
Approach to Abnormal Liver Tests Anne Larson, MD Hepatology University of Washington.
45
Approach to Abnormal Liver Tests Anne Larson, MD Hepatology University of Washington
-
Upload
ruth-barrett -
Category
Documents
-
view
216 -
download
1
Transcript of Approach to Abnormal Liver Tests Anne Larson, MD Hepatology University of Washington.

Approach to Abnormal Liver Tests
Anne Larson, MDHepatology
University of Washington

Anne Larson MD
Case 1 – 65 y/o woman
comes to you to establish care
complaintsfatiguepruritisdry eyes
past historyhysterectomy for fibroids 10 years agono alcohol, tobacco or drug use

Anne Larson MD
Case 1 – 65 y/o woman
examspider angiomatamild splenomegalyotherwise normal

Anne Larson MD
Case 1 – 65 y/o woman
screening labs revealplatelets 90,000 - alk phos 4x ulnbilirubin normal - albumin 3.3 (nl >3.5)AST/ALT normal - PT normal
what do you want to do next?be thinking about this

Anne Larson MD
Case 2 – 43 y/o female
complaining of4 days of prolonged, severe RUQ painfever, severe nausea, some vomitingworse after eating
Past History20 yr ago began periodic attacks
evening RUQ pain, fluctuating intensity, no feverslasting 1-4 hours with residual RUQ tenderness

Anne Larson MD
Case 2 – 43 y/o female
Past History (cont)during last 8 years, continued episodes
pain more intense and prolonged, accompanied by penetrating pain to back below scapulamarked tenderness in RUQ persisting days
told in the past she had gallstones

Anne Larson MD
Case 3
Examtemp 38.5°C pulse 100 uncomfortable/sweatingmarked tenderness in RUQ with splinting(+) Murphy's signicterusbilirubin 6 mg/dl - alk phos 3x nl (~400 U/L)ALT 100 mg/dl - normal albumin, PTWBC 28,000 - GGT 150 U/L (nl <45)
how would you proceed?

Anne Larson MD
Approach to Abnormal Liver Tests
If patient is asymptomatic
The First Step:
repeat the tests to confirm the resultsmake sure to stop all alcohol use

Anne Larson MD
The Diagnosis
No single test is sufficient
No single battery of tests is sufficient

Anne Larson MD
The Diagnosis
Most liver disease can be diagnosed by:
taking a meticulous history
recognizing the pattern of enzyme elevations
rationally selecting a few “second-line” tests and imaging studies

Anne Larson MD
Types of Liver Tests
grouped by the liver function they assess
measures of hepatobiliary cell injury
measures of transport efficiency of organic compounds
measures of hepatic synthetic function

Anne Larson MD
Tests Reflecting Cell Injury
Aminotransferases (ALT & AST)
Alkaline Phosphatases
Transpeptidases
5’-Nucleotidase

Anne Larson MD
Tests Reflecting Cell Injury
Aminotransferases
Catalyze -amino group transfersaspartate or alanine ketoglutarate
indicators of liver cell (hepatocyte) injurysensitive but not specificmost useful marker of cell inflammation or necrosisrepresent a “leak” from damaged cells

Anne Larson MD
Tests Reflecting Cell Injury
Aminotransferases - cont
aspartate aminotransferase (AST)in cytosol and mitochondrialiver > heart > skeletal muscle > kidneys > brain > pancreas > lungs > WBCs > RBCs
alanine aminotransferase (ALT)in cytosolpredominantly livermore sensitive and specific than AST

Anne Larson MD
Tests Reflecting Cell Injury
Aminotransferases – cont.
elevated in nearly all liver diseases (ALT > AST)
marked is usually hepatocellular disease
levels may/may not reflect extent of damage
do not correlate with eventual outcome
usually <500 in obstructive jaundice
usually parallel each otherAST > ALT with EtOH, fulminant, and pregnancy

Anne Larson MD
Tests Reflecting Cell Injury
Alkaline Phosphatase
catalyzes organic phosphate estersthe enzyme is bound to hepatic canalicular membrane
elevation may be due to induction of enzyme synthesis rather than inability of liver to secrete it into the bile
increases seen with cell injury or obstructionslight to moderate (1-2x) – usually hepatocellularlarge increases (3-10x) – obstruction or cholestasis
Anne Larson MD
Tests Reflecting Cell Injury
Alkaline Phosphatase – cont.
isolated elevationsinfiltrative disease – tumor, abscess, granuloma, amyloid
Non-liver causes of elevations:bone disease » diabeteschronic renal failure » intestinal diseaserenal cancer » genetic (pseudoelevation)pregnancy » osteitis deformanssepsis (esp. GNRs) » multiple bone fracturesHodgkin's disease » intraabdominal infectionshypothyroidism » pernicious anemiacongenital hypophosphatasia » zinc deficiency

Anne Larson MD
Tests Reflecting Cell Injury
-glutamyl transpeptidase (GGT)
catalyzes transfer of -glutamyl groupshigh concentrations in bile ductule epithelial cells
useful to exclude “bone” source for Alk Phoscorrelates with alk phos levels in liver disease
sensitive but not specific in renal failure, MI, pancreatitis, diabetes

Anne Larson MD
Tests Reflecting Cell Injury
GGT – cont.
Causes of elevations:liver disease » pancreatic diseasealcohol » renal diseasecardiac disease » obesityradiotherapy » diabetesdrugs – GGT is “inducible”
phenobarbital anticoagulantsdilantin oral contraceptivesacetaminophen tricyclic antidepressants

Anne Larson MD
Tests Reflecting Cell Injury
5’-Nucleotidase (5NT)
hydrolyzes 5’ phosphates from nucleotidesassociated with canalicular and sinusoidal membranes
physiologic function unknown
only hepatobiliary tissue can release 5’-NT
specific for hepatic disease
highest in cholestatic conditions
Anne Larson MD
Tests Measuring Transport Efficiency
Hepatic clearance reflects:
1. delivery to hepatocyte (blood flow)
2. uptake by hepatocyte

Anne Larson MD
Tests Measuring Transport Efficiency
HemoglobinHemoglobin(1)(1)
HemeHeme
B-Alb (2)B-Alb (2)
Other TissueOther TissueCytochromes, etc.Cytochromes, etc.
AlbAlb

Anne Larson MD
Tests Measuring Transport Efficiency
Hepatic clearance reflects:
1. delivery to hepatocyte (blood flow)
2. uptake by hepatocyte
3. transport within hepatocyte
4. molecular alterations within hepatocyte

Anne Larson MD
Tests Measuring Transport Efficiency
HemoglobinHemoglobin(1)(1)
HemeHeme
B (3)B (3)
Conjugated (4)Conjugated (4)
B-Alb (2)B-Alb (2)
Other TissueOther TissueCytochromes, etc.Cytochromes, etc.
AlbAlb

Anne Larson MD
Tests Measuring Transport Efficiency
Hepatic clearance reflects:
1. delivery to hepatocyte (blood flow)
2. uptake by hepatocyte
3. transport within hepatocyte
4. molecular alterations within hepatocyte
5. secretion by hepatocyte into bile
6. passage down bile ducts into duodenum
Anne Larson MD
Tests Measuring Transport Efficiency
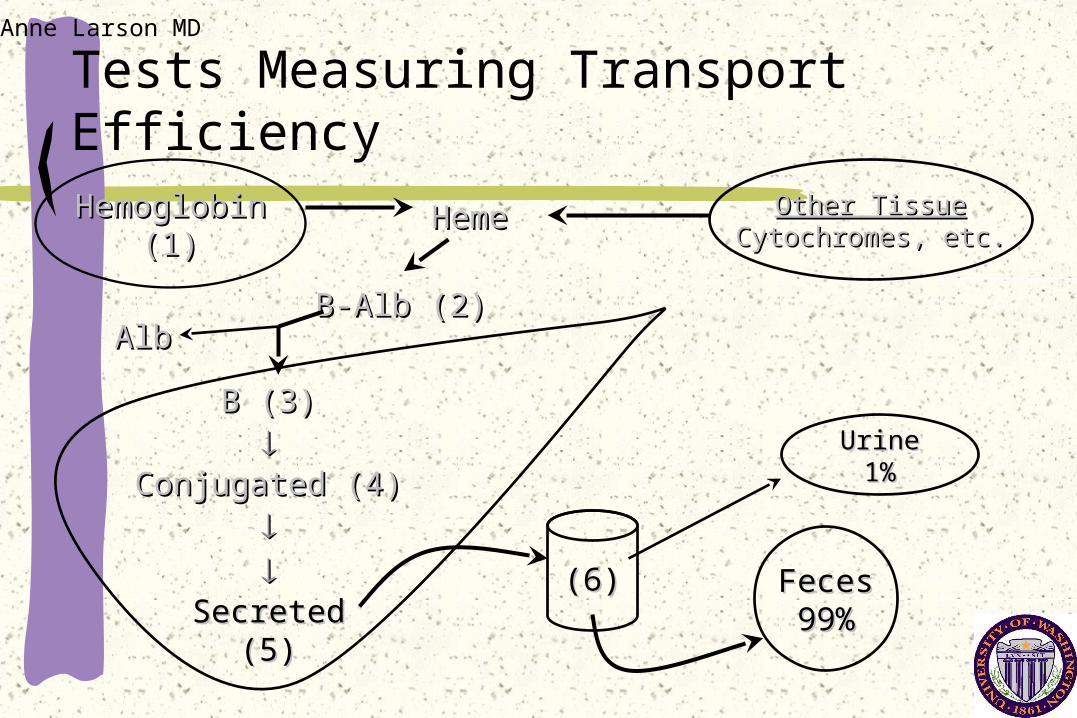
HemoglobinHemoglobin(1)(1)
HemeHeme
B (3)B (3)
Conjugated (4)Conjugated (4)
SecretedSecreted(5)(5)
B-Alb (2)B-Alb (2)
Other TissueOther TissueCytochromes, etcCytochromes, etc..
(6)(6) FecesFeces99%99%
UrineUrine1%1%
AlbAlb
Anne Larson MD
Tests Measuring Transport Efficiency
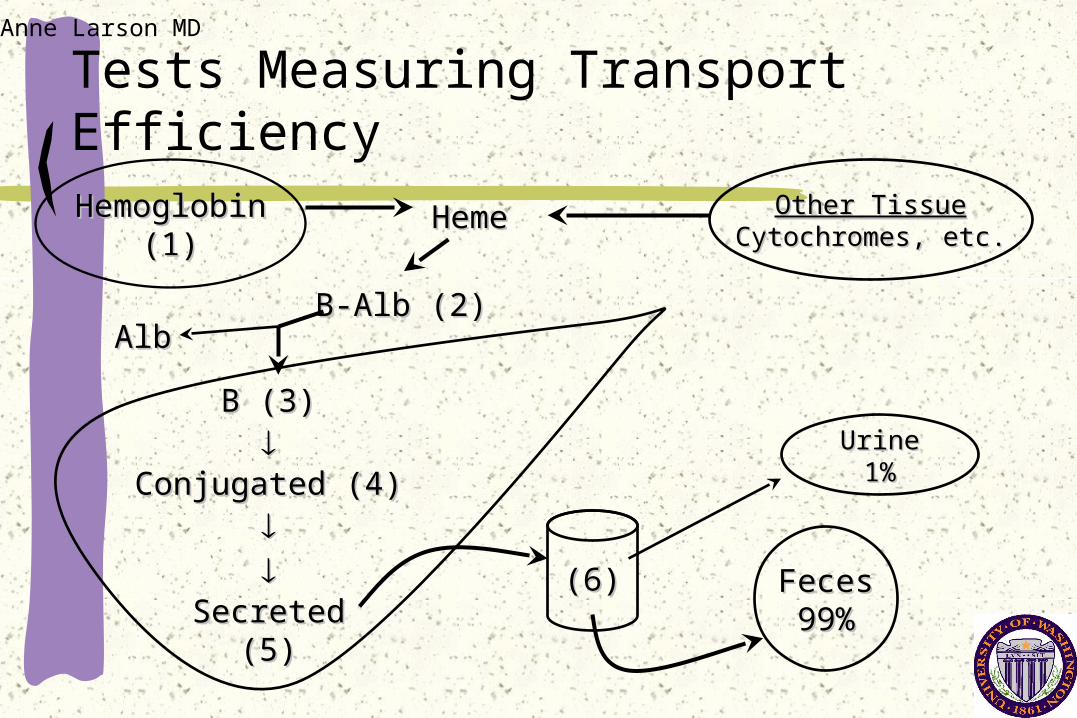
HemoglobinHemoglobin(1)(1)
HemeHeme
B (3)B (3)
Conjugated (4)Conjugated (4)
SecretedSecreted(5)(5)
B-Alb (2)B-Alb (2)
Other TissueOther TissueCytochromes, etc.Cytochromes, etc.
(6)(6) FecesFeces99%99%
UrineUrine1%1%
AlbAlb

Anne Larson MD
Tests Measuring Transport Efficiency
Remember, hepatic clearance reflects:
1. delivery to hepatocyte hemolysis
2. uptake by hepatocyte shunts, drugs (i.e., sulfa)
3. transport within hepatocyte drugs, genetics
4. molecular alterations within hepatocyte genetics
5. secretion into bile cell damage, genetics
6. passage down bile ducts obstruction

Anne Larson MD
Transport Efficiency
Bilirubinderived mainly from hemoglobin (95%)
continuous production (300 mg daily)
normal liver reserve can rev up 2-3 times
normal values of “total” bilirubin = 0.1-1.0 mg/dL
conjugated plus unconjugateddirect plus indirect
jaundice evident with levels >3.0 mg/dL

Anne Larson MD
Tests Measuring Transport Efficiency
Types of Bilirubin
Direct Bilirubin Indirect Bilirubinconjugated unconjugated
water soluble lipid solublepolar non-polar
seen in urine not in urine

Anne Larson MD
Tests Measuring Synthetic Function
Prothrombin Time (PT)AlbuminNumber Connection Tests / mental status
The liver is the only source of albumin and the prothrombin group of clotting factors

Anne Larson MD
Tests Measuring Synthetic Function
Prothrombin Time (PT)sick liver can’t make clotting factors
factors 2, 5, 7, 9, 10 (made only in the liver)
prolonged PT reflects failure of liver synthesis
Other causes of prolongation:congenital deficienciesconsumptive coagulopathies (i.e., DIC)drugs (i.e., warfarin)vitamin K deficiency (i.e., dietary, bile output)

Anne Larson MD
Tests Measuring Synthetic Function
Albumin
most important plasma protein made by the liveraccounts for 65% of protein in serumhalf-life ~17-21 days
useful indicator of liver function
Other causes of decrease:sepsis or multiple organ failureacute liver failuredietary

Anne Larson MD
Tests Measuring Synthetic Function
Number Connection Test
liver is site of detoxification
failure leads to toxins in blood
toxins unknown
encephalopathy is sign of liver synthetic failure

Anne Larson MD
The Approach
Important questions to address:
acute vs. chronic (6 months, ?cirrhosis)
hepatocellular vs. cholestatic
asymptomatic vs. symptomatic?impaired function
recent insults to the liver?EtOH, medications, pregnancy, hepatitis, herbs, gallstones, hypotension, toxins

Anne Larson MD
The Approach
Hepatocellular Injury
mainly AST & ALT +/- AP, GGT, bilirubin 2 enzyme elevations high likelihood of liver dzguides:
Mild (<3 x normal)fatty liver, EtOH, chronic hepatitis
Moderate (2-10 x normal)EtOH, chronic hepatitis, cirrhosis, neoplasm, gallstones
Severe (>10x normal; usually >1,000)ischemic, viral, toxic (e.g., acetaminophen, herbs)

Anne Larson MD
The Approach
Cholestatic Liver Disease
mainly alkaline phosphatase & GGT +/- bilirubin
determine source of AP
determine fraction of bilirubin elevatedif all indirect, generally not liver
ultrasound and/or CT scanto rule out obstructive disease, tumors, gallstones

Anne Larson MD
The Approach
Chronic Liver Disease
6 months of abnormal liver tests
symptomsasymptomatic – majority of casesfatiguearthralgiaspruritisjaundice

Anne Larson MD
The Approach
Chronic Liver Disease – cont.
Common Causes – 95% of cases:
Hepatitis C - (+) HCV-Ab and HCV-PCRHepatitis B – (+) HBsAg and HBV-DNAAlcoholic liver diseaseHemochromatosis – fasting Fe/TIBC >50%; ferritinAutoimmune hepatitis – (+) ANA, (+) ASMA, IgG

Anne Larson MD
The Approach
Chronic Liver Disease – cont.
Less Common Causes
Primary Biliary Cirrhosis (PBC) - (+) AMA; IgMPrimary Sclerosing Cholangitis (PSC) – abnormal ERCPWilson’s Disease ( ceruloplasmin)1-Antitrypsin Deficiency ( 1AT level)
Drugs (i.e., MTX, INH, amiodarone, methyldopa)

Anne Larson MD
The Approach
Chronic Liver Disease – cont.
signs of cirrhosisspider angiomatagynecomastiaportal hypertension (caput medusa)palmar erythema (seen in 10-15% of normal population)
advanced end stage liver disease – refer pronto!ascites » albuminvarices » prothrombin timeencephalopathy

Anne Larson MD
Case
screening labs revealplatelets 90,000 - alk phos 4x nlbilirubin normal - albumin 3.4 (nl >3.5)AST/ALT normal - PT normal
what are the possible diagnoses?what do you want to do next?

Anne Larson MD
Case 1
Further lab testing:HAV (-) HBV (-) HCV (-)ANA (-)ASMA (-)AMA (+) 1:1280iron studies normal
ultrasound – splenomegaly, small liver, no bil dil
What Next?

Anne Larson MD
Case
Answer:
primary biliary cirrhosisjust beginning to decompensate send for OLT

Anne Larson MD
Summary
No ideal study or battery to evaluate liver
abnormal liver tests are often the first sign of liver disease
normal or minimally elevated tests don’t exclude serious disease or cirrhosis
liver biopsy remains the gold standard to detecting and determining cause of disease


















