
AQA as GCE a Level Biology Unit 1 'Biology and Disease' Summary Notes
96
Unit 1 - Biology and disease AQA AS Biology Unit 1: ‘Biology & Disease’ Summary Notes
Transcript of AQA as GCE a Level Biology Unit 1 'Biology and Disease' Summary Notes
Unit 1 - Biology and disease
AQAAS Biology
Unit 1:‘Biology & Disease’
Summary Notes
Unit 1 - Biology and disease
Biochemistry
Organisation of matter Matter: anything that occupies space and has mass. All forms of matter are made up of elements. The elements hydrogen, carbon and oxygen make up most of the human body. Atoms: the smallest unit of matter that are unique to a particular element. Molecules: units of two or more atoms bonded together. Protons: positive particles. Neutrons: neutral particles. Electrons: negative particles.
BondingIonic bonding: An association between 2 oppositely charged ions. Charged particles (ions) have a change in the number of their electrons. Negative ions gain electrons. Positive ions lose electrons.
Covalent bonding: Atoms share electrons. Single bond – 1 pair shared, eg H2. Double bond – 2 pairs shared, eg O2. Triple bond – 3 pairs shared, eg N2. Polarity: Some covalent molecules are polar.
o Atoms of different elements do not exert the same pull. o The net charge is balanced. o Eg. water.
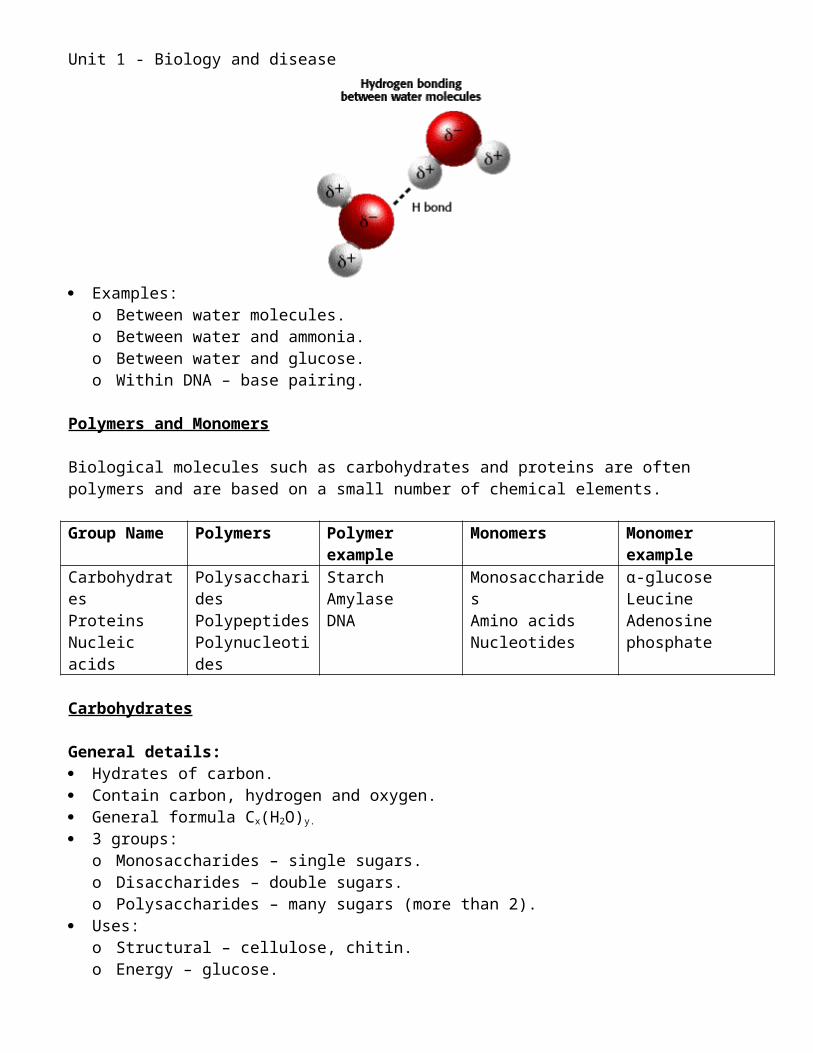
Hydrogen bonding: ‘Van Der Waal’s forces’. An atom of a molecule interacts with another hydrogen atom that is already taking part in a
covalent bond. Due to polarity – the overall charge of each molecule is neutral, but the distribution of
electrons is uneven. Individually weak. Collectively stabilising.
Examples:
Unit 1 - Biology and disease
o Between water molecules.o Between water and ammonia.o Between water and glucose.o Within DNA – base pairing.
Polymers and Monomers
Biological molecules such as carbohydrates and proteins are often polymers and are based on a small number of chemical elements.
Group Name Polymers Polymer example
Monomers Monomer example
CarbohydratesProteinsNucleic acids
PolysaccharidesPolypeptidesPolynucleotides
StarchAmylaseDNA
MonosaccharidesAmino acidsNucleotides
α-glucoseLeucineAdenosine phosphate
Carbohydrates
General details: Hydrates of carbon. Contain carbon, hydrogen and oxygen. General formula Cx(H2O)y.
3 groups:o Monosaccharides – single sugars.o Disaccharides – double sugars.o Polysaccharides – many sugars (more than 2).
Uses:o Structural – cellulose, chitin.o Energy – glucose.o Storage – glycogen, starch.o In nucleic acids – ribose, deoxyribose.
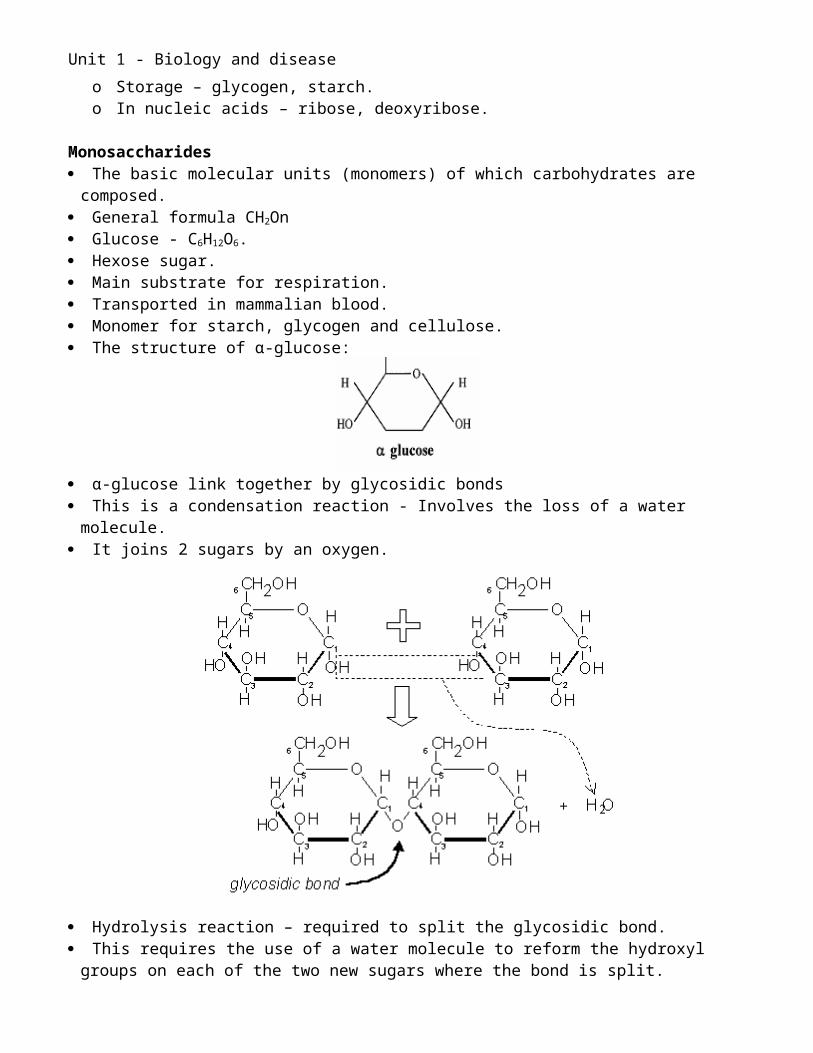
Monosaccharides The basic molecular units (monomers) of which carbohydrates are composed. General formula CH2On Glucose - C6H12O6. Hexose sugar. Main substrate for respiration. Transported in mammalian blood. Monomer for starch, glycogen and cellulose. The structure of α-glucose:
Unit 1 - Biology and disease
α-glucose link together by glycosidic bonds This is a condensation reaction - Involves the loss of a water molecule. It joins 2 sugars by an oxygen.
Hydrolysis reaction – required to split the glycosidic bond. This requires the use of a water molecule to reform the hydroxyl groups on each of the two
new sugars where the bond is split.
Disaccharides Maltose is formed by condensation of two α-glucose molecules Maltose has an α 1,4 glycosidic bond – between carbons 1 and 4. Maltose is a reducing sugar. Sucrose is formed by condensation of glucose and fructose. Sucrose is a non-reducing sugar. Lactose is formed by condensation of glucose and galactose. Lactose is a reducing sugar.
Polysaccharides Polysaccharide = ‘many sugars’. Polymers of monosaccharides. Formed by condensation reactions. Variable numbers of monosaccharides. Branched or unbranched chains. May be folded. Insoluble due to size. Exert no osmotic influence. Do not diffuse easily. Split into disaccharides and monosaccharides by hydrolysis.
Starch Found in most parts of a plant in starch grains.
Unit 1 - Biology and disease
Food reserve from excess glucose. Food supply in seeds for germination. Important food supply in animals. Made of α glucose. Compact for storage. 2 constituent structures:
o Amylose: Approx 20% of starch. α 1,4 glycosidic bonds. Spiral structure held together by hydrogen bonds.
o Amylopectin: Approx 80& of starch. α 1,4 and α 1,6 bonds. Branched chains.
Unit 1 - Biology and disease
Proteins
Polymers of amino acids. Large molecular mass. Wide variety of functions. Carbon, hydrogen, oxygen and nitrogen. Usually sulphur as well. Each species has a particular range of proteins. Determined by the genetic code. Make up two-thirds of total dry mass of cell Make up 18% of human body (second only to water) Most complex and diverse group of biological compounds
Range of Functions:
Function ExamplesStructure Collagen (bone, cartilage, tendon), Keratin (hair) Actin
(muscle)Enzymes Amylase, pepsin, catalaseTransport Haemoglobin (oxygen)Active transport Sodium – Potassium pumps in cell membranesMuscles Myosin and actinHormones Insulin, glucagonAntibodies Immunoglobulins
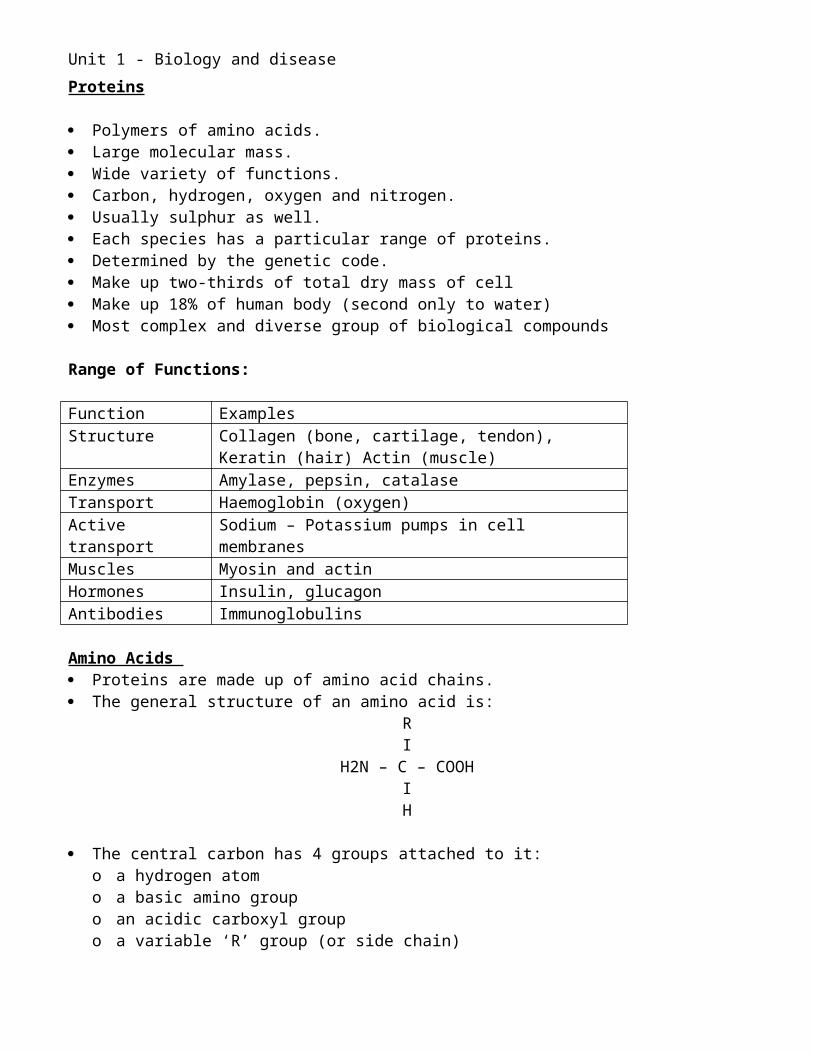
Amino Acids Proteins are made up of amino acid chains. The general structure of an amino acid is:
RI
H2N – C – COOHIH
The central carbon has 4 groups attached to it:o a hydrogen atomo a basic amino groupo an acidic carboxyl groupo a variable ‘R’ group (or side chain)
There are 20 naturally occurring amino acids in living organisms. Half of these can be created in the body – non-essential amino acids. The other half must be consume in the diet – essential amino acids.
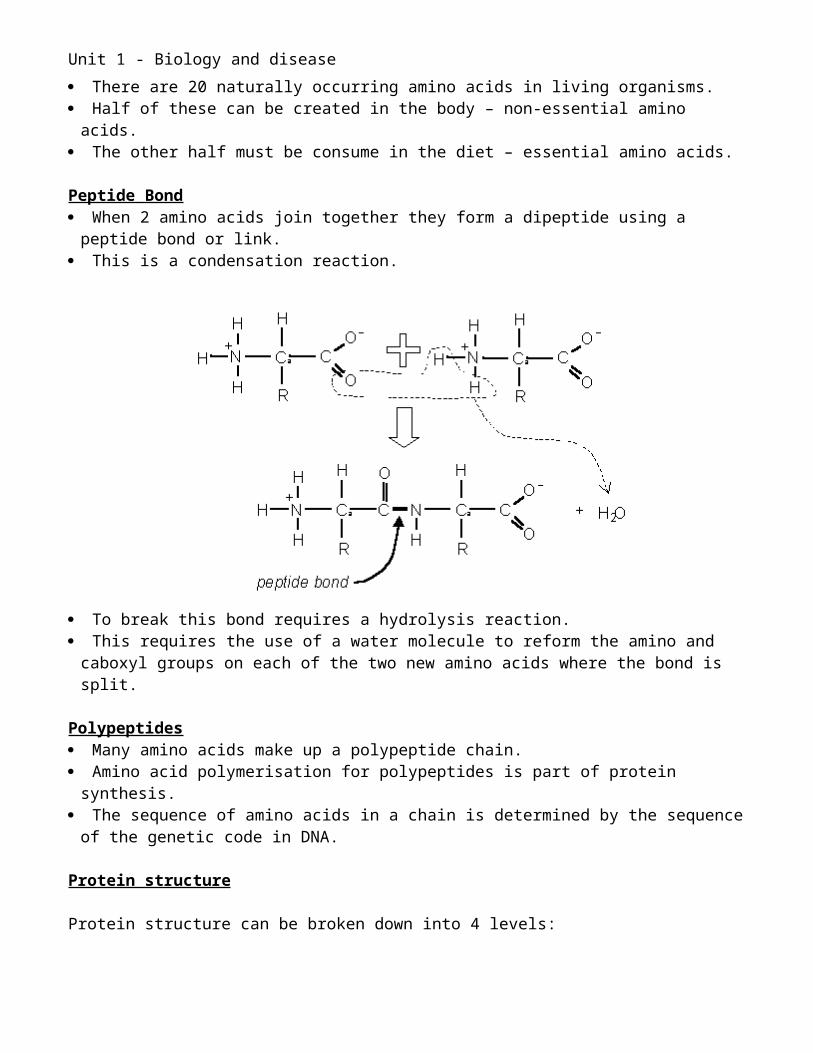
Peptide Bond When 2 amino acids join together they form a dipeptide using a peptide bond or link. This is a condensation reaction.

Unit 1 - Biology and disease
To break this bond requires a hydrolysis reaction. This requires the use of a water molecule to reform the amino and caboxyl groups on each
of the two new amino acids where the bond is split.
Polypeptides Many amino acids make up a polypeptide chain. Amino acid polymerisation for polypeptides is part of protein synthesis. The sequence of amino acids in a chain is determined by the sequence of the genetic code
in DNA.
Protein structure
Protein structure can be broken down into 4 levels:
Primary structure The primary structure refers to the sequence of amino acids Determines rest of protein structure
Secondary structure Amino acid chains fold and move to take up a particular shape Amino acids find the most stable hydrogen bonds Most common secondary structures are α-helix and the β-sheet
Alpha –helix: A regular spiral Held together by hydrogen bonds Very stable Forms part of most proteins
Beta-pleated sheet: A zig-zag formation Consisting of two or more chains
Unit 1 - Biology and disease
Running parallel to each other Linked by hydrogen bonds.
Tertiary structure Overall three-dimensional shape formed by the folding up of a whole polypeptide chain. Every protein has a unique tertiary structure, which is responsible for its properties and
function. Tertiary structure held together by bonds between the R groups of the amino acids. There
are 3 different types:o hydrogen bonds – weako ionic bonds – between oppositely charged R groups, quite strongo disulphide bridges – strong covalent bonds between sulphur on cysteine R groups.
Quarternary structure Final three-dimensional structure This is how different polypeptide chains are joined together. Also includes non-protein prosthetic groups which are present in some proteins. Eg, haemoglobin is a globular protein with 4 polypeptide chains, each with a haem group
(containing an atom of iron).
Fibrous proteins: Long supercoiled chains. Secondary structure is important. Many polypeptide chains run parallel, cross-linked with bonds, eg disulphide bridges. Stable, and structurally strong. Examples:
o Keratin – skin, hair, bones.o Collagen – skin, bones and tendons.o Fibrin – blood clots
Globular Proteins:
Unit 1 - Biology and disease
More spherical. Smaller ones are soluble. Specific shape. Tertiary and quaternary structure forms specific shape. Often part of the protein has a complementary shape to another specific molecule. Examples:
o Hormones – eg insulin and glucagon attach to receptors on cell membraneso Enzymes – active site specific to substrateo Antibodies – complementary to specific antigenso Haemoglobin
Lipids
General details: Large, varied group of organic compounds. Contain carbon, hydrogen and oxygen. Insoluble in water. Dissolve in organic solvents, eg alcohol. 3 main types:
o Triglycerides.o Phospholipids.o Steroids.
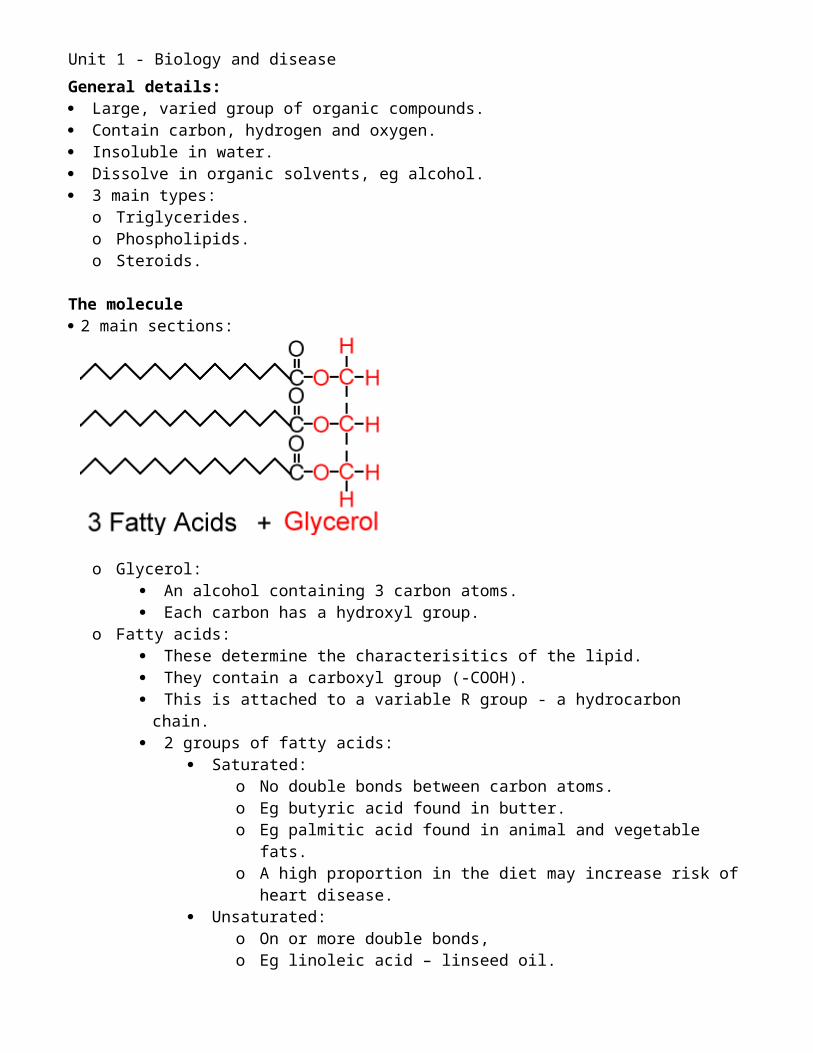
The molecule 2 main sections:
o Glycerol: An alcohol containing 3 carbon atoms. Each carbon has a hydroxyl group.
o Fatty acids: These determine the characterisitics of the lipid. They contain a carboxyl group (-COOH). This is attached to a variable R group - a hydrocarbon chain. 2 groups of fatty acids:
Saturated:o No double bonds between carbon atoms.o Eg butyric acid found in butter.

Unit 1 - Biology and disease
o Eg palmitic acid found in animal and vegetable fats.o A high proportion in the diet may increase risk of heart disease.
Unsaturated:o On or more double bonds,o Eg linoleic acid – linseed oil.o Eg oleic acid – found in olive oil.o Polyunusaturated have 2 or more.o Monounsaturated have one.
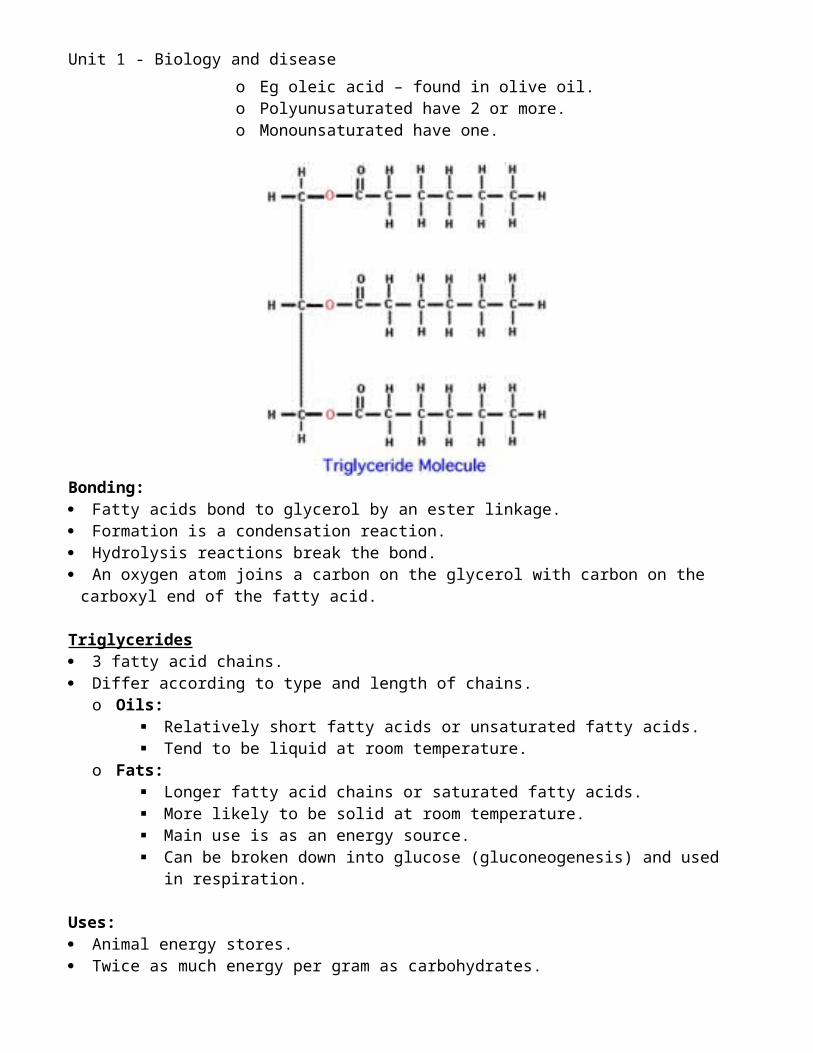
Bonding: Fatty acids bond to glycerol by an ester linkage. Formation is a condensation reaction. Hydrolysis reactions break the bond. An oxygen atom joins a carbon on the glycerol with carbon on the carboxyl end of the fatty
acid.
Triglycerides 3 fatty acid chains. Differ according to type and length of chains.
o Oils: Relatively short fatty acids or unsaturated fatty acids. Tend to be liquid at room temperature.
o Fats: Longer fatty acid chains or saturated fatty acids. More likely to be solid at room temperature. Main use is as an energy source. Can be broken down into glucose (gluconeogenesis) and used in respiration.
Uses: Animal energy stores. Twice as much energy per gram as carbohydrates.
Unit 1 - Biology and disease
Ideal for the low mass required for locomotion. Insulation: Conduct heat slowly. Protection of vital organs. Waterproofing fur and feathers with oil secretions.
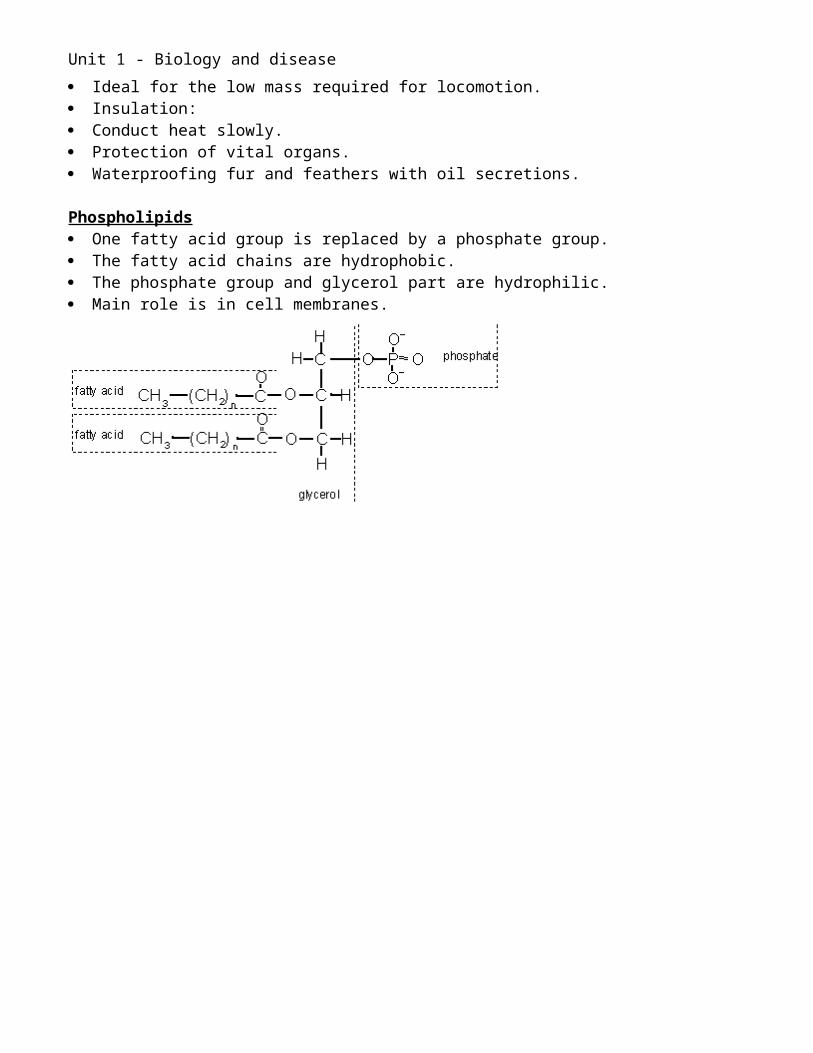
Phospholipids One fatty acid group is replaced by a phosphate group. The fatty acid chains are hydrophobic. The phosphate group and glycerol part are hydrophilic. Main role is in cell membranes.
Unit 1 - Biology and disease
Microscopes
Units of measure
1 meter = 1,000 mm = 1,000,000 µm = 1,000,000,000 nm1 millimeter (mm) = 1/1000 m1 micrometer (µm) = 1/1,000,000 m = 1/1000 mm1 nanometer (nm) = 1/1,000,000,000 m = 1/1000,000 mm = 1/1000 µm
Examples:Frog egg = 1mmHuman egg = 100 µmMost animal cell = 10 to 30 µmMost plant cells = 10 to 100 µmProkaryotic cells = 1 µmMitochondria = 0.5 to 1 µmChloroplast = 5 µmNucleus = 7 µmVirus = 10 to 300 nmRibosome = 30 nm
Magnification : The ratio of how much bigger a sample appears when viewed under the microscope than its
actual size. The resolution limits how much detail can be seen.
Calculating magnification from photographs:
Magnification = length in photographReal length
Calculating real length from photographs:
Real length = Length in photographMagnification
NB for both, convert the length in the photograph into the same units that are used for the specimen. This is usually in micrometers.
Resolution The smallest separation at which two separate objects can be distinguished (or resolved). The greater the resolving power, the more detail can be seen. The resolution of an image is limited by the wavelength of radiation used to view the sample. When objects in the specimen are smaller than the wavelength of the radiation being used,
they do not interrupt the waves, and so are not detected. The resolving power of a light microscope is limited by the wavelength of light (400-600nm
for visible light). Objects closer than 200nm will still only be seen as one point, no matter how great the
magnification.
Unit 1 - Biology and disease
Electrons have a much lower wavelength than light. A beam of electrons has an effective wavelength of less than 1 nm. Electron microscopes have higher resolution.
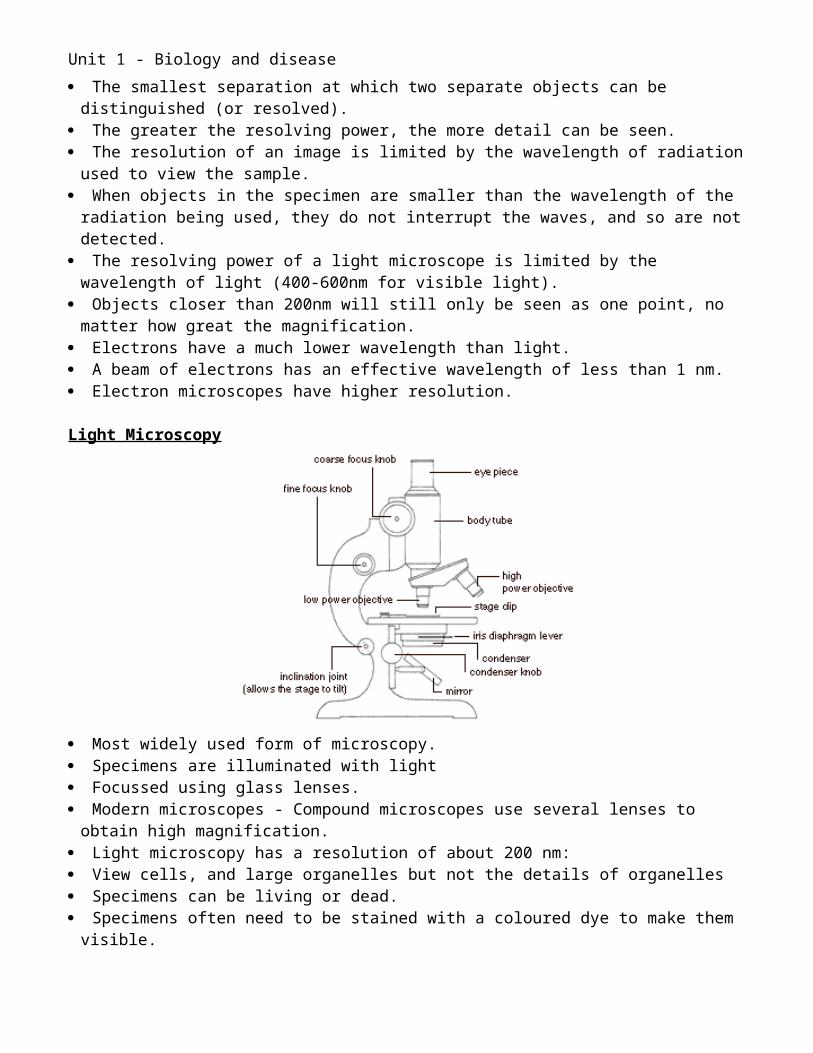
Light Microscopy
Most widely used form of microscopy. Specimens are illuminated with light Focussed using glass lenses. Modern microscopes - Compound microscopes use several lenses to obtain high
magnification. Light microscopy has a resolution of about 200 nm: View cells, and large organelles but not the details of organelles Specimens can be living or dead. Specimens often need to be stained with a coloured dye to make them visible. Many different stains are available that stain specific parts of the cell such as DNA, lipids,
cytoskeleton, etc.
Electron Microscopy. Developed in 1930s. Uses a beam of electrons to "illuminate" the specimen. Electrons behave like waves. Produced using a hot wire Focussed using electromagnets Detected using a phosphor screen or photographic film A beam of electrons has an effective wavelength of less than 1 nm. Resolving power is enough to view small sub-cellular ultrastructure. Mitochondria, ER and membranes can be seen in detail.
Problems Specimens must be fixed in plastic or covered in heavy metals. Viewed in a vacuum. Therefore, specimens must be dead. The electron beam can damage specimens.
Unit 1 - Biology and disease
Must be stained with an electron-dense chemical, usually heavy metals like osmium, lead or gold.
People argue that many observed structures could be artefacts - due to the preparation process and not real.
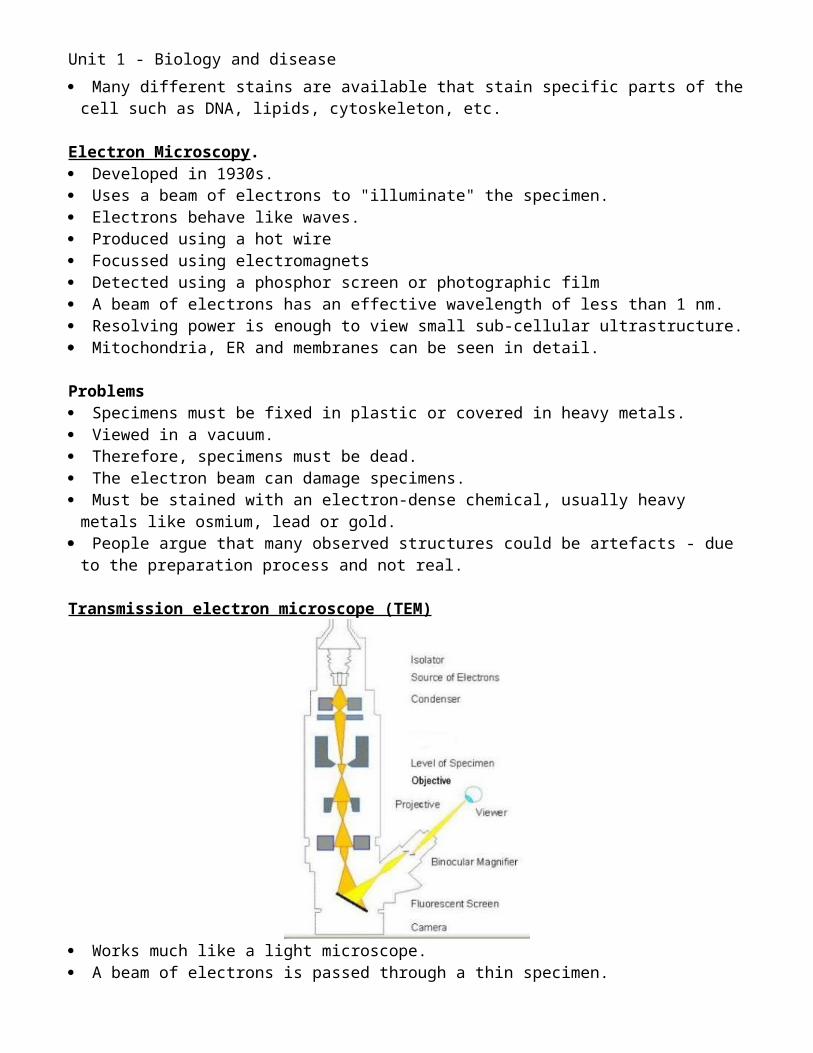
Transmission electron microscope (TEM)
Works much like a light microscope. A beam of electrons is passed through a thin specimen. Electrons are focussed to form an image on a fluorescent screen or on film. Most common form of electron microscope. Best resolution – 0.2 nm Creates a 2-dimensional flat image.
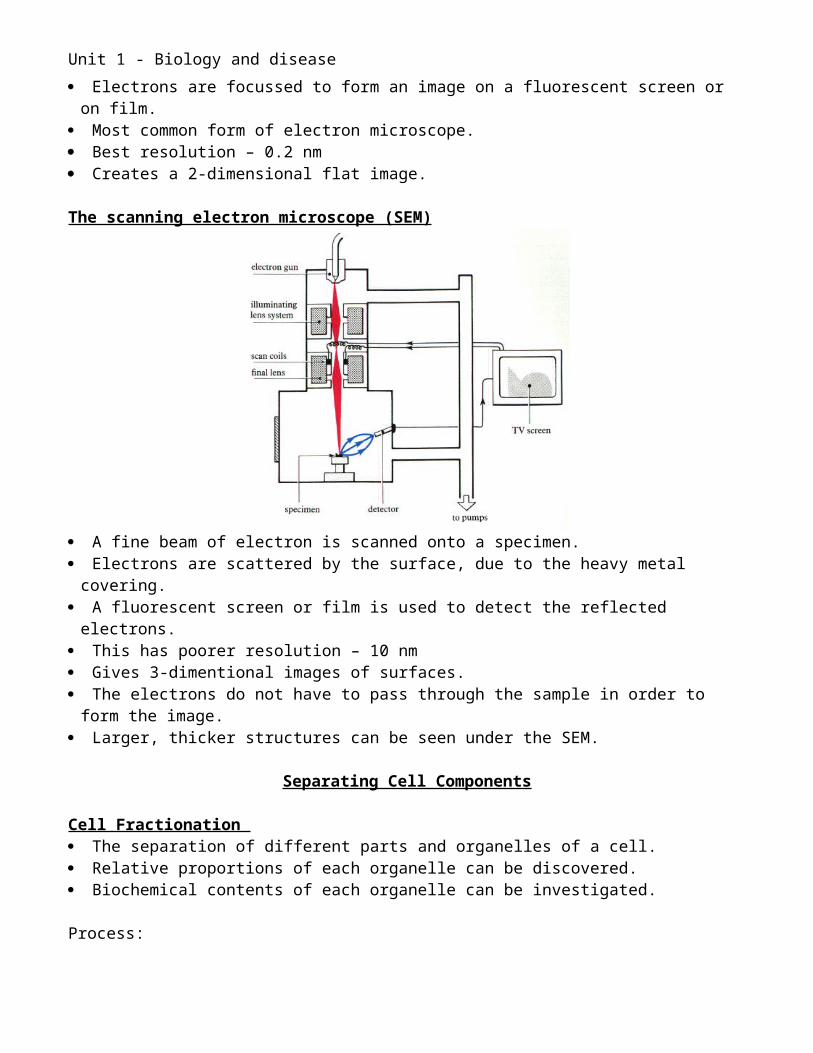
The scanning electron microscope (SEM)
A fine beam of electron is scanned onto a specimen.
Unit 1 - Biology and disease
Electrons are scattered by the surface, due to the heavy metal covering. A fluorescent screen or film is used to detect the reflected electrons. This has poorer resolution – 10 nm Gives 3-dimentional images of surfaces. The electrons do not have to pass through the sample in order to form the image. Larger, thicker structures can be seen under the SEM.
Separating Cell Components
Cell Fractionation The separation of different parts and organelles of a cell. Relative proportions of each organelle can be discovered. Biochemical contents of each organelle can be investigated.
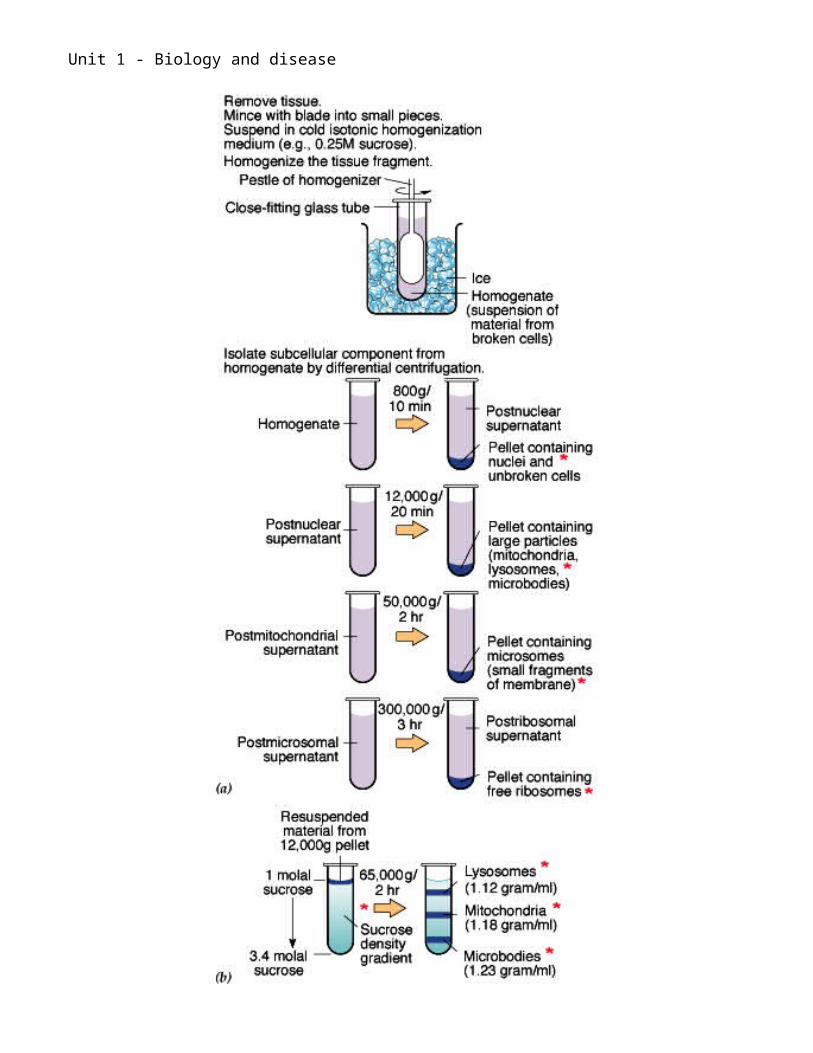
Process:1. Place tissue (e.g. liver, heart, leaf, etc) in ice-cold isotonic buffer.
Cold to stop enzyme reactions. Isotonic to stop osmosis. Buffer to stop pH changes.
2. Grind tissue in a blender to break open cells –homogenation.3. Filter to remove insoluble tissue e.g. fat, connective tissue, plant cell walls, etc. This filtrate
is now called a cell-free extract.
Differential Centrifugation A centrifuge is a piece of equipment, driven by a motor, that puts an object in rotation
around a fixed axis, applying a force that is perpendicular to the axis. The centrifuge works using the sedimentation principle, where the centripetal acceleration is
used to separate substances of greater and lesser density. Svedberg unit – used to compare sizes of ribosomes – a measure of their density.
Process:1. Centrifuge filtrate at low speed and remove pellet.2. Repeat at increasingly higher speeds.3. Each pellet removed contains structures of lower density.
Density gradient centrifugation. The cell-free extract is centrifuged in a dense solution Eg sucrose or caesium chloride The fractions separate out into layers with the densest fractions near the bottom of the tube.
Heaviest NucleiMitochondriaLysosomes
Lightest Ribosomes
Unit 1 - Biology and disease
Unit 1 - Biology and disease
Cells
Cell = the smallest unit of life. All living organisms are made of cells. There are unicellular organisms that consist of one cell:
o Bacteriao Blue-green bacteriao Protozoao Yeast
These individual cells must carry out all of the essential life proceses Other organisms are made of many cells. These are multicellular organisms:
o Animalso Plantso Mushroomso Seaweed
In these the life processes can be delegated to different organs and tissues.
Two main divisions of cells Prokaryotic cells:
o Bacteriao Blue-green bacteria
Eukaryotic cellso Animalso Plantso Fungi o Protoctista
Pro = before Eu = true Karyo = nucleus
Prokaryotic Cells
Example:o Cholera – Vibrio cholerae
Prokaryote = ‘before the nucleus’ Simple cells containing no membrane bound organelles Considered to be the earliest form of life on Earth.
Unit 1 - Biology and disease
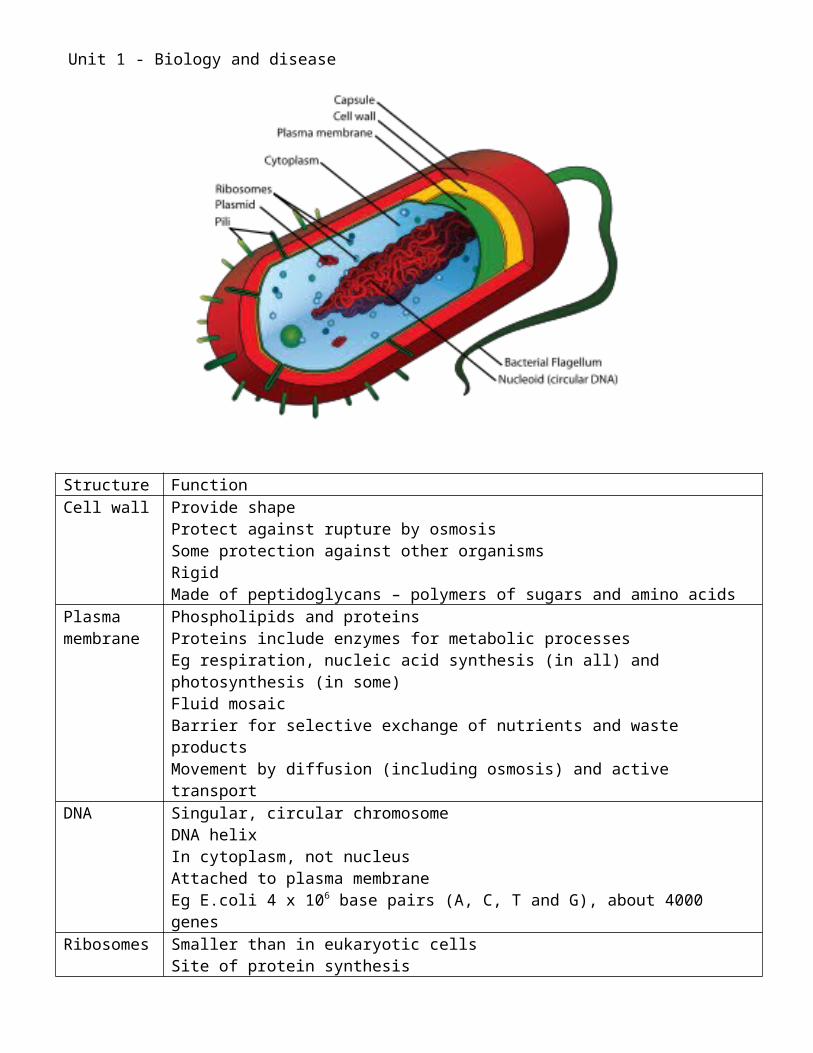
Structure FunctionCell wall Provide shape
Protect against rupture by osmosisSome protection against other organismsRigidMade of peptidoglycans – polymers of sugars and amino acids
Plasma membrane
Phospholipids and proteinsProteins include enzymes for metabolic processesEg respiration, nucleic acid synthesis (in all) and photosynthesis (in some)Fluid mosaicBarrier for selective exchange of nutrients and waste productsMovement by diffusion (including osmosis) and active transport
DNA Singular, circular chromosomeDNA helixIn cytoplasm, not nucleusAttached to plasma membraneEg E.coli 4 x 106 base pairs (A, C, T and G), about 4000 genes
Ribosomes Smaller than in eukaryotic cellsSite of protein synthesis
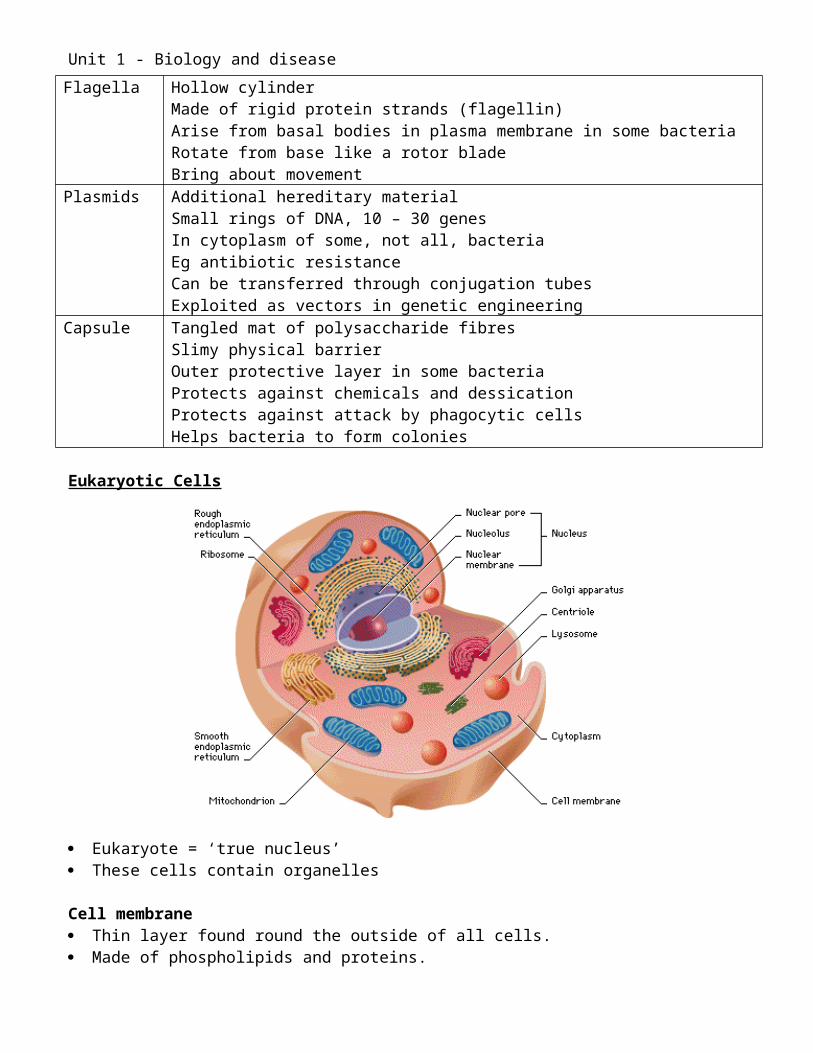
Flagella Hollow cylinderMade of rigid protein strands (flagellin)Arise from basal bodies in plasma membrane in some bacteriaRotate from base like a rotor bladeBring about movement
Plasmids Additional hereditary materialSmall rings of DNA, 10 – 30 genesIn cytoplasm of some, not all, bacteriaEg antibiotic resistance
Unit 1 - Biology and disease
Can be transferred through conjugation tubesExploited as vectors in genetic engineering
Capsule Tangled mat of polysaccharide fibresSlimy physical barrierOuter protective layer in some bacteriaProtects against chemicals and dessicationProtects against attack by phagocytic cellsHelps bacteria to form colonies
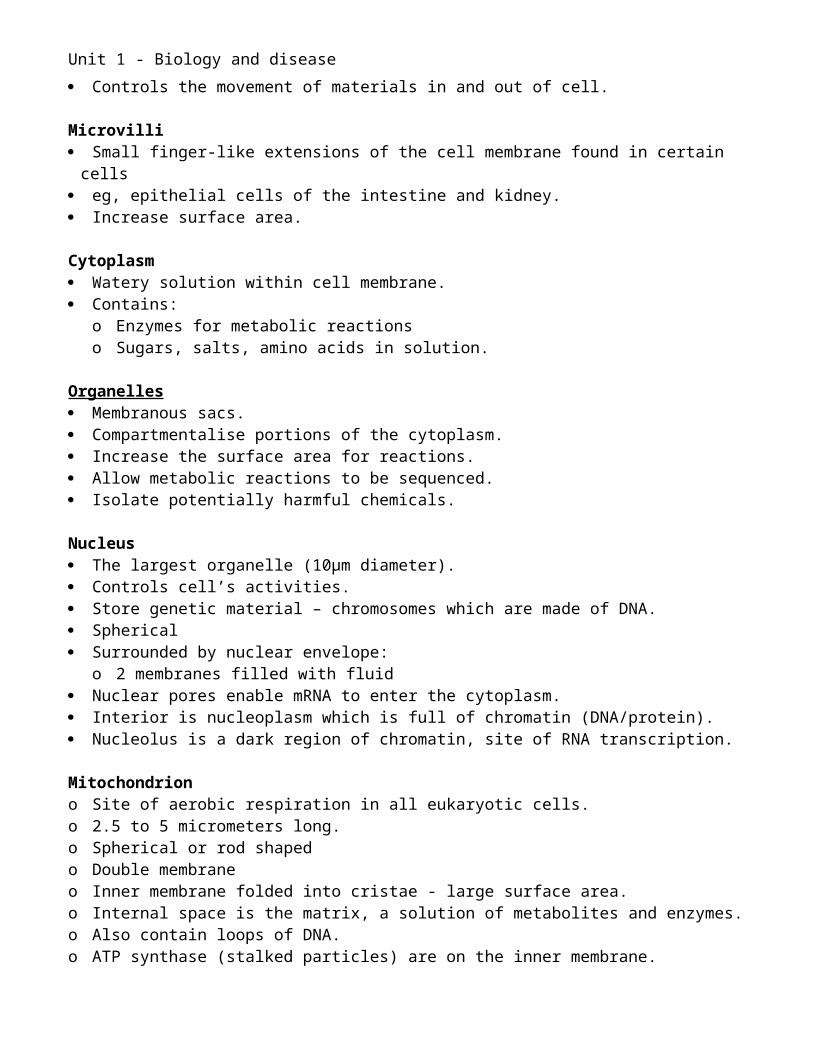
Eukaryotic Cells
Eukaryote = ‘true nucleus’ These cells contain organelles
Cell membrane Thin layer found round the outside of all cells. Made of phospholipids and proteins. Controls the movement of materials in and out of cell.
Microvilli Small finger-like extensions of the cell membrane found in certain cells eg, epithelial cells of the intestine and kidney. Increase surface area.
Cytoplasm Watery solution within cell membrane. Contains:
o Enzymes for metabolic reactionso Sugars, salts, amino acids in solution.
Unit 1 - Biology and disease
Organelles Membranous sacs. Compartmentalise portions of the cytoplasm. Increase the surface area for reactions. Allow metabolic reactions to be sequenced. Isolate potentially harmful chemicals.
Nucleus The largest organelle (10μm diameter). Controls cell’s activities. Store genetic material – chromosomes which are made of DNA. Spherical Surrounded by nuclear envelope:
o 2 membranes filled with fluid Nuclear pores enable mRNA to enter the cytoplasm. Interior is nucleoplasm which is full of chromatin (DNA/protein). Nucleolus is a dark region of chromatin, site of RNA transcription.
Mitochondrion o Site of aerobic respiration in all eukaryotic cells.o 2.5 to 5 micrometers long.o Spherical or rod shapedo Double membraneo Inner membrane folded into cristae - large surface area.o Internal space is the matrix, a solution of metabolites and enzymes.o Also contain loops of DNA.o ATP synthase (stalked particles) are on the inner membrane.o Site of latter stages of respiration.o Metabolically active cells contain numerous mitochondria.o Number of cristae also increases with increased activity.
Ribosomes o Smallest and most abundant ‘organelles’o Not membranouso Site of protein synthesiso Made in nucleoluso Made of protein and RNAo Found either in cytoplasm or attached to the rough endoplasmic reticulum (RER)o Larger type (80S)o Often found in groups called polysomes
Endoplasmic reticulum (ER)o An elaborate system of membranes.o Forms part of the cytoplasmic skeleton.o Extends from the nuclear membrane.o Series of flattened stacks called cisternae.o Enables substances to be synthesised and transported.
Unit 1 - Biology and disease
o Rough ER (RER)o Studded with ribosomes, gives it rough appearanceo Polypeptides synthesised by ribosomes are passed into it.o Pass proteins to Golgi body for further processing.
o Smooth ER (SER)o No ribosomes.o Involved in synthesising and transporting steroids.
Vesicleso Small membrane bound organelles.o Deliver substance around cell.o Take substances:o From ER to Golgio From Golgi to cytoplasm - lysosomeso From Golgi to cell membrane for exocytosis – secretory vesicles
o Eg release of digestive enzymes.
Golgi body (Golgi apparatus)o Series of flattened membrane sacs.o Similar structure to ER.o More compact and curved.o Transports proteins from the RER to the cell membraneo Vesicles of RER fuse with the Golgi on one sideo Contents of the vesicles enter the Golgio Steroids may be modified.o Proteins may acquire tertiary/quaternary structure.o Other groups may be added.o Vesicles bud off the other side and move into the cytoplasm.
Lysosomes o A type of vesicle.o Contain enzymes.o Used to breakdown unwanted toxins or organelles to recycle materials.o Eg used in phagocytosis.
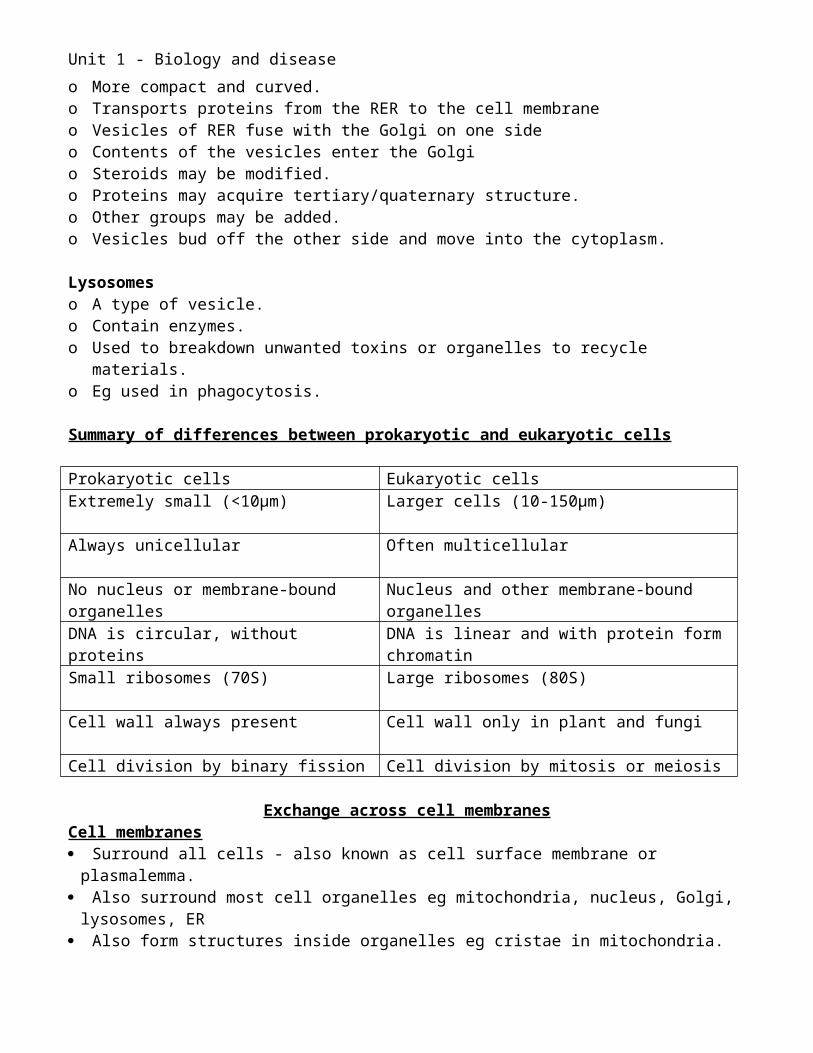
Summary of differences between prokaryotic and eukaryotic cells
Prokaryotic cells Eukaryotic cellsExtremely small (<10μm) Larger cells (10-150μm)
Always unicellular Often multicellular
No nucleus or membrane-bound organelles
Nucleus and other membrane-bound organelles
DNA is circular, without proteins DNA is linear and with protein form chromatinSmall ribosomes (70S) Large ribosomes (80S)
Unit 1 - Biology and disease
Cell wall always present Cell wall only in plant and fungi
Cell division by binary fission Cell division by mitosis or meiosis
Exchange across cell membranesCell membranes Surround all cells - also known as cell surface membrane or plasmalemma. Also surround most cell organelles eg mitochondria, nucleus, Golgi, lysosomes, ER Also form structures inside organelles eg cristae in mitochondria.
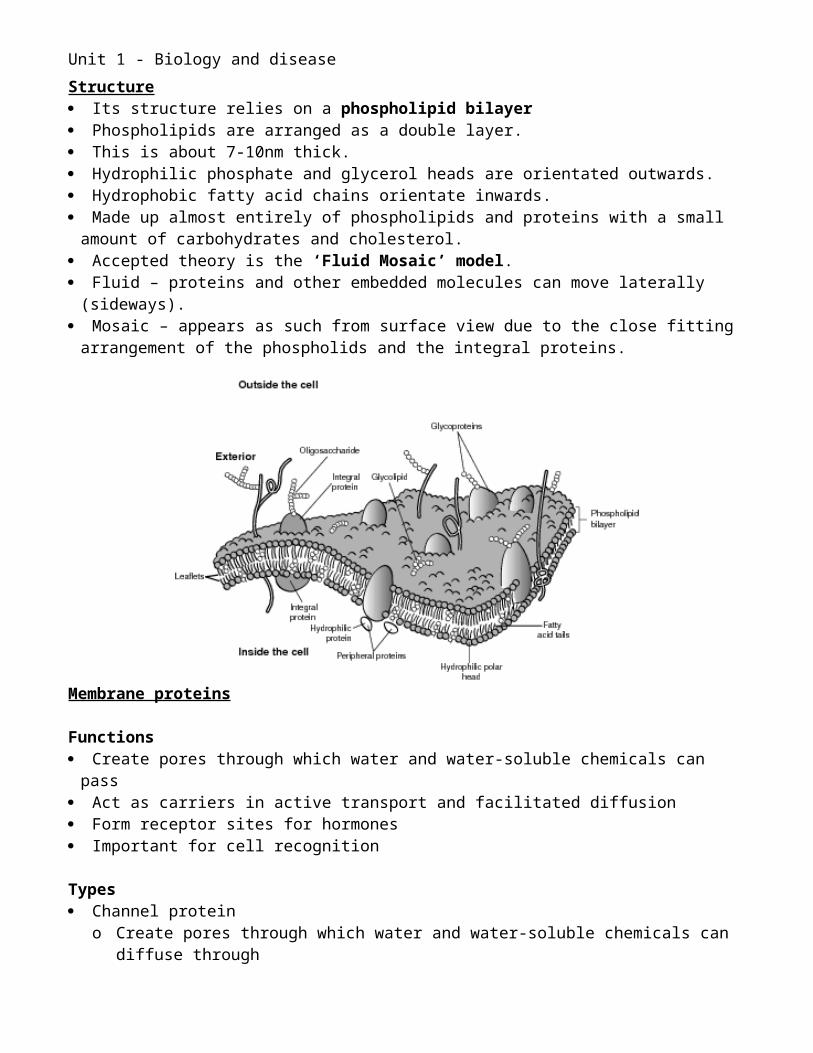
Structure Its structure relies on a phospholipid bilayer Phospholipids are arranged as a double layer. This is about 7-10nm thick. Hydrophilic phosphate and glycerol heads are orientated outwards. Hydrophobic fatty acid chains orientate inwards. Made up almost entirely of phospholipids and proteins with a small amount of carbohydrates
and cholesterol. Accepted theory is the ‘Fluid Mosaic’ model. Fluid – proteins and other embedded molecules can move laterally (sideways). Mosaic – appears as such from surface view due to the close fitting arrangement of the
phospholids and the integral proteins.
Membrane proteins
Functions Create pores through which water and water-soluble chemicals can pass Act as carriers in active transport and facilitated diffusion Form receptor sites for hormones Important for cell recognition
Unit 1 - Biology and disease
Types Channel protein
o Create pores through which water and water-soluble chemicals can diffuse through Carrier proteins
o Involved in facilitated diffusion and active transport Glycoprotein;
o A protein attached to polysaccharide chaino Helps cells to recognise each other
Other constituents of the cell membrane Glycolipids
o Polysaccharide chain attached to a lipid (in place of the phosphate group)o Also help recognition
Cholesterol stabilises the cell membrane.
Movement across membranes
o All living cells are surrounded by water.o Examples:
o Plant cells have a cellulose cell wall but inside this there is a tissue fluid that bathes the cell membrane too.
o In mammals their bodies are covered in a layer of dead cells, below this the cells are living and bathed in tissue fluid.
o Therefore all transport in and out of cells happens in solution.o This transport can happen by various mechanisms.
Diffusion
o Definition: The movement of particles within a gas or liquid from a region of high concentration to a region of lower concentration until an equilibrium is reached.
o All particles in liquids and gases are in constant random motiono If there is a difference in concentration between parts of a gas or liquid, these random
movements carry particles from the area of high concentration to the area of lower concentration.
o The difference in concentration between two areas is the concentration gradient. o The particles move down this gradient.o This continues until the particles become evenly dispersed – dynamic equilibrium.o Diffusion is the main process by which substances move over short distances and is
essential for exchange to occur in all cells.o Diffusion is a passive process = requires no energy
Size and nature of diffusing particle o Fat-soluble molecules can pass through lipid bilayer eg alcohol and steroidso Small molecules such as oxygen and carbon dioxide can diffuse through small pores
between the phospholipidso Larger water-soluble molecules such as glucose and amino acids must pass through
protein pores.
Unit 1 - Biology and disease
o Very large molecules cannot diffuse into cells at all.
Factors affecting the rate of diffusiono Surface area:
o The greater the surface area the greater the rate of diffusion.o Microvilli increase the surface area in some cells.
o Distance:o Determined by the thickness of the membrane.o The greater the distance the slower the rate of diffusion.
o Concentration gradient:o The greater the concentration gradient the greater the rate of diffusion.o Diffusion is more efficient if the gradient can be maintained. o This is done by transporting the substance away once diffused or combining with
other chemicals so it cannot diffuse back.
Fick’s Law:
Rate of Diffusion is proportional to: Surface area x concentration difference distanceFacilitated diffusiono Some substances that may not normally diffuse across a membrane are facilitated (helped)
by proteins in the membrane.o Like diffusion this process is down a concentration gradient and is passive – there is no
energy input.o 2 types:
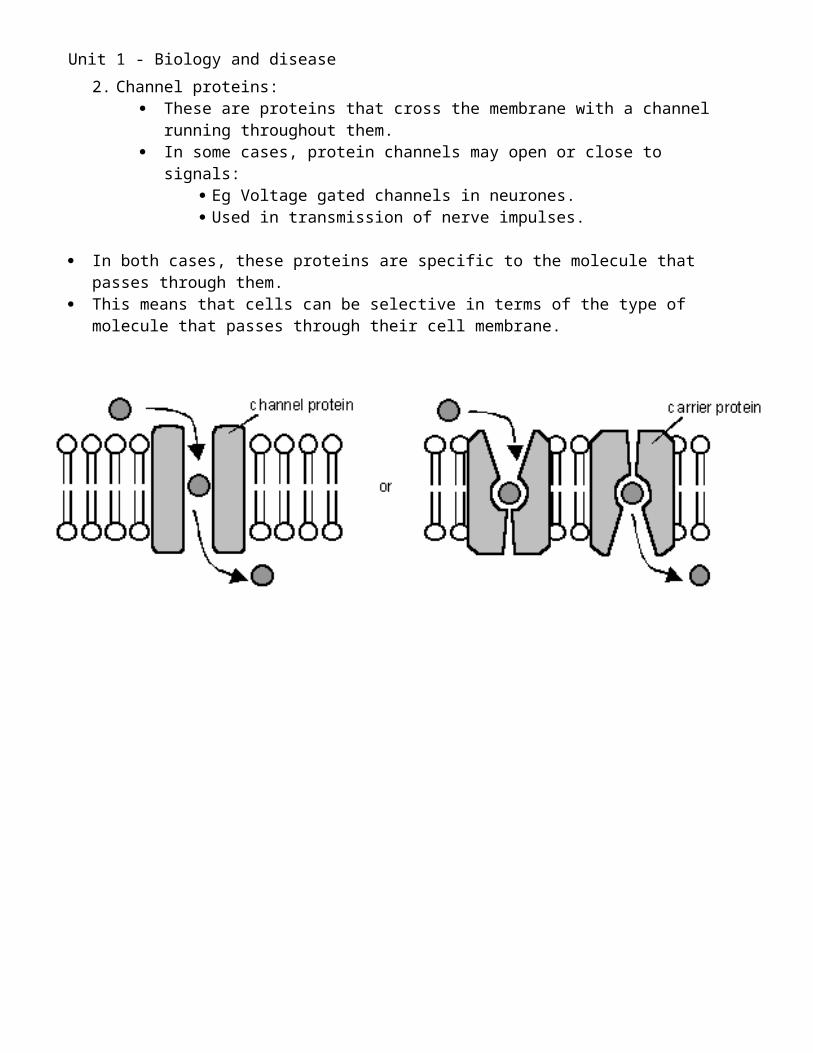
1. Carrier proteins: The molecule binds to protein Protein changes shape Molecule ends up facing the other side of the membrane and is released.
2. Channel proteins: These are proteins that cross the membrane with a channel running throughout
them. In some cases, protein channels may open or close to signals:
Eg Voltage gated channels in neurones. Used in transmission of nerve impulses.
In both cases, these proteins are specific to the molecule that passes through them. This means that cells can be selective in terms of the type of molecule that passes through
their cell membrane.
Unit 1 - Biology and disease
Unit 1 - Biology and disease
Osmosis
o Definition: The net movement of water molecules from a region of their higher concentration to a region of their lower concentration, through a partially permeable membrane.
Explanationo How does water cross the cell membrane?
o Channel proteins – permanently open which allow unrestricted movement of water at all times.
o Lipid pores – although the lipid bilayer is theoretically impermeable to water, water is able to pass through tiny temporary holes that open up as the lipids move around
o Any molecule dissolved in water is known as a solute. o Water molecules are polar.o Solute molecules are attracted to the water molecules, resulting in their being less free-
moving water molecules.o Solute molecules also impede (get in the way of) the movement of water molecules.o Therefore the presence of solute molecules reduces the opportunities for water to cross the
cell membrane.o Osmosis is affected by the relative concentrations of solutes in the two fluids either side of a
membrane.
Water Potentialo A measure of the free kinetic energy of water molecules.o In an equation, the symbol for water potential = ψ (Greek letter ‘psi’)o Units for measurement = kPa (kilopascals) pressure units.o The higher the water potential, the greater the tendency of water molecules to leave a
solution by osmosis.o In standard conditions (25˚C and 100kPa) pure water has a water potential of zero.( ψ= 0)o The addition of solute molecules lowers this value. o More concentrated solution = more negative ψ o Water diffuses from less negative ψ to more negative ψo Eg. from -100kPa to –200kPa
o Better definition:Osmosis is the net movement of water molecules from a region of higher (less negative) water potential to a region of lower (more negative) water potential, across a partially permeable membrane.
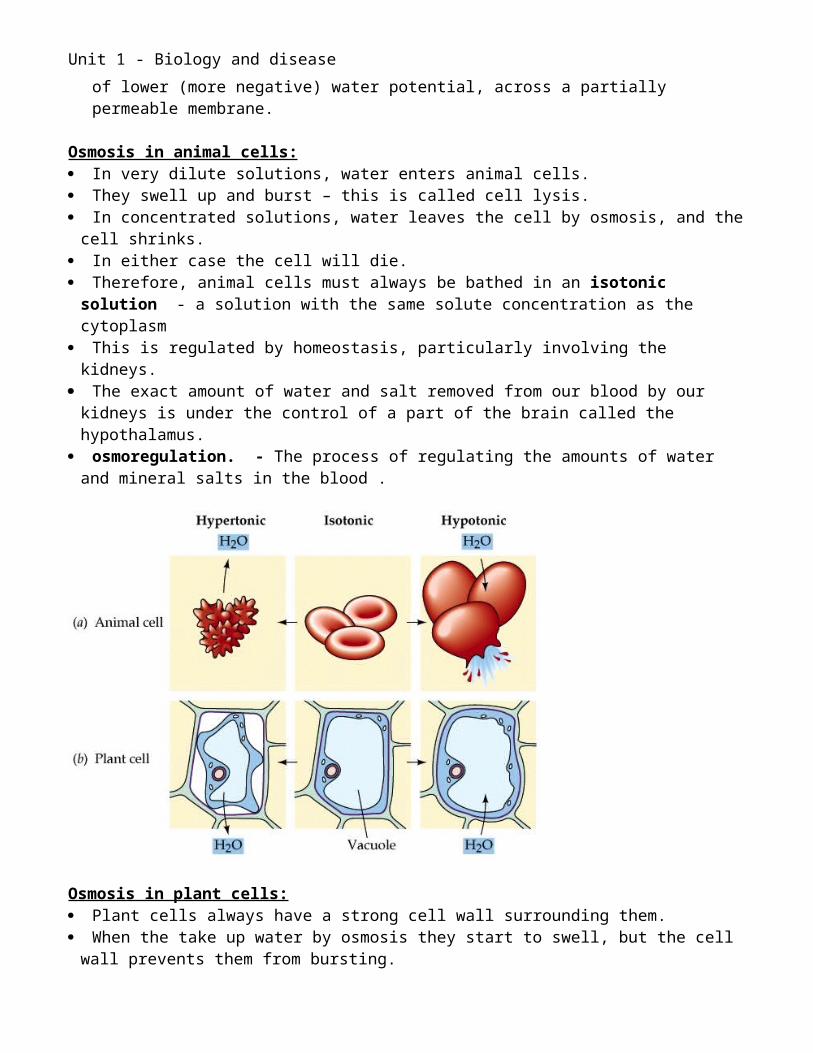
Osmosis in animal cells: In very dilute solutions, water enters animal cells. They swell up and burst – this is called cell lysis. In concentrated solutions, water leaves the cell by osmosis, and the cell shrinks. In either case the cell will die. Therefore, animal cells must always be bathed in an isotonic solution - a solution with the
same solute concentration as the cytoplasm This is regulated by homeostasis, particularly involving the kidneys. The exact amount of water and salt removed from our blood by our kidneys is under the
control of a part of the brain called the hypothalamus.
Unit 1 - Biology and disease
osmoregulation. - The process of regulating the amounts of water and mineral salts in the blood .
Osmosis in plant cells: Plant cells always have a strong cell wall surrounding them. When the take up water by osmosis they start to swell, but the cell wall prevents them from
bursting. Plant cells become "turgid" when they are put in dilute solutions. Turgid means swollen and hard. The pressure inside the cell rises. This pressure works against osmosis. Eventually the internal pressure of the cell is so high that no more water can enter the cell. Turgidity is very important to plants because this is what make the green parts of the plant
"stand up" into the sunlight. When plant cells are placed in concentrated sugar solutions they lose water by osmosis and
they become "flaccid". In this case, plants wilt. The contents of the cells have shrunk and pulled away from the cell wall: they are said to be
plasmolysed. When plant cells are placed in a solution which isotonic they are in a state between turgidity
and flaccidity - incipient plasmolysis.
Unit 1 - Biology and disease
Active transport
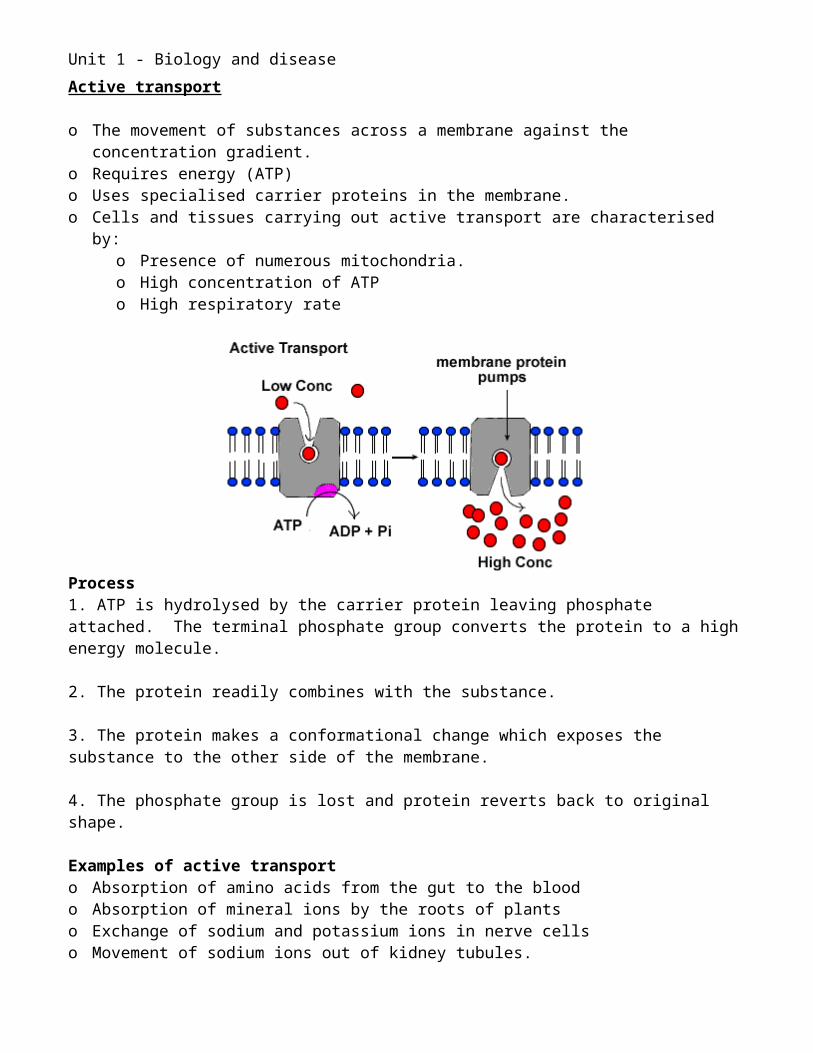
o The movement of substances across a membrane against the concentration gradient.o Requires energy (ATP)o Uses specialised carrier proteins in the membrane.o Cells and tissues carrying out active transport are characterised by:
o Presence of numerous mitochondria.o High concentration of ATPo High respiratory rate
Process1. ATP is hydrolysed by the carrier protein leaving phosphate attached. The terminal phosphate group converts the protein to a high energy molecule.
2. The protein readily combines with the substance.
3. The protein makes a conformational change which exposes the substance to the other side of the membrane.
4. The phosphate group is lost and protein reverts back to original shape.
Examples of active transporto Absorption of amino acids from the gut to the bloodo Absorption of mineral ions by the roots of plantso Exchange of sodium and potassium ions in nerve cellso Movement of sodium ions out of kidney tubules.
o Cells can manipulate osmosis by actively transporting ions to one side of the membrane:o Examples:
Active transport of sodium ions in Kidney tubules Active uptake of mineral ions by Root hair cells Active uptake of specific ions in the small and large intestines
Unit 1 - Biology and disease
Disease
Pathogens Pathogen = a disease inducing organism. The host is the affected organism. Disease = an abnormal condition of an organism that impairs bodily functions. Pathogens include bacteria, viruses and fungi. Bacteria:
o Bacteria are simple, prokaryotic cells – structure is covered later.o They contain no nucleus or membrane bound organelles.o Not all are pathogenic.o Bacteria can tolerate a wide range of conditions, and multiply rapidly.o They often release toxins too.
Viruses:o Viruses are not strictly cells.o They are particles comprising of a protein coat containing genetic material and enzymes.o All viruses are pathogenic.o They must live as a parasite by invading host cells to reproduce – obligate parasites.
Fungio Fungi are more complex, eukaryotic cells.o They have a nucleus and other membrane bound organelles.o Not all are pathogenic.o Fungi reproduce relatively slowly, and rarely infect internal tissues.o They tend to infect external epithelium.
Examples in syllabus:o Cholera
o A bacteriumo Affects the digestive systemo Releases toxinso Causes severe diarrhoea
o Tuberculosiso A bacteriumo Affects the lungs
o Influenzao A viruso Affects the lungs and trachea.o Host’s immune system releases chemicals, which cause fever, muscle aches and
fatigue.
To cause a disease, the pathogen must:1. Enter the body: Gas-exchange system Digestive system Urinogenital system Skin
Unit 1 - Biology and disease
2. Colonise an area of the body: Attachment to the cell membrane, often of epithelial cells.
3.Move into tissues: Secretion of proteolytic enzymes:
o Break down basement membrane of epithelial cells.o Enter tissues/fluids underneath.
4. Multiply: Generation time decreases, stimulated by new environment Rapid multiplication
5. Damage the host’s tissues: When pathogens enter host cells, these cells are often destroyed. Some pathogens release toxins:
o Exotoxins: Soluble proteins Released into environment by the pathogen Travel in blood Effect other parts of body Examples:
Botulinum toxin – muscle paralysis Tetanus neurotoxin – muscle paralysis Gangrene toxin – breaks down cell membranes Enterotoxins - affect intestinal epithelium.
o Endotoxins: Part of the pathogen cell membrane Liberated when the pathogen is destroyed. Responsible for:
Skin rashes Fever Increased permeability of blood vessels, resulting in:
o Severe drop in blood pressureo Circulatory failureo Death
6. Spread – invasiveness: Pathogens may move through lymph vessels and blood stream. Lodge in particular tissues. Rapid multiplication.
Diseases influenced by lifestyleo Lifestyle can affect human health.o Specific risk factors are associated with various diseases.
o Exerciseo Stresso Diet:
Unit 1 - Biology and disease
Salt Fat Malnutrition
o Smokingo Alcohol consumptiono Exposure to:
Car fumes Pollution Coal dust Radiation Asbestos
o Changes in lifestyle may also be associated with a reduced risk of contracting these conditions.
Examples in syllabus:o Asthma:
o Can be cause by numerous allergens eg dust, smoking.o Effects lung function.
o Fibrosis of the lungs:o Can be caused by coal dust.o Effects lung function
o Emphysemao Can be caused by smoking.o Effects lung function
o Atheromao Can be caused by excessive fat (LDLs) in the dieto Effects arteries and blood flow
o Aneurysmo Localised swelling of a blood vessel.o Can rupture causing internal bleeding and death.o Can be exacerbated by smoking and high cholesterol.
o Thrombosiso Formation of a clot in a blood vessel.o Blocks blood flow in or leading to an organ or tissue.o Can be exacerbated by smoking and high cholesterol.
o Coronary heart disease (CHD)o Formation of plaques on the walls of the coronary arteries that supply the muscle of
the heart.o Can limit blood flow to the heart muscle.o If dislodged, can result in:
Myocardial infarction: Blood supply to the heart muscle is interrupted
o Can be exacerbated by smoking and high cholesterol.o Lactose intolerance
o Can be brought about by reduced exposure to milk in the diet.o Production of lactase decreases with time.
Unit 1 - Biology and disease
o Exposure to other diseases can increase the likelihood of lactose intolerance, eg coeliac disease.
Diseases influenced by genetic factorso Some diseases occur due to errors in the DNA.o The onset of these may be exacerbated by lifestyle.
Examples in syllabus:o Cystic fibrosis
o An inherited conditiono Genetic emphysema
o An inherited conditiono A predisposition to this degenerative disease.o Smoking will accelerate its onset.
o Lactose intoleranceo An inherited predisposition to developing lactose intolerance.
What is risk? A measure of the probability that damage to health will occur as a result of a given hazard However, we also need to consider the consequences of the hazard. Eg More people are exposed to car fumes, but smoking probably has greater adverse
consequences than exposure to car fumes. Risk is measured as a percentage.
o 0 % = no harm will occuro 100% = harm will certainly occur
This must be comparative with another scenario Eg not taking exercise vs taking exercise. How much exercise is taken? This data must be provided. Timescale also needs to be provided.
Cancer A class of diseases in which a group of cells display the traits of:
o uncontrolled growth (growth and division beyond the normal limits), o invasion (intrusion on and destruction of adjacent tissues), o and sometimes metastasis (spread to other locations in the body via lymph or blood).
Most cancers form a tumor but some, like leukemia, do not. Nearly all cancers are caused by abnormalities in the genetic material of the transformed
cells. These abnormalities may be due to the effects of carcinogens, such as tobacco smoke,
radiation, chemicals, or infectious agents. They may be randomly acquired through errors in DNA replication, Or, they may be inherited, and thus present in all cells from birth. There are complex interactions between carcinogens and the host genome. This may explain why only some develop cancer after exposure to a known carcinogen.
The link between Lifestyle and Cancer
Unit 1 - Biology and disease
Evidence suggests that around half of all cases of cancer diagnosed in the UK could be avoided if people made changes to their lifestyle.
Smokingo Smoking tobacco is the greatest risk factor for cancer.o It causes more than one in four cancer deaths and has killed six million people over the
last 50 years. Body weight
o Being overweight is known to increase the risk of cancer. Physical activity
o Independent of body weight, people with higher levels of physical activity have a reduced risk of colon and probably breast cancer.
Diet o Various constituents of diet may be increase the chance of contracting cancero Also, various constituents of diet may be protective against cancer.o Eg eating a balanced diet, which contains plenty of fruit and vegetables, can help to
prevent cancer. Sunlight
o Excessive exposure to ultra-violet radiation is the most important modifiable risk factor for skin cancer.
Occupation o Contact with certain harmful substances in the workplace can cause cancer. o Most known occupational carcinogens are either banned or well regulated within the UK.o 9 out of 10 people who develop mesothelioma (a rare type of cancer affecting the lining
of the lung and abdomen) have had contact with asbestos.
Correlations and causal relationships
Causal relationships - a logical relationship between one event (called cause) and another event (called effect).
There will be a correlation between the cause and the effect.
Correlation – a linear relationship between two variables, where an increase or decrease in one variable coincides with an increase or decrease in the other variable.
However, correlation does not imply causation. There may be another variable that causes both of these variables to change.
Example:o Numerous studies showed that women who were taking combined hormone replacement
therapy (HRT) also had a lower-than-average incidence of CHD.o This lead doctors to propose that HRT was protective against CHD. o However, controlled trials showed that HRT actually caused a small and significant increase
in risk of CHD. o Re-analysis of the data showed that women undertaking HRT were more likely to be from
socio-economic groups with better than average diet and exercise regimes. o The two were coincident effects of a common cause, rather than cause and effect.
Unit 1 - Biology and disease
The link between smoking and lung cancer
o The incidence of lung cancer is highly correlated with smoking. o The link between tobacco and cancer was established more than 50 years ago.o Correlations can also be made between smoking and socio-economic backgound.o Therefore, there may be other causative agents.o Estimated 90% of lung cancer deaths are caused by smoking.o Among male smokers, the lifetime risk of developing lung cancer is 17.2%. o Among female smokers, the risk is 11.6%. o This risk is significantly lower in non-smokers:
o 1.3% in men and 1.4% in women. o Cigarette smoke contains over 60 known carcinogens o Additionally, nicotine appears to depress the immune response to malignant growths in
exposed tissue.o The length of time a person smokes as well as the amount smoked increases the person's
chance of developing lung cancer.o If a person stops smoking, this chance steadily decreases as damage to the lungs is
repaired and contaminant particles are gradually removed.o There is evidence that lung cancer in never-smokers has a better prognosis than in
smokers.o Patients who smoke at the time of diagnosis have shorter survival than those who have quit.o Passive smoking is a cause of lung cancer in non-smokers. o Studies from the U.S have consistently shown a significant increase in relative risk among
those exposed to passive smoke.

Unit 1 - Biology and disease
Enzymes
Enzymes are complex chemicals that control reactions in living cells. Enzymes are biological catalysts. They can be used over and over again. They are effective in small amounts. Discovered in 1900 in yeast, enzyme means ‘in yeast’. There are 40,000 different enzymes in human cells, each controlling a different chemical
reaction Increase the rate of reactions by up to 1012 times. Without enzymes the speed of reactions would not support life.
Enzyme Classification Most enzymes end with –ase Some enzymes are given one word names, where the prefix denotes the substrate eg
protease. Other enzymes are given systematic names:
o First word = name of substrateo Second word starts with the type of reaction
Dehydrogenase Oxidase Phosphorylase Carboxylase Decarboxylase Polymerase
o Complete third word with suffix –ase Eg cytochrome oxidase Eg DNA polymerase
Enzyme structure and functiono Enzymes are globular proteins.o Their function is determined by their complex structure.o The reaction takes place in the active site.o Only a few amino acids are involved – catalytic amino acids.o The tertiary structure brings them together.o The substrate binds here, the rest of the protein acts as support.o Enzymes are specific, they only bind with one substrate and control one reaction.o The substrate and the active site are complementary.o Enzymes combine with their substrates to from temporary enzyme-substrate
complexes.o They are released as products due to their change in shape.o Enzymes are not altered or used up by reactions, so can be re-used.o Many enzymes need other chemicals to function – coenzymeso Enzyme function can be slowed or stopped by inhibitors
Enzyme + Substrate Enzyme-substrate complex Enzyme + Products
Unit 1 - Biology and disease
Mechanism of action
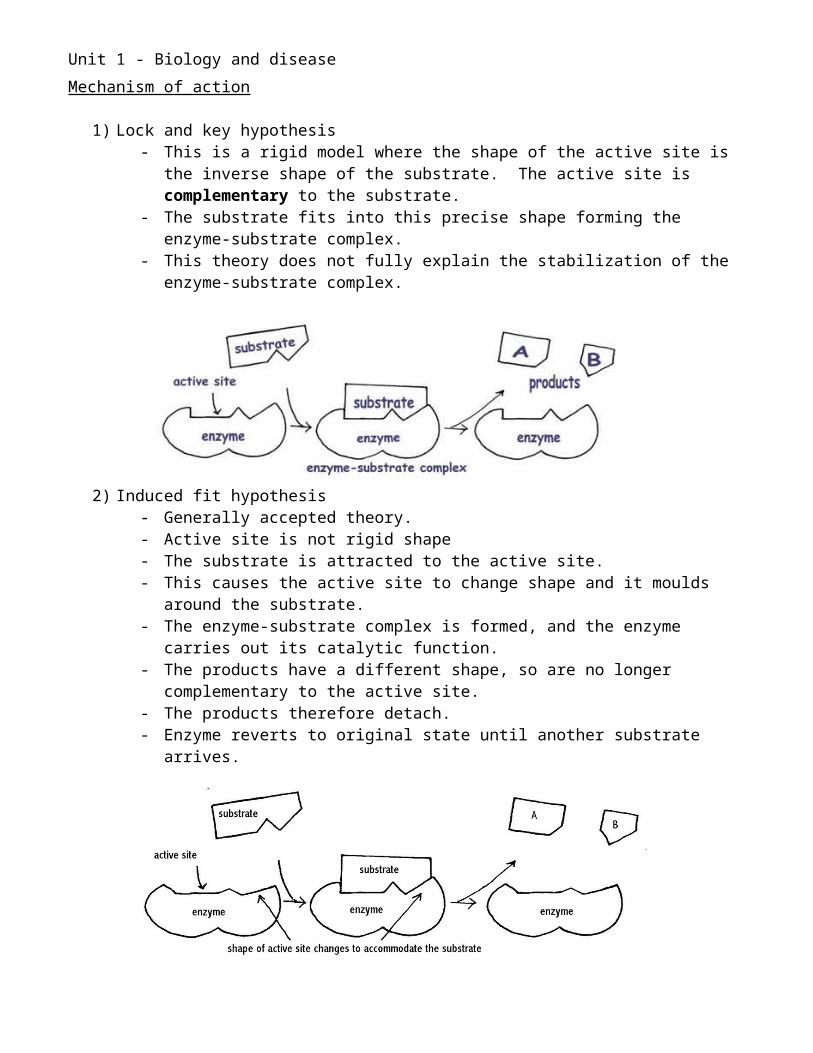
1) Lock and key hypothesis- This is a rigid model where the shape of the active site is the inverse shape of the
substrate. The active site is complementary to the substrate.- The substrate fits into this precise shape forming the enzyme-substrate complex.- This theory does not fully explain the stabilization of the enzyme-substrate
complex.
2) Induced fit hypothesis- Generally accepted theory.- Active site is not rigid shape- The substrate is attracted to the active site.- This causes the active site to change shape and it moulds around the substrate.- The enzyme-substrate complex is formed, and the enzyme carries out its catalytic
function.- The products have a different shape, so are no longer complementary to the
active site.- The products therefore detach.- Enzyme reverts to original state until another substrate arrives.
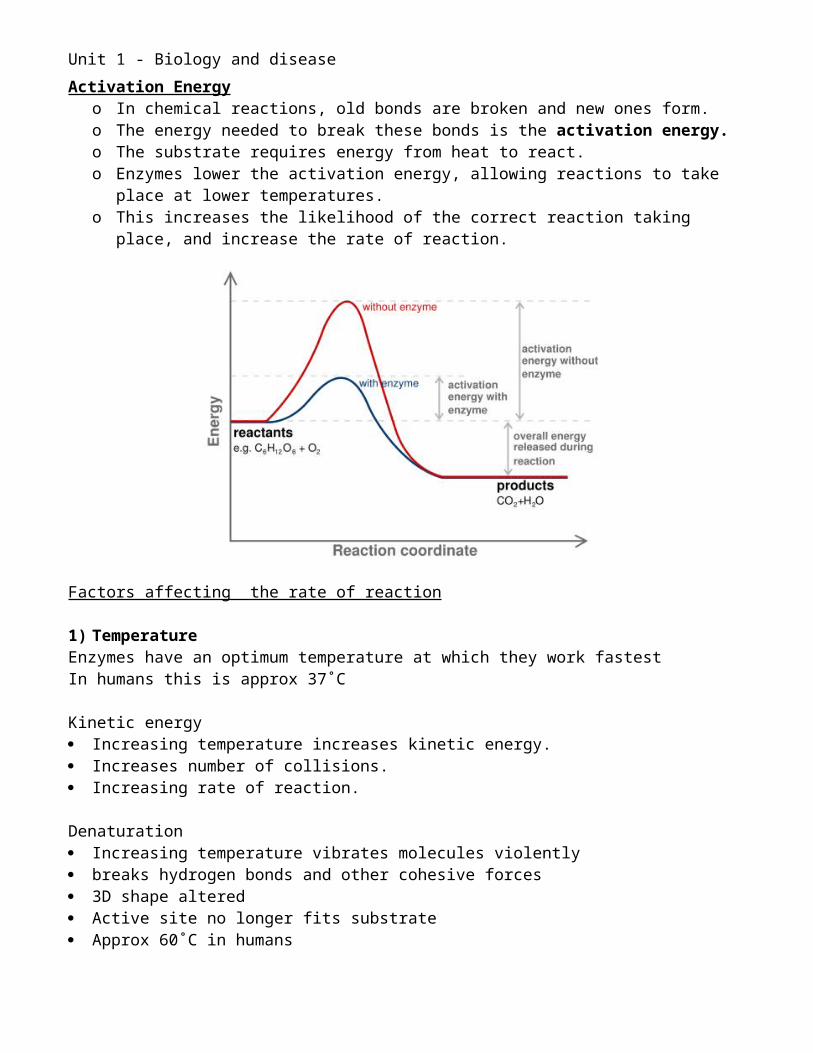
Activation Energyo In chemical reactions, old bonds are broken and new ones form.o The energy needed to break these bonds is the activation energy.o The substrate requires energy from heat to react.o Enzymes lower the activation energy, allowing reactions to take place at lower
temperatures.o This increases the likelihood of the correct reaction taking place, and increase the rate of
reaction.
Unit 1 - Biology and disease
Factors affecting the rate of reaction
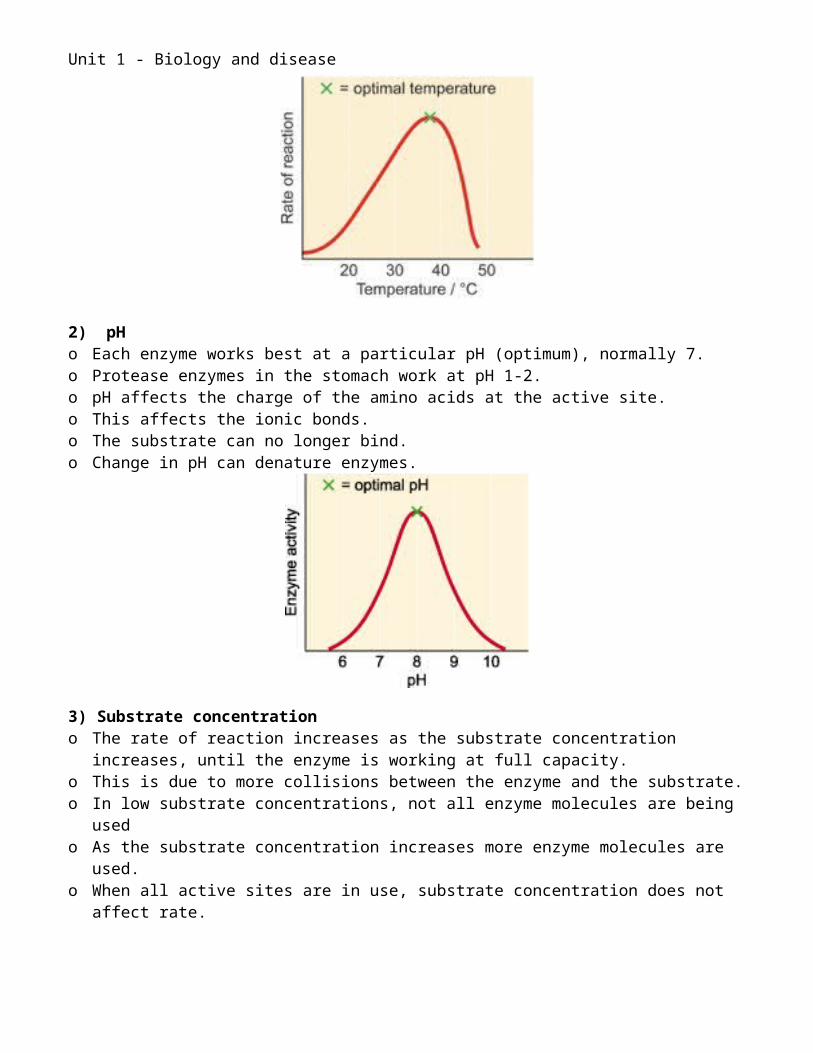
1) TemperatureEnzymes have an optimum temperature at which they work fastestIn humans this is approx 37˚C
Kinetic energy Increasing temperature increases kinetic energy. Increases number of collisions. Increasing rate of reaction.
Denaturation Increasing temperature vibrates molecules violently breaks hydrogen bonds and other cohesive forces 3D shape altered Active site no longer fits substrate Approx 60˚C in humans
Unit 1 - Biology and disease
2) pH o Each enzyme works best at a particular pH (optimum), normally 7.o Protease enzymes in the stomach work at pH 1-2.o pH affects the charge of the amino acids at the active site.o This affects the ionic bonds.o The substrate can no longer bind.o Change in pH can denature enzymes.
3) Substrate concentrationo The rate of reaction increases as the substrate concentration increases, until the enzyme is
working at full capacity.o This is due to more collisions between the enzyme and the substrate.o In low substrate concentrations, not all enzyme molecules are being usedo As the substrate concentration increases more enzyme molecules are used.o When all active sites are in use, substrate concentration does not affect rate.
Unit 1 - Biology and disease
Enzyme inhibition
o Inhibitors can slow down or stop the catalytic activity of enzymes.o Inhibition is a natural process, a mechanism to switch enzymes on or off when needed.o Inhibition tends to be reversible as the enzyme returns to normal when the inhibitor is
removed.o Reversible inhibitors can be competitive or non-competitive
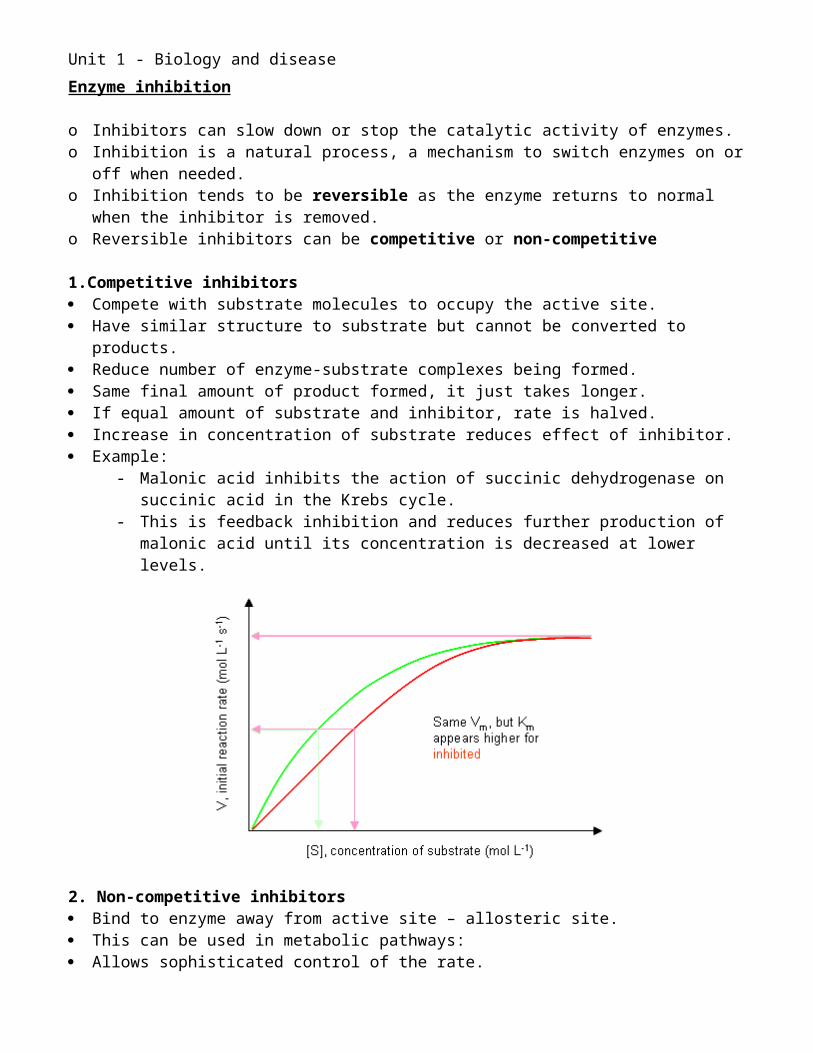
1.Competitive inhibitors Compete with substrate molecules to occupy the active site. Have similar structure to substrate but cannot be converted to products. Reduce number of enzyme-substrate complexes being formed. Same final amount of product formed, it just takes longer. If equal amount of substrate and inhibitor, rate is halved. Increase in concentration of substrate reduces effect of inhibitor. Example:
- Malonic acid inhibits the action of succinic dehydrogenase on succinic acid in the Krebs cycle.
- This is feedback inhibition and reduces further production of malonic acid until its concentration is decreased at lower levels.
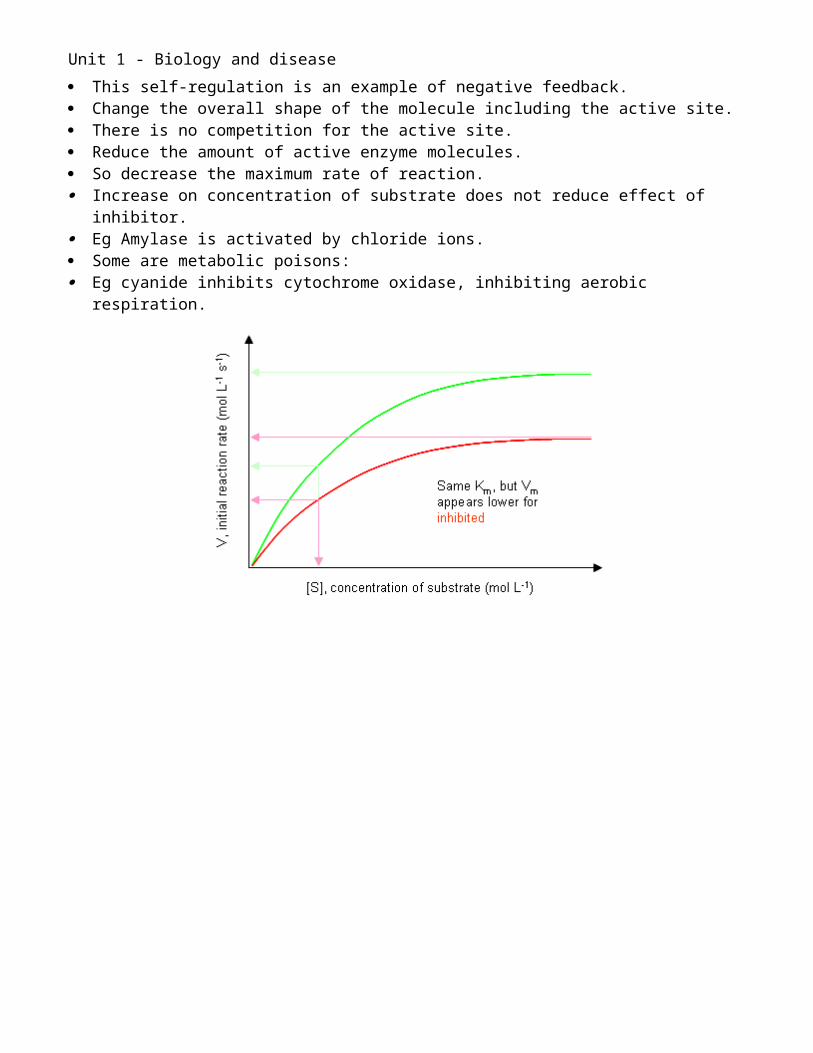
2. Non-competitive inhibitors Bind to enzyme away from active site – allosteric site. This can be used in metabolic pathways: Allows sophisticated control of the rate. This self-regulation is an example of negative feedback. Change the overall shape of the molecule including the active site. There is no competition for the active site. Reduce the amount of active enzyme molecules. So decrease the maximum rate of reaction. Increase on concentration of substrate does not reduce effect of inhibitor. Eg Amylase is activated by chloride ions. Some are metabolic poisons:
Unit 1 - Biology and disease
Eg cyanide inhibits cytochrome oxidase, inhibiting aerobic respiration.
Unit 1 - Biology and disease
Digestion
Ingestion: the taking of nutrients into the organism.Nutrients: organic molecules in food. Most of these are large and insoluble.Digestion: the process by which large, insoluble organic molecules in food are broken down into small, soluble organic molecules, to enable their absorption into the blood stream.Absorption: the process by which small, soluble nutrient molecules pass from the lumen of the gut into the blood stream.Assimilation: the processes by which the cells metabolise the nutrient molecules.Egestion: the removal of undigested food molecules from the organism (in humans this is mainly cellulose).
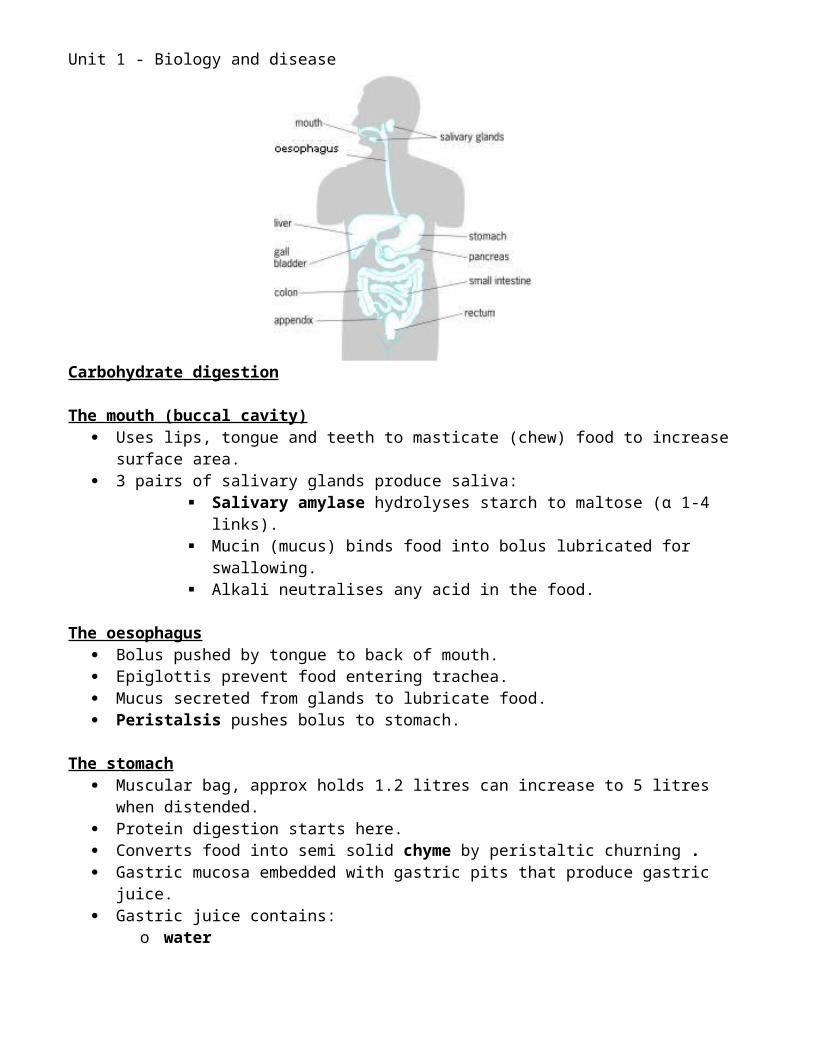
Humans are heterotrophs - they take nutrients in from their surroundings. They digest food, and absorb simple molecules that are produced. To do this they need a gut. In mammals this is an alimentary canal This is a muscular tube from mouth to anus. The alimentary canal is in well defined regions
o buccal cavity (mouth)o oesophaguso stomacho small intestine:
duodenum ileum
o caecumo appendixo large intestine:
colon rectum
Digestive system consists of alimentary canal and glands that secrete into it.o Salivary glands – into moutho Pancreas – into duodenumo Liver (via the gall bladder) – into duodeum
Unit 1 - Biology and disease
Carbohydrate digestion
The mouth (buccal cavity) Uses lips, tongue and teeth to masticate (chew) food to increase surface area. 3 pairs of salivary glands produce saliva:
Salivary amylase hydrolyses starch to maltose (α 1-4 links). Mucin (mucus) binds food into bolus lubricated for swallowing. Alkali neutralises any acid in the food.
The oesophagus Bolus pushed by tongue to back of mouth. Epiglottis prevent food entering trachea. Mucus secreted from glands to lubricate food. Peristalsis pushes bolus to stomach.
The stomach Muscular bag, approx holds 1.2 litres can increase to 5 litres when distended. Protein digestion starts here. Converts food into semi solid chyme by peristaltic churning . Gastric mucosa embedded with gastric pits that produce gastric juice. Gastric juice contains:
o watero hydrochloric acid – creates pH 2 which kills bacteria – this denatures amylase.o pepsin – digests proteins, so digests the amylase.
Chyme is gradually released over 3-4 hours. Pyloric sphincter controls exit in small squirts.
The small intestine Over 6 metres in lengths Duodenum is approx 25cm in length. Ileum is over 5.5 metres. Luminal epithelium (inner tissue layer) is folded into villi – 0.5mm to 1mm long
o increase surface areao in contact with more food.
Luminal epithelial e is folded into microvilli o Further increase surface area.
Digestion in the small intestineThere are three main secretions of digestive juices:
Bile Created by the liver. Stored in gall bladder. Secreted via bile duct into small intestine. Contains no enzymes. Contains alkali which neutralises acidic chyme for enzymes.
Pancreatic juice Secreted by the pancreas via the pancreatic duct to the duodenum.
Unit 1 - Biology and disease
It is alkaline to neutralise stomach acid, provides optimum pH for enzymes. Contains various enzymes, including:
o Pancreatic amylase – this completes hydrolysis of starch to maltose.
Intestinal juice Secreted from the cells covering villi. Contains alkali and mucus. Contains few, if any, enzymes.
Membrane-Bound Enzymes Bound to luminal membrane of epithelial cells. May be found in intestinal juice due to sloughing of these cells.
o Carbohydrases – hydrolyse glycosidic bonds, releasing monosaccharides: Sucrase digests sucrose to glucose and fructose Maltase digests maltose to glucose Lactase digests lactose to glucose and galactose
Absorption in the small intestine
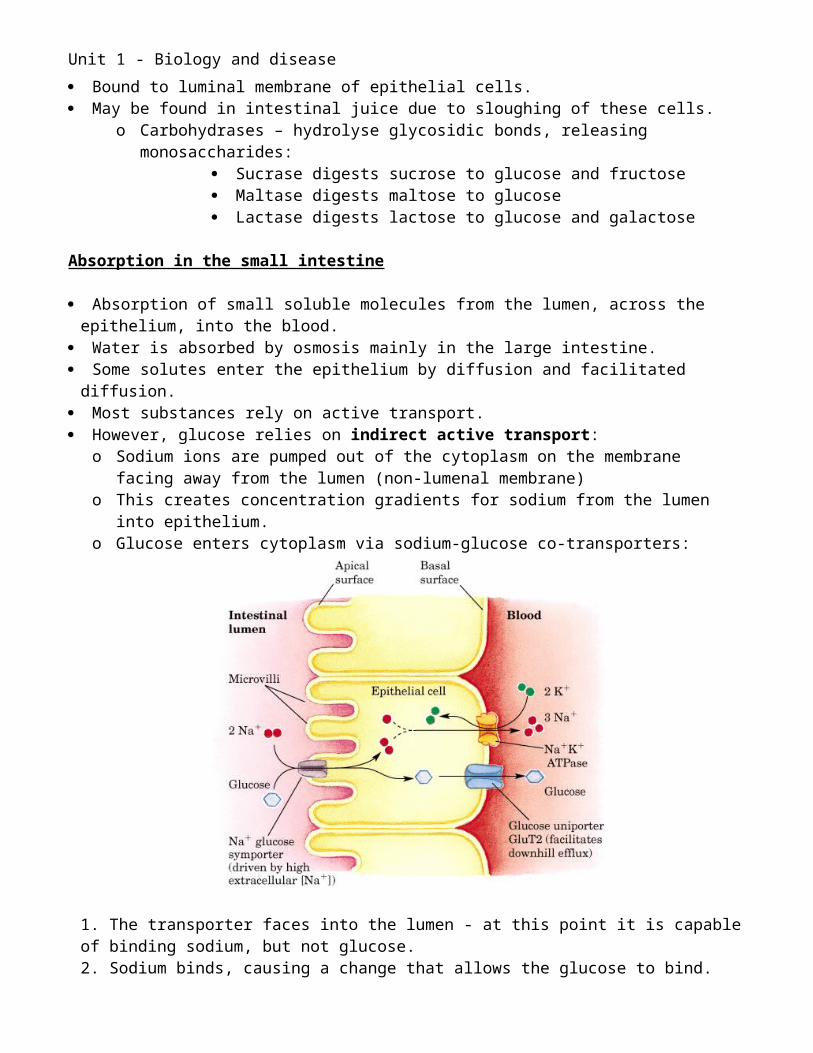
Absorption of small soluble molecules from the lumen, across the epithelium, into the blood. Water is absorbed by osmosis mainly in the large intestine. Some solutes enter the epithelium by diffusion and facilitated diffusion. Most substances rely on active transport. However, glucose relies on indirect active transport:
o Sodium ions are pumped out of the cytoplasm on the membrane facing away from the lumen (non-lumenal membrane)
o This creates concentration gradients for sodium from the lumen into epithelium.o Glucose enters cytoplasm via sodium-glucose co-transporters:
Unit 1 - Biology and disease
1. The transporter faces into the lumen - at this point it is capable of binding sodium, but not glucose.2. Sodium binds, causing a change that allows the glucose to bind. 3. Glucose binds and the transporter changes shape allowing sodium and glucose to be moved inside the cell 4. Sodium and glucose detach from the co-transporter into the cytoplasm.
This establishes a concentration gradient for glucose from cytoplasm towards the blood. Glucose leaves the cytoplasm by facilitated diffusion.
Adaptations of the small intestine (ileum) to maximise absorption: Large surface area:
o Long – 6mo Foldedo Villio Microvilli
Maintaining concentration gradients:o Peristalsis delivers more nutrientso Active transport removes nutrients from lumeno Extensive capillary network provides an excellent blood supply to remove nutrients
from epithelial cells. Short distances:
o One cell thick epitheliumo Capillaries lie next to epithelial cells.o Thin walls around capillaries.
The large intestine Excess water from digestive secretions are absorbed. The undigested food is expelled as faeces.
Lactose intolerance Lactose is the major sugar found in milk. It is a disaccharide. Lactase hydrolyses lactose into glucose and galactose. These are then absorbed into the blood stream. Lactose production naturally declines slightly after childhood. People with lactose intolerance do not secrete enough lactose. They are unable to digest significant amounts of lactose. Lactose remains in the intestines. Bacteria metabolise this sugar, and produce large volumes of gas. This causes abdominal bloating, cramps and flatulence. The lactose reduces the water potential in the intestines. The large intestine cannot reabsorb enough water. This can result in diarrhoea.
Causes1. Primary lactase deficiency:
Unit 1 - Biology and disease
Genetic factors cause the production of lactase to decline at a young age (after 2 years old).
2. Secondary lactase deficiency Diseases can reduce the lactase production. Examples – Celiac disease and Crohn’s disease.
Cholera An infectious disease caused by the bacterium Vibrio cholerae. Transmitted through ingesting contaminated water or food. If enough are consumed, some may survive stomach acid. They use their flagella to propel themselves into the epithelial cells. Cholera produces toxins. These interact with chloride protein pumps in the small intestine. This increases secretion of chloride ions into the lumen of the small intestine. This establishes a water potential gradient from the epithelium into the lumen. Vast quantities of water are lost by osmosis. This results in severe diarrhoea. This results in severe dehydration. Also, essential electrolytes are lost – these are ions, including sodium and potassium. These are required for metabolic processes in cells. Vomiting may also exacerbate fluid losses. Internal organs fail, coma results, followed by cardiac arrest and death.
Oral rehydration solution (ORS) – Oral rehydration therapy. A mixture of glucose and electrolytes (sodium, potassium, chloride and citrate ions) in
sachets. Each is mixed with a specific volume of water (1 litre). This provides a specific concentration of glucose and electrolytes. Water – for rehydration Sodium – enables use of sodium-glucose cotransporters. Glucose – also enables use of sodium-glucose cotransporters. Therefore, sodium and glucose can be absorbed quickly. Potassium, chloride and citrate ions can also be absorbed. Minimal training and expertise is required to administer this. It is relatively cheap, and can save many lives in developing countries.
Testing and trialling new drugs1. Research leads to the development of a new drug.2. Apply for a patent.3. Investigate potential adverse effects by chemical testing and using laboratory animals.4. Test on small group of healthy volunteers (eg 50) to check for side effects.5. Test on a larger group who have the disease (eg 200) to check for effectivity.6. Double blind trial on a much larger group with the disease.
Half receive a placebo – treated exactly the same but receive no active ingredient. Half receive the active ingredient. Neither patient nor doctor know who receives which. Results are sent to research scientists.
7. Findings are published in a journal. Other scientists review the findings (peer review). They may replicate the experiments to check for repeatability of the results.
Unit 1 - Biology and disease
8. A licence may be granted many years after the initial development, by which time there may not be many years left for the patent.
9. Monitoring continues all the time the drug is available.
Ethical issues associated with ORS use Patients are already severely ill. They may not be in a fit state to commit to the trial. Also, new formulations may not work. They may even make the symptoms worse. In double blind trials, half the patients receive no active ingredients, so will not improve. Greatest incidence of diarrhoea diseases is in developing countries. Pharmaceutical companies profit from this. Also governments may receive payments, but the patients may not be recompensed. Human rights issues have improved in recent years.
Unit 1 - Biology and disease
Lungs & Gas exchange
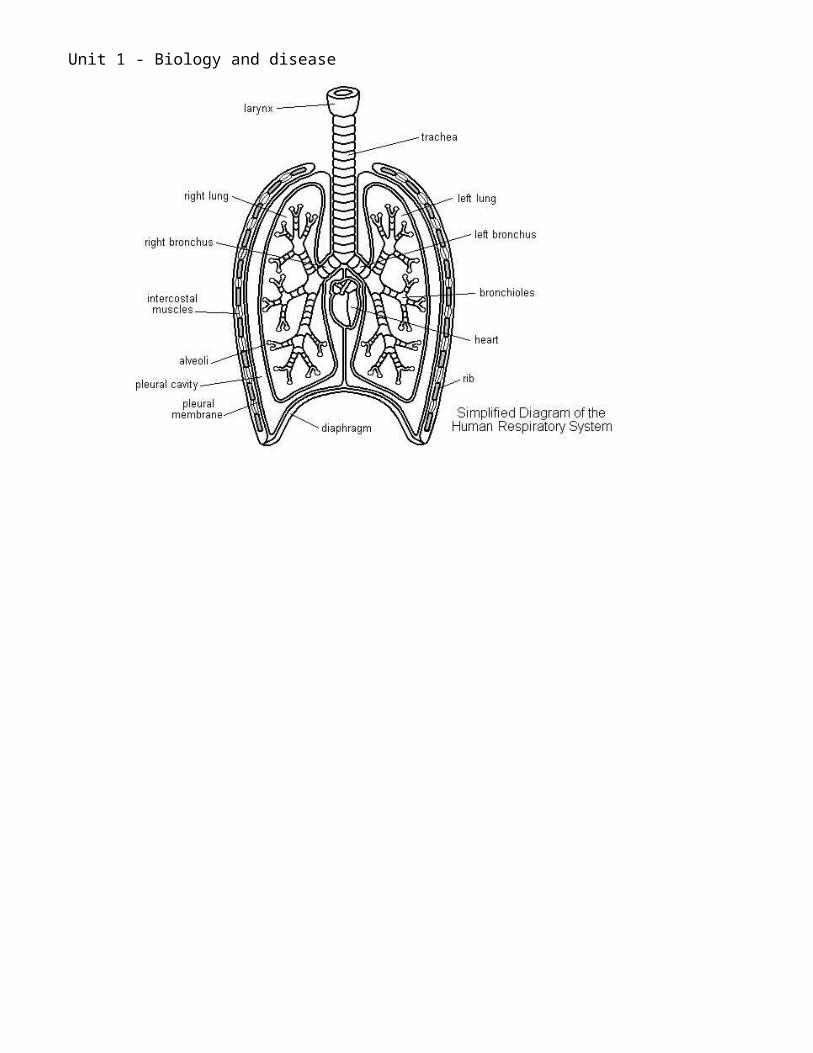
Structure of the thoraxLungs Site of gaseous exchange Located in thorax Require ventilation Left smaller than right – it overlaps the heart
Rib cage Bony case enclosing lungs and heart 12 pairs attached dorsally to vertebrae Top 10 pairs are attached ventrally to sternum, remaining ribs are ‘floating’
Muscles Intercostal muscles between ribs, responsible for movement External – contracts – ribs move up and out - inspiration Internal – contract – ribs move down and in - expiration Diaphragm – muscular sheet which separates thorax from abdomen
Pleural membranes 2 membranes that secrete pleural fluid. The fluid filled cavity is lower than atmospheric pressure. This prevents the lungs deflating.

Unit 1 - Biology and disease
Air ways
Trachea Rings of cartilage prevent tube collapsing when internal pressure drops. Lined with ciliated epithelium.
Bronchi Trachea divides into 2 bronchi. These tubes enter each lung Supported by cartilage
Bronchioles Branch throughout each lung. Support from cartilage gradually decreases
Alveoli Spherical sacs Major site of gas exchange 100μm in diameter Lined with flattened epithelial cells (approx 300 million) Makes a vast area for exchange (40-60m2)
Unit 1 - Biology and disease
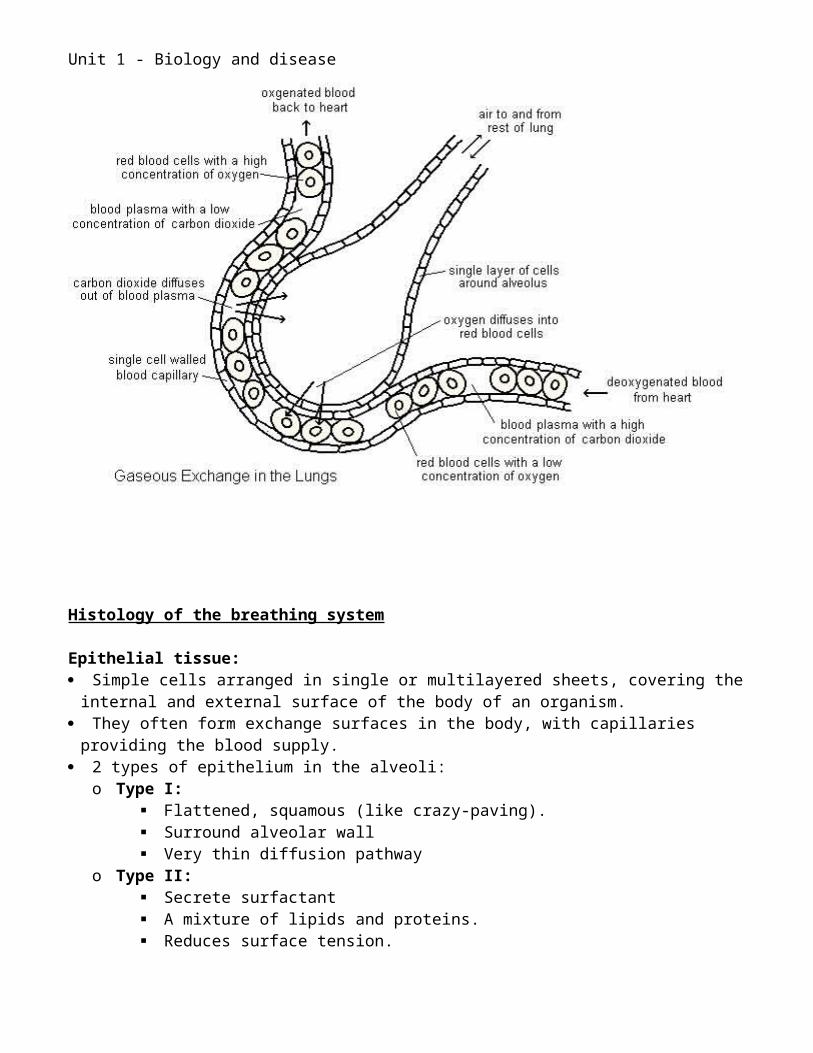
Histology of the breathing system
Epithelial tissue: Simple cells arranged in single or multilayered sheets, covering the internal and external
surface of the body of an organism. They often form exchange surfaces in the body, with capillaries providing the blood supply. 2 types of epithelium in the alveoli:
o Type I: Flattened, squamous (like crazy-paving). Surround alveolar wall Very thin diffusion pathway
o Type II: Secrete surfactant A mixture of lipids and proteins. Reduces surface tension. Prevents alveoli collapsing and provides elastic recoil for lungs
Connective tissue Supporting layer beneath epithelium. Made of fine fibres – collagen and elastin
Blood vessels Capillary walls are made of endothelial cells. Flattened cells forming a narrow tube with a common basement membrane. Pores (fenestrations) between cells enable exchange. Extremely narrow, so red blood cells squeeze through. Slows down passage allowing more time for diffusion. Increase surface area of cell in contact with endothelium Network of capillaries from pulmonary artery. Unite to form pulmonary vein.
Unit 1 - Biology and disease
Gas Exchange Gases are exchanged due to concentration gradients. Oxygen diffused into blood from alveolar air. Carbon dioxide diffuses into alveolar air from blood.
Gas Percentage VolumeInspired air Expired air
Oxygen 20.90 15.3Carbon dioxide 0.03 3.6Nitrogen 78.60 74.9Water Vapour 0.47 6.2
Fick’s law:
Rate of diffusion is proportional to: surface area X difference in concentration Thickness of surface
Surface area:o Large due to alveoli.o Many small spherical sacs.
Concentration gradients maintained through:o Pulmonary ventilationo Circulation of the blood.
Thickness of surface:o Single layer of squamous epitheliumo SIngle layer of endothelium
Unit 1 - Biology and disease
Pulmonary ventilation – Breathing Air movements occur due to pressure difference between atmosphere and alveolar air If intrapulmonary pressure > atmospheric pressure = Expiration If atmospheric pressure > intrapulmonary pressure = Inspiration
Pressure differences are achieved in the thoracic cavity Through the action of the intercostals muscles and positioning of the diaphragm. A pleural sac surrounds each lung. The outer membrane is attached to the rib cage, the inner to the lungs. The inner cavity is at a pressure below atmospheric pressure. This prevents the lungs deflating. When the thorax moves, the lungs do too. Alveoli are elastic and collapse if not held stretched by the thorax. The secrete surfactant which prevents them sticking together.
Mechanism of inspiration
Contraction of diaphragm Contraction of external intercostal muscles
Flattens and descends Pulls ribs upwards and Outwards
Thorax cavity lengthens Diameter of thorax increases
Increase in thorax volume
Lungs expand
Alveolar pressure drops
Pressure gradient establishedFrom atmosphere to alveoli
INSPIRATION
Unit 1 - Biology and disease
Mechanism of expiration
Relaxation of diaphragm Contraction of internalIntercostal muscles
Returns to domed position Ribs move downwardsAnd inwards
Thorax cavity shortens Diameter of thorax Decreases
Decrease in thorax volume
Elastic recoil of lungs
Lungs decrease in size
Increase in intrapulmonary pressure
Pressure gradient established fromAlveoli to atmosphere
EXPIRATION
Forced inspiration/expiration Abdominal muscles used This greatly increases intrapulmonary pressure Eg. coughing or blowing up balloon.
Unit 1 - Biology and disease
Measurements of pulmonary ventilation
SpirometerMeasures volumes of air expired and inspiredUsed to diagnose ventilation deficienciesCreates a spirogram
Tidal volume (TV): Volume of air breathed in or out during quiet breathing About 500cm3 in adults
Breathing rate = the number of inspiration/expiration cycles per minute
Pulmonary ventilation = tidal volume X breathing rate ie the volume of air breathed in or out per minute during quiet breathing.
The biological basis of lung disease
P ulmonary tuberculosis
Tuberculosis (TB) is an infectious disease It is caused by the bacterium Mycobacterium tuberculosis. TB most commonly affects the lungs but also can involve almost any organ of the body. Today TB usually can be treated successfully with antibiotics.
Transmission Someone who has a TB lung infection coughs, sneezes, shouts, or spits. People who are nearby can then possibly breathe the bacteria into their lungs. A person can become infected with TB when minute particles of infected sputum are inhaled
from the air. You don't get TB by just touching the clothes or shaking the hands of someone who is
infected. Tuberculosis is transmitted primarily from person to person by breathing infected air during
close contact. There is a form of atypical tuberculosis, however, that is transmitted by drinking
unpasteurized milk.
Course of infection When the inhaled tuberculosis bacteria enter the lungs, they multiply. This causes a local lung infection (pneumonia). The local lymph nodes associated with the lungs may also become involved with the
infection and usually become enlarged. In addition, TB can spread to other parts of the body. The body's immune (defense) system, however, can fight off the infection and stop the
bacteria from spreading. The immune system does so ultimately by forming scar tissue around the TB bacteria and
isolating it from the rest of the body. If the body is able to form scar tissue around the TB bacteria, then the infection is contained
in an inactive state.
Unit 1 - Biology and disease
Such an individual typically has no symptoms and cannot spread TB to other people. The scar tissue and lymph nodes may eventually harden, like stone, due to the process of
calcification of the scars (deposition of calcium from the bloodstream in the scar tissue). These scars often appear on x-rays and imaging studies like round marbles and are referred
to as a granuloma. Sometimes, however, the body's immune system becomes weakened, and the TB bacteria
break through the scar tissue and can cause active disease, referred to as secondary TB. TB can spread to other locations in the body:
o The kidneys, bone, and lining of the brain and spinal cord (meninges).
Symptoms TB infection usually occurs initially in the upper part of the lungs. The usual symptoms that occur with an active TB infection are;
o General tiredness or weaknesso Weight loss, o Fever, and night sweats.
If the infection in the lung worsens, then further symptoms can include:o Coughingo Chest paino Coughing up of sputum (material from the lungs) and/or bloodo Shortness of breath.
If the infection spreads beyond the lungs, the symptoms will depend upon the organs involved.
Pulmonary Fibrosis Pulmonary Fibrosis involves scarring of the lung. Gradually, the air sacs of the lungs become replaced by fibrotic tissue. When the scar forms, the tissue becomes thicker. Diffusion distances are increased. This causes an irreversible loss of the tissues for efficient gaseous exchange.
Symptoms Shortness of breath, particularly with exertion Chronic dry, hacking cough Fatigue and weakness Discomfort in the chest Loss of appetite Rapid weight loss
Causes It could be an autoimmune disorder, and there may genetic predisposition. The fibrotic process is a reaction to microscopic injury to the lung. Macrophages accumulate in connective tissue. They stimulate the creation of fibrous tissue. Associations have been made with the following:
Inhaled environmental and occupational pollutants Cigarette smoking Diseases such as Scleroderma, Rheumatoid Arthritis, Lupus and Sarcoidosis
Unit 1 - Biology and disease
The after effects of a viral infection Certain medications Therapeutic radiation
Asthma Asthma causes the bronchi to become inflamed and swollen. Bronchi are more sensitive than normal. It could be inherited. It could also be caused due to a lack of exposure to certain substances in early childhood.
Triggers: Certain substances, or triggers, can irritate them:
o House dust miteso Animal furo Polleno Tobacco smokeo Cold airo Chest infections.
Symptoms: When the bronchi are irritated, they become narrow and the muscles around them tighten. This can increase the production of sticky mucus. This causes wheezing and coughing and shortness of breath. Pulmonary ventilation is reduced. This effects the maintenance of efficient concentration gradients in the alveoli. This results in inefficient gas exchange. The severity of the symptoms of asthma differs from person to person, from mild to severe. The narrowing of the airways is usually reversible - occurring naturally, or through the use of
medicines. A severe asthma attack can be life threatening and may require hospital treatment.
Emphysema Emphysema causes the walls of the alveoli to break down. Larger air spaces are formed. Total surface area available for gas exchange is greatly reduced.
Causes: The single most common cause of emphysema is smoking. Heavy cigarette smokers are most at risk from emphysema and chronic bronchitis. The damage to your airway begins when tobacco smoke temporarily paralyses the cilia that
line the bronchial tubes. These hairs usually sweep irritants and pathogens out of the airways, The temporary paralysis prevents them from doing this. The irritants remain in your bronchial tubes and pass into your alveoli This inflames the tissue and damaging the walls. Breathing in industrial pollutants can also contribute to the development of emphysema. In a few, rare cases (about 2%) emphysema is the result of defective genes. This type is called alpha antitrypsin (AAT) deficiency emphysema.
Unit 1 - Biology and disease
AAT is a protein that blocks the action of an enzyme that breaks down the walls of the alveoli.
If you are deficient in the protein, it can lead to progressive damage that will eventually result in emphysema.
Symptoms Shortness of breath when exerting yourself. Eventually, this shortness of breath may occur even when you are at rest. Difficulty breathing Coughing Wheezing Excess mucus production A bluish tint to the skin (cyanosis)
Unit 1 - Biology and disease
The Heart
Position Middle of thorax Above diaphragm Behind sternum Between 2 lungs Partially overlapped by left lung Apex points towards left of thorax.
Cardiac muscle Major tissue in the heart wall is cardiac muscle Cardiac muscle tissue = myocardium Branching cells which can share nuclei Cells are cross striated like skeletal muscle. Transmit electrical excitation Capable of contracting and relaxing repeatedly for life.
Blood supply Provided by coronary artery Delivers oxygenated blood to the heart muscle Branches from aorta Receives 5% of total cardiac output Dense capillary network Coronary veins return blood to heart directly into right atrium through coronary sinus.
Associated Blood Vessels
Unit 1 - Biology and disease
Vena Cavao Carries deoxygenated blood from body tissues into right atrium.
Pulmonary arteryo Carries deoxygenated blood from right ventricle to lungs
Pulmonary veino Carries oxygenated blood from lungs back to left atrium.
Aortao Carries oxygenated blood from left ventricle to respiring body tissues.
Internal structure Atria (sing. Atrium):
o Relax to receive blood from veins: Venae cavae into right atrium Pulmonary veins into left atrium.
o Thin walled o Elastico Contract to push blood into ventricles:
Rings of muscles surround veins at their point of entry Contract to close off veins. Prevents reflux of blood into veins.
Ventricles:o Myocardium thicker than atria.
Distance to ventricles is very small.o Myocardium of left ventricle 3 times thicker than right.
Creates higher blood pressure in systemic circulation:o Essential for efficient function of organs.o Allow for tissue fluid formation.
Lower blood pressure in pulmonary circulation:o Prevents rupture of delicate pulmonary arteries.
o Separated by septum.o Relax to receive blood from atria.o Contract to push blood through arteries:
Left ventricle into aorta. Right ventricle into pulmonary artery.
Valves Responsible for heart sounds. Ensure unidirectional flow of blood though heart. Atrioventricular valves:
o Between atria and ventricles.o Prevent blood flowing back into atria when ventricles contract.o Higher pressure in ventricles causes them to close back towards atria.o Causes ‘lub sound’.o Chordae tendinae:
Fibrous cords
Unit 1 - Biology and disease
Attach loose edge of valves to wall of ventricle.o Attached by papillary muscle:
Contract when ventricle contracts. Tighten the chordae tendinae.
o Tricuspid valve: 3 flaps. Right side of heart.
o Bicuspid valve (mitral valve): 2 flaps. Left side of heart.
Pocket/semilunar valves:o At entrance of aorta and pulmonary artery.o Hence aortic and pulmonary valves.o Prevent back flow of blood into ventricles.o When ventricles relaxo Pressure in ventricle drops below pressure in arteries.o Causes valves to fill with blood.o Creates ‘dub’ sound
The Cardiac Cycle A rhythmic series of events. Resulting in each beat of the heart. At rest, average 72 beats per minute. One cardiac cycle = approx 0.83 secs.
Diastole:o Relaxation of atria and ventricles.o Atria fill with blood from veins.o Pocket valves close – dub.o Blood starts to move into ventricles.
Atrial systole:o Atria contract.o Increases pressure.o Pushes blood into ventricles.o Passes though atrioventricular valves.o Ventricles remain relaxed.
Ventricular systole:o Ventricles contract.o Atria relax.o Higher pressure in ventricles than atria.o Atriventricular valves close – lub.o Pocket valves open.o Blood flows into arteries.
Pressure Changes During the Cardiac Cycle. Blood always flows from a high pressure to a lower pressure, unless prevented by
valves.
Unit 1 - Biology and disease
Graph starts at atrial systoleo Point at which atrial pressure rises above 0 kPa
Ventricular systole occurs when pressure in ventricles exceeds pressure in atria.o A.V. valves close.o Causes increase in pressure in atria.
Blood flows into arteries when pressure in ventricles exceeds pressure in arteries.o Pocket valves open.
Diastole occurs when pressure in ventricles drops below pressure in arteries.o Pocket valves close.o Pressure in arteries maintained relatively high.o Due to elastic recoil of artery walls.
Atrioventricular valves open when pressure in ventricles drops below pressure in atria.o Pressure in atria rises back towards 0 kPa as they fill with blood.
Extra detail: Electrocardiogram (ECG)
Electrodes placed on skin. Changes in voltage displayed on oscilloscope:

Unit 1 - Biology and disease
o P wave = electrical excitation of atriao QRS complex = excitation of ventricles.o T wave = recovery (repolarisation) of ventricles.
Phonocardiogram (PCG): Records heart sounds. Caused by valves closing. Lub dub.
Conducting tissues of the Heart The heart beat is initiated from within the heart muscle. Heart muscle is myogenic:
o It is self exciting.o It can contract on its own without needing nerve impulses.
It maintains a continuous, inherent rhythm through electrical excitation of localised areas. This leads to contraction of cardiac muscle. This is called myogenic stimulation. Modified cardiac muscle cells coordinate this sequence of events. They conduct the excitation through the walls of the heart.
Sino Atrial Node (SAN): Small group of specialised cells. In wall of right atrium. Near opening of superior vena cava. Referred to as the ‘pacemaker’. Initiates the heart beat. Electrical excitation passes across both atria causing them to contract.
Atrio Ventricular Node (AVN): Small group of specialised cells. Between the 2 atria. Electrical activity reaches the AVN Delays passage of excitation down the septum
Unit 1 - Biology and disease
This enables the atria to empty before ventricles contract Passes electrical excitation down septum.
Bundle of His: Specialised non-contractile cardiac muscle fibres (Purkinje fibres) Lead down the interventricular septum to apex. Electrical excitation passes down this. They radiate upwards from the apex around the ventricle walls. Excitation passes up through these. Ventricle contracts from apex upwards.
Cardiac output Normal heart rate = approx 72 beats per minute. Varies from 50 to 200 beats per minute. Approximately 75 cm3 of blood pumped from each ventricle. Cardiac output is the volume of blood pumped by one ventricle of the heart in one minute Cardiac output = heart rate X stroke volume. Measured in dm3min-1
Heart Disease
Atheroma An accumulation and swelling in artery walls that is made up of cells that contain lipids and
fibrous connective tissue. Also referred to as plaques. The swelling occurs between the endothelium lining and the smooth muscle wall of the
artery They occur due to macrophages that have taken up low-density lipoprotein (LDL). This is associated with high cholesterol levels. This is associated with high levels of saturated fats in the diet. The plaque calcifies and hardens over time.
Aneurysm Atheroma can cause weakening of the arterial wall. Can be due to atheroma. This can lead to a localized, blood-filled dilation (balloon-like bulge) of a blood vessel. Aneurysms most commonly occur in:
o Arteries at the base of the brain – causing a strokeo Aorta.
The bulge in a blood vessel can burst. This results in haemorrhage. The larger an aneurysm becomes, the more likely it is to burst.
Thrombosis Thrombosis occurs if a plaque breaks through the endothelium. It develop a rough surface. This causes the formation of a clot or thrombus inside a blood vessel. This obstructs the flow of blood through the circulatory system. It can be dislodged, being carried down into smaller arteries, blocking blood flow.

Unit 1 - Biology and disease
The tissue affected is starved of essential nutrients and oxygen. When thrombosis affects important arteries it can be fatal or cause serious illness:
o In the coronary arteries it may cause a heart attack – myocardial infarctiono In the brain with blood it may cause a stroke.
Coronary Heart Disease Coronary heart disease (CHD) occurs due to the accumulation of plaques within the walls of
the coronary arteries. These supply the myocardium (the muscle of the heart) with oxygen and nutrients. Most individuals with CHD show no evidence of disease for decades as the disease
progresses. Gradually, blood flow to the heart muscle reduces. This puts extra strain on the heart. Myocardial infarction Myocardial infarction is commonly known as a heart attack. Occurs when a dislodged thrombosis enters a coronary artery, or one of its branches. The blood supply to a part of the heart is interrupted. The resulting ischemia or oxygen shortage, if left untreated for a sufficient period, can
cause damage and/or death of heart tissue. It is the leading cause of death for both men and women all over the world. Infarction = tissue death due to oxygen starvation. It can be the cause of cardiac arrest, which is the stopping of the heartbeat. Severe myocardial infarction may lead to heart failure, in which the pumping action of the
heart is impaired. Symptoms of acute myocardial infarction include;
o chest pain (typically radiating to the left arm or left side of the neck)o shortness of breatho nausea, vomitingo palpitations, sweating, and anxiety (often described as a sense of impending doom).
Risk factors Hereditary factors – can increase the risk of high cholesterol and high blood pressure. High cholesterol:
o Essential for cell membranes.o However, high levels can cause plaques.o Due to a high concentration of low-density lipoproteins in the blood.o This is linked to high levels of saturated fats in the diet.
High blood pressure.o Puts more stress on blood vessels.o Increases risk of aneurysms or thromboses.o Can also cause blood vessels to harden and thicken, reducing blood flowo Various risk factors:
Salt – can increase blood pressure Smoking:
Nicotine causes a narrowing of arteries, leading to high blood pressure. Carbon monoxide reduces how much oxygen is carried of haemoglobin. The heart works harder to supply the tissues with oxygen.
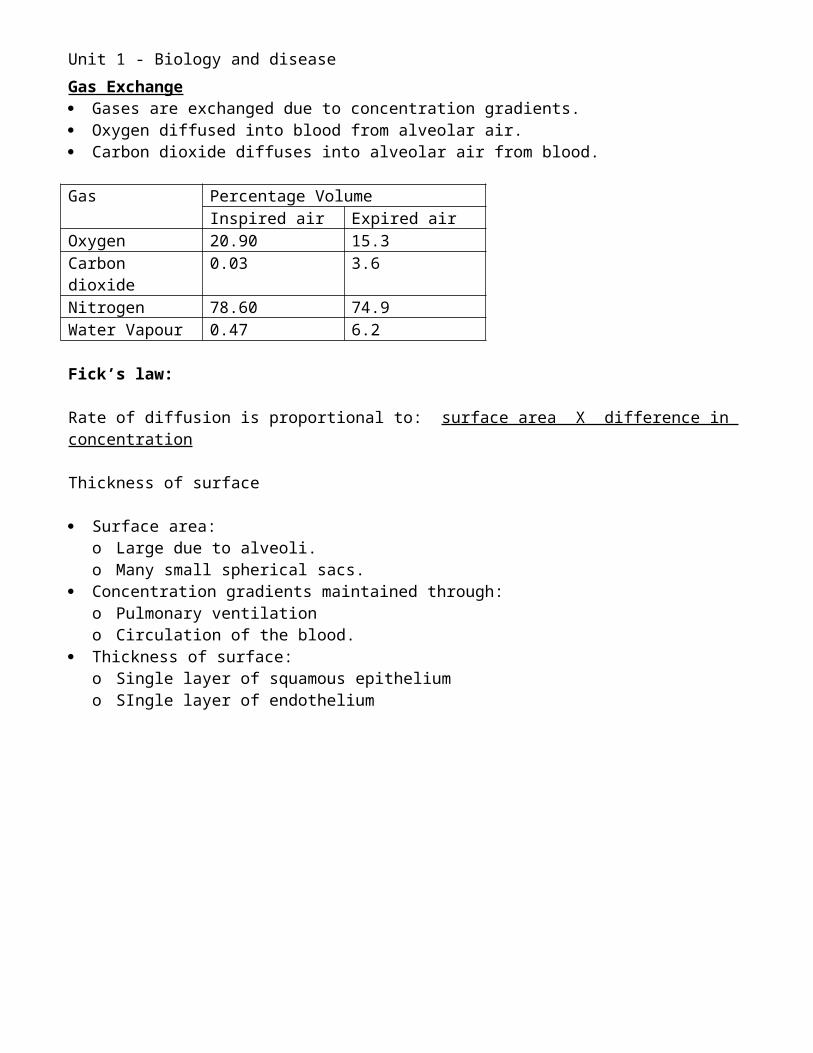
Unit 1 - Biology and disease
This also increases blood pressure. Stress
o To reduce the risk of heart disease: Increase intake of antioxidants eg vitamin C Increase fibre intake - cellulose
Age – Incidence increases in men over 60 and women over 65.
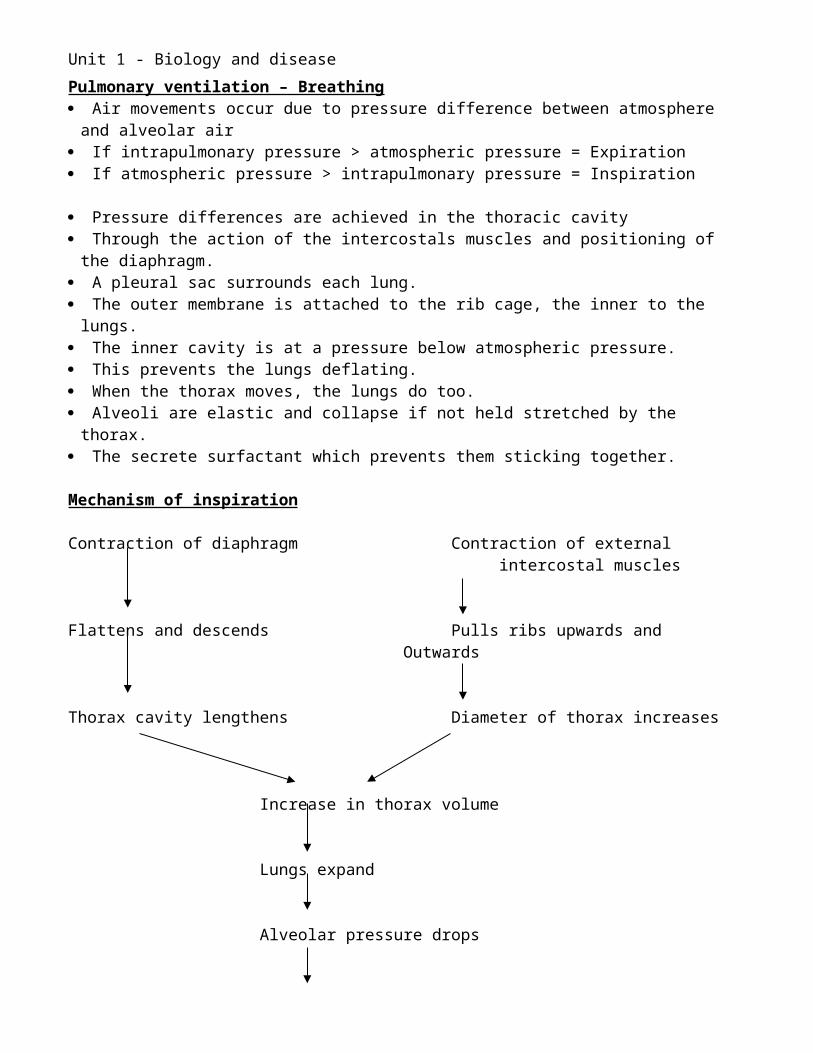
Unit 1 - Biology and disease
Immunology
Phagocytosis Process by which large particles are taken up by cells. Via plasma membrane derived vesicles. A form of endocytosis. 2 reasons for phagocytosis:
o To protect against pathogens. Prevents them spreading
To dispose of dead, dying or damaged cells. Process:
o Histamine released where tissue is damaged:o This attracts phagocyteso It causes dilation of blood capillaries.o Tissue fluid escapes into tissues.o Causes inflammation.o Phagocytes pass into tissue fluid.o Pathogens release chemicals.o Phagocyte moves towards the pathogen up the concentration gradient.o The pathogen attaches to the phagocyteo The phagocyte forms pseudopodia around the pathogen.o The edges of the pseudopodia meet and fuse.o This encloses the pathogen in a phagosome.o Lysosomes migrate towards the phagosome.o They fuse with the phagosome and release lytic enzymes inside it.o These enzymes break down the pathogen.o The products are absorbed by the pahgocyte.o If the phagocyte survives it may carry out more phagocytosis.o Pus = dead bacteria and phagocytes.
The Immune Response Antigens = specific chemicals on the cell surface membrane of foreign cells (non-self). They are characterisitic of the individual. They may be:
o Proteinso Polysaccharideso Glycoproteinso Glycolipids
Eg red blood cells have isohaemaglutinnogen A or B, or both or neither. Foreign cells have foreign markers – antigens. Recognised as foreign by leucocytes.
o On cell surface of a microorganism.o On the surface of a virus.o On the cell surface of a tissue or organ transplant.
Provoke an immune response.
The role of Antigen presenting cells (APCs):
Unit 1 - Biology and disease
Macrophages ingest bacteria/viruses. Display bacterial antigens on membranes. ‘Antigen presentation’. Attach to specific T and B cells in lymph nodes.
Lymphocytes 2 main groups:
o T cells: Mature in the thymus Cause a cellular response to infection.
o B cells: Mature in the bone marrow. Cause a humoral response to infection. They release antibodies.
Specificity:o Each T and B cell is able to react with one antigen. o There are receptor sites on the surface membrane.o These provide the specificity in antigen binding. o Antigens of the body's own cells are excluded.o Capable of differentiating between 'self' and 'non-self'.o Only react against the 'non-self' molecules. – foreign antigens.
Production of lymphocytes Originally derive from stem cells of the bone marrow. Pass to the lymph glands in the chest, where:
o They multiply. o They are processed and activated. o Occurs largely during foetal life and early childhood.o They are tested for their ability to recognise and bond to antigens.o By APCs.o If they bond the T and B cells are killed.o Those that survive will recognize foreign antigens.
There is theoretically a pair of T and B cells for each potential foreign antigen.
Specificity: Each T-cells is able to react with one antigen. Receptor sites sit on the surface membrane. Provide the specificity in antigen binding. Antigens of the body's own cells are excluded. Capable of recognising 'self' and 'non-self'. Only react against the 'non-self' molecules.
Cellular Immune Response by T cells T cells are approached by APCs – clonal selection Specific T cell responds. T cells will only respond to antigens presented in this way. Form clones by mitosis – clonal expansion Various types of T cells are produced.
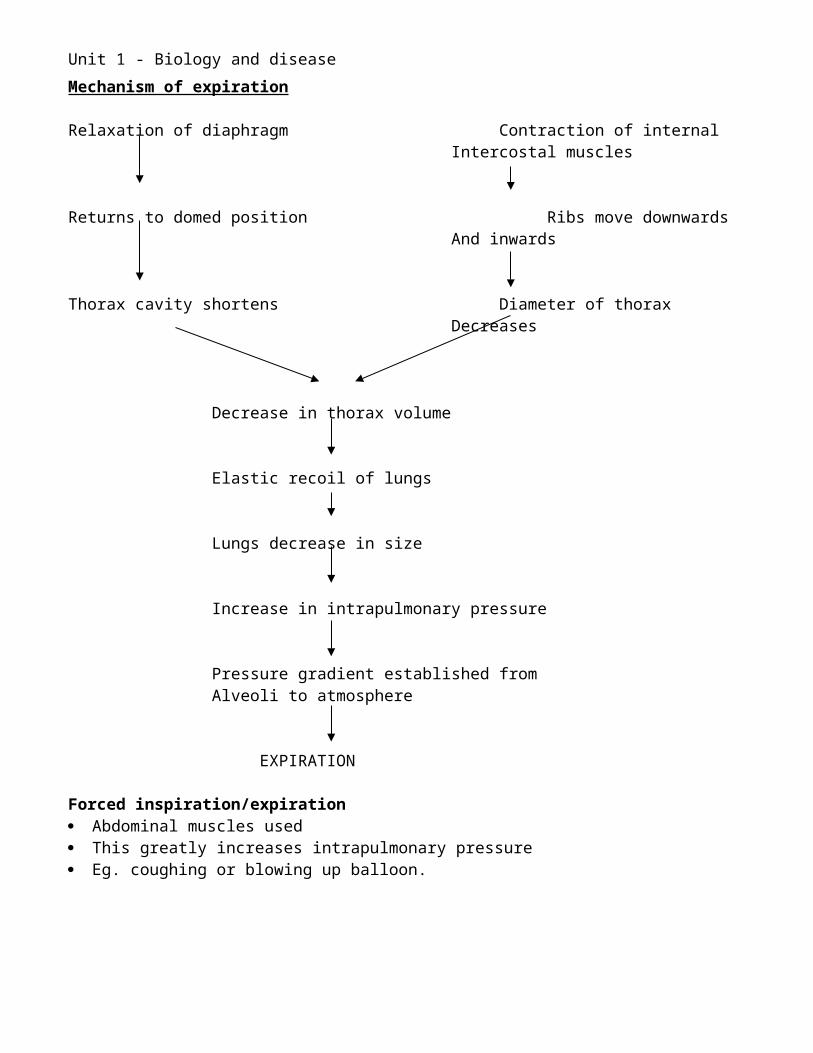
Unit 1 - Biology and disease
Helper T-cellso (These are the type of cell attacked by HIV.)o Secretes small proteins called cytokines.o Activate Killer T cells to multiply.o Stimulate APC to destroy itself.o Activate B cells to respond to antigens.
Killer T-cells o Destroy infected cells.o Release protein that instructs the cell to destroy itself.o Open protein pores in membrane.o Affect permeability of cell.o Cell bursts.o This prevents viruses replicating inside the cell.o Reduces chances of other cells being infected.
Memory T-cellso Remain in the body after the pathogens have been killed.o Enable rapid response to future infection.
Humoral immunity by B cells
Antibodies:o Proteins called immunoglobulins.o Produced by B cells,o Most Y-shaped.o 2 identical binding sites for its antigen.o One on either arm.o 4 polypeptide chains.o 2 identical heavy chains.o 2 identical and smaller light chainso Held together by disulphide bonds.
Unit 1 - Biology and disease
Process:o B cells have some of their specific antibodies attached to their cell membrane.o These act as specific receptors.o APCs attach to these on a specific B cell – clonal selection.o T cells release cytokines which cause the B cell to proliferates by mitosis – clonal expansion.o Forms millions of clones.o Release them into the circulation at the lymph nodes.o Some of the activated B-cells turn into memory cells.o Other clones are called plasma cells.o These produce specific antibodies.o 2000 per second.o Attach to specific antigens.o Form antibody-antigen complexes.
The role of antibodies:o Agglutination of antigens.o Precipitation of soluble toxins.o Stimulation of phagocytosis.o Prevent pathogenic bacteria attaching to cell membranes.
Immunological Memory o Initial immunological response to infection = primary response.o After recovering from an infection:
o The concentration of antibodies against the infectious agent gradually declines.o May take weeks, months, or even years. o Eventually, no antibodies can be detected. o However, the person is still immune.
o A second exposure usually brings about a more rapid and larger response to the antigen. o This is called the secondary response.
The main features of the secondary antibody response:
Unit 1 - Biology and disease
o The response is specifico Due to memory cells:
o T cells and B cells.o Created during the formation of clones.o Some of the progeny cells revert to small lymphocytes.o Multiply rapidly next time the antigen enters the body. o The secondary reponse is therefore much larger and much faster than the primary
reponse.o The person is immune.
o Memory cells must have long life spans.o Provide long-lasting immunity.o In fact, there is evidence in humans that some small lymphocytes survive at least 20 years.
Antigenic variability: Eg Influenza virus
Characteristics of Influenzao Influenza is a virus.o Single-stranded RNA genome.o 8 separate RNA strands. o The genome is enclosed within a lipoprotein envelope. o Also contains enzyme RNA polymerase.
Unit 1 - Biology and disease
Infection: The reservoir is acute infection in other human beings. Spread is rapid via aerial droplets through sneezing. Inhalation into the respiratory tract. Host cells are epithelial cells of bronchi and bronchioles Its antigens attache to the receptors on outside of the host cell. Taken into the cell by endocytosis. Viral RNA is released into the cell cytoplasm.
Cause of disease: The virus takes over the cell's productivity. Toxins are released. This destroys the epithelial cells.
Why is influenza difficult to treat?o Antibiotics do not cure viruses.o Can be used on secondary infections.o Its antigens change frequently due to mutations.o Also, the 8 separate RNA strands.
o Increase the potential for recombinants to form.o Gene segments may interchange if two different viruses infect the same cell.o This may contribute to the rapid development of new flu strains.o Avian and pig strains allow more reservoirs for recombination.
o There is great antigenic variability.o This increases the chance of a virus displaying new antigens to infect the host.o Memory cells do not exist, so a primary immune response is required.
Unit 1 - Biology and disease
VACCINATION
Passive immunity Introduction of antibodies from outside the body Natural – breast milk Artificial - when disease is likely to result in death before immunity is developed Eg rabies (virus) and tetanus (bacterium) Antibodies are produced by other mammals & serum is injected
Active immunity Production of antibodies by individual’s immune system Natural – response to infection Artificial – introduction of vaccines into the body
Vaccines Vaccines contain antigens. Derived from pathogens. Protect against infection by that organism. Without suffering illness. Important that vaccine does not trigger symptoms of the disease.
Killed virulent organisms Eg cholera bacterium Killed using chemicals.
Live non-virulent strains Eg rubella virus.
o German measles.o Mild rash and fever.
Production:o Virulence is greatly reduced by :
Growing at high or low temperatures or without oxygen or with certain chemicals
Or, encourage mutations by repeated sub culturing. Produces same antigens. Lacks virulence.
Isolated antigens from a pathogen Eg influenza virus Production:
o Laboratory procedure.o Removal of antigens from pathogen.o No occasional rogue micro organisms.
Administration:o Injection into:
Elderly Medical staff. People with respiratory disorders.
Unit 1 - Biology and disease
o Annual administration.o To provide immunity to current strains.
Development of new vaccineso New vaccines are created through laboratory research.o Quite often this is by profit making organisations.o Papers are published.o Methodology needs to be critically assessed by other scientists.o Different scientists have different opinions.o Opinions may be biased due to:
o Whom the scientists work for.o Scientists current views and beliefs.
o Accepting new scientific developments takes time.o Once accepted, rigorous testing is necessary before a licence is granted for its production
and use.
A new vaccine must:o Be safe and effective.o Have few side effects:
o Most vaccines will have some side effects.o These can be acute in some cases.o This could discourage use if people do not consider the vaccination to be essential.
o Be economically viable – it must be possible to vaccinate all vulnerable individuals.o Have available methods of production, transport and storage need to be developed, eg is
refrigeration necessary?o Be accepted by the scientific community if it is to be administered.o Be accepted by the public.
Vaccination programmeso Vaccinations should be administered to the larges possible group of people at the same
time.o This is called ‘herd’ immunization.o Requires 985 to 90% of the population to be immunised.o This reduces the chance of the microorganism to find a suitable host.o People who have not successfully acquired immunity are therefore less likely to be exposed
to the pathogen.o Some of these people are likely to be more vulnerable than others, eg young, old and those
with compromised immune systems.
MMRo A triple vaccine for:
o Measles Can cause convulsions, disability or death.
o Mumps Can cause deafness, meningitis, sterility in males.
o Rubella If infection occurs during pregnancy, it can affect the fetus:
Unit 1 - Biology and disease
Deafness, blindness and other development problems.o Injection into infants:
o 2 administrations:o At 12 to 15 months:
Coincides with weaning from breastfeeding. Passive immunity from Mother declines
o At 3 to 5 years: Some individuals do not acquire immunity from the earlier vaccination
o I988 – vaccine introducedo 2000 - Dr Wakefiled published a report suggesting that MMR might caused autism.o Based on tests on 25 children.o The lawyers working for parents of children with autism funded his research.o Many parents opted not to have their children vaccinated.o Correlation noticed – autism emerged at around 14 months.o Further research on much larger samples (30,000 in Japan) has shown there was no link.o Parents had to assess the conflicting evidence, data and opinions.o In the mean time, children were not being immunized.o Some children have therefore been badly affected by these diseases.o They are not necessarily the children who were not immunized.
Ethics of vaccineso Development involves animal testing.o Trials are carried out on humans – who should be tested?o Vaccination programmes are expensive:
o How long should they run for?o If vaccination stops, could the disease re emerge?o Eg TB
o Side effects are greater in some people than others:o In some cases, long-term problems arise.o The incidence of this must be far lower than the chance of getting the disease.
o Vaccinations are not compulsory:o How should be encouraged to become immunized.o Could vaccination be enforced to prevent epidemics, eg bird flu?
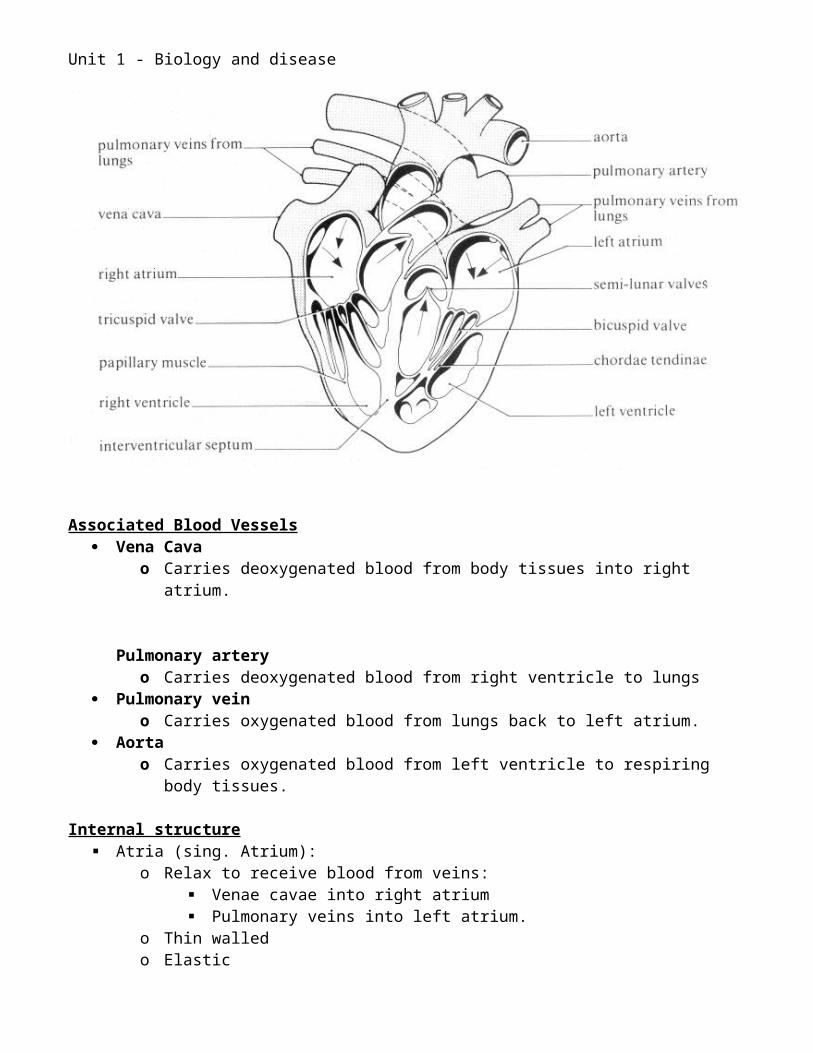
Unit 1 - Biology and disease
Monoclonal antibodies
The specificity of antibodies enables them to target other types of molecules found in the body, such as: o receptors or other proteins present on the surface of normal cells.o molecules present uniquely on the surface of cancer cells.
The response of the immune system to any pathogen is polyclonal. o Plasma cells manufacture antibodies of a great range of structures in response to the
many antigens present on a single pathogen. Monoclonal antibodies are antibodies of a single specificity that are all being synthesised by
clones of a single plasma cell that can be grown indefinitely.
Production of monoclonal antibodies It is difficult to grow plasma cells out of the body. They die out after a few generations because of the limited growth potential of all normal
somatic cells.
César Milstein and Georges Köhler 1975: Awarded a Nobel Prize 1984 Plasma can become cancerous. The unchecked proliferation of such a cell is called a myeloma. Köhler and Milstein found a way to combine myeloma cells with plasma cells. They fused myeloma cells with plasma cells from an immunized mouse. The technique is called somatic cell hybridization. The result is a hybridoma.
1. Immunise a mouse with the desired antigen.
Unit 1 - Biology and disease
2. Remove plasma cells from its spleen.3. Treat mice to encourage them to develop cancer tumours.4. Remove tumour cells from the spleen.5. Mix plasma cells with myeloma cells.6. Use detergent to facilitate fusion of adjacent plasma membranes. This creates some
hybridomas.7. Separate and then culture individual cells.8. Identify the cells that have been produced by successful fusions that have the desired
qualities: The ability to grow continually The ability to produce large amounts of pure antibody.
Problems with monoclonal therapy Mouse antibodies are recognised by the human immune system as foreign. The human patient mounts an immune response against them, producing HAMA ("human
anti-mouse antibodies"). These not only cause the therapeutic antibodies to be quickly eliminated from the host, but
also form immune complexes that cause damage to the kidneys. Monoclonal antibodies raised in humans would lessen the problem, but few people would
want to be immunized in an attempt to make them and most of the attempts that have been made have been unsuccessful.
Using genetic engineering it is possible to make mouse-human hybrid antibodies in an attempt to reduce the problem of HAMA – Chimeric or humanized antibodies.
Uses of monoclonal antibodies Cancer treatment:
o The monoclonal antibody is created that is specific to antigens on cancer cells.o It is attached to an enzyme that will activate a drug that will then only kill the cancer cells.
Diagnostic tests to detect small amounts of drugs, toxins or hormones, e.g. monoclonal antibodies to human chorionic gonadotropin (HCG) are used in pregnancy test kits
Diagnosis of AIDS by the ELISA test. Monoclonal antibodies can be used to treat viral diseases. There is some evidence to
suggest that antibodies may lead to a cure for AIDS. To classify strains of a single pathogen, e.g. Neisseria gonorrhoe.
Ethical issues They are potentially a major medical advance. Cancer and diabetes have been successfully treated. However, there have been some deaths associated with their use. Testing requires human volunteers. Production involves mice. Cancer is induced in mice. Transgenic mice are being developed to humanise the antibodies – human genes are put
into mice.


















