Application of Polymerase Chain Reaction (PCR ...library.iugaza.edu.ps/thesis/67545.pdf ·...
105
The Islamic University – Gaza Deanary of Higher Education Faculty of Science Master of Biological Sciences Medical Technology Application of Polymerase Chain Reaction (PCR), Bacteriological Culture, Immunoassay, and Microscopy for Detection and Identification of Gastrointestinal Pathogens in Children, Gaza – Palestine Prepared by Farid Hassan Abu ELAmreen Supervisors Prof. Fadel A. Sharif Dr. Abdalla A. Abed Submitted in Partial Fulfillment of Requirements for the Degree of Master of Biological Sciences/Medical Technology Faculty of Science. March 2006
-
Upload
vuongtuyen -
Category
Documents
-
view
237 -
download
1
Transcript of Application of Polymerase Chain Reaction (PCR ...library.iugaza.edu.ps/thesis/67545.pdf ·...

93
The Islamic University – Gaza Deanary of Higher Education
Faculty of Science Master of Biological Sciences
Medical Technology
Application of Polymerase Chain Reaction (PCR), Bacteriological Culture, Immunoassay, and Microscopy for
Detection and Identification of Gastrointestinal Pathogens in Children, Gaza – Palestine
Prepared by Farid Hassan Abu ELAmreen
Supervisors
Prof. Fadel A. Sharif Dr. Abdalla A. Abed
Submitted in Partial Fulfillment of Requirements for the Degree of Master of Biological Sciences/Medical Technology
Faculty of Science.
March 2006
94
Declaration I hereby declare that this submission is my own work and that, to the best of my
knowledge and belief, it contains no material previously published or written by
another person nor material which to a substantial extent has been accepted for
the award of any other degree of the university of other institute, except where
due acknowledgment has been made in the text.
Signature Name Date
Farid Farid Hassan Abu ELAmreen March-2006
Copy right. translated or stored in , No part of this work can be copied: Reservedsl RightAl
any retrieval system, without prior permission of the authors.
i

95
Abstract Acute gastroenteritis and diarrhea are common and costly problems that cause
significant morbidity and mortality in children worldwide. In Palestine, diarrhea is
one of the major causes of many outpatient visits and hospitalizations. In order
to improve knowledge on the etiology of gastroenteritis and diarrhea in our
patient population, stool specimens from 150 children less than 5 years of age
suffering from acute gastroenteritis and diarrhea and admitted to the central
pediatric hospital in Gaza strip (ElNasser pediatric hospital) were investigated
for various common enteropathogens by conventional and molecular
techniques. Enteropathogens were detected in 51.3% of the diarrheal samples.
A single enteric pathogen was detected in 40.0% of the children, while, multiple
pathogens were detected in 11.3% of the specimens.
The most important cause of diarrhea revealed by this study was rotavirus as it
represented 28.0% of the etiologic agents, detected by
immunochromatographic assay.
Shigella was the most common bacterial pathogen as identified by PCR (6.0%),
although bacteriological culture showed (4.0%) only, followed by Campylobacter
(4.7%) identified by PCR only, E.coli O157:H7 identified by PCR and culture
(4.7%, 4.0%, respectively), Salmonella sp was found in only 2.0% of the
specimens by both PCR and culture.
By microscopical examination Entamoeba histolytica/dispar was found in
15.3%, Giardia intestinalis in 1.33%, and Strongyloids stercolaris in 0.7% of the
samples.
Shigella and Salmonella isolates were tested for their susceptibility to common
antimicrobial agents and most of the isolates were resistant to ampicillin, and
trimethoprim/sulfamethoxazole.
Findings from this study demonstrated that rotavirus, E. coli O157:H7 and
Campylobacter, which are not screened for during routine examinations of stool
samples in Palestinian health laboratories in Gaza strip, were significant
enteropathogens in the studied children.
The detection of rotavirus will decrease the cost of hospitalization and prevent
the unnecessary use of antibiotics. Moreover, the high detection rate of
ii
96
rotavirus points toward the need for considering a childhood vaccine for this
pathogen.
The results of the study highlight the value of using a combination of traditional
and molecular techniques in the diagnosis of diarrheal disease in this
population.
To the best of our knowledge, this is the first study in Gaza investigating several
kinds of possible enteric pathogens in diarrhea in children less than 5 years of
age.
Key words Polymerase Chain Reaction; Gastroenteritis; Diarrhea; Rotavirus; Gaza;
Enteropathogens.
iii
97
الطرق المناعية و المجهرية في الكشف ، المزارع البكتيرية، PCRتطبيقات تقنية
.فلسطين، عن المسببات المعوية الممرضة في أطفال غزة :الملخص
يعتبر اإلسهال وااللتهابات المعوية الحادة من األمراض الشائعة في فلسطين آسائر بلدان العالم والتي تؤدي إلي
.ات آما تضيف عبئًا ماديًا آبيرًا آكلفة العالج واإلقامة داخل المستشفيات نسبة عالية من الوفي
تهدف الدراسة إلي التعرف على األسباب الميكروبية المؤدية إلي اإلسهال وااللتهابات المعوية حيث أجريت الدراسة
مستشفى ( في فلسطين في أآبر مستشفيات األطفال2005في الفترة من بداية شهر مايو إلي نهاية شهر أغسطس
طفل دون سن الخامسة من العمر أدخلوا المستشفى نتيجة اإلسهال 150وشملت الدراسة ) غزة–النصر لألطفال
.وااللتهابات المعوية
والمزارع البكتيرية والفحوصات المناعية PCR تقنية تم جمع العينات الالزمة من األطفال وفحصت باستخدام
.مجهريةوال
من المرضى مصابين % 04من العينات حيث وجد أن % 51.3 ميكروب مما نسبته 94سة تم عزل خالل الدرا
.مصابين بأآثر من نوع واحد من الميكروبات % 11.3بنوع واحد من الميكروبات و
باستخدام % 28وجدت الدراسة أن فيروس الروتا آان المسبب الرئيسي اللتهابات المعوية حيث شكل ما نسبته
باستخدام % 06.باستخدام المزارع البكتيرية و % 04.ص المناعي ، ثم تال ذلك بكتيريا الشيجال عزلت بنسبة الفح
O157:H7 و بكتيريا االيشيريشياآوالي PCRباستخدام تقنية % 4.7 ثم الكامبيلوباآتر وجدت بنسبة PCRتقنية
وفي النهاية بكتيريا السلمونيال PCRخدام تقنية باست % 4.7باستخدام المزارع البكتيرية و % 4 0.عزلت بنسبة
. PCRباستخدام المزارع البكتيرية و تقنية % 2.0 عزلت بنسبة
من العينات الموجبة حيث آان طفيل % 17.33 وجد أن الطفيليات المعوية شكلت ما نسبته جهريبالفحص الم
0.7وسترونجلويدس سترآورالس % 1.33ة بنسبة ثم الجارديا المعوي % 15.3االنتميبا هستوليتكا األعلى بنسبة
. %
وجدت الدراسة أن معظم بكتيريا الشيجال والسلمونيال آانت مقاومة لعدد من المضادات الحيوية وخاصة االمبيسيلين
.لكليهما % 77.8والسلفاميثوآسازول بنسبة
تائج التي يتم الحصول عليها وسرعتها في في مراآز الخدمات الصحية لدقة الن PCRتوصي الدراسة بإدخال تقنية
.التشخيص وذلك باالضافة للفحوصات التقليدية
اللذان O157:H7آما توصي بإدخال الفحوصات الالزمة للتعرف على فيروس الروتا وبكتيريا االيشيريشيا آوالي
الروتا بسبب ارتفاع نسبة ال يتم الكشف عنهما بالفحص الروتيني العادي باالضافة الى تطعيم االطفال ضد فيروس
وتوصي بسرعة الكشف عنه مما يقلل من انتشاره ويقلل من استخدام الكثير من المضادات الحيوية ، االصابة به
.الغير فعالة لعالج مثل هذه الحاالت
يشار إلي أن هذه أول دراسة تجرى في قطاع غزة في الكشف عن العديد من الميكروبات المسببة لالسهال .هابات المعوية عند االطفالوااللت
iv
98
TABLE OF CONTENTS
CONTENTS Page
DECLARATION …………………………………………………….……….…………….…………………………..i ABSTRACT (English)…………………………… ……………………………………………………….………..ii ABSTRACT (Arabic)……………………………… …………………………………………………… .………..iv TABLE OF CONTENTS …..……………………………………..……………….…………………………… ……v LIST OF TABLES....………..……………………………………… …………….……………….……………... vii LIST OF FIGURES ……………………………………………..…………………….…………………….… ….viii ABBREVIATIONS………………………………………………..………………………………………… ………ix DEDICATION ……………….…………………………………..…………………….………….…………………..x ACKNOWLEDGEMENTS …….……………………….…………………………………….……………xi
CHAPTER 1 INTRODUCTION........................................................................................................................... 1 CHAPTER 2 Literature review.......................................................................................................................... 4
2.1. Infectious diarrhea ................................................................................................. 4 2.2. Shigella .................................................................................................................. 5 2.3. Salmonella ............................................................................................................. 6 2.4. E coli O157:H7 ...................................................................................................... 7 2.5. Campylobacter....................................................................................................... 9 2.6. Rotavirus.............................................................................................................. 10 2.7. Parasitic Diarrhea................................................................................................. 12 2.8. Enteropathogens................................................................................................... 12 2.9. Detection and identification of enteropathogens by PCR.................................... 22
CHAPTER 3 Materials and Methods.............................................................................................................. 27
3.1. Materials .............................................................................................................. 27 3.1.1. PCR primers.................................................................................................. 27 3.1.2. Bacterial Culture Media................................................................................ 27 3.1.3. Reagents and Materials................................................................................. 28 3.1.4. Enzymes........................................................................................................ 28 3.1.5. Commercial Kits ........................................................................................... 28 3.1.6. Apparatus and Equipments ........................................................................... 29
3.2. Study population .................................................................................................. 29 3.2.1. Sample collection.............................................................................................. 30 3.2.2. Ethical Considerations ...................................................................................... 30 3.2.3. Data Analysis.................................................................................................... 30 3.3. Parasites detection................................................................................................ 30 3.4. Rotavirus detection .............................................................................................. 31
3.4.1. Principle of the procedure............................................................................. 31 3.5. Bacterial Detection by Culture ............................................................................ 32 3.6. Identification of E.coli, Salmonella, and Shigella ............................................... 32
3.6.1. Colony morphology ...................................................................................... 33 3.6.2. Gram stain..................................................................................................... 33 3.6.3. Biochemical tests .......................................................................................... 33
3.6.3.1. Oxidase test............................................................................................ 33 3.6.3.2. Hy.enterotest .......................................................................................... 34 3.6.3.3. The API-20E test kit .............................................................................. 34 3.6.3.4. Fluorescence production on MUG medium........................................... 35
3.6.4. Serological tests ............................................................................................ 36 3.6.4.1. Anti-Shigella agglutination sera ............................................................ 36
v

99
CONTENTS Page
3.6.4.2. Anti Salmonella agglutination sera........................................................ 36 3.6.4.3. Anti E. coli O157:H7 latex test kit ........................................................ 37
3.7. Antimicrobial susceptibility testing by disk diffusion......................................... 38 3.8. Polymerase Chain Reaction (PCR)...................................................................... 39
3.8.1. Preparation of Fecal Specimens for PCR Assays ......................................... 39 3.8.2. DNA Extraction from stool........................................................................... 39 3.8.3. Detection and measurement of extracted DNA ............................................ 41
3.8.3.1. Agarose gel electrophoresis ................................................................... 41 3.8.3.2. Spectrophotometery ............................................................................... 41
3.9. Detection of Shigella by PCR.............................................................................. 42 3.9.1. Temperature cycling program....................................................................... 42 3.9.2. Expected Shigella PCR results ..................................................................... 42
3.10. Detection of Salmonella by PCR....................................................................... 43 3.10.1. Temperature cycling program..................................................................... 44 3.10.2. Expected Salmonella PCR results............................................................... 44
3.11. Detection of E.coli O157:H7 by PCR................................................................ 44 3.11.1. Temperature cycling program..................................................................... 45 3.11.2. Expected E.coli O157:H7 PCR results ....................................................... 45
3.12. Detection of Campylobacter coli/jejuni by PCR ............................................... 46 3.12.1. Temperature cycling program..................................................................... 47 3.12.2. Expected Campylocacter PCR results ........................................................ 47
CHAPTER 4 RESULTS.................................................................................................................................... 48
4.1. Age group distribution of the study population ................................................... 48 4.2. Prevalence of Enteropathogens............................................................................ 49 4.3. PCR Results ......................................................................................................... 51 4.4. Comparison of Bacteriological Stool Culture, and PCR Assay........................... 53 4.5. Mixed Infections .................................................................................................. 54 4.6. Occurrence of Enteropathogens among the different age groups........................ 55 4.7. Clinical features and infection ............................................................................. 55 4.8. Enteropathogens distributed by residence of the subjects ................................... 56 4.9. Antimicrobial Susceptibility of Shigella and Salmonella isolates....................... 57
CHAPTER 5 DISCUSSION.............................................................................................................................. 59 CHAPTER 6 CONCLUSION and RECOMMENDATIONS.............................................................................. 73 CHAPTER 7 REFERENCES............................................................................................................................ 77
APPENDICES ............................................................................................................ 88
vi

100
List of Tables
Table Page
Table 3.1. Sequence of the primers used in PCR ...................................................................... 27
Table 3.2. Tests of Hy.enterotest used for differentiating the genera of Enterobacteriacea .... 34
Table 3.3. Shigella PCR reaction mixture for ipaH gene............................................................ 42
Table 3.4. Salmonella PCR reaction mixture for 16S rDNA gene .............................................. 43
Table 3.5. E.coli O157:H7 PCR reaction mixture using uidA gene ............................................ 45
Table 3.6. Campylobacter c/j PCR reaction mixture for 16S rDNA gene................................... 46
Table 4.1. Age group distribution of the study subjects............................................................. 48
Table 4.2. Distribution of the specimens in terms of residence area of the subjects. ................ 49
Table 4.3. Enteropathogens identified in the 150 studied specimens ........................................ 50
Table 4.4. Comparison between bacteriological stool culture, and PCR assay in detecting three
bacterial enteropathogens........................................................................................................... 53
Table 4.5. Occurrence of mixed infections by enteric pathogens............................................... 54
Table 4.6. Occurrence of mixed infections by age group ........................................................... 54
Table 4.7. Enteropathogens encountered among the different age groups............................... 55
Table 4.8. Clinical symptoms in relation to infections in 150 children with diarrhea .................. 56
Table 4.9. Enteropathogens distributed by residence ................................................................ 56
Table 4.10. Antibiotic susceptibility of Salmonella and Shigella isolates.................................. 57
vii
101
List of Figures
Figure Page
Figure 2.1. Rotavirus particles.................................................................................................... 11
Figure 3.1. Interpretation of rotavirus results ............................................................................. 32
Figure 3.2. Colony morphology of selected bacteria.................................................................. 33
Figure 3.3. Hy enterotest results for selected bacteria............................................................... 34
Figure 3.4. The API-20E test kit ................................................................................................. 35
Figure 3.5. E.coli O157:H7 does not produce fluorescent product on MUG medium................ 36
Figure 4.1. Frequency of the identified enteropathogens........................................................... 50
Figure 4.2. Gel electrophoresis for DNA extracted from stool samples by AccuPrep Stool DNA
Extraction Kit. .............................................................................................................................. 51
Figure 4.3. Specific amplification of Shigella specific invasion plasmid antigen H locus DNA by
PCR............................................................................................................................................. 51
Figure 4.4. The 16S rDNA gene PCR assay specific for Salmonella species. ……….…………51
Figure 4.5. PCR for identification of E.coli O157:H7 targeting uidA........................................... 52
Figure 4.6. 16S rDNA-based PCR assay specific for C. jejuni and C. coli. .............................. 52
Figure 4.7. Interpretation of rotavirus results ............................................................................. 53
Figure 4.8. Antibiotic resistance for Salmonella and Shigella isolates..................................... 58
viii
102
ABBREVIATIONS
µl Micro liter ADH Arginine dehydrogenase bp Base pair CDC Center of Disease Control and Prevention CFU Colony forming unit CIT Citrate DAEC Diffusely adherent Escherichia coli DNA Deoxyribonucleic acid dNTPs Deoxynucleotide triphosphates EAEC Enteroaggregative Escherichia coli EDTA Ethylenediaminetetraacetic acid EHEC Enterohemorrhagic Escherichia coli EIEC Enteroinvasive Escherichia coli ELISA Enzyme-linked immunosorbent assay EM Electron microscope ETEC Enterotoxigenic Escherichia coli g Gram GEL Gelatin liquifaction GN broth Gram negative broth H antigen Flagellar antigen H2S Hydrogen sulfide HE agar Hektoen enteric agar HUS Hemorrhagic uremic syndrome LA Latex agglutination LDC Lysine Decarboxylase mg Milli gram MgCl2 Magnesium chloride MH agar Muller Hinton agar MUG 4-methylumbelliferyl-β-D-glucuronide NCCLS National Committee for Clinical Laboratory Standards NSF Non sorbitol fermenter O antigen Somatic antigen O.D Optical density ODC Ornithine Decarboxylase ONPG o-Nitrophenyl-beta-galactopyranoside PAGE Polyacrylamide gel electrophoresis PCR Polymerase chain reaction PFGE Pulsed field gel electrophoresis RAPD Random amplified polymorphic DNA RFLP Restriction Fragment Length Polymorphism rpm Round Per Minute rRNA Ribosomal RNA RT-PCR Reverse transcriptase PCR SMAC agar Sorbitol-MacConkey agar SS agar Salmonella shigella agar STEC Shiga toxin-producing Escherichia coli SXT Trimethoprim/sulfamethoxazole Tris Base Hydroxymethyl aminomethane URE Urease URTIs Upper respiratory tract infections Vi antigen Capsular antigen VP Voges Proskauer WHO World Health Organization XLD agar Xylose Lysine Deoxycolate agar
ix
103
To my beloved parents and family
to my wife,
to my sons,
Osama, Mohamed, Hassan, and Mohanad
and
to my daughter
Lina
x
104
Acknowledgements
This work has been carried out at the Medical Technology laboratories in the
Islamic University of Gaza, Palestine.
I would like to express my sincere thanks to all the people who directly or
indirectly have contributed to this work. In particular, I would like to thank:
Mr. Tarek Omar Aggad - Chairman & CEO of Arab Palestinian Investment Co.
Ltd (APIC) and the staff of the Medical Supplies & Services Co. Gaza Palestine
especially Dr. Sohail Obeed for their excellent funding of this work.
Professor Fadel A. Sharif, my great supervisor for being professional,
encouraging and enthusiastic, for your great knowledge and tremendous
intelligence, without your stimulating, critical discussions, comments, and great
help, this work would not have been completed.
Dr. Abdalha A. Abed co-supervisor for your great help, very nice
comments, discussions, and great support.
I would like to extend my thanks to all the staff at the Department of the
biological sciences, particularly Dr. Abbood Kichaoi, for their support and help.
Dr. Randa Elkhodary always having an open door and encouraging my
questions and ideas.
Miss. Najah Eliwa, Head manager of the AlShifa Hospital Central
laboratory for her generous support, orientation, and very good comments.
Mr. Nasser Abu Shaaban, for all their helpful and friendly support in the
lab work.
All the staff at the ElNasser Pediatric Hospital (physicians, nurses, and
lab technicians), and special thanks to Dr. Abderahman Eisa the director of
ElNasser Pediatric Hospital, and to Mr. Shaker Abu Shaaban the director of the
ElNasser Pediatric Hospital laboratory.
All the staff at the Medical Microbiology Department of AlShifa Hospital
Laboratory, Gaza, where I am working, for their support and help.
I am deeply grateful to Mr. Arafat Elhindawy, Mr. Hassan Eltiby for their
helpful and friendly support.
xi

105
For all of the laughs and good times, I would also like to thank my friends
and colleagues, for all of their support and guidance and encouraging; good
luck to all.
Finally, I want to say that my beloved family especially my brothers and
sisters, my wife, they always stand beside me and give me encouragement all
time and for their never-ending love and support. I am so proud of my family.
xii

1
CHAPTER 1 INTRODUCTION
Gaza Strip is an elongated area located in an arid to semi-arid region. It is
bordered by Egypt from the South, the green line from the North, Nagev desert
from the East and the Mediterranean Sea from the West. The total surface area
of the Gaza Strip is 360 km2, and its population has been estimated to be 1,3
million for the year 2004, two thirds of them are mainly concentrated in eight
refugee camps. 49.4% of the population in Gaza strip is under 15 years old
(1,117). Acute gastroenteritis, (infectious diarrhea) is one of the leading causes of
illnesses and death in infants and children throughout the world, especially in
developing countries. This is so in Asia, Africa and Latin America, where an
estimated 2.5 million deaths occur each year in children less than 5 years of
age (88,128). Diarrhea is also one of the leading causes of deaths among the
population in Gaza Strip (16).
Gastroenteritis (human enterocolitis) is a disease characterized by fever and
diarrhea. This disease is characterized by painful abdominal cramps and
frequent defecation of blood and mucus, attributed to penetration and
destruction of colonic epithelia by invasive microorganisms. Symptoms can
include nausea, vomiting, diarrhea, fever, abdominal cramping and/or pain and
a general feeling of tiredness. Approximately 9% of all hospitalizations of
children younger than 5 years are due to diarrhea and dehydration (14). Investigations on diarrheal diseases in young children demonstrated that
Salmonella spp., Cryptospordium, Campylobacter spp. and rotavirus were the
major pathogens in Gaza Strip, and overcrowding was linked with an increased
risk of diarrhea (1,151).
Worldwide, the most common pathogens that cause this disease are:
Salmonella spp., Shigella spp., Campylobacter spp., E. coli O157:H7, Listeria
monocytogenes, Vibrio cholera, Yersinia enterocolitica, Rotavirus,
Cryptosporidium spp, Entamoeba histolytica, and Giardia intestinalis (lamblia).
These pathogens can cause potentially serious diseases which may be fatal,
especially in children. The common route of infection by these pathogens is the
ingestion of contaminated foods and drinks (13).
2
Rotavirus is a major cause of severe gastroenteritis among children. This virus
is transmitted by fecal-oral route and constitutes an important cause of
nosocomial gastroenteritis.
Timely diagnosis of rotavirus infection in patients with acute diarrhea helps
determine appropriate treatment, prevents the unnecessary use of drugs and
minimizes the spread of the disease (123,143).
The identification and diagnosis in Palestinian health laboratories is done only
for Salmonella spp. and Shigella spp, through culture, biochemical and
serological assays, while Entamoeba histolytica, Giardia intestinalis and
helminthes are diagnosed by direct microscopic slide method. The other
pathogens, however, are not routinely diagnosed (117). Data from the health laboratories all over Gaza Strip show that the detection
rate of Salmonella spp. is very low (about 0.4% in the year 2004) and even
lower for Shigella spp. (0.4, 1.2 and 0.12%, in the respective years 2002, 2003
and 2004). Moreover, data concerning cases of Campylobacter, E. coli
O157:H7 and rotavirus and their relation to infection in Palestinian children are
extremely scarce (115,116,117). One of the modern techniques for identifying enteropathogens relies on PCR
amplification assays with specifically designed nucleotide primers. PCR is
suggested, by many investigators to be safer, more sensitive and more rapid
than the ordinary culture methods for the diagnosis of bacteria or viruses (17). In the present study both conventional and molecular diagnostic (PCR)
techniques were used for analyzing stool samples collected from 0-5 years old
children with acute diarrhea for the presence of the four common bacterial
enteropathogens: Salmonella spp., Shigella spp., Campylobacter spp., and E.
coli O157:H7. Moreover, the occurrence of parasites and rotavirus in the
samples were investigated by microscopic examination and an
immunochromatographic method, respectively.
3
Microorganisms are present in the nature between heaven and earth. In stool
there are microorganisms which are considered as beneficial, and those which
are harmful. Our objectives were to perform a detailed molecular and
microbiological investigation of some potential pathogens associated with
diarrhea, to characterize the isolates, and to assess clinical symptoms and the
epidemiological factors related to the diarrheal disease in children less than 5
years of age in Gaza, Palestine.
Specifically the aims of the present study were as follows:
1. To detect and identify bacterial enteric pathogens from fecal
samples in children less than 5 years of age in Gaza, Palestine.
2. To assess the antibiotic susceptibility of isolated Shigella and
Salmonella strains in these children.
3. To determine the role of Group A rotavirus in causing diarrhea in
children in Gaza.
4. To determine the role of the common parasites in causing
diarrhea in children in Gaza.
5. To investigate the sensitivity and performance characteristics of a
direct PCR on stool samples as compared to conventional
techniques for diagnosis of certain enteropathogenic bacteria.
Hence, four of the most relevant enteropathogens were selected
for this study: Salmonella spp., Shigella spp., Campylobacter
jejuni/coli. and E. coli O157:H7.
4
Chapter 2 Literature review
2.1. Infectious diarrhea
Diarrhea is one of the principal causes of morbidity and mortality among
children in the developing world. In 1982, on the basis of a review of active
surveillance data from studies conducted in the 1950s, 1960s and 1970s, it was
estimated that 4.6 million children died annually from diarrhea (163). In 1992, a review of studies conducted in the 1980s suggested that diarrheal
mortality had declined to approximately 3.3 million annually (24). Recent investigations show that diarrhea accounted for a median of 21% of all
deaths of children aged under 5 years in developing areas and countries, being
responsible for 2.5 million deaths per year. Increases in immunization coverage,
better health care access, improvements in water and sanitation, and other
socioeconomic changes affect both diarrheal mortality and childhood nutrition.
Improvement of the techniques and methods used in the detection of
enteropathogens may justifying the decreased rates of mortality (60,88). Two converging factors highlight the growing need for clear guidelines for the
diagnosis and management of infectious diarrhea.
First, there is increasing recognition of a widening array of enteric pathogens
associated with illnesses of the gastrointestinal tract. Agents such as discussed
before cause about 1.3 billion cases of diarrheal illnesses in the world each
year. Many of these organisms are easily transmitted through food or water or
from one person to another, and some are devastating particularly, to
individuals with compromised immune systems (55,59). With the rapid globalization and industrialization of our food supply and with a
multiplicity of recognized pathogens and diagnostic tools, the challenges of
determining optimal, cost-effective means for appropriate diagnosis, clinical
management, and public health control of diarrheal illnesses are great (43). The second factor arises from our having entered an era when health care is
increasingly managed with an eye to cost containment. Critical to developing a
cost effective approach to the evaluation and management of infectious
diarrhea is the selective use of available diagnostic methods, therapies, and
preventive measures. These must be targeted to the clinical scenarios in which
5
they will yield the greatest benefits, and certain factors must be taken into
account: the patient’s history, exposure, and immune status, and the nature of
the illness: its severity and duration and whether the process is inflammatory or
hemorrhagic. Clear guidelines are needed for the application of diagnostic
methods to identify enteric infections that require specific therapy or are
responsive to control measures (59). Oral rehydration, clinical and epidemiological evaluation, performance of
selective fecal studies, administration of selective antimicrobial therapy,
contraindicated antidiarrheals, and available immunizations will continue to
evolve as improved understanding of pathogenesis and development and use
of inexpensive, rapid tests improve diagnosis and management of infectious
diarrheal illness, one of the most common clinical syndromes in our society
(171,184).
2.2. Shigella
This bacterium was named as Shigella by the Japanese bacteriologist K. Shiga
who used bacterial culture to investigate an epidemic of acute dysentery in
Japan in 1898. Shigella is moderately-sized, gram-negative rod-shaped,
facultative anaerobes, nonspore forming, closely related to E. coli. They are
usually non-motile, oxidase negative, and do not ferment lactose. Shigella
belongs to the Enterobacteriacae family (186,129). There are 4 known species of Shigella with multiple serotypes: A (S.
dysenteriae, 12 serotypes); B (S. flexneri, 6 serotypes); C (S. boydii, 18
serotypes); and D (S. sonnei, 1 serotype), S. flexneri is the predominant species
in endemic areas, accounting for approximately 50% of culture-positive cases
(152). Shigella is the primary causative agent of bacillary dysentery throughout the
developing world. According to the World Health Organization, the annual
number of Shigella episodes throughout the world was estimated to be 164.7
million, of which 163.2 million were in the developing countries (with 1.1 million
deaths) and 1.5 million in industrialized countries. A total of 69% of all episodes
and 61% of all deaths are attributable to shigellosis involved children under 5
years of age (89,186).

6
A definitive diagnosis of Shigella infection can be made by isolating the
organism from stool and serotyping the isolate. Culture is also required to
determine the antimicrobial sensitivity. The standard procedure for detection of
Shigella spp. is based on isolation on selective culture media followed by
identification by biochemical tests and agglutination assays (81). This process
may take 48-72h or even longer to obtain results. Since Shigella are very
fastidious organisms, appropriate collection, rapid transport to the laboratory
and rapid plating of the sample are important for isolation. Such conditions are
often difficult to attain in developing countries. Thus, rapid, highly sensitive and
specific techniques based on genetic characteristics have been developed.
PCR is the best known of these techniques and is often used as a test for the
detection and identification of pathogenic microorganisms. Several PCR
protocols for detection of Shigella in feces (73,190), food (100), and water (23) have been published. These protocols use primers directed at sequences
located on the invasion plasmid of Shigella spp. (100,190).
2.3. Salmonella
Members of the genus Salmonella are gram-negative, facultatively anaerobic,
rod-shaped, non-spore-forming bacteria. They are usually motile, oxidase
negative, and do not ferment lactose, the genus Salmonella belongs to
Enterobacteriaceae family (86). First described in 1880 and cultured in 1884, the bacterium has been named
after Daniel E. Salmon, the pathologist who first isolated the organism from
porcine intestines. The majority of Salmonella cause food poisoning and
gastroenteritis in humans all over the world, but one species, S. typhi, frequently
disseminates into the blood and causes a severe form of salmonellosis called
typhoid fever (62). Currently, the CDC (Center of Disease Control and Prevention) recognizes two
species which are divided into seven subspecies: S. enterica (six subspecies)
and S.bongori (one subspecies). The subspecies are divided into over 50
serogroups based on somatic (O) antigens present. The serogroups are further
divided into over 2300 serotypes. Salmonellae can be serotyped according to
their particular complement of somatic (O), capsular (Vi), and flagellar (H)
antigens (32,152).
7
Conventional methods for detecting and identifying Salmonella involve cultural,
biochemical and immunological assays, that rely on phenotypic
characterization. These methods require selective enrichment and plating,
which often take several days to complete the identification (172). Although bacteriological assays have historically been the method of choice for
the recovery of Salmonella from feces and environmental samples (35,38,167), the whole procedure takes at least 3 days to complete. These methods are
generally time-consuming (10,30). Several alternative analysis strategies have been proposed, and PCR in
particular has been found to be a highly specific molecular diagnostic tool
(67,142). Multiplex PCR methods for detecting Salmonella have been published utilizing
specific gene sequences as targets. Such methods are simple, inexpensive,
and sensitive and enable the quick and precise detection of the most prevalent
serotypes of Salmonella in human clinical samples (10,172). PCR has become an important technique for more-rapid detection of pathogens
in feces and environmental samples when an isolate is not required
(35,38,167). Few investigations have evaluated Salmonella-targeted PCR primers with
intestinal bacteria. In determining which PCR primers were best suited for
detection of Salmonella in stool samples, the 16S rDNA primer sets were
approved for their applicability to gastrointestinal samples (194).
2.4. E coli O157:H7
E. coli O157:H7 is one of hundreds of strains of the bacterium Escherichia coli.
They are gram-negative, facultatively anaerobic, rod-shaped, non-spore-forming
bacteria. They are usually motile, oxidase negative, ferment lactose, and belong
to the Enterobacteriaceae family. Although most strains are harmless and live in
the intestines of healthy humans and animals, this strain produces a powerful
toxin and can cause severe illness.
E. coli O157:H7 was first recognized as a human pathogen in 1982 (78), and it
is increasingly recognized as an important cause of sporadic and outbreak-
associated bloody diarrhea (145).
8
An estimated 73,480 illnesses, 62,458 hospitalizations and 61 deaths occur
each year in the United States from this pathogen (113). E. coli serotype O157:H7 is designated by its somatic (O) and flagellar (H)
antigens. From both a clinical and public health standpoint, E. coli O157:H7 is
by far the most important serotype in the world that cause bloody diarrhea.
Children with gastrointestinal infections caused by E. coli O157:H7 are at risk
for the hemolytic-uremic syndrome (HUS) that can be fatal as it causes acute
kidney failure (189). In many hospitals and private laboratories, a routine stool culture does not
include testing for E coli O157:H7. Sorbitol-MacConkey (SMAC) agar is the
standard culture medium for E coli O157: H7 (152). Unlike 80 to 90 percent of E. coli strains, E. coli O157:H7 does not ferment
sorbitol rapidly. The colorless, sorbitol-negative colonies can then be assayed
for the O157 antigen and H antigen with the use of commercially available
antiserum (107). SMAC medium stool culture is a simple, inexpensive, rapid, and reliable means
of detecting E. coli O157:H7 (108). Some laboratories also test E. coli O157 strains for the enzyme B-
glucuronidase using agar medium containing the substrate 4-methylumbelliferyl-
β-D-glucuronide (MUG) (138). When MUG is cleaved by this enzyme, a
fluorescent product is produced that is detectable with long-wave ultraviolet
light. Unlike approximately 92% of E. coli, E. coli O157:H7 and nonmotile E. coli
O157 strains that produce Shiga-like toxins lack the enzyme and are MUG
negative. For this reason the MUG assay is used in conjunction with testing for
sorbitol fermentation and agglutination with E. coli O157 antiserum as a useful
screening test for toxigenic strains of O157 (65). Culture may also be
problematic due to the large numbers of other flora that either overgrow or
mimic the non-sorbitol-fermenting E. coli O157:H7 (169). Investigators have documented the use of conventional culture methods and
PCR for the detection of E. coli O157:H7. The PCR for E. coli O157:H7 that is
not readily detected by conventional culture has proved its ability to provide
rapid same day results (65,102)
9
2.5. Campylobacter
Campylobacter species are microaerophilic, motile with a single polar flagellum,
Gram negative, usually curved or spiral rod-shaped bacteria, 0.2-0.5µm wide
and 0.5-0.8 µm long, non-fermenting, oxidase positive, and grow optimally at
37° or 42°C (77). It is one of the most common causes of bacterial diarrhea in the world, fifteen
species of Campylobacter have been described, two of these; Campylobacter
jejuni and Campylobacter coli, account for the majority of human infections.
Campylobacter species can cause mild to severe diarrhea, with loose, watery
stools often followed by bloody diarrhea (162,166). In most industrialized countries Campylobacter have become the most
frequently reported cause of bacterial gastrointestinal illness. It affects all ages,
but peak incidence appears to be in the ages 1 to 5 years. Campylobacteriosis
occurs much more frequently in the summer months than in the winter (185). Identification of campylobacters is well known to be problematic, principally
because of their complex taxonomy, biochemical inertness, and fastidious
growth requirements. Darting motility in a fresh fecal specimen observed by
dark-field or phase-contrast microscopy or characteristic vibrio forms visible
after Gram staining permit a presumptive diagnosis. The diagnosis is confirmed
by isolating the organism from a fecal culture or, rarely, from a blood culture
(74,152). Conventional cultural methods for detecting Campylobacter spp. involve
enrichment in selective broth, followed by isolation on selective differential agar.
Campylobacter spp. have demanding growth requirements because they need
to be incubated under microaerobic conditions (5% O2, 10% CO2, and 85%
N2), at 37°C or 42°C for 48 hours. A further 24 to 48 h is required for full
phenotypic identification, which makes the task of isolation laborious, costly and
time consuming (47). Culture methods are biased toward the detection of C. jejuni and C. coli. A
number of the antimicrobial agents incorporated into the commonly used
selective media (e.g., Preston agar, Skirrow agar, and Butzler agar) may inhibit
growth of some Campylobacter species. Cephalothin, colistin, and polymyxin B
can be inhibitory to some strains of C. jejuni and C. coli. As a result,
10
microbiological methods do not provide a true measure of the frequency and
diversity of Campylobacter species associated with diarrhea and their feces
(39). Recently, genetic methods have been used to identify Campylobacter
species (48,85,150). Molecular methods based on PCR amplification may provide an alternative to
culture methods for the detection of Campylobacter in clinical specimens. The
application of PCR based assays for the detection of Campylobacter species in
clinical and food samples has been previously reported by several authors.
These reports describe amplification of a number of DNA targets including e.g.,
16S rDNA, 23S rDNA, ceuE, and mapA (54,85,94). The application of PCR provides a more accurate description of the prevalence
of Campylobacter species associated with diarrhea (119). The 16S rDNA-based PCR assay specific for C. jejuni and C. coli. Regions
were identified from an alignment of 16S rRNA gene sequences in which the
sequences for C. jejuni and C. coli differed from those of all other
Campylobacter species. A primer pair was designed for coidentification of the
two species. The primers were tested against the DNAs of the type strains of all
species in the genus Campylobacter. After PCR an amplicon of 854 bp was
generated from all the tested strains of both C. jejuni and C. coli but not from all
the tested strains of the other Campylobacter species. There was no reaction
with any other non Campylobacter species (101).
2.6. Rotavirus
The wheel-like (Latin rota = wheel) particles of rotavirus were first identified as a
human pathogen in 1973 by Bishop et al., when characteristic particles were
observed in the cytoplasm of duodenal epithelial cells obtained from young
children admitted to the hospital for treatment of acute diarrhea (20,79,83). Rotavirus is a 65-70 nm RNA virus of the family Reoviridae, icosahedral, with
segmented double-stranded (11 segments). It is classified into seven
serogroups A-G, Group A subtypes 1, 2, 3, 4 constitute the main human
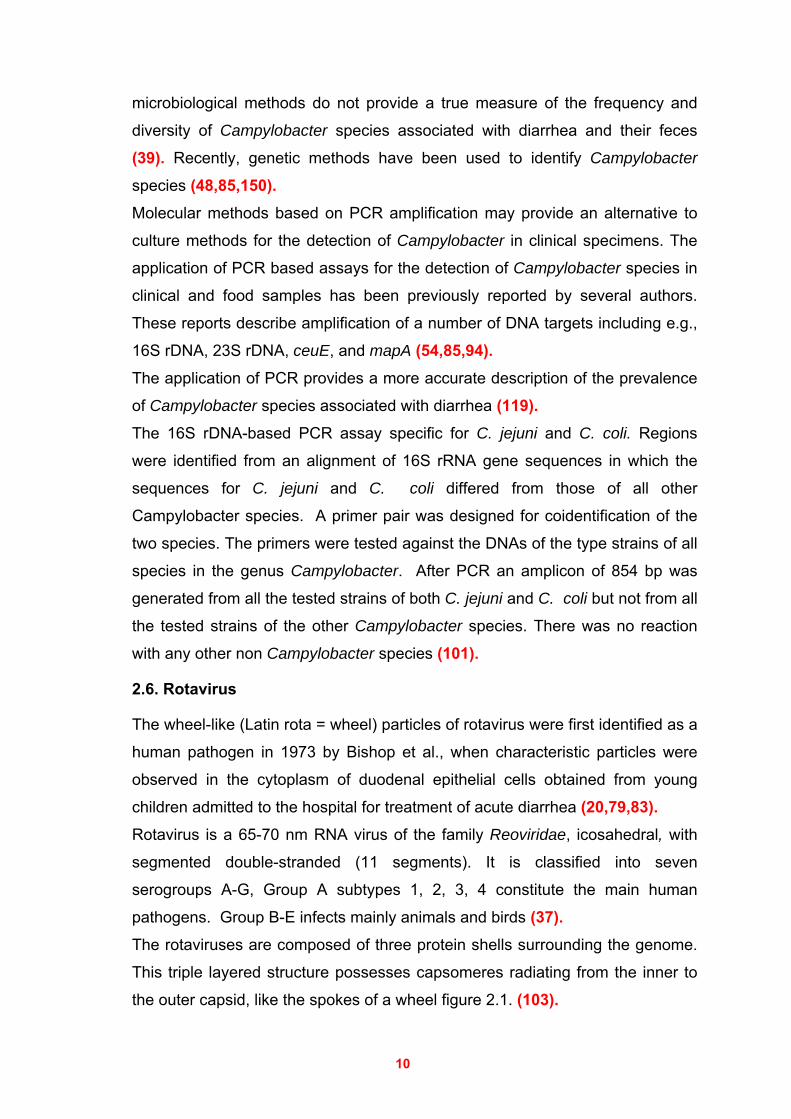
pathogens. Group B-E infects mainly animals and birds (37). The rotaviruses are composed of three protein shells surrounding the genome.
This triple layered structure possesses capsomeres radiating from the inner to
the outer capsid, like the spokes of a wheel figure 2.1. (103).
11
Figure 2.1. Rotavirus particles.
Viral pathogens account for approximately 70% of episodes of acute infectious
diarrhea in children, and rotavirus is the most commonly implicated virus. Group
A rotaviruses are responsible for 30–60% of all cases of severe watery diarrhea
in young children (26,27,122). The death rate due to rotavirus infection is responsible for 21 % for low-income
countries, 17% for low-middle income countries, 9% for high-middle income
countries, and 1 % for high-income countries (137). In temperate climates, rotavirus is the main cause of winter gastroenteritis (79), in Israel and Jordan, however, hospitalization due to rotavirus diarrhea have
been shown to occur more frequently in the summer (42,132), whereas in the
tropics it is found all the year round, with less-defined seasonal variation (131). In Gaza Palestine, Sallon et al. (1994) and Simhon et.al (1990) investigated the
etiology of diarrheal diseases in children and they found that rotavirus
represented 6.8% and 6.9%, respectively (151,161). Rotavirus was the most common organism detected in children with diarrhea in
various countries e.g., 14% in Southern Israel (42), 26.6% in Zliten, Libya (7), 28.6% in Alexandria, Egypt (140), 34.6% in Saudi Arabia (46). In Jordan,
Youssef et al. (2000) and Meqdam et al. (1997) recorded the incidence of
rotavirus as 33% and 40%, respectively (114,192).
12
Rotavirus is responsible for many cases of gastroenteritis in children as seen in
bout 42% in Argentina, 35% in Iran, 46% in Vietnam (57,118,131) and in 30-
50% of the hospitalized patients in Europe, and 16% to 36% in Turkey (9). It is not possible to distinguish diarrhea caused by rotavirus clinically, because
diarrhea, vomiting, fever, and dehydration are not absolutely associated with
rotavirus infection (87,131,195). The most commonly used tests in diagnosing rotavirus infections are electron
microscopy, latex agglutination (LA), enzyme-linked immunosorbent assays
(ELISA), polyacrylamide gel electrophoresis (PAGE), immunochromatographic
methods and molecular tests (9,29,34). Simple to use ELISA, immunochromatographic tests and latex agglutination kits
have been developed. These antigen detection systems have become the tests
of choice in the clinical settings (29,56,75).
The sensitivity and specificity rates for immunochromatography were found to
be as high as ELISA, and RT-PCR. These methods may thus be used as a
reliable test for diagnosis of rotavirus infection (29,141,160).
2.7. Parasitic Diarrhea
Several species of protozoa and helminthes can cause diarrheal disease. The
exposure to enteric parasites is more common in tropical and developing
countries. Some of the more common causes of parasitic diarrhea are
Entamoeba histolytica, Giardia intestinalis, Cryptosporidium sp, and other
intestinal parasites (152).
2.8. Enteropathogens
Wierzba et al. (2006) in Egypt studied 714 patients with diarrhea, they found
that 23% had rotavirus-associated diarrhea, 14% were ETEC-associated
diarrhea, 1.0% Campylobacter-associated diarrhea and Shigella-associated
diarrhea represented 2%. Rotavirus-associated cases presented with
dehydration, vomiting, and were often hospitalized. Children with Shigella- or
Campylobacter-associated diarrhea were reported as watery diarrhea and
rarely dysentery. ETEC did not have any clinically distinct characteristics.
Helms et al. (2006) in Denmark studied foodborne bacterial infection and
hospitalization among 52,121 patients. They found that (14.4%) were
13
hospitalized with a diagnosis of gastroenteritis. A total of (17.7%) of the
hospitalized patients with infections due to S. enterica and (10.8%) of the
infections were due to Campylobacter species.
Nguyen et al. (2005) studied the prevalence of enteric pathogens in 884
children aged less than 5 years (627 with diarrhea, 257 ages matched controls)
in Hanoi, Vietnam. A multiplex PCR was successfully developed to identify
diarrhoeagenic E. coli strains from fecal sample in a single reaction. Of the 884
processed fecal samples, 172 strains of diarrhoeagenic E. coli were identified
with the significantly higher prevalence in the diarrhea group compared to the
healthy ones. In addition, 19 Shigella strains were isolated. Imipenem,
ciprofloxacin, nalidixic acid, cefotaxime, and cefuroxime were active against E.
coli and Shigella strains, while high frequencies of resistance to ampicillin,
chloramphenicol, and trimethoprim-sulphamethoxazole were shown. Of the 884
samples, group A rotavirus was identified in 45% of the children with diarrhea,
and 3.5% in the healthy ones showing a significant difference. Within the
diarrhea group, the highest prevalence was seen in children aged 13-24
months, and in males more than in females. More than 20% of rotavirus-
infected children had association with diarrheagenic E. coli or Shigella spp.
Diniz-Santos et al. (2005) studied the epidemiological and microbiological
aspects of acute bacterial diarrhea in 260 positive stool cultures of children
between 0 and 15 years of age during two years at a pediatric tertiary care
facility in Salvador, Brazil. Bacterial strains had been presumptively identified by
culturing in selective media and by biochemical testing and their antimicrobial
susceptibility patterns were automatically detected by the MicroScan Walkaway
System. Most of the patients (42.7%) were between one and four years of age.
Shigella was the commonest pathogen, being found in 141 (54.3%) of the
cultures, while Salmonella was found in 100 (38.4%) of the cultures and
enteropathogenic E. coli in 19 (7.3%). Salmonella was the main causal agent of
diarrhea in children younger than five years old, whereas Shigella was the most
frequent pathogen isolated from the stools of children between five and 15
years old. The peaks of incidence corresponded to the periods of school
vacations. Shigella specimens presented a very high resistance rate to
14
trimethoprim-sulfamethoxazole (90.1%) and to ampicillin (22.0%), while
Salmonella presented very low resistance rates to all drugs tested.
Nimri et al. (2004) in Jordan investigated the polymicrobial infections in 220
children with diarrhea in a rural population. Potential pathogenic agents isolated
from 143 (65%) children were identified by molecular and standard
microbiological methods. Co-infections with two or more agents were detected
in 50 (35%) cases. E. coli, Shigella spp, Giardia and Entamoeba histolytica
were found to be predominant.
Amar et al. (2004) in the UK detected gastrointestinal pathogens by
microscopy, bacteriological culture, immunoassays and PCR in 92 fecal
samples of patients with community-acquired diarrhea. Conventional techniques
detected a single potential etiological agent in 15% of the samples, whereas
results of PCR detected evidence of at least one agent in 41% of the samples.
Overall, the detection rates for the different pathogens were as follows:
adenovirus serogroup F, 1%; Campylobacter spp., 7.6%; Salmonella spp., 4%;
enteroaggregative E. coli, 9.8%; enteropathogenic E. coli, 6.5%; enterotoxigenic
Clostridium perfringens, 3%; Cryptosporidium spp., 13%; and Giardia spp.,
11%. Results for the detection of Salmonella spp., Campylobacter spp. and C.
perfringens were similar by both techniques, whereas Cryptosporidium and
Giardia spp. were detected 22 times more often by PCR than by conventional
microscopy. The results of this small study clearly demonstrate the advantages
of PCR-based methods compared to conventional techniques for the detection
of gastrointestinal pathogens.
Nimri and Meqdam. (2004) in Jordan investigated the enteropathogens
associated with cases of gastroenteritis in a rural population in 180 children. All
samples were examined for parasites and bacterial pathogens by culture and
PCR. Pathogens and potential enteropathogens were identified in 140 (77.8%)
of the patients, with more than one pathogen being recovered from 67 (37.2%)
of the patients. Potentially pathogenic parasites were observed in 90 (50%)
patients; those that were associated significantly with diarrhea were Giardia
lamblia, Blastocystis hominis, Cryptosporidium spp., Entamoeba histolytica and
15
Cyclospora cayetanensis. Pathogenic bacteria were isolated from 72 (40%)
patients, and, of these, 62.5% were resistant to at least one antibiotic, and
30.6% of these were multiresistant. Diarrheagenic Escherichia coli strains were
found in 14.3% of the specimens. The most common enteropathogenic bacteria
found were Shigella spp., Campylobacter jejuni and Yersinia enterocolitica.
Vargas et al. (2004) in Tanzania investigated the etiology of diarrhea in 451
children less than five years of age, the stool specimens were divided into 348
from the dry season and 103 from the rainy season. Overall, diarrheagenic
Escherichia coli (35.7%) were the predominant enteropathogen, with
enterotoxigenic E. coli, enteroaggregative E. coli, and enteropathogenic E. coli
being the most prevalent. Moreover, enteroaggregative E. coli (63% versus
35.5%), Shigella spp. (24% versus 12%), and rotavirus (23% versus 4%) were
more prevalent in the dry season than in the rainy season and enterotoxigenic
E. coli (51.6% versus 20%) and Giardia intestinalis (14% versus 1%) were more
prevalent in the rainy season.
Schnack et al. (2003) in Brazil investigated the prevalence of enteropathogens
associated with diarrheal disease in 94 infants < 5 years old. Cryptosporidium
(85.1%) topped the list of parasite isolates, followed by Entamoeba histolytica
(56.4%) and Giardia intestinalis (4.3%). Four samples contained
enteropathogenic Escherichia coli (4.3%). Samonella and Shigella, however,
were not detected, and only one sample contained rotavirus (1.1%).
Battikhi (2002) in Jordan conducted on epidemiological study on 1400
Jordanian patients suffering from diarrhea for bacterial pathogens and Rotavirus
over a four- year period (1997-2000). Pathogenic bacteria were identified in 343
patients (24.5%), most often from children. Salmonella spp. was the most
frequently isolated organism in 10.7% of the patient's cultures, followed by
enteropathogenic Escherichia coli (EPEC) in 3.9%, Shigella spp. in 0.8% and
Campylobacter spp. in 0.9%. Resistance to ampicillin was observed in 42.2% of
the Salmonella, 77.0% of the Shigella, and 31.0% of the EPEC isolates.
Cotrimoxazole resistance was observed in 34.0% of the Shigella and 13.0% of
16
the EPEC isolates and 77.0% of Campylobacter isolates. Rotavirus was
identified in 373 (26.6%) of the samples.
Souza et al. (2002) in Sao Paulo (Brazil) studied the etiologic profile of acute
diarrhea in 154 children aging less than 5 years.
Intestinal pathogens were detected in 112 (72.8%) cases. The association of
two or more intestinal pathogens occurred in 47 (30.5%) cases.
The pathogens identified were, rotavirus: 32 (20.8%), bacteria: 53 (34.4%),
both: 25 (16.2%), and 2 (1.4%) with Giardia intestinalis (in one case associated
with rotavirus and in another one associated with bacteria).
Altogether, there were 105 bacterial isolates; 90 were Escherichia coli (EPEC
27, DAEC 24, ETEC 21 and EAEC 18), 12 were Shigella sp, 2 were Salmonella
sp, and one was Yersinia sp. Children with mixed infections (viral and bacterial)
had increased incidence of severe vomiting, dehydration and hospitalization.
Ballal and Shivananda (2002) in India investigated the occurrence of rotavirus
and enteric pathogens in infantile diarrhea. Rotavirus in the feces has been
detected by Latex agglutination and accounted for 19.6% of the diarrhea with
maximum incidence (65%) in the 7-12 months age group. Bacterial etiological
agents continued to play a significant role (69.6%) in diarrheal diseases.
Enteroaggregative E. coli was common in the age group 25-36 months,
shigellosis in the 37-60 months group and Salmonella typhimurium enteritis in
the 7-12 months of age. The other pathogens isolated were vibrio cholerae
(4.98%), species of Aeromonas (15.92%), along with Cryptosporidium (6.47%)
and Candida albicans (3.98%).
Khan et al. (2002) in Bangladesh investigated the trend in isolation of Vibrio
cholerae, Shigella, and Salmonella in neonates with diarrhea. The study
population included 240 neonates who were admitted with acute diarrhea and
other medical complications to the inpatient department of large Hospital,
Dhaka, Bangladesh, in 2001. A single enteric pathogen was detected in 71
(29.5%), and multiple pathogens were detected in 12 (5%) of the neonates.
17
Enteropathogens identified were as follows: V. cholerae O1 (17.5%), Shigella
spp. (9.1%), Salmonella spp. (3.3%), Aeromonas spp. (3.7%), and Hafnia alvei
in (0.8%) of the neonates.
Urio et al. (2001) in Gaborone, Botswana investigated the Shigella and
Salmonella strains isolated from 221 children under 5 years, and their antibiotic
susceptibility patterns. They isolated Shigella from (21%) and Salmonella (3%).
S. boydii (13%) was the most prevalent Shigella species followed by S. flexneri
(6%) and S. sonnei (2%). Salmonella species were S. typhimurium and S.
paratyphi. Antibiograms of the predominant isolates showed that most Shigella
species were resistant to ampicillin but susceptible to chloramphenicol. The
Salmonella species were susceptible to chloramphenicol, collistin-sulphate,
gentamicin, cotrimoxazole, and ampicillin.
El-Sheikh and, El-Assouli. (2001) investigated the prevalence of viral,
bacterial and parasitic enteropathogens among young children with acute
diarrhea in Jeddah, Saudi Arabia, in 576 fecal samples collected from children
<5 years old suffering from acute diarrhea and attending hospitals and
outpatient clinics. One or more enteropathogens were identified in 45.6% of the
stool specimens. Mixed infections were detected in 12.2% of the diarrheal
cases. Rotavirus was detected in 34.6% of the specimens of the hospitalized
patients and in 5.9% of the specimens of the outpatients. Other etiologic agents
recognized included E. coli (13%), of which 3.8% were enteropathogenic E. coli
(EPEC) and 1.9% enterohaemorrhagic E. coli. Other detected pathogens were:
Klebsiella pneumoniae (4%), Giardia intestinalis (3.1%), Salmonella sp. (3%),
Shigella flexneri (2.6%), Entamoeba histolytica (2.2%), Trichuris trichiura,
Hymenolepis nana, and Ascaris lumbricoides (0.7% each), and Candida
albicans (0.5%).
Orlandi et al. (2001) in Brazil, investigated the prevalence of enteropathogens
associated with diarrheal disease in 130 infants living in the poor urban areas of
Porto Velho, Rondonia. 80% of diarrheal cases were observed in the groups
under 2 years of age. Rotavirus (19.2%) was the most frequent enteropathogen
associated with diarrhea, followed by Shigella flexneri (6.15%) and S. sonnei
18
(1.5%) and Salmonella sp. (6.9%). Enterotoxigenic E. coli infections (3.1%),
enteropathogenic E. coli (2.3%), enteroinvasive E. coli (0.8%) and Yersinia
enterocolitica (0.8%). Mixed infections were frequent, associating rotavirus,
EPEC and Salmonella sp. with Entamoeba histolytica and Giardia intestinalis.
Ono et al. (2001) in Nepal, studied the seasonal distribution of
enteropathogens detected from diarrheal stool samples. A total of 334 diarrheal
fecal samples (from 210 males and 124 females) collected in Kathmandu,
Nepal, were studied for various kinds of enteropathogens. Overall, 33%
(111/334) of the fecal samples were positive for one or more enteropathogens.
Enteropathogen detection rates in summer, winter, spring, and autumn were
61% (40/66), 52% (45/87), 31% (25/81), and 25% (25/100), respectively.
Altogether eight species of bacteria, three types of viruses, and five species of
protozoan parasites were detected with considerable seasonal variations.
Among the bacterial isolates, enteropathogenic Escherichia coli topped the list
followed by Vibrio sp. Only one sample had Shigella (S. sonnei). Rotavirus type
A was the most frequently detected among the enteric viruses, followed by
human enterovirus and human adenovirus, respectively. Among the enteric
protozoan parasites, Giardia intestinalis was the most frequently detected
followed by Cryptosporidium parvum. Detection of bacterial and protozoan
pathogens showed a slightly high tendency in the summer season compared
with that in the other seasons, whereas the detection of viruses was significantly
higher in the winter season.
Youssef et al. (2000) in Jordan investigated the incidence of enteric pthogens
in 265 children with gastroenteritis by PCR & conventional methods; they
detected enteropathogens in 66.4% of the examined patients. A single enteric
pathogen was detected in 50.9% of the children, and multiple pathogens were
detected in 15.5%. The prevalence of enteropathogens identified was as
follows: rotavirus (32.5%), enteropathogenic Escherichia coli (12.8%),
enteroaggregative E. coli (10.2%), enterotoxigenic E. coli (5.7%), Shigella spp.
(4.9%), Entamoeba histolytica (4.9%), Salmonella spp. (4.5%), Campylobacter
jejuni/coli (1.5%), Cryptosporidium spp. (1.5%), enteroinvasive E. coli (1.5%),
Giardia intestinalis (0.8%) and Yersinia enterocolitica (0.4%). No Vibrio
19
cholerae, Shiga toxin-producing E. coli, microsporidia, adenovirus or small
round viruses were detected.
Wasfy et al. (2000) in Egypt investigated the incidence, isolation and antibiotic
susceptibility of Salmonella, Shigella, and Campylobacter from acute enteric
infections in 6,278 patients, presenting to the Abbassia Fever Hospital.
Their results showed that Salmonella predominated, totalling 465 isolates,
followed by Shigella with 258 isolates, and Campylobacter with 146 isolates. Of
the Shigella isolates, 124 were Shigella flexneri, 49 were S. sonnei, 47 were S.
dysenteriae (mainly serotype 1, 2, and 3), and 38 were S. boydii.
Campylobacter spp. comprised 92 Campylobacter jejuni and 54 C. coli isolates.
Isolation of Salmonella was highest during the months of February-March,
June-July, and October- November, while that of Shigella was maximal on July
to October. Isolation of Campylobacter increased during May-June and again
during August-October. Although Salmonella was sensitive to amikacin,
aztreonam, ceftriaxone, and nalidixic acid, it was, however, resistant to
erythromycin, streptomycin, ampicillin, chloramphenicol, and tetracycline.
Shigella (>80%) was sensitive to amikacin, ceftriaxone, cephalothin,
sulphamethoxazole-trimethoprim (except S. sonnei), aztreonam, and nalidixic
acid. Resistance (>50%) was noted only for ampicillin, chloramphenicol, and
tetracycline. C. jejuni and C. coli were resistant to cephalothin, aztreonam, and
streptomycin. Some of the above antibiotics were employed to characterize the
Egyptian isolates, but did not have any clinical utility in the treatment of
diarrhea. Significant differences (p<0.05) were observed in the resistance
profiles of Shigella and Salmonella between late 1980s and early 1990s. The
results suggest the use of fluoroquinolones or a third-generation cephalosporin
as an empirical treatment of enteric diseases. However, alternative control
strategies, including the aggressive development of broadly protective vaccines,
may be more effective approaches to curbing morbidity and mortality due to
acute enteric infections.
Shubair et al (2000) studied the Palestinian intestinal parasites and diarrhea, in
children. The intestinal parasites were found to be prevalent in Gaza, with an
overall prevalence of 24.5%. Giardia intestinalis (62.2%) was the most common
20
parasite, followed by Ascaris Iumbricoides (20.0%), then Entamoeba histolytica
(18.0%).
Shallow et al. (2000) in USA studied the regional variation in the incidence of
laboratory-confirmed bacterial foodborne illnesses. In this study 12,125 cases
were identified.The incidence per 100,000 population was highest for
Campylobacter (15.7%), followed by Salmonella (14.4%), and Shigella (7.9%).
Lower incidences were reported for E. coli O157 (2.1%), Yersinia (0.4%),
Listeria (0.3%) and Vibrio (0.2%). The incidence of Campylobacter and
Salmonella among infants proved particularly high, although substational
regional variations were observed.
Albert et al. (1999) in Bangladesh investigated the enteropathogens associated
with childhood diarrhea, in 814 cases of diarrhea, 0 to 5 years of age. A
potential enteric pathogen was isolated from 74.8% of diarrheal children.
The study identified these pathogens as being significantly associated with
diarrhea; the study identified the enteropathogenic E. coli, Aeromonas spp., V.
cholerae O139, enterotoxigenic Bacteroides fragilis, Clostridium difficile, and
Cryptosporidium parvum, as being significantly associated with diarrhea.
Plesiomonas shigelloides, Salmonella spp., diffusely adherent E. coli,
enteroaggregative E. coli, Entamoeba histolytica, and Giardia lamblia were not
significantly associated with diarrhea. The major burden of diseases due to
most pathogens occurred in the first year of life, and infections with multiple
pathogens were common.
Yoshida et al. (1998) in Japan studied the bacteriological and virological
etiologies of sporadic acute gastroenteritis in 1,564 samples, 722 (46.2%) were
enteropathogen positive cases, and mixed infection was observed in about 15%
of the positive cases. Among 13 different kinds of enteropathogens identified,
the most prevalent one was pathogenic E. coli (20.7%), followed by
Campylobacter spp. (10.0%), rotavirus (8.8%), Salmonella spp. (3.9%),
adenovirus (1.9%), ECHO virus (0.9%), Vibrio parahaemolyticus (0.8%),
poliovirus (0.7%), Aeromonas spp. and Coxsackie B virus (both 0.6%). In
addition, Shigella sonnei (3 cases), S. paratyphi-A (1 case) and
21
enterohemorrhagic E. coli O157: H7 (2 cases) were also detected. A higher
detection ratio was recorded in February, August and November, reflecting
respectively by month a higher frequency of Rotavirus and food-poisoning
causing enteric bacteria.
Rohner et al. (1997) in Switzerland studied the etiological agents of infectious
diarrhea. A total of 13,965 specimens from 7,124 patients (1.96 specimens per
patient) were cultured, yielding 369 (2.6%) Salmonella spp., 408 (2.9%)
Campylobacter spp., and 79 (0.6%) Shigella spp. The cumulative positivity rate
of 6.1% decreased to 2.7% when patients received antimicrobial agents. The
positivity rate for 5,912 specimens obtained from patients hospitalized for <3
days was 12.6%, whereas it dropped to 1.4% for patients hospitalized for >3
days. Of 3,837 stool samples originating from pediatric patients, 8.8% were
positive, and 5.1% of 10,128 samples from adults were positive. Rotaviruses
were detected in 190 of 1,601 (11.9%) samples.
Lerman et al. (1994) in Israel studied the epidemiology of acute diarrheal
diseases in children. A total of 284 diarrheal fecal samples were studied for
various enteropathogens, they isolated enteropathogens in 40% of the diarrheal
episodes from which stool cultures were obtained. The identification rates of the
various enteropathogens were: diarrheagenic Escherichia coli, 11%; Shigella
spp., 10%; Giardia lamblia, 10%; Salmonella spp., 4%; Staphylococcus aureus,
3%; Campylobacter jejuni, 1%. Children less than 12 months of age had a lower
incidence of acute diarrheal diseases during the months they were being
breast-fed than children that were fed with formula during the same period. And
also in Israel Finkelstein et al. (2002) evaluated the impact of a serious
bacterial etiology in clinical dysentery in hospitalized children and determined if
children at high risk could be identified on the basis of clinical or laboratory
parameters. The study population included 60 children admitted to the hospital
with clinical dysentery over a 16-month period. Stool cultures were positive for
Shigella spp. in 18 children (30%), and Salmonella spp. in 15 children (25%),
Campylobacter jejuni was identified in one patient (2%). There were no
significant differences in clinical characteristics or laboratory parameters
between children with positive and negative stool cultures.

22
Na'was and, Abo-Shehada. (1991) in Jordan carried out a study on the
bacterial and parasitic causes of acute diarrhea in Northern Jordan in 200
patients. One or more bacterial or parasitic enteropathogens were isolated from
79 patients (39.5%). Prevalence rates for these pathogens were as follows:
enterotoxigenic Escherichia coli, 9%; enteropathogenic E. coli, 9%; Salmonella
spp. 7%; Campylobacter spp, 5.5%; Yersinia enterocolitica, 4.5%; Shigella spp,
4%; Aeromonas spp, 3.5%; enterotoxigenic Clostridium perfringens, 2%; Vibrio
spp, 2%; and Plesiomonas shigelloides, 0.5%. Both Giardia intestinalis and
Entamoeba histolytica were detected in 2% of the stool samples examined.
2.9. Detection and identification of enteropathogens by PCR
The use of PCR for detecting and identifying enteric pathogens is rapid and
easy while the conventional identification methods are not only time consuming,
but also require an experienced laboratory technician to isolate and identify
bacterial colonies accurately. Studies in several parts of the world have shown
that the sensitivity and specificity of a direct PCR method for the detection of
enteric pathogens in stool samples is quite high when compared with
conventional methods (90,91,93,98,177). Naravaneni and Jamil (2005) in India employed PCR-based techniques for the
rapid detection of food-borne pathogens by using molecular techniques. Salmonella and Escherichia coli were undertaken. Suitable primers were
designed based on specific genes fimA of Salmonella and gene afa of
pathogenic E. coli for amplification. This study has established that fimA and afa
primers were specific for detecting Salmonella and pathogenic E. coli,
respectively, in the environmental samples. Thus a rapid, sensitive and reliable
technique for the detection of Salmonella and pathogenic E. coli was
developed.
Lukinmaa et al. (2004) in Finland studied the application of molecular genetic
methods in the diagnosis and epidemiology of food-borne bacterial pathogens.
Salmonella enterica, Campylobacter and Yersinia species, Shiga toxin-
producing Escherichia coli (STEC), Listeria monocytogenes and Clostridium

23
perfringens were the bacterial pathogens constituting the greatest burden of
food-borne disease in Finland. Several molecular genetic methods have been
applied to diagnose, discriminate and survey these bacteria. PCR, PCR-RFLP
(Restriction Fragment Length Polymorphism) and PFGE (Pulsed Field Gel
Electrophoresis) are the most widely and successfully used. However, these
methods are unable to replace conventional and internationally standardized
phenotyping methods.
Iijima et al. (2004) in Japan improved the detection rate of diarrheagenic
bacteria in human stool specimens by a rapid real-time PCR assay. A rapid
laboratory system has been developed and evaluated for its ability to
simultaneously identify major diarrheagenic bacteria, including Salmonella
enterica, Vibrio parahaemolyticus, Campylobacter jejuni and Shiga toxin-
producing Escherichia coli, in stool specimens by real-time PCR. Specific
identification was achieved by using selective TaqMan probes, detecting two
targets in each pathogen. A positive result was scored only when both targets of
a pathogen were amplified and the difference between threshold cycles for
detection was less than five. Diagnosis of enteric bacterial infections using this
highly sensitive method, including DNA extraction and real-time PCR, requires
only 3 h. Forty stool specimens related to suspected food poisoning outbreaks
were analyzed: 16 (40%) of these samples were found to be positive for
diarrheagenic bacteria using a conventional culture method; while 28 (70%)
were positive using the real-time PCR assay. Of the 12 PCR-positive but
culture-negative cases, 11 patients had consumed pathogen-contaminated or
high-risk food. Analysis of fecal samples from 105 outpatients who complained
of diarrhea and/or abdominal pain identified 19 (18%) patients as being positive
for diarrheagenic bacteria using the culture method. An additional six (6%)
patients were found to be positive by PCR analysis.
Li et al. (2004) in China studied the detection and identification of enteric
pathogens using PCR. A set of conventional PCR assays were applied to detect
and identify Salmonella, Shigella, and E. coli O157:H7 directly from pure
cultures and fecal samples. Shigella primers were derived from ipaH gene
coding for invasive plasmid relative antigen and which exists on both plasmid

24
and the genome. The primers of Salmonella were designed from the 16S rDNA
sequence. The primers of E. coli O157:H7 were taken from eaeA gene. The
detection system included common PCR, semi-nested PCR and RAPD
(Random amplified polymorphic DNA).This method was more sensitive, specific
and efficient and its processing was rapid and simple. For example, the method
could be used to specifically detect and identify Salmonella, Shigella, and E. coli
O157:H7, and its sensitivity ranged from 3 to 50 Colony Forming Unit (CFU),
and its detection time was 4 hours. This PCR method, therefore, can serve as a
routine and practical protocol for detecting and identifying pathogenic
microorganisms from clinical samples.
Hong et al. (2004) in China improved an application of oligonucleotide array
technology for the rapid detection of pathogenic bacteria of foodborne
infections.
A rapid and accurate method for detection of common pathogenic bacteria in
foodborne infections was established by using oligonucleotide array technology.
Nylon membrane was used as the array support. A mutation region of the 23S
rDNA gene was selected as the discrimination target from 14 species of
bacteria causing foodborne infections and two unrelated bacterial species. A
pair of universal primers was designed for PCR amplification of the 23S rDNA
gene. Twenty-one species specific oligonucleotide detection probes were
synthesized and spotted onto the nylon membranes. The 23S rDNA gene
amplification products of 14 species of pathogenic bacteria were hybridized to
the oligonucleotide array. Hybridization results were analyzed with digoxigenin-
linked enzyme reaction. Results indicated that nine species of pathogenic
bacteria (Escherichia coli, Campylobacter jejuni, Shigella dysenteriae, Vibrio
cholerae, Vibrio parahaemolyticus, Proteus vulgaris, Bacillus cereus, Listeria
monocytogenes and Clostridium botulinum) showed high sensitivity and
specificity for the oligonucleotide array. Two other species (Salmonella enterica
and Yersinia enterocolitica) gave weak cross-reaction with E. coli, but the
reaction did not affect their detection. After redesigning the probes, positive
hybridization results were obtained with Staphylococcus aureus, but not with
Clostridium perfringens and Streptococcus pyogenes. The oligonucleotide array
can also be applied to samples collected in clinical settings of foodborne
25
infections. The superiority of oligonucleotide array over other tests lies on its
rapidity, accuracy and efficiency in the diagnosis, treatment and control of
foodborne infections.
Fukushima et al. (2003) in Japan studied the use of duplex real-time SYBR
(SYNERGY BRANDS) Green PCR assays for detection of 17 species of food- or
waterborne pathogens in stools.
The 17 species of food- or waterborne pathogens examined were
enteroinvasive Escherichia coli, enteropathogenic E. coli, enterohemorrhagic E.
coli, enterotoxigenic E. coli, enteroaggregative E. coli, Salmonella spp., Shigella
spp., Yersinia enterocolitica, Yersinia pseudotuberculosis, Campylobacter
jejuni, Vibrio cholerae, Vibrio parahaemolyticus, Vibrio vulnificus, Aeromonas
spp., Staphylococcus aureus, Clostridium perfringens, and Bacillus cereus. The
detection levels were approximately 105 food or waterborne pathogenic bacteria
per g of stool. The protocol for processing stool specimens for less than 104
food- or waterborne pathogenic bacteria per g of stool required an overnight
enrichment step to achieve adequate sensitivity. However, the rapid
amplification and reliable detection of specific genes of greater than 105 food or
waterborne pathogenic bacteria per gram samples should facilitate the
diagnosis and management of food- or waterborne outbreaks.
Leushner and Kelly (2001) in Canada studied the detection of pathogenic
enteric bacteria in stool by multiplex PCR. They detected 4 species (the most
common causes of bacterial diarrhea) i.e., Salmonella, Shigella, Campylobacter
spp., and E. coli O157:H7 by multiplex PCR in the same reaction tube.
Sharma and Carlson (2000) in the US studied the simultaneous detection of
Salmonella strains and Escherichia coli O157:H7 with fluorogenic PCR and
single-enrichment-broth culture. A multiplex fluorogenic PCR assay for
simultaneous detection of pathogenic Salmonella strains and Escherichia coli
O157:H7 was developed and evaluated for use in detecting very low levels of
these pathogens in meat and feces. Two sets of primers were used to amplify a
junctional segment of virulence genes sipB and sipC of Salmonella and an
intragenic segment of gene eae of E. coli O157:H7. Fluorogenic reporter probes

26
were included in the PCR assay for automated and specific detection of
amplified products. The assay could detect <10 CFU of Salmonella enterica
serovar Typhimurium or E. coli O157:H7 per g of meat or feces artificially
inoculated with these pathogens and cultured for 6 to 18 h in a single
enrichment broth. Detection of amplification products could be completed in <4
hour after enrichment.
Vidal et al. (2004) in Chile employed multiplex PCR for the diagnosis of enteric
infections associated with diarrheagenic Escherichia coli, Vanniasinkam et al. (1999) in Australia used PCR for the detection of Campylobacter spp. in clinical
specimens, Gilbert et al. (2003) in USA developed a triplex PCR assay for the
specific detection of Campylobacter jejuni, Salmonella spp., and Escherichia
coli O157:H7 from food, Matar et al. (2002) in Lebanon conducted a multiplex-
PCR-based detection and genotyping of diarrhoeagenic Escherichia coli in
diarrhoeal stools, Kumar et al. (2003) in India investigated the Salmonella spp.
in tropical seafood by PCR, Alvarez et al (2004) in Spain, developed a
multiplex PCR technique for the detection and the epidemiological typing of
Salmonella in human clinical samples. More studies have showen the
importance of PCR for detection of many enteropathogens e.g., Kulkarni et al, (2002) and Lawson et al. (1999) studies on Campylobacter, in Dutta et al, (2001) and Islam et al (1998) investigations on Shigella, Feder et al, (2001)
and Kurowski et al. (2002) reports on Salmonella, Beutin et al, (2004) and
Cubbon et al, (1996) work on Escherichia coli O157:H7.
Actually, several studies have shown that PCR techniques are far more
sensitive and specific than culture methods in detecting various
enteropathogens and efficient and its processing was rapid and simple.
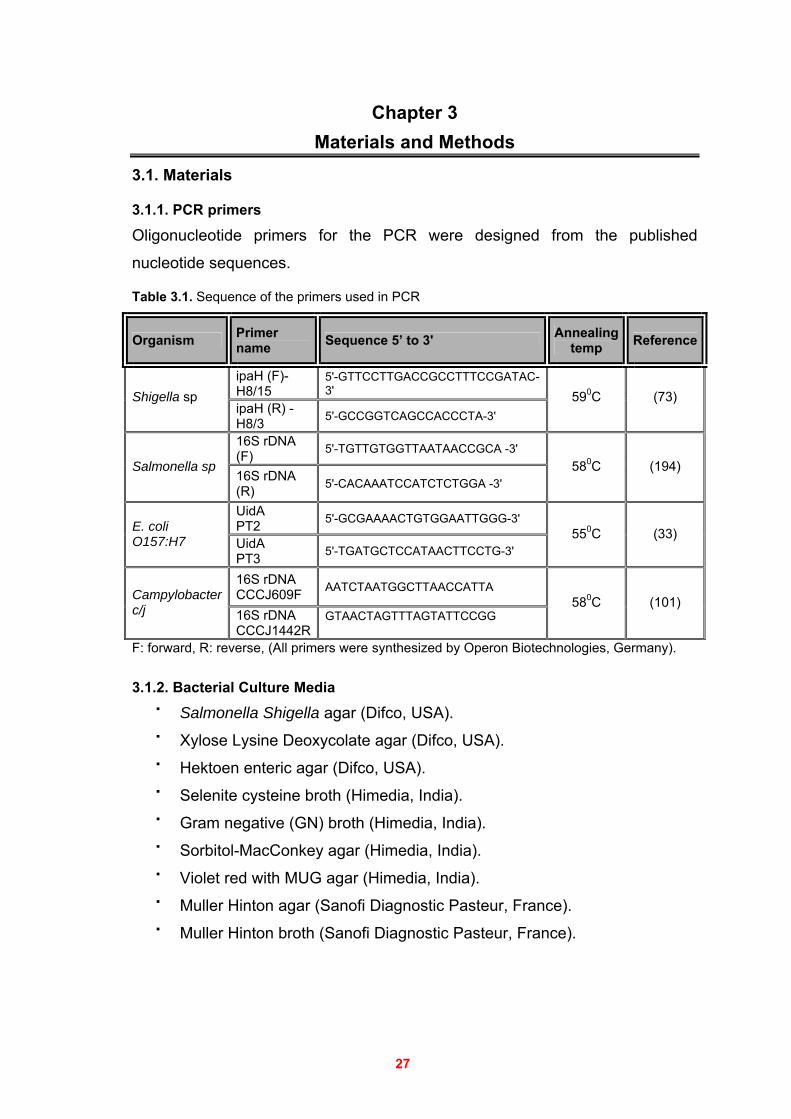
27
Chapter 3 Materials and Methods
3.1. Materials
3.1.1. PCR primers
Oligonucleotide primers for the PCR were designed from the published
nucleotide sequences.
Table 3.1. Sequence of the primers used in PCR
Organism Primer name Sequence 5’ to 3' Annealing
temp Reference
ipaH (F)- H8/15
5'-GTTCCTTGACCGCCTTTCCGATAC-3' Shigella sp
ipaH (R) - H8/3 5'-GCCGGTCAGCCACCCTA-3'
590C (73)
16S rDNA (F) 5'-TGTTGTGGTTAATAACCGCA -3'
Salmonella sp 16S rDNA (R) 5'-CACAAATCCATCTCTGGA -3'
580C (194)
UidA PT2 5'-GCGAAAACTGTGGAATTGGG-3' E. coli
O157:H7 UidA PT3 5'-TGATGCTCCATAACTTCCTG-3'
550C (33)
16S rDNA CCCJ609F AATCTAATGGCTTAACCATTA Campylobacter
c/j 16S rDNA CCCJ1442R
GTAACTAGTTTAGTATTCCGG
580C (101)
F: forward, R: reverse, (All primers were synthesized by Operon Biotechnologies, Germany).
3.1.2. Bacterial Culture Media
Salmonella Shigella agar (Difco, USA).
Xylose Lysine Deoxycolate agar (Difco, USA).
Hektoen enteric agar (Difco, USA).
Selenite cysteine broth (Himedia, India).
Gram negative (GN) broth (Himedia, India).
Sorbitol-MacConkey agar (Himedia, India).
Violet red with MUG agar (Himedia, India).
Muller Hinton agar (Sanofi Diagnostic Pasteur, France).
Muller Hinton broth (Sanofi Diagnostic Pasteur, France).
28
3.1.3. Reagents and Materials
Gram stain (Industrias Aulabor S.A. Spain)
Oxidase test (Hy.laboratories Ltd, Israel)
Agarose Molecular Biology grade (Promega, USA)
DNA molecular weight marker 100 (Promega, USA)
dNTPs: (dATP, dCTP, dGTP and dTTP) (Promega, USA)
EDTA disodium salt (Promega, USA).
Absolute Ethanol (Sigma, USA)
Ethidium bromide (Promega, USA).
Absolute Isopropanol (Sigma, USA)
Pipettes Research (Eppendrof)
Tris base[hydroxymethyl aminomethane (Promega, USA)
Acetic acid (Sigma, USA)
DNAse, RNAse free Water (Promega, USA).
Microfuge tubes - 1.5 mL capacity.
Microfuge tubes for PCR - thin wall 0.2 mL and 0.5 mL capacity PCR buffer, MgCl2 (Euroclone - Italy) .
Antibiotic disks (Oxoid Ltd, UK)
Bacterial positive control
3.1.4. Enzymes
Taq DNA polymerase, (Euroclone, Italy) .
3.1.5. Commercial Kits
Rotavirus detection (RotaStick one step test kit - Novamed Ltd.,
Jerusalem)
The API-20E test kit (bioMerieux, Inc., France)
Hy.enterotest (Hy.laboratories Ltd, Israel)
Anti-Shigella agglutination sera (BIORAD, France)
Anti Salmonella agglutination sera (BIORAD, France)
Anti E. coli O157:H7 Latex Test Kit (Plasmatic, UK)
AccuPrep Stool DNA Extraction Kit (Bioneer, Korea)
29
3.1.6. Apparatus and Equipments
Thermal Cycler (Eppendrof Mastercycler Personal ) .
L.G. Microwave Oven.
Hoefer Shortwave UV Light Table (Transilluminator)
Digital Camera
Vortex Mixer.
Power Supply (Biorad)
Micro Centrifuge
Freezer , Refrigerator
Electrophorosis Tank
Petri dishes
Incubator
Spectrophotometer UV-Vis
Water Bath
Weight Mod.
Microscope
Computer
3.2. Study population
During the peak of diarrheal season (May-August of 2005), 150 children up to 5
years of age who were admitted with acute diarrheal diseases to ElNasser
Pediatric Hospital Gaza, were enrolled in the study. Diarrhea was defined as
the passage of three or more loose or watery stools in the preceeding 24 hours.
A questionnaire was completed for each patient containing the following
information: age, gender, address, clinical data, fever, vomiting, dehydration
status and previous hospitalization.
Vomiting was defined as the forceful expulsion of gastric contents occurring at
least once in a 24 hours period. Fever was defined as an under arm measured
temperature > 37.2°C, and dehydration level was assessed following the
recommendations of WHO Program for Control of Diarrheal Diseases and was
done by the pediatricians (59,129). After the informed consent was obtained from the parents of the subjects, a
pediatrician filled out the information relevant to clinical symptoms and illness
onset on a standardized questionnaire, the rest of the questionnaire was filled
30
by the parents of the children, refer to Appendix A for a complete listing of the
items on this questionnaire.
3.2.1. Sample collection
Fecal samples (one per each subject), from children with diarrhea were
collected as soon as the children were admitted to the ElNasser pediatric
Hospital Gaza by the help of their parents.
Each stool specimen was collected in a special container, kept at 4°C, and
processed within 3 hours for collection. The residual of each sample, after the
first culture on the media, immunoassay and microscopy, was kept at -70°C for
further work e.g., DNA extraction, and PCR analysis
3.2.2. Ethical Considerations
An authorization to carry out the study was obtained from Helsinki (Declaration
of Helsinki the most widely accepted guideline on medical research involving
human subjects) using an agreement letter prepared from the Islamic university
of Gaza. Parents gave their consent for participation in the study and all the
information that were obtained about the subjects as well as the parents were
kept confidential; refer to Appendix B for more details.
3.2.3. Data Analysis
The data was entered, sorted and analyzed by a personal computer using
SPSS 8.0 statistical package, differences in proportions were assessed by a
Chi-square test, P values <0.05 were considered statistically significant.
3.3. Parasites detection
A smear of fecal specimens with 0.9% saline was examined microscopically for
the presence of leukocytes, red blood cells and parasites. In addition, stool
samples were examined in iodine wet mounts. Slides were scanned by light
microscopy at 100 X and 400 X magnifications.
31
3.4. Rotavirus detection
Stool samples were analyzed for group A rotavirus using RotaStick one step
test kit for determination of rotavirus in human feces (Novamed Ltd., Jerusalem)
following the manufacturer's instructions.
3.4.1. Principle of the procedure
The principle of the kit depends on a rapid immunochromatographic test for the
qualitative screening of human fecal samples for detecting the presence of
rotavirus antigen.
In brief, 0.1 g of stool specimen was added to 0.6 ml of buffer solution in a test
tube. The content of test tube was then mixed vigorously by vortex to suspend
the specimen. After sedimentation of large particles to the bottom of the tube (2-
5 min), the dipstick test strip was placed vertically into the sample tube and
removed after 10 seconds or when the fluid had reached the middle of the test
area of the dipstick. The test strip contains a mobile monoclonal rabbit origin
anti-Rotavirus antibody conjugated to colloidal gold particles. Then, a
polyclonal rabbit origin anti-rotavirus antibody is immobilized in the test area of
the strip. If the stool sample extract contains rotavirus antigens, these form
antigen antibody complexes with the gold particles. These complexes migrate
along the dipstick to the immobilized capture antibody, and a positive test band
becomes visible. An immobilized anti-rabbit antibody captures the remaining
conjugate, forming a control band, which indicates proper performance of the
test procedure. The test is judged positive when, in addition to the control band,
a clearly distinguishable purple band becomes visible in the test window. This
second band works as an internal control and indicates proper performance of
the test. Figure 3.1 below illustrates the interpretation of results.
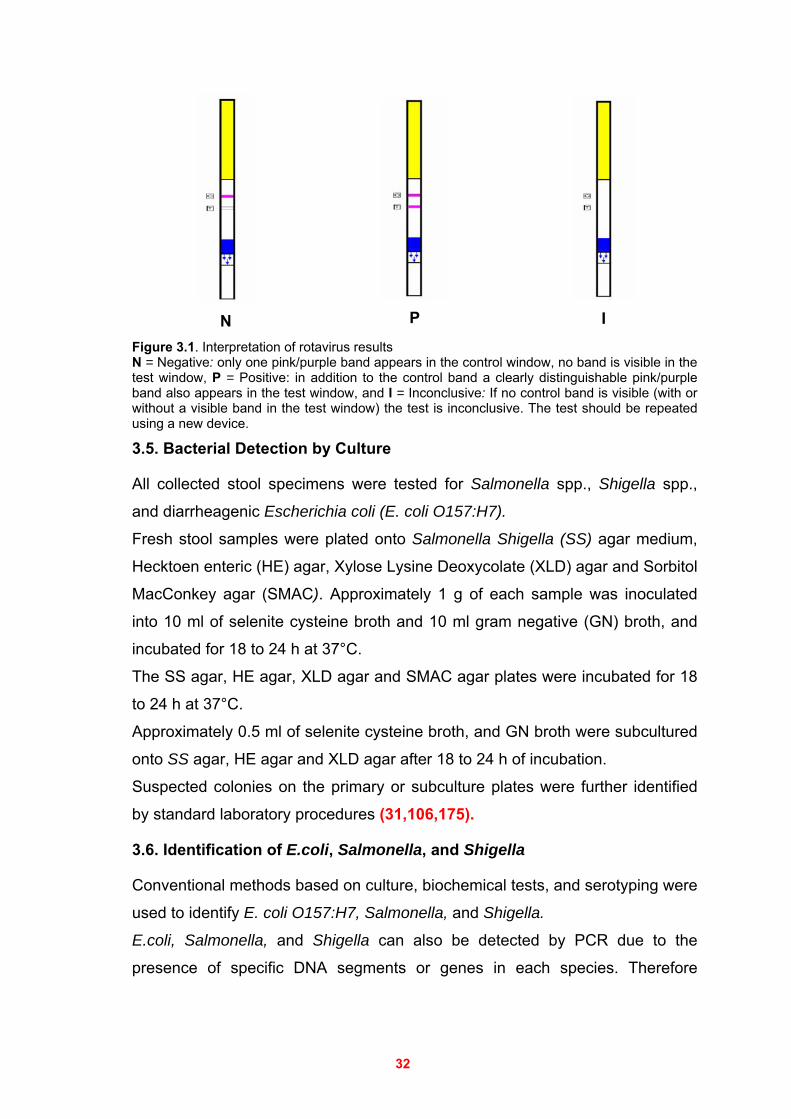
32
N
P
I
Figure 3.1. Interpretation of rotavirus results N = Negative: only one pink/purple band appears in the control window, no band is visible in the test window, P = Positive: in addition to the control band a clearly distinguishable pink/purple band also appears in the test window, and I = Inconclusive: If no control band is visible (with or without a visible band in the test window) the test is inconclusive. The test should be repeated using a new device.
3.5. Bacterial Detection by Culture
All collected stool specimens were tested for Salmonella spp., Shigella spp.,
and diarrheagenic Escherichia coli (E. coli O157:H7).
Fresh stool samples were plated onto Salmonella Shigella (SS) agar medium,
Hecktoen enteric (HE) agar, Xylose Lysine Deoxycolate (XLD) agar and Sorbitol
MacConkey agar (SMAC). Approximately 1 g of each sample was inoculated
into 10 ml of selenite cysteine broth and 10 ml gram negative (GN) broth, and
incubated for 18 to 24 h at 37°C.
The SS agar, HE agar, XLD agar and SMAC agar plates were incubated for 18
to 24 h at 37°C.
Approximately 0.5 ml of selenite cysteine broth, and GN broth were subcultured
onto SS agar, HE agar and XLD agar after 18 to 24 h of incubation.
Suspected colonies on the primary or subculture plates were further identified
by standard laboratory procedures (31,106,175).
3.6. Identification of E.coli, Salmonella, and Shigella
Conventional methods based on culture, biochemical tests, and serotyping were
used to identify E. coli O157:H7, Salmonella, and Shigella.
E.coli, Salmonella, and Shigella can also be detected by PCR due to the
presence of specific DNA segments or genes in each species. Therefore
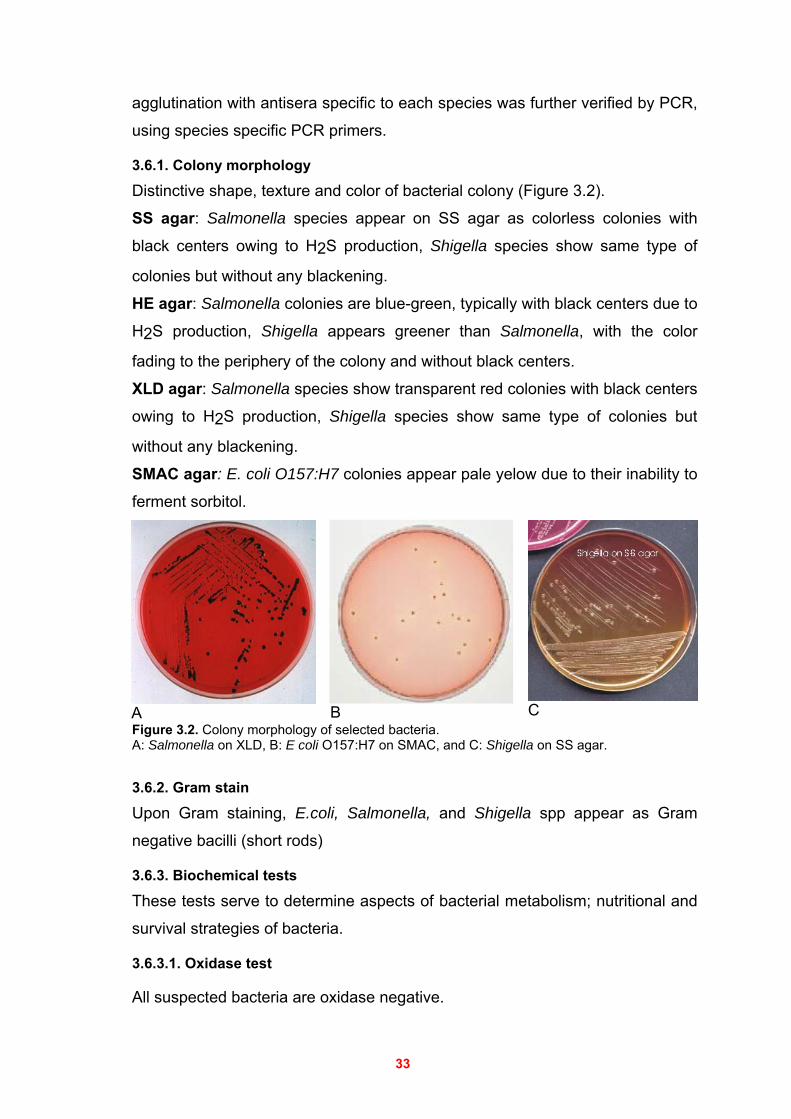
33
agglutination with antisera specific to each species was further verified by PCR,
using species specific PCR primers.
3.6.1. Colony morphology
Distinctive shape, texture and color of bacterial colony (Figure 3.2).
SS agar: Salmonella species appear on SS agar as colorless colonies with
black centers owing to H2S production, Shigella species show same type of
colonies but without any blackening.
HE agar: Salmonella colonies are blue-green, typically with black centers due to
H2S production, Shigella appears greener than Salmonella, with the color
fading to the periphery of the colony and without black centers.
XLD agar: Salmonella species show transparent red colonies with black centers
owing to H2S production, Shigella species show same type of colonies but
without any blackening.
SMAC agar: E. coli O157:H7 colonies appear pale yelow due to their inability to
ferment sorbitol.
A B C Figure 3.2. Colony morphology of selected bacteria. A: Salmonella on XLD, B: E coli O157:H7 on SMAC, and C: Shigella on SS agar. 3.6.2. Gram stain
Upon Gram staining, E.coli, Salmonella, and Shigella spp appear as Gram
negative bacilli (short rods)
3.6.3. Biochemical tests
These tests serve to determine aspects of bacterial metabolism; nutritional and
survival strategies of bacteria.
3.6.3.1. Oxidase test
All suspected bacteria are oxidase negative.
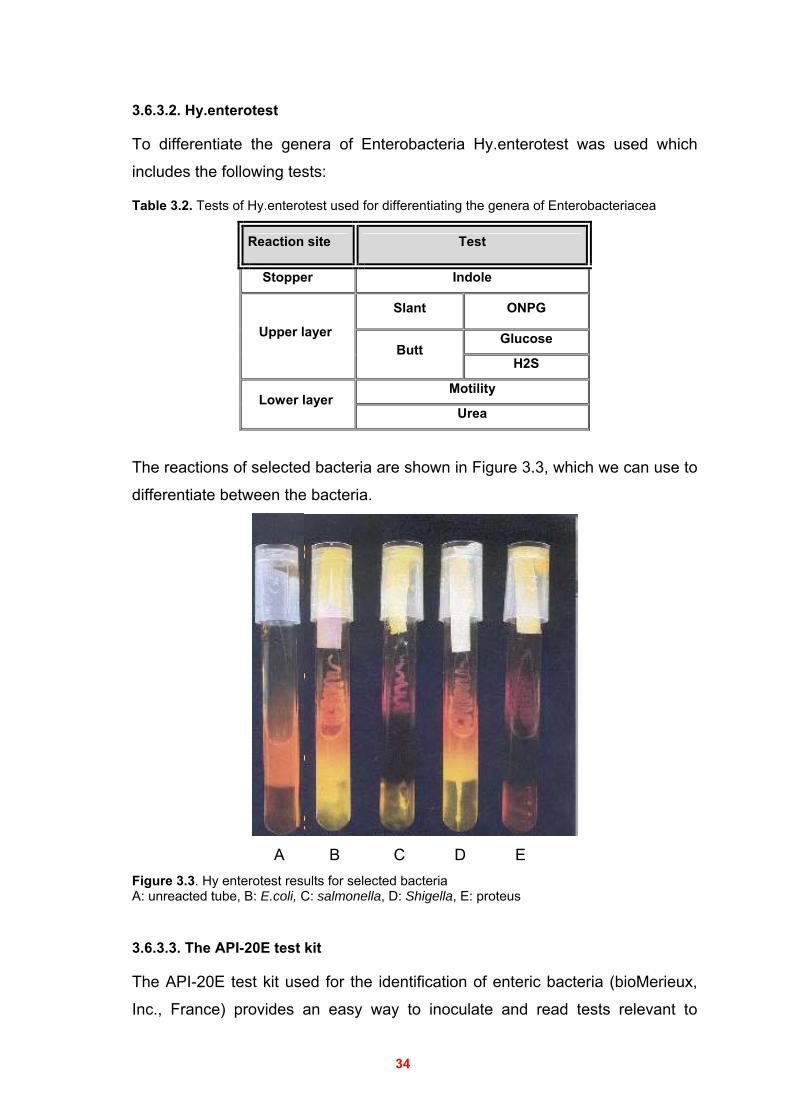
34
3.6.3.2. Hy.enterotest
To differentiate the genera of Enterobacteria Hy.enterotest was used which
includes the following tests:
Table 3.2. Tests of Hy.enterotest used for differentiating the genera of Enterobacteriacea
Reaction site Test
Stopper Indole
Slant ONPG
Glucose Upper layer Butt
H2S
Motility Lower layer
Urea
The reactions of selected bacteria are shown in Figure 3.3, which we can use to
differentiate between the bacteria.
A B C D E
Figure 3.3. Hy enterotest results for selected bacteria A: unreacted tube, B: E.coli, C: salmonella, D: Shigella, E: proteus
3.6.3.3. The API-20E test kit
The API-20E test kit used for the identification of enteric bacteria (bioMerieux,
Inc., France) provides an easy way to inoculate and read tests relevant to
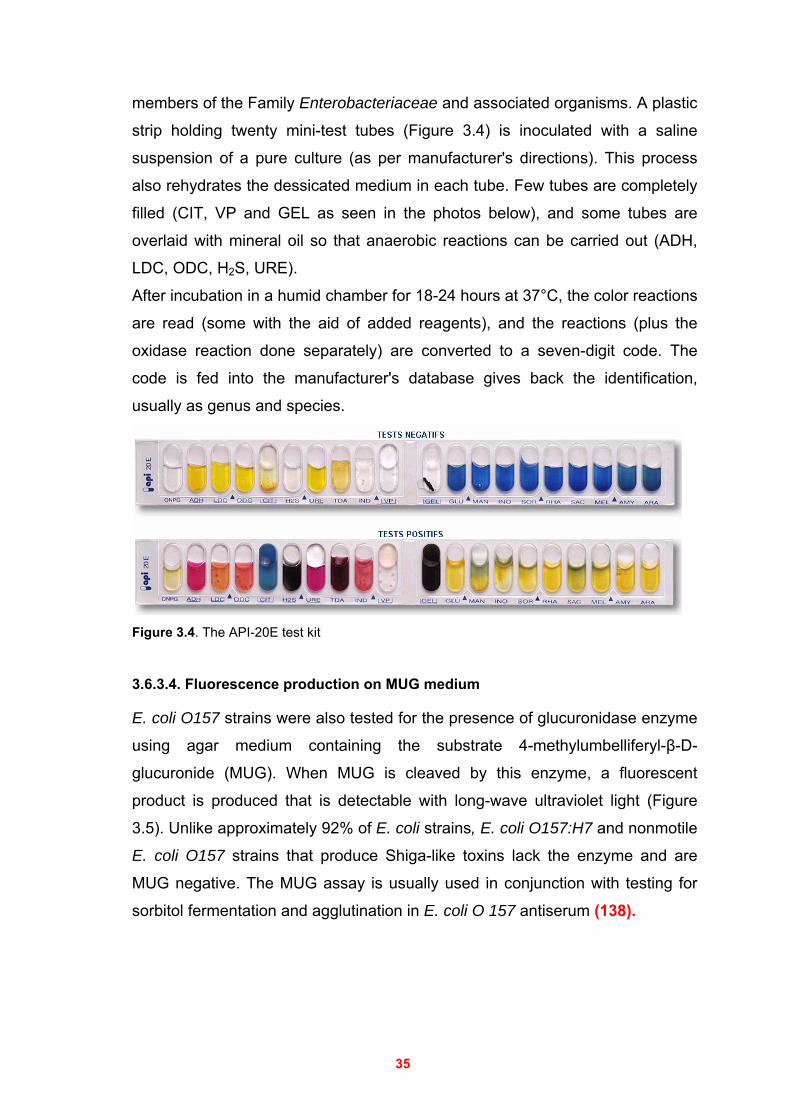
35
members of the Family Enterobacteriaceae and associated organisms. A plastic
strip holding twenty mini-test tubes (Figure 3.4) is inoculated with a saline
suspension of a pure culture (as per manufacturer's directions). This process
also rehydrates the dessicated medium in each tube. Few tubes are completely
filled (CIT, VP and GEL as seen in the photos below), and some tubes are
overlaid with mineral oil so that anaerobic reactions can be carried out (ADH,
LDC, ODC, H2S, URE).
After incubation in a humid chamber for 18-24 hours at 37°C, the color reactions
are read (some with the aid of added reagents), and the reactions (plus the
oxidase reaction done separately) are converted to a seven-digit code. The
code is fed into the manufacturer's database gives back the identification,
usually as genus and species.
Figure 3.4. The API-20E test kit
3.6.3.4. Fluorescence production on MUG medium
E. coli O157 strains were also tested for the presence of glucuronidase enzyme
using agar medium containing the substrate 4-methylumbelliferyl-β-D-
glucuronide (MUG). When MUG is cleaved by this enzyme, a fluorescent
product is produced that is detectable with long-wave ultraviolet light (Figure
3.5). Unlike approximately 92% of E. coli strains, E. coli O157:H7 and nonmotile
E. coli O157 strains that produce Shiga-like toxins lack the enzyme and are
MUG negative. The MUG assay is usually used in conjunction with testing for
sorbitol fermentation and agglutination in E. coli O 157 antiserum (138).
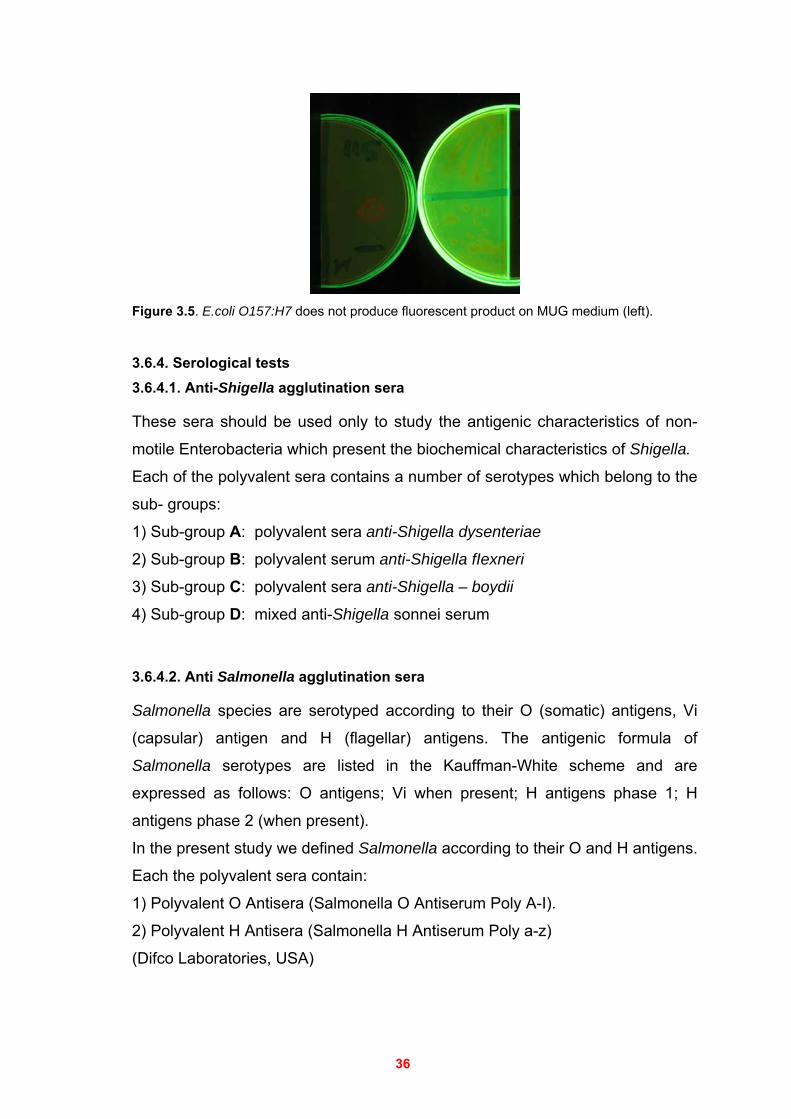
36
Figure 3.5. E.coli O157:H7 does not produce fluorescent product on MUG medium (left).
3.6.4. Serological tests 3.6.4.1. Anti-Shigella agglutination sera
These sera should be used only to study the antigenic characteristics of non-
motile Enterobacteria which present the biochemical characteristics of Shigella.
Each of the polyvalent sera contains a number of serotypes which belong to the
sub- groups:
1) Sub-group A: polyvalent sera anti-Shigella dysenteriae
2) Sub-group B: polyvalent serum anti-Shigella fIexneri
3) Sub-group C: polyvalent sera anti-Shigella – boydii
4) Sub-group D: mixed anti-Shigella sonnei serum
3.6.4.2. Anti Salmonella agglutination sera
Salmonella species are serotyped according to their O (somatic) antigens, Vi
(capsular) antigen and H (flagellar) antigens. The antigenic formula of
Salmonella serotypes are listed in the Kauffman-White scheme and are
expressed as follows: O antigens; Vi when present; H antigens phase 1; H
antigens phase 2 (when present).
In the present study we defined Salmonella according to their O and H antigens.
Each the polyvalent sera contain:
1) Polyvalent O Antisera (Salmonella O Antiserum Poly A-I).
2) Polyvalent H Antisera (Salmonella H Antiserum Poly a-z)
(Difco Laboratories, USA)
37
The technique used for both Salmonella and Shigella.
On a clean glass slide a drop of serum was deposited. Using a platinum loop a
small amount of bacteria, from an 18 hours old culture on nutrient agar, was
gradually mixed with the serum to form a light uniform suspension.
Agglutination is observed in the corresponding serum after a maximum of one
minute.
3.6.4.3. Anti E. coli O157:H7 latex test kit
The Plasmatic E.coli test kit is a latex agglutination test for the rapid
identification of E.coli sero-group O157. The test is best used in conjunction
with Sorbitol MacConkey Agar. E.coli O157 strains cannot ferment sorbitol and
will therefore give colourless colonies. The majority of other E.coli strains is
capable of fermenting sorbitol and therefore, gives characteristic pink colonies.
The non-sorbitol fermenting (NSF) colonies were further tested by the latex
agglutination method. Principle of the method
This method depends on latex particles coated with an antiserum against E.coli
O157 antigen. When the latex particles are mixed with fresh colonies of E.coli
O157 the bacteria will bind the antiserum, causing the latex particles to visibly
agglutinate (Positive). Bacteria which are not O157 serotype will not bind to the
antiserum and will not result in agglutination (Negative) Sample preparation
Non-sorbitol fermenting (NSF) colonies may be taken directly from the Sorbitol
MacConkey plate or NSF isolates may be subcultured onto non-selective media
for testing. At least 10 different NSF colonies should be tested, to ensure that
any mixed strains or contaminants are not detected. Use of control latex will
ensure that the tested colonies do not autoagglutinate. The method
Using the provided pipette, one drop of saline was placed onto two separate
circles of a reaction slide, using a sterile loop, colonies of the organism to be
investigated were picked and emulsified in the drop of saline in one of the
circles on the slide. The same is repeated with the second drop.
One drop of test latex reagent was then added to one of the drops of saline and
one drop of control latex reagent to the other, using the loop, the test reagent
38
and control reagent were thoroughly mixed. The slide was rotated for two
minutes while observing for agglutination. Interpretation of results
A positive result is indicated by agglutination with the test reagent, whilst the
control reagent should appear milky and smooth.
3.7. Antimicrobial susceptibility testing by disk diffusion
Antibiotic susceptibility of bacteria was determined using the disk diffusion
method as described by the National Committee for Clinical Laboratory
Standards (NCCLS). Approximately 4 mm thick Mueller-Hinton agar was prepared from a dehydrated
base according to the manufacturer’s recommendations.
The inoculums for antimicrobial susceptibility testing of bacterial isolates were
prepared from fresh pure cultures. The cell suspensions of the bacterial isolates
were prepared in sterile Mueller-Hinton broth. A cell suspension equal to a
density of a 0.5 McFarland turbidity standard was used for inoculation.
When the proper density is achieved, a cotton swab was dipped into the
bacterial suspension excess fluid was removed by pressing and rotating the
swab against the wall of the tube.
The swab was used to inoculate the entire surface of the Mueller-Hinton agar
plate three times, rotating the plate 60 degrees between each inoculation.
The inoculum was allowed to dry before placing the disks on the plates. Drying
usually takes only a few minutes, and should take no longer than 15 minutes.
After the plate was dry, the antimicrobial disks were placed on the plates.
Sterile forcep was used to place the disks on the Mueller Hinton agar and taped
them gently to ensure that they adhere to the agar. Diffusion of the drug in the
disk begins immediately; therefore, once a disk contacts the agar surface, the
disk should not be moved.
The plates were incubated in an inverted position for 18–24 hours at 37°C. After
overnight incubation, the diameter was measured of each zone of inhibition with
a ruler or a caliper. In all measurements, the zones of inhibition were measured
as the diameters from the edges of the last visible colony, and the results were
recorded in millimeters (mm). Inhibition zone diameters were compared to the
reference list of the manufactures.
39
Salmonella, and Shigella species were tested against the following antibiotics:
Ampicillin, Piperacillin, Cephalexin, Cefuroxime Ceftazidim, Ceftriaxone,
Amikacin, Gentamicin, Doxycycline, Sulfamethoxazol/Trimethoprim,
Ciprofloxacin, Nalidixic acid, Chloramphenicol, Cefaclor and Meropenem.
(72,175,187).
3.8. Polymerase Chain Reaction (PCR)
3.8.1. Preparation of Fecal Specimens for PCR Assays
Processing of specimens is the most critical step in PCR assays. Although it is
not essential to isolate DNA in great purity, it is necessary to remove or
inactivate substances that may inhibit PCR assays. Stool specimens are known
to contain potent PCR inhibitors, most of which have not been identified.
A washing step was used in order to decrease the concentration of PCR
inhibitors. The fecal debris, which is inhibitory to PCR, was then removed by
low-speed centrifugation. The kit extraction eliminates other contaminants
(biological, proteins polysaccharide, and bile acids) in stool suspensions that
may inhibit PCR (111,144,181). The stored (–70 °C) fecal samples were thawed before processing. To
maximize the bacterial populations present in the fecal specimen, approximately
one gram feces specimen was added to 5 ml of sterile 0.85% NaCl and mixed
by inverting and vortexing the tubes. The samples were then centrifuged at low
speed (2000) rpm for 2 min to pellet larger fecal debris. The supernatant was
transferred to a new tube and then centrifuged at 12000 rpm for 5 min to pellet
the bacterial cells. The cells in the pellets were washed three times with normal
saline and once with water, resuspended in 0.1 ml of distilled water, and their
DNA was extracted using AccuPrep Stool DNA Extraction Kit (Bioneer, Korea)
according to the manufacturer’s protocol except that in the final step only 100 µl
(instead of 200 µl) of heated elution buffer (70 0C) was used.
3.8.2. DNA Extraction from stool
The AccuPrep Stool DNA Extraction Kit can quickly and conveniently extract up
to 5µg of DNA from about 100 to 200 mg of stool. In the presence of chaotropic
salt, DNA is bound to glass fibers fixed in a column. Proteins and other
contaminants are removed through washing steps, and the DNA isolated and
eluted in the final elution step. The process does not require the use of
40
dangerous organic solvents or ethanol precipitation steps. Also, DNA is
efficiently extracted regardless of the condition of the stool. The kit contains the following Reagents:
Proteinase K, lyophilized
Stool Lysis buffer (SL)
Binding buffer (ST)
Washing buffer 1 (W1)
Washing buffer 2 (W2)
Elution buffer (E) Procedure of Extracting DNA from Stool 20 ul proteinase k (25 mg/ml) was added to 1.5 mL microcentrifuge tube,
washed stool sample pellets were then added, followed by 400 ul Stool Lysis
buffer (SL) and the mixture was mixed by light vortexing for about 30 seconds,
complete mixing is essential for maximum lysis. The tubes were then incubated
at 60 °C for 10 min.
After 10 mins incubation, the tubes were centrifuged 12,000rpm for 5 mins,
then the supernatant was transferred to a new tube, 400 ul Binding buffer (ST)
was added, and the tubes were incubated again at 60 °C for 10 min.
After 10 mins incubation 100µl absolute isopropanol was added, mixed by
lightly vortexing for about 5 seconds, and the mixture was transferred into the
binding column. The lid was closed and the column was centrifuged for 1 min at
8,000 rpm, or until the liquid has completely passed.
The binding column was transferred to a new 2 ml collection tube, after
centrifugation, 500µl Washing buffer 1 (W1) was added to the column, and the
column was centrifuged again for 1min at 8,000 rpm.
After centrifugation, the binding column was transferred to a new 2 ml collection
tube, 500µl Washing buffer 2 (W2) was added, and centrifuged for 1min at
8,000 rpm.
The column was further centrifuged at 13,000 rpm for 1 min to completely
remove alcohol. The binding column was transferred to a 1.5 ml collection tube,
100µl of heated (700C) elution buffer was added, and the column was let to
stand for 5 min to allow the buffer to permeate the column. The DNA was then
eluted by spinning down at 8,000 rpm for 1 min.
41
The eluted DNA solution can directly be used, or stored at 4°C or –20°C for
longer storage periods.
3.8.3. Detection and measurement of extracted DNA 3.8.3.1. Agarose gel electrophoresis
The quality of the isolated DNA was determined by running 5 ul of each sample
on 1.0% ethidium bromide stained agarose gels and the DNA was visualized on
a short wave U.V. transilluminator, the results were documented by
photography.
3.8.3.2. Spectrophotometery
The optical density (O.D.) at 260 nm of diluted fractions of the isolated DNA
samples was measured by a spectrophotometer and the DNA concentration
was calculated by considering 1 O.D.(260 nm) = 50 ug/ml DNA and taking into
account the dilution factor.
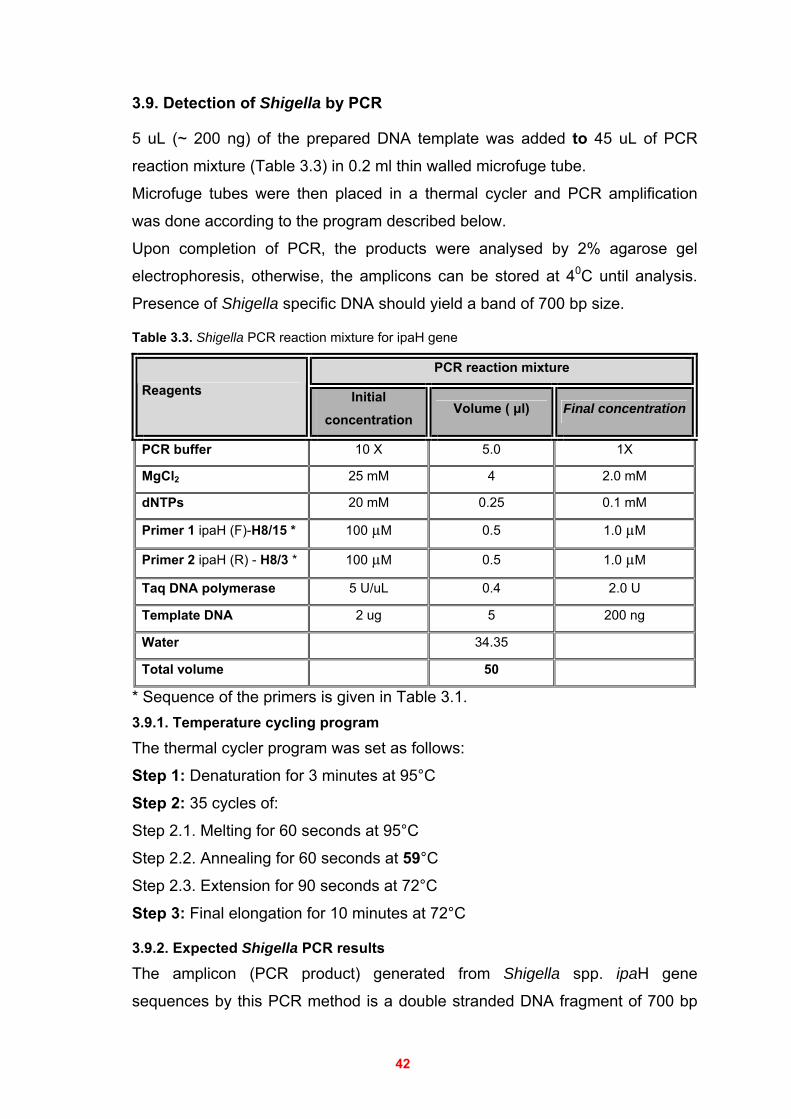
42
3.9. Detection of Shigella by PCR
5 uL (~ 200 ng) of the prepared DNA template was added to 45 uL of PCR
reaction mixture (Table 3.3) in 0.2 ml thin walled microfuge tube. Microfuge tubes were then placed in a thermal cycler and PCR amplification
was done according to the program described below.
Upon completion of PCR, the products were analysed by 2% agarose gel
electrophoresis, otherwise, the amplicons can be stored at 40C until analysis.
Presence of Shigella specific DNA should yield a band of 700 bp size.
Table 3.3. Shigella PCR reaction mixture for ipaH gene
PCR reaction mixture Reagents Initial
concentration Volume ( μl) Final concentration
PCR buffer 10 X 5.0 1X
MgCl2 25 mM 4 2.0 mM
dNTPs 20 mM 0.25 0.1 mM
Primer 1 ipaH (F)-H8/15 * 100 µM 0.5 1.0 µM
Primer 2 ipaH (R) - H8/3 * 100 µM 0.5 1.0 µM
Taq DNA polymerase 5 U/uL 0.4 2.0 U
Template DNA 2 ug 5 200 ng
Water 34.35
Total volume 50
* Sequence of the primers is given in Table 3.1. 3.9.1. Temperature cycling program
The thermal cycler program was set as follows:
Step 1: Denaturation for 3 minutes at 95°C
Step 2: 35 cycles of:
Step 2.1. Melting for 60 seconds at 95°C
Step 2.2. Annealing for 60 seconds at 59°C
Step 2.3. Extension for 90 seconds at 72°C
Step 3: Final elongation for 10 minutes at 72°C
3.9.2. Expected Shigella PCR results
The amplicon (PCR product) generated from Shigella spp. ipaH gene
sequences by this PCR method is a double stranded DNA fragment of 700 bp
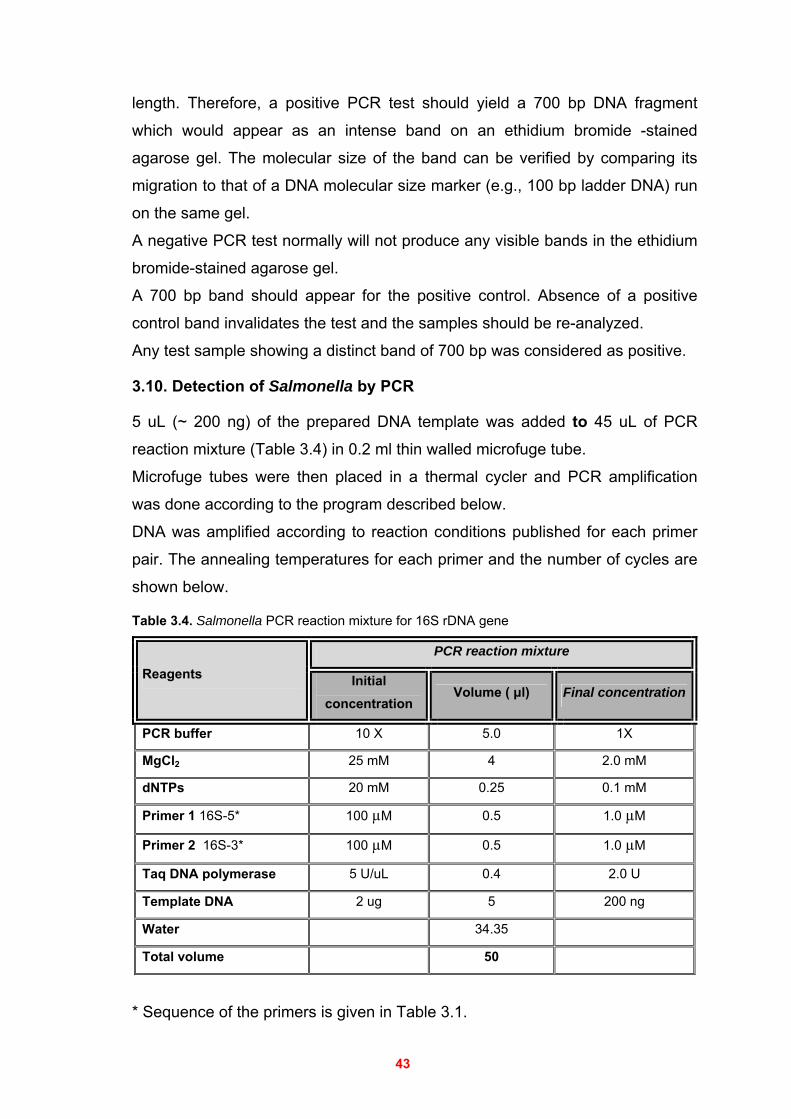
43
length. Therefore, a positive PCR test should yield a 700 bp DNA fragment
which would appear as an intense band on an ethidium bromide -stained
agarose gel. The molecular size of the band can be verified by comparing its
migration to that of a DNA molecular size marker (e.g., 100 bp ladder DNA) run
on the same gel.
A negative PCR test normally will not produce any visible bands in the ethidium
bromide-stained agarose gel.
A 700 bp band should appear for the positive control. Absence of a positive
control band invalidates the test and the samples should be re-analyzed.
Any test sample showing a distinct band of 700 bp was considered as positive.
3.10. Detection of Salmonella by PCR
5 uL (~ 200 ng) of the prepared DNA template was added to 45 uL of PCR
reaction mixture (Table 3.4) in 0.2 ml thin walled microfuge tube. Microfuge tubes were then placed in a thermal cycler and PCR amplification
was done according to the program described below.
DNA was amplified according to reaction conditions published for each primer
pair. The annealing temperatures for each primer and the number of cycles are
shown below.
Table 3.4. Salmonella PCR reaction mixture for 16S rDNA gene
PCR reaction mixture Reagents Initial
concentration Volume ( μl) Final concentration
PCR buffer 10 X 5.0 1X
MgCl2 25 mM 4 2.0 mM
dNTPs 20 mM 0.25 0.1 mM
Primer 1 16S-5* 100 µM 0.5 1.0 µM
Primer 2 16S-3* 100 µM 0.5 1.0 µM
Taq DNA polymerase 5 U/uL 0.4 2.0 U
Template DNA 2 ug 5 200 ng
Water 34.35
Total volume 50
* Sequence of the primers is given in Table 3.1.
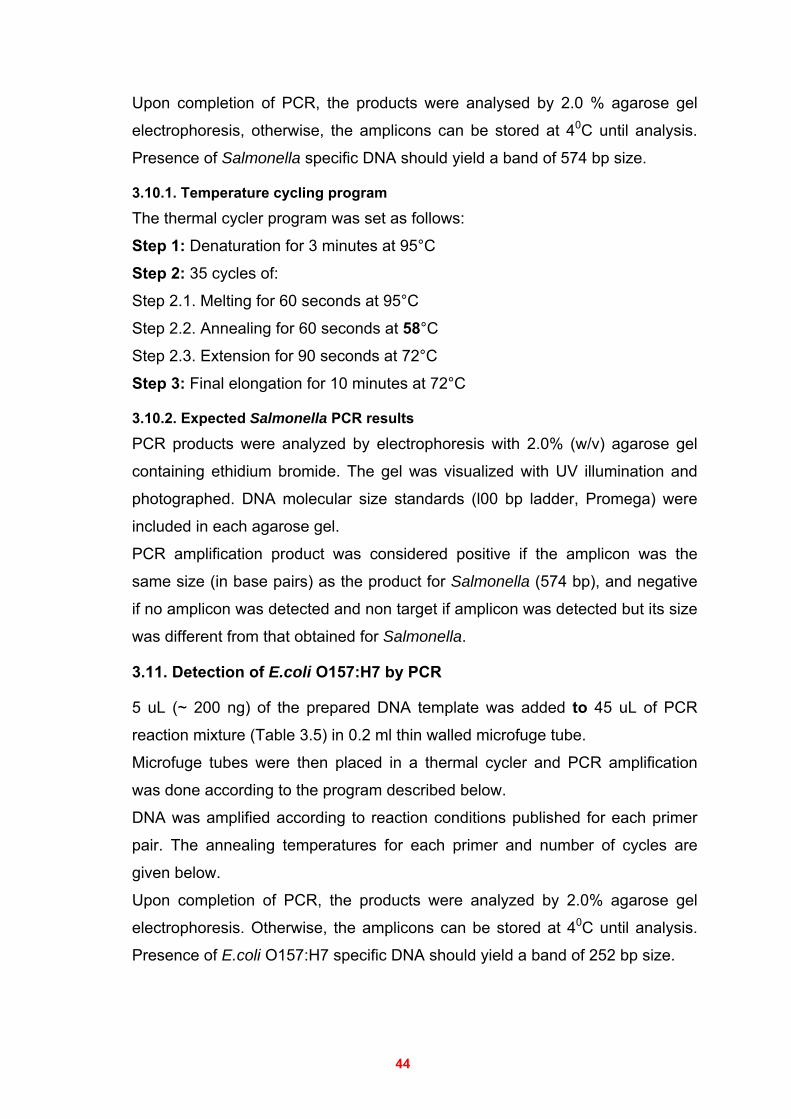
44
Upon completion of PCR, the products were analysed by 2.0 % agarose gel
electrophoresis, otherwise, the amplicons can be stored at 40C until analysis.
Presence of Salmonella specific DNA should yield a band of 574 bp size.
3.10.1. Temperature cycling program
The thermal cycler program was set as follows:
Step 1: Denaturation for 3 minutes at 95°C
Step 2: 35 cycles of:
Step 2.1. Melting for 60 seconds at 95°C
Step 2.2. Annealing for 60 seconds at 58°C
Step 2.3. Extension for 90 seconds at 72°C
Step 3: Final elongation for 10 minutes at 72°C
3.10.2. Expected Salmonella PCR results
PCR products were analyzed by electrophoresis with 2.0% (w/v) agarose gel
containing ethidium bromide. The gel was visualized with UV illumination and
photographed. DNA molecular size standards (l00 bp ladder, Promega) were
included in each agarose gel.
PCR amplification product was considered positive if the amplicon was the
same size (in base pairs) as the product for Salmonella (574 bp), and negative
if no amplicon was detected and non target if amplicon was detected but its size
was different from that obtained for Salmonella.
3.11. Detection of E.coli O157:H7 by PCR
5 uL (~ 200 ng) of the prepared DNA template was added to 45 uL of PCR
reaction mixture (Table 3.5) in 0.2 ml thin walled microfuge tube. Microfuge tubes were then placed in a thermal cycler and PCR amplification
was done according to the program described below.
DNA was amplified according to reaction conditions published for each primer
pair. The annealing temperatures for each primer and number of cycles are
given below.
Upon completion of PCR, the products were analyzed by 2.0% agarose gel
electrophoresis. Otherwise, the amplicons can be stored at 40C until analysis.
Presence of E.coli O157:H7 specific DNA should yield a band of 252 bp size.
45
Table 3.5. E.coli O157:H7 PCR reaction mixture using uidA gene
PCR reaction mixture Reagents Initial
concentration Volume ( μl) Final concentration
PCR buffer 10 X 5.0 1X
MgCl2 25 mM 4 2.0 mM
dNTPs 20 mM 0.25 0.1 mM
Primer 1 PT2* 100 µM 0.5 1.0 µM
Primer 2 PT3* 100 µM 0.5 1.0 µM
Taq DNA polymerase 5 U/uL 0.4 2.0 U
Template DNA 2 ug 5 200 ng
Water 34.35
Total volume 50
* Sequence of the primers is given in Table 3.1.
3.11.1. Temperature cycling program
The thermal cycler program was set as follows:
Step 1: Denaturation for 3 minutes at 95°C
Step 2: 35 cycles of:
Step 2.1. Melting for 60 seconds at 95°C
Step 2.2. Annealing for 60 seconds at 55°C
Step 2.3. Extension for 90 seconds at 72°C
Step 3: Final elongation for 10 minutes at 72°C
3.11.2. Expected E.coli O157:H7 PCR results
A positive PCR test should yield a 252 bp DNA fragment which would appear as
an intense band on an ethidium bromide-stained 2.0% agarose gel. The
molecular size of the band can be verified by comparing its migration to that of a
DNA molecular size marker (100 bp ladder DNA) run on the same gel.
A negative PCR test normally will not produce any visible bands in the ethidium
bromide-stained agarose gel.
The PCR products were visualized with UV illumination and the results were
documented by photography.
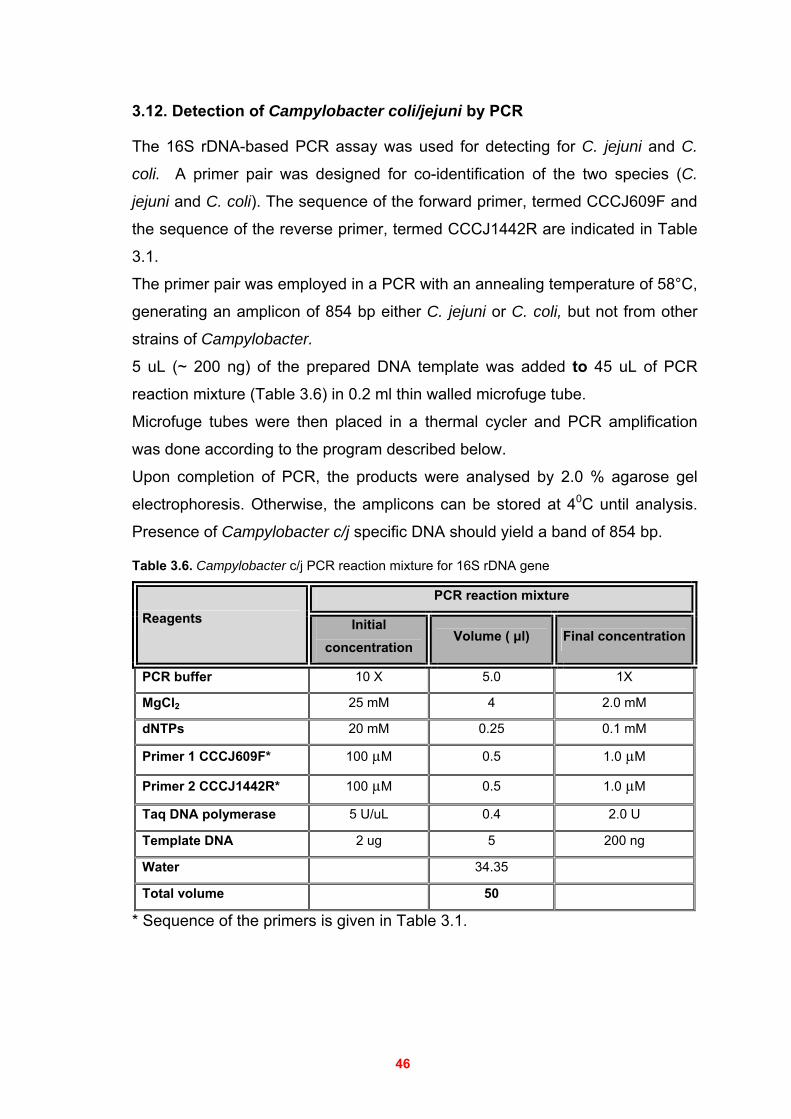
46
3.12. Detection of Campylobacter coli/jejuni by PCR
The 16S rDNA-based PCR assay was used for detecting for C. jejuni and C.
coli. A primer pair was designed for co-identification of the two species (C.
jejuni and C. coli). The sequence of the forward primer, termed CCCJ609F and
the sequence of the reverse primer, termed CCCJ1442R are indicated in Table
3.1.
The primer pair was employed in a PCR with an annealing temperature of 58°C,
generating an amplicon of 854 bp either C. jejuni or C. coli, but not from other
strains of Campylobacter.
5 uL (~ 200 ng) of the prepared DNA template was added to 45 uL of PCR
reaction mixture (Table 3.6) in 0.2 ml thin walled microfuge tube. Microfuge tubes were then placed in a thermal cycler and PCR amplification
was done according to the program described below.
Upon completion of PCR, the products were analysed by 2.0 % agarose gel
electrophoresis. Otherwise, the amplicons can be stored at 40C until analysis.
Presence of Campylobacter c/j specific DNA should yield a band of 854 bp.
Table 3.6. Campylobacter c/j PCR reaction mixture for 16S rDNA gene
PCR reaction mixture Reagents Initial
concentration Volume ( μl) Final concentration
PCR buffer 10 X 5.0 1X
MgCl2 25 mM 4 2.0 mM
dNTPs 20 mM 0.25 0.1 mM
Primer 1 CCCJ609F* 100 µM 0.5 1.0 µM
Primer 2 CCCJ1442R* 100 µM 0.5 1.0 µM
Taq DNA polymerase 5 U/uL 0.4 2.0 U
Template DNA 2 ug 5 200 ng
Water 34.35
Total volume 50
* Sequence of the primers is given in Table 3.1.
47
3.12.1. Temperature cycling program
The thermal cycler program was set as follows:
Step 1: Denaturation for 3 minutes at 95°C
Step 2: 35 cycles of:
Step 2.1. Melting for 60 seconds at 95°C
Step 2.2. Annealing for 60 seconds at 59°C
Step 2.3. Extension for 90 seconds at 72°C
Step 3: Final elongation for 10 minutes at 72°C
3.12.2. Expected Campylocacter PCR results
The amplicon (PCR product) generated from Campylobacter c/j spp. 16S rDNA
gene should yield a fragment of 854 bp length. Therefore, a positive PCR test
should yields a 854 bp DNA fragment which would appear as an intense band
on an agarose gel. The molecular size of the band can be verified by comparing
its migration to that of a DNA molecular size marker (e.g., 100 bp ladder DNA)
run on the same gel.
A negative PCR test does not normally produce any visible bands in the
agarose gel.
A 854 bp band should appear for the positive control. Absence of a positive
control band invalidates the test and the samples should be re-analyzed.
Any test sample showing a distinct band at 854 bp was considered as positive.
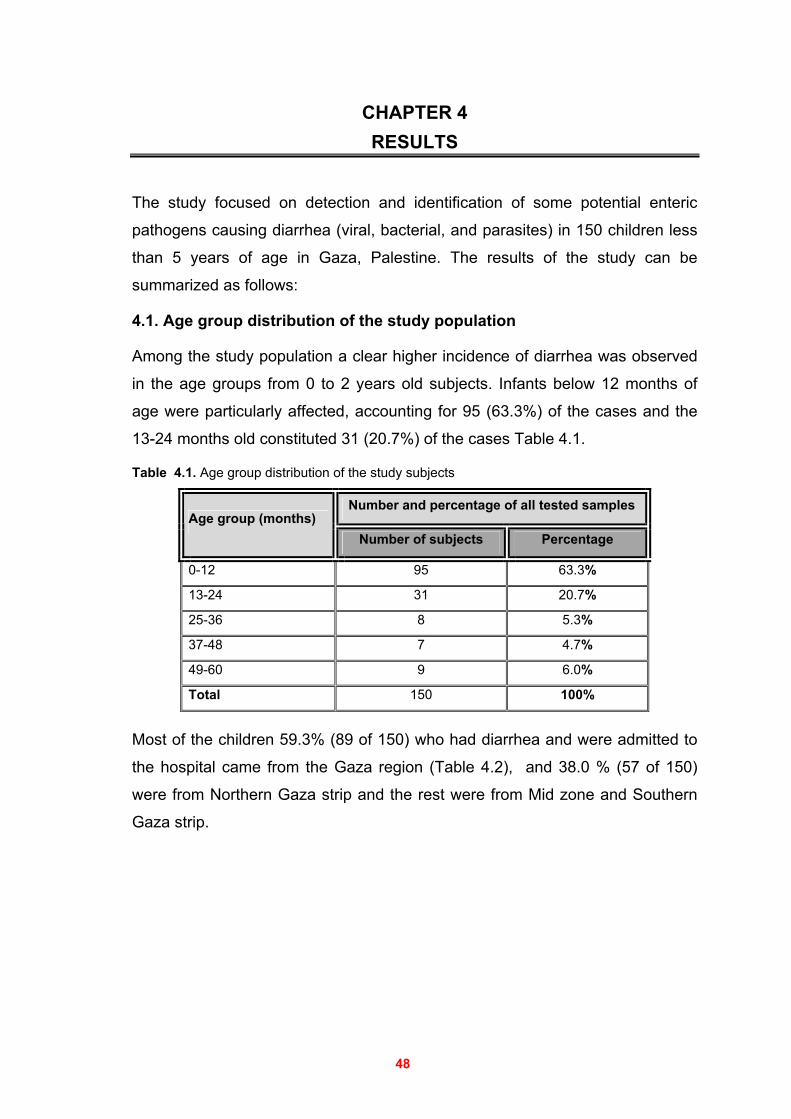
48
CHAPTER 4 RESULTS
The study focused on detection and identification of some potential enteric
pathogens causing diarrhea (viral, bacterial, and parasites) in 150 children less
than 5 years of age in Gaza, Palestine. The results of the study can be
summarized as follows:
4.1. Age group distribution of the study population
Among the study population a clear higher incidence of diarrhea was observed
in the age groups from 0 to 2 years old subjects. Infants below 12 months of
age were particularly affected, accounting for 95 (63.3%) of the cases and the
13-24 months old constituted 31 (20.7%) of the cases Table 4.1.
Table 4.1. Age group distribution of the study subjects
Number and percentage of all tested samples Age group (months)
Number of subjects Percentage
0-12 95 63.3%
13-24 31 20.7%
25-36 8 5.3%
37-48 7 4.7%
49-60 9 6.0%
Total 150 100%
Most of the children 59.3% (89 of 150) who had diarrhea and were admitted to
the hospital came from the Gaza region (Table 4.2), and 38.0 % (57 of 150)
were from Northern Gaza strip and the rest were from Mid zone and Southern
Gaza strip.
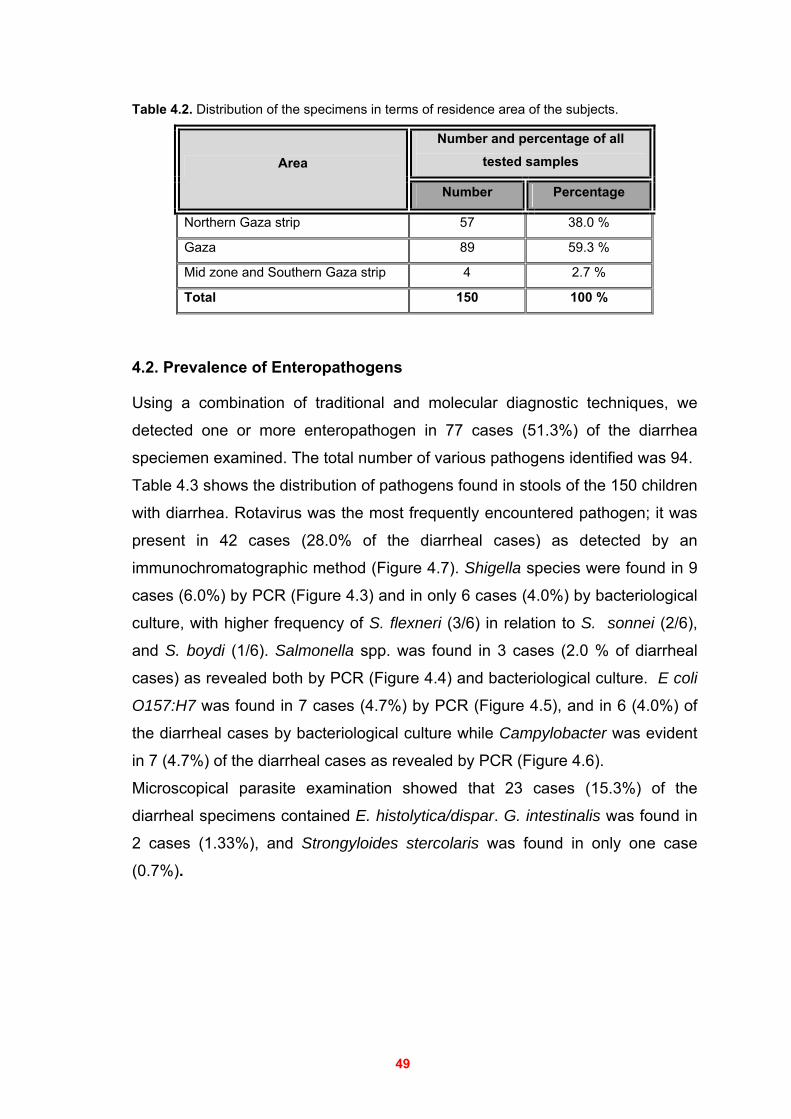
49
Table 4.2. Distribution of the specimens in terms of residence area of the subjects.
Number and percentage of all tested samples Area
Number Percentage
Northern Gaza strip 57 38.0 %
Gaza 89 59.3 %
Mid zone and Southern Gaza strip 4 2.7 %
Total 150 100 %
4.2. Prevalence of Enteropathogens
Using a combination of traditional and molecular diagnostic techniques, we
detected one or more enteropathogen in 77 cases (51.3%) of the diarrhea
speciemen examined. The total number of various pathogens identified was 94.
Table 4.3 shows the distribution of pathogens found in stools of the 150 children
with diarrhea. Rotavirus was the most frequently encountered pathogen; it was
present in 42 cases (28.0% of the diarrheal cases) as detected by an
immunochromatographic method (Figure 4.7). Shigella species were found in 9
cases (6.0%) by PCR (Figure 4.3) and in only 6 cases (4.0%) by bacteriological
culture, with higher frequency of S. flexneri (3/6) in relation to S. sonnei (2/6),
and S. boydi (1/6). Salmonella spp. was found in 3 cases (2.0 % of diarrheal
cases) as revealed both by PCR (Figure 4.4) and bacteriological culture. E coli
O157:H7 was found in 7 cases (4.7%) by PCR (Figure 4.5), and in 6 (4.0%) of
the diarrheal cases by bacteriological culture while Campylobacter was evident
in 7 (4.7%) of the diarrheal cases as revealed by PCR (Figure 4.6).
Microscopical parasite examination showed that 23 cases (15.3%) of the
diarrheal specimens contained E. histolytica/dispar. G. intestinalis was found in
2 cases (1.33%), and Strongyloides stercolaris was found in only one case
(0.7%).
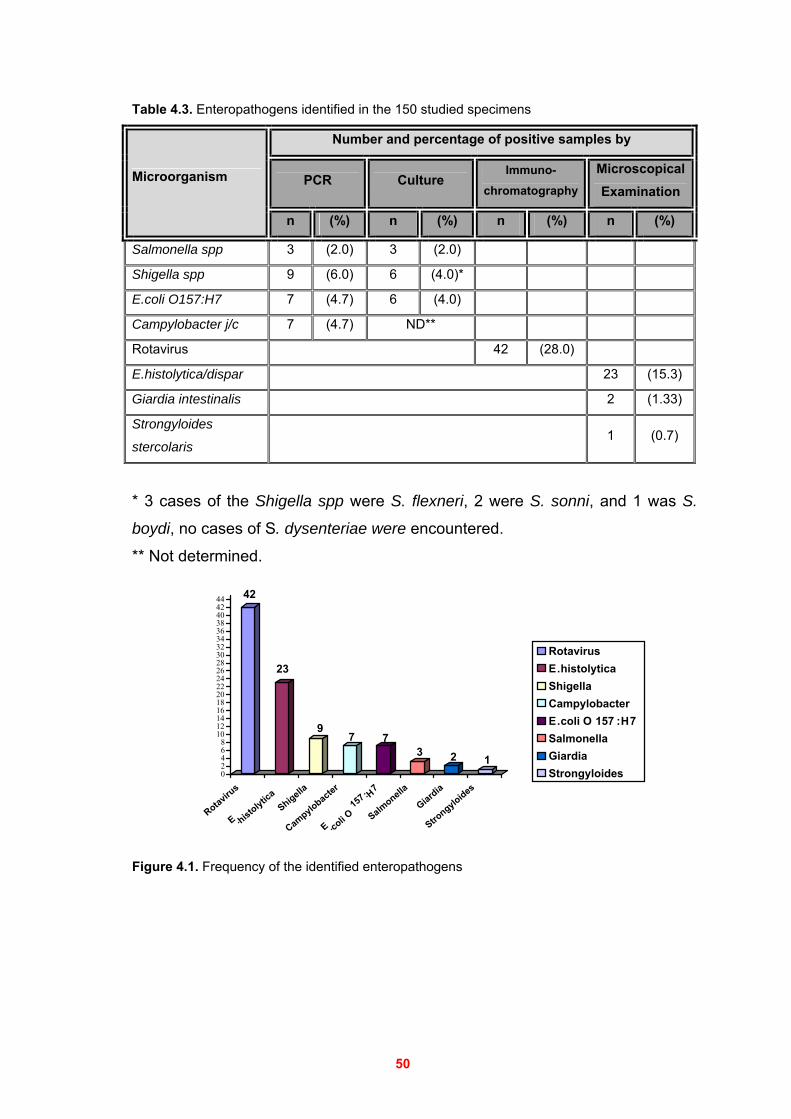
50
Table 4.3. Enteropathogens identified in the 150 studied specimens
Number and percentage of positive samples by
PCR Culture Immuno-
chromatography
Microscopical Examination
Microorganism
n (%) n (%) n (%) n (%)
Salmonella spp 3 (2.0) 3 (2.0)
Shigella spp 9 (6.0) 6 (4.0)*
E.coli O157:H7 7 (4.7) 6 (4.0)
Campylobacter j/c 7 (4.7) ND**
Rotavirus 42 (28.0)
E.histolytica/dispar 23 (15.3)
Giardia intestinalis 2 (1.33)
Strongyloides
stercolaris 1 (0.7)
* 3 cases of the Shigella spp were S. flexneri, 2 were S. sonni, and 1 was S.
boydi, no cases of S. dysenteriae were encountered.
** Not determined.
42
23
97 7
3 2 102468
101214161820222426283032343638404244
Rotavirus
E .histolytic
aShigella
Campylobacter
E .coli O
157 :H7
Salmonella
Giardia
Strongyloides
RotavirusE.histolyticaShigellaCampylobacterE.coli O 157 :H7SalmonellaGiardia Strongyloides
Figure 4.1. Frequency of the identified enteropathogens
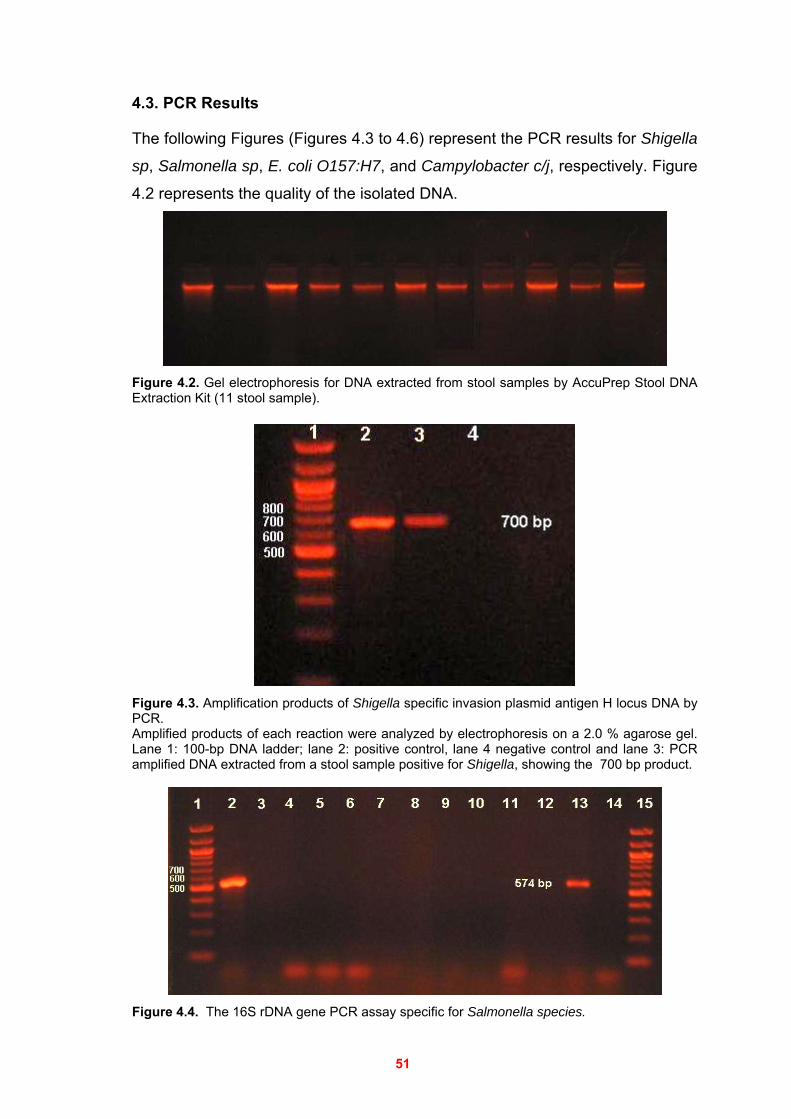
51
4.3. PCR Results
The following Figures (Figures 4.3 to 4.6) represent the PCR results for Shigella
sp, Salmonella sp, E. coli O157:H7, and Campylobacter c/j, respectively. Figure
4.2 represents the quality of the isolated DNA.
Figure 4.2. Gel electrophoresis for DNA extracted from stool samples by AccuPrep Stool DNA Extraction Kit (11 stool sample).
Figure 4.3. Amplification products of Shigella specific invasion plasmid antigen H locus DNA by PCR. Amplified products of each reaction were analyzed by electrophoresis on a 2.0 % agarose gel. Lane 1: 100-bp DNA ladder; lane 2: positive control, lane 4 negative control and lane 3: PCR amplified DNA extracted from a stool sample positive for Shigella, showing the 700 bp product.
Figure 4.4. The 16S rDNA gene PCR assay specific for Salmonella species.
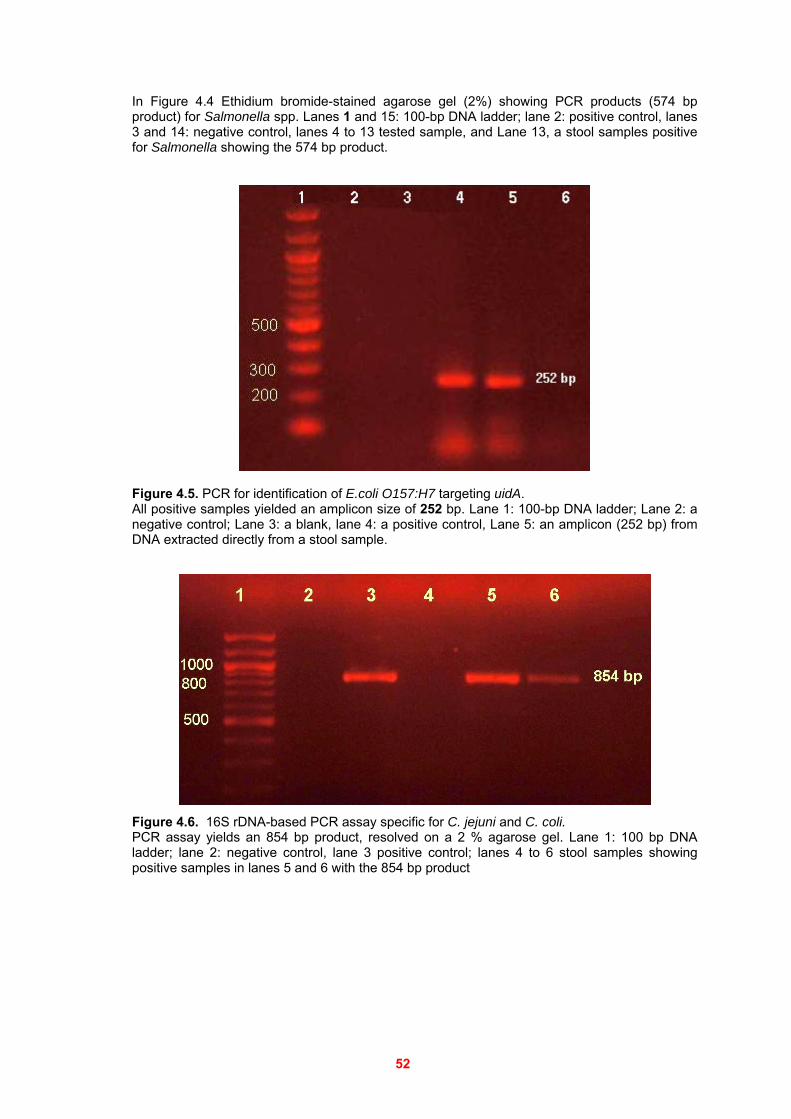
52
In Figure 4.4 Ethidium bromide-stained agarose gel (2%) showing PCR products (574 bp product) for Salmonella spp. Lanes 1 and 15: 100-bp DNA ladder; lane 2: positive control, lanes 3 and 14: negative control, lanes 4 to 13 tested sample, and Lane 13, a stool samples positive for Salmonella showing the 574 bp product.
Figure 4.5. PCR for identification of E.coli O157:H7 targeting uidA. All positive samples yielded an amplicon size of 252 bp. Lane 1: 100-bp DNA ladder; Lane 2: a negative control; Lane 3: a blank, lane 4: a positive control, Lane 5: an amplicon (252 bp) from DNA extracted directly from a stool sample.
Figure 4.6. 16S rDNA-based PCR assay specific for C. jejuni and C. coli. PCR assay yields an 854 bp product, resolved on a 2 % agarose gel. Lane 1: 100 bp DNA ladder; lane 2: negative control, lane 3 positive control; lanes 4 to 6 stool samples showing positive samples in lanes 5 and 6 with the 854 bp product
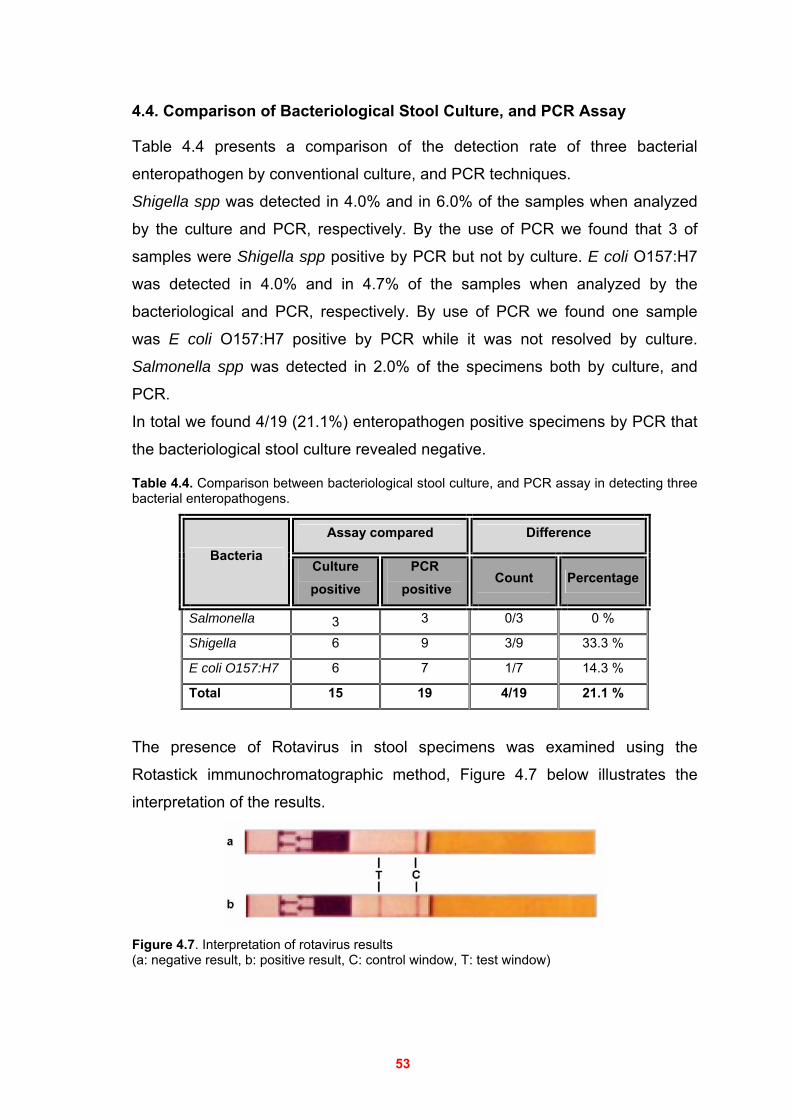
53
4.4. Comparison of Bacteriological Stool Culture, and PCR Assay
Table 4.4 presents a comparison of the detection rate of three bacterial
enteropathogen by conventional culture, and PCR techniques.
Shigella spp was detected in 4.0% and in 6.0% of the samples when analyzed
by the culture and PCR, respectively. By the use of PCR we found that 3 of
samples were Shigella spp positive by PCR but not by culture. E coli O157:H7
was detected in 4.0% and in 4.7% of the samples when analyzed by the
bacteriological and PCR, respectively. By use of PCR we found one sample
was E coli O157:H7 positive by PCR while it was not resolved by culture.
Salmonella spp was detected in 2.0% of the specimens both by culture, and
PCR.
In total we found 4/19 (21.1%) enteropathogen positive specimens by PCR that
the bacteriological stool culture revealed negative.
Table 4.4. Comparison between bacteriological stool culture, and PCR assay in detecting three bacterial enteropathogens.
Assay compared Difference Bacteria
Culture positive
PCR positive
Count Percentage
Salmonella 3 3 0/3 0 %
Shigella 6 9 3/9 33.3 %
E coli O157:H7 6 7 1/7 14.3 %
Total 15 19 4/19 21.1 %
The presence of Rotavirus in stool specimens was examined using the
Rotastick immunochromatographic method, Figure 4.7 below illustrates the
interpretation of the results.
Figure 4.7. Interpretation of rotavirus results (a: negative result, b: positive result, C: control window, T: test window)
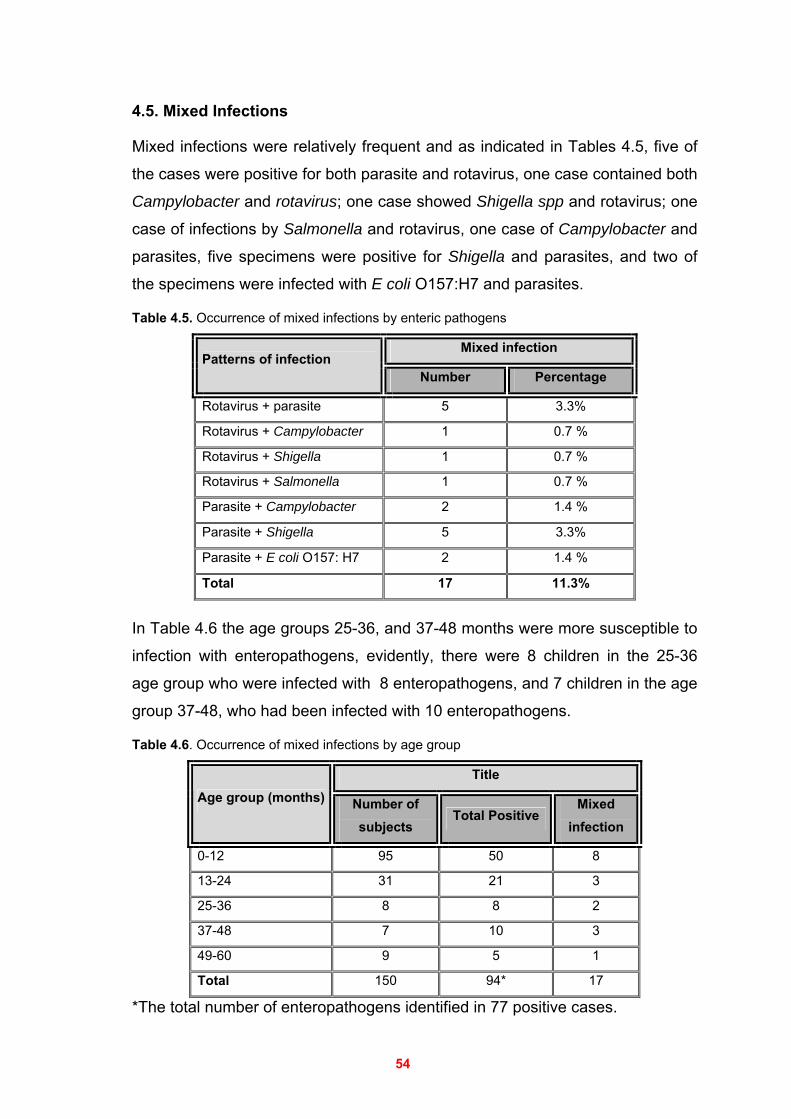
54
4.5. Mixed Infections
Mixed infections were relatively frequent and as indicated in Tables 4.5, five of
the cases were positive for both parasite and rotavirus, one case contained both
Campylobacter and rotavirus; one case showed Shigella spp and rotavirus; one
case of infections by Salmonella and rotavirus, one case of Campylobacter and
parasites, five specimens were positive for Shigella and parasites, and two of
the specimens were infected with E coli O157:H7 and parasites.
Table 4.5. Occurrence of mixed infections by enteric pathogens
Mixed infection Patterns of infection
Number Percentage
Rotavirus + parasite 5 3.3%
Rotavirus + Campylobacter 1 0.7 %
Rotavirus + Shigella 1 0.7 %
Rotavirus + Salmonella 1 0.7 %
Parasite + Campylobacter 2 1.4 %
Parasite + Shigella 5 3.3%
Parasite + E coli O157: H7 2 1.4 %
Total 17 11.3%
In Table 4.6 the age groups 25-36, and 37-48 months were more susceptible to
infection with enteropathogens, evidently, there were 8 children in the 25-36
age group who were infected with 8 enteropathogens, and 7 children in the age
group 37-48, who had been infected with 10 enteropathogens.
Table 4.6. Occurrence of mixed infections by age group
Title Age group (months) Number of
subjects Total Positive
Mixed infection
0-12 95 50 8
13-24 31 21 3
25-36 8 8 2
37-48 7 10 3
49-60 9 5 1
Total 150 94* 17
*The total number of enteropathogens identified in 77 positive cases.
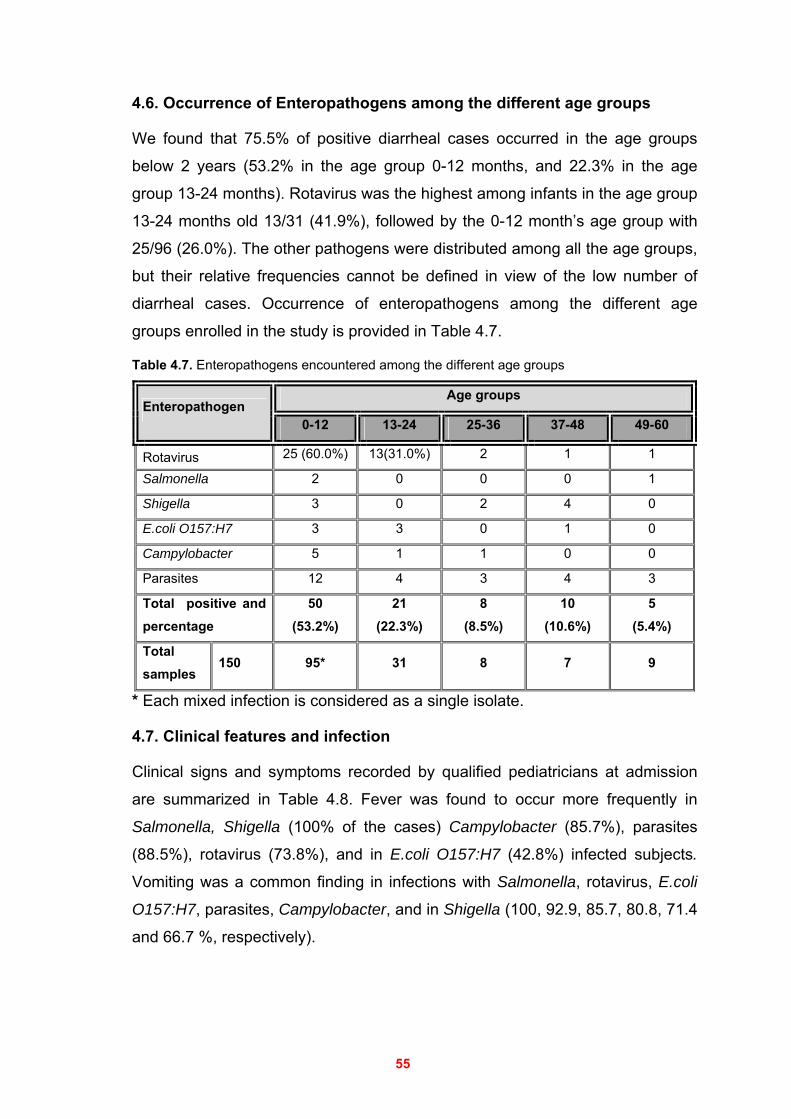
55
4.6. Occurrence of Enteropathogens among the different age groups
We found that 75.5% of positive diarrheal cases occurred in the age groups
below 2 years (53.2% in the age group 0-12 months, and 22.3% in the age
group 13-24 months). Rotavirus was the highest among infants in the age group
13-24 months old 13/31 (41.9%), followed by the 0-12 month’s age group with
25/96 (26.0%). The other pathogens were distributed among all the age groups,
but their relative frequencies cannot be defined in view of the low number of
diarrheal cases. Occurrence of enteropathogens among the different age
groups enrolled in the study is provided in Table 4.7.
Table 4.7. Enteropathogens encountered among the different age groups
Age groups Enteropathogen
0-12 13-24 25-36 37-48 49-60
Rotavirus 25 (60.0%) 13(31.0%) 2 1 1
Salmonella 2 0 0 0 1
Shigella 3 0 2 4 0
E.coli O157:H7 3 3 0 1 0
Campylobacter 5 1 1 0 0
Parasites 12 4 3 4 3
Total positive and percentage
50 (53.2%)
21 (22.3%)
8 (8.5%)
10 (10.6%)
5 (5.4%)
Total samples
150 95* 31 8 7 9
* Each mixed infection is considered as a single isolate.
4.7. Clinical features and infection
Clinical signs and symptoms recorded by qualified pediatricians at admission
are summarized in Table 4.8. Fever was found to occur more frequently in
Salmonella, Shigella (100% of the cases) Campylobacter (85.7%), parasites
(88.5%), rotavirus (73.8%), and in E.coli O157:H7 (42.8%) infected subjects.
Vomiting was a common finding in infections with Salmonella, rotavirus, E.coli
O157:H7, parasites, Campylobacter, and in Shigella (100, 92.9, 85.7, 80.8, 71.4
and 66.7 %, respectively).

56
The dehydration status of the diarrheal children was observed more common in
rotavirus infection, (14.3%), followed by Shigella (11.1%), and E.coli O157:H7
(11.1%).
Table 4.8. Clinical symptoms in relation to infections in 150 children with diarrhea
Clinical symptoms
Fever Vomiting Dehydration Enteropathogen
n (%) n (%) n (%)
Rotavirus (n = 42) 31 (73.8) 39 (92.9) 6 (14.3)
Salmonella (n = 3) 3 (100) 3 (100) 0 (0.0)
Shigella (n = 9) 9 (100) 6 (66.7) 1 (11.1)
E.coli O157:H7 (n = 7) 3 (42.8) 6 (85.7) 1 (11.1)
Campylobacter (n = 7) 6 (85.7) 5 (71.4) 0 (0.0)
Parasites (n = 26) 23 (88.5) 21 (80.8) 0 (0.0)
4.8. Enteropathogens distributed by residence of the subjects
Most 59.6 % (56/94) of the fecal samples tested positive for enteropathogens
were from Gaza region while 40.4 % were from outside Gaza (39.4 % from
Northern Gaza strip, 1.0% from Mid zone and Southern Gaza strip) Table 4.9.
Moreover, the distribution of rotavirus by residence was statistically significant
(p<0.05)
Table 4.9. Enteropathogens distributed by residence
Area Enteropathogen Northern
Gaza Strip Gaza
Mid zone and Southern Gaza Strip
Total
Rotavirus 9 32 1 42
Salmonella 0 3 0 3
Shigella 5 4 0 9
E.coli O157:H7 5 2 0 7
Campylobacter 4 3 0 7
Parasites 14 12 0 26
Total Positive (%) 37
(64.9%)
56
(62.9%)
1
(25.0%) 94
Total tested sample 57 89 4 150
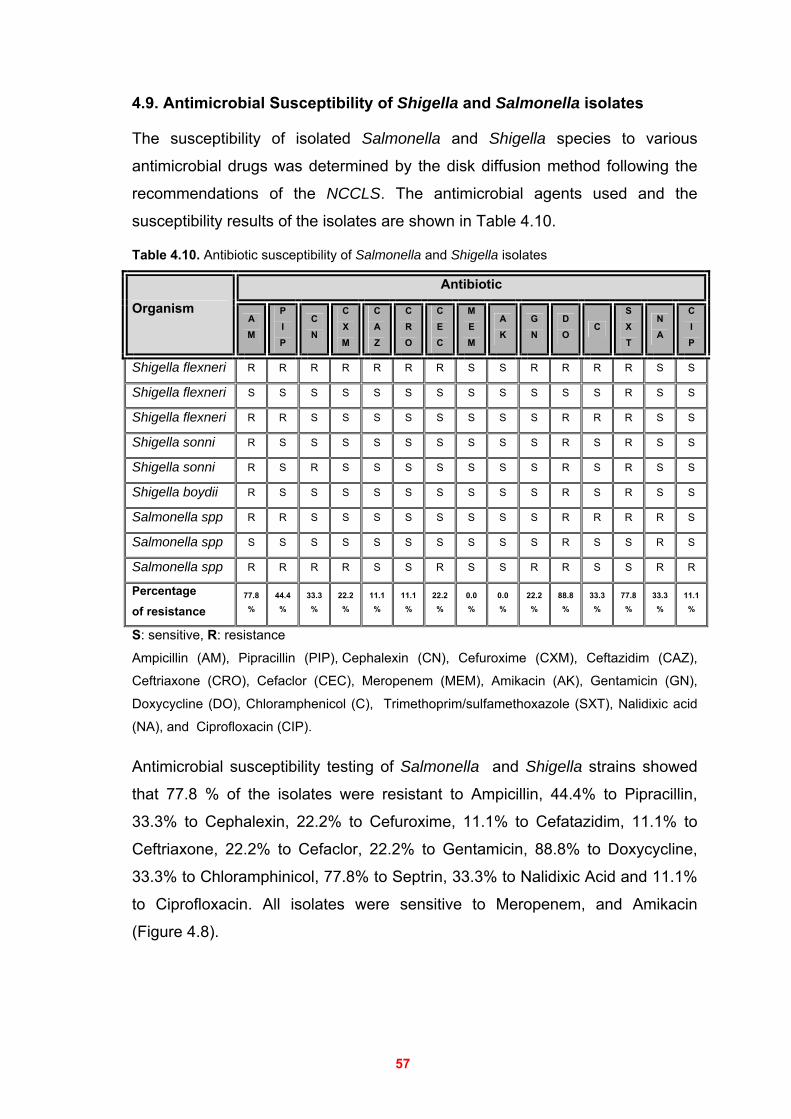
57
4.9. Antimicrobial Susceptibility of Shigella and Salmonella isolates
The susceptibility of isolated Salmonella and Shigella species to various
antimicrobial drugs was determined by the disk diffusion method following the
recommendations of the NCCLS. The antimicrobial agents used and the
susceptibility results of the isolates are shown in Table 4.10.
Table 4.10. Antibiotic susceptibility of Salmonella and Shigella isolates
Antibiotic
Organism A M
P I P
C N
C X M
C A Z
C R O
C E C
M E M
A K
G N
D O
C S X T
N A
C I P
Shigella flexneri R R R R R R R S S R R R R S S
Shigella flexneri S S S S S S S S S S S S R S S
Shigella flexneri R R S S S S S S S S R R R S S
Shigella sonni R S S S S S S S S S R S R S S
Shigella sonni R S R S S S S S S S R S R S S
Shigella boydii R S S S S S S S S S R S R S S
Salmonella spp R R S S S S S S S S R R R R S
Salmonella spp S S S S S S S S S S R S S R S
Salmonella spp R R R R S S R S S R R S S R R
Percentage of resistance
77.8 %
44.4 %
33.3 %
22.2 %
11.1 %
11.1 %
22.2 %
0.0 %
0.0 %
22.2 %
88.8 %
33.3 %
77.8 %
33.3 %
11.1 %
S: sensitive, R: resistance
Ampicillin (AM), Pipracillin (PIP), Cephalexin (CN), Cefuroxime (CXM), Ceftazidim (CAZ),
Ceftriaxone (CRO), Cefaclor (CEC), Meropenem (MEM), Amikacin (AK), Gentamicin (GN),
Doxycycline (DO), Chloramphenicol (C), Trimethoprim/sulfamethoxazole (SXT), Nalidixic acid
(NA), and Ciprofloxacin (CIP).
Antimicrobial susceptibility testing of Salmonella and Shigella strains showed
that 77.8 % of the isolates were resistant to Ampicillin, 44.4% to Pipracillin,
33.3% to Cephalexin, 22.2% to Cefuroxime, 11.1% to Cefatazidim, 11.1% to
Ceftriaxone, 22.2% to Cefaclor, 22.2% to Gentamicin, 88.8% to Doxycycline,
33.3% to Chloramphinicol, 77.8% to Septrin, 33.3% to Nalidixic Acid and 11.1%
to Ciprofloxacin. All isolates were sensitive to Meropenem, and Amikacin
(Figure 4.8).
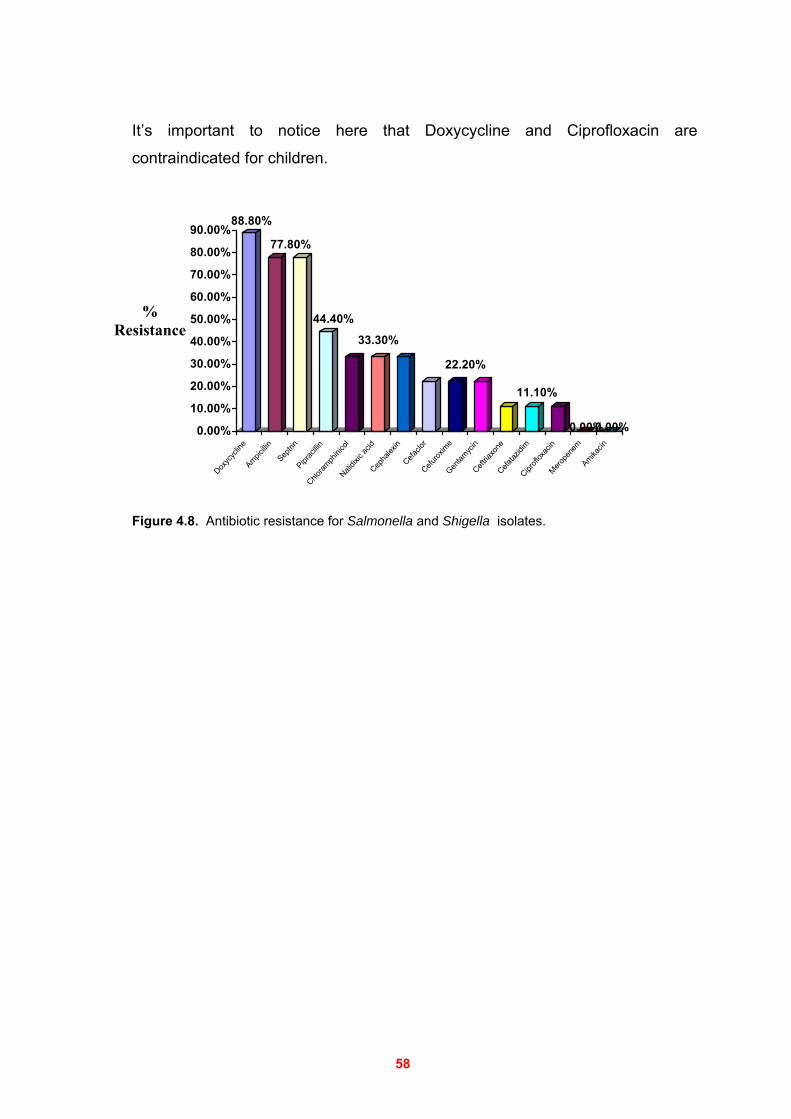
58
It’s important to notice here that Doxycycline and Ciprofloxacin are
contraindicated for children.
88.80%
77.80%
44.40%
33.30%
22.20%
11.10%
0.00%0.00%0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%Dox
ycyc
line
Ampicillin
Septrin
Piprac
illinChlo
ramph
inico
lNali
dixic
acid
Cepha
lexin
Cefaclo
rCefu
roxim
eGen
tamyc
inCeft
riaxo
neCefa
tazidi
mCipr
oflox
acin
Merope
nem
Amikacin
Figure 4.8. Antibiotic resistance for Salmonella and Shigella isolates.
% Resistance

59
Chapter 5 DISCUSSION
Diarrhea remains one of the most common illnesses of children and one of the
major causes of infant and childhood mortality in developing countries.
Considering the usually scanty resources available in the third world countries,
a reduction in diarrhea-related mortality may be possible by identifying high risk
subjects and targeting them for intensive intervention. In the present study, we
were able to identify most of the etiologic agents significantly associated with
early childhood diarrhea.
The aim of this study was to determine the prevalence of enteropathogens,
including bacteria, rotavirus, and parasites, causing diarrhea among children
less than five years old in Gaza, Palestine.
To our knowledge, this is the first study in Gaza investigating several kinds of
possible enteric pathogens in diarrhea in children less than 5 years of age. The
study emphasizes the role of rotavirus, Salmonella, Shigella, Campylobacter
coli/jejuni (c/j), E coli O157:H7 and Parasites in the study group.
This new knowledge on the etiology of diarrhea in the examined patients will
help us plan future studies on various aspects of diarrheal diseases in this
population.
Out of the 150 diarrheal patients enrolled in the study, 63.3% were less than 1
year of age, and 83.9% were less than 2 years of age. This shows a strong
tendency of diarrhea to occur among children less than 2 years of age. This
finding is consistent with other studies conducted in the middle east countries
and various other developing countries where the major burden of diseases due
to most pathogens occurred in the first and second years of life (1,46,127,164). Prevalence of enteropathogens: According to the current study, the
percentage of examined diarrheal cases with a known etiology is 51.5%. When
compared to other studies, this percentage is still lower than that reported by
Nimri and Meqdam (2004) in Jordan where 77.8% of their samples had a
potential enteric pathogen, Souza et al. (2002) in Sao Paulo where 72.8% of
their samples were positive, Albert et al. (1999) in Bangladesh where 74.8% of
the samples had enteropathogens, and Youssef et al. (2000) in Jordan where
66.4% of the samples showed enteric pathogens.
60
However, our percentage is higher than that reported by Battikhi (2002) in
Jordan where he recorded 24.5% as enteropathogens positive, Na'was and
Abo-Shehada (1991) in Jordan where they found 39.5%, and Khan et al.,
(2002) in Bangladesh where 29.5% of the samples had potential enteric
pathogens.
Meanwhile our finding is nearly congruent with that of other studies, such as
that of El-Sheikh and El-Assouli (2001) in Saudi Arabia where they reported that
45.6% of their samples had potential enteric pathogens, and Yoshida et al.
(2000) in Japan where, 46.2% of their samples contained enteropathogens.
These variations could be explained by differences in the study population (e.g.,
genetics of the different ethnic groups), endemicity of enteropathogens,
socioeconomic and specific practices prevalent among the different populations.
In principal, enteric pathogens in feces infect humans via contaminated fluids,
and foods, and personal contact; factors that are associated with the living
standards of people.
Rotavirus is the most common: In the 150 investigated children with diarrhea,
group A rotavirus was the most frequently identified enteric pathogen, where it
was found in 28.0% of the children with diarrhea versus 17.3%, of those with
bacteria. However, parasites played another important role and represented
17.3% of the enteropathogens. These figures are in agreement with those
reported in many studies on diarrhea (192). Moreover, mixed infections were
relatively frequent, as 11.3% of the specimens were found to contain more than
one enteropathogen (68,70). The high incidence of rotavirus recorded in the present study conforms to other
recent investigations, which showed an increasing rate of this virus as a causing
agent of diarrhea, even in developing countries (41). For example, rotavirus was
the most frequent enteropathogen (15 to 40%) encountered in three studied
regions neighboring Palestine namely, Jordan, Egypt, and the occupied
territories (42,188,192). Timely diagnosis of rotavirus infection in patients with acute diarrhea helps
determine appropriate treatment, prevents the unnecessary use of antibiotics
and minimizes the spread of the disease (123,143).
61
In the current study the prevalence of rotavirus infection was significantly higher
in the children less than 2 years of age than in the older ones. The highest
prevalence was seen in children from 13 to 24 months of age 13/31 (41.9%),
followed by those less than 1 year of age 25/95 (26.3%), and the prevalence
decreased in the older children. This result is similar to that published by other
authors (19,80,165). There is a difference in the age distributions of rotavirus infections in developing
and developed countries. In the former, the highest rates occur during the first
year of life. However, in developed countries the peak rates of infection occur
in the second year of life. This could lead to recommending early application of
rotavirus vaccine to children in developing countries (131). Moreover, our study
indicated that there was a trend of decreasing rates of rotavirus infection in the
older children. This might partly be explained by the fact that older children
acquired protective immunity during previous, probably subclinical, exposures to
rotavirus and they therefore become more resistant to infection with this agent
(76,105). Our results emphasize the importance of considering rotavirus
vaccines, which have been undergoing field trials for several years (19,80,165). Although, many recent studies on rotavirus were done in countries neighboring
Palestine, no studies on this virus have been carried out in Gaza since 1994
(151). While numerous studies have demonstrated rotavirus to be a common cause of
diarrhea among young children living in developing nations, most of the studies
have been hospital-based, which potentially detect only the more severe cases
of diarrhea, and thus may underestimate the true incidence of rotavirus
associated diarrhea (19,80). Compared with the community-based study of
rotavirus conducted on Palestinian children in Gaza by Sallon et al. (1994) and
Simhon et.al. (1990), rotavirus was isolated nearly four times less frequently
than in the present study.
Interestingly, incidence of rotavirus disease was observed to be similar in both
industrialized and developing countries, suggesting that adequate control may
not be achieved by improvements in water supply, hygiene, and sanitation.
Thus, the development, trial, and widespread use of rotavirus vaccines were
recommended to prevent severe and fatal rotavirus disease (137).
62
The current study was done during the late spring and summer seasons,
rotavirus infections however, are known to be more common in the winter
season, consequently the true prevalence of rotavirus may be well over than
28.0% if the study has been done during the cold season, and this further
potentiates the importance of rotavirus etiology in diarrhea (49,105,154). Parasites: E histolytica/dispar was the second most common enteric pathogen
found in the present study, the isolation rate was 15.3%, which indicates the
importance of this pathogen among the diarrheal infectious factors. Meanwhile
our finding is nearly congruent with that of other studies, for example Shubair et
al. (2000) found that the prevalence of Entamoeba histolytica among school
children in Gaza was (18.0%), and also in Gaza, AL-Zain and Al-Hindi (2005)
found that Entamoeba histolytica/dispar was evident in 11.4% in the less than 4
years old children. The isolation rate was (1.33%) for Giardia intestinalis and
(0.7%) for Srongyloides stercoralis (11,159). Bacterial enteropathogens: Shigella was the third most common enteric
pathogen identified in the present study, the isolation rate was 6.0%, followed
by Campylobacter c/j (4.7%), E coli O157:H7 (4.7%), and Salmonella (2.0%).
The enteropathogens thus identified reflect the importance of these
microorganisms in the epidemiology of childhood diarrhea in our region and
suggest that either these enteropathogens are more common in our
environment or that they are associated with more severe presentations, as
patients with more severe disease are more likely to seek medical help.
The infections with bacterial, parasitic and some viral pathogens peaked during
the summer time when there are suitable conditions such as humidity and high
temperature which facilitate the bacterial growth and dissemination.
Intestinal nematodes do not seem to play a significant role in diarrheal diseases
in the study area. The low rate of nematodes isolated from the investigated
patients suggests a low incidence of those pathogens in the Gaza region
particularly for patients at this age.
63
Mixed infections: Mixed infections were relatively frequent, among the children
with diarrhea where 17 out of the 150 (11.3%) studied children had infection
with two or more pathogens.
Several previous studies have shown mixed infections in stool samples from
children with diarrhea, including various combinations of different types of
enteropathogens (46,164). In our study, most of the mixed infections were rotavirus with parasite (3.3%),
and Shigella with parasites (3.3%). These findings are in agreement with other
studies conducted in developing countries that reported one or more of these
pathogens (21,129,136,192). Improvement of the techniques and methods used in the detection of
enteropathogens may justify the high rates of detection of mixed infections. Children 3- 4 years old are more susceptible to infection: According to our
results the age groups 25-36, and 37-48 months were more susceptible to
infection with enteropathogens, evidently, there were 8 children in the 25-36
age group who were infected with 8 enteropathogens, and 7 children in the age
group 37-48, who had been infected with 10 enteropathogens. The highest
levels of incidence of most enteropathogens in these two age groups could be
due to several reasons such as: the increased prevalence of enteropathogens
in the environment, increased exposure of those children to environmental
pathogens, the unaware consumption of contaminated foods and drinks, the
relative ease of infection by enteropathogens through the fecal-oral route of
transmission and the bad hygiene practices of children particularly at those
ages.
However, the parental and the social habits of increased attention to younger
children may partially explain the bias observed in the enteropathogen
distribution of the younger age groups.
Looking at children up to 5 months of age, the prevalence of enteropathogens
were 9 cases with rotavirus, 2 cases with parasites, one case with
Campylobacter, and there was no Shigella, Salmonella or E coli O157:H7
recorded.
The low rate of occurrence of bacterial enteropathogens in early infancy (the
first 5 months of life) may be due to breastfeeding, the breastfed infants are less
64
likely to develop bacteria-associated diarrhea, is well documented in the
literature (4,97,176).
In addition to the age distribution of enteropathogenic infections, many studies
have indicated a higher ratio of infected males as compared to females. In our
study the demographic information, epidemiological data and clinical symptoms
show that among the 150 children, the male/female ratio of children with respect
to diarrhea was 1.24, no reasonable explanation has yet been given for this
distribution, but it is possible that the cultural or behavioral norms in our study
area are contributing factors. For example, it is a common practice in many
families to preferentially seek medical care for boys. The genetics of males,
however, may be another contributing factor in the higher susceptibility of males
to get enteropathogenic infections (44,68,130). Enteropathogens in Gaza region: Most of the patients (89/150 ; 59.3%)
admitted with acute gastroenteritis were from the Gaza region, 38.0% (57/150)
were from Northern Gaza Strip, and 2.7% (4/150) were from Mid zone and
Southern Gaza Strip. It is important to note that there is no pediatric hospital in
Northern Gaza Strip. The low number of cases admitted from the mid zone and
Southern Gaza Strip is due to the continuous closures and separation of Gaza
from the Southern area by the Israeli occupation during the study period, and
the presence of some hospitals in that area.
Our results show that the prevalence of enteropathogens identified in diarrhea
specimens was comparable in Northern Gaza Strip (64.9%), and Gaza region
(62.9%).
These high percentages and as pointed earlier, may indicate that either the
enteropathogens are quit prevalent in those environments or that they are
associated with more severe presentations.
The present study revealed that rotavirus was the microorganism associated
most frequently (36.0%) with gastroenteritis in the Gaza region, followed by
parasites and bacteria (13.5% each).
Many authors showed agreement with our results that rotavirus infects children
in urban areas more than the rural areas (112,136).

65
Therefore, the reason of increased rotavirus prevalence in Gaza region might
be due to nosocomial infections in neonatal nurseries, particularly present more
in urban areas than rural ones, especially when mothers spend most of their
time outside the home (worker female), and where the management of rotavirus
infection is difficult.
Enteropathogens in Northern Gaza Strip: In Northern Gaza Strip we found
that parasites and bacteria were the most common pathogens (24.6% each)
followed by rotavirus (15.8%). Differences in the frequency of enteropathogens
in both regions may be due to the different living standards, educational level,
and the agricultural practices. Another important factor is the contaminated
drinking water which represents a potential source of infection (132). Furthermore, the practice of dumping solid wastes in the streets and raising
animals in the living area, as it is common to see children playing in and around
waste disposal sites in Gaza Strip, can certainly cause serious health problems (5). Additionally, flies, other insects and rats are important vehicles in spreading
infectious agents from rotting and contaminated wastes (82). Why do children attend hospitals for investigation? The reasons for
children enrolled in this study to attend the hospital for examination were: (i)
diarrhea only, (ii) diarrhea with vomiting, (iii) diarrhea and fever, and (iv)
diarrhea together with vomiting and fever. Although most of the children
received oral rehydration fluid before hospitalization, some of them were still
dehydrated. Dehydration was more common in children with rotavirus diarrhea.
The most common risks with diarrheal illnesses are dehydration and, in
developing countries, malnutrition. Thus, the critical initial treatment must
include rehydration, which can be accomplished with an oral glucose or starch
containing electrolyte solution in the vast majority of the cases (129). Clinical signs of gastroenteritis: It is not possible to distinguish diarrhea
caused by most enteropathogens clinically, because diarrhea, vomiting, fever ,
and dehydration are not absolutely associated with any of these
enteropathogens infections.
66
Watery stools were predominant (67.3%), followed by mucous stools (21.4%).
Other types of stool accounted for 11.3% of the cases.
Children singly infected with Shigella, or Salmonella had fever with average
temperature significantly higher than that of those infected with rotavirus or
other enteropathogens. Fever has been shown to be a common symptom in
diarrhea caused by Shigella and Salmonella by other authors (15,51). Our study supports the conclusions from other studies that enteropathogens
induce a clinical illness characterized by vomiting, diarrhea, fever, and
dehydration, or various combinations of these symptoms (19,129,164,192). Antimicrobial agents: Antibiotic therapy is not appropriate in the management
of simple gastroenteritis even when a bacterial cause is suspected because
most cases of acute diarrhea are of viral etiology or self-limited.
Antibiotics are recommended for treating bloody diarrhea to shorten the duration
of illness, decrease morbidity and mortality, and reduce the duration of bacterial
shedding (59,148). Antimicrobial resistance among the major bacterial causes
of bloody diarrhea is increasing worldwide (186). Despite this, a recent multicenter study from Europe showed that 44% of
physicians would use antibiotics (43). Furthermore, some studies suggest that
the empiric use of antibiotics in children with E coli O157:H7 infections may
increase the risk of hemolytic uremic syndrome (HUS) (30,139). In spite of the relatively small size of the study sample, we believe that our data
provide useful information about the antimicrobial resistance of Shigella and
Salmonella isolates. In order to help practitioners to choose an adequate
antimicrobial drug to start empirical therapy in a patient with severe diarrhea
without knowledge of a specific pathogen, we assessed the antimicrobial
resistance patterns of Shigella and Salmonella spp that could be isolated.
Antimicrobial susceptibility patterns among the 9 bacterial (3 Salmonella, 6
Shigella) isolates tested from persons with diarrhea were shown in Table 4.10.
The antibiograms of Salmonella and Shigella isolates, showed that the most
frequent patterns of resistance were exhibited towards doxycycline (88.8%),
ampicillin and trimethoprim/sulfamethoxazole (SXT) (77.8% each), cefatazidim,
67
ceftriaxone, and ciprofloxacin had the low resistance pattern, whereas all the
isolates were sensitive to Meropenem, and Amikacin.
Shigella is becoming more resistant to the commonly used antibiotics especially
in the developing countries (3,64,149). However, the prevalence of resistance to
the same antibiotics is lower in developed countries (15,36). The reason could
be the more appropriate usage of antibiotics in the developed as compared to
the developing countries.
Several studies have indicated the high resistance of Salmonella, Shigella to
ampicillin, SXT and doxycyclines which is in agreement with our study
(110,129,168). Multiple antibiotic resistant enteric pathogens have been reported in many
developing countries, especially Pakistan, India, Bangladesh, and The
Philippines (147). In most pediatric hospitals the empirical antimicrobial drugs used in the
treatment of gastroenteritis and diarrhea patients is the intravenous ampicillin,
and the physicians usually prescribe SXT after discharge from the hospital.
The high resistence of our isolates to SXT and ampicillin observed may be
because in the primary heath care in Gaza strip, SXT is the most commonly
used antimicrobial drug for the treatment of gastroenteritis and diarrhea, while
amoxycillin is the most frequently prescribed antibiotic for the treatment of
upper respiratory tract infections (URTIs).
As in the developing countries, ampicillin, chloramphenicol and SXT are widely
used to treat diarrhea because of their low cost and ready availability. Most
children in our community treated with antibiotics had been purchased from
private drug outlets.
Our study results show that Shigella isolates were completely sensitive to
nalidixic acid. Other studies have also found little resistance to nalidixic acid
among Shigella in many countries (4,28). The use of nalidixic acid is recommended by the World Health Organization for
the management of acute bloody diarrhea in children, and it may remain an
important option for the treatment of acute infectious diarrhea, especially in
services that cannot afford far more expensive drugs (184).
68
However, in areas where nalidixic acid has been introduced as the drug of
choice to treat presumptive shigellosis, a marked increase in corresponding
resistance has been observed (4,15). Misuse of antibiotics has resulted in increased resistance to most of the
commonly used drugs for treatment. A call to regulate the use of antimicrobials
may be necessary.
According to our study, ampicillin, trimethoprim/sulfamethoxazole, and
doxycycline should not be used for treatment of diarrhea in children. Moreover,
it should be taken into consideration that in spite of the low bacterial resistance
to amikacin and meropenem, if they were widely used, a rapid emergence of
resistance would likely to occur.
According to the results of this study and in very severe cases, with evidence of
dissemination of disease, intravenous amikacin or meropenem, cefatazidim,
ceftriaxone, and ciprofloxacin is the best choice.
It is worth noting here that it has been recommended by the NCCLs in 1999
that, aminoglycosides and first generation cephalosporins may appear active in
vitro but are not effective clinically and should not be reported as susceptible
(NCCLs 1999) (126). In conclusion, the current study highlights the necessity for continuous
monitoring of antibiotic resistance in diarrhea related bacterial pathogens.
Some of the above antibiotics were employed to characterize the isolates, but
did not have any clinical utility in the treatment of diarrhea.
Bacterial detection methods: Shigella species were identified in 6 cases
(4.0%) by bacteriological culture, Shigella flexneri was found with the highest
prevalence (50%) among the isolated Shigella spp, emphasizing the importance
of this pathogen in the epidemiology of childhood bacterial diarrhea in Gaza,
and indicating that either S. flexnerri is more common in our environment or it is
more associated with severe diarrheal presentations.
Shigella flexneri was the predominant species isolated among Shigella spp.
during this study, followed by S. sonnei. This finding is consistent with other
reports from developing countries such as India, Bangladesh, Brazil, Tanzania,
Egypt, and Thailand. Our results are in good agreement with this trend
(148,170).
69
The prevalence of Shigella recorded in this study is similar to that reported by
other investigators in many neighboring countries such as Saudi Arabia, Jordan,
Lebanon, Kuwait, and Israel (96,120,121,155,193), with the exception of one
study from Saudi Arabia which reported that over 17% of the tested specimens
were positive for Shigella (8). Our percentage is however higher than the detection rate of Gaza strip health
laboratories for Shigella which was 0.2 % (117). Three cases (2%) proved positive for Salmonella both by culture and PCR. The
detection rate of Gaza strip health laboratories for Salmonella is only 0.4 %
(117). Other reports from Gaza and neighboring countries indicate that the detection
rate of Salmonella ranges from 2% to 18% (8,121,151,155). The very low detection rate of Salmonella and Shigella by Gaza strip health
laboratories might be due to the low sensitivity of the culture methods
employed, since they use only one or two selective agar media (usually SS agar
and Selenite-F enrichment broth) for isolation of these bacteria.
Selenite-F broth is not suitable, particularly for isolation of S. paratyphi A and S.
choleraesuis. Additionally, some strains of Shigella fail to multiply at all in this
enrichment broth (174). Moreover, many studies have pointed that SS agar,
could inhibit the growth of many strains of Shigella (106,180). Another factor that may explain the low recovery of Salmonella or Shigella from
stool specimens cultures in Gaza strip health laboratories is the delay in
ordering stool cultures since physicians sometimes ask for stool cultures after >
4 days of hospitalization and after children treatment had failed.
The recovery rate of Salmonella spp., Shigella spp., and Campylobacter spp.
from stool culture has been shown to decrease by more than the quarter when
patients have been hospitalized for > 3 days (146). Additionally, antibiotic therapy prior to specimen collection and delay for > 3 h in
delivering some of the specimens to the laboratory for processing could be
responsible for the low yield of bacterial cultures.
In this study at least three selective media and two enrichment broths were
employed, and in addition to the usual biochemical tests and serotyping, the
bacteriological screening was reinforced by a molecular approach i.e., PCR
assays.
70
E. coli O157:H7 was found in 6 (4.0%) diarrheal cases by bacteriological
culture. This microorganism is not routinely analyzed in our clinical laboratories.
E coli O157:H7 has been associated with 10-15% of bloody diarrheas by
several investigators (145,157). Children with gastrointestinal infections caused by E. coli O157:H7 are at risk
for the hemolytic-uremic syndrome (HUS) which can be fatal as it may lead to
acute kidney failure. Furthermore, some studies suggest that the empiric use of
antibiotics in children with E coli O157:H7 infections may increase the risk of
HUS (52,189). Consequently, the identification of the causative agent of
diarrhea may be life-saving.
PCR is more sensitive and specific than conventional culture methods:
Identification of Campylobacter is well known to be problematic, principally
because of their complex taxonomy, biochemical inertness, and fastidious
growth requirements (74,152). As a result of the fastidiousness and diversity of Campylobacter, it is clear that
no one medium will provide an accurate measure of their occurrence.
Furthermore, inexperienced personnel can easily overlook Campylobacter
colonies, and the species may be missed. For this reason, the use of PCR-
based detection methods is becoming more attractive.
Campylobacter c/j was detected in 4.7% (7/150) of the stool samples when
analyzed by PCR assay. It was isolated in Gaza two times more frequently than
in the present study (151). Culture methods are biased toward the detection of Campylobacter spp. since a
number of antimicrobial agents is commonly incorporated into the selective
media (e.g., Preston agar, Skirrow agar, and Butzler agar). These drugs may
inhibit the growth of some Campylobacter species. Cephalothin, colistin, and
polymyxin B can be inhibitory to some strains of C. jejuni and C. coli (39). As a
result, microbiological methods do not provide a true measure of the frequency
and diversity of Campylobacter species associated with diarrhea.
The etiological agents could not be determined in 73 (48.7%) of the 150
investigated specimens. The causative agents might be bacterial, viral or other
infectious agents not considered in this research. Chemicals, oral antibiotics,

71
stress, food allergies or dietary indiscretion are other factors that may cause
diarrhea. Actually the problem of recognizing an associated pathogen in all
diarrhea specimens is usually difficult, even during the onset of outbreaks
(59,129). Shigella spp was detected in 4.0% and in 6.0% of the stool samples when
analyzed by the bacteriological culture and PCR assay, respectively. By the use
of PCR we found that 3 of the samples were Shigella spp positive by PCR and
not by culture. E coli O157:H7 was detected in 4.0% and in 4.7% of the samples
when analyzed by conventional culture method and PCR, respectively. By use
of PCR we found one sample of E coli O157:H7 that was positive by PCR while
it was not resolved by culture. Salmonella spp was detected in 2.0% of the
specimens by both culture, and PCR.
In total we found that 4/19 (21.1%) enteropathogen positive specimens by PCR
that the bacteriological stool cultures failed to detect.
PCR is a selective, sensitive, and specific assay that can detect a small number
of culturable as well as non-culturable organisms. Such detection is especially
important for Shigellae, since they can produce disease by as few as 10 to 100
organisms. In our study, the use of PCR technique improved the rate of
detecting Shigellae in stool samples from 6 to 9 positive samples; which is
33.3% (3/9) higher than the conventional culture method. Moreover, the time
requirement of this technique is quite shorter when compared to that of the
culture technique.
The assay was extremely reliable, being able to detect 100% of culture-
confirmed bacterial infections in the study specimens. Furthermore, it also
detected 4 culture negative clinically important gastroenteritis cases, indicating
the high level of efficiency of the assay system. Thus, PCR may be judged as
superior for its rapidity and sensitivity in the detection of Shigellae. Moreover,
since this method is applied without cultivation of the organism on synthetic
media, nonculturable populations of Shigellae can also by detected by this
method.
The PCR assay can be chosen as an alternative to the culture technique, and
can further be used for identifying asymptomatic carriers who serve as potential
reservoirs of Shigellae, and silently transmit the disease within the community.
72
Relative to microbiological isolation, PCR was found to be more sensitive for
detecting Campylobacter in many studies; the advantages of PCR over
conventional isolation methods witnessed in this study are congruent with the
conclusions of Lawson et al. who found that direct PCR of human feces
provided unique data in detection of Campylobacter (94,101).
Our method requires approximately 4 h, from manipulating samples to reading
the results. This time includes 1 h for DNA extraction from the stool specimens
and 2-3 h for the PCR assay as compared to 48-72 hours of standard stool
culture. It detected pathogens in culture negative stool specimens derived from
patients who had been linked to gastroenteritis or a food poisoning outbreak.
Hence, we conclude that this PCR-based method contributes to improvement of
the rapid diagnosis of enteric bacterial infections, whilst yielding higher
detection rates of causative agents (71). Other advantages include its high sensitivity, specificity and ease of operation,
furthermore, no radio-isotopes or their dangerous concomitants are involved.
Two problems are associated with the detection of bacteria in stool by PCR:
stool matrices may inhibit the PCR, and the PCR cannot distinguish the DNA of
living cells from that of dead cells. To overcome these two problems, several
investigators have used DNA isolation and purification methods using a
modified procedures such as a ready kits for isolation, and various enrichment
culture methods (63,69,124,182). We believe that enrichment culture methods may be helpful in distinguishing
living cells from dead cells. Therefore, we applied a short enrichment culture
step (3-4 hours) with BHI (brain heart infusion broth) medium prior to PCR
detection of Salmonella, Shigella, and E. coli O157:H7 (181). Bacterial DNA was prepared by a simple DNA extraction method with the use of
a ready-to-use kit in order to reduce the potential inhibitory effects of PCR by
stool matrices.
Finally the applications of the techniques such as PCR, immunoassay, and
culture will improve the quality of detection of the pathogens. This will make the
clinical diagnosis better and help the pediatricians in treatment of children with
diarrhea.
73
CHAPTER 6 CONCLUSION and RECOMMENDATIONS
The present study focused on detection and identification of some potential
enteric pathogens causing diarrhea (viral, bacterial, and parasites) in 150
children less than 5 years of age in Gaza, Palestine. The results of the study
can be summarized as follows:
1. Analysis of data according to age showed a significant association with
diarrhea for all enteropathogens in the first two years of life except for
Shigella, which had an overall association with diarrhea in older age
group.
2. We found that 75.5% of positive diarrheal cases occurred in the age
groups below 2 years (53.2% in the age group 0-12 months, and 22.3%
in the age group 13-24 months). Rotavirus was the highest (13/31,
41.9%) among infants in the age group 13-24 months old.
3. We detected one or more enteropathogen in 77 cases (51.3%) of the
diarrhea patients examined.
4. Mixed infections were relatively frequent mainly and were in the form of
rotavirus with parasite, and Shigella with parasite.
5. Rotavirus was confirmed as the most common pathogen in childhood
diarrhea (28.0% of the diarrheal cases), especially in children less than 2
years. This fact, in combination with the severity of the infections,
warrants consideration of a rotavirus vaccine in the childhood
immunization program. Timely diagnosis of rotavirus infection in patients
with acute diarrhea helps determine appropriate treatment, prevents the
unnecessary use of antibiotics, minimizes the spread of the disease and
decreases the cost of hospitalization.
6. The current study was done during the late spring and summer seasons,
rotavirus infections however, are known to be more common in the winter
season, consequently the true prevalence of rotavirus may be well over
than 28.0% if the study has been done during the cold season, and this
further potentiates the importance of rotavirus etiology in diarrhea.
74
7. Shigella species were found in 9 cases (6.0%) by PCR and in only 6
cases (4.0%) by bacteriological culture, with higher frequency of S.
flexneri (3/6) in relation to S. sonnei (2/6), and S. boydii (1/6).
8. Salmonella spp. was found in 3 cases (2.0 % of diarrheal cases) as
revealed both by PCR and bacteriological culture.
9. E. coli O157:H7 was found in 7 cases (4.7%) by PCR, and in 6 (4.0%) of
the diarrheal cases by bacteriological culture.
10. Campylobacter was evident in 7 (4.7%) of the diarrheal cases as
revealed by PCR only.
11. By the use of PCR we found that 4/19 (21.1%) of enteropathogens
positive specimens by PCR that the bacteriological stool culture revealed
negative. PCR seem to be safer, more sensitive and more rapid than the
conventional culture methods for the diagnosis of bacteria. PCR-based
method contributes to improvement of the rapid diagnosis of enteric
bacterial infections, whilst yielding higher detection rates of causative
agents. Our findings highlight the value of using a combination of
traditional and molecular techniques in the diagnosis of diarrheal disease
in this population.
12. Our study also emphasizes the importance of E. histolytica/dispar in
causing diarrhea at the study age.
13. The age groups 25-36, and 37-48 months were more susceptible to
infection with enteropathogens (especially Shigella and parasites). The
development of a polyvalent vaccine that covers strains of S. flexneri and
S. sonnei would be predicted to provide protection against Shigella
infections occurring in Palestine.
14. Fever, vomiting, diarrhea and dehydration were the most common
clinical signs of the studied enteropathogens. We recommend visiting a
Health Care Professional if your child has diarrhea as well as vomiting or
fever. The dehydration status of the diarrheal children was observed
more common in rotavirus infection, (14.3%), followed by Shigella
(11.1%), and E. coli O157:H7 (11.1%).
15. The antibiograms of Salmonella and Shigella isolates, showed that the
most frequent patterns of resistance were exhibited towards Doxycycline
(88.8%), Ampicillin and trimethoprim/sulfamethoxazole (77.8% each),
75
cefatazidim, ceftriaxone, and ciprofloxacin had the low resistance
pattern, whereas all the isolates were sensitive to Meropenem, and
Amikacin. Ampicillin, trimethoprim/sulfamethoxazole, and doxycycline
should not be used for treatment of diarrhea in children. Amikacin or
meropnem, cefatazidim and ceftriaxone are the best choice for treatment
of infectious diarrhea. The current study highlights the necessity for
continuous monitoring of antibiotic resistance in diarrhea related bacterial
pathogens
16. We recommend the use of both Selenite cysteine broth and GN broth for
pre-enrichment of stool samples beside the use of a minimum of two
selective agar media other than SS agar ( such as HE and/or XLD) to
solve the very low detection rate of Salmonella and Shigella by Gaza
strip health laboratories. Additionally, antibiotic therapy prior to specimen
collection and delay for > 3 h in delivering some of the specimens to the
laboratory for processing should be minimized as they may be
responsible for the low yield of bacterial cultures. We recommend
physicians to request Salmonella spp., Shigella spp., and Campylobacter
spp. cultures as early as patients are hospitalized.
17. We recommend that hospital and private laboratories in Gaza strip to
detect all diarrheal stool samples for rotavirus and to culture routinely
stool specimens on sorbitol-MacConkey agar, the standard culture
medium for E coli O157: H7. We also strongly encourage health care
providers to determine the etiology of diarrhea before prescribing
antibiotics. Children with gastrointestinal infections caused by E. coli
O157:H7 are at risk of developing hemolytic-uremic syndrome (HUS)
which can be fatal as it may lead to acute kidney failure.
18. Improved hygiene, health education, drinking clean water, breast feeding
(which helps in providing passive immunity in the newborn for at least 6
months) are highly recommended in order to minimize the infection rate
of many enteropathogens. Furthermore, the practice of dumping solid
wastes in the streets and raising animals in the living areas should be
minimized

76
Finally, diarrhea is still a health problem in children not only in Gaza, but also
nationwide in Palestine. Some enteric pathogens such as rotavirus, Entamoeba
histolytica/dispar, and Shigella, are the major causes of diarrhea. This study has
highlighted many of the enteric pathogens that cause diarrhea in children in
Gaza. The application of techniques such as PCR and immunoassay will
improve the quality of detection of the pathogens. This will make the clinical
diagnosis better and help the pediatricians in treatment of children with
diarrhea. The findings from the study will also help the policy makers to improve
the health care program to provide better services to children.
To our knowledge, this is the first study in Gaza investigating several kinds of
possible enteric pathogens in diarrhea in children less than 5 years of age.
Based on the preliminary data presented by this study, further work is needed in
order to provide a broader picture of the burden of rotavirus and other
enteropathogens in children less than 5 years old all over Gaza strip.
##########
77
CHAPTER 7 REFERENCES
1. Abu Mourad T.A. (2004). Palestinian refugee conditions associated with intestinal parasites and diarrhoea: Nuseirat refugee camp as a case study. Pub Heal. 118, 131–142
2. Abu-Elyazeed RR, Wierzba T F., Frenck R W., Putnam S D., Rao M R., Savarino S J., Kamal K A., Peruski L F., Abd-El Messih I A., El-Alkamy S A., Naficy A B., and Clemens J D. (2004). Epidemiology of Shigella-associated diarrhea in rural Egyptian children. Am J Trop Med Hyg. 71(3):367-72.
3. Adeleye A, and Adetosoye I, 1993. Antimicrobial resistance patterns and plasmid survey of Salmonella and Shigella isolated is Ibadan, Nigeria. East Afr Med J 70: 259–262.
4. Ahmed F, Clemens D, Rao R, Ansaruzzaman M, and Haque E. (1997). Epidemiology of shigellosis among children exposed to cases of Shigella dysentery: a multivariate assessment. Am J Trop Med Hyg 56: 258–264
5. Al-Agha M. (1997). Environmental management in the Gaza Strip. Environ Impact Assess Rev;17:65—76.
6. Albert J, Faruque S, Faruque M, Sack B, and Mahalanabis D. (1999). Case-control study of enteropathogens associated with childhood diarrhea in Dhaka, Bangladesh. J Clin Microbiol. 37(11):3458-64.
7. Ali MB, Ghenghesh KS, Aissa RB, Abuhelfaia A, and Dufani M. (2005). Etiology of childhood diarrhea in Zliten, Libya. Saudi Med J. 26(11):1759-65.
8. Al-Jurayyan NA, al Rashed AM, al-Nasser MN, al- Mugeiren MM, and al Mazyad AS. (1994). Childhood bacterial diarrhoea in a regional hospital in Saudi Arabia: clinicoaetiological features. J Trop Med Hyg 97:87-90.
9. Altindis M, Yavru S, Simsek A, Ozkul A, Ceri A, and Koc H. (2004). Rotavirus infection in children with acute diarrhea as detected by latex agglutination, ELISA and polyacrylamide gel electrophoresis. Indian Pediatr. 41(6):590-4.
10. Alvarez J, Sota M, Vivanco AB, Perales I, Cisterna R, Rementeria A, and Garaizar J. (2004). Development of a multiplex PCR technique for detection and epidemiological typing of salmonella in human clinical samples. J Clin Microbiol. 42(4):1734-8.
11. AL-Zain B and Al-Hindi A. (2005). Distribution of Strongyloides stercoralis and other intestinal parasites in household in Beit-lahia city, Gaza Strip, Palestine. Annals of alquds med. 1: 48-52
12. Amar CF, East C, Maclure E, McLauchlin J, Jenkins C, Duncanson P, and Wareing DR. (2004). Blinded application of microscopy, bacteriological culture, immunoassays and PCR to detect gastrointestinal pathogens from faecal samples of patients with community-acquired diarrhoea. Eur J Clin Microbiol Infect Dis. 23(7):529-34.
13. American Medical Association; Centers for Disease Control and Prevention; Center for Food Safety and Applied Nutrition et al. (2001). Diagnosis and management of foodborne illnesses: a primer for physicians. MMWR Recomm Rep. 26;50(RR-2) 1-69
14. Armon K, and Elliott E. (2000). Acute gastroenteritis. Evidence based pediatrics and child health. BMJ. 273-286
15. Ashkenazi, S, May-Zahav M, Sulkes J, Zilberberg R, and Samra Z. (1995). Increasing antimicrobial resistance of Shigella isolates in Israel during the period 1984 to 1992. Antimicrob. Agents Chemother. 39:819-823.
16. Awad R, and Abu Arquob O. (2000). The status of health in Palestine: HMIS-MOH 2001.
17. Babalola O. (2003). Molecular techniques: An overview of methods for the detection of bacteria. Afric J of Biotech 2 (12): 710-713.
18. Ballal M, and Shivananda PG. (2002). Rotavirus and enteric pathogens in
78
infantile diarrhoea in Manipal, South India. Indian J Pediatr. 69(5):393-6. 19. Barnes G, Uren E, Stevens K, and Bishop R. (1998). Etiology of Acute
Gastroenteritis in Hospitalized Children in Melbourne, Australia, from April 1980 to March 1993. J Clin Microbiol. 36(1): 133–138.
20. Bass D. (1996). Rotaviruses and other agents of viral gastroenteritis. In: Nelson text book of pediatrics 15th edition. p914-916. W.B. Saunders Co. London.
21. Battikhi MN. (2004). Bloody diarrhoea cases caused by Shigella and amoeba in Jordan. New Microbiol. 27(1):37-47.
22. Battikhi MN. (2002). Epidemiological study on Jordanian patients suffering from diarrhoea. New Microbiol. 25(4):405-12.
23. Bej A. K., Steffan R. J., DiCesare J. L., Haf L. and Atlas R. M. (1991). Detection of Escherichia coli and Shigella spp. in water using the polymerase chain reaction and gene probes for uid. Appl. Environ. Microbiol. 57(4), 1013-1017.
24. Bern C, Martines J, de Zoysa I, and Glass RI. (1992). The magnitude of the global problem of diarrhoeal disease: a ten-year update. Bulletin of the World Health Organization; 70:705-14.
25. Beutin L, Krause G, Zimmermann S, Kaulfuss S, and Gleier K. (2004). Characterization of Shiga toxin-producing Escherichia coli strains isolated from human patients in Germany over a 3-year period. J Clin Microbiol. 42(3):1099-108.
26. Blachlow NR, and Greenberg HB. (1991). Review article: viral gastroenteritis. New Engl Jof Med 325:252–264
27. Bon F, Fascia P, Dauvergne M, Tenenbaum D, Planson H, Petion AM, Pothier P, and Kohli E. (1999). Prevalence of group A rotavirus, human calicivirus, astrovirus, and adenovirus type 40 and 41 infections among children with acute gastroenteritis in Dijon, France. J of Clin Microbio 37:3055–3058
28. Brooks JT, Shapiro RL, Kumar L, Wells JG, Phillips-Howard PA, Shi YP, Vulule JM, Hoekstra RM, Mintz E, and Slutsker L. (2003). Epidemiology of sporadic bloody diarrhea in rural Western Kenya. Am J Trop Med Hyg. 68(6):671-7.
29. Buser J, Risch L, Rutz T, Manang S, and Munzinger J. (2001). Comparison of rotavirus latex agglutination test with two rapid immunochromatographic test devices for detection of rotavirus in human feces. Eur J Clin Microbiol Infect Dis 20: 295-296.
30. Butler T, Islam MR, Azad MA, and Jones PK, (1987). Risk factors for development of hemolytic uremic syndrome during shigellosis. J Pediatr 110: 894–897.
31. Cappuccino J., and Sherman N., (2002). Microbiology A Laboratory Manual 6th ed. Pearson Education, Inc.
32. CDC. (2002). Salmonella Surveillance Summary, Atlanta, Georgia: US Department of Health and Human Services, CDC, 2003.
33. Cebula TA, Payne W L, and Feng P. (1995). Simultaneous identification of strains of Escherichia coli serotype O157:H7 and their Shiga-like toxin type by mismatch amplification mutation assay-multiplex PCR. J of Clin Microbiol. 33(1): 248 – 250
34. Chakravarti A, Kumar S, Mittal SK, and Broor S. (1991). Comparison of latex agglutination and polyacrylamide gel electrophoresis with enzyme linked immunosorbent assay for detecting human rotavirus in stool specimens. Indian Pediatr. 28: 507-10.
35. Chiu, C.-H., and J. T. Ou. (1996). Rapid identification of Salmonella serovars in feces by specific detection of virulence genes, invA and spvC, by an enrichment broth culture-multiplex PCR combination assay. J. Clin. Microbiol. 34:2619–2622.
36. Chu, Y. W., Houang E. T., Lyon D. J., Ling J. M., T. K. Ng, and Cheng A. F. (1998). Antimicrobial resistance in Shigella flexneri and Shigella sonnei in Hong Kong, 1986 to 1995. Antimicrob. Agents Chemother. 42:440-443.
37. Clark B, and McKendrick M. (2004). A review of viral gastroenteritis. Curr
79
Opin Infect Dis. 17(5):461-9. 38. Cohen, N. D., Martin L. J., Simpson R. B., Wallis D. E., and Neibergs H. L.
(1996). Comparison of polymerase chain reaction and microbiological culture for detection of salmonellae in equine feces and environmental samples. Am. J. Vet. Res. 57:780–786.
39. Corry, J. E., Post D. E., Colin P., and Laisney M. J. (1995). Culture media for the isolation of campylobacters. Int. J. Food Microbiol. 26:43-76.
40. Cubbon MD, Coia JE, Hanson MF, and Thomson-Carter FM (1996). A comparison of immunomagnetic separation, direct culture and polymerase chain reaction for the detection of verocytotoxin-producing Escherichia coli O157 in human faeces. J Med Microbiol. 44(3):219-22.
41. Cunliffe NA, Kilgore PE, Breese JS, Steele AD, Luo N, and Hart CA, et al. (1998). Epidemiology of rotavirus diarrhoea in Africa: A review to assess the need for rotavirus immunization. Bull Wld Hlth Organ;76:525-37.
42. Dagan R, Bar-David Y, Sarov B, Katz M, Kassis I, Greenberg D, Glass RI, Margolis CZ, and Sarov I. (1990). Rotavirus diarrhea in Jewish and Bedouin children in the Negev region of Israel: epidemiology, clinical aspects and possible role of malnutrition in severity of illness. Pediatr Infect Dis J. May;9(5):314
43. Davidson G, Barnes G, Bass D, Cohen M, Fasano A, Fontaine O, and Guandalini S. (2002). Infectious diarrhea in children: Working Group Report of the First World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 35 (2): S143-50.
44. Diniz-Santos D R, Santana J S, Barretto J R, Andrade M, and Silva L R. (2005). Epidemiological and Microbiological Aspects of Acute Bacterial Diarrhea in Children from Salvador, Bahia, Brazil. The Braz J of Infec Disea. 9(1):77-83
45. Dutta S, Chatterjee A, Dutta P, Rajendran K, Roy S, Pramanik KC, and Bhattacharya SK. (2001). Sensitivity and performance characteristics of a direct PCR with stool samples in comparison to conventional techniques for diagnosis of Shigella and enteroinvasive Escherichia coli infection in children with acute diarrhoea in Calcutta, India. J of Med Microbiol. 50(8): 667 - 674.
46. El-Sheikh SM, and El-Assouli SM. (2001). Prevalence of viral, bacterial and parasitic enteropathogens among young children with acute diarrhoea in Jeddah, Saudi Arabia. J Health Popul Nutr. 19(1):25-30.
47. Endtz, H. P., Ruijs G. J., Zwinderman A. H., Van der Reijden T., Biever M., and Mouton R. P. (1991). Comparison of six media, including a semisolid agar, for the isolation of various Campylobacter species from stool specimens. J. Clin. Microbiol. 29:1007–1010.
48. Eyers, M., Chapelle S., Van Camp G., Goossens H., and De Wachter R. (1993). Discrimination among thermophilic Campylobacter species by Polymerase chain reaction amplification of 23S rRNA gene fragments. J. Clin. Microbiol. 31:3340–3343.
49. Fang ZY, Yang H, Qi J, Zhang J, Sun LW, Tang JY, Ma L, Du ZQ, He AH, Xie JP, Lu YY, Ji ZZ, Zhu BQ, Wu HY, Lin SE, Xie HP, Griffin DD, Ivanoff B, Glass RI, and Gentsch JR. (2002). Diversity of rotavirus strains among children with acute diarrhea in China: 1998-2000 surveillance study. J. Clin. Microbiol. 40:1875–1878.
50. Feder I, Nietfeld JC, Galland J, Yeary T, Sargeant JM, Oberst R, Tamplin ML, and Luchansky JB. (2001). Comparison of cultivation and PCR-hybridization for detection of Salmonella in porcine fecal and water samples. J Clin Microbiol. 39(7):2477-84.
51. Finkelistein, Y., Moran O., Avitzur Y., Nussinovitch M., Harel L., and Volovitz B., et al. ( 2002). Clinical dysentery in hospitalized children. Infection. 30: 132-135.
52. Fischer H, König P, Dierich MP, and Allerberger F. (2001). Hemolytic uremic syndrome surveillance to monitor trends in infection with Escherichia coli 0157 and non-0157 EHEC. Ped Infect Dis J. 20: 316-8.
53. Fukushima H, Tsunomori Y, and Seki R. (2003). Duplex real-time SYBR
80
green PCR assays for detection of 17 species of food- or waterborne pathogens in stools. J Clin Microbiol. 41(11):5134-46.
54. Giesendorf, B. A., and Quint W. G.. 1995. Detection and identification of Campylobacter spp. using the polymerase chain reaction. Cell. Mol. Biol. 41:625–638.
55. Gil A I, Lanata C F, Kleinau E F, and Penny M E. (2004). Strategic report 11, children’s feces disposal practices in developing countries and interventions to prevent diarrheal diseases, a literature review. U.S. Agency for International Development Washington, DC 20523
56. Gilbert C, Winters D, O'Leary A, and Slavik M. (2003). Development of a triplex PCR assay for the specific detection of Campylobacter jejuni, Salmonella spp., and Escherichia coli O157:H7. Mol Cell Probes. 17(4):135-8.
57. Giordano MO, Ferreyra LJ, Isa MB, Martinez LC, Yudowsky SI, and Nates SV. (2001). The epidemiology of acute viral gastroenteritis in hospitalized children in Cordoba City, Argentina: an insight of disease burden. Rev Inst Med Trop Sao Paulo. 43(4):193-7.
58. Grennan, B., Osullivan N. A., Fallon R., Carroll C., Smith T., Glennon M., and and Maher M. (2001). PCR-ELISAs for the detection of Campylobacter jejuni and Campylobacter coli in poultry samples. BioTechniques 30:602–610.
59. Guerrant RL, Van Gilder T, Steiner TS, Thielman NM, Slutsker L, Tauxe RV, Hennessy T, Griffin PM, DuPont H, Sack RB, Tarr P, Neill M, Nachamkin I, Reller LB, Osterholm MT, Bennish ML, and Pickering LK. (2001). Practice guidelines for the management of infectious diarrhea. Clin Infect Dis 32: 331–351.
60. Guerrant RL. (1998). Why America must care about tropical medicine: threats to global health and security from tropical infectious diseases. Am J Trop Med Hyg. 59(1): 3–16
61. Helms M, Simonsen J, and Molbak K. (2006). Foodborne bacterial infection and hospitalization: a registry-based study. Clin Infect Dis. 15;42(4):498-506.
62. Herikstad H., Motarjemi Y., and Tauxe R. V. (2002). Salmonella surveillance: a global survey of public health serotyping. Epidemiol. Infect. 129:1-8
63. Hill. W. E. (1996). The polymerase chain reaction: applications for the detection of foodborne pathogens. Cril. Rev. Food Sci. Nutr. 36: 123-173.
64. Hoge C. W., Gambel J. M., Srijan A., Pitarangsi C., and Echeverria P. (1998). Trends in antibiotic resistance among diarrheal pathogens isolated in Thailand over 15 years. Clin. Infect. Dis. 26:341-345
65. Holland JL, Louie L, Simor AE, and Louie M. (2000). PCR detection of Escherichia coli O157:H7 directly from stools: evaluation of commercial extraction methods for purifying fecal DNA. J Clin Microbiol. 38(11):4108-13.
66. Hong BX, Jiang LF, Hu YS, Fang DY, and Guo HY. (2004). Application of oligonucleotide array technology for the rapid detection of pathogenic bacteria of foodborne infections. J Microbiol Methods. 58(3):403-11.
67. Hoorfar J., Ahrens P., and Radstrom P. (2000). Automated 5' nuclease PCR assay for identification of Salmonella enterica. J. Clin. Microbiol. 38:3429-3435
68. Howard P, Alexander ND, Atkinson A, Clegg AO, Gerega G, Javati A, Kajoi M, Lupiwa S, Lupiwa T, Mens M, Saleu G, Sanders RC, West B, and Alpers MP. (2000). Bacterial, viral and parasitic aetiology of paediatric diarrhoea in the highlands of Papua New Guinea. J Trop Pediatr. 46(1):10-14.
69. Hsu, S. and Tsen H. (2001). PCR primers designed from malic acid dehydrogenase gene and their use for detection of Escherichia coli in water and milk samples. Int J Food Microbiol. 64:1-11
70. Huilan S, Zhen LG, Mathan MM, Mathew MM, Olarte J, Espejo R, Khin Maung U, Ghafoor MA, Khan MA, and Sami Z, et al. (1991). Etiology of acute diarrhoea among children in developing countries: a multicentre study
81
in five countries. Bull WHO; 69(5):549-555. 71. Iijima Y, Asako N. T., Aihara M., and Hayashi K. (2004). Improvement in
the detection rate of diarrhoeagenic bacteria in human stool specimens by a rapid realtime PCR assay. J Med Microbiol 53, 617–622
72. Isenberg H. (1998). Essential procedures for clinical microbiology. ASM Press. Washington, D.C.
73. Islam M, Hossain M, Hasan M, Rahman MM, Fuchs G, Mahalanabis D, Baqui AH, and Albert MJ. (1998). Detection of Shigellae from stools of dysentery patients by culture and polymerase chain reaction techniques. J Diarrhoe Disea Res. 16(4): 248 - 251.
74. Jan M. H, Carlos A and Tony T. (1998). Bacteriological Analytical Manual, 8th Edition, Revision A, Chapter 7. http://www.cfsan.fda.gov/-ebam/bam-7.html
75. Jenkins, C.T. (1988). An evaluation of five commercially available kits for the diagnosis of rotavirus infection. Serodia and Immunoth in Infect Dis. 2: 137-141.
76. Jiang, B., Gentsch J. R., and Glass R. I. (2002). The role of serum antibodies in the protection against rotavirus disease: an overview. Clin. Infect. Dis. 34: 1351–1361.
77. Joklik WK, Willett HP, Amos DB, and Wifert CM. (1992). Campylobacter, Helicobacter, and Spirillum. In: Zinsser Microbiology 20th ed. p676-679. Appleton and Lange, USA
78. Joklik WK, Willett HP, Amos DB, and Wifert CM. (1992). Salmonella, Shigella, Escherichia coli. In: Zinsser Microbiology 20th ed. p556-563. Appleton and Lange, USA.
79. Joklik WK, Willett HP, Amos DB, and Wifert CM. (1992). Viruses in Gastrointestinal Tract infection. In: Zinsser Microbiology 20th ed. p556-563. Appleton and Lange, USA.
80. Jones F., Wang E., Petric M., Corey P., Moineddin R., and Fearon M., et al. (2000). Hospitalization for community-acquired, rotavirus-associated diarrhea: a prospective, longitudinal, population-based study during the seasonal outbreak. Arch. Pediatr. Adolesc. Med. 154:578–585.
81. June G. A., Sherrod P. S., Imaguana R. M., Andrews W. H. and Hammack T. S. (1993). Effectiveness of the Bacteriological Analytical Manual culture method for the recovery of Shigella sonnei from selected foods. J. AOAC. Int. 76(6): 1240-1248.
82. Kaschl A, EL Nahhal Y, Abu Mourad T, and Romheld V. (1998). Long-term field experiment to examine the agricultural application of municipal solid waste compost in the Gaza Strip. VDLUFA-Schriftenreihe. 49:271—3.
83. Katyal R, Rana SV, and Singh K. (2000). Rotavirus infections. Acta Virol. 44(5):283-8.
84. Khan AM, Sattar S, Jahan SA, Faruque ASG, Hossain MS. (2002). Trend in Isolation of Vibrio cholerae, Shigella, and Salmonella in Neonates with Diarrhoea Admitted to ICDDR,B Hospital, Dhaka, Bangladesh. ICDDR,B: Centre for Health and Population Research. 2003:139
85. Kiehlbauch J. A., Plikaytis B. D., Swaminathan B., Cameron D. N., and Wachsmuth I. (1991). Restriction fragment length polymorphisms in the ribosomal genes for species identification and subtyping of aerotolerant Campylobacter species. J. Clin. Microbiol. 29:1670–1676.
86. Koneman E. (1997). Enterobacteriacae In: Color Atlas and Textbook of Diagnostic Microbiology 5th ed. p171-242. Lippincott-Raven publishers, USA.
87. Korycka M. (2004). Nosocomial rotavirus infections. Przegl Epidemiol. 58(3):467-73.
88. Kosek M, Bern C, and Guerrant RL (2003). The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull World Health Organ. 81(3):197-204.
89. Kotloff K, Winickoff J, Ivanoff B, Clemens JD, Swerdlow DL, Sansonetti PJ, Adak GK, and Levine MM. (1999). Global burden of Shigella infections: implications for vaccine development and implementation of control
82
strategies. Bulletin of the World Health Organization. 77(8): 651 - 666. 90. Kulkarni SP, Lever S, Logan JM, Lawson AJ, Stanley J, and Shafi MS.
(2002). Detection of campylobacter species: a comparison of culture and polymerase chain reaction based methods. J Clin Pathol. 55(10):749-53.
91. Kumar S H, Sunil R, Venugopal MN, Karunasagar I, and Karunasagar I. (2003). Detection of Salmonella spp. in tropical seafood by polymerase chain reaction. Int J Food Microbiol. 15, 88(1), 91-5
92. Kurowski PB, Traub-Dargatz JL, Morley PS, and Gentry-Weeks CR. (2002). Detection of Salmonella spp in fecal specimens by use of real-time polymerase chain reaction assay. Am J Vet Res. 63(9):1265-8.
93. Lampel K., Orlandi P A., and Kornegay L. (2000). Improved template preparation for PCR-based assays for detection of food-borne bacterial pathogens. App Envir Microbiol. 66 (10): 4539-4542
94. Lawson AJ, Logan JM, Oneill GL, Desai M, and Stanley J. (1999). Large-scale survey of Campylobacter species in human gastroenteritis by PCR and PCR-enzyme-linked immunosorbent assay. J Clin Microbiol. 37(12):3860-4.
95. Legros D, Paquet C, Dorlencourt F, and Le Saoult E. (1999). Risk factors for death in hospitalized dysentery patients in Rwanda. Trop Med Int Health 4: 428–432
96. Leibovici L, Yahav J, Mates A, Linn S, and Danon YL. (1986). Etiological and clinical characteristics of diarrhea in young adults, with special reference to Shigella gastroenteritis. Mil Med;151:655-9.
97. Lerman Y, Slepon R, and Cohen D. (1994). Epidemiology of acute diarrheal diseases in children in a high standard of living rural settlement in Israel. Pediatr Infect Dis J. 13(2):116-22.
98. Leushner and Kelly. (2001). Molecular diagnostics research: clinical research. Pathogenic enteric bacteria. Data provided by Leushner J. and Kelly M., MDSMetro Laboratory Services, Burnaby, BC, Canada. QIAGEN: Customer application article, issue no 4, 2000, page 21.
99. Li JW, Shi XQ, Chao FH, Wang XW, Zheng JL, and Song N. (2004). A study on detecting and identifying enteric pathogens with PCR. Biomed Environ Sci. 17(1):109-20.
100. Lindqvist R. (1999) Detection of Shigella spp. in food with a nested PCR method-sensitivity and performance compared with a conventional culture method. J. Appl. Microbiol. 86, 971-978.
101. Linton, P., Lawson A. J., Owen R. J., and Stanley J. (1997). PCR detection and identification to species level and fingerprinting of C. jejuni and C. coli direct from diarrheic samples. J. Clin. Microbiol. 35:2568-2572
102. Louie M, Read S, Simor AE, Holland J, Louie L, Ziebell K, Brunton J, and Hii J. (1998). Application of multiplex PCR for detection of non-O157 verocytotoxin-producing Escherichia coli in bloody stools: identification of serogroups O26 and O111. J. Clin. Microbiol. 36:3375-3377
103. Ludert JE, Gil F, Liprandi F, and Esparza J. (1986). The structure of the rotavirus inner capsid studied by electron microscopy of chemically disrupted particles. J Gen Virol. 67: 1721–1725.
104. Lukinmaa S, Nakari UM, Eklund M, and Siitonen A. (2004). Application of molecular genetic methods in diagnostics and epidemiology of food-borne bacterial pathogens. APMIS. 112(11-12):908-29.
105. Maneekarn N., and Ushijima H. (2000). Epidemiology of rotavirus infection in Thailand. Pediatr. Int. 42:415–421.
106. Manual for the laboratory identification and antimicrobial susceptibility testing of bacterial pathogens of public health concern in the developing world. Haemophilus influenzae, Neisseria meningitidis, Streptococcus pneumoniae, Neisseria gonorrhoeae, Salmonella serotype Typhi, Shigella, and Vibrio cholerae WHO/CDC. WHO/CDS/CSR/RMD/2003.6
107. March SB, and Ratnam S. (1989). Latex agglutination test for detection of Escherichia coli serotype O157. J Clin Microbiol. 27:1675-1677
108. March SB, and Ratnam S. (1986). Sorbitol-MacConkey medium for detection of Escherichia coli O157:H7 associated with hemorrhagic colitis. J
83
Clin Microbiol. 23:869-872 109. Matar GM, Abdo D, Khneisser I, Youssef M, Zouheiry H, Abdelnour G, and
Harakeh HS. (2002). The multiplex-PCR-based detection and genotyping of diarrhoeagenic Escherichia coli in diarrhoeal stools. Ann Trop Med Parasitol. 96(3):317-24.
110. Materu SF, Lema OE, Mukunza HM, Adhiambo CG, and Carter JY. (1997). Antibiotic resistance patterns of Vibrio cholerae and Shigella causing diarrhoea outbreaks in the eastern African region. East Afr Med J 74: 193–197.
111. Matsuki T, Watanabe K, Fujimoto J, Miyamoto Y, Takada T, Matsumoto K, Oyaizu H, and Tanaka R. (2002). Development of 16S rRNA-gene-targeted group-specific primers for the detection and identification of predominant bacteria in human feces. Appl Environ Microbiol. 68(11):5445-51.
112. Meneghetti A C, Bolognini A M, and Lauretti F. (2001). Incidence of Group A Rotavirus in Urban and Rural Areas of the City of Londrina-Brazil, from 1995 to 1997. Braz. arch. Boil. 44 (3): 257-261.
113. Mead, P.S., Slutsker, L., Dietz, V., McCaig, L.F., Bresee, J.S., Shapiro, C., Griffin, P.M. and Tauxe, R.V. (1999). Food-related illness and death in the United States. Emerg Infect. Dis, 5, 607–625.
114. Meqdam M., Youssef M.T. Nimri. LF. Shurman. A.A. Rawashdeh. M.O. and Al-Khdour. M.S. (1997). Viral gastroenteritis among young children in Northern Jordan. J. Trop. Pediatr. 43, 349-352.
115. Ministry of Health. Health Status in Palestine, The Annual Report 2002, Gaza, Palestine, Health Information Center 2003.
116. Ministry of Health. Health Status in Palestine, The Annual Report 2003, Gaza, Palestine, Health Information Center 2004.
117. Ministry of Health. Health Status in Palestine, The Annual Report 2004, Gaza, Palestine, Health Information Center 2005.
118. Modarres S, Modarres S and Oskoii N. (1995). Rotavirus infection in infants and young children with acute gastroenteritis in the Islamic Republic of Iran. East Med Heal. 1(2): 210-214.
119. Monteiro L., Bonnemaison D., Vekris A., Petry K. G., Bonnett J., Vidal R., Cabrita J., and Megraud F. (1997). Complex polysaccharides as PCR inhibitors in feces: Helicobacter pylori model. J. Clin. Microbiol. 35:995–998.
120. Mubashir M, Khan A, Baqai R, Iqbal J, Ghafoor A, and Zuberi S et al. (1990). Causative agents of acute diarrhoea in the first 3 years of life: hospital-based study. J Gastroenterol Hepatol; 5:264-70.
121. Na’was TE, and Abo-Shehada MN. (1991). A study of the bacterial and parasitic causes of acute diarrhea in Northern Jordan. J Diarrhoeal Dis Res. 9:305-9.
122. Naficy AB, Abu-Elyazeed R, Holmes JL, Rao MR, Savarino SJ, Kim Y, Wierzba TF, Peruski L, Lee YJ, Gentsch JR, Glass RI, and Clemens JD. (1999). Epidemiology of rotavirus diarrhea in Egyptian children and implications for disease control. Am J Epidemiol 150: 770–777
123. Naik TN. (2004). Rapid diagnosis of rotavirus infection: key to prevent unnecessary use of antibiotics for treatment of childhood diarrhoea. Indian J Med Res. 119(2): 1-8.
124. Nakano S, Kobayashi T, Funabiki K, Matsumura A, Nagao Y, and Yamada T. (2003). Development of a PCR assay for detection of Enterobacteriaceaea in foods. J food prot. 66 (10): 1798-1804.
125. Naravaneni R, and Jamil K. (2005). Rapid detection of food-borne pathogens by using molecular techniques. J Med Microbiol. 54(1):51-4.
126. National Committee for Clinical Laboratory Standards. Performance standards for antimicrobial susceptibility testing. 9th Informational Supplement. Document M100-S9. NCCLS 1999., Wayne, Pa. USA.
127. Nazer H, al-Jobeh I, Qubain H, and Abdul Latif D. (1993). Diarrhoea: a continuing health problem in Jordanian infants. J Trop Pediatr. 39:95—6.
128. Nelson E, Ko W, Kwan , Leung SF, Poon KH, Chow CB, Sin WK, Wong YK, and Yeung CY. (2003). Guidelines for the management of acute diarrhoea in young children. HK J Paediatr. 8:203-236
84
129. Nguyen TV. (2005). Children’s diarrhea in Hanoi, Vietnam importance of enteric pathogens, Pub. by Karolinska University Press Stockholm, Sweden
130. Nguyen TV, Le Van P, Le Huy C, Gia KN, and Weintraub A. (2005). Detection and characterization of diarrheagenic Escherichia coli from young children in Hanoi, Vietnam. J Clin Microbiol. 43(2):755-60.
131. Nguyen TV, Le Van P, Le Huy C, and Weintraub A. (2004). Diarrhea caused by rotavirus in children less than 5 years of age in Hanoi, Vietnam. J Clin Microbiol. 42(12):5745-50
132. Nimri L, and Hijazi S. (1996). Rotavirus associated diarrhea in children in refugee camp in Jordan. J Diarrhoeal Dis Res. 14:1—4.
133. Nimri LF, Elnasser Z, and Batchoun R. (2004). Polymicrobial infections in children with diarrhoea in a rural area of Jordan. FEMS Immunol Med Microbiol. 42(2):255-9.
134. Nimri LF, and Meqdam M. (2004). Enteropathogens associated with cases of gastroenteritis in a rural population in Jordan. Clin Microbiol Infect. 10(7):634-9.
135. Ono K, Rai SK, Chikahira M, Fujimoto T, Shibata H, Wada Y, Tsuji H, Oda Y, Rai G, Shrestha CD, Masuda K, Shrestha HG, Matsumura T, Hotta H, Kawamura T, and Uga S. (2001). Seasonal distribution of enteropathogens detected from diarrheal stool and water samples collected in Kathmandu, Nepal. Southeast Asian J Trop Med Public Health. 32(3):520-526.
136. Orlandi PP, Silva T, Magalhaes GF, Alves F, de Almeida Cunha RP, Durlacher R, and da Silva LH. (2001). Enteropathogens associated with diarrheal disease in infants of poor urban areas of Porto Velho, Rondonia: a preliminary study. Mem Inst Oswaldo Cruz. 96(5):621-5.
137. Parashar UD, Hummelman EG, Bresee JS, Miller MA, and Glass RI. (2003). Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis. 9(5):565-72.
138. Paton J. and Adrienne W. Paton. (1998). Pathogenesis and diagnosis of shiga toxin-producing Escherichia coli infections. Clin Microbiol Rev. 11(3): 450–479.
139. Pavia AT, Nichols CR, Green DP, Tauxe RV, Mottice S, Greene KD, Wells JG, Siegler RL, Brewer ED, and Hannon D, et al. (1990). Hemolytic-uremic syndrome during an outbreak of Escherichia coli O157:H7 infections in institutions for mentally retarded persons: clinical and epidemiologic observations. J Pediatr. 116(4):544-551.
140. Pazzaglia G, Bourgeois AL, Araby I, Mikhail I, Podgore JK, Mourad A, Riad S, Gaffar T, and Ramadan AM. (1993). Campylobacter-associated diarrhoea in Egyptian infants: epidemiology and clinical manifestations of disease and high frequency of concomitant infections. J Diarrhoeal Dis Res. 11(1):6-13.
141. Public Health Laboratory. Evaluation of seven commercial assays for detecting group A rotavirus. East Virology Advisory Committee (England). http://www.novamed.co.il/technical.html
142. Rahn K., De Grandis S. A., Clarke R. C., McEwen S. A., Galan J. E. Ginocchio R. Curtiss III, and Gyles C. L. (1992). Amplification of an invA gene sequence of Salmonella typhimurium by polymerase chain reaction as a specific method of detection of Salmonella. Mol. Cell. Probes 6:271-279
143. Rajesh P.K., Kalyani M., Anbumani N., and Mallika M. (2005). A Short-term study of diarrhoea among children under five years of age in Chennai, Tamilnadu, with special reference to rotavirus. Indian J Pract Doc. 2 (3) 7-8.
144. Ramotar K, Waldhart B, Church D, Szumski R, and Louie TJ. (1995). Direct detection of verotoxin-producing Escherichia coli in stool samples by PCR. J Clin Microbiol. 33(3):519-24.
145. Riley LW, Remis RS, Helgerson SD, McGee HB, Wells JG, and Davis BR, et al. (1983). Hemorrhagic colitis associated with a rare Escherichia coli serotype. N Engl J 308:681-5.
146. Rohner P, Pittet D, Pepey B, Nije-Kinge T, and Auckenthaler R. (1997). Etiological agents of infectious diarrhea: Implications for requests for
85
microbial culture. J Clin Microbiol. 35 (6): 1427–1432.
147. Rowe B, Ward LR, and Threlfall EJ. (1997). Multidrug-resistant Salmonella typhi: a worldwide epidemic. Clin Infect Dis 24 (1): S106–S109
148. Sack DA, Lyke C, McLaughlin C, and Suwanvanichkij V. (2001). Antimicrobial resistance in shigellosis, cholera, and campylobacteriosis. World Health Organization. Geneva.
149. Sack R B., Rahman M., Yunus M., and Khan E. H. (1997). Antimicrobial resistance in organisms causing diarrheal disease. Clin. Infect. Dis. 24(1):S102-S105
150. Salama, S. M., Garcia M. M., and Taylor D. E. (1992). Differentiation of the subspecies of Campylobacter fetus by genomic sizing. Int. J. Syst. Bacteriol. 42:446–450.
151. Sallon S, el-Shawwa R, Khalil M, Ginsburg G, el Tayib J, el-Eila J, Green V, and Hart CA. (1994). Diarrhoeal disease in children in Gaza. Ann Trop Med Parasitol. 88(2):175-82.
152. Samuel B. (1996). Medical Microbiology. The University of Texas Medical Branch at Galveston–Tx, USA
153. Schnack FJ, Fontana Ld Lde M, Barbosa PR, Silva LS, Baillargeon CM, Barichello T, Povoa MM, Cavasini CE, and Machado RL. (2003). Enteropathogens associated with diarrheal disease in infants (< 5 years old) in a population sample in Greater Metropolitan Criciuma, Santa Catarina State, Brazil. Cad Saude Publica. 19(4):1205-8.
154. Seo J. K., and Sim J. G. (2000). Overview of rotavirus infections in Korea. Pediatr. Int. 42:406–410.
155. Sethi SK, and Khuffash F. (1989). Bacterial and viral causes of acute diarrhoea in children in Kuwait. J Diarrhoeal Dis Res. 7:85-8.
156. Shallow S, Samuel M, Rothrock G, Vugia D, and Fiorentino T et al. (2000). Preliminary FoodNet Data on the Incidence of Foodborne Illnesses- Selected Sites, United States, MMWR 2001 / 50(13);241-246. CDC.
157. Sharif F. and Arafa H. (2004). Occurrence of Escherichia coli O157 in Gaza strip: a preliminary study. Journal of the Islamic university of Gaza (natural sciences series), 12 (1): 51-56.
158. Sharma V. and Carlson S. (2000). Simultaneous detection of salmonella strains and escherichia coli O157:H7 with fluorogenic PCR and single-enrichment-broth culture. App Envir Microbiol, 66 (12): 5472-5476
159. Shubair ME, Yassin MM, al-Hindi A, al-Wahaidi AA, Jadallah SY, and Abu Shaaban N al-D. (2000). Intestinal parasites in relation to haemoglobin level and nutritional status of school children in Gaza. J Egypt Soc Parasitol. 30(2):365-75.
160. Shulman L.M. and Silberstein I. Group A Rotaviruses in Feces: Comparison of Rotavirus One-Step Dipstick Membrane Test with an ELISA. Central Virology Laboratory, Public Health Laboratories Israel Ministry of Health, The Chaim Sheba Medical Center, Tel Hashomer, Israel. http://www.novamed.co.il/technical.html
161. Simhon A, Abed Y, Schoub B, Lasch EE, and Morag A. (1990). Rotavirus infection and rotavirus serum antibody in a cohort of children from Gaza observed from birth to the age of one year. Int J Epidemiol. 19(1):160-163.
162. Skirrow, M. B. (1994). Diseases due to Campylobacter, Helicobacter and related bacteria. J. Comp. Pathol. 111:113-149
163. Snyder JD, and Merson MH. (1982). The magnitude of the global problem of acute diarrhoeal disease: a review of active surveillance data. Bull WHO. 60:604-606.
164. Souza E, Martinez MB., Taddei CR., Mukai Li., Gilio AE., Racz ML., Silva L, Ejzenberg B, and Okay Y. (2002). Etiologic profile of acute diarrhea in children in Sao Paulo. J Pediatr (Rio J). 78(1):31-8.
165. Staat M. A., Azimi P H., Berke T., Roberts N., Bernstein D I., Ward R L., Pickering L K., and Matson D. O. (2002). Clinical presentations of rotavirus infection among hospitalized children. Pediatr. Infect. Dis. J. 21:221–227.
166. Stephen L. W. and Jordan P J. (2003). Evaluation of 11 PCR assays for
86
species-level identification of campylobacter jejuni and campylobacter coli. J Clin Microbiol, 41 (1): 330-336
167. Stone, G. G., Oberst R. D., Hays M. P., McVey S., and Chengappa M. M. (1994). Detection of salmonella serovars from clinical samples by enrichment broth cultivation-PCR procedure. J. Clin. Microbiol. 32:1742–1749.
168. Subekti D, Oyofo BA, Tjaniadi P, Corwin A L, Larasati W, Putri M, Simanjuntak CH, Punjabi NH, Taslim J, Setiawan B, Djelantik AAG, Sriwati L, Sumardiati A, Putra E, Campbell J R, and Lesmana M. (2001). Surveillance of Shigella spp. in Indonesia: the emergence or re-emergence of S. dysenteriae. Emerg Infect Dis 7: 137–140
169. Szalanski AL, Owens CB, McKay T, and Steelman CD. (2004). Detection of Campylobacter and Escherichia coli O157:H7 from filth flies by polymerase chain reaction. Med Vet Entomol. 18(3):241-6.
170. Tjaniadi P, Lesmana M, Subekti D, Machpud N, Komalarini S, Santoso W, Simanjuntak CH, Punjabi N, Campbell JR, Alexander WK, Beecham HJ 3rd, Corwin AL, and Oyofo B. (2003). Antimicrobial resistance of bacterial pathogens associated with diarrheal patients in Indonesia. Am J Trop Med Hyg. 68(6):666-70
171. Townes JM, Quick R, Gonzales OY, Linares M, Damiani E, Bopp CA, Wahlquist SP, Hutwanger LC, Hanover E, Mintz ED, and Tauxe RV. (1997). Etiology of bloody diarrhea in Bolivian children: implications for empiric therapy. J Infect Dis 175: 1527–1530
172. Trkov M, and Avgustin G. (2003). An improved 16S rRNA based PCR method for the specific detection of Salmonella enterica. Int J Food Microbiol. 15;80(1):67
173. Urio EM, Collison EK, Gashe BA, Sebunya TK, and Mpuchane S. (2001). Shigella and Salmonella strains isolated from children under 5 years in Gaborone, Botswana, and their antibiotic susceptibility patterns. Trop Med Int Health. 6(1):55-9.
174. Uyttendaele M., Bagamboula C F., Smet E De., Van Wilder S. and Debevere J. (2000). Evaluation of culture media for enrichment and isolation of shigella sonnei and S. flexneri. Int. J. Food Microbiol. 70:255-265
175. Vandepitte J, Verhaegen J, Engbaek K, Rohner P, Piot P, and Heuck CC. (2003). Basic Laboratory Procedures in Clinical Microbiology 2nd ed. World Health Organization. Geneva
176. VanDerslice J, Popkin B, and Briscoe J. (1994). Drinking-water quality, sanitation, and breast-feeding: their interactive effects on infant health. WHO Bull. 72: 589–601
177. Vanniasinkam T., Lanser J. A. and Barton M. D. (1999). PCR for the detection of Campylobacter spp. in clinical specimens. Letters in Applied Microbiology. 28:52-56
178. Vargas M, Gascon J, Casals C, Schellenberg D, Urassa H, Kahigwa E, Ruiz J, and Vila J. (2004). Etiology of diarrhea in children less than five years of age in Ifakara, Tanzania. Am J Trop Med Hyg. 70(5):536-9.
179. Vidal R, Vidal M, Lagos R, Levine M, and Prado V. (2004). Multiplex PCR for diagnosis of enteric infections associated with diarrheagenic Escherichia coli. J Clin Microbiol. 42(4):1787-9.
180. Voogt N., Raes M., Wannet W.J.B., Henken N.M. and Van de Giessen A.W. (2001). Comparison of selective enrichment media for the detetection of Salmonella in poultry faeces. Lett. Appl. Microbiol. 32:89–92.
181. Wang RF, Cao WW, and Cerniglia CE. (1996). PCR detection and quantitation of predominant anaerobic bacteria in human and animal fecal samples. Appl Environ Microbiol. 62(4):1242-7.
182. Wang R. E, Cao W W., and Cerniglia C. E. (1997). A universal protocol for PCR detection of 13 species of foodborne pathogens in foods. J. Appl. Microbiol 83:727-736.
183. Wasfy MO, Oyofo BA, David JC, Ismail TF, el-Gendy AM, Mohran ZS, Sultan Y, and Peruski LF Jr. (2000). Isolation and antibiotic susceptibility of
87
Salmonella, Shigella, and Campylobacter from acute enteric infections in Egypt. J Health Popul Nutr. 18(1):33-8.
184. WHO (1994).The management of bloody diarrhoea in young children. WHO, Geneva, Swizterland, (WHO/CDD/94.49).
185. WHO (2001). The Increasing Incidence of Human Campylobacteriosis. Report and Proceedings of a WHO Consultation of Experts, Copenhagen, Denmark, 21-25 November 2000. World Health Organization, Department of Communicable Disease Surveillance and Response. http://www.who.int/emc-documents/zoonoses/whocdscsraph20017c.html
186. WHO Guidelines for the control of Shigellosis, including epidemics due to Shigella dysenteriae type 1; http://www.who.int/child-adolescenthealth/new_publications/child_health/isbn_94_4_159233_0.pdf
187. WHO (2005). Guidelines on Standard Operating Procedures for Microbiology. http://w3.whosea.org/microbio/
188. Wierzba TF, Abdel-Messih IA, Abu-Elyazeed R, Putnam SD, Kamal KA, Rozmajzl P, Ahmed SF, Fatah A, Zabedy K, Shaheen HI, Sanders J, and Frenck R. (2006). Clinic-based surveillance for bacterial- and rotavirus-associated diarrhea in egyptian children. Am J Trop Med Hyg. 74(1):148-53.
189. Wong CS, Jelacic S, Habeeb RL, Watkins SL, and Tarr PI. (2000). The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 342:1930–1936
190. Yavzori M., Cohen D., Wasserlauf R., Ambar R., Rechavi G. and Ashkenazi S. (1994). Identifcation of Shigella species by DNA amplication of different loci of the Shigella virulence plasmid. Eur. J. Clin. Microbiol. Infect. Dis. 13(3): 232-237.
191. Yoshida I, Hayashi Y, Katayama K, and Yamada S. (1998). Bacteriological and virological studies on the cause of sporadic acute gastroenteritis in Tama, Tokyo (1991-1996). Kansenshogaku Zasshi. 72(6):599-608.
192. Youssef M, Shurman A, Bougnoux M, Rawashdeh M, Bretagne S, and Strockbine N. (2000). Bacterial, viral and parasitic enteric pathogens associated with acute diarrhea in hospitalized children from northern Jordan. FEMS Immunol Med Microbiol. 28(3):257-63
193. Zaman R. (1992). Campylobacter enteritis in Saudi Arabia. Epidemiol Infect. 108:51-58.
194. Ziemer CJ, and Steadham SR.. (2003). Evaluation of the specificity of Salmonella PCR primers using various intestinal bacterial species. Lett Appl Microbiol. 37(6):463-9.
195. Zvizdic S, Telalbasic S, Beslagic E, Cavaljuga S, Maglajlic J, Zvizdic A, and Hamzic S. (2004). Clinical characteristics of rotaviruses disease. Bosn J Basic Med Sci. 4(2):22-4.
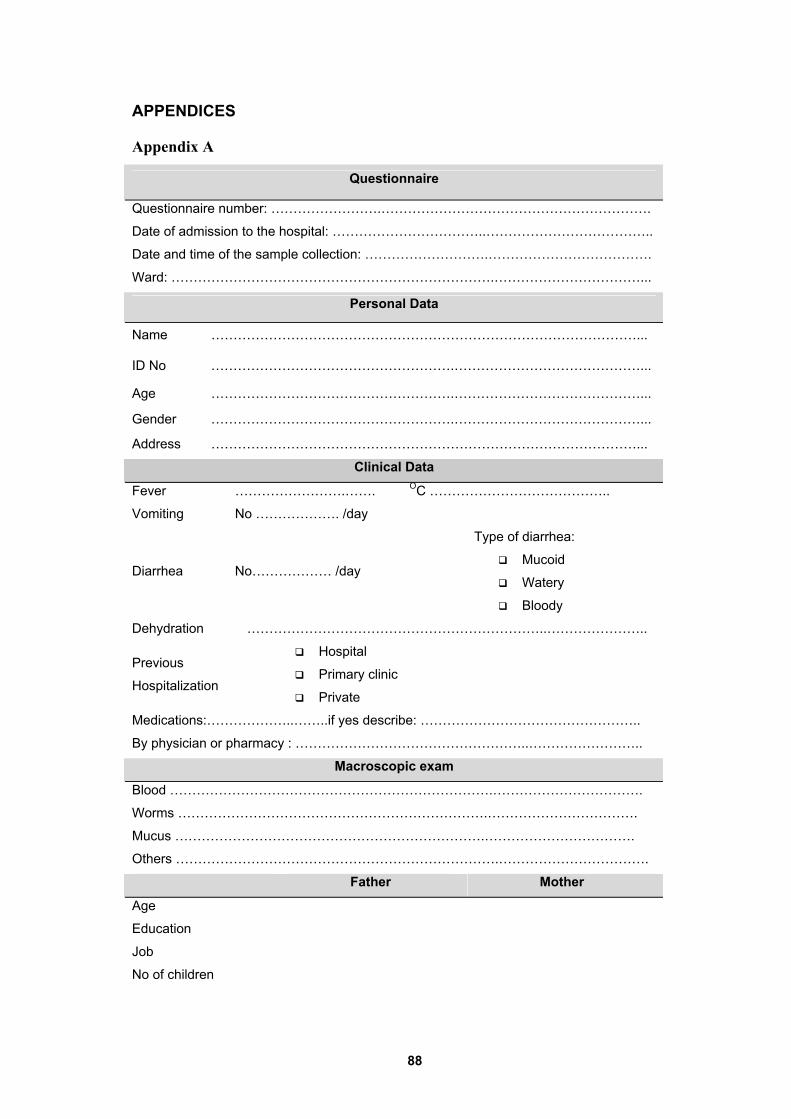
88
APPENDICES
Appendix A
Questionnaire
Questionnaire number: …………………….…………………………………………………….
Date of admission to the hospital: ……………………………..………………………………..
Date and time of the sample collection: ……………………….……………………………….
Ward: ……………………………………………………………….……………………………...
Personal Data
Name ……………………………………………………………………………………...
ID No ……………………………………………….……………………………………...
Age ……………………………………………….……………………………………...
Gender ……………………………………………….……………………………………...
Address ……………………………………………………………………………………...
Clinical Data
Fever …………………….……. OC …………………………………..
Vomiting No ………………. /day
Diarrhea No……………… /day
Type of diarrhea:
Mucoid
Watery
Bloody
Dehydration …………………………………………………………..…………………..
Previous
Hospitalization
Hospital
Primary clinic
Private Medications:………………..……..if yes describe: …………………………………………..
By physician or pharmacy : ……………………………………………..…………………….. Macroscopic exam
Blood ……………………………………………………………….…………………………….
Worms …………………………………………………………….…………………………….
Mucus …………………………………………………………….…………………………….
Others ……………………………………………………………….…………………………….
Father Mother
Age
Education
Job
No of children
89
Appendix B
Security

90
Appendix C
Helsinki
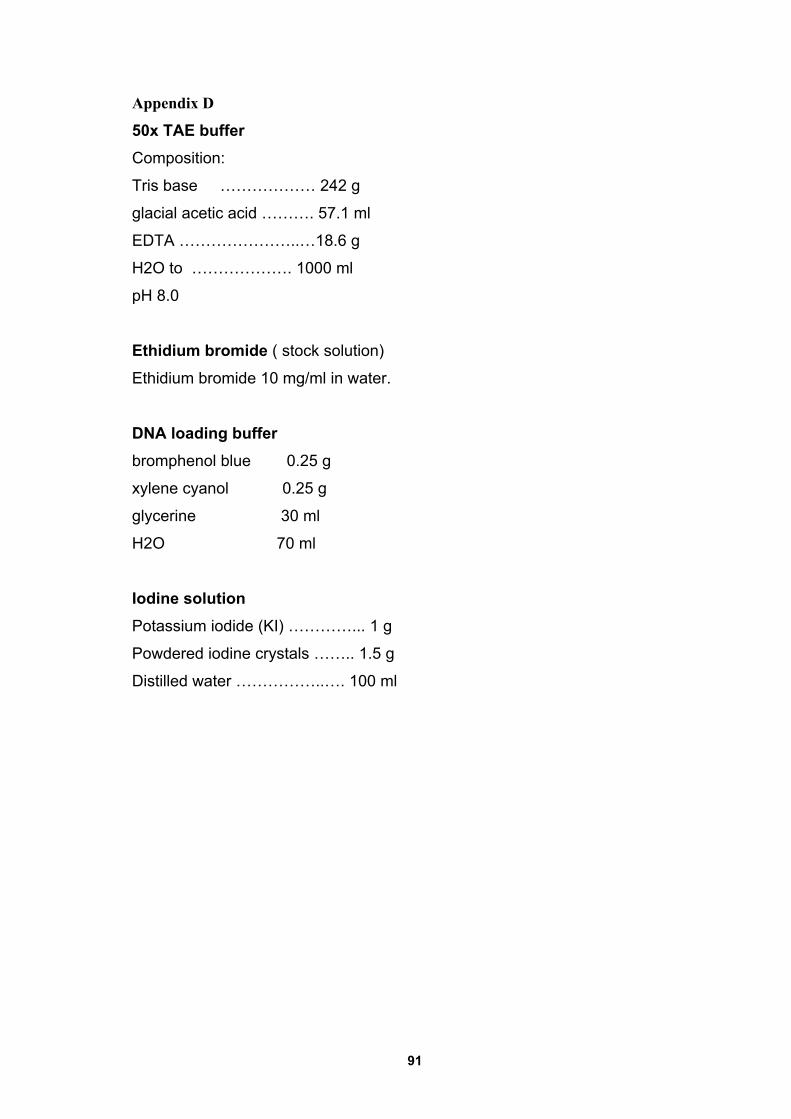
91
Appendix D
50x TAE buffer Composition:
Tris base ……………… 242 g
glacial acetic acid ………. 57.1 ml
EDTA …………………..…18.6 g
H2O to ………………. 1000 ml
pH 8.0
Ethidium bromide ( stock solution)
Ethidium bromide 10 mg/ml in water.
DNA loading buffer bromphenol blue 0.25 g
xylene cyanol 0.25 g
glycerine 30 ml
H2O 70 ml
Iodine solution Potassium iodide (KI) …………... 1 g
Powdered iodine crystals …….. 1.5 g
Distilled water ……………..…. 100 ml
92
Appendix E Shigella polyvalent (BIO-RAD, France):
1) Sub-group A : 2 polyvalent sera
• Serum A1 : anti-Shigella dysenteriae: 1,3,4,5,6
• Serum A2 : anti-Shigella-dysenteriae: 2, 7, 8
2) Sub - group B: 1 polyvalent serum
• Anti-Shigella fIexneri serum, it agglutinates the 6 serotypes of this
subgroup.
3) Sub-group C : 3 polyvalent sera
• Serum C1 : anti-Shigella – boydii: 1, 2, 3, 4
• Serum C2 : anti-Shigella - boydii: 8, 10, 14
• Serum C3: anti-Shigella- boydii: 5, 7, 9,11,15
4) Sub-group D: 1 mixed anti-Shigella sonnei serum
• It agglutinates, the 2 phases of this species.