Approach to Dm Pt.

of 71
-
Upload
shreeja-maheshwari -
Category
Documents
-
view
217 -
download
0
Transcript of Approach to Dm Pt.
-
8/14/2019 Approach to Dm Pt.
1/71
APPROACH TOPPROACH TODIABETESIABETESMELLITUSELLITUSPATIENTATIENT
PRESENTED BY :
Roll No : 648
SHREEJA MAHESHWARI
-
8/14/2019 Approach to Dm Pt.
2/71
HyperglycemiaHyperglycemia
DrowsyDrowsy
FlushedFlushed
ThirstyThirsty
-
8/14/2019 Approach to Dm Pt.
3/71
Diabetes MellitusDiabetes Mellitus
HYPERGLYCEMIAHYPERGLYCEMIA: fluid/electrolyte: fluid/electrolyte
imbalance.imbalance. PolyuriaPolyuria
Sodium, chloride, potassium excretedSodium, chloride, potassium excreted
PolydipsiaPolydipsia from dehydrationfrom dehydration
PolyphagiaPolyphagia: cells are starving, so person: cells are starving, so person
feels hungry despite eating huge amounts offeels hungry despite eating huge amounts offood. Starvation state remains until insulin isfood. Starvation state remains until insulin is
available.available.
-
8/14/2019 Approach to Dm Pt.
4/71
Skin problems-Skin Infections leading to boils,carbuncles or abscesses.-Oral & Genital candidiasis
-
8/14/2019 Approach to Dm Pt.
5/71
Diabetes MellitusDiabetes Mellitus
Major risk factorsMajor risk factors Family history -Family history - A history of diabetes in first-degreeA history of diabetes in first-degree
relatives is a potent risk factor for diabetes. Type 2relatives is a potent risk factor for diabetes. Type 2diabetes appears to have a stronger geneticdiabetes appears to have a stronger genetic
component than type 1.component than type 1. ObesityObesity Origin (Afro-American, Hispanic, Native American,Origin (Afro-American, Hispanic, Native American,
Asian-American)Asian-American) Age (older than 45)Age (older than 45)
History of gestational diabetesHistory of gestational diabetes High cholesterolHigh cholesterol HypertensionHypertension Vascular disease (cerebro-, cardio- or peripheralVascular disease (cerebro-, cardio- or peripheral
vascular )vascular )
-
8/14/2019 Approach to Dm Pt.
6/71
DIET & LIFE STYLE HISTORYDIET & LIFE STYLE HISTORY
Regularity of mealsRegularity of meals
Content of fatty foodsContent of fatty foods
Content of fruits &Content of fruits &vegetablesvegetables
Contents of sugary foodsContents of sugary foods
Content of saltContent of salt
Alcohol intakeAlcohol intake
Smoking historySmoking history
Occupational historyOccupational history
Physical activityPhysical activity
-
8/14/2019 Approach to Dm Pt.
7/71
HISTORY IN DIAGNOSEDHISTORY IN DIAGNOSED
PATIENTSPATIENTS
HOME GLUCOSEHOME GLUCOSETESTING IN PREVIOUSLYTESTING IN PREVIOUSLY
DIAGNOSED PTS.DIAGNOSED PTS.
INSULIN INJECTIONS INSULIN INJECTIONS
Ascertain whether theAscertain whether thepatient self injects, deliverypatient self injects, delivery
device, site chosen, anddevice, site chosen, and
whether they experiencewhether they experience
any problems.any problems.
-
8/14/2019 Approach to Dm Pt.
8/71
SYMPTOMS OFSYMPTOMS OF
COMPLICATIONS OF DIABETESCOMPLICATIONS OF DIABETESMACROVASCULAR DISEASE
1. CORONARY HEART DISEASE Pt.
has less severe chest pain symptom
known as silent ischemia due to
autonomic neuropathy. Only symptom
can be breathlessness.
2. PERIPHERAL VASCULAR DISEASE
Pt. present with claudication. There
may be foot ulceration.
3. CEREBROVASCULAR DISEASE
Pt. may present with stroke
syndrome. TIA are common.
-
8/14/2019 Approach to Dm Pt.
9/71
MICROVASCULAR DISEASEMICROVASCULAR DISEASE1.1. RETINOPATHYRETINOPATHY May be asymptomatic until it cause significant May be asymptomatic until it cause significant
visual loss, acute due to retinal hemorrhage or insidious due tovisual loss, acute due to retinal hemorrhage or insidious due tocataract or maculopathy.cataract or maculopathy.
2.2. NEPHROPATHYNEPHROPATHY May be asymptomatic until uraemic symptoms May be asymptomatic until uraemic symptomsensues like fatigue, breathlessness, tachypnoea, pleuritic chestensues like fatigue, breathlessness, tachypnoea, pleuritic chestpain and pruritus.pain and pruritus.
3.3. NEUROPATHYNEUROPATHY
Peripheral sensory neuropathyPeripheral sensory neuropathy numbness, a feeling of walking on numbness, a feeling of walking oncotton wool and paraesthesias or burning, sharp shooting pains.cotton wool and paraesthesias or burning, sharp shooting pains.
Proximal motor neuropathyProximal motor neuropathy (Femoral neuropathy) uncommon but(Femoral neuropathy) uncommon butpresents with deep pain and parasthesiae in upper anterior thigh,presents with deep pain and parasthesiae in upper anterior thigh,followed by wasting of quadriceps muscle.followed by wasting of quadriceps muscle.
MononeuropathiesMononeuropathies particularly affecting the median nerve of the hand particularly affecting the median nerve of the hand(carpal tunnel syndrome ) This presents with parasthesiae and(carpal tunnel syndrome ) This presents with parasthesiae andnumbness in the median nerve distribution of the hand (lateral two-numbness in the median nerve distribution of the hand (lateral two-
and-half digits), and is again worse at night. Similar symptoms mayand-half digits), and is again worse at night. Similar symptoms mayoccur in the foot (tarsal tunnel syndrome). Cranialoccur in the foot (tarsal tunnel syndrome). Cranialmononeuropathies are raremononeuropathies are rare
Autonomic Neuropathy-Autonomic Neuropathy- symptoms includes impotence, gustatorysymptoms includes impotence, gustatorysweating, urinary retention or incontinence, dizziness or syncopesweating, urinary retention or incontinence, dizziness or syncopedue to postural hypotension, constipation or diarrhoea, and nauseadue to postural hypotension, constipation or diarrhoea, and nauseavomiting due to diabetic gastroparesis.vomiting due to diabetic gastroparesis.
-
8/14/2019 Approach to Dm Pt.
10/71
EXAMINATION OFEXAMINATION OF
THE DAIBETIC PATIENTTHE DAIBETIC PATIENTAcute hyperglycemic crises Acute hyperglycemic crises 1. Severely dehydrated with dry mucous membranes and reduced skin1. Severely dehydrated with dry mucous membranes and reduced skin
turgor.turgor.
2. Hypotension and tachycardia2. Hypotension and tachycardia
3. Signs of diabetic ketoacidosis3. Signs of diabetic ketoacidosis
Non acute cases :Non acute cases :1. Ascertain BMI1. Ascertain BMI
2. Blood pressure erect and supine2. Blood pressure erect and supine
3. Injection sites3. Injection sites
4. Dermatological examination4. Dermatological examination
5. Examination of eyes5. Examination of eyes6. Examination of CVS6. Examination of CVS
7. Examination of Feet7. Examination of Feet
-
8/14/2019 Approach to Dm Pt.
11/71
COMMONLY ENCOUNTERED MANIFESTATIONSCOMMONLY ENCOUNTERED MANIFESTATIONS Skin thickeningSkin thickening Microvascular manifestations in the skinMicrovascular manifestations in the skin .. Neuropathy of the footNeuropathy of the foot Infection of the skin in diabetesInfection of the skin in diabetes .. Yellow skin and nailsYellow skin and nails
DISTINCT BUT UNCOMMON MANIFESTATIONSDISTINCT BUT UNCOMMON MANIFESTATIONS
Necrobiosis lipoidicaNecrobiosis lipoidica Necrobiosis lipoidica is a distinct skin manifestation which is moreNecrobiosis lipoidica is a distinct skin manifestation which is more
commonly found in patients who also have diabetes mellitus.commonly found in patients who also have diabetes mellitus. Diabetic bullaeDiabetic bullae With no other apparent cause, diabetics may develop blisters, usuallyWith no other apparent cause, diabetics may develop blisters, usually
on the extremities.on the extremities.
Disseminated granuloma annulareDisseminated granuloma annulare Patients who develop disseminated granuloma annulare have beenPatients who develop disseminated granuloma annulare have beennoted to commonly have diabetes mellitus.noted to commonly have diabetes mellitus.
Kyrle diseaseKyrle disease An uncommon but distinct finding in diabetic patients with renal disease.An uncommon but distinct finding in diabetic patients with renal disease. Cutaneous side effects of insulin injectionCutaneous side effects of insulin injection
Patients who need daily insulin to control their sugar metabolism mayPatients who need daily insulin to control their sugar metabolism maydevelop secondary skin problems.develop secondary skin problems.
Dermatological examinationDermatological examination
-
8/14/2019 Approach to Dm Pt.
12/71
Anterolateral neck region and dorsum of right hand of a diabetic patientAnterolateral neck region and dorsum of right hand of a diabetic patient
with acanthosis nigricans. It is recognized by the darker velvety skin.with acanthosis nigricans. It is recognized by the darker velvety skin.
The dorsum of the fingers are similarly involved with velvety skin.The dorsum of the fingers are similarly involved with velvety skin. It isIt is
associated with increased epidermal thickness.associated with increased epidermal thickness.
Velvety appearance consists ofVelvety appearance consists of
multiple closely spacedmultiple closely spaced
micropapules.micropapules.
PEBBLES - ACANTHOSIS NIGRICANSPEBBLES - ACANTHOSIS NIGRICANS
-
8/14/2019 Approach to Dm Pt.
13/71
pebbles - thick skin of diabetespebbles - thick skin of diabetesmellitusmellitus
Although he does not have acanthosisnigricans, he does have similardiscrete micropapules located on theknuckle area of this finger..
Proximal nail fold skin of a diabeticProximal nail fold skin of a diabeticpatient who demonstratespatient who demonstratesmicropapules or "pebbles" in themicropapules or "pebbles" in theabsence of acanthosis nigricans.absence of acanthosis nigricans.
Note that the micropapules in thisNote that the micropapules in thispatient are far less exaggerated thanpatient are far less exaggerated thanthose which occur in acanthosisthose which occur in acanthosisnigricans.nigricans. ..
-
8/14/2019 Approach to Dm Pt.
14/71
Distal inter-phalangeal joint and dorsum of the distal aspectDistal inter-phalangeal joint and dorsum of the distal aspect
of the left foot diabetic patients demonstrating pebbling.of the left foot diabetic patients demonstrating pebbling.
Clinically thickened skin is common on the dorsum of theClinically thickened skin is common on the dorsum of the
hand (especially over the knuckles) and sometimes even onhand (especially over the knuckles) and sometimes even on
the dorsum of the toes.the dorsum of the toes.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10052m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10044m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10080m.jpg -
8/14/2019 Approach to Dm Pt.
15/71
DIABETICDIABETICSCLEREDEMASCLEREDEMA
Occurs in about threeOccurs in about threepercent of diabetics andpercent of diabetics andis almost totally limitedis almost totally limited
to those with adult onsetto those with adult onsetdisease.disease.
There is visible thickeningThere is visible thickeninginvolving skin on theinvolving skin on theback of the neck and theback of the neck and theupper back.upper back.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10080m.jpg -
8/14/2019 Approach to Dm Pt.
16/71
Diabetic Hand SyndromeDiabetic Hand SyndromeDiabetic hand syndrome consists of joint limitations (inability toDiabetic hand syndrome consists of joint limitations (inability to
fully extend a finger) and thickened skin of the hand, especiallyfully extend a finger) and thickened skin of the hand, especiallyinvolving the dorsum of the fingersinvolving the dorsum of the fingers palpably thickened skinpalpably thickened skin
Some patients with diabetes mellitus develop thickening of theSome patients with diabetes mellitus develop thickening of theskin on the fingers which is termed "scleroderma-like". Thisskin on the fingers which is termed "scleroderma-like". Thisterminology does not imply that existence of vasculitis, orterminology does not imply that existence of vasculitis, or
Raynaud's phenomenon, only that the skin is thicker.Raynaud's phenomenon, only that the skin is thicker.
Joint limitationJoint limitationIn addition to thickened skin, diabetic hand syndrome isIn addition to thickened skin, diabetic hand syndrome is
characterized by joint limitation. Often diabetics developcharacterized by joint limitation. Often diabetics developasymptomatic joint limitations of the fingers. This limitation isasymptomatic joint limitations of the fingers. This limitation isusually minor and not incapacitating. Thick skin and jointusually minor and not incapacitating. Thick skin and jointlimitation seem to correlate with retinopathylimitation seem to correlate with retinopathy..
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10033m.jpg -
8/14/2019 Approach to Dm Pt.
17/71
The patient's finger on the right is pushingagainst the examiner's fingers on the left.The finger skin is taught and when thepatient pushed, his finger blanched exceptfor a periungual blush.
Diabetic Hand SyndromeDiabetic Hand Syndrome
The examiner is attempting to tent the dorsal
finger skin which is distal to the proximal
interphalangeal joint of this patient . With non-diabetic subjects, it is fairly easy to pick up a
fold of skin on the dorsum of the fingers. This
is often not the case in persons with diabetes.
The fifth finger demonstrates a typical minor
joint limitation. The fifth finger cannot fully
extend.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10039m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10073m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10039m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10033m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10074m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10034m.jpg -
8/14/2019 Approach to Dm Pt.
18/71
The hands of two patients with diabetes mellitus and the diabeticThe hands of two patients with diabetes mellitus and the diabetic
hand syndrome. The patients are attempting to fully appose thehand syndrome. The patients are attempting to fully appose the
palms and fingers. The patient on the left illustrates moderatepalms and fingers. The patient on the left illustrates moderate
limitation. The patient on the right has significant impairment.limitation. The patient on the right has significant impairment.
PRAYER SIGN(CHEIROARTHROPATHY
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10074m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10034m.jpg -
8/14/2019 Approach to Dm Pt.
19/71
Erythema of the proximal nail fold.Erythema of the proximal nail fold.
Shin of a patient demonstratingShin of a patient demonstratinghyperpigmented atrophic macules.hyperpigmented atrophic macules.
The patient relates previous traumaThe patient relates previous traumafor each of these spots.for each of these spots.
PERIUNGUAL ERYTHEMAPERIUNGUAL ERYTHEMA
Microvascular disease is a major complication of diabetes mellitus.Microvascular disease is a major complication of diabetes mellitus.
At the capillary level, this can be due to both a structural (e.g.At the capillary level, this can be due to both a structural (e.g.
thickened capillary wall) and functional problems (increased bloodthickened capillary wall) and functional problems (increased bloodviscosity). Impaired blood flow due to increased viscosity results inviscosity). Impaired blood flow due to increased viscosity results in
dilated capillary loops, and such clinical manifestations as facialdilated capillary loops, and such clinical manifestations as facial
blush and periungual erythema.blush and periungual erythema.
DERMOPATHYDERMOPATHY
-
8/14/2019 Approach to Dm Pt.
20/71
DERMOPATHYDERMOPATHY
Diabetic dermopathy is a condition characterized by the presenceDiabetic dermopathy is a condition characterized by the presence
of multiple hyperpigmented atrophic macules on the legs. Typicalof multiple hyperpigmented atrophic macules on the legs. Typical
lesions are depressed (atrophic) and appear to have post-lesions are depressed (atrophic) and appear to have post-
inflammatory hyperpigmentation. The occurrence of 4 or moreinflammatory hyperpigmentation. The occurrence of 4 or moresuch lesions is almost always limited to persons with diabetes.such lesions is almost always limited to persons with diabetes.
PIGMENTED PURPURAPIGMENTED PURPURA
-
8/14/2019 Approach to Dm Pt.
21/71
PIGMENTED PURPURAPIGMENTED PURPURA
Pigmented purpura of the legs is most often encountered in thePigmented purpura of the legs is most often encountered in the
elderly diabetic. These areas of spontaneous focal extravasationelderly diabetic. These areas of spontaneous focal extravasation
from the microcirculation are recognized as brown to red maculesfrom the microcirculation are recognized as brown to red macules
and patches.and patches.Erythematous, brown, and golden macular changes on theErythematous, brown, and golden macular changes on the
shins. The small erythematous areas, representing recentshins. The small erythematous areas, representing recent
vascular hemorrhage gradually enlarge, turn brown, andvascular hemorrhage gradually enlarge, turn brown, and
coalesce with neighboring lesions.coalesce with neighboring lesions.
With resolution, the lesionWith resolution, the lesionhave a golden appearance.have a golden appearance.
Close-up view of the shin demonstrating theClose-up view of the shin demonstrating the
presence of diabetic dermopathy and pigmentedpresence of diabetic dermopathy and pigmented
purpura. The dermopathy is distinguished by thepurpura. The dermopathy is distinguished by the
atrophy whereas the changes involved withatrophy whereas the changes involved with
pigmented purpura are macular.pigmented purpura are macular.
-
8/14/2019 Approach to Dm Pt.
22/71
SENSORY NEUROPATHYSENSORY NEUROPATHYAnother major complication of diabetes mellitus is developmentAnother major complication of diabetes mellitus is developmentof neuropathy. Relative to the skin, the most commonof neuropathy. Relative to the skin, the most commonmanifestations involve legs and feet. Sensory neuropathy allowsmanifestations involve legs and feet. Sensory neuropathy allowstrauma to occur to the feet from ill-fitting shoes which may thentrauma to occur to the feet from ill-fitting shoes which may thenresult in ulceration.result in ulceration.
callus and ulcer on the distalcallus and ulcer on the distalaspect of the right second toe.aspect of the right second toe.
multiple erosions on themultiple erosions on thedorsal aspect of the toes.dorsal aspect of the toes.
MOTOR NEUROPATHYMOTOR NEUROPATHY
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10084m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10082m.jpg -
8/14/2019 Approach to Dm Pt.
23/71
MOTOR NEUROPATHYMOTOR NEUROPATHYMotor neuropathy results in weakened intrinsic foot muscles. The toesMotor neuropathy results in weakened intrinsic foot muscles. The toes
dorsiflex and the foot splays (becomes wider) on weight -bearing. This newdorsiflex and the foot splays (becomes wider) on weight -bearing. This new
shape may no longer fit the previous shoes and, along with sensoryshape may no longer fit the previous shoes and, along with sensory
neuropathy, may potentiate trauma and ulceration.neuropathy, may potentiate trauma and ulceration.
CHARCOT FOOTCHARCOT FOOTWith loss of sensation and weak intrinsic muscles, the foot may fractureWith loss of sensation and weak intrinsic muscles, the foot may fracture
when stressed. Multiple fractures allowed to heal without realignment resultwhen stressed. Multiple fractures allowed to heal without realignment result
in the distortion of shape.in the distortion of shape.
The toes are being drawn upward.The toes are being drawn upward. Sensory and motor neuropathy.Sensory and motor neuropathy.
She started to run bare foot and heard thShe started to run bare foot and heard thsnapping sound in her feet .snapping sound in her feet .
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10087m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10085m.jpg -
8/14/2019 Approach to Dm Pt.
24/71
CANDIDA INFECTIONCANDIDA INFECTIONCandida albicansCandida albicans is a frequent pathogen in the skin ofis a frequent pathogen in the skin ofdiabetics usually involving the groin or genital region. Candidadiabetics usually involving the groin or genital region. Candida
involvement of the groin region and uncircumcised penis tendinvolvement of the groin region and uncircumcised penis tendto occur in men who have poor control of their diabetes.to occur in men who have poor control of their diabetes.
the groin region has erythema andthe groin region has erythema and
multiple satellite papulesmultiple satellite papules
erythema of the glans peniserythema of the glans penis
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/C20085m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/C20086m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/C20084m.jpg -
8/14/2019 Approach to Dm Pt.
25/71
The hands may also becomeThe hands may also become
involved with Candida. Usual sitesinvolved with Candida. Usual sites
of infection include proximal nailof infection include proximal nail
fold and intertriginous areas whichfold and intertriginous areas which
allow for natural moisture toallow for natural moisture to
accumulate.accumulate.
MALIGNANT EXTERNALMALIGNANT EXTERNAL
OTITISOTITISExternal otitis is a common, howeverExternal otitis is a common, however
in diabetics it may become a seriousin diabetics it may become a seriousproblem. The patient complains ofproblem. The patient complains of
severe ear pain from the otitis. Thesevere ear pain from the otitis. The
infection, due toinfection, due to PseudomonasPseudomonas, may, may
even gain access to cranial nerves.even gain access to cranial nerves.
Examination of the ear canal revealsExamination of the ear canal reveals
polypoid growths.polypoid growths.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10030m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/C20084m.jpg -
8/14/2019 Approach to Dm Pt.
26/71
STAPHYLOCOCCUS
INFECTIONAbscess involving the left arm of
a diabetic patient. This patient
developed a carbuncle at the site
of insulin injection.
This patient has an ankle ulcer which
developed an erythematous halo and a red
streak going up the leg. This vascular ulcer
is complicated by cellulitis and
lymphangitis
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10066m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10065m.jpg -
8/14/2019 Approach to Dm Pt.
27/71
DERMATOPHYTE INFECTIONDERMATOPHYTE INFECTION
annular erythematous scaling plaque ofannular erythematous scaling plaque of
dermatophyte infection.dermatophyte infection.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10070m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10054m.jpg -
8/14/2019 Approach to Dm Pt.
28/71
YELLOW NAILSYELLOW NAILS
The skin and nails ofThe skin and nails of
patients with diabetes tendpatients with diabetes tend
to take on a yellow hue,to take on a yellow hue,probably due toprobably due to
metabolism of glucosemetabolism of glucose
which has become linkedwhich has become linked
to protein.to protein.
YELLOW SKINYELLOW SKIN
Persons with diabetesPersons with diabetes
often have a yellow hueoften have a yellow hue
to the skin, best seen onto the skin, best seen on
the palms and soles.the palms and soles.
Probably due to yellowProbably due to yellow
glucosylation end-glucosylation end-
productsproducts
NECROBIOSIS LIPOIDICANECROBIOSIS LIPOIDICA
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10055m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10054m.jpg -
8/14/2019 Approach to Dm Pt.
29/71
NECROBIOSIS LIPOIDICANECROBIOSIS LIPOIDICA
Although necrobiosis is a classic finding in diabetes, it is ratherAlthough necrobiosis is a classic finding in diabetes, it is ratheruncommon (less than one percent) and may also occur inuncommon (less than one percent) and may also occur inpersons who do not have the disease. Typical involvementpersons who do not have the disease. Typical involvementoccurs on the legs as bilateral erythematous, brown or yellowoccurs on the legs as bilateral erythematous, brown or yellowplaques with raised margins and central atrophy. The surface ofplaques with raised margins and central atrophy. The surface ofa lesion often becomes somewhat transparent and enlargeda lesion often becomes somewhat transparent and enlargedblood vessels may be seen in the lesion.blood vessels may be seen in the lesion.
the early papule stagethe early papule stagecharacteristiccharacteristictranslucency andtranslucency andenlargement ofenlargement ofunderlyingunderlying
cutaneous bloodcutaneous bloodvessels.vessels.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10010m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10002m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10007m.jpg -
8/14/2019 Approach to Dm Pt.
30/71
SPONTANEOUS BLISTERS IN DIABETESSPONTANEOUS BLISTERS IN DIABETES
Lesions may rupture, develop an ulcer orLesions may rupture, develop an ulcer or
become secondarily infected.become secondarily infected.
http://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10026m.jpghttp://dermatology.cdlib.org/DOJvol1num2/diabetes/diabetes-images/D10074m.jpg -
8/14/2019 Approach to Dm Pt.
31/71
DIABETIC NEUROPATHYDIABETIC NEUROPATHY
Diabetic Neuropathy is a common complication of DM. It usually includesDiabetic Neuropathy is a common complication of DM. It usually includesmicro vascular injury to the small blood vessels leading to your nerves.micro vascular injury to the small blood vessels leading to your nerves.Diabetic Neuropathy is damage to nerves caused by the prolongedDiabetic Neuropathy is damage to nerves caused by the prolongedeffect of high sugar levels in the blood.effect of high sugar levels in the blood.
Diabetic neuropathyDiabetic neuropathy is caused by the walls of the blood vessels that supplyis caused by the walls of the blood vessels that supplythe nerves becoming thicker. The end result of this is less nutrients arethe nerves becoming thicker. The end result of this is less nutrients areunable to get to the nerves as well as a demyelinization. This slows theunable to get to the nerves as well as a demyelinization. This slows theability of the nerves to conduct impulses back to the brain.ability of the nerves to conduct impulses back to the brain.
The four types are :The four types are :
-Peripheral that affects the extremities of the body, notably the feet-Peripheral that affects the extremities of the body, notably the feet
-Autonomic that affects the autonomic nervous system-Autonomic that affects the autonomic nervous system
-Proximal the areas affects are the hips, thighs and buttocks-Proximal the areas affects are the hips, thighs and buttocks
-Focal a focused group of nerves in any region of the body.-Focal a focused group of nerves in any region of the body.
There are two forms of neuropathies that can form with diabetes;There are two forms of neuropathies that can form with diabetes;
http://www.diabeticsupplie-s.us/diabetic-neuropathyhttp://www.diabeticsupplie-s.us/diabetic-neuropathyhttp://www.diabeticsupplie-s.us/diabetic-neuropathy -
8/14/2019 Approach to Dm Pt.
32/71
There are two forms of neuropathies that can form with diabetes;There are two forms of neuropathies that can form with diabetes;
polynueropathies and mononeuropathies.polynueropathies and mononeuropathies.
PolynueropathiesPolynueropathies are the most common in those with diabetesare the most common in those with diabetes
and is a bilateral sensory disorder. The symptoms for this formand is a bilateral sensory disorder. The symptoms for this form
are most common in the toes and feet and normally appearare most common in the toes and feet and normally appearthere first.there first.
MononeuropathiesMononeuropathies are isolated events that affect singleare isolated events that affect single
nerves. The symptoms of this form of neuropathy are entirelynerves. The symptoms of this form of neuropathy are entirely
dependent on which nerve is affected.dependent on which nerve is affected.
http://images.google.co.in/imgres?imgurl=http://fammed.washington.edu/residency/sports/images/eponyms/mano_test_phalen.jpg&imgrefurl=http://fammed.washington.edu/residency/sports/webpages/eponyms.html&usg=__WRyUR6Aa0uRtEn0fBfCRh8mEewE=&h=480&w=640&sz=63&hl=en&start=8&tbnid=XVMIKsKsvVUrgM:&tbnh=103&tbnw=137&prev=/images%3Fq%3Dphalens%2Bsign%26gbv%3D2%26hl%3Den%26sa%3DG -
8/14/2019 Approach to Dm Pt.
33/71
CARPAL
TUNNEL
SYNDROME
http://images.google.co.in/imgres?imgurl=http://images.vortala.com/chiropractor/graphics/AUS_Parent_Images/ct2.jpg&imgrefurl=http://www.sfholistichealth.com/printformat.asp%3Fchiropractor%3D171S&usg=__HnSZyAnjeBCuK-05TVKAz3Hg5Dk=&h=286&w=450&sz=20&hl=en&start=10&tbnid=SdXE4Zi8PTEpuM:&tbnh=81&tbnw=127&prev=/images%3Fq%3Dtinel%2527s%2Bsign%26gbv%3D2%26hl%3Denhttp://images.google.co.in/imgres?imgurl=http://fammed.washington.edu/residency/sports/images/eponyms/mano_test_phalen.jpg&imgrefurl=http://fammed.washington.edu/residency/sports/webpages/eponyms.html&usg=__WRyUR6Aa0uRtEn0fBfCRh8mEewE=&h=480&w=640&sz=63&hl=en&start=8&tbnid=XVMIKsKsvVUrgM:&tbnh=103&tbnw=137&prev=/images%3Fq%3Dphalens%2Bsign%26gbv%3D2%26hl%3Den%26sa%3DG -
8/14/2019 Approach to Dm Pt.
34/71
INSULIN INJECTION SITEINSULIN INJECTION SITE
LIPOATROPHY AND LIPOHYPERTROPHYLIPOATROPHY AND LIPOHYPERTROPHY
DIABETIC NEPHROPATHY
http://images.google.co.in/imgres?imgurl=http://www.sanitasmed.com/img/ypsomed/click20.jpg&imgrefurl=http://www.sanitasmed.com/ypsomed2.html&usg=__TBnGeDvbSqRP1XaovorrRJBPxcg=&h=127&w=193&sz=5&hl=en&start=4&tbnid=v-HGObMWvJh3VM:&tbnh=68&tbnw=103&prev=/images%3Fq%3Dlipohypertrophy%26gbv%3D2%26hl%3Den%26sa%3DGhttp://images.google.co.in/imgres?imgurl=http://www.childrenwithdiabetes.com/clinic/i/lipoatrophy21024.jpg&imgrefurl=http://www.childrenwithdiabetes.com/dteam/2006-10/d_0d_e99.htm&usg=__4SGP_vVO_DF0IZcX_p-OUMDoJ5s=&h=963&w=1024&sz=502&hl=en&start=9&tbnid=Rynlp_BJ_g-tyM:&tbnh=141&tbnw=150&prev=/images%3Fq%3Dlipoatrophy%26gbv%3D2%26hl%3Den%26sa%3DG -
8/14/2019 Approach to Dm Pt.
35/71
DIABETIC NEPHROPATHY
Diabetic nephropathy
refers to kidney problemswhich result from diabetes
mellitus. These include the
excretion of protein in the
urine (proteinuria) and
slowly developing kidney
failure. Diabetes interferesDiabetes interferes
with the function of thewith the function of the
glomerular tuft. Whenglomerular tuft. When
enough of these tufts haveenough of these tufts havebeen affected, kidneybeen affected, kidney
failure results.failure results.
ProteinuriaProteinuria
-
8/14/2019 Approach to Dm Pt.
36/71
ProteinuriaProteinuria
Most people with establishedMost people with established
diabetic nephropathy havediabetic nephropathy have
urine containing largeurine containing large
quantities of protein (knownquantities of protein (knownas proteinuria), which theiras proteinuria), which their
doctors can detect using adoctors can detect using a
dipstick urine test.dipstick urine test.
High blood pressureHigh blood pressure
Another related condition of diabetic nephropathy is high bloodAnother related condition of diabetic nephropathy is high bloodpressure (hypertension). Hypertension will speed up existing kidneypressure (hypertension). Hypertension will speed up existing kidney
disease, so treatment of even mild hypertension is necessary for thosedisease, so treatment of even mild hypertension is necessary for those
with diabetes. Because the function of the kidney deteriorates andwith diabetes. Because the function of the kidney deteriorates and
protein is lost, puffy swelling of the body tissues, especially the legs,protein is lost, puffy swelling of the body tissues, especially the legs,
can occur. This is called the nephrotic syndrome.can occur. This is called the nephrotic syndrome.
MOUTH COMPLICATIONSMOUTH COMPLICATIONS
-
8/14/2019 Approach to Dm Pt.
37/71
MOUTH COMPLICATIONSMOUTH COMPLICATIONS
Periodontal disease is infection and inflammation of the gums. It canPeriodontal disease is infection and inflammation of the gums. It cancause gum recession, bone and tooth loss. High blood sugars causecause gum recession, bone and tooth loss. High blood sugars causeinflammation of the gums and promote infection.inflammation of the gums and promote infection.
Periodontal diseasePeriodontal disease
Common signs of periodontal disease are gums that are swollen andCommon signs of periodontal disease are gums that are swollen andbleed easily. Chronic high blood sugar can also cause yeast infectionsbleed easily. Chronic high blood sugar can also cause yeast infectionsin the mouth and dental caries.in the mouth and dental caries.
-
8/14/2019 Approach to Dm Pt.
38/71
Heart Disease & StrokeHeart Disease & StrokeVascular disease can affect all blood vessels inVascular disease can affect all blood vessels in
the body. Blocked arteries in the brain can leadthe body. Blocked arteries in the brain can leadto a TIA (transient ischemic attack) or stroke.to a TIA (transient ischemic attack) or stroke.
Blocked arteries in the heart can lead to chestBlocked arteries in the heart can lead to chest
pain (e.g., angina) or a heart attack. Blockedpain (e.g., angina) or a heart attack. Blocked
arteries in the legs can cause problems witharteries in the legs can cause problems with
circulation and walking. Erectile problems alsocirculation and walking. Erectile problems alsocan be due to blocked arteries.can be due to blocked arteries.
Vascular diseaseVascular disease
It is caused by stiffening and clogging ofIt is caused by stiffening and clogging of
arteries (atherosclerosis). In diabetes, when thearteries (atherosclerosis). In diabetes, when the
blood sugar is chronically high, excessiveblood sugar is chronically high, excessiveamounts of glucose attach to the inner walls ofamounts of glucose attach to the inner walls of
the blood vessels, decreasing their elasticity.the blood vessels, decreasing their elasticity.
Elevated blood sugars also causeElevated blood sugars also cause
atherosclerosis by promoting plaqueatherosclerosis by promoting plaque
formation.formation.
DIABETIC RETINOPATHYDIABETIC RETINOPATHY
-
8/14/2019 Approach to Dm Pt.
39/71
DIABETIC RETINOPATHYDIABETIC RETINOPATHY
People with diabetes have an increased chance of developing a varietyPeople with diabetes have an increased chance of developing a varietyof eye problems, includingof eye problems, including cataractscataracts andand glaucomaglaucoma. Typically,. Typically,
changes begin to take place in the retina after a patient has beenchanges begin to take place in the retina after a patient has beenliving with diabetes for 10 to 15 years. The effect of diabetes on theliving with diabetes for 10 to 15 years. The effect of diabetes on theretina and vitreous is called diabetic retinopathy.retina and vitreous is called diabetic retinopathy.
In the earliest phase of the disease, known asIn the earliest phase of the disease, known as background diabeticbackground diabeticretinopathyretinopathy, the arteries in the retina become weakened and leak,, the arteries in the retina become weakened and leak,forming small, dot-like hemorrhages. These leaking vessels oftenforming small, dot-like hemorrhages. These leaking vessels often
lead to swelling or edema in the retina, which may result inlead to swelling or edema in the retina, which may result indecreased vision.decreased vision.
The next stage is known asThe next stage is known as proliferative diabetic retinopathyproliferative diabetic retinopathy. In this. In thisstage, circulation problems lead to oxygen-deprivation in some areasstage, circulation problems lead to oxygen-deprivation in some areasof the retina. New, fragile, blood vessels develop as the circulatoryof the retina. New, fragile, blood vessels develop as the circulatorysystem attempts to maintain adequate oxygen levels within thesystem attempts to maintain adequate oxygen levels within theretina. This is called neovascularization. The delicate vesselsretina. This is called neovascularization. The delicate vesselshemorrhage easily and blood may leak into the retina and vitreous,hemorrhage easily and blood may leak into the retina and vitreous,causing spots or floaters, and an overall decrease in vision.causing spots or floaters, and an overall decrease in vision.
A th di f th ti d b l l
http://www.stlukescataract.com/http://www.stlukescataract.com/http://www.stlukeseye.com/Conditions/Glaucoma.asphttp://www.stlukeseye.com/Conditions/Glaucoma.asphttp://www.stlukeseye.com/Conditions/Glaucoma.asphttp://www.stlukescataract.com/ -
8/14/2019 Approach to Dm Pt.
40/71
As the disease progresses even further, continued abnormal vessel
growth and scarring can result in serious problems such as retinal
detachment and glaucoma.
Signs and Symptoms
Blurred vision - often linked to blood sugar levels- often linked to blood sugar levelsFloaters and flashesFloaters and flashesSudden loss of visionSudden loss of vision
DIABETIC CATARACT
-
8/14/2019 Approach to Dm Pt.
41/71
Investigations for Diabetes MellitusInvestigations for Diabetes Mellitus
Glucose can be estimated chemically and enzymatically. If the fasting blood glucose valueGlucose can be estimated chemically and enzymatically. If the fasting blood glucose value
is more than 126 mg/dl or the random blood glucose value is more than 200 mg/dl, thenis more than 126 mg/dl or the random blood glucose value is more than 200 mg/dl, thenit is considered to be a case of diabetes.it is considered to be a case of diabetes.
Glucose Tolernce Test: (GTT)Glucose Tolernce Test: (GTT)
This test is used to measure the glucose tolerance in a person. The blood is drawn atThis test is used to measure the glucose tolerance in a person. The blood is drawn atintervals of 30 mins each. The first sample is fasting, at 30 mins, 60 min, 120 mins andintervals of 30 mins each. The first sample is fasting, at 30 mins, 60 min, 120 mins and180 mins. In all five samples are collected.180 mins. In all five samples are collected.
The most important role of GTT is to help in the investigation of symptomless glycosuria.The most important role of GTT is to help in the investigation of symptomless glycosuria.
Glycosylated HaemoglobinGlycosylated Haemoglobin
Of all the glycated forms of Hb, HbA1c is the most stable. More than 80 per cent of theOf all the glycated forms of Hb, HbA1c is the most stable. More than 80 per cent of theglycated form is the HbA1c. Hence, its measurement is taken to be the ideal parameterglycated form is the HbA1c. Hence, its measurement is taken to be the ideal parameterto understand the Long term diabetic control. This is the most important tool forto understand the Long term diabetic control. This is the most important tool formonitoring diabetes. This test refers to the hemoglobin component formed by interactionmonitoring diabetes. This test refers to the hemoglobin component formed by interaction
with glucose, since half life of RBCs is approximately 120 days; a single HbA1cwith glucose, since half life of RBCs is approximately 120 days; a single HbA1cdetermination can give information about glycemic control in the preceding 8-12 weeks.determination can give information about glycemic control in the preceding 8-12 weeks.
It is estimated by HPLC method, which is considered to be gold standard. The advantage isIt is estimated by HPLC method, which is considered to be gold standard. The advantage isthat this test does not require any dietary preparations, has low sensitivity but highthat this test does not require any dietary preparations, has low sensitivity but highspecificity compared to oral glucose tolerance test.specificity compared to oral glucose tolerance test.
-
8/14/2019 Approach to Dm Pt.
42/71
Microalbumin (MAU)Microalbumin (MAU)
MAU as the name suggests, is the first warning signal to an impendingMAU as the name suggests, is the first warning signal to an impending
Nephropathy - if attention is not paid to keep diabetes under control. Patients withNephropathy - if attention is not paid to keep diabetes under control. Patients with
microalbuminuria have a greater risk for developing renal failure, vascular damagemicroalbuminuria have a greater risk for developing renal failure, vascular damageand risk for cardiovascular damage. It can be estimated by immunoturbidometry andand risk for cardiovascular damage. It can be estimated by immunoturbidometry and
nephelometry:nephelometry:
InsulinInsulin
This test is used for determination of concentration of bioavailable insulin in theThis test is used for determination of concentration of bioavailable insulin in the
patients. Total insulin exists in free and bound form. In patients without insulinpatients. Total insulin exists in free and bound form. In patients without insulinantibodies, total and free levels are similar, but in patients with insulin antibodiesantibodies, total and free levels are similar, but in patients with insulin antibodies
total insulin levels are dependant on the binding capacity of the circulatingtotal insulin levels are dependant on the binding capacity of the circulating
endogenous insulin antibody and availability of insulin to bind to antibody sites. Thisendogenous insulin antibody and availability of insulin to bind to antibody sites. This
test is used to determine dosage of IDDM with insulin antibodies.test is used to determine dosage of IDDM with insulin antibodies.
Insulin AntibodiesInsulin Antibodies
Most common antibodies are IgG, IgM, IgA & IgE Abs have been reported. TheseMost common antibodies are IgG, IgM, IgA & IgE Abs have been reported. These
antibodies are generally seen in pre-Type I DM as well as DM pts with exogenousantibodies are generally seen in pre-Type I DM as well as DM pts with exogenous
bovine or human porcine insulin.bovine or human porcine insulin.
Free InsulinFree Insulin
-
8/14/2019 Approach to Dm Pt.
43/71
Free InsulinFree Insulin
Increased levels of free insulin are seen:Increased levels of free insulin are seen:
Exogenous insulinExogenous insulin
InsulinomaInsulinoma
Insulin resistanceInsulin resistance
Type II DM.Type II DM.
ProinsulinProinsulin
Proinsulin is produced in beta cells of pancreas and cleaved into insulin and C-peptideProinsulin is produced in beta cells of pancreas and cleaved into insulin and C-peptide
before release into circulation.before release into circulation.
Increased levels are seen inIncreased levels are seen in
InsulinomasInsulinomasSevere hypoglycemic hypoinsulinomasSevere hypoglycemic hypoinsulinomas
Hyperproinsulinemia.Hyperproinsulinemia.
Proinsulin inhibits hepatic production of glucose thus useful in type II DM.TG & HDLProinsulin inhibits hepatic production of glucose thus useful in type II DM.TG & HDL
concentrations improve with proinsulinconcentrations improve with proinsulin
GAD AntibodiesGAD Antibodies
GAD-65 Antibodies: GAD is known as Glutamic Acid Decarboxylase. They are detectedGAD-65 Antibodies: GAD is known as Glutamic Acid Decarboxylase. They are detectedin approximately 90 per cent of patients who are newly diagnosed of Type I DM and 80in approximately 90 per cent of patients who are newly diagnosed of Type I DM and 80
per cent of pre-diabetic individuals and first degree relative of patients with IDDM.per cent of pre-diabetic individuals and first degree relative of patients with IDDM.
C-PeptideC-Peptide
C-peptide is cleaved from proinsulin and released into circulation in the course of insulinC-peptide is cleaved from proinsulin and released into circulation in the course of insulin
biosynthesis. C-peptide is used for assessment of pancreatic islet cell function.biosynthesis. C-peptide is used for assessment of pancreatic islet cell function.
-
8/14/2019 Approach to Dm Pt.
44/71
Testing :Testing :
Fasting Plasma Glucose Test
(FPG) - (cheap, fast)
*fasting B.G.L. 100-125 mg/dl
signals pre-diabetes
*>126 mg/dl signals diabetes
Oral Glucose Tolerance Test
(OGTT)
*tested for 2 hrs after
glucose-
rich drink
*140-199 mg/dl signals pre-
diabetes
*>200 mg/dl signals diabetes
80 to 90 mg per 100 ml, is the normal fasting blood glucose
concentration in humans and most mammals which is
associated with very low levels of insulin secretion.
A.K.A.: Glycated Hemoglobin tests
A1C
-
8/14/2019 Approach to Dm Pt.
45/71
Triad of TreatmentTriad of Treatment
DietDiet
MedicationMedication
Oral hypoglycemicsOral hypoglycemics
InsulinsInsulins
ExerciseExercise
-
8/14/2019 Approach to Dm Pt.
46/71
Diabetes treatmentDiabetes treatment
ExerciseExercise Under physician supervisionUnder physician supervision Check glucose priorCheck glucose prior
DietDiet Lower calorieLower calorie
Fewer foods of high glycemic indexFewer foods of high glycemic index
Spread meals evenlySpread meals evenly
-
8/14/2019 Approach to Dm Pt.
47/71
Diabetes Oral MedicationsDiabetes Oral Medications
SulfonylureasSulfonylureas
BiguanidesBiguanides Sulfonylureas and biguanide combinationSulfonylureas and biguanide combination
drugsdrugs
ThiazolidinedionesThiazolidinediones
Alpha-glycosidase inhibitorsAlpha-glycosidase inhibitors
MeglitinidesMeglitinides
6 Classes :
-
8/14/2019 Approach to Dm Pt.
48/71
SulfonylureasSulfonylureas
Stimulate pancreas to secrete insulinStimulate pancreas to secrete insulin Glyburide (Diabeta) [Prototype Pro p 393]Glyburide (Diabeta) [Prototype Pro p 393] Diabenese (chlorpropamide)Diabenese (chlorpropamide)
Glucotrol (Glipizide), Gliclazide, GlibenclamideGlucotrol (Glipizide), Gliclazide, Glibenclamide
Mechanism of ActionMechanism of Action Sulfonylureas interact with receptors on pancreaticSulfonylureas interact with receptors on pancreatic -cells to block-cells to block
ATP-sensitive potassium channelsATP-sensitive potassium channels
This, in turn, leads to opening of calcium channelsThis, in turn, leads to opening of calcium channels
Which leads to the production of insulinWhich leads to the production of insulin
Adverse reactionsAdverse reactions HypoglycemiaHypoglycemia
Water retention/edemaWater retention/edema
PhotosensitivityPhotosensitivity
-
8/14/2019 Approach to Dm Pt.
49/71
BiguanidesBiguanides
Decreases liver production of glucoseDecreases liver production of glucose
Decreases intestinal absorption of glucoseDecreases intestinal absorption of glucose
Improves cell sensitivity to insulinImproves cell sensitivity to insulin
Example: MetforminExample: Metformin
GI upset, flatulenceGI upset, flatulence Cardiac (CHF, MI)Cardiac (CHF, MI)
-
8/14/2019 Approach to Dm Pt.
50/71
ThiazolidinedionesThiazolidinediones
Increase cellular sensitivity to insulinIncrease cellular sensitivity to insulin Pioglitazone (Actos)Pioglitazone (Actos)
Rosiglitazone (Avandia)Rosiglitazone (Avandia)
Patient should have liver enzymesPatient should have liver enzymes
checked periodicallychecked periodically
-
8/14/2019 Approach to Dm Pt.
51/71
D-PhenylalanineD-Phenylalaninederivativesderivatives
Nateglinide (Starlix)Nateglinide (Starlix)
Rapid onset, short half-lifeRapid onset, short half-life Good for those with rapid post prandial rise inGood for those with rapid post prandial rise in
blood glucoseblood glucose
-
8/14/2019 Approach to Dm Pt.
52/71
CombinationsCombinations
GlucovanceGlucovance Glyburide and MetforminGlyburide and Metformin
AvandametAvandamet Avandia and MetforminAvandia and Metformin
-
8/14/2019 Approach to Dm Pt.
53/71
lpha glycosidase inhibitorslpha glycosidase inhibitorsBlock enzymes that help digest starchesBlock enzymes that help digest starches slowing theslowing the
rise in B.G.L.rise in B.G.L.
MeglitinidesMeglitinidesStimulate more insulin production ;Stimulate more insulin production ;
dependant upon level of glucose presentdependant upon level of glucose present
- Precose (acarbose),
- Glyset (miglitol)
- Prandin (repaglinide)
- Starlix (nateglinide)
I liInsulin
-
8/14/2019 Approach to Dm Pt.
54/71
InsulinInsulin
Made inMade in betabeta cells of the pancreascells of the pancreas
Moves glucose into cells (thus actsMoves glucose into cells (thus actslike growth hormone in a way)like growth hormone in a way)
Moves potassium into cells (canMoves potassium into cells (canbuy time in emergencies)buy time in emergencies)
Who need insulin medicineWho need insulin medicine Type I diabetes patients whoseType I diabetes patients whose
body produces no insulin.body produces no insulin. Type 2 diabetes patients that doType 2 diabetes patients that do
not always produce enoughnot always produce enoughinsulin.insulin.
Treatment
subcutaneous injection
http://images.google.co.in/imgres?imgurl=http://www.petinsurance.com/healthzone/pet-articles/pet-health/~/media/All%2520PHZ%2520Images/Article%2520images/123diabetessyringe.ashx&imgrefurl=http://www.petinsurance.com/healthzone/pet-articles/pet-health/Pets-With-Diabetes.aspx&usg=__HO2luWsQjuesA8wOap84KfHouWk=&h=424&w=283&sz=123&hl=en&start=21&tbnid=477UpwIWHIcoiM:&tbnh=126&tbnw=84&prev=/images%3Fq%3Ddiet%2Bfor%2Bdiabetes%2Bmellitus%26gbv%3D2%26ndsp%3D20%26hl%3Den%26sa%3DN%26start%3D20 -
8/14/2019 Approach to Dm Pt.
55/71
Stage 1 Insulin was extracted from the glands ofcows and pigs. (1920s)
Stage 2 Convert pig insulin into human insulin byremoving the one amino acid that distinguishes themand replacing it with the human version.
Insulin drug evolution
-
8/14/2019 Approach to Dm Pt.
56/71
Stage 3Stage 3
Insert the humanInsert the human
insulininsulin gene into E. coli andgene into E. coli andcultureculture thethe recombinantrecombinantE.coliE.colito produce insulinto produce insulin (trade name(trade name= Humulin= Humulin). Yeast is also). Yeast is alsousedused to produce insulinto produce insulin (trade(tradename = Novolinname = Novolin) (1987).) (1987).
Recombinant DNA technology has also made it possible tomanufacture slightly-modified forms of human insulin thatwork faster (Humalog and NovoLog) or slower(Lantus) than regular human insulin.
-
8/14/2019 Approach to Dm Pt.
57/71
Types of insulin
Regular insulins
Insulin analogs
Pre-mixed insulin
Short peptide mimics
SITES OF INJECTION
-
8/14/2019 Approach to Dm Pt.
58/71
Regular insulins:Regular insulins:
Human insulinHuman insulin: Humulin: Humulin(from E.coli),(from E.coli),
NovalinNovalin(from yeast)(from yeast)
NPHNPH - neutral protamine Hagedorn (NPH),- neutral protamine Hagedorn (NPH),protamine mixed.protamine mixed.
Lente insulin / Ultralente insullinLente insulin / Ultralente insullin--
zinczincaddedadded
-
8/14/2019 Approach to Dm Pt.
59/71
Insulin Analogs:Insulin Analogs:
Fatty Acid Acylated insulinsFatty Acid Acylated insulins
Insulin Lispro (Humalog) (1996)Insulin Lispro (Humalog) (1996)
Insulin Aspart (NovoLog) (2000)Insulin Aspart (NovoLog) (2000)
Insulin Glargine (Lantus) (2002)Insulin Glargine (Lantus) (2002)
Insulin Detemir (Levemir) (Jun.,2005)Insulin Detemir (Levemir) (Jun.,2005)
Insulin Glulisine (Apidra) (Jan., 2006)Insulin Glulisine (Apidra) (Jan., 2006)
I li tiI li ti
-
8/14/2019 Approach to Dm Pt.
60/71
Insulin preparationsInsulin preparationsgiven ONLY with syringes marked in unitsgiven ONLY with syringes marked in units
Rapid actingRapid acting (lispro,(lispro,
asparte)asparte)
Short actingShort acting (regular)(regular) Intermediate actingIntermediate acting
(NPH)(NPH)
Long actingLong acting UltralenteUltralente
[Glargine/Lantus][Glargine/Lantus]
-
8/14/2019 Approach to Dm Pt.
61/71
Rapid acting insulinRapid acting insulin
Lispro (Lispro (Humolog,Humolog, Novolog Aspart)Novolog Aspart) Onset of actionOnset of action
15-30 minutes [may come on in 5 minutes]15-30 minutes [may come on in 5 minutes]
Peak of actionPeak of action
1 - 2 hours1 - 2 hours
DurationDuration
3 4 hours3 4 hours
-
8/14/2019 Approach to Dm Pt.
62/71
Short acting insulinsShort acting insulins
Regular (clear so can be given IV)Regular (clear so can be given IV) Onset of actionOnset of action
0.5 to 1 hour0.5 to 1 hour
Peak of actionPeak of action
2 4 hours2 4 hours
Duration of actionDuration of action
6 8 hours6 8 hours
-
8/14/2019 Approach to Dm Pt.
63/71
Intermediate acting insulinsIntermediate acting insulins
NPHNPH, Lente (chemicals added. Cloudy), Lente (chemicals added. Cloudy) Onset of actionOnset of action
1 4 hours1 4 hours
Peak of actionPeak of action
4 12 hours4 12 hours
Duration of actionDuration of action
18 24 hours18 24 hours
-
8/14/2019 Approach to Dm Pt.
64/71
Long acting insulinsLong acting insulins
UltralenteUltralente Onset of actionOnset of action
4 8 hours4 8 hours
Peak of actionPeak of action
18 hours18 hours
Duration of actionDuration of action
24 36 hours24 36 hours
-
8/14/2019 Approach to Dm Pt.
65/71
Once a day insulinOnce a day insulin
Glargine/LantusGlargine/Lantus Cannot be diluted or mixed in syringe with anyCannot be diluted or mixed in syringe with any
other insulinother insulin
Slow, steady releaseSlow, steady release Daily dosing [usually at bedtime]Daily dosing [usually at bedtime]
Refrigerated or tosses every 14 daysRefrigerated or tosses every 14 days
-
8/14/2019 Approach to Dm Pt.
66/71
Combination insulinsCombination insulins
70/30 (70% NPH and 30% regular)70/30 (70% NPH and 30% regular)
Humolog 70/30 (Humolog and regular)Humolog 70/30 (Humolog and regular)
Fewer injectionsFewer injections
Rotate sites to decreaseRotate sites to decrease lipodystrophylipodystrophy
-
8/14/2019 Approach to Dm Pt.
67/71
MiscellaneousMiscellaneous
ByettaByetta for type II Diabetics takingfor type II Diabetics taking
sulfonylureas or combinationsulfonylureas or combination Mimics physiologic glucose controlMimics physiologic glucose control
Inhances insulin secretion only in presence ofInhances insulin secretion only in presence ofhyperglycemiahyperglycemia
Insulin secretion decreases as blood glucoseInsulin secretion decreases as blood glucose
approaches normalapproaches normal
NeutontinNeutontin for Diabetic nerve painfor Diabetic nerve pain
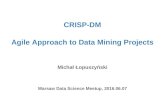
Amino Acid Substitutons
-
8/14/2019 Approach to Dm Pt.
68/71
Myristicacid
LysDetemir
ArgThrLysProGlyGlargine
ThrGluProLysAsnGlulisin
e
ThrProLysAsnLispro
ThrLysAspartic
acid
AsnAspart
ThrLysProAsnAsnHuman
B31AndB32
B30B29B28B3A21Source/Type
B- chain PositionA-chain
Position
Amino Acid Substitutons
rapid-acting
long-acting
-
8/14/2019 Approach to Dm Pt.
69/71
-
8/14/2019 Approach to Dm Pt.
70/71
Dawn Phenomenon vs Somogyis effectDawn Phenomenon vs Somogyis effect Dawn phenomenonDawn phenomenon
Blood sugar rises in early morningBlood sugar rises in early morning
Somogyis (rebound) effectSomogyis (rebound) effect
Blood sugar rise in morning as reaction toBlood sugar rise in morning as reaction tohypoglycemic episode due tohypoglycemic episode due to
counterregulatory hormone release.counterregulatory hormone release.
-
8/14/2019 Approach to Dm Pt.
71/71