APTA, Kevin Hassett, September 24, 2002 1 APTA Passenger Information Systems.

1
Current evidence for the management of lower
extremity tendinopathies
American Physical Therapy Association Combined Sections Meeting 2015
Indianapolis, Indiana February 4-7, 2015
Disclosure
• The authors/presenters of this session declare that no relevant financial relationship exists
2
Course Objectives • Upon the completion of this session, the participant will be able to: • Identify current research explaining the pathophysiology for tendinopathy
development. • Recognize the findings from current research explaining the physiological
processes for tendon remodeling. • Describe various risk factors for the development of posterior tibialis tendinopathy. • Identify the best practices for examining a patient with posterior tibialis
tendinopathy. • Describe the findings from current literature regarding the management of
posterior tibialis tendinopathy. • Describe various risk factors for the development of triceps surae tendinopathy. • Identify the best practices for examining a patient with triceps surae tendinopathy. • Describe the findings from current literature regarding the management of triceps
surae tendinopathy. • Describe various risk factors for the development of patellar tendinopathy. • Identify the best practices for examining a patient with patellar tendinopathy. • Describe the findings from current literature regarding the management of patellar
tendinopathy. 3

2
Tendon: homeostasis, Degradation and remodeling
Craig R. Denegar, PT, PhD, ATC, FNATA University of Connecticut
Storrs, Connecticut
Purpose – review the role of mechanical signaling on tendon
homeostasis and the paradox of exercise as an effective
treatment for overuse disease • Tendon structure & homeostasis • Basics of mechanobiology • Tendon disease: etiology, progression and
histology • Repair mechanisms: Role of the tenocyte and
tendon progenitor cell 5
What maintains homeostasis and tendon health?
6

3
TENDON 7
Gap junctions are the specialized regions where cells connect via chemical / electrical signals
Cell to Cell interaction
8
Tenocyte
Compression Shear Tension
Mechanotransduction
Gene / Protein Expression Growth Factors
ECM Protein production
Matrix Remodeling Enzymes (MMPs)
remodeling / repair
Tendon Homeostasis
Healthy Tendon 9

4
Mechanobiology • Mechanically mediated signal transduction
(mechanotransduction) is involved in a myriad of physiologic processes such as: – touch and pain sensation, – hearing and vestibular function – blood pressure control – cell volume regulation – tissue growth and adaptation.
• Involves cellular / extracellular interaction
10
Mechanobiology
Mechanical Load
gene expression, protein translation, and
posttranslational modification
protein synthesis in the
ECM
11
ECM Production ECM Remodeling
12

5
What goes wrong? • Overload or Underload?
• Damage to extracellular collagen framework due to overload (and thus loss of signaling to the tenocyte), or fragility of the collagen composition or lack of activity induced mechanical stimulation lead to TENDINOPATHY!!
13
Tenocyte
Compression Shear Tension
Mechanotransduction
Gene / Protein Expression Growth Factors
Inadequate ECM protein production
Matrix Remodeling Enzymes (MMPs)
Pro-inflammatory Cytokines (IL-1, IL-6)
Tendinopathy
ECM protein degeneration
Overuse Catabolic Cascade
14
GFs: ECM Production
MMPs: ECM Remodeling
Relative Imbalance
15

6
Understanding tendon pathology & nomenclature
Tendonitis: inflammation, pain and swelling
Tendinopathy: description of clinical presentation
of tendon overuse
Tendinosis: degeneration of ECM in the absence of
active inflammatory cells.
16
Tendinopathy – a progressive disorder
• Reactive tendinopathy • Tendon disrepair (failed healing) • Degenerative tendinopathy
Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009; 43:409-16.
17
Fiber disorganization and increased proteoglycan content in degenerated
tendon
18

7
Tendon: “Challenged Healing” • Tendon is characterized as having
limited vascularity
• Greater autocrine / paracrine influence
on homeostasis and thus repair
• Cellular crisis
– Tenocyte & tendon progenitor cells 19
A Note on Epidemiology – loading is not the only factor
• Tendinopathy is associated with activity and overuse
• Obesity however increases risk of lower AND upper extremity tendinopathy
20
Link with obesity and insulin insensitivity
• Prevalence of tendinopathy and low grade systemic inflammation in obese patients with decreased insulin sensitivity – Systemic low grade inflammatory state due to
release of adipokines TNF-α, IL-6.
• Macrophages and other inflammatory cells surround fat cells. Free glucose molecules attach to collagen, impair crosslinking.
• Less mechanical signal transduction 21

8
Tendon repair – more than up-regulating tenocytes
22
If the tenocyte dies, what happens? Tendon Stem / Progenitor Cells (TSPCs)
• Recently Identified (2007) • Promote repair through:
• cellular proliferation → tenocyte differentiation → repair
• Promote Tendinopathy through: • Differentiation into fat, cartilage and bone cells
(adipocytes, chondrocytes, osteocytes) → failed repair → common histologic changes
23
Tendon stem cell niche
• Just as mature tenocyte relies on attachment
and surrounding extracellular matrix, the tendon
progenitor cell relies on it’s environment for
survival and activation / differentiation
24
9
Evidence suggests mechanical loading regulates stem cell proliferation &
differentiation • Tendon Stem / progenitor Cells (TSPCs) were
isolated from the patellar and Achilles tendons of 15 New Zealand white rabbits (female, 4–6 months, 3–4 kg).
• Cell culture dish containing microgrooves and coated with ProNectin-F (promotes cell attachment)
• 4% & 8% stretch vs control (no stretch) at 0.5Hz for 12h
25
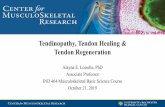
Evidence suggests mechanical loading regulates stem cell proliferation & differentiation
Cell proliferation measured 3days post
↑ 18% ↑ 36% ↑ 77% ↑ 193%
Patella Tendon (PTSC)
Achilles Tendon (ATSC)
26
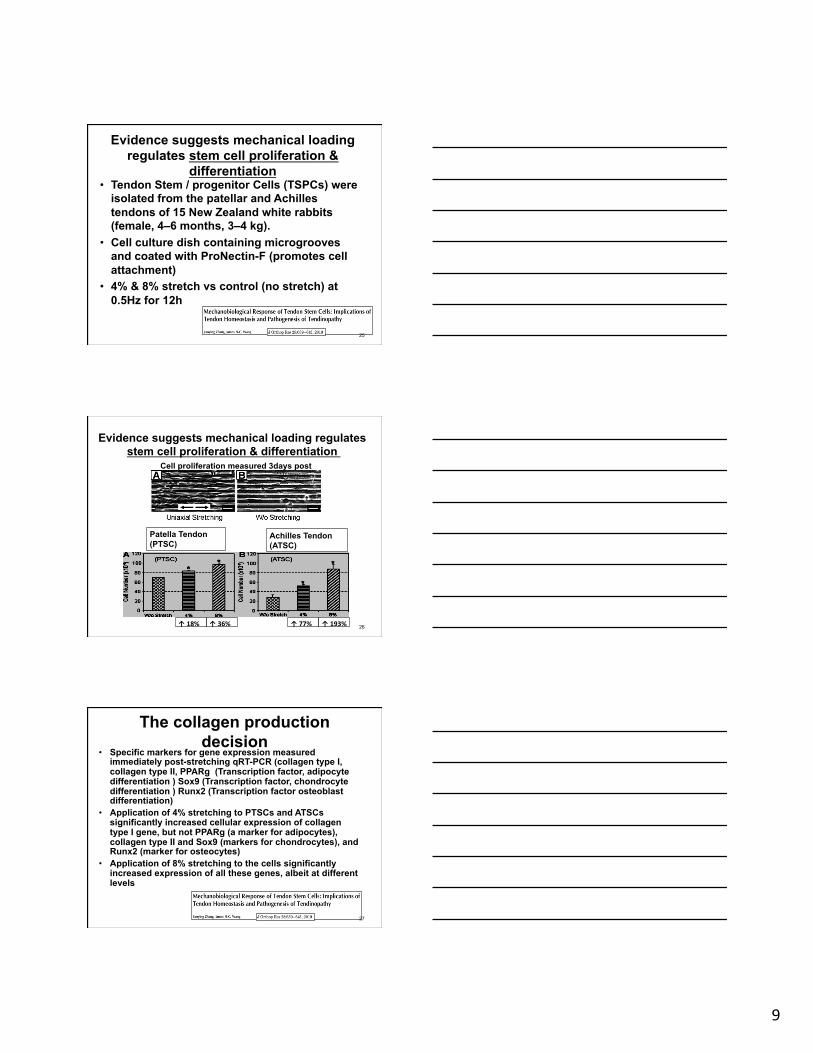
The collagen production decision
• Specific markers for gene expression measured immediately post-stretching qRT-PCR (collagen type I, collagen type II, PPARg (Transcription factor, adipocyte differentiation ) Sox9 (Transcription factor, chondrocyte differentiation ) Runx2 (Transcription factor osteoblast differentiation)
• Application of 4% stretching to PTSCs and ATSCs significantly increased cellular expression of collagen type I gene, but not PPARg (a marker for adipocytes), collagen type II and Sox9 (markers for chondrocytes), and Runx2 (marker for osteocytes)
• Application of 8% stretching to the cells significantly increased expression of all these genes, albeit at different levels
27
10
Cell differentiation with 4% and 8%
28
Considerations • Data from animal modeling
• Stretching loads do not equate to human in-vivo
loading
• Data suggest the different tendons may have
unique responses
29
But clinical evidence for effective treatment through exercise
exists
30

11
Before closing – a note on phoresis
• Does the phoresis (phono or ionto) effect treatment outcome?
• Research offer a mixed message • Study at the cell level tells an important
story
• The effects of dexamethasone on human patellar tendon stem cells: implications for dexamethasone treatment of tendon injury. Zhang J, Keenan C, Wang JH, J Orthop Res. 2013;31:105-10.
31
Effect of Dexamethasone on Tendon Progenitor Cells
Collagen I
Adipogenesis
Chondrogenesis 32
Summary • Mechanical load stimulates tendon cells through
integrin receptors and is essential to tendon health and tendon repair
• Tendinopathy is characterized by disorganized collagen, increased proteoglycan and often fat and bony accumulation
• Progenitor cell differentiation is an important consideration in understanding repair (not just a function of fibroblasts)
33
12
Posterior Tibialis Tendinopathy
Gary Wilkerson, EdD, ATC University of Tennessee at Chattanooga
Combined Sections Meeting 2015
Indianapolis, IN February 4-7, 2015
Disclosures
• No relevant financial relationship exists that could be viewed as a conflict of interest
35
Learning Objectives
• Upon the completion of this session, the participant will be able to: 1. Describe various risk factors for the development
of posterior tibialis tendinopathy. 2. Identify the best practices for examining a patient
with posterior tibialis tendinopathy. 3. Describe the findings from current literature
regarding the management of posterior tibialis tendinopathy.
4. Relate the possible role of posterior tibialis dysfunction in the development of chronic ankle instability
36

13
Role of Posterior Tibialis Muscle
37
1
2
Up to 10X BW
37 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Tendon • Primary insertion on navicular tuberosity • Dynamic stabilizer of medial longitudinal arch
– Subjected to great mechanical stress • Eccentric action: Heel strike to mid-stance
– Deceleration of pronation • Concentric action: Mid-stance to push-off
– Supination of foot (increased rigidity)
• Pathology – Tenosynovitis – Longitudinal tears – Complete rupture
38 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Tendon Dysfunction
• Early identification and treatment of PTTD critical
• 4 distinct stages of –
– Progressive weakening
– Tissue degeneration
– Structural deformity
39 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

14
Posterior Tibialis Tendon Dysfunction • Stage 1:
– PT weakness without rearfoot or forefoot deformity – Loss of strength may be progressive or sudden – Aching discomfort on medial aspect of ankle and
foot • Exacerbated by activity and relieved by rest
• Stage 2: – Some degree of rearfoot valgus and forefoot
abduction • Accentuated by increased axial loading • Manual repositioning into normal alignment possible
– Persistent discomfort; medial swelling may be evident
40 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Heel Elevation Test 41
41
NORMAL Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Tendon Dysfunction
• Stage 3: – Rigidity of both the rearfoot and forefoot – Osteoarthritic degeneration of subtalar joint – Development of lateral aching (bony impingement)
• Contact of calcaneus with fibular malleolus
• Stage 4: – Elongation of the deltoid ligament – Valgus displacement of talus within tibiofibular
mortise
42 Myerson, 1996
Property of G. Wilkerson, not to be distributed without permission 2/7/2015

15
Posterior Tibialis Tendinosis
43
Distraction of Joint Surfaces
(Tension)
SUBTALAR EVERSION
43 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Effect of Achilles Tendon Tightness
44 Biga ,2009
• Achilles Tendon tightness restricts tibia rotation over talus (reduced range of dorsiflexion)
• Anterior margin of tibia exerts downward force on talus that depresses MLA
• Tibia rotates over talus (dorsiflexion of talocrural joint) as body mass moves from posterior to anterior position during the stance phase of gait
44 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Medial vs. Lateral Pathology?
• Impaired ability to effectively control foot and ankle displacements: 1. Posterior tibialis tendon dysfunction
• Excessive Eversion (Pronation) 2. Lateral ankle sprain
• Excessive Inversion (Supination)
• Intricate “gear” and “strap” mechanisms transfer torque from the to the leg, and vice versa
45 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

16
Subtalar Inversion + External Leg Rotation
46
Axis for Frontal Plane Tilt of the Talus
Axis for Transverse Plane Internal Rotation of Talus
Functional Axis for Subtalar Joint Inversion
46 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Muscle Weakness
• May be a consequence of arthogenic inhibition
– Wilkerson et al, 1997 – Munn et al, 2003
• May be a predisposing factor for LAS – Baumhauer et al, 1995 – Willems et al, 2005
47 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Evertor/Invertor (E/I) Strength Ratio
Baumhauer JF, et al: A prospective study of ankle injury risk factors. Am J Sports Med. 1995;23(5):564-570. • 145 college-aged athletes tested at 30°/s
• 15 athletes subsequently sustained LAS
• Mean E/I peak torque ratio for uninjured = .80
• 67% of injured had E/I peak torque ratio >1.00
48
48 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

17
Evertor/Invertor (E/I) Strength Ratio
Wilkerson GB, Pinerola JJ, Caturano RW: Invertor vs. evertor peak torque and power deficiencies associated with lateral ankle ligament injury. J Orthop Sports Phys Ther. 1997;26(2):78-86.
– 15 acute & 15 chronic injured subjects – 30°/s Evertor to Invertor Peak Torque Ratio
– “Optimal” E/I @ 30°/s = .75 to .85
49
49
Test 1 Test 2 ACUTE 1.18 .81 CHRONIC .96 .83
* Test 1 to Test 2: 25 ±8 days
Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Supination at Heel-Lift/Push-Off
50
Internal Inversion Moment
External Inversion Moment
RIGHT FOOT
50 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Effect of Weightbearing on Injured Ankle Following Inversion Sprain?
• With chronic lateral ankle instability, progressive application of body weight to involved extremity: – Pronation of foot (medial longitudinal arch
depression)
– Internal rotation and anterior translation of talus • Caputo et al, 2009 • Omori et al, 2004 • Tochigi, 2003
51 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

18
Optimal Stimulus for Adaptation?
• Some combination of strain magnitude, frequency, rate, and duration appears to set lower and upper limits for catabolic and anabolic tenocyte functions – < 3% insufficient to induce tendon adaptation – > 8% likely to cause microscopic tendon degeneration
• 55% MVC 2.5-3% strain • 90% MVC 4.5-5% strain
• Major disadvantage of elastic band resistance: – Lack of a means to accurately quantify resistance
52 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Muscle Strengthening • ER of foot with heel elevated
– Elastic cord resistance – Evertor/Invertor co-contraction
• 3 X per week for 3 weeks; n=19 • ~ 40% isometric peak force increase
53
ROTEX Simply Stable
Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Posterior Tibialis Muscle Strengthening
54 54 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

19
Posterior Tibialis Muscle Weakness
• Prolonged duration of stance phase pronation • Talus will remain in an internally rotated position
– Heel begins to rise – Forefoot rapidly supinates – Leg externally rotates
• Tibia excursion over talus within transverse plane – Subluxation during every repetition of gait cycle – Intra-articular shear loading
• Hashimoto & Inokuchi, 1997
55 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Tibia-Talus-Calcaneus Alignment
56 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Dynamic Control of Rotary Displacements Within the Transverse Plane
• Strategies: 1. Eccentric strengthening of Post. Tibialis
2. Support for Medial Longitudinal Arch
3. Taping for subtalar joint stabilization
4. Core stabilization training
57 Property of G. Wilkerson, not to be distributed without permission 2/7/2015

20
Medial Longitudinal Arch – Pronation – Chippaux-Smirak Foot Width Index (FWI)
• FWI = Line B / Line A – Line A: Widest portion of anterior 1/3 of foot – Line B: Most narrow portion of middle 1/3 parallel to Line A
58
Low Medial Longitudinal Arch Arch Height FWI
High ≤ .29 Normal .30 - .39
Low ≥ .40
Mei-Dan et al, 2005 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Arthrogenic Muscle Inhibition
)
59 Property of G. Wilkerson, not to be distributed without permission 2/7/2015
Summary • Early identification and treatment of PTTD is
critical to prevent progressive degeneration
• Tendinosis may result from a combination of diminished muscle strength and joint instability
• The ankle is far more susceptible to arthritic degeneration than generally recognized
• Somewhat paradoxical concepts appear to provide a plausible explanation for the exceedingly high rate of chronic ankle instability
Property of G. Wilkerson, not to be distributed without permission 2/7/2015

21
Achilles Tendinopathy
R. Barry Dale, PT, PhD, OCS, SCS, ATC, CSCS Associate Professor
University of South Alabama Mobile, AL
Triceps Surae Anatomy
• Gastrocnemius – Medial head – Lateral head
• Soleus • Plantaris
– InserBon • Achilles tendon
– Mostly equal contribuBons from gastrocnemius and soleus
62
Achilles Tendon Anatomy
• Thickest and strongest in the body – Average length 15 cm (11-‐26 cm range) – Average width is 6.8 cm at origin, 1.8 cm at midsecBon
– Rounded width of 3.4 cm at inserBon
63

22
Achilles Tendon Anatomy
• Three main vascular areas – Proximal (posterior Bbial artery) – MidsecBon (peroneal artery) – Distal (posterior Bbial artery) – Mid-substance of tendon
• Poor blood supply • Increased injury incidence?
64
Achilles Tendon Disorders
• Mid-‐porBon tendinopathy • Paratendinopathy • InserBonal tendinopathy • Rupture
65
Achilles Tendon Disorders
• Prevalence of Tendinopathy – AthleBc vs. non-‐AthleBc populaBon
• ~30% do not engage in phys. act. (Ames et al. 2008)
– Adolescent populaBon • 1.8% for Achilles; 5.8% for patellar (Cassel et al. 2014) • 12-‐18% for gymnasts (Emerson et al. 2010)
66

23
Achilles Tendon Disorders
• Prevalence of Tendinopathy – Adult populaBon
• Age • AcJvity level
67
Achilles Tendon Disorders
• Risk Factors (Magnan et al. 2014) – Intrinsic
• Age, gender, body mass, tendon temperature, systemic diseases, muscle properJes (strength, flexibility, history, & anamoly), geneJc predisposiJon, blood supply
68
Achilles Tendon Disorders
• Risk Factors (Magnan et al. 2014) – Extrinsic
• MedicaJons • Overuse
69

24
Achilles Tendon Disorders
• Risk Factors – Body Mass Index (BMI) (Klein et al. 2013)
• Overweight: 2.6 Jmes more likely than normal BMI • Obese paJents: 6.6 Jmes more likely
• Pathogenesis algorithm (Magnan et al. 2014)
70
Continuum
71
ExaminaBon of Achilles Tendon
• Imaging – ~ One-‐third of symptomaBc tendons
• show histopathological changes (van Sterkenburg and van Dijk, 2011)
• Subclinical progresses into clinical – DiagnosBc Ultrasound Imaging – Shear-‐wave Elastography
• Highly specific, low sensiJvity (Aubry et al. 2014)
72

25
Achilles Imaging
• DiagnosBc Ultrasound • Normal
– Hyperechoic(genecity) • Abnormal
– Hypoechoic – NeovascularizaBon
73
Achilles Imaging • VascularizaBon Grading System (Del Buono et al. 2012) • Grade I
– One vessel into the tendon • Grade II
– Two vessels into the tendon • Grade III
– Neovascularisation involving less than 50 % of tendon thickness • Grade IV
– Neovascularisation involving from 50 % to 90 % of tendon thickness
• Grade V – Neovascularisation involving more than 90 % of tendon
thickness
74
ExaminaBon of Achilles Tendinopathy
• Importance of proper examinaBon – One cannot assume that all Achilles-‐related pain is tendinopathy
– DifferenBaBon is important • IntervenJonal success depends upon proper subgrouping
75

26
ExaminaBon of Achilles Tendinopathy
• Clinical Exam (Rieman et al. 2014) – Morning sBffness – PalpaBon for crepitus – Arc sign – Royal London Hospital test – Tendon loading test
• Passive dorsiflexion • Single-‐leg raise • Hop test
– The Sargeant Hop Test
76
ExaminaBon of Achilles Tendinopathy
• Clinical Exam – SubjecBve
• c/o pain with iniJal loading and eases with sustained acJvity
77
ExaminaBon of Achilles Tendinopathy
• Victorian Institute of Sport Assessment-Achilles (VISA-A) scores
• The American Orthopedic Foot and Ankle Society hindfoot scale (AOFAS)
• Functional Index of the Leg and Lower Limb (FILLA)
• Roles and Maudsley Score
78

27
IntervenBons for Achilles Tendon
• Footwear modificaBons – Lies – Rocker shoes
• Microtenotomy • Soe-‐Bssue mobilizaBon
– Instrumented – Manual
79
IntervenBons for Achilles Tendon
• Whole-‐body vibraBon • Extracorporeal shockwave therapy • Cryo-ultrasound • Laser
– Cold Air and High Energy Laser Therapy (CHELT) – Low-‐level laser
• Human Tecar
80
IntervenBons for Achilles Tendon
• TherapeuBc Exercise – Strengthening
• Classic eccentric studies – Stanish and Curwin – Alfredson – Meta-‐Analyses
http://app.isai.co.uk/app_helper/app_web_mobile/23/Custom_82159.html 81

28
IntervenBons for Achilles Tendon
• TherapeuBc Exercise – Evidence for strengthening – Mid-‐porBon tendinopathy (Zwiers et al. 2014, Rowe et al. 2012)
• Eccentric loading, 12-‐week program – Strong evidence
• Mixed-‐modal strengthening
82
IntervenBons for Achilles Tendon
• TherapeuBc Exercise – Stretching
• Mechanical sJmulus vs. intervenJon for inflexibility • Controversy with range of moJon and inflexibility with Achilles tendinopathy (Mahieu et al. 2006)
83
Summary
• Achilles tendinopathy is a common disorder that has a variable presentation
• Clinical differentiation is important during the clinical examination – mid-portion vs. insertional
• Evidence is strong for exercise interventions for mid-portion tendinopathy
84

29
Contact Information R. Barry Dale, PhD, PT, ATC 5721 USA Drive North Room 2011 Mobile, AL 36688 [email protected]
85
Patellar Tendinopathy (aka Jumper’s Knee)
Jeremiah Tate, PT, PhD Assistant Professor
Department of Physical Therapy University of Tennessee at Chattanooga
Patellar Tendinopathy (Warden and Brukner, 2003)
• Activity related anterior knee pain
• Focal tenderness at inferior patella pole/proximal tendon
• Abnormal tendon tissue
87

30
Prevalence • Elite athletes (Lian et al, 2005)
– 45% and 32% prevalence in volleyball and basketball players, respectively.
• Recreational athletes (Zwerver et al, 2011) – Overall prevalence of 8.5% – Highest prevalence in volleyball players (14.5%)
and lowest amongst soccer players (2.5% – 2x as common in males – Risk factors: loading characteristics, younger
age, taller body stature, and higher body weight
88
Risk Factors (van der Worp et al, 2011)
• No strong or moderate evidence for any risk factor associated with patellar tendinopathy
• Limited evidence related to: – Weight, body mass index, waist-to-hip ratio,
limb length inequality, arch height, quadriceps and hamstring flexibility, quadriceps strength, and vertical jump performance
89
Sports Specialization • Hall et al (2014) analyzed
relative risks of knee pain in adolescent females who specialized in 1 sport vs. playing multiple sports
• Findings demonstrated a 4-fold increase in developing Sinding-Larsen-Johansson, patellar tendinopathy and Osgood- Schlatter’s Disease in those who specialized.
90

31
Continuum Model (Cook and Purdam, 2009)
91
Pathophysiology
• Morphology – Individuals with patellar tendinopathy demonstrated
larger tendons compared to non-involved side and controls (Cook, 2000; Zhang et al, 2014)
• Elasticity – Individuals with patellar tendinopathy demonstrated
increased proximal tendon stiffness compared to non-involved side and controls (Zhang et al, 2014)
• Stiffness was associated with pain and dysfunction
– Others have demonstrated similar stiffness throughout the entire tendon (Kongsgaard, 2010)
92
Clinical Exam
• History of exercise-associated knee pain at the inferior pole of the patella
• Focal tenderness at the inferior pole of the patella
• Differential Diagnosis – Patellofemoral pain syndrome – Osgood-Schlatter’s Disease – Sinding-Larsen-Johansson
93

32
Imaging (Peers and Lysens, 2005)
• Radiographs – May identify bony abnormalities (eg, Osgood-
Schlatter’s or Sinding-Larsen-Johansson)
• Ultrasonography – Disruption of collagen fibers and areas of focal
hypoechogenicity
• MRI – Focal thickening of tendon (increased signal
intensity); tendon tears in proximal tendon in areas of tendinosis
94
Radiographs
Osgood-Schlatter’s Sinding-Larsen-Johansson
http://www.ultrasoundcases.info/Slide-View.aspx?cat=509&case=3976
http://radiopaedia.org/articles/osgood-schlatter-disease
95
Diagnostic Ultrasound (Hoksrud et al, 2006)
96

33
Diagnostic Ultrasound (Hoksrud et al, 2006)
97
MRI (Warden et al, 2007)
Normal Abnormal
98
Outcome Measures
• Numeric pain rating scale
• Victorian Institute of Sport Assessment Patella (VISA-P) Questionnaire
• Vertical jump performance (height & power)
99

34
VISA-P Questionnaire (Visentini et al, 1998)
• 0 to 100 points – 100 points = no pain and normal function
• Questions – Pain with sitting, walking downstairs, active
knee extension, full lunge, squatting, during or after 10 single leg hops, current sports/physical activity participation, and irritability
100
Conservative Management (Peers and Lysens, 2005)
• Training & risk factor modifications • Symptomatic approach
– Relative rest – NSAIDS/ice – Modalities (electrotherapy, US, laser)
• Loading Program • Peritendinous injections • Extracorporeal Shock Wave Therapy
101
Loading Programs (Pearson and Hussain, 2014)
• Both the Alfredson Protocol using a decline squat and heavy-slow resistance training have been demonstrated to be effective in treatment of patellar tendinopathy.
102
35
Alfredson Protocol (Zwerver et al, 2007)
• Squats on decline board (25°)
• Contraction type – Eccentric
• 3 sets of 15 performed twice daily for 12 weeks
• Progressed by increasing load via backpack
• Pain up to moderate levels (ie, 3/10 VAS)
103
Biomechanics of Single-Leg Decline Squat
(Zwerver et al, 2007)
• Single leg squat on decline boards (ranging between 15-30° resulted in increased knee extensor moment and reduced hip extensor and ankle plantar flexion moments
• Recommended to limit knee flexion to 60° due to steeper increase in patellofemoral joint reaction forces
104
Heavy Slow Resistance (Kongsgaard, 2010)
• 3 main exercises – Squat, leg press, and hack squat
• Performed 3x/week
• 4 sets of each exercise – Week 1 - 15 repetition maximum (RM) – Weeks 2-3 – 12 RM – Weeks 4-5 – 10 RM – Weeks 6-8 – 8 RM – Weeks 9-12 – 6 RM
105

36
Peritendinous Injections (van Ark et al, 2011)
• Dry needling – Stimulate inflammatory
response
• Platelet-rich plasma (PRP)/Autologous blood – “cocktail” of growth factors
• Sclerosis/high-volume – Reduce/eliminate
neovacularization and accompanying nerve fibers
• Aprotinin – Collagenase inhibitor
(Hoksrud, AJSM, 2006) 106
Extracorporeal Shock Wave Therapy (ESWT)
• ESWT has been demonstrated as superior to other conservative treatments and equal to long-term surgical outcomes. (Mani-Babu et al, 2014)
http://www.physio-chelsea.co.uk/shockwave.html
107
Surgical Managment • Longitudinal tenotomy (Bahr et al, 2006)
– Removal of abnormal tendon tissue – Similar results compared to eccentric exercise
group – Recommended only after failure of conservative
treatment
• Arthroscopic shaving (Willberg, 2011) – Targets tissue with high blood flow and nerves on
dorsal aspect of tendon – Fast recovery (6-8 weeks) with good results
108

37
Thank You!
Questions???