Are Communication Deviance and Expressed Emotion Related to
11
Are Communication Deviance and Expressed Emotion Related to Family History of Psychiatric Disorders in Schizophrenia? by Kenneth L. Subotnik, Michael J. Qoldstein, Keith H. Nuechterlein, Stephanie M. Woo, and Jim Mint? Abstract Studies have reported that certain measures of intrafa- milial transactions are associated with an increased risk both for the initial onset of schizophrenia and for its recurrence following the initial episode of disorder. Two of the most studied of these are communication deviance (CD), a measure of subclinical thought disor- der expressed in speech, and expressed emotion (EE), defined as notable attitudes of criticism and/or emo- tional overinvolvement manifested in a semistructured interview. A previous study (Goldstein et al. 1992) examined whether these two measures were associated with the presence of a diagnosable psychiatric disorder in the biological parents of recent-onset schizophrenia patients. In general, they were not. The present study went one step further. It examined whether these same measures were correlated with family history of schiz- ophrenia or affective disorder in the biological parents and siblings of these same parents. High EE was not associated with a greater family history of schizophre- nia spectrum disorders among the parent's parents and siblings but was unexpectedly found to be inversely associated with familial affective disorders. In contrast, CD was associated with a family history of schizophrenia spectrum disorders among the parent's parents and siblings. The findings are consistent with the possibility that CD may be an indicator of a genetic vulnerability factor for schizophrenia. Keywords: Schizophrenia, thought disorder, fam- ily study, communication deviance, expressed emotion, vulnerability indicator, family environment. Schizophrenia Bulletin, 28(4):719-729, 2002. Certain measures of intrafamilial transactions have been consistently associated with an increased risk for recur- rence of schizophrenic psychosis following the initial episode of the disorder (see Goldstein 1987, and Hooley and Hiller 2001, for reviews of these findings). Two attri- butes that have been studied extensively are (1) the clarity of communication between parents and their offspring and (2) affective attitudes and behaviors expressed toward another family member, usually one who has manifested some signs of a psychiatric disorder. The work of Wynne and Singer provides the best operational criteria for dis- turbed communicational processes, which they termed communication deviance (CD; Wynne and Singer 1963a, 1963£; Wynne et al. 1977). Note that the CD measure identifies not psychiatric deviance but specific aspects of communication style. The most heavily researched con- struct related to affective attitude is expressed emotion (EE; Brown et al. 1972), defined as notable attitudes of criticism and/or emotional overinvolvement manifested in a semistructured interview, the Camberwell Family Inter- view (CFI; Brown and Rutter 1966). A major assumption underlying this line of research, particularly in the case of biological parents of young adult schizophrenia patients, has been that these measures reflect ongoing family transactions that are stressors for persons who are in regular contact with high-CD or high- EE relatives (Nuechterlein et al. 1989; Miklowitz and Stackman 1992; Hooley and Gotlib 2000). There are other possible explanations of their apparent clinical signifi- cance. For example, these attributes may represent indirect assessments of a major psychiatric disorder in the parent. That question has been studied. The results have been largely, although not entirely, negative. A previous report (Goldstein et al. 1992) on a sample of 56 parents of 41 recent-onset schizophrenia patients found that high CD in relatives was not related to the presence of either a past or a present psychiatric disorder. Negative findings were also obtained for the CFI-EE assessment. The Five-Minute Speech Sample Method (FMSS-EE; Magafia et al. 1986) did suggest that relatives with a lifetime diagnosis of a severe psychiatric disorder were more likely to have high FMSS-EE, and that tendency was even stronger using a composite index based on both the CFI- and FMSS-EE measures, which were separated by a 4- to 5-week period. Send reprint requests to Dr. K. L. Subotnik, Department of Psychiatry and Biobehavioral Sciences, University of California, Los Angeles, 300 UCLA Medical Plaza, Room 2240, Los Angeles, CA 90095-6968; e- mail: [email protected]. 719 Downloaded from https://academic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 December 2021
Transcript of Are Communication Deviance and Expressed Emotion Related to
Are Communication Deviance and ExpressedEmotion Related to Family History of
Psychiatric Disorders in Schizophrenia?
by Kenneth L. Subotnik, Michael J. Qoldstein, Keith H. Nuechterlein,Stephanie M. Woo, and Jim Mint?
Abstract
Studies have reported that certain measures of intrafa-milial transactions are associated with an increasedrisk both for the initial onset of schizophrenia and forits recurrence following the initial episode of disorder.Two of the most studied of these are communicationdeviance (CD), a measure of subclinical thought disor-der expressed in speech, and expressed emotion (EE),defined as notable attitudes of criticism and/or emo-tional overinvolvement manifested in a semistructuredinterview. A previous study (Goldstein et al. 1992)examined whether these two measures were associatedwith the presence of a diagnosable psychiatric disorderin the biological parents of recent-onset schizophreniapatients. In general, they were not. The present studywent one step further. It examined whether these samemeasures were correlated with family history of schiz-ophrenia or affective disorder in the biological parentsand siblings of these same parents. High EE was notassociated with a greater family history of schizophre-nia spectrum disorders among the parent's parentsand siblings but was unexpectedly found to beinversely associated with familial affective disorders.In contrast, CD was associated with a family history ofschizophrenia spectrum disorders among the parent'sparents and siblings. The findings are consistent withthe possibility that CD may be an indicator of agenetic vulnerability factor for schizophrenia.
Keywords: Schizophrenia, thought disorder, fam-ily study, communication deviance, expressed emotion,vulnerability indicator, family environment.
Schizophrenia Bulletin, 28(4):719-729, 2002.
Certain measures of intrafamilial transactions have beenconsistently associated with an increased risk for recur-rence of schizophrenic psychosis following the initialepisode of the disorder (see Goldstein 1987, and Hooleyand Hiller 2001, for reviews of these findings). Two attri-butes that have been studied extensively are (1) the clarityof communication between parents and their offspring and
(2) affective attitudes and behaviors expressed towardanother family member, usually one who has manifestedsome signs of a psychiatric disorder. The work of Wynneand Singer provides the best operational criteria for dis-turbed communicational processes, which they termedcommunication deviance (CD; Wynne and Singer 1963a,1963£; Wynne et al. 1977). Note that the CD measureidentifies not psychiatric deviance but specific aspects ofcommunication style. The most heavily researched con-struct related to affective attitude is expressed emotion(EE; Brown et al. 1972), defined as notable attitudes ofcriticism and/or emotional overinvolvement manifested ina semistructured interview, the Camberwell Family Inter-view (CFI; Brown and Rutter 1966).
A major assumption underlying this line of research,particularly in the case of biological parents of youngadult schizophrenia patients, has been that these measuresreflect ongoing family transactions that are stressors forpersons who are in regular contact with high-CD or high-EE relatives (Nuechterlein et al. 1989; Miklowitz andStackman 1992; Hooley and Gotlib 2000). There are otherpossible explanations of their apparent clinical signifi-cance. For example, these attributes may represent indirectassessments of a major psychiatric disorder in the parent.That question has been studied. The results have beenlargely, although not entirely, negative. A previous report(Goldstein et al. 1992) on a sample of 56 parents of 41recent-onset schizophrenia patients found that high CD inrelatives was not related to the presence of either a past ora present psychiatric disorder. Negative findings were alsoobtained for the CFI-EE assessment. The Five-MinuteSpeech Sample Method (FMSS-EE; Magafia et al. 1986)did suggest that relatives with a lifetime diagnosis of asevere psychiatric disorder were more likely to have highFMSS-EE, and that tendency was even stronger using acomposite index based on both the CFI- and FMSS-EEmeasures, which were separated by a 4- to 5-week period.
Send reprint requests to Dr. K. L. Subotnik, Department of Psychiatryand Biobehavioral Sciences, University of California, Los Angeles, 300UCLA Medical Plaza, Room 2240, Los Angeles, CA 90095-6968; e-mail: [email protected].
719
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Schizophrenia Bulletin, Vol. 28, No. 4, 2002 K.L. Subotnik et al.
The present study took this line of research one stepfurther to consider whether our previous findings weregenerally negative because, by virtue of their parenthoodstatus, these relatives would be unlikely to have a severepsychiatric disorder such as schizophrenia (Gottesman1991). Therefore, we decided to examine the question ofwhether CD and even EE tap a predisposition to a psychi-atric disorder that is not clinically expressed. If these mea-sures were found to be related to a family history of aschizophrenia-related disorder among the subject's parentsand siblings, this would be consistent with a familiallytransmitted predispositional factor for schizophrenia,which other evidence suggests is primarily genetic in ori-gin (Kendler 2000). Some evidence supportive of this viewhas recently been presented by Docherty et al. (19996) foranother index of communication disturbance. Therefore,we examined whether high levels of EE or CD wererelated to a family history of schizophrenia spectrum dis-orders in the parents and siblings of the biological parentsof individuals with schizophrenia. A contrast measure of afamily history of affective disorder was also examined inrelation to EE and CD.
Methods
Subjects. The current study involved linkage of datafrom three separate protocols, each of which contributeddata in some form to the current analyses. These protocolsinvolved separate informed consent procedures, differentresearch measures, and different inclusion criteria.
Contributing Project 1: Developmental Processesin Schizophrenic Disorders (principal investigator[PI]: K.H.N.). The main protocol was the first one withinthe Developmental Processes in Schizophrenic Disordersproject, a longitudinal prospective study of the earlycourse of schizophrenia in young adult patients(Nuechterlein et al. 1992). This project followed 104patients with a recent onset of schizophrenia. As part ofthe initial protocol, Developmental Processes in Outcome,significant others with whom the patients had at leastweekly contact were asked to participate in a researchinterview, the CFI (Vaughn and Leff 1976), to assess EE(CFI-EE). At least one biological parent in 67 families, fora total of 105 parent-subjects, participated.
Because the biological parents of the patients, not thepatients themselves, were the subjects in the present study,the patient sample will be described only briefly here. Acomplete description of the selection criteria for thepatient sample can be found in Nuechterlein et al. (1992).All patients were required to have a diagnosis of schizo-phrenia or schizoaffective disorder, mainly schizophrenic,by Research Diagnostic Criteria (RDC; Spitzer et al.
1978), with the patient's first psychotic episode occurringless than 2 years prior to project contact. An active psy-chotic period of at least 2 weeks was required. Thepatients were screened and selected from consecutiveadmissions to four local public psychiatric hospitals andreferrals to the University of California, Los Angeles(UCLA) Adult Psychiatry outpatient department. Familyhistory of psychiatric illness was not considered in patientselection. Patients with current significant and habitualdrug and alcohol abuse, or with a history of abuse thatmade the diagnosis of schizophrenia ambiguous, wereexcluded. At the time of entry into the study, the mean ageof the 67 patients was 23.2 years (standard deviation [SD]= 4.6, range 18 to 44 years); the mean years of school was12.5 (SD = 1.8, range 8 to 16 years); and 57 patients (85%)were male, 10 were female. Sixty patients were non-His-panic Caucasian, 3 were Hispanic, 1 was Asian, and 3were of mixed racial background.
Contributing Project 2: Coping Behavior inSchizophrenia (UCLA Family Project; PI: M.J.G.).Approximately 4 to 5 weeks after the patients began out-patient treatment as part of Project 1, the parents wereasked to participate in a second, separate protocol toassess family attitudes and interactions. A total of 94 bio-logical parents participated in Project 2. A measure ofsubclinical thought disorder (i.e., CD) administered at theUCLA Family Project was used for this report.
Contributing Project 3: The UCLA Family Study(PI: K.H.N.). The third protocol was a family study ofpsychiatric disorders and neurocognitive vulnerability fac-tors. At least 1 biological family member from 79 of the104 families of the Developmental Processes in Outcomepatients participated. Of the 158 biological parents ofpatients in these 79 families, 111 were interviewed in per-son. Of those parents not directly interviewed (n - Al), 25(10 mothers and 15 fathers) were deceased, 7 (2 mothersand 5 fathers) lived far from Los Angeles and were notavailable to be interviewed, 5 (fathers) could not belocated, and 10 (3 mothers and 7 fathers) declined to beinterviewed. Thus, of the 121 living parents who werelocated, lived locally, and were contacted by the researchteam, 92 percent were directly interviewed.
Demographics of parents. Ninety-eight parent-sub-jects (60 mothers and 38 fathers) participated in bothProject 1 and Project 3. These parent-subjects were anaverage of 55 years old at the time of the Family Studyassessment (SD = 7.5). They had a mean of 13.9 years ofeducation (SD = 2.8) and a mean socioeconomic status of2.9 (SD = 1.2) (Hollingshead 1957). Eighty-six parent-subjects were Caucasian, 6 were Hispanic, 2 were African-American, 2 were Asian, and 2 were of mixed racial back-ground. Somewhat fewer (89) parent-subjects participatedin both Project 2 and Project 3. These 89 subjects were
720
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Communication Deviance and Expressed Emotion Schizophrenia Bulletin, Vol. 28, No. 4, 2002
demographically similar to the 98 participants in bothProject 1 and Project 3. The 98 parent-subjects in the cur-rent report include the 56 originally described in the priorreport of the relationship of CD and EE to the personalpsychiatric history of the parents (Goldstein et al. 1992).
ProceduresProcedures from Project 1. As described above, the CFI(Vaughn and Leff 1976) was administered to parent-sub-jects to assess EE as part of the Developmental Processesstudy. The CFI was administered within a month of thepatient's index hospital admission or soon thereafter.
Procedures from Project 2. After discharge from thehospital, the patients and the adult relatives with whomthey had at least weekly contact were informed of the sep-arate study, Coping Behavior in Schizophrenia, in whichother family assessment data were collected. If theyagreed to participate, which required a separate informedconsent process and form, they were scheduled for a ses-sion approximately 4 to 5 weeks after the patient was dis-charged. A seven-card version of the ThematicApperception Test (TAT) was individually administered toeach subject to assess CD. The instructions requested thatthe subject make up a story for each card covering whatled up to the scene portrayed in the picture, what wasoccurring in the picture, how the characters were thinkingor feeling, and how the story might end. The subjects' sto-ries were audiotaped, converted to transcripts, and scoredaccording to a 27-category system based on the originalWynne-Singer system for operationalizing the constructof CD as modified by Jones (1977) for the TAT. The TAT-CD system results in a mean z score representing the 27categories weighted by their frequency relative to thelength of the total speech record, and expressed in SDunits based on previously collected normative data. Inaddition, six factor scores are available from these databased on the original work of Jones (1977); these scoresdefine specific clusters of the ways that CD can be mani-fested in the respondents' stories. The interrater reliability(intraclass correlation) for the mean z score was 0.99 (p <0.0001). The average intraclass correlation for the six fac-tors was 0.90 (range 0.82 to 0.98, p < 0.001 for each;Miklowitz et al. 1986, 1991). All coders of CFI-EE andTAT-CD were blind to the diagnostic data that were col-lected subsequently from the parents of the schizophreniapatients. Also, separate teams of raters made the CFI andTAT-CD ratings, and each team operated without theknowledge of the other's data.
Procedures from Project 3. Because the UCLA FamilyStudy was separate from the Developmental Processes
study, it involved only a subgroup of parents who chose toparticipate (a separate informed consent process and formwere completed). The staff who collected these diagnosticdata had no overlap with those who collected the EE andCD data.
The first part of the Family Study involved face-to-face diagnostic interviews with the parent. Clinical psychi-atric syndromes were assessed with the Diagnostic Inter-view Schedule (DIS; Robins et al. 1981), withsupplemental questions regarding psychotic symptomsselected from the Present State Exam (PSE; Wing et al.1974); the supplemental questions were asked if there wasevidence of the symptoms. The presence of any of fiveselected personality disorders (schizotypal, paranoid,schizoid, avoidant, and borderline) was assessed using theStructured Clinical Interview for DSM-HI-R (SCID-II;Spitzer et al. 1987). Extensive followup questions wereasked if indicated by the subject's response to the initialprobe question for any individual criterion.
Following this interview concerning personal historyof psychiatric disorders, each parent then participated in afamily history interview that covered psychiatric disordersin the first and second degree relatives, plus the cousins, ofthe schizophrenia patient. All family history diagnoseswere based on symptoms reported by the interviewee anddid not rely on the interviewee's memory of what diag-noses had been given to the family members. This historywas collected using the Relative Psychiatric History for-mat developed by Gershon (1985). Diagnosis for the non-interviewed second and third degree relatives was madeusing the Family History Research Diagnostic Criteria(Andreasen et al. 1977). Personality disorder symptomswere assessed with the SCID-II, which we adapted for afamily history interview format as follows. Initial screen-ing questions were used to assess for the presence of per-sonality disorder symptoms in the subject's first and sec-ond degree relatives. If there was evidence of personalitypathology relevant to one or more of the five personalitydisorders examined here, the SCID-II questions for thesedisorders were asked in the third person. StandardDSM-III-R (American Psychiatric Association 1987) cri-teria were used to rate personality disorder diagnoses.When family history information on these relatives wasalso available from the subject's spouse, a consensus diag-nosis was made from these sources.
The Family Study interviewers had clinical training inpsychiatric diagnosis and had substantial experience con-ducting structured diagnostic interviews. Training in theuse of the modified DIS/PSE involved didactic instruction,co-rating taped interviews, and live interviews (Fogelsonet al. 1991; Subotnik et al. 1997). David Fogelson, M.D.,trained the staff to administer the SCID-II and family his-tory interview through a three-step procedure involving (1)
721
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Schizophrenia Bulletin, Vol. 28, No. 4, 2002 K.L. Subotnik et al.
having staff rate sample interviews conducted by Dr.Fogelson with feedback from him on their symptom rat-ings and diagnoses; (2) administering practice interviewswith other staff and the trainer; and (3) administering themodified DIS/PSE, SCID-II, and family history interviewto at least five subjects drawn from the adult inpatient ser-vice at the UCLA Neuropsychiatric Hospital and a tempo-rary employment agency. Interviewers were considered tohave completed training when there was at least 90 per-cent agreement between their symptom ratings and the rat-ings of Dr. Fogelson. Ongoing weekly supervision wasprovided to prevent drift in rating standards over time.Reasonable reliability for assessing personality disordersymptom dimensions using the SCID-II was establishedbased on 45 cases (intraclass correlations were 0.82 forborderline, 0.73 for schizotypal, 0.70 for paranoid, 0.60for schizoid, and 0.84 for avoidant; Fogelson et al. 1991).The diagnoses that were generated for schizophrenia,schizophrenia-related psychoses, and schizophrenia spec-trum personality disorders using the family historymethod were previously shown to have excellent speci-ficity and positive predictive value but low sensitivity(Fogelson et al., in press).
Following the collection of family history data, thefamily history of each biological parent of a patient wascharacterized by the presence of schizophrenia spectrumdisorders and affective disorders in the parent-subject'sown parents or siblings. This family history characteriza-tion excludes the offspring of these parent-subjects toavoid confounding the genetic loading of mothers andfathers within the same family. Although having such afamily history of schizophrenia spectrum disorders in sib-lings or parents does not formally represent obligate car-rier status, it might be considered a proxy for such a car-rier status, given that all parent-subjects had at least oneoffspring with schizophrenia. If any parent or sibling of aparent had a diagnosis of RDC schizophrenia, RDCschizoaffective disorder, mainly schizophrenia, orDSM-IJI-R schizotypal or paranoid personality disorder,that parent-subject was classified as meeting this proxycriteria for schizophrenia liability carrier status. This wastrue for 14 (14.3%) of the family histories of the 98 par-ents who participated in both Projects 1 and 3. If any par-ent or sibling of a parent-subject satisfied criteria for RDCschizoaffective disorder, mainly affective, RDC manic dis-order, or RDC major depressive disorder, the parent-sub-ject was classified as having an affective disorder familialliability. This was true for 21 (21.4%) of the family histo-ries of the 98 parents who participated in Projects 1 and 3,with 5 of these 21 parent-subjects also meeting proxy cri-teria for schizophrenia spectrum disorder liability carrierstatus. Sixty-eight parents had none of the above diag-noses in their parents or siblings. Note that those families
may have contained individuals with other psychiatric dis-orders that were not examined in relation to the familyinteraction variables under study.
Data Analyses
The statistical model for the analysis of CD (a continu-ous and unimodally distributed variable) was a generallinear mixed model (SAS PROC MIXED). Family his-tory among the parent-subject's own parents and sib-lings ("positive," "negative") and parent-subject gender(i.e., mother, father) were fixed design effects in a 2 X 2crossed design. Personal lifetime psychiatric history(presence of any psychiatric disorder1) was included as acovariate. Random family and error effects (assumed tobe independent) modeled possible nonindependencewithin families (in fact, within-family correlation wastrivial, accounting for no more than 1% of the variancein any analysis). The presence or absence of any of theassessed personal RDC or DSM-III-R disorders wasentered as a covariate so that variance associated withpersonal psychiatric pathology would be accounted forstatistically. The dichotomous EE variable was analyzedwith the same design, using the Generalized EstimatingEquation (GEE) approach of Liang and Zeger (1986).The GEE analyses specified a logit link function, bino-mial error, and the exchangeable correlation structure (infact, any specification of the correlation structure wouldproduce the same results in this model because there wasonly one covariance to model with a maximum of twomeasures per family). The GEE program reports sepa-rate robust t tests for each of the fixed parameter esti-mates. Significant interactions of family history by par-ent status were followed up with analyses for eachparent separately, using simple contingency tables andchi-square tests of significance. Separate analyses wereconducted for family history (among parents and sib-lings) of schizophrenia spectrum disorders and affectivedisorders.
Results
CFI-EE. CFI-EE data from Project 1 were available for98 of the subjects (60 mothers and 38 fathers) who alsoparticipated in Project 3. Fifty-two participants (53%)
'Twenty-six mothers (43.3%) had one or more of the following life-time personal psychiatric diagnoses: RDC schizophrenia; schizoaffec-tive, manic, or major depressive disorder; DSM-III-R generalized anxi-ety disorder, or DSM-III-R avoidant. paranoid, schizotypal, schizoid, orborderline personality disorder. Similarly, 16 fathers (42.1%) had one ormore of these psychiatric diagnoses.
722
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021
Communication Deviance and Expressed Emotion Schizophrenia Bulletin, Vol. 28, No. 4, 2002
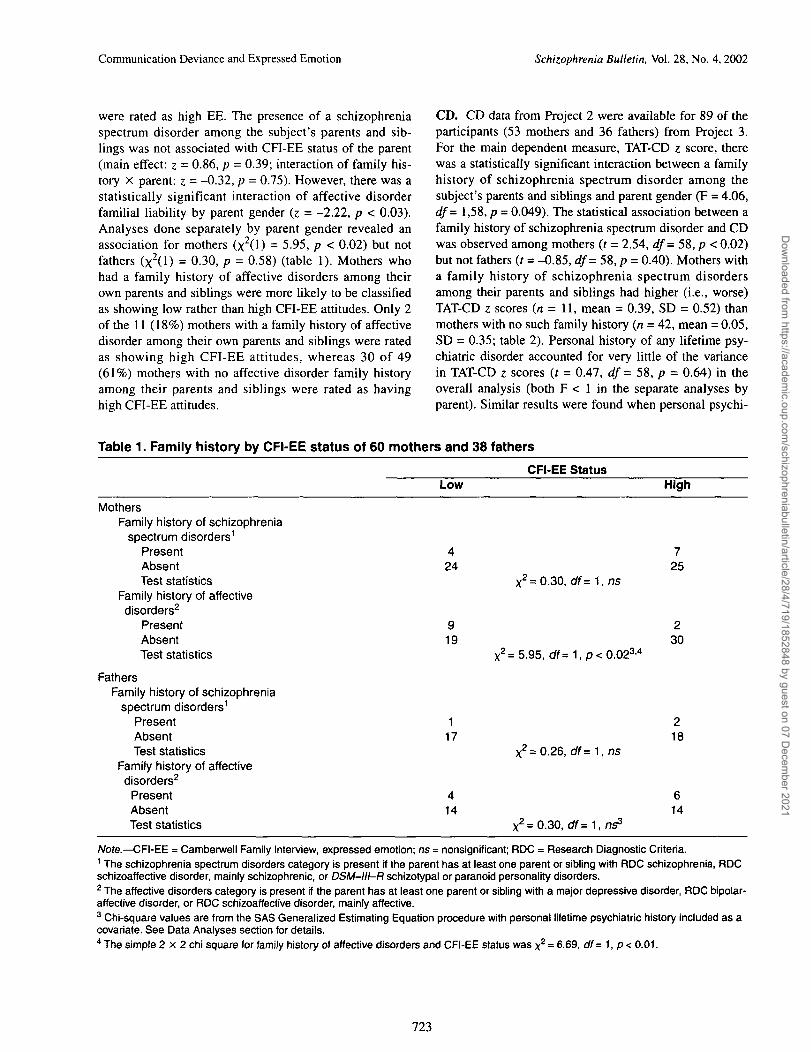
were rated as high EE. The presence of a schizophreniaspectrum disorder among the subject's parents and sib-lings was not associated with CFI-EE status of the parent(main effect: z = 0.86, p = 0.39; interaction of family his-tory X parent: z = -0.32, p = 0.75). However, there was astatistically significant interaction of affective disorderfamilial liability by parent gender (z = -2.22, p < 0.03).Analyses done separately by parent gender revealed anassociation for mothers (x2(l) = 5.95, p < 0.02) but notfathers (x2(l) = 0.30, p = 0.58) (table 1). Mothers whohad a family history of affective disorders among theirown parents and siblings were more likely to be classifiedas showing low rather than high CFI-EE attitudes. Only 2of the 11 (18%) mothers with a family history of affectivedisorder among their own parents and siblings were ratedas showing high CFI-EE attitudes, whereas 30 of 49(61%) mothers with no affective disorder family historyamong their parents and siblings were rated as havinghigh CFI-EE attitudes.
CD. CD data from Project 2 were available for 89 of theparticipants (53 mothers and 36 fathers) from Project 3.For the main dependent measure, TAT-CD z score, therewas a statistically significant interaction between a familyhistory of schizophrenia spectrum disorder among thesubject's parents and siblings and parent gender (F = 4.06,df = 1,58, p = 0.049). The statistical association between afamily history of schizophrenia spectrum disorder and CDwas observed among mothers (r = 2.54, df= 58, p < 0.02)but not fathers (f = -0.85, df= 58, p = 0.40). Mothers witha family history of schizophrenia spectrum disordersamong their parents and siblings had higher (i.e., worse)TAT-CD z scores (n = 11, mean = 0.39, SD = 0.52) thanmothers with no such family history {n = 42, mean = 0.05,SD = 0.35; table 2). Personal history of any lifetime psy-chiatric disorder accounted for very little of the variancein TAT-CD z scores (t = 0.47, df = 58, p = 0.64) in theoverall analysis (both F < 1 in the separate analyses byparent). Similar results were found when personal psychi-
Table 1. Family history by CFI-EE status of 60 mothers and 38 fathers
CFI-EE StatusLow High
MothersFamily history of schizophrenia
spectrum disorders1
PresentAbsentTest statistics
Family history of affectivedisorders2
PresentAbsentTest statistics
FathersFamily history of schizophrenia
spectrum disorders1
PresentAbsentTest statistics
Family history of affectivedisorders2
PresentAbsentTest statistics
424
919
X2=0.30, df=-\,ns
X2=5.95, df=1,p<0.023'4
117
414
X 2 =0.26 , df=1, ns
X 2= 0.30, df =1,
725
230
218
614
Note.—CFI-EE = Camberwell Family Interview, expressed emotion; ns = nonsignificant; RDC = Research Diagnostic Criteria.1 The schizophrenia spectrum disorders category is present if the parent has at least one parent or sibling with RDC schizophrenia, RDCschizoaffective disorder, mainly schizophrenic, or DSM-III-R schizotypal or paranoid personality disorders.2 The affective disorders category is present if the parent has at least one parent or sibling with a major depressive disorder, RDC bipolar-affective disorder, or RDC schizoaffective disorder, mainly affective.3 Chi-square values are from the SAS Generalized Estimating Equation procedure with personal lifetime psychiatric history included as acovariate. See Data Analyses section for details.4 The simple 2 x 2 chi square for family history of affective disorders and CFI-EE status was x2 = 6.69, <#= 1, p < 0.01.
723
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Schizophrenia Bulletin, Vol. 28, No. 4, 2002 K.L. Subotnik et al.
Table 2. Family history of lifetime psychiatric diagnoses byTAT-CD mean z scores for 53 mothers and36 fathers
TAT-CD z(SD)Mothers Fathers
Family history of schizophrenia spectrum disorders1
PresentAbsentTest statistics
Family history of affective disorders3
PresentAbsentTest statistics
0.39(0.52), n= 110.05 (0.35), n = 42
t=2.54, df= 58, p<0.022
0.06(0.62), n= 110.14(0.35), n = 42
f = -0.54, df = 58, ns
0.15(0.44), n = 4-0.03(0.31), n = 32f = 0.85, df= 33, ns
-0.01 (0.35), /?= 100.19(0.45), n = 26f = 1.27, df= 35, ns
Note.—ns = nonsignificant; RDC = Research Diagnostic Criteria; SD = standard deviation; TAT-CD = Thematic Apperception Test, commu-nication deviance.1 The schizophrenia spectrum disorders category is present if the parent has at least one parent or sibling with RDC schizophrenia, RDCschizoaffective disorder, mainly schizophrenic, or DSM-III-R schizotypal or paranoid personality disorders.2 t test values are from the SAS general linear mixed model with personal lifetime psychiatric history as a covariate. See Data Analysessection for details.3 The affective disorders category is present if the parent has at least one parent or sibling with a major depressive disorder, RDC bipolar-affective disorder, or RDC schizoaffective disorder, mainly affective.
atric history was limited to the presence or absence ofschizophrenia spectrum disorders (i.e., RDC schizophre-nia, RDC schizoaffective disorder, mainly schizophrenia,or DSM-III-R schizotypal or paranoid personality disor-der). There were no significant relationships between anyof the six CD factors and family history of schizophreniaspectrum in the subjects' siblings or parents (p values forthe main effect of family history ranged from 0.65 to 0.96,median = 0.86; for the interaction of family history byparent gender from 0.10 to 0.92, median = 0.44). No sig-nificant relationship was found between family history ofaffective disorder among the subjects' parents and siblingsand the subjects' TAT-CD z scores.
Discussion
EE level of parents was not related to the degree of theirfamilial liability to schizophrenia spectrum disorders. Thisis consistent with the general belief that EE does notreflect a subclinical schizophrenia spectrum disorder. Thissuggests that the oft-replicated finding that high-EEparental status predicts higher relapse rates for patientswith schizophrenia cannot be accounted for by anotherknown prognostic variable: a family history of schizophre-nia spectrum disorders.
We found that familial affective disorder (among par-ents and siblings of the parent-subjects) was associatedwith reduced rather than increased likelihood of manifest-ing high-EE attitudes. A direct comparison to a previousliterature is not possible because no prior studies havedirectly examined EE in relationship to family psychiatric
history. A genetic basis for the observed relationship ispossible but cannot be either confirmed or ruled out basedon this family study. An environment explanation of thisrelationship might be that prior exposure to a severelydepressed relative may ameliorate somewhat the tendencyto be critical of one's own psychiatrically ill child and maypromote the development of more tolerant attitudes.
One might wonder why prior exposure to a familymember with an affective disorder, but not prior exposureto a schizophrenia-related disorder, is associated withlower EE attitudes toward an offspring with schizophrenia.Several aspects need consideration. As we have pointedout elsewhere, EE is likely to arise in the difficult contextin which relatives of schizophrenia patients struggle tofind ways of relating to their relative with severe mentaldisorder (Miklowitz et al. 1989; Strachan et al. 1989;Rosenfarb et al. 1995, 2000; Woo et al. 1997). Schizophre-nia-related disorders are more likely than depressive disor-ders to involve a sustained family burden due to specificdisturbed behaviors and social performance deficits, whichhave been found to be associated with high-EE attitudes(Jackson et al. 1990). Thus, sustained exposure to schizo-phrenia may not lead as commonly to development of tol-erant attitudes toward major psychiatric disorders. Previ-ous exposure to a family member who experienced one ormore depressive episodes from which recovery occurredwithout persistent disturbed behaviors and functionalimpairment, on the other hand, may result in more hopefuland tolerant attitudes when an offspring later develops apsychiatric disorder.
The picture for CD looks quite different. The meanacross all 27 CD items (standardized) was positively asso-
724
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Communication Deviance and Expressed Emotion Schizophrenia Bulletin, Vol. 28, No. 4, 2002
ciated with presence of a family history of schizophreniaspectrum disorder in the respondent's parents and siblings,albeit only on the maternal side. Scores on this measurewere not associated with a personal psychiatric diagnosisin these parents. Separate analyses of the six CD factorscores did not point to any specific component of CD, sug-gesting that it was overall CD that was related to maternalfamily history.
This pattern in a family pedigree—the presence ofschizophrenia spectrum disorder in either the parents orsiblings of an individual, notable levels of CD in that indi-vidual, and schizophrenia in the individual's offspring(i.e., the patient)—is genetically interpretable. The parentof the patient in this situation is the probable carrier ofsome psychosis-predisposing gene or genes. CD in suchbiological parents of a schizophrenia patient might serveas a subclinical indicator of a genetic predisposition topsychotic disorder.
The notion that CD may be a subtle manifestation of agenetic vulnerability to schizophrenia would be furthersupported if CD was also related to neurocognitive deficitsin first degree relatives that are putative indicators of vul-nerability factors for schizophrenia (Nuechterlein andDawson 1984; Asarnow et al. 1991; Braff 1993). Wagenerand colleagues found relationships within biological par-ents of schizophrenia patients between CD and perform-ance on the Continuous Performance Test (CPT) and theSpan of Apprehension (SPAN) test (Wagener et al. 1986).We have similarly found that some parental CD factorscores in the current sample are significantly associatedwith those parents' own CPT and SPAN performance(Subotnik et al. 1999). However, a relationship betweenneurocognitive measures and communication disturbancein parents of schizophrenia patients has not consistentlybeen found (Docherty and Gordinier 1999).
We found that the association between parental CDlevels and presence of schizophrenia spectrum disorder inparents and siblings of these parents was significant formothers, but not fathers, of schizophrenia patients. Thisraises the question of gender effects. There is some evi-dence that family morbid risk for schizophrenia may behigher among female than male schizophrenia patients(Goldstein 1995), and DeLisi and Crow (1989) raised thepossibility of a sex-linked transmission pattern. Our datacannot definitively tell us whether the observed relation-ship truly holds only for mothers, for several reasons.First, the rate of participation of fathers was lower than formothers, limiting statistical power for fathers. Althoughthe data for fathers were in the same direction as for moth-ers, only four of the fathers had a parent or sibling with aschizophrenia spectrum disorder. Second, we believe thatthe fathers were not as knowledgeable as historians aboutpsychiatric disorders in their family members as were the
mothers. This would have decreased our sensitivity todetect psychiatric disorders in the father's parents and sib-lings.
The finding that a subtle form of thought disorder isassociated with a familial history of schizophrenia spec-trum disorders is consistent with the findings of Dochertyet al. (1999fo) for another index of communication abnor-malities, the Communication Disturbances Index (CDI),and a family history of psychotic disorders. CDI in parentsof schizophrenia patients was significantly associated witha family history of psychotic disorders. While, by the sim-plest genetic view, one would expect that CDI in parentswould be directly associated with CDI in their offspringwith schizophrenia, Docherty et al. (1999a) found that thiswas not the case. Instead, CDI scores in parents were asso-ciated with overall symptom severity in their offspringwith schizophrenia. However, Shenton et al. (1989) didfind such a parent-offspring correlation using theRorschach Thought Disorder Index. Thus, whether there isa straightforward parent-offspring similarity in subtlethought disorder levels remains unclear and may dependon the measure of thought disorder that is used.
An alternative to the genetic view regarding influ-ences on CD might be that CD, at least in part, is a resultof exposure to an immediate family member with schizo-phrenia spectrum disorder (Miklowitz and Stackman1992). Prior studies of environmental effects have focusedalmost exclusively on the possible impact of parent CD onoffspring schizophrenia spectrum disorder. However, thereis some evidence that contact with one's offspring withschizophrenia might lead to disordered communication inthe parent (Liem 1974).
The complex interplay between genetic and environ-mental influences on thought disorder is seen in an intrigu-ing study of adopted-away offspring of mothers withschizophrenia (Wahlberg et al. 1997a, 19976). Their find-ings suggest that exposure to parental CD might potentiatea genetic predisposition to schizophrenia. They reportedan interaction between having a biological parent withschizophrenia and environmental exposure to a thought-disordered adoptive parent. Offspring with a biologicalparent who had schizophrenia were more likely to developthought disorder when reared by adoptive parents withhigh, as compared to low, CD. Offspring without a biolog-ical parent with schizophrenia were unlikely to developthought disorder regardless of the adoptive parents' levelsof CD.
One possible concern is the representativeness of thecurrent sample. The mean educational level of the subsetof 98 parents (13.9 years ± 2.8 SD) in this report seemshigh, but it is not significantly different from the meaneducational level of all parents of the 104 schizophreniapatients from Project 1 who were potential participants
725
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Schizophrenia Bulletin, Vol. 28, No. 4, 2002 K.L. Subotnik et al.
(13.3 years ± 2.5 SD). Thus, we have little reason to sus-pect that the educational level of these 98 subjects reflectsa selection bias within our sample. It is also possible thatparents who hold less critical attitudes toward their ill off-spring or who exhibit fewer communication abnormalitieswould be more likely to participate in two or moreresearch studies associated with the research clinic provid-ing treatment for their offspring with schizophrenia. Withregard to EE status, our sample of participants in bothProjects 1 and 3 was not different than all participants inProject 1 (53% in the current sample classified as highCFI-EE versus 48% of all Project 1 participants). The pre-sent sample also did not appear to be biased in its distribu-tion of TAT-CD scores in comparison to other studies.Miklowitz et al. (1986) reported TAT-CD data on 205 rela-tives of schizophrenia patients drawn from three separatesites in the United States that were very close to the meanTAT-CD z score in the present study (mean = 0.13, SD =0.41; Miklowitz et al. [1986] sample, mean = 0.15, SD =0.36).
Another potential concern with this study is the use ofthe SCID-II in a family history format. The SCID-II inter-view for the family history format is quite similar to thatfor the direct interview format, and both use fullDSM-III-R criteria. Given that some personality disordersymptoms may be more accurately rated based on thereports of significant others rather than self-report, thisformat may be especially valuable for personality disor-ders. Although we have shown good reliability for admin-istration of the direct interview format (Fogelson et al.1991), this novel use of the SCID-II has not been vali-dated and needs further study.
In summary, we found that a family history of affec-tive disorder is associated with lower rates of EE amongparents of schizophrenia patients. This suggests that priorexposure to a severely depressed relative might promotethe development of more tolerant (i.e., lower EE) attitudestoward one's own child as he or she struggles with a recentonset of schizophrenia. In contrast, our CD results suggestthat high parental CD scores may be a vulnerability indi-cator for level of genetic loading for schizophrenia.Although this genetic loading may not always expressitself in a frank psychotic disorder, it may result in cogni-tive deficits, one of which is tapped by the CD measure.This type of family study, of course, cannot separate sociallearning from genetic influences on CD, so furtherresearch is needed to clarify the origins of CD.
ReferencesAmerican Psychiatric Association. DSM-III-R:Diagnostic and Statistical Manual of Mental Disorders.3rd ed., revised. Washington, DC: APA, 1994.
Andreasen, N.C.; Endicott, J.; Spitzer, R.L.; and Winokur,G. The family history method using diagnostic criteria.Archives of General Psychiatry, 34:1229-1235, 1977.
Asarnow, R.F.; Granholm, E.; and Sherman, T. Span ofapprehension in schizophrenia. In: Steinhauer, S.R.;Gruzelier, J.H.; and Zubin, J., eds. Handbook ofSchizophrenia. Vol. 5. Neuropsychology, Psychophysiology,and Information Processing. Amsterdam, The Netherlands:Elsevier, 1991. pp. 335-370.
Braff, D.L. Information processing and attention dysfunc-tions in schizophrenia. Schizophrenia Bulletin,19(4):233-259, 1993.
Brown, G.W.; Birley, J.L.T.; and Wing, J.K. Influence offamily life on the course of schizophrenic disorders: Areplication. British Journal of Psychiatry, 121:241-258,1972.
Brown, G.W., and Rutter, M. The measurement of familyactivities and relationships: A methodological study.Human Relations, 19:241-263, 1966.
Butzlaff, R.L., and Hooley, J.M. Expressed emotion andpsychiatric relapse: A meta-analysis. Archives of GeneralPsychiatry, 55:547-552, 1998.
DeLisi, L.E., and Crow, T.J. Evidence for a sex chromo-some locus for schizophrenia. Schizophrenia Bulletin,15(3):431-440, 1989.
Docherty, N.M., and Gordinier, S.W. Immediate memory,attention, and communication disturbances in schizophre-nia patients and their relatives. Psychological Medicine,29:189-197, 1999.
Docherty, N.M.; Gordinier, S.W.; Hall, M.J.; and Cutting,L.P. Communication disturbances in relatives beyond theage of risk for schizophrenia and their associations withsymptoms in patients. Schizophrenia Bulletin,25(4):851-862, 1999a.
Docherty, N.M.; Rhinewine, J.P.; Labhart, R.P.; andGordinier, S.W. Communication disturbances and familypsychiatric history in parents of schizophrenia patients.Journal of Nervous and Mental Disease, 186:761-768,1999ft.
Fogelson, D.L.; Nuechterlein, K.H.; Asarnow, R.F.;Payne, D.L.; and Subotnik, K.L. Validity of the familyhistory method for diagnosing schizophrenia, schizophre-nia-related psychoses, and schizophrenia spectrum per-sonality disorders in first-degree relatives of schizophrenicprobands. Schizophrenia Research, in press.
Fogelson, D.L.; Nuechterlein, K.H.; Asarnow, R.F.;Subotnik, K.L.; and Talovic, S.A. Interrater reliability ofthe Structured Clinical Interview for DSM-III-R, Axis II:Schizophrenia spectrum and affective spectrum disorders.Psychiatry Research, 39:55-63, 1991.
726
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021
Communication Deviance and Expressed Emotion Schizophrenia Bulletin, Vol. 28, No. 4, 2002
Gershon, E.S. "Relative Psychiatric History (RPH)Symptom Checklist Interview." 1985. Available from Dr.Elliot Gershon, Bldg 10, Room 3N218, National Instituteof Mental Health, Bethesda, MD 20892.
Goldstein, J.M. Gender and the familial transmission ofschizophrenia. In: Seeman, M.V., ed. Gender andPsychopathology. Washington, DC: American PsychiatricPress, 1995. pp. 201-226.
Goldstein, M.J. The UCLA High-Risk Project.Schizophrenia Bulletin, 13(3):505-514, 1987.
Goldstein, M.J.; Talovic, S.A.; Nuechterlein, K.H.;Fogelson, D.L.; Subotnik, K.L.; and Asamow, R.F. Familyinteraction versus individual psychopathology: Do theyindicate the same processes in the families of schizo-phrenics? British Journal of Psychiatry, 161(Suppl18):97-102, 1992.
Gottesman, I.I. Schizophrenia Genesis. New York, NY:Freeman, 1991.
Hollingshead, A.B. 'Two-Factor Index of Social Position."1957. Available from Dr. August B. Hollingshead,Department of Sociology, Yale University, P.O. Box 208265,New Haven, CT, 06520-8265.
Hooley, J.M., and Gotlib, I.H. A diathesis-stress conceptu-alization of expressed emotion and clinical outcome.Applied and Preventive Psychology, 9:135-151, 2000.
Hooley, J.M., and Hiller, J.B. Family relationships andmajor mental disorder: Risk factors and preventive strate-gies. In: Sarason, B.R., and Duck, S., eds. PersonalRelationships: Implications for Clinical and CommunityPsychology. New York, NY: Wiley, 2001. pp. 135-151.
Jackson, H.J.; Smith, N.; and McGorry, P. Relationshipbetween expressed emotion and family burden in psy-chotic disorders: An exploratory study. Acta PsychiatricaScandinavica, 82:243-249, 1990.
Jones, J. Patterns of transactional style deviance in theTAT's of parents of schizophrenics. Family Process,16:327-337, 1977.
Kendler, K.S. Schizophrenia genetics. In: Sadock, B.J.,and Sadock, V.A., eds. Comprehensive Textbook ofPsychiatry. Vol. 1. Philadelphia, PA: Lippincott, 2000. pp.1147-1159.
Liang, K.H., and Zeger, S.L. Longitudinal data analysisusing generalized linear models. Biometrika, 13:13-22,1986.
Liem, J.H. Effects of verbal communication of parentsand children: A comparison of normal and schizophrenicfamilies. Journal of Consulting and Clinical Psychology,42:438-450, 1974.
Magana, A.B.; Goldstein, M.J.; Karno, M.; Miklowitz,D.J.; Jenkins, J.; and Falloon, I.R.H. A brief method for
assessing expressed emotion in relatives of psychiatricpatients. Psychiatry Research, 17:203-212, 1986.
Miklowitz, D.J.; Goldstein, M.J.; Doane, J.A.;Nuechterlein, K.H.; Strachan, A.M.; Snyder, K.S.; andMagana-Amato, A. Is expressed emotion an index of atransactional process? I. Parents' affective style. FamilyProcess, 28:153-167, 1989.
Miklowitz, D.J., and Stackman, D. Communicationdeviance in the families of schizophrenic and other psy-chiatric patients: Current state of the construct. In: Walker,E.F.; Dworkin, R.H.; and Cornblatt, B.A., eds. Progress inExperimental Psychopathology Research. Vol. 15. NewYork, NY: Springer, 1992. pp. 1^6.
Miklowitz, D.J.; Strachan, A.M.; Goldstein, M.J.; Doane,J.A.; and Snyder, K.S. Expressed emotion and communi-cation deviance in the families of schizophrenics. Journalof Abnormal Psychology, 95:60-66, 1986.
Miklowitz, D.J.; Velligan, D.I.; Goldstein, M.J.;Nuechterlein, K.H.; Gitlin, M.J.; Ranlett, G.; and Doane,J. Communication deviance in families of schizophrenicand manic patients. Journal of Abnormal Psychology,100:163-173, 1991.
Nuechterlein, K.H., and Dawson, M.E. Information pro-cessing and attentional functioning in the developmentalcourse of schizophrenic disorders. Schizophrenia Bulletin,10(2): 160-203, 1984.
Nuechterlein, K.H.; Dawson, M.E.; Gitlin, M.; Ventura,J.; Goldstein, M.J.; Snyder, K.S.; Yee, CM.; and Mintz, J.Developmental processes in schizophrenic disorders:Longitudinal studies of vulnerability and stress.Schizophrenia Bulletin, 18(3):387^25, 1992.
Nuechterlein, K.H.; Goldstein, M.J.; Ventura, J.;Dawson, M.E.; and Doane, J.A. Patient-environmentrelationships in schizophrenia: Information processing,communication deviance, autonomic arousal, and stress-ful life events. British Journal of Psychiatry, 155(Suppl5):84-89, 1989.
Robins, L.N.; Helzer, J.E.; Croughan, J.; and Ratcliff,K.S. National Institute of Mental Health DiagnosticInterview Schedule. Archives of General Psychiatry,38:381-389, 1981.
Rosenfarb, I.S.; Goldstein, M.J.; Mintz, J.; andNuechterlein, K.H. Expressed emotion and subclinicalpsychopathology observable within the transactionsbetween schizophrenia patients and their family members.Journal of Abnormal Psychology, 104:259-267, 1995.
Rosenfarb, I.S.; Nuechterlein, K.H.; Goldstein, M.J.; andSubotnik, K.L. Neurocognitive vulnerability, interpersonalcriticism, and the emergence of unusual thinking bypatients with schizophrenia during family transactions.Archives of General Psychiatry, 57:1174-1179, 2000.
727
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Schizophrenia Bulletin, Vol. 28, No. 4, 2002 K.L. Subotnik et al.
Shenton, M.E.; Solovay, M.R.; Holzman, P.S.; Coleman,M.; and Gale, H.J. Thought disorder in the relatives ofpsychotic patients. Archives of General Psychiatry,46:897-901, 1989.
Spitzer, R.L.; Endicott, J.; and Robins, E. ResearchDiagnostic Criteria: Rationale and reliability. Archives ofGeneral Psychiatry, 35:773-782, 1978.
Spitzer, R.L.; Williams, J.B.W.; and Gibbon, M.Structured Clinical Interview for DSM-III-R PersonalityDisorders (SCID-II). New York, NY: BiometricsResearch Department, 1987.
Strachan, A.M.; Feingold, D.; Goldstein, M.J.; Miklowitz,D.J.; and Nuechterlein, K.H. Is expressed emotion anindex of a transactional process? II. Patient's coping style.Family Process, 28:169-181, 1989.
Subotnik, K.L.; Nuechterlein, K.H.; Asarnow, R.F.;Fogelson, D.L.; Goldstein, M.J.; and Talovic, S.A.Depressive symptoms in the early course of schizophre-nia: Relationship to familial psychiatric illness. AmericanJournal of Psychiatry, 154:1551-1556, 1997.
Subotnik, K.L.; Nuechterlein, K.H.; Asarnow, R.F.;Goldstein, M.J.; Fogelson, D.L.; and Torquato, R.D."Communication Deviance Is Associated With PutativeGenetic Vulnerability Indicators in Relatives ofSchizophrenia Patients." Paper presented at the biennialmeeting of the International Congress on SchizophreniaResearch, Santa Fe, NM, April 1999. [SchizophreniaResearch, 36 (special issue), 185.]
Vaughn, C.E., and Leff, J.P. The influence of family andsocial factors on the course of psychiatric illness: A com-parison of schizophrenic and depressed neurotic patients.British Journal of Psychiatry, 129:125-137, 1976.
Wagener, D.K.; Hogarty, G.E.; Goldstein, M.J.; Asarnow,R.F.; and Brown, A. Information processing and commu-nication deviance in schizophrenic patients and theirmothers. Psychiatry Research, 18:365-377, 1986.
Wahlberg, K.E.; Wynne, L.C.; Keskitalo, P.; Koistinen, P.;Tarvainen, R.; Hakko, H.; Lahti, I.; Laksy, K.; Moring, J.;Naarala, M.; Sorri, A.; Seitamaa, M.; and Tienari, P."Communication Deviance of the Adoptive Parents andPoor Cognitive Functioning of the Adoptees." Paper pre-sented at the Sixth Biennial Meeting of the InternationalCongress on Schizophrenia Research, Colorado Springs,CO, April 1997a.
Wahlberg, K.E.; Wynne, L.C.; Oja, H.; Keskitalo, P.;Pykalainen, L.; Lahti, I.; Moring, J.; Naarala, M.; Sorri,A.; Seitamaa, M.; Laksy, K.; Kolassa, J.; and Tienari, P.Gene-environment interaction in vulnerability to schizo-phrenia: Findings from the Finnish adoptive family studyof schizophrenia. American Journal of Psychiatry,154:355-362, \997b.
Wing, J.K.; Cooper, J.; and Sartorius, N. TheMeasurement and Classification of Psychiatric Symptoms:An Instruction Manual for the PSE and CATEGOPrograms. London, U.K.: Cambridge University Press,1974.
Woo, S.M.; Goldstein, M.J.; and Nuechterlein, K.H.Relatives' expressed emotion and non-verbal signs of sub-clinical psychopathology in schizophrenic patients.British Journal of Psychiatry, 170:58-61, 1997.
Wynne, L.C., and Singer, M.T. Thought disorder and fam-ily relations of schizophrenics: I. A research strategy.Archives of General Psychiatry, 9:191-198, 1963a.
Wynne, L.C., and Singer, M.T. Thought disorder and fam-ily relations of schizophrenics: II. A classification offorms of thinking. Archives of General Psychiatry,9:199-206,19636.
Wynne, L.C.; Singer, M.T; Bartko, J.J.; and Toohey, M.Schizophrenics and their families: Recent research onparental communication. In: Tanner, J.M., ed.Developments in Psychiatric Research. London, U.K.:Hodder and Stoughton, 1977. pp. 254-286.
Acknowledgments
We thank Professor K.Y. Liang, School of Public Health,Johns Hopkins University, Baltimore, MD, for giving usthe SAS macro code for the Generalized Estimating Equa-tion analyses and for providing consultation on its use.Responsibility for the analyses rests with us.
We would also like to thank the following individualsfor their assistance in collecting and/or coding the datareported here: Jeri Doane, Ph.D.; Portia Loughman, B.A.;Martha Magana, B.A.; Sandra Malik, B.A.; Margaret Rea,Ph.D.; Karen Snyder, M.A.; Dawn Velligan, Ph.D.; andSybil Zaiden, B.A. We also acknowledge the statisticalservices of Sun Hwang, M.S., M.P.H., of the University ofCalifornia, Los Angeles Clinical Research Center forSchizophrenia (principal investigator: Robert P. Liberman,M.D.).
This research was supported in part by National Insti-tute of Mental Health grants MH37705, MH49716,MH45112, MH30911, and MH08744 and by a grant fromthe John D. and Catherine T. MacArthur Foundation.
The Authors
Kenneth L. Subotnik, Ph.D., is Associate Research Psy-chologist and Adjunct Associate Professor, Department ofPsychiatry and Biobehavioral Sciences; Michael J. Gold-stein, Ph.D., (deceased) was Professor in the Departmentsof Psychology and of Psychiatry and Biobehavioral Sci-ences; and Keith H. Nuechterlein is Professor in the
728
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021

Communication Deviance and Expressed Emotion Schizophrenia Bulletin, Vol. 28, No. 4, 2002
Departments of Psychiatry and Biobehavioral Sciences Psychiatry and Biobehavioral Sciences, University of Cal-and of Psychology, University of California, Los Angeles. ifornia, Los Angeles. Jim Mintz is Professor in the Depart-Stephanie M. Woo is Assistant Professor of Psychology, ment of Psychiatry and Biobehavioral Sciences, Univer-Pepperdine University, and Assistant Clinical Professor of sity of California, Los Angeles.
729
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/28/4/719/1852848 by guest on 07 D
ecember 2021