Type I Diabetes Prevention Ronen Gurfinkel, PGY5 April 3, 2013.
Approach to Acute Respiratory Problems
Royal Victoria HospitalStéphane Beaudoin
Respirology Resident
PGY5

Objectives
To help residents develop an effective approach to the evaluation of dyspnea and hypoxia
To help residents become more familiar with the management of common acute respiratory emergencies
– Acute severe asthma– Massive hemoptysis– Pneumothorax

Approach to Dyspnea: some Pearls
Dyspnea is a complex subjective sensation Dyspnea ≠ tachypnea Dyspnea ≠ hypoxemia
Dyspnea must be differentiated from Pain Fatigue Weakness, deconditioning
Hence, a complaint of dyspnea must be qualified and quantified Departure from baseline and progression in time Specific impairments Use of a standardized scale: MRC, NYHA
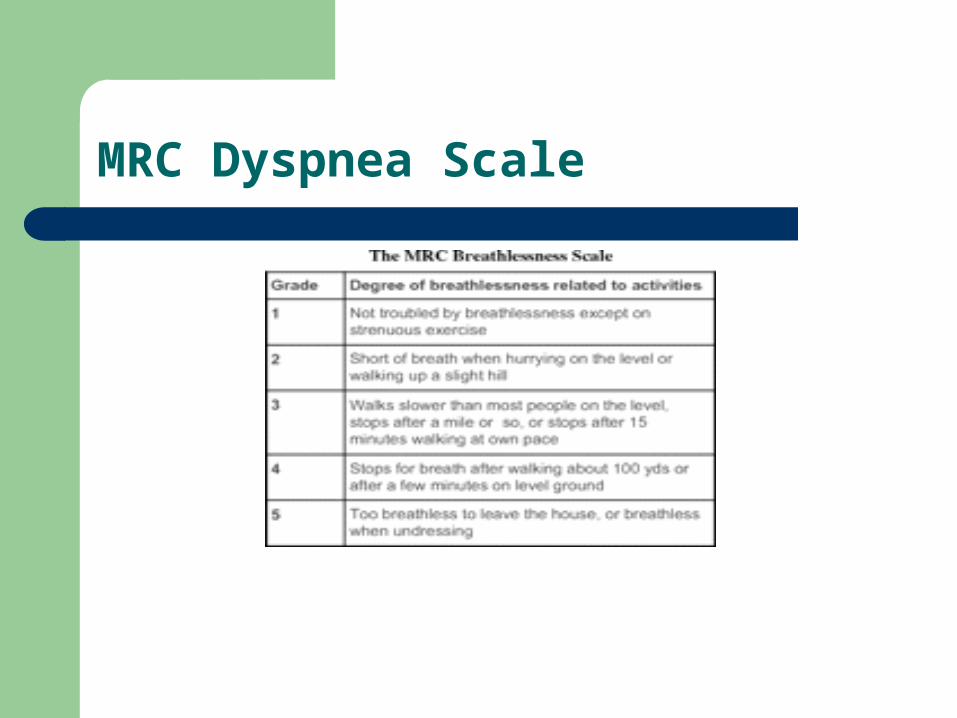
MRC Dyspnea Scale

Combined Approach to Dyspnea
– Respiratory
– Upper airways• Anaphylaxis / Foreign body / tumor• Vocal cord dysfunction
– Lower airways• Anaphylaxis / Foreign body / tumor• Bronchospasm / exacerbation of obtructive lung disease / toxic inhalation / infection
– Chest wall / Pleura• Effusion / tumor / PTx
– Parenchyma• Infectious, inflammatory, neoplastic disorder / CHF
– Vasculature• PE, chronic pulmonary HTN
Cardiovascular
– CHF, arrhythmia, effusion/tamponade, valvvular dysfunction– Shock
Metabolic
– Anemia / metabolic acidosis / intoxications
Other
– Pregnancy– Pain, anxiety– Hyperventilation– Neuromuscular disorders
The 6 Causes of Hypoxemia
Low O2 content of inspired gas High altitude
V/Q mismatch Alveolar filling or airway obstruction or vascular anomalies
Shunt Pulmonary (AVM, lobar / lung collapse) or extra-pulmonary (PFO)
Hypoventilation Central, neuromuscular, myopathic, obesity, chronic lung disease
Low DLCO Interstitial lung disease, Pulm HTN
Low Mixed Venous O2 sat % Shock / low output state
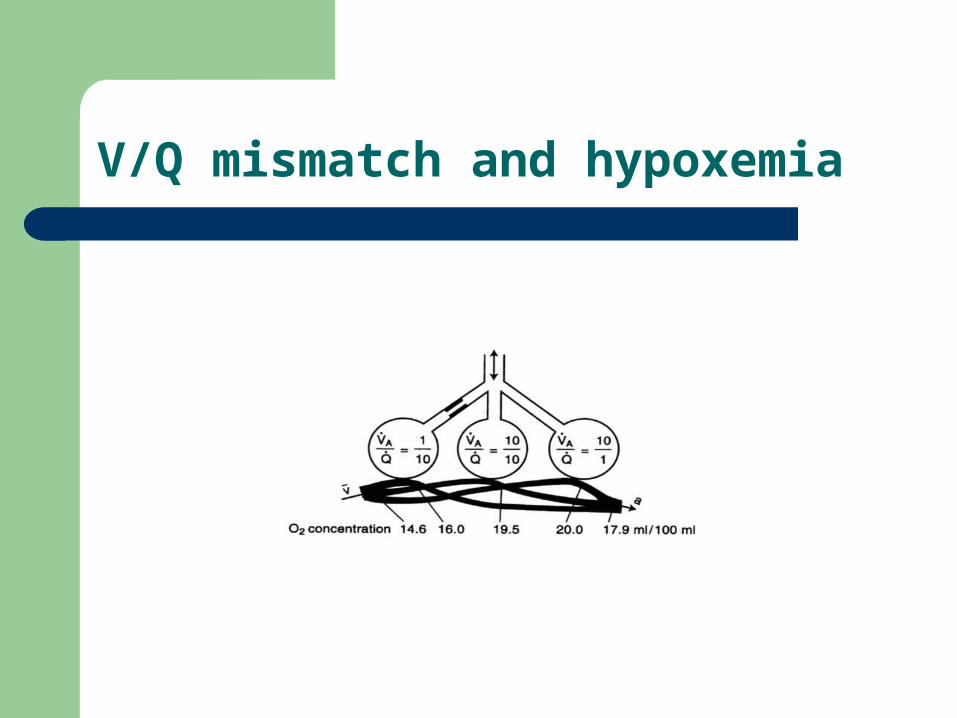
V/Q mismatch and hypoxemia
The A-a Gradient
The efficiency of gas exchange can be assessed by comparing the measured arterial oxygen pressure (PaO2, via ABG) to the hypothesized ideal or maximal alveolar oxygen pressure
A-a gradient = PAO2- PaO2
PAO2 = [FiO2 x (Patm- PH20)] – (PACO2 / RQ)
Under conditions of normal gas exchange (no V/Q anomalies / minimal shunt and normal DLCO), the difference between those is small
A normal A-a gradient in the face of hypoxemia narrows the differential to:– Low inspired O2 content
– Hypoventilation
Limitations– Normal or expected A-a gradient varies with age:
A-a gradient = 2.5 + (0.21 x age)
– FiO2, RQ, PH2O are imprecise in most clinical situations and the full equation is actually more complex
– At high FiO2, the expected A-a gradient increases, but the exact magnitude is difficult to establish ( hence less reliable when high FiO2 used)
Approach to Hypoxemia
ABC’s, iv access, O2, monitoring– Airway difficulty assessment
Clinical assessment– Relevant history– Meticulous physical exam
CXR
ABG for pCO2 and A-a gradient

Acute Severe Asthma

Acute Severe Asthma
Predictors of a life-threatening attack– Prior ICU stay or intubation / ≥ 2 hospitalizations or > 3 ER visits in past year– Poor perception of symptoms by pt– Frequent use of relief bronchodilators– Low SES / Psychiatric illness, drug use– Cardiovascular or respiratory comorbidities
“All that wheezes is not asthma”!– DDx
CHF / bronchiolitis / toxic inhalation Foreign body aspiration / tumor / anaphylaxis PE, pneumonia, PTx Vocal cord dysfunction Hyperventilation
Flow rates are absolutely required for diagnosis and are the best method to follow the evolution of an attack
Acute Asthma
ABC’s, iv, O2, monitoring– Airway difficulty assessment
Clinical Assessment– Markers of severity
Silent chest Pulsus paradoxus Hypoxemia / hypercapnia (beware of normocapnea) RR > 25-30 / HR >110 / inability to speak FEV1 < 30% predicted
CXR is of low yield (done to exclude complications or alternative diagnoses)
Flow rates are absolutely required for diagnosis and are the best method to follow the evolution of an attack
– ABG should be done if hypoxemia is present, in cases of severe distress, or if admission is contemplated
Acute Asthma: Management
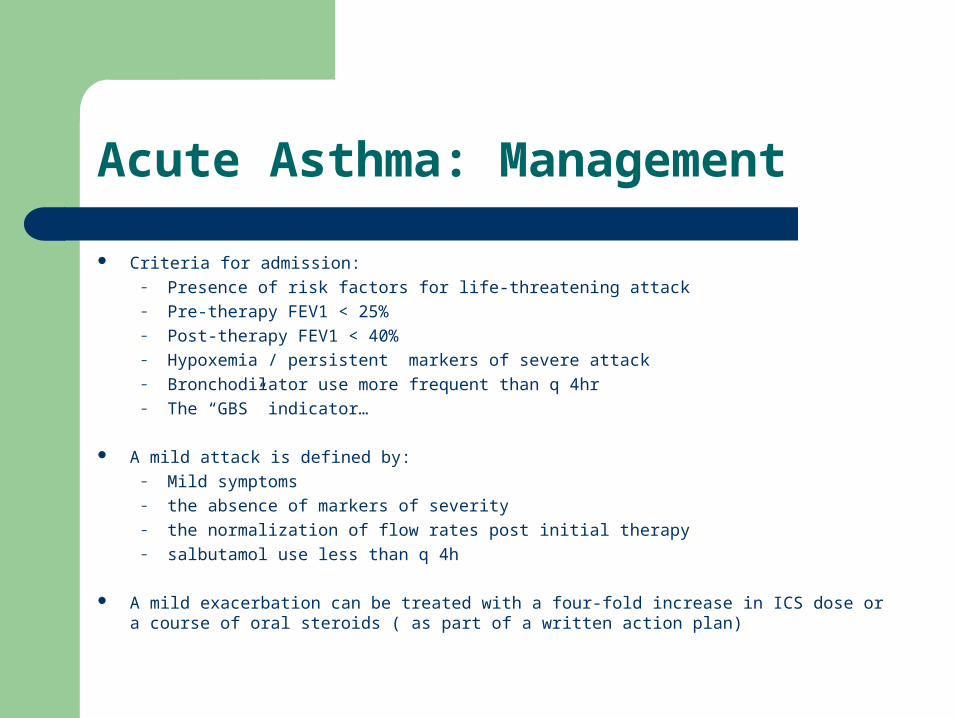
Criteria for admission:– Presence of risk factors for life-threatening attack– Pre-therapy FEV1 < 25%– Post-therapy FEV1 < 40%– Hypoxemia / persistent markers of severe attack– Bronchodilator use more frequent than q 4hr– The “GBS” indicator…
A mild attack is defined by:– Mild symptoms– the absence of markers of severity– the normalization of flow rates post initial therapy– salbutamol use less than q 4h
A mild exacerbation can be treated with a four-fold increase in ICS dose or a course of oral steroids ( as part of a written action plan)

Acute Asthma: Management
Bronchodilators: MDI with spacer as effective as nebulized…– Salbutamol
MDI: 4-8 puffs q 20 min then q 1h Neb: 2.5-5 mg q 20 min then q 1h
– Ipratropium: provides an added bronchodilator effect acutely MDI: 4-8 puffs q 20 min then q 1h Neb: 500 mcg q 20 min then q1 h
Corticosteroids: dosing is controversial, but 40-60 mg likely sufficient– Route: po is equivalent to iv and is preferred unless pt is vomiting– Duration: 7-14 days, no taper– Need for higher iv doses in ICU pts is not clear
Magnesium sulfate– May provide a modest additional bronchodilation, but its impact on outcome is not clear– Most effective in severe airflow limitation, if response to bronchodilators is poor
Methylxanthines have no role in acute setting
The use of Heliox is controversial
Acute Asthma: Management
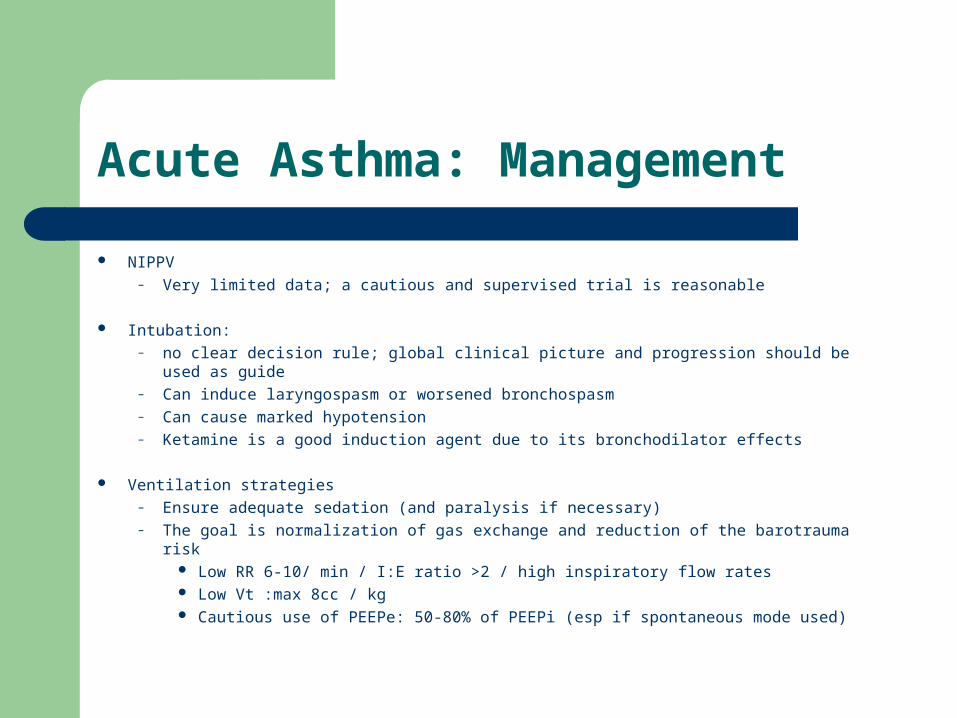
NIPPV– Very limited data; a cautious and supervised trial is reasonable
Intubation: – no clear decision rule; global clinical picture and progression should be used as guide– Can induce laryngospasm or worsened bronchospasm– Can cause marked hypotension– Ketamine is a good induction agent due to its bronchodilator effects
Ventilation strategies– Ensure adequate sedation (and paralysis if necessary)– The goal is normalization of gas exchange and reduction of the barotrauma risk
Low RR 6-10/ min / I:E ratio >2 / high inspiratory flow rates Low Vt :max 8cc / kg Cautious use of PEEPe: 50-80% of PEEPi (esp if spontaneous mode used)

The 5 Commandments of Asthma
Identify and address potential triggering factors– URTI, non-compliance, smoking, irritant exposure, allergies, NSAIDS,
beta-blockers
Review and optimize puffer technique
Prescribe ICS to all pts
Educate pt about his illness
Vaccinate for Influenza at least

Massive Hemoptysis

A case
62 F known for some “chronic lung disease”
Presented with ~ 180 cc of fresh hemoptysis over 1.5 day, in context of purulent secretions and worsened dyspnea (MRC 2→3)
Massive Hemoptysis
Massive Hemoptysis

Massive Hemoptysis
Definition is controversial: 100 cc/24h to 1,000 cc/24h– Rate of bleeding should also be considered– Consequences such as hypoxemia, need for admission / intubation should
also be considered
Only 5-15% of all hemoptysis cases are considered massive
Mortality is significant– Up to 38% in recent studies
Significant epistaxis and UGI bleed must first be excluded
The importance of the little cup…

Massive Hemoptysis
Etiology: relative frequencies vary considerably based on center/population– Most common causes:
Bronchiectasis TB Mycetoma Lung Malignancy Diffuse alveolar hemorrhage (hemoptysis can be minimal) Idiopathic Others
Anatomic origin– Bronchial arteries → 90%– Non-bronchial arteries → 5 %– Pulmonary vessels → 5 %

Massive Hemoptysis
Management Goals:– Stabilize the respiratory and hemodynamic status– Identify the site of bleeding– Identify the cause of bleeding– Treat the underlying cause and / or perform active procedures to
abort bleeding
In palliative situations:– Relieve anxiety, dyspnea, psychological distress
Green surgical towels and morphine iv

Massive Hemoptysis
ABC’s, iv access, O2, monitoring– ICU admission– Correct coagulopathy and hemodynamics– X-match and keep units in reserve
Focused Hx and physical exam
CXR / CT with angio protocol (aortogram)
Bronchoscopy: goal is localization of bleeding– Timing is controversial– Bronchoscopic interventions are temporizing at best
Massive Hemoptysis: Management
Supportive care is crucial
Bleeding side down (lateral decubitus)
Intubation required if resp failure is present or if very large amount of blood expectorated
– Largest ETT possible– Seek help for selective intubation with either single or double-lumen tube (if
bleeding side known)– Otherwise immediate bronchoscopy for localization and airway clearance
First line definitive procedure is Bronchial Artery Embolization– Surgery now reserved for refractory cases despite multiple embolizations,
trauma, PA rupture, mycetoma
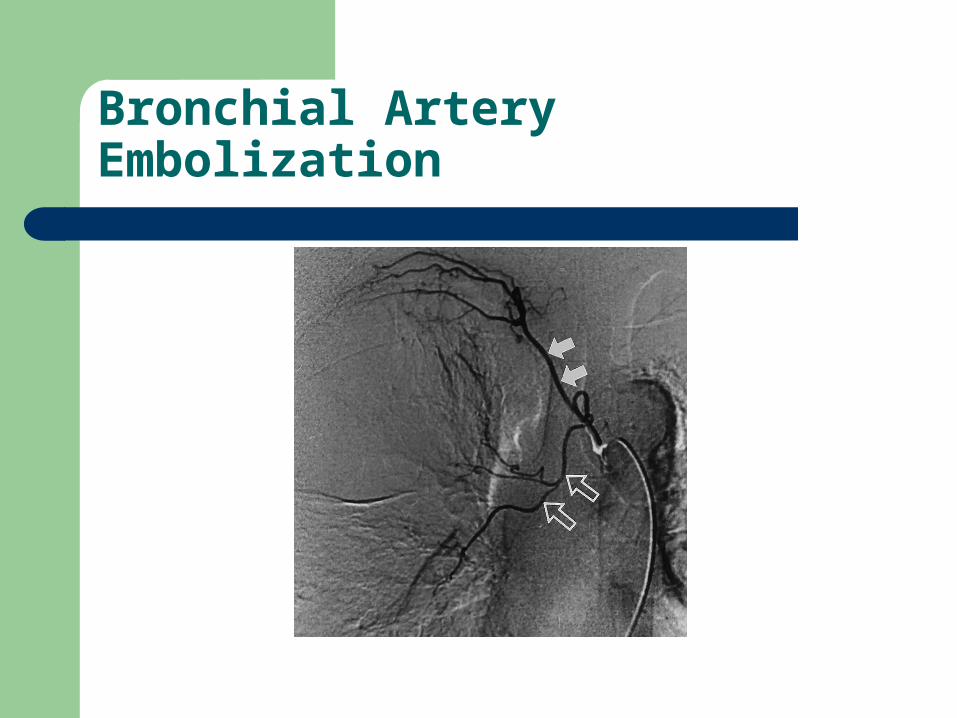
Bronchial Artery Embolization
Massive Hemoptysis: Special Case
83 M 3 hrs post CABG x 3, MAZE, redo MVR, TV ring annuloplasty
Called for large amount of fresh blood coming from ETT– What is the cause?– What should be done?

Pneumothorax

18 M with chest pain and mild dyspnea for 1 week
Review of Physiology
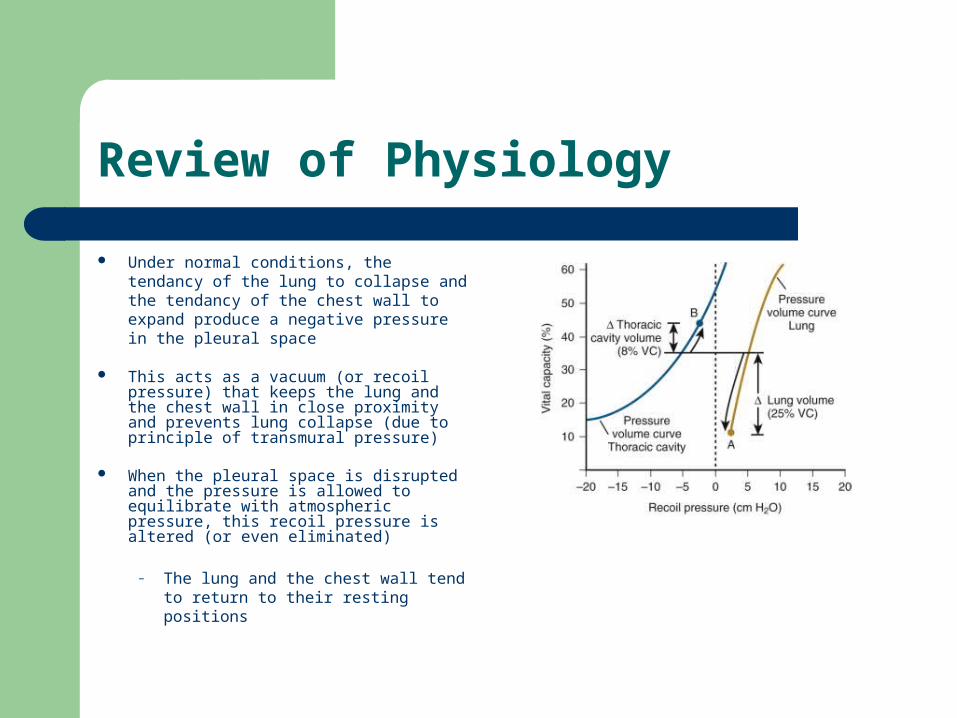
Under normal conditions, the tendancy of the lung to collapse and the tendancy of the chest wall to expand produce a negative pressure in the pleural space
This acts as a vacuum (or recoil pressure) that keeps the lung and the chest wall in close proximity and prevents lung collapse (due to principle of transmural pressure)
When the pleural space is disrupted and the pressure is allowed to equilibrate with atmospheric pressure, this recoil pressure is altered (or even eliminated)
– The lung and the chest wall tend to return to their resting positions

Classification
Spontaneous Primary PTx: in a patient without apparent underlying pulmonary disease
Thought to be caused by the rupture of an air-containing space within or in vicinity to the visceral pleura, usually at the apex
Although patients have no apparent underlying lung disease, up to 80% have blebs or bullae on CT examination
Male sex, smoking, tall stature, and genetics are risk factors Recurrence rate of 39% in ipsilateral lung and 15% in contralateral lung
Spontaneous Secondary PTx: in a patient with underlying pulmonary disease
Almost any lung condition can be associated with the development of a PTx COPD is by far the most common etiology nowadays Although the exact mechanism varies, the principles underlying the development of primary
PTx are likely also playing a role (exacerbated by airway/parenchymal inflammation and architecture disruption)
Recurrence rates are usually higher and depend on the underlying etiology
Traumatic Pneumothorax(including iatrogenic)
Pneumothorax: Clinical Features
History:– Acute onset of pleuritic chest pain, usually at rest, +/- dyspnea– Symptoms can be out of proportion to the extent of lung collapse, especially in
secondary pneumothorax where the reserve is limited– Trauma (even blunt) to exclude
Physical Exam:– Hypoxemia
Severe hypoxemia due to shunting rare in primary PTx ≤25%– Major alterations in vitals usually only seen in tension PTx– Hyperexpanded hemithorax with ↑resonance, yet ↓excursion, ↓ vesicular sounds and
fremitus
– Contralateral tracheal deviation; s/c emphysema– Hamman sign: clicking/crunching sounds with heart beats influenced by position and
respiration
Tension Pneumothorax
Tension PTx is a clinical diagnosis
– Evidence of sudden deterioration in a patient known to have a PTx or highly suspected of having one should prompt initiation of therapy
severe hypoxemia, tachycardia, contralateral tracheal shift, ↑ JVP, shock
– Radiologic signs are not specific
– Caused by a one-way valve phenomenon producing a positive pleural pressure during most of the resp cycle
Main consequence is reduction of venous return/ cardiac output
Treatment consists of oxygen administration and immediate needle aspiration in 2nd ICS at mid-clavicular line and insertion of a chest tube

Radiological Diagnosis
A standard erect PA CXR is sufficient– Expiratory views are only marginally more sensitive and are not recommended for routine use
A sharply demarcated white pleural line without lung markings lateral to it is diagnostic– Mimickers: skin fold, tubings, ribs – Use of expiratory views /lateral decubitus views if unclear– A pleural effusion is present in up to15-25% of cases (usually an eosinophilic pleuritis in reaction to
the presence of air; rarely hemorrhagic)
Supine patients– Deep sulcus sign / upper quadrant lucency / ↑sharpness of cardiac border or hemidiaphragm
CT scan recommended only if:– Diagnosis suspected despite normal CXR– To better define underlying disorder

Pneumothorax in a supine patient

Pneumothorax Size Estimation
Several quantification/measurement methods exist, and none is perfect
– Most show good correlation, but poor agreement– Standard is measurement by CT volumetrics
Size estimation methods– Light Index
% PTX = 1 – (lung diamater3/hemithorax diameter3)– Rhea Method
% PTx determined by plotting the average of 3 interpleural distances on a nomogram
– Collins Method% PTX = 4.2 + [4.7 x ( sum of interpleural distances)]

Pneumothorax Size Estimation
Measurement methods proposed by the BTS and ACCP to classify PTx as small/ large
– ACCP: large defined as ≥ 3cm apex to cupola
– BTS: large defined as > 2cm lung to chest wall at hilar level
From MacDuff et al.Management of spontaneous pneumothorax: BritishThoracic Society pleural disease guideline 2010. Thorax 2010;65(Suppl 2):ii18eii31. figure 1
Management
Good quality evidence to guide clinical decision making is lacking
Data from available evidence difficult to compare due to the use of:– Different measurement methods– Different definitions/ decision thresholds
Guidelines produced by the BTS and the ACCP as well as recommendations from major textbooks differ in many apsects and are largely based on expert consensus
Nevertheless, there has been a shift towards more conservative initial treatment and reliance on patient’s status rather than PTx size
In general, treatment is more aggressive in secondary PTx cases

Management: Initial Therapy
All sources agree that asymptomatic patients with small PTx (primary or secondary) should be managed conservatively and observed
– The exact observation period and the follow up schedule is not well-established ( the ACCP recommends 3-6hrs of observation and f/u CXR the next day)
Unless contraindicated, all patients should receive high concentration oxygen therapy
– Can lead to a 4-fold increase in the reabsorption rate
Smoking cessation is of crucial importance
Question
How long does it take for a 25% PTx to resolve?
The reabsorption rate varies from 1.25-2.2% of a hemithorax volume per day
– Hence it would take 12-13 d to resolve completely!
Management of Primary PTx
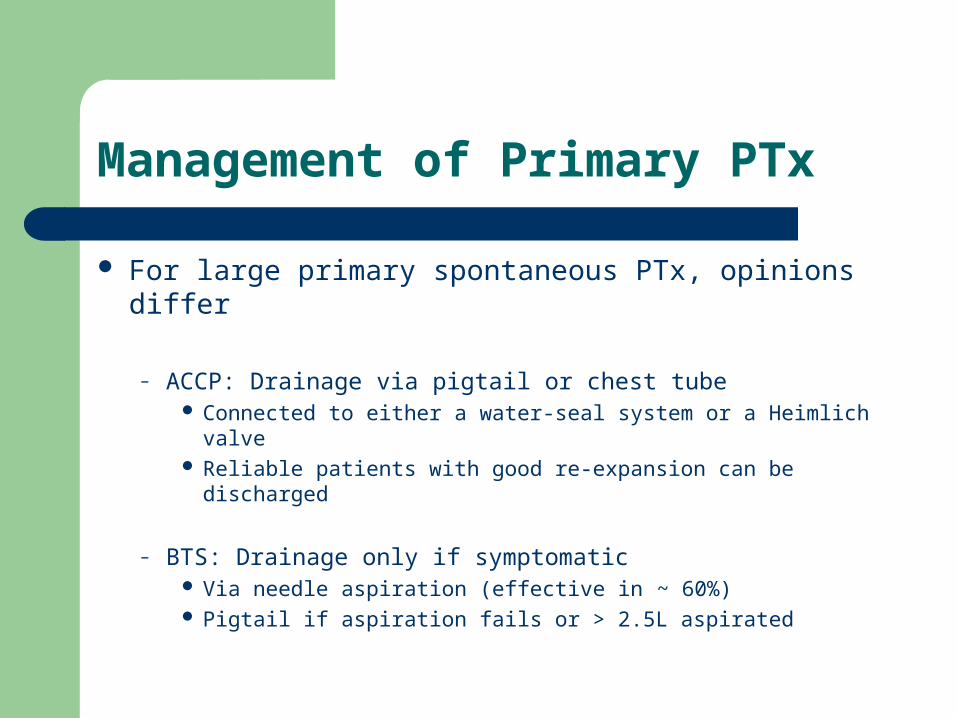
For large primary spontaneous PTx, opinions differ
– ACCP: Drainage via pigtail or chest tube Connected to either a water-seal system or a Heimlich valve Reliable patients with good re-expansion can be discharged
– BTS: Drainage only if symptomatic Via needle aspiration (effective in ~ 60%) Pigtail if aspiration fails or > 2.5L aspirated
Management of Secondary PTx
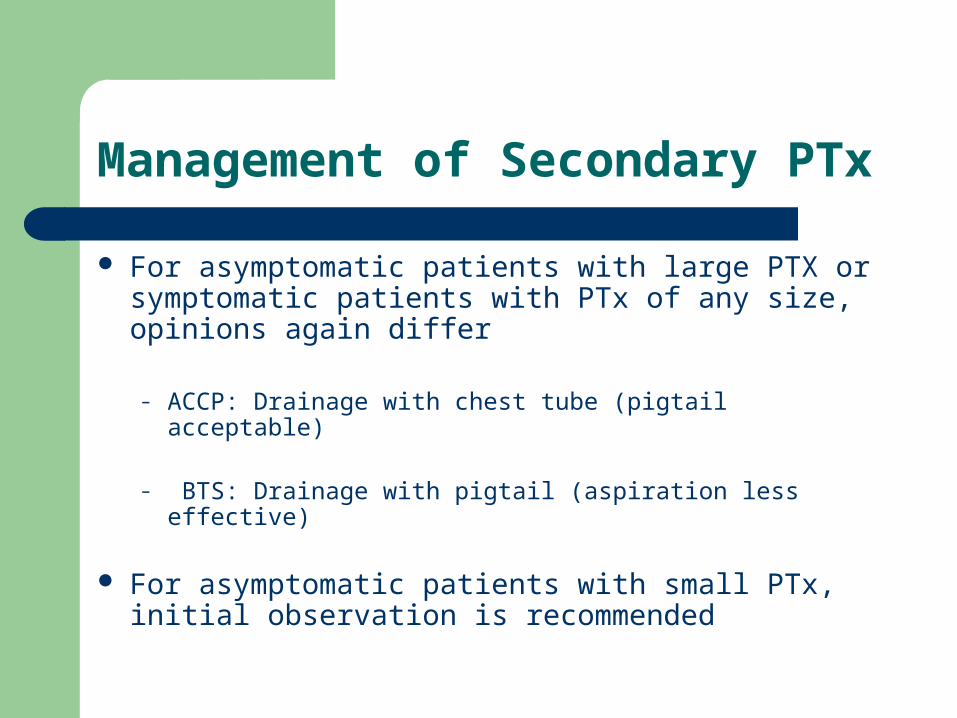
For asymptomatic patients with large PTX or symptomatic patients with PTx of any size, opinions again differ
– ACCP: Drainage with chest tube (pigtail acceptable)
– BTS: Drainage with pigtail (aspiration less effective)
For asymptomatic patients with small PTx, initial observation is recommended
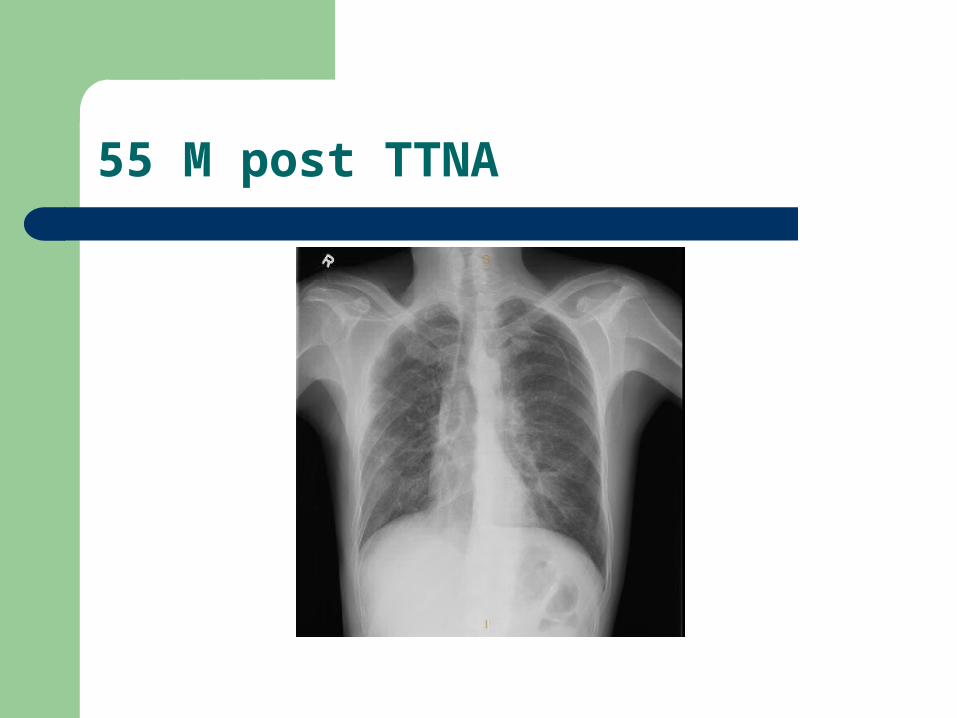
55 M post TTNA
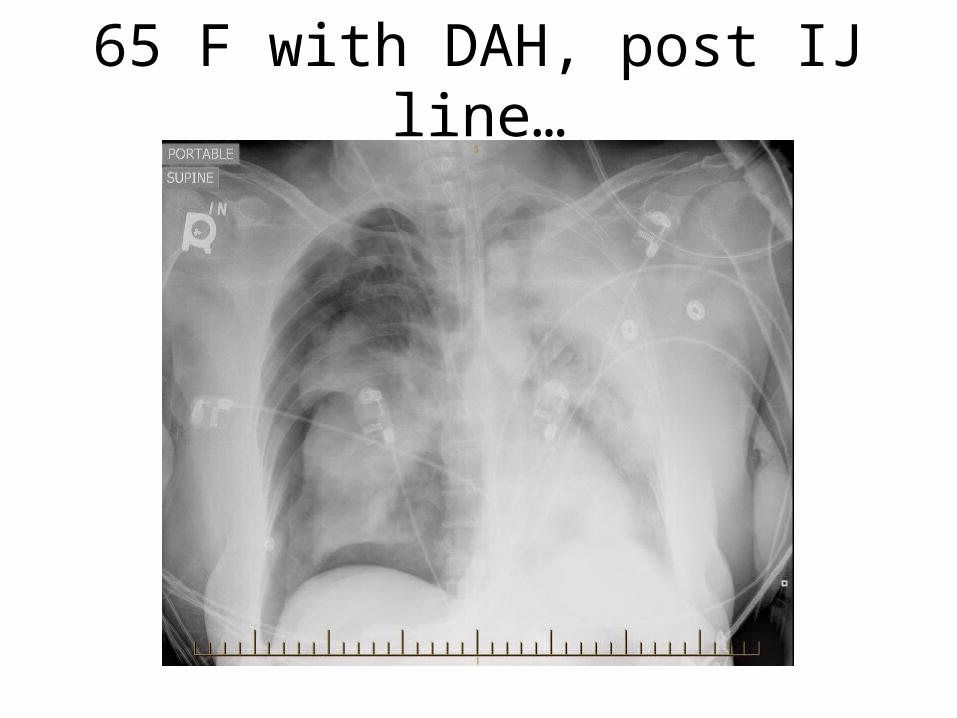
65 F with DAH, post IJ line…
Post-resolution Management
Return to normal activities allowed when free of symptoms– Return to contact sports/ heavy exercise upon complete resolution of PTx
Air travel recommendations (BTS guidelines)
– No evidence that air travel precipitates recurrence– If no surgery is performed, patients may wish to wait one year given that most
recurrences occur ≤ 1yr– If surgery is performed, travel is safe upon recovery– Waiting at least one week after CXR resolution is recommended (2 weeks if
traumatic)
Diving recommendations (BTS guidelines)
– Presence of blebs/bullae are a contra-indication– Previous spontaneous PTx is a contra-indication unless a bilateral surgical
pleurectomy performed with normal lung Fx and CT post op
Summary
An affective approach to dyspnea / hypoxemia is the key to an accurate diagnosis
The management of asthma starts by the exclusion of alternative diagnoses, risk stratification, and early bronchodilator and corticosteroid therapy
The management of massive hemoptysis consists of patient stabilization, localization of the bleeding and identification of its cause, all leading to definitive interventions
The management of a pneumothorax depends on its type, its size and its clinical consequences
– A tension PTx is a clinical diagnosis and required prompt intervention
Useful References
2010 CTS Asthma Guidelines
2010 GINA Asthma Guidelines
Analytic review: management of life-threatening asthma in adults. Mannam P, MD Siegel. Journal of intensive Care Medicine 2010.
Massive Hemoptysis: An update on the role of bronchoscopy in diagnosis and management. Sakr L, Dutau H. Respiration 2010.
2010 BTS guidelines for Pneumothorax Evaluation & Management