyThere are no adequate data fromthe use of crisantaspase (ErwiniaL-asparaginase) in pregnantwomen. Limited reports inhumans of the use of E. coliasparaginase in combination withother antineoplastics duringpregnancy did not providesufficient data to conclude.However, based on effects onembryonal/foetal developmentshown in pre-clinical studies (seesection 5.3),Erwinase should not be usedduring pregnancy unless thepotential benefit justifies thepotential risk to the fetus.

15 to 20%, respectively.DataAnimal DataIn embryofetal developmentstudies, asparaginase Erwiniachrysanthemi was administeredintramuscularly every other dayduring the period oforganogenesis to pregnant rats(at 3000, 6000, or 12000IU/m ) and rabbits (at 120,300, or 480 IU/m ). In ratsgiven 12000 IU/m(approximately 0.5 times themaximum recommendedhuman dose), maternal toxicityof decreased body weight gainwas observed, as well as a fetalfinding of increased incidenceof partially undescended thymictissue.
In rabbits, maternal toxicityconsisting of decreased bodyweight was observed at 480IU/m (approximately 0.02times the maximumrecommended human dose).Increased post-implantationloss, a decrease in the numberof live fetuses, and grossabnormalities (e.g., absentkidney, absent accessory lunglobe, additional subclavianartery, and delayed ossification)were observed at doses of≥120 IU/m (approximately0.005 times the maximumrecommended human dose).
FertilityThere are no human data on theeffect of crisantaspase onfertility. In rats, crisantaspase didnot affect male and femalefertility. However, a decrease insperm count was observed inmale rats (see section 5.3). Therelevance of this finding tohumans is not known.
8.2 LactationRisk SummaryThere are no data on thepresence of asparaginaseErwinia chrysanthemi in humanor animal milk, the effects onthe breastfed child, or theeffects on milk production.Because of the potential forserious adverse reactions in thebreastfed child, advise patientsthat breastfeeding is notrecommended duringtreatment with ERWINAZE, andfor 3 months after the lastdose.
Breast feedingIt is not known whethercrisantaspase (Erwinia L-asparaginase) is excreted inhuman breast milk. Potentialserious adverse reactions mayoccur in nursing infants,therefore Erwinase should bediscontinued during breast-feeding.
8.3 Females and Males ofReproductive PotentialPregnancy TestingPregnancy testing isrecommended for females ofreproductive potential beforestarting ERWINAZE treatment.
ContraceptionFemalesERWINAZE can cause embryo-fetal harm when administeredto pregnant women [see Use in
Women of childbearingpotential/Contraception in malesand femalesWomen of childbearing potentialshould use effectivecontraception and avoidbecoming pregnant while beingtreated with asparaginase-containing chemotherapy.
Since an indirect interactionbetween components of the oralcontraception and asparaginase
222
2
2

Specific Populations (8.1)].Advise females of reproductivepotential to use effectivecontraception during treatmentwith ERWINAZE and for 3months after the final dose.Since an indirect interactionbetween oral contraceptivesand ERWINAZE cannot be ruledout, a method of contraceptionother than oral contraceptivesshould be used in women ofchildbearing potential.
cannot be ruled out, oralcontraceptives are notconsidered sufficiently safe insuch clinical situation. A methodother than oral contraceptivesshould be used in women ofchildbearing potential.
Men should use effectivecontraceptive measures and beadvised to not father a child whilereceiving asparaginase.
The time period followingtreatment with asparaginasewhen it is safe to becomepregnant or father a child isunknown. As a precautionarymeasure it is recommended towait for three months aftercompletion of treatment.However, treatment with otherchemotherapeutic agents shouldalso be taken into consideration.
8.4 Pediatric UseThe safety and effectiveness ofERWINAZE have beenestablished in pediatric patientsages1 year and older as acomponent of a multi-agentchemotherapeutic regimen forthe treatment of patients withacute lymphoblastic leukemia(ALL) who have developedhypersensitivity to E. coli-derived asparaginase and theinformation on this use isdiscussed throughout thelabeling.
d. Pediatric populationCompared with children, theincidence of hepatic andpancreatic toxicities and ofvenous thromboembolic eventsmay be increased in adolescentsand young adults.
8.5 Geriatric UseClinical studies of ERWINAZEdid not include geriatricpatients.
e. Other special populationsNo special individual populationsof patients have been identified inwhich the safety profile differsfrom that defined above.
Overdosage There are no correspondingclinical data for ErwinazeUSPI
4.9 OverdoseThere is no known antidote forasparaginase overdoses. Nodata are available on theelimination (peritoneal or byhaemodialysis) of the product.Patients who accidentally receivean overdose of L-asparaginaseshould be monitored closely andreceive any appropriatesymptomatic and supportivetreatment.
12 CLINICALPHARMACOLOGY
5. PHARMACOLOGICALPROPERTIES5.1 PharmacodynamicpropertiesPharmacotherapeutic group:other antineoplastic agents ATCcode: L01XX02
12.1 Mechanism of ActionAsparaginase Erwiniachrysanthemi catalyzes thedeamidation of asparagine to
Mechanism of actionL-asparaginase catalyses thedeamination of asparagine toaspartic acid with the release of

aspartic acid and ammonia,resulting in a reduction incirculating levels of asparagine.The mechanism of action ofERWINAZE is thought to bebased on the inability ofleukemic cells to synthesizeasparagine due to lack ofasparagine synthetase activity,resulting in cytotoxicity specificfor leukemic cells that dependon an exogenous source ofamino acid asparagine for theirprotein metabolism andsurvival.
ammonia.
Asparagine is an amino acidfound incorporated into mostproteins, and protein synthesis ishalted in its absence, therebyinhibiting RNA and DNA synthesiswith a resulting halt to cellularproliferation.
As lymphoblastic cells are lackingasparagine synthetase activitythey are dependent uponexogenous asparagine. The anti-tumour activity of L-asparaginase is a result of thesustained depletion ofexogenous asparagine.
It has also been noted thatasparaginase, in addition to itsasparaginase activity, hassignificant glutaminase activity. Itcatalyses the deamination ofglutamine in glutamic acid withthe release of ammonia.
Glutamine may lead to alternativeasparagine synthesis andtherefore glutamine depletionmay complement asparaginedepletion. However, exactpotential of this glutaminaseactivity remains unknown.
12.3 PharmacokineticsBased on a population PKmodel, the mean (%CV) half-lifeof intravenous ERWINAZE was7.51 (23.9%) hours in contrastto a mean (%CV) half-life of15.6 (20%) hours reported forintramuscular ERWINAZE.These differences in PKbetween intravenous andintramuscular ERWINAZE arereflected in the proportion ofpatients with 2-day and 3-daynadir serum asparaginaseactivity (NSAA) levels ofasparaginase Erwiniachrysanthemi ≥ 0.1 or 0.4IU/mL [see Clinical Studies (14)].
Following administration ofERWINAZE 25,000International Units/mintramuscularly to 48 ALLpatients aged ≥ 2 years to ≤18 years in Study 1 on aMonday, Wednesday, andFriday schedule for 6 doses,100% of patients whocompleted Course 1 achievedNSAA levels ≥ 0.1 InternationalUnits/mL at either 48 hours(n=35) or 72 hours (n=13)post dose 3. Eighty percent(28/35) of those evaluated at48 hours and 38% (5/13)
5.2 PharmacokineticpropertiesBased on a population PK model,the mean (%CV) half-life ofcrisantaspase is 7.5 (24%) hoursafter intravenous infusion incontrast to 15.6 (20%) hoursafter intramuscular injection. L-asparaginase penetrates throughto the cerebrospinal fluid to asmall degree and is also found inlymph.
Serum trough asparaginaseactivity ≥ 0.1 U/mL has beendemonstrated to correlate withasparagine depletion (asparagine< 0.4 mcg/mL or 3 μM) and toserum levels that predict clinicalefficacy.
Clinical trialsStudy 1 (AALL07P2) was asingle-arm, multicentre, open-label, safety and clinicalpharmacology trial, whichenrolled ALL patients who wereunable to continue to receivepegaspargase due tohypersensitivity reactions. Themain outcome measure was theproportion of patients whoachieved a serum troughasparaginase level ≥ 0.1IU/mL, which correlates with
2

evaluated at 72 hours had nadirserum asparaginase activitylevels ≥ 0.4 InternationalUnits/mL [see Clinical Studies(14)].
Following intravenousadministration of ERWINAZE25,000 International Units/mto 24 evaluable patients (aged≥ 1 year to ≤ 17 years) inStudy 2 on a Monday,Wednesday, and Fridayschedule, 83% (20/24) and43% (9/21) of patients whocompleted Course 1 achievedNSAA levels ≥ 0.1 InternationalUnits/mL at 48 hours post-dose5 and 72 hours post dose 6,respectively. Twenty-ninepercent (7/24) of thoseevaluated at 48 hours and nopatients (0/21) evaluated at 72hours had nadir serumasparaginase activity levels ≥0.4 International Units/mL [seeClinical Studies (14)].
Drug Interaction StudiesNo formal drug interactionstudies between ERWINAZEand other drugs have beenperformed
asparagine depletion andpredicts clinical efficacy. Patientsreceived Erwinase 25,000 IU/mintramuscularly for two weeks(total 6 doses) as a replacementfor each scheduled dose ofpegaspargase.
Out of 58 patients enrolled, 48were evaluable for the mainoutcome measure in the firsttreatment course. The medianage was 11 years (2 to 18 years)and 59% were male.
Study 2 (100EUSA12) was asingle-arm, multicentrepharmacokinetic study inpatients with ALL/LBL who haddeveloped hypersensitivity tonative E. coli asparaginase,pegaspargase, or calaspargasepegol. Patients received Erwinase25,000 IU/m intravenously 3days per week for up to 30weeks. The main outcomemeasure was the proportion ofpatients with 2-day nadir serumasparaginase activity (NSAA)levels after the fifth dose ≥ 0.1IU/mL.
Out of 30 patients enrolled, 24were evaluable for the mainoutcome measure in the firsttreatment course. The medianage was 7 years (1-17 years)and 63% were male.The results of the two studiesare presented in the table below.Proportion of patients withsustained asparaginase activity
Neutralising antibodiesAs with other L-asparaginasepreparations, development ofspecific neutralising antibodieshas been reported with repeateddosing and is associated withreduced L-asparaginase activity.
Cerebrospinal fluid activityAfter IM administration of 25,000IU/m Erwinase per week for 16weeks, CSF L-asparagine levelswere undetectable 3 days afterlast administration in 5 of 8children (62.5%), and in 2 of 8children (25%) after both the 5thand 6th administration duringreinforced re-induction therapy.
Carcinogenesis,Mutagenesis,Impairment of
13 NONCLINICALTOXICOLOGY13.1 Carcinogenesis,
5.3 Preclinical safety dataAdverse reactions not observedin clinical studies, but seen in
2
2
2
2

Fertility Mutagenesis, Impairmentof FertilityNo long-term carcinogenicitystudies in animals have beenperformed with asparaginaseErwinia chrysanthemi. Nostudies that assess themutagenic potential ofasparaginase Erwiniachrysanthemi have beenconducted.
In a fertility and early embryonicdevelopment study in rats,asparaginase Erwiniachrysanthemi had no effect onmale or female fertility whenadministered intramuscularly atdoses of up to 12000 IU/m(approximately 0.50 times themaximum recommendedhuman dose) every other dayfor a total of 35 doses. Findingsin males included decreasedsperm count at doses of morethan 3000 IU/m(approximately 0.12 times themaximum recommendedhuman dose).
animals at exposure levels similarto clinical exposure levels andwith possible relevance to clinicaluse were as follows:
Reproduction and developmenttoxicityEmbryotoxicity studies withErwinia L-asparaginase havegiven evidence of teratogenicpotential in rabbits. In addition,pre-clinical experience with otherasparaginase preparations hasshown teratogenic potential inrats, mice and rabbits with dosesin the therapeutic ranges.
In a fertility and early embryonicdevelopment study in rats, IMadministration of crisantaspasehad no effect on male and femalefertility at doses approximately50% of the recommendedhuman dose (based on bodysurface area). However, a 12 to15% decrease in sperm countwas observed at dosesapproximately 12 to 50% of therecommended human dose.
CarcinogenicityNon-clinical studies have notbeen conducted to evaluate thecarcinogenic or mutagenicpotential of crisantaspase.Crisantaspase is an enzyme forwhich the structure and welldocumented activity do notsuggest any carcinogenic ormutagenic potential.
Clinical data 14 CLINICAL STUDIESThe efficacy of ERWINAZE forthe treatment of patients withacute lymphoblastic leukemia(ALL) who have developedhypersensitivity to E. Coli-derived asparaginase as acomponent of a multi-agentchemotherapeutic regimen wasestablished in Study 1, a single-arm, multi-center, open-label,safety and clinicalpharmacology trial. Additionalsafety data were obtained inthe ERWINAZE MasterTreatment Protocol (EMTP), anexpanded access program [seeAdverse Reactions (6)]. Study 1enrolled patients treated onNational Cancer Institute (NCI)-sponsored cooperative groupALL protocols who were unableto continue to receivepegaspargase due tohypersensitivity reactions. Themain outcome measure wasdetermination of the proportionof patients who achieved aserum trough asparaginase
5.2 PharmacokineticpropertiesBased on a population PK model,the mean (%CV) half-life ofcrisantaspase is 7.5 (24%) hoursafter intravenous infusion incontrast to 15.6 (20%) hoursafter intramuscular injection. L-asparaginase penetrates throughto the cerebrospinal fluid to asmall degree and is also found inlymph.
Serum trough asparaginaseactivity ≥ 0.1 U/mL has beendemonstrated to correlate withasparagine depletion (asparagine< 0.4 mcg/mL or 3 μM) and toserum levels that predict clinicalefficacy.
Clinical trialsStudy 1 (AALL07P2) was asingle-arm, multicentre, open-label, safety and clinicalpharmacology trial, whichenrolled ALL patients who wereunable to continue to receivepegaspargase due to
2
2

level greater than or equal to0.1 International Units/mL.Serum trough asparaginaseactivity ≥ 0.1 InternationalUnits/mL has beendemonstrated to correlate withasparagine depletion(asparagine < 0.4 mcg/mL or 3μM) and to serum levels thatpredict clinical efficacy. Patientsreceived ERWINAZE 25,000International Units/mintramuscularly for two weeks(total 6 doses) as areplacement for eachscheduled dose ofpegaspargase remaining ontheir original treatmentprotocol.
Fifty-eight patients wereenrolled in Study 1, of these 48were evaluable for the mainoutcome measure based onavailability of pharmacokineticsamples in Course 1. Themedian age was 11 years (2 to18 years); 59% were male, 78%were White, 10% wereBlack/African American, 5%were Asian, and 7% were otheror unknown. A total of 35%were Hispanic or Latino.
Study 1 met its main outcomemeasure of demonstrating thatgreater than 50% of thepatients achieved the pre-specified trough asparaginaseactivity level of ≥ 0.1International Units/mL at 48 or72 hours following the thirddose. Results for the mainoutcome measure and for anexploratory analysis using ahigher cut-off (trough serumasparaginase activity levels ≥0.4 International Units/mL arepresented in Table 3 [seeClinical Pharmacology (12.3)].
The safety and efficacy ofintravenous administrationwere determined in Study 2 bycharacterizing the PK of a25,000 International Units/mERWINAZE dose given 3 daysper week on a Monday,Wednesday, and Fridayschedule for up to 30 weeks.This open-label, single-arm,multicenter PK study enrolled30 patients. The main outcomemeasure was determination ofthe proportion of patients with2-day NSAA levels (48-hourlevels taken after the fifth dose)≥ 0.1 International Unit/mL inthe first 2 weeks of ERWINAZEtreatment.
hypersensitivity reactions. Themain outcome measure was theproportion of patients whoachieved a serum troughasparaginase level ≥ 0.1IU/mL, which correlates withasparagine depletion andpredicts clinical efficacy. Patientsreceived Erwinase 25,000 IU/mintramuscularly for two weeks(total 6 doses) as a replacementfor each scheduled dose ofpegaspargase.
Out of 58 patients enrolled, 48were evaluable for the mainoutcome measure in the firsttreatment course. The medianage was 11 years (2 to 18 years)and 59% were male.
Study 2 (100EUSA12) was asingle-arm, multicentrepharmacokinetic study inpatients with ALL/LBL who haddeveloped hypersensitivity tonative E. coli asparaginase,pegaspargase, or calaspargasepegol. Patients received Erwinase25,000 IU/m intravenously 3days per week for up to 30weeks. The main outcomemeasure was the proportion ofpatients with 2-day nadir serumasparaginase activity (NSAA)levels after the fifth dose ≥ 0.1IU/mL.
Out of 30 patients enrolled, 24were evaluable for the mainoutcome measure in the firsttreatment course. The medianage was 7 years (1-17 years)and 63% were male.
The results of the two studiesare presented in the table below.Proportion of patients withsustained asparaginase activity
Cerebrospinal fluid activityAfter IM administration of 25,000IU/m Erwinase per week for 16weeks, CSF L-asparagine levelswere undetectable 3 days afterlast administration in 5 of 8children (62.5%), and in 2 of 8children (25%) after both the 5thand 6th administration duringreinforced re-induction therapy.
2
2
2
2
2
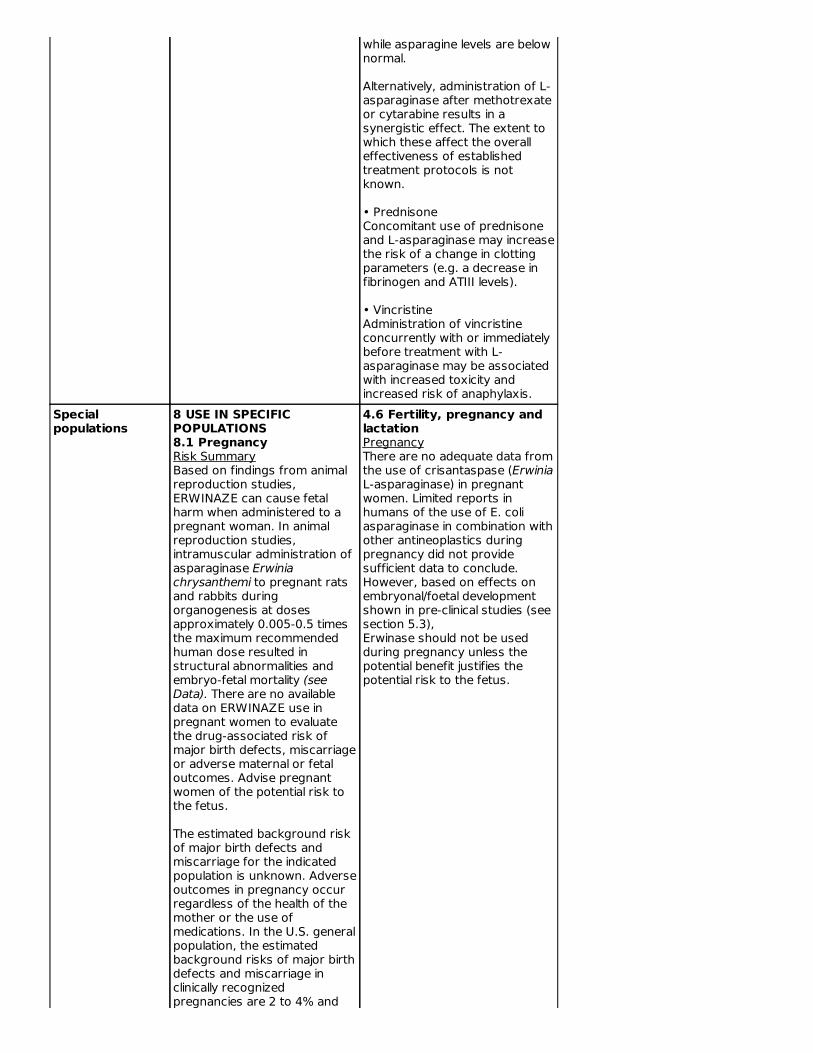
Of the thirty patients enrolled,24 were evaluable for the mainoutcome measure based on thepharmacokinetic samples inCourse 1. The median age was7 years (1-17 years), 63% weremale, 27% were Hispanic orLatino, 83% were White, 3%were Black/African American,7% were Asian, and 7% wereother (American Indian, AlaskaNative, or Indian).
In Study 2, serum asparaginaseactivity of asparaginase Erwiniachrysanthemi was determinedin 24 evaluable patients (aged ≥1 year to ≤17 years) followingintravenous administration ofERWINAZE 25,000International Units/m . Fiveminutes after the 60-minuteinfusion in Course 1, the meanasparaginase activity level was12.65 ± 3.16 InternationalUnit/mL post-dose 1 and 12.11± 3.11 International Unit/mLpost dose 4. The main studyobjective was met with anasparaginase activity level of ≥0.1 International Units/mL 48hours after the fifth doseobserved in 83% of patients.The 72-hour post dose 6asparaginase activity level of ≥0.1 International Unit/mL wasthe secondary endpoint, with43% of patients achieving thisendpoint. Results are presentedin Table 3 [see ClinicalPharmacology (12.3)].
Supply, storageand handling
16 HOWSUPPLIED/STORAGE ANDHANDLINGERWINAZE is a sterile, whitelyophilized powder supplied in aclear 3 mL glass vial. Eachcarton of ERWINAZE (NDC57902-249-05) contains 5 vials.Each single vial (NDC 57902-249-01) contains 10,000International Unitsasparaginase Erwiniachrysanthemi.
Store unused or unopened vialsand cartons at 36°F to 46°F(2°C to 8°C). Protect from light.Do not use ERWINAZE afterthe expiration date on the vial.
6.5 Nature and contentsof containerType 1 clear neutral glass vials of3 ml nominal capacity, closedwith 13 mm halobutyl freeze-drying stoppers and aluminiumoverseals, containing a whitelyophilised solid.Pack size: 5 vials.
6.4 Special precautionsfor storageStore in a refrigerator (+2°C to+8°C).For storage conditions of thereconstituted medicinal product,see section 6.3.
17 PATIENT COUNSELINGINFORMATIONHypersensitivity
There is no correspondingsection for Erwinase SmPC
2

Inform patients of the risk ofallergic reactions, includinganaphylaxis. Instruct patientson the symptoms of allergicreactions and to seek medicaladvice immediately if theyexperience such symptoms[see Warnings and Precautions(5.1)].
PancreatitisInstruct patients on the risk ofpancreatitis and to seek medicaladvice immediately if theyexperience abdominal pain [seeWarnings and Precautions(5.2)].
Glucose IntoleranceInstruct patients on the risk ofhyperglycemia and glucoseintolerance. Advise patients toseek medical advice if theyexperience excessive thirst orany increase in the volume orfrequency of urination [seeWarnings and Precautions(5.3)].
ThrombosisInstruct patients on the risk ofthrombosis and hemorrhageand to seek medical adviceimmediately if they experienceheadache, arm or leg swelling,shortness of breath, and chestpain [see Warnings andPrecautions (5.4)].
Pregnancy and LactationAdvise female patients ofreproductive potential to useeffective contraceptivemethods while receivingERWINAZE and for at least 3months after the last dose.Advise patients to notify theirhealthcare provider immediatelyin the event of a pregnancy orif pregnancy is suspectedduring ERWINAZE treatment[see Use in Specific Populations(8.3)]. Advise lactating womennot to breastfeed duringtreatment with ERWINAZE andfor at least 3 months after thelast dose [see Use in SpecificPopulations (8.2)].
Companyinformation
Manufactured by:Jazz Pharmaceuticals, Inc.3170 Porter Drive, Palo Alto, CA94304U.S. License No. 1901
Erwinaze is a registeredtrademark of Porton BiopharmaLimited used under license byJazz Pharmaceuticals.
7. MARKETINGAUTHORISATION HOLDERPorton Biopharma Limited ManorFarm RoadPorton Down, Salisbury, SP4 0JGUnited Kingdom
8. MARKETINGAUTHORISATION NUMBER(S)PL 44403/0002
®

PRINCIPAL DISPLAY PANEL5 Vials NDC 57902-249-05asparaginase Erwiniachrysanthemi Erwinaze®
For injection, Intramuscularor Intravenous Use10,000 International Unitsper Vial
Rx Only Single Dose Vial.Discard unused portion.
9. DATE OF FIRSTAUTHORISATION/RENEWALOF THE AUTHORISATIONFirst authorisation: 19 July 1985Latest renewal: 25 May 2006
10. DATE OF REVISION OFTHE TEXT06/2020
Erwinase U.K. Package Leaflet, Information for the PatientPackage leaflet: Information for the patient Erwinase10,000 IU, Powder for solution for injection/infusion Crisantaspase (L-asparaginase fromErwinia chrysanthemi)Read all of this leaflet carefully before you start receiving this medicinebecause it contains important information for you.
---
What is in this leaflet1. What Erwinase is and what it is used for2. What you need to know before you are given Erwinase.3. How Erwinase is given4. Possible side effects5. How to store Erwinase6. Contents of pack and other information
1. What Erwinase is and what it is used forHow does Erwinase workErwinase is an anti-blood-cell-cancer treatment from the pharmacotherapeutic group:Antineoplastic and immunomodulating agents. It works by lowering the levels ofasparagine in your body, a substance the cancer cells need to survive.What this medicine is used forErwinase is used for the treatment of a cancer of the white blood cells called AcuteLymphoblastic Leukaemia, in patients aged 4 months and above, who have developedallergic reactions to E.coli derived asparaginase.Erwinase may be used alone or with other treatments.2. What you need to know before you are given ErwinaseYou should not be given Erwinase if:■ you have previously had a severe allergic reaction to the active substance(Crisantapase- L- asparaginase from Erwinia chrysanthemi) or are allergic to any of theother ingredients of this medicine (see section 6).■ You have, or have previously, had serious problems with your pancreas (severepancreatitis) from using a medicine containing L-asparaginase■ You have serious problems with your pancreas (severe pancreatitis)Warnings and precautionsTalk to your doctor or pharmacist or nurse before taking Erwinase.The following complications may arise during treatment with Erwinase:
Serious life threatening allergic reactions. The hospital will have the necessaryprecautions in place to deal with such situations.Inflammation of the pancreas. If you experience abdominal pain this may be a sign ofpancreatitis and should be reported to your doctor immediately. Fatal outcomesassociated with pancreatitis have occurred.Increases in your blood sugar levels (Hyperglycemia). This can be controlled by
Keep this leaflet. You may need to read it again.If you have any further questions, ask your doctor or your pharmacist.If you get any side effects, talk to your doctor or pharmacist or nurse. Thisincludes any possible side effects not listed in this leaflet. See section 4.

receiving insulin sometimes even to fatal amounts (Hyperglycemia). This can becontrolled by receiving insulin.Bleeding and blood clot disorders. During treatment your body’s ability to preventexcessive bleeding may be affected. In the case you experience any significantbleeding your treatment will be stopped. Your doctor will determine if, and when,treatment can be restarted.Liver dysfunctions can be caused or worsened. Discontinuation of Erwinase will beconsidered in the event of a severe reaction. Treatment can be restarted under closemonitoring, but only once at least near complete recovery is achieved.Neurological disorders have been reported with fatal outcomes. Posterior reversibleencephalopathy syndrome (characterised by headache, confusion, seizures andvisual loss) may require blood- pressure lowering medicines and in case of seizure,anti-epileptic treatment.Kidney impairment due to high levels of a substance called uric acid in your bloodfrom the chemotherapy.Reduced immune system that may increase your chances of an infection.
Monitoring during treatment with ErwinaseYou will be monitored closely during and after treatment with Erwinase for:
Allergic reactionsPancreas, kidney and liver functionsNormal blood content
For traceability purposes your health care professional will record the product name andbatch number for each dose of Erwinase you receive.Other medicines and ErwinaseTell your doctor or your pharmacist if you are taking or have recently taken any othermedicines, including medicines obtained without a prescription, particularly any of thefollowing:
Types of medicines used to treat cancer called ‘methotrexate’ or ‘cytarabine’ as theycan affect the way Erwinase works.Prednisone which is used in cancer treatment may increase the risk of a change inclotting.Vincristine which is used in cancer treatment, this can increase the toxic effects ofboth medicinal products and increase the risk of anaphylaxis.Oral contraceptives.
Your doctor or your nurse will not mix Erwinase with other medicines in the sameinfusion.However you will probably be given other medicines before, during or after Erwinasetreatment as part of your course of therapy.PregnancyIf you are pregnant, think you may be pregnant, or are planning to have a baby, askyour doctor or pharmacist for advice before taking this medicine.BreastfeedingYou must not breast-feed your baby during your treatment with Erwinase, there may bea risk to the feeding child.Fertility & Family planningPotential for a decrease in male fertility cannot be out ruled.When appropriate both men and women should use necessary contraceptive measuresbefore, and for at least three months after treatment with Erwinase. Women should usea form of contraception other than oral contraceptives.Driving and using machinesErwinase can cause dizziness and drowsiness. This can affect your coordination andtherefore your ability to drive and operate machinery.Erwinase contains sodium and glucoseErwinase contains the following ingredients:■ sodium (less than 23 mg per dose). You can consider this medicine as essentiallysodium free if you are on a salt-free or low-salt diet.■ glucose. If you are diabetic, please note that each bottle of Erwinase contains 5 mg

glucose.3. How Erwinase is givenDosageErwinase will only be given to you by health care professionals who are experienced ingiving chemotherapy.Your doctor will decide what dose to administer, how often you will be given Erwinaseand for how long. It varies according to your body weight, your specific condition beingtreated, and your response to therapy.Method of administrationErwinase can be given to you in one of the following ways:a) Into a vein (intravenous use). This may be given over 1 to 2 hours.b) Into a muscle (intramuscular use).If you are given more Erwinase than you shouldIf you are concerned that you have been given too much Erwinase, contact your doctoror another healthcare professional immediately.If you think you have missed a dose of ErwinaseIf you are concerned that you have missed a dose, contact your doctor or anotherhealthcare professional immediately.If you have any further questions on this product, ask your doctor, pharmacist ornurse.4. Possible side effectsLike all medicines, Erwinase can cause side effects, although not everybody gets them.Erwinase will be given under strict medical supervision and your doctor may give youother medicines to treat these side effects. Most of the side effects will stop once youstop taking Erwinase.Serious side effectsTell your doctor immediately if you experience:
Severe allergic reactions including blue discolouration of the lips and extremities(possible symptoms of hypoxia), swelling of the face and/or, shortness of breath,increased heart rate; wheezing, difficulty swallowing, hay fever like symptoms, rash,chills, flushing, high or low blood pressure, vomitingRedness, pain, swelling, bruising, or hardening of the skin at the site of the injectionDamage to the Central Nervous System symptoms may include coma,encephalopathy, hallucinations, muscle weakness, confusion, dizziness, drowsiness,agitation, difficulty speakingArm, leg or calf pain with or without swelling (symptoms of blood clots in the arm orleg), abdominal pain (symptoms of a blood clot in the area of the stomach, intestines,and kidneys) chest pain spreading to the arms, neck, jaw, back or stomach, feelingsweaty and breathless (which may be symptoms of a heart attack/myocardialinfarction)Pain near your stomach or in your back (this may be inflammation of your pancreas)High blood sugar levels (hyperglycemia)Increased frequency of bleeding events including bruising even if you have not beeninjuredChanges in liver functions (identified by laboratory testing)
Other side effectsTalk to your doctor if you get any of the following:Very common side effects (may affect more than 1 in 10 people):
-
-
-
--
Infections, including blood infections caused by bacteria (sepsis). This may be dueto low levels of white cells in your blood. You may experience fever, a rapid heartrate, confusion or a rash.Decreases in normal blood content. Some of which may be due to reduced bonemarrow activity.Increase in blood fats, bilirubin, creatinine, urea levels and certain liver enzymes-your doctor will monitor these.Weight lossGeneralised pain/Muscle pains

-
Common (may affect up to 1 in 10 people) side effects include:
------
Uncommon (may affect up to 1 in 100 people) side effects include:
-----
Rare (may affect up to 1 in 1,000 people) side effects include:
-
Not known (frequency cannot be estimated from the available data)
-----
Additional side effects in children and adolescentsLiver, pancreas and blood clotting side effects may be higher in adults compared tochildren.Reporting of side effectsIf you get any side effects, talk to your doctor or,pharmacist. This includes any possibleside effects not listed in this leaflet. You can also report side effects directly via MHRAYellow Card in Google Play or Apple App Store.By reporting side effects you can help provide more information on the safety of thismedicine.5. How to store ErwinaseKeep this medicine out of the sight and reach of children.Erwinase will not be used after the expiry date printed on the label after “EXP”. Theexpiry date refers to the last day of the month.The unopened Erwinase vials will be stored in a refrigerator (between +2°C to +8°C) bythe hospital.After reconstitution, the product should be used within 15 minutes. If the delay is morethan 15 minutes, the solution should be withdrawn into a glass or polypropylene syringeand used within 8 hours. The reconstituted product should be stored below 25°C.6. Contents of the pack and other informationWhat Erwinase containsThe active substance is crisantaspase (L-asparaginase from Erwinia chrysanthemi). Eachvial contains 10,000 International units of cristanaspase (L-asparaginase from Erwiniachrysanthemi).The other excipients are sodium chloride (See section 2) and glucose monohydrate (Seesection 2).What Erwinase looks like and contents of the packErwinase is provided as a powder for solution for injection/infusionIt comes as a white lyophilized powder in a clear glass bottle with a rubber stopper andan aluminium seal. Each pack contains 5 glass bottles of powder.Marketing Authorisation Holder and Manufacturer
Nausea
Difficulty breathing or stopping breathingMucositis (inflammation of the digestive tract)DiarrhoeaAbdominal pain/discomforttiredness or headacheHigh temperature
life threatening complications of uncontrolled diabetesHigh blood levels of ammoniaFits (convulsions)Build up of fats in the liverKidney dysfunction
Posterior reversible encephalopathy syndrome (a condition characterised byheadache, confusion, seizures and visual loss).
Inflammation of the salivary gland at the back of the throatLiver failure, increased mass of liver, jaundiceDecreased albumin levels in the blood causing water retentionBlistering and peeling of the skin (Toxic epidermal necrolysis)Joint pain

Porton Biopharma Limited, Manor Farm Road,Porton Down, Salisbury, SP4 0JG United KingdomThis leaflet was last revised in June 2020Erwinase is a registered trademark of Porton Biopharma Limited.
PRINCIPAL DISPLAY PANELErwinase Carton
Erwinase Vial
ERWINASE asparaginase injection, powder, lyophilized, for solution
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:81561-413
Route of Administration INTRAMUSCULAR, INTRAVENOUS
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
ASPARAGINASE ERWINIA CHRYSANTHEMI (UNII: D733ET3F9O)(ASPARAGINASE - UNII:G4FQ3CKY5R)
ASPARAGINASE ERWINIACHRYSANTHEMI
10000 [iU] in 1 mL
Inactive IngredientsIngredient Name Strength
DEXTROSE MONOHYDRATE (UNII: LX22YL083G) 5 mg in 1 mLSODIUM CHLORIDE (UNII: 451W47IQ8X) 0.5 mg in 1 mL
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date

Porton Biopharma Limited
1 NDC:81561-413-05 5 in 1 CARTON 06/01/2021
1 NDC:81561-413-01
1 mL in 1 VIAL, GLASS; Type 0: Not a CombinationProduct
Marketing InformationMarketing Category Application Number or
Monograph CitationMarketing Start
DateMarketing End
DateUnapproved drug for use in drugshortage 06/01/2021
Labeler - Porton Biopharma Limited (220514820)
EstablishmentName Address ID/FEI Business Operations
Porton Biopharma Limited 220514820 manufacture(81561-413)
Revised: 6/2021








![Original Article - Endourology/Urolithiasis · follow-up of urolithiasis [1]. Prior to the use of computed tomography (CT), intravenous urography (IVU) was the Radiation dosing in](https://static.fdocuments.net/doc/165x107/5c8ae9ae09d3f232478d1cdb/original-article-endourologyurolithiasis-follow-up-of-urolithiasis-1-prior.jpg)









