
Appendix A: Suturing Techniques: All-Inside Repair Techniques978-3-642-30544-3/1.pdfradius fracture,...
26
349 F. del Piñal et al. (eds.), Arthroscopic Management of Ulnar Pain, DOI 10.1007/978-3-642-30544-3, © Springer-Verlag Berlin Heidelberg 2012 Appendix A: Suturing Techniques: All-Inside Repair Techniques Introduction Wrist arthroscopy has developed rapidly in the last decade. From a purely diagnostic tool, it has become more and more a treatment tool. Distal radius fracture, osteotomies, or arthrodesis are now commonly performed under arthroscopy by the most active teams. The need to place sutures inside the joint is an everyday scenario in any busy arthros- copy practice. Suturing dorsal tears is undoubtedly one of the most common among them (Chap. 8). Dorsal capsular tears have been treated by suturing the TFC proper to the dorsal capsule, placing the knot outside the joint over an external bolster or a button [3]. If the suture had been placed blindly, there was a risk of entrapping the dorsal branch of the ulnar nerve [7, 10], this occurring in up to 50 % of the cases in a cadav- eric study [8]. Additionally, the button or bolster could cause skin irritation, skin necrosis, and even septic arthritis [11]. A mini-open approach minimized this risk, the nerve could be protected, and the suture placed on top of the capsule or the floor of the ECU sheath (see Chap. 8 and Appendix B). The knot, which needed several throws, created a new set of complications, namely, irritation of the ECU tendon or the nerve itself. A second operation may be needed to remove the knot, even if resorbable material was used [2, 9]. To circumvent these problems, sev- eral devices have been presented in the literature. In this appendix, I would like to describe in detail two methods for an all-in suturing in the wrist joint that leaves the knot inside and that requires no special equipment. All-Inside Variant 1 Mattress Suture with a Tuohy Needle (Fig. A.1) The technique has been applied for capsular suturing, TFC frontal tears, reattachments to the fovea of the TFC in combination with anchors [5], and repair of volar structures such as the volar scapho-lunate ligament [6]. Step 1: A Tuohy needle loaded with a thread is inserted proximal to the tear perforating both the capsule and the TFC proper. Step 2: The thread is pushed into the joint and the end (henceforth named end A) grabbed with grasper introduced from 6R. End A is now retrieved out of the joint and secured with a mos- quito to avoid slippage. At this moment, end A is outside the joint, the needle is loaded with the thread, and the other end of the suture (henceforth named B) is also outside of the joint. Appendices F. del Piñal, M.D., Dr. Med. Hand-Wrist and Plastic Surgery, Private Practice and Mutua Montañesa, Paseo de Pereda 20-1º, E-39004 Santander, Spain email: [email protected], [email protected]
Transcript of Appendix A: Suturing Techniques: All-Inside Repair Techniques978-3-642-30544-3/1.pdfradius fracture,...

349F. del Piñal et al. (eds.), Arthroscopic Management of Ulnar Pain, DOI 10.1007/978-3-642-30544-3, © Springer-Verlag Berlin Heidelberg 2012
Appendix A: Suturing Techniques: All-Inside Repair Techniques
Introduction
Wrist arthroscopy has developed rapidly in the last decade. From a purely diagnostic tool, it has become more and more a treatment tool. Distal radius fracture, osteotomies, or arthrodesis are now commonly performed under arthroscopy by the most active teams. The need to place sutures inside the joint is an everyday scenario in any busy arthros-copy practice. Suturing dorsal tears is undoubtedly one of the most common among them (Chap. 8 ).
Dorsal capsular tears have been treated by suturing the TFC proper to the dorsal capsule, placing the knot outside the joint over an external bolster or a button [3]. If the suture had been placed blindly, there was a risk of entrapping the dorsal branch of the ulnar nerve [7, 10], this occurring in up to 50 % of the cases in a cadav-eric study [8]. Additionally, the button or bolster could cause skin irritation, skin necrosis, and even septic arthritis [11]. A mini-open approach minimized this risk, the nerve could be protected, and the suture placed on top of the capsule or the
fl oor of the ECU sheath (see Chap. 8 and Appendix B ). The knot, which needed several throws, created a new set of complications, namely, irritation of the ECU tendon or the nerve itself. A second operation may be needed to remove the knot, even if resorbable material was used [2, 9]. To circumvent these problems, sev-eral devices have been presented in the literature. In this appendix, I would like to describe in detail two methods for an all-in suturing in the wrist joint that leaves the knot inside and that requires no special equipment.
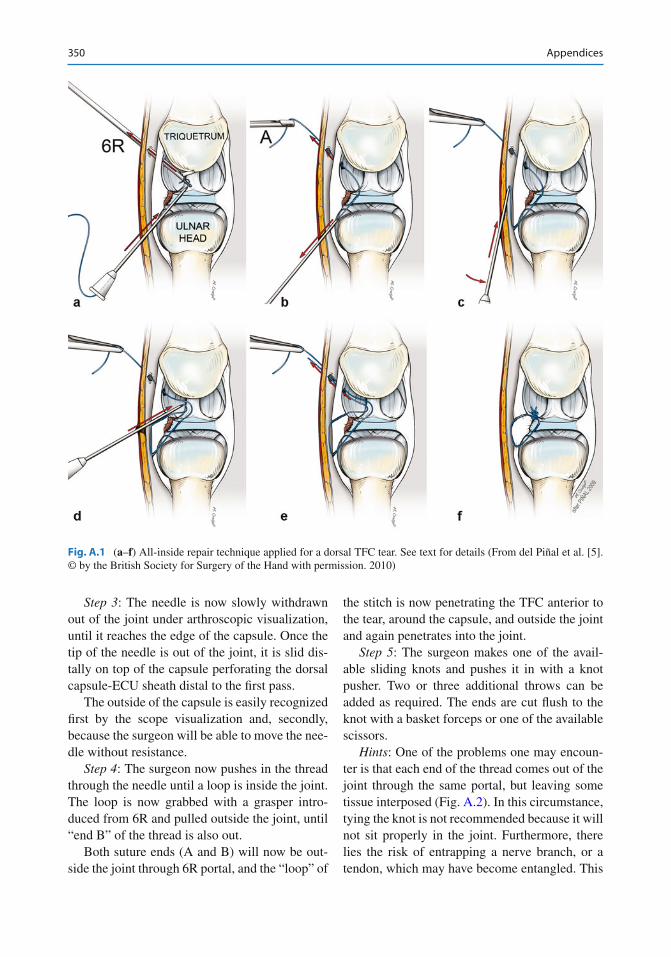
All-Inside Variant 1 Mattress Suture with a Tuohy Needle (Fig. A.1 )
The technique has been applied for capsular suturing, TFC frontal tears, reattachments to the fovea of the TFC in combination with anchors [5], and repair of volar structures such as the volar scapho-lunate ligament [6].
Step 1 : A Tuohy needle loaded with a thread is inserted proximal to the tear perforating both the capsule and the TFC proper.
Step 2 : The thread is pushed into the joint and the end (henceforth named end A) grabbed with grasper introduced from 6R. End A is now retrieved out of the joint and secured with a mos-quito to avoid slippage.
At this moment, end A is outside the joint, the needle is loaded with the thread, and the other end of the suture (henceforth named B) is also outside of the joint.
Appendices
F. del Piñal , M.D., Dr. Med. Hand-Wrist and Plastic Surgery , Private Practice and Mutua Montañesa , Paseo de Pereda 20-1º, E-39004 Santander , Spainemail: [email protected], [email protected]
350 Appendices
Step 3 : The needle is now slowly withdrawn out of the joint under arthroscopic visualization, until it reaches the edge of the capsule. Once the tip of the needle is out of the joint, it is slid dis-tally on top of the capsule perforating the dorsal capsule-ECU sheath distal to the fi rst pass.
The outside of the capsule is easily recognized fi rst by the scope visualization and, secondly, because the surgeon will be able to move the nee-dle without resistance.
Step 4 : The surgeon now pushes in the thread through the needle until a loop is inside the joint. The loop is now grabbed with a grasper intro-duced from 6R and pulled outside the joint, until “end B” of the thread is also out.
Both suture ends (A and B) will now be out-side the joint through 6R portal, and the “loop” of
the stitch is now penetrating the TFC anterior to the tear, around the capsule, and outside the joint and again penetrates into the joint.
Step 5 : The surgeon makes one of the avail-able sliding knots and pushes it in with a knot pusher. Two or three additional throws can be added as required. The ends are cut fl ush to the knot with a basket forceps or one of the available scissors.
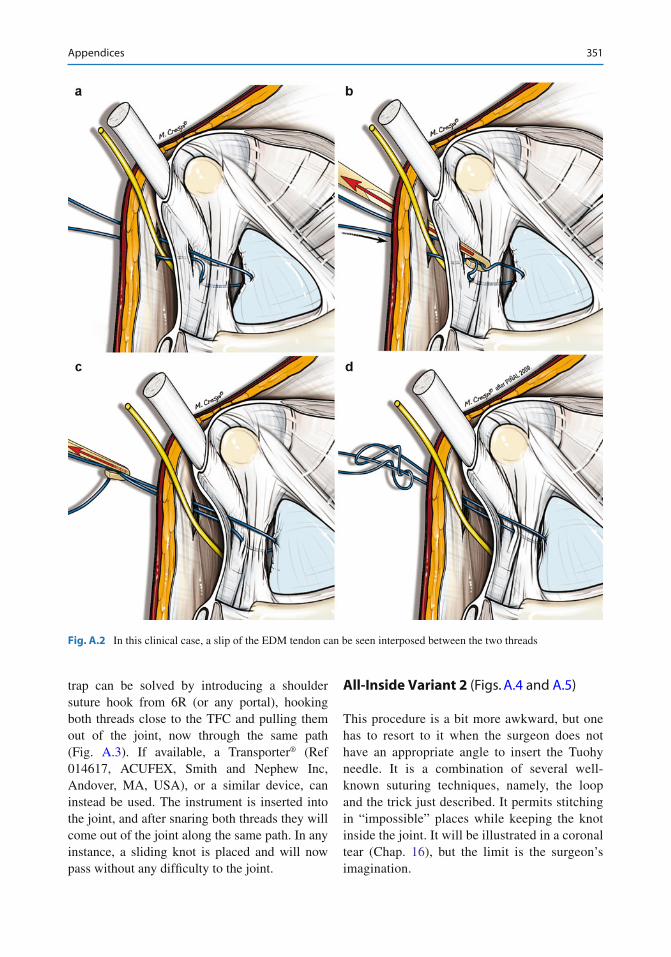
Hints : One of the problems one may encoun-ter is that each end of the thread comes out of the joint through the same portal, but leaving some tissue interposed (Fig. A.2 ). In this circumstance, tying the knot is not recommended because it will not sit properly in the joint. Furthermore, there lies the risk of entrapping a nerve branch, or a tendon, which may have become entangled. This
Fig. A.1 ( a – f ) All-inside repair technique applied for a dorsal TFC tear. See text for details (From del Piñal et al. [5]. © by the British Society for Surgery of the Hand with permission. 2010)
351Appendices
trap can be solved by introducing a shoulder suture hook from 6R (or any portal), hooking both threads close to the TFC and pulling them out of the joint, now through the same path (Fig. A.3 ). If available, a Transporter® (Ref 014617, ACUFEX, Smith and Nephew Inc, Andover, MA, USA), or a similar device, can instead be used. The instrument is inserted into the joint, and after snaring both threads they will come out of the joint along the same path. In any instance, a sliding knot is placed and will now pass without any dif fi culty to the joint.
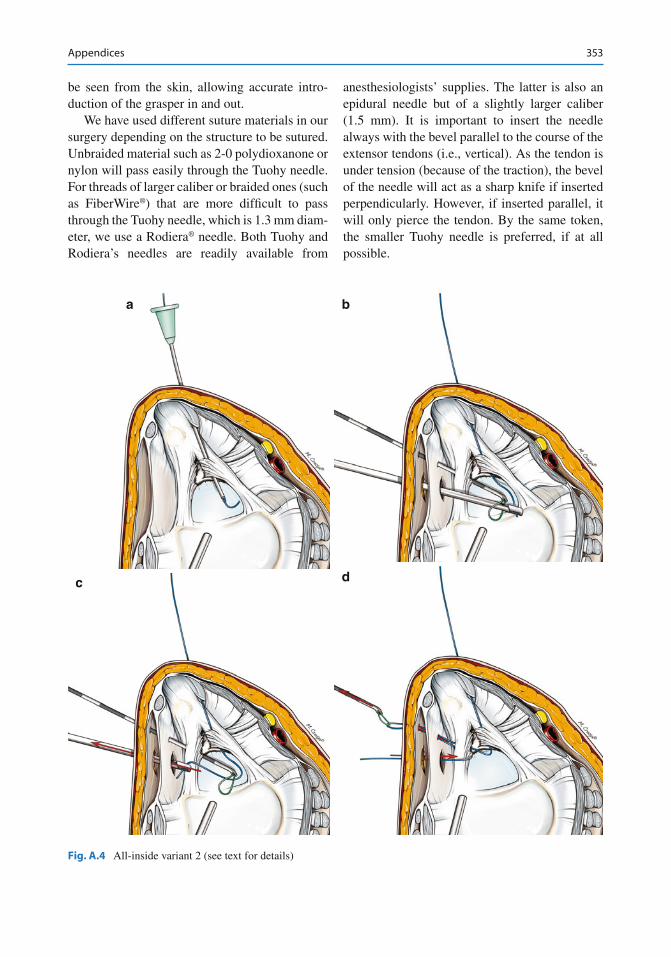
All-Inside Variant 2 (Figs. A.4 and A.5 )
This procedure is a bit more awkward, but one has to resort to it when the surgeon does not have an appropriate angle to insert the Tuohy needle. It is a combination of several well-known suturing techniques, namely, the loop and the trick just described. It permits stitching in “impossible” places while keeping the knot inside the joint. It will be illustrated in a coronal tear (Chap. 16 ), but the limit is the surgeon’s imagination.
Fig. A.2 In this clinical case , a slip of the EDM tendon can be seen interposed between the two threads
352 Appendices
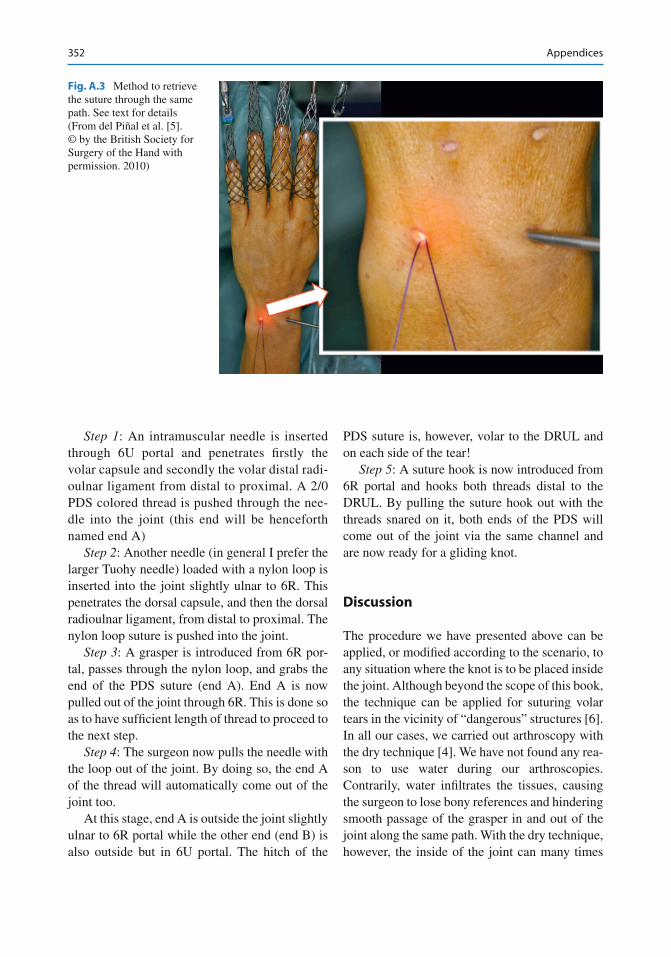
Step 1 : An intramuscular needle is inserted through 6U portal and penetrates fi rstly the volar capsule and secondly the volar distal radi-oulnar ligament from distal to proximal. A 2/0 PDS colored thread is pushed through the nee-dle into the joint (this end will be henceforth named end A)
Step 2 : Another needle (in general I prefer the larger Tuohy needle) loaded with a nylon loop is inserted into the joint slightly ulnar to 6R. This penetrates the dorsal capsule, and then the dorsal radioulnar ligament, from distal to proximal. The nylon loop suture is pushed into the joint.
Step 3 : A grasper is introduced from 6R por-tal, passes through the nylon loop, and grabs the end of the PDS suture (end A). End A is now pulled out of the joint through 6R. This is done so as to have suf fi cient length of thread to proceed to the next step.
Step 4 : The surgeon now pulls the needle with the loop out of the joint. By doing so, the end A of the thread will automatically come out of the joint too.
At this stage, end A is outside the joint slightly ulnar to 6R portal while the other end (end B) is also outside but in 6U portal. The hitch of the
PDS suture is, however, volar to the DRUL and on each side of the tear!
Step 5 : A suture hook is now introduced from 6R portal and hooks both threads distal to the DRUL. By pulling the suture hook out with the threads snared on it, both ends of the PDS will come out of the joint via the same channel and are now ready for a gliding knot.
Discussion
The procedure we have presented above can be applied, or modi fi ed according to the scenario, to any situation where the knot is to be placed inside the joint. Although beyond the scope of this book, the technique can be applied for suturing volar tears in the vicinity of “dangerous” structures [6]. In all our cases, we carried out arthroscopy with the dry technique [4]. We have not found any rea-son to use water during our arthroscopies. Contrarily, water in fi ltrates the tissues, causing the surgeon to lose bony references and hindering smooth passage of the grasper in and out of the joint along the same path. With the dry technique, however, the inside of the joint can many times
Fig. A.3 Method to retrieve the suture through the same path. See text for details (From del Piñal et al. [5]. © by the British Society for Surgery of the Hand with permission. 2010)
353Appendices
be seen from the skin, allowing accurate intro-duction of the grasper in and out.
We have used different suture materials in our surgery depending on the structure to be sutured. Unbraided material such as 2-0 polydioxanone or nylon will pass easily through the Tuohy needle. For threads of larger caliber or braided ones (such as FiberWire®) that are more dif fi cult to pass through the Tuohy needle, which is 1.3 mm diam-eter, we use a Rodiera® needle. Both Tuohy and Rodiera’s needles are readily available from
anesthesiologists’ supplies. The latter is also an epidural needle but of a slightly larger caliber (1.5 mm). It is important to insert the needle always with the bevel parallel to the course of the extensor tendons (i.e., vertical). As the tendon is under tension (because of the traction), the bevel of the needle will act as a sharp knife if inserted perpendicularly. However, if inserted parallel, it will only pierce the tendon. By the same token, the smaller Tuohy needle is preferred, if at all possible.
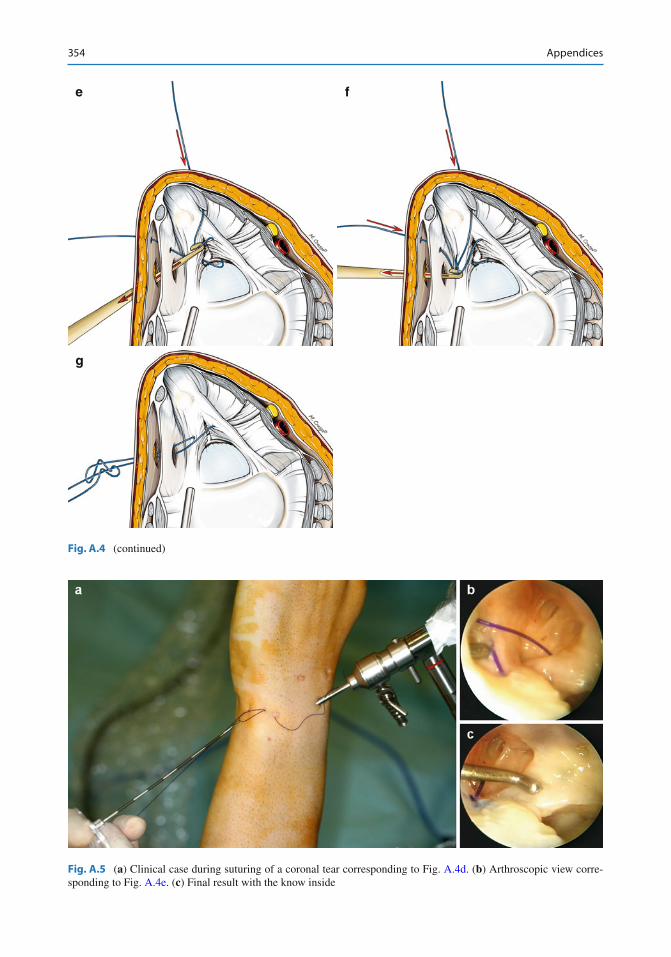
Fig. A.4 All-inside variant 2 (see text for details)
a
c d
b
354 Appendices
e
g
f
Fig. A.4 (continued)
Fig. A.5 ( a ) Clinical case during suturing of a coronal tear corresponding to Fig. A.4d . ( b ) Arthroscopic view corre-sponding to Fig. A.4e . ( c ) Final result with the know inside
355Appendices
Intravenous needles or intramuscular needles are not recommended for the all-inside technique we propose here. First of all, the inner core of the point is sharp, and in step 4 (of procedure 1), the thread can be cut, as there is some pulling required before end B is outside the joint. More impor-tantly, however, is that they are too sharp, and besides cutting too much, they provide no “feel” when the surgeon has to creep with the tip of the needle on the dorsal capsule in step 3 (of proce-dure 1). The epidural needle is comparatively much blunter, and the surgeon will notice when the capsule has been passed and “feels” the tip of the needle when sliding on top of the hard surface of the capsule. It is critical that the surgeon stays immediately on top of the outer surface of the capsule when moving the needle distally. If the needle has been withdrawn too much, there will be a risk of entangling a tendon or a nerve branch when reintroducing the needle into the joint. If
this were to accidentally happen, the suture should be removed and the process repeated.
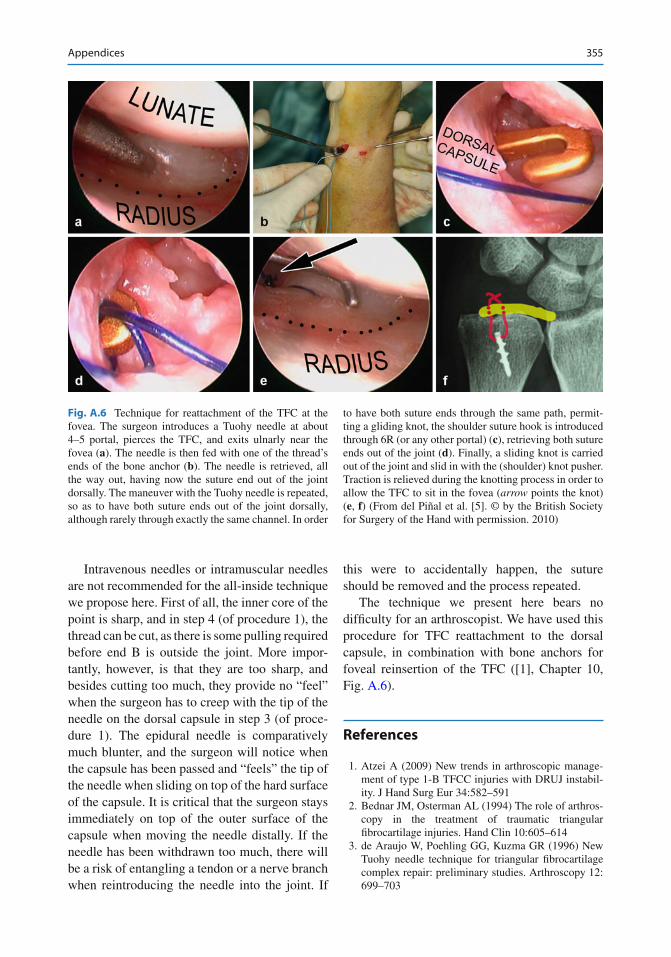
The technique we present here bears no dif fi culty for an arthroscopist. We have used this procedure for TFC reattachment to the dorsal capsule, in combination with bone anchors for foveal reinsertion of the TFC ([1], Chapter 10, Fig. A.6 ).
References
1. Atzei A (2009) New trends in arthroscopic manage-ment of type 1-B TFCC injuries with DRUJ instabil-ity. J Hand Surg Eur 34:582–591
2. Bednar JM, Osterman AL (1994) The role of arthros-copy in the treatment of traumatic triangular fi brocartilage injuries. Hand Clin 10:605–614
3. de Araujo W, Poehling GG, Kuzma GR (1996) New Tuohy needle technique for triangular fi brocartilage complex repair: preliminary studies. Arthroscopy 12:699–703
Fig. A.6 Technique for reattachment of the TFC at the fovea. The surgeon introduces a Tuohy needle at about 4–5 portal, pierces the TFC, and exits ulnarly near the fovea ( a ). The needle is then fed with one of the thread’s ends of the bone anchor ( b ). The needle is retrieved, all the way out, having now the suture end out of the joint dorsally. The maneuver with the Tuohy needle is repeated, so as to have both suture ends out of the joint dorsally, although rarely through exactly the same channel. In order
to have both suture ends through the same path, permit-ting a gliding knot, the shoulder suture hook is introduced through 6R (or any other portal) ( c ), retrieving both suture ends out of the joint ( d ). Finally, a sliding knot is carried out of the joint and slid in with the (shoulder) knot pusher. Traction is relieved during the knotting process in order to allow the TFC to sit in the fovea ( arrow points the knot) ( e , f ) (From del Piñal et al. [5]. © by the British Society for Surgery of the Hand with permission. 2010)

356 Appendices
4. del Piñal F, García-Bernal FJ, Pisani D, Regalado J, Ayala H, Studer A (2007) Dry arthroscopy of the wrist: surgical technique. J Hand Surg Am 32:119–123
5. del Piñal F, García-Bernal FJ, Cagigal L, Studer A, Regalado J, Thams C (2010) A technique for arthroscopic all-inside suturing in the wrist. J Hand Surg Eur 35:475–479
6. del Piñal F, Studer A, Thams C, Glasberg A (2011) An all-inside technique for arthroscopic suturing of the volar scapholunate ligament. J Hand Surg Am 36:2044–2046
7. Estrella EP, Hung LK, Ho PC, Tse WL (2007) Arthroscopic repair of triangular fi brocartilage com-plex tears. Arthroscopy 23:729–737
8. McAdams TR, Hentz VR (2002) Injury to the dorsal sensory branch of the ulnar nerve in the arthroscopic
repair of ulnar-sided triangular fi brocartilage tears using an inside-out technique: a cadaver study. J Hand Surg 27A:840–844
9. Pederzini LA, Tosi M, Prandini M, Botticella C (2007) All-inside suture technique for Palmer class 1B trian-gular fi brocartilage repair. Arthroscopy 23:1130.e1–1130.e4
10. Tsu-Hsin Chen E, Wei JD, Huang VW (2006) Injury of the dorsal sensory branch of the ulnar nerve as a complication of arthroscopic repair of the triangular fi brocartilage. J Hand Surg 31-B:530–532
11. Yao J, Dantuluri P, Osterman AL (2007) A novel tech-nique of all-inside arthroscopic triangular fi brocartilage complex repair. Arthroscopy 23:1357.e1–1357.e4

357Appendices
Appendix B: Suturing Techniques: Double Loop Technique for Large Dorsal TFCC Rupture
Introduction
According to the classi fi cation of Palmer and Werner [5], type I traumatic TFCC lesions are further classi fi ed into four types where 1B is a peripheral lesion at the ulnar insertion of the TFCC. These are the most frequent and well-known lesions.
On occasions, we have come across certain lesions which are not in standard classi fi cations. The TFCC tear is much broader than in the clas-sical type 1B lesions. The lesion begins in the prestyloid recess and ends almost at the radial insertion of the ligament. This leads to minor degrees of DRUJ instability, and the classic sin-gle stitch may be insuf fi cient. Hence, we modi fi ed the classic suture to a double loop suture.
Arthroscopic Analysis
Classic TFCC arthroscopy is performed through a 3–4 radiocarpal portal and a probe through the 6R portal. The tension of the TFCC is evaluated using the so-called trampoline test – positive when the TFCC is lax, indicating a peripheral lesion.
The “hook test” involves traction on the ulnar part of the TFCC at the styloid recess with a probe. The test is positive if the TFCC can be brought toward the radial border of the radioulnar joint. This test detects foveal detachment, partic-ularly if the distal component is intact. In this case, arthroscopic exploration of the radioulnar joint becomes necessary. Lesions of the distal and proximal components of the TFCC can be isolated or in association, and only DRUJ arthros-copy can show an isolated lesion of the proximal component (foveal attachment) of the TFCC.
When faced with a complete dorsal detach-ment without foveal detachment, traditional sim-ple suture of the distal component can no longer suf fi ce. We describe an original suture technique with a double loop, allowing easy repair of these extensive lesions.
Technique
This technique is usually performed as day sur-gery under axillary block anesthesia with an arm tourniquet. The arm is placed on a table, and trac-tion is applied to the hand and forearm in the axis of the forearm. The joint is distended by saline injection, and a wrist arthroscope (2.4 mm) is introduced through the usual 3–4 radiocarpal portal. A probe is introduced through the 6R radiocarpal portal, and the trampoline and “hook” tests are performed.
The DRUJ may be explored through a radioul-nar portal (RUP). This is a tight joint and arthros-copy is often dif fi cult, especially if the proximal portion of the TFCC is intact. When detached, it is easy to explore the foveal insertion of the TFCC.
In case of an extensive peripheral lesion, rein-sertion is carried out using the double loop tech-nique (Fig. B.1a, b ).
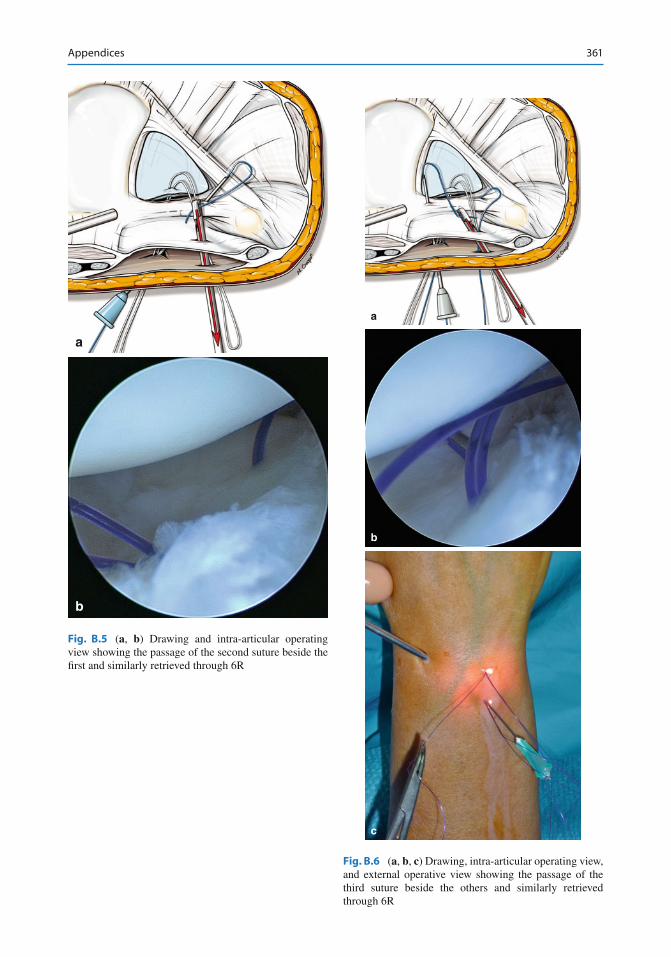
The scar tissue at the zone of the tear is fi rst debrided and freshened using a synovial resector, and synovectomy is performed (Fig. B.2a, b ). An intramuscular needle is inserted into the RUP via the capsule directed obliquely distally and laterally. Its exit is veri fi ed via the TFCC detachment zone exactly at the center. A loop of absorbable suture is passed through the needle from outside (Fig. B.3a , b), retrieved with a forceps and pulled out through the 6R radiocarpal portal (Fig. B.4a, b ). We usually use a PDS 3.0 or 4.0 absorbable suture according to the size of the wrist. A second intramuscular needle is placed radially adjacent to the radial insertion of the TFCC through the same portal in the same direction through the capsule and the TFCC (Fig. B.5a, b ). A second suture is passed through this needle and pulled out through 6R.
A third intramuscular needle is placed ulnarly adjacent to the styloid recess of the TFCC through the same approach in the same direction through
Christophe Mathoulin Institut de la main, Clinique Jouvenet , 6 square Jouvenet 75016 Paris , Franceemail: [email protected]
358 Appendices
the capsule and the TFCC (Fig. B.6a, b, c ), and a third absorbable suture through the needle is like-wise pulled out through 6R.
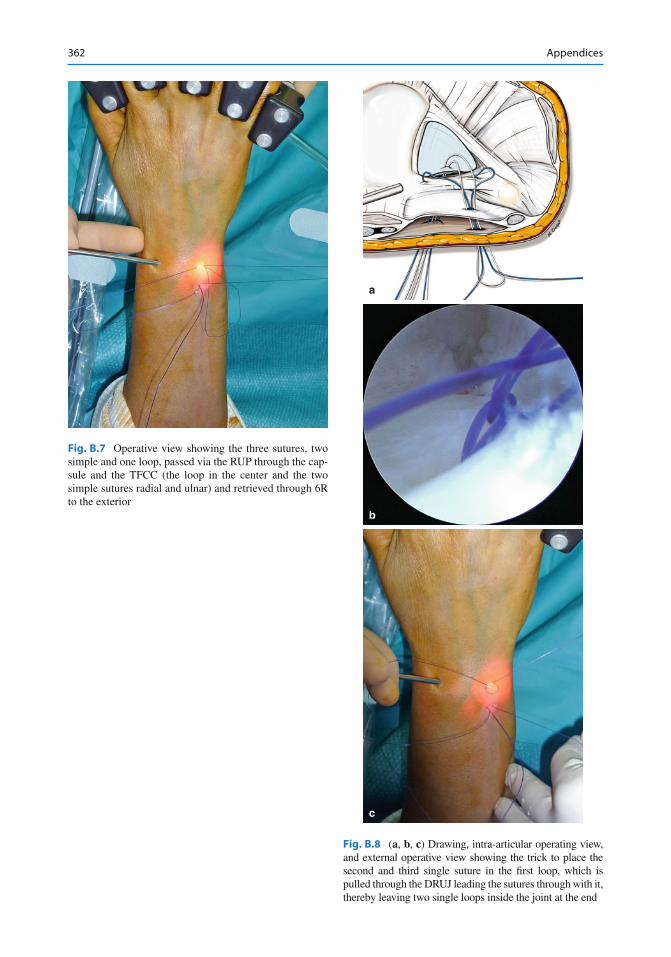
Thus, at this stage, we have three sutures, two simple and one loop, passed via the DRU portal through the capsule and the TFCC (the loop in the center and the two simple sutures radial and ulnar) and retrieved through 6R to the exterior (Fig. B.7 ).
The two simple sutures are passed through the loop outside the joint. The loop is pulled out through the DRUJ portal pulling the two simple sutures through behind it at the center of the TFCC lesion where their ends can be retrieved at the DRUJ portal (Figs. B.8a, b, c and B.9 ).
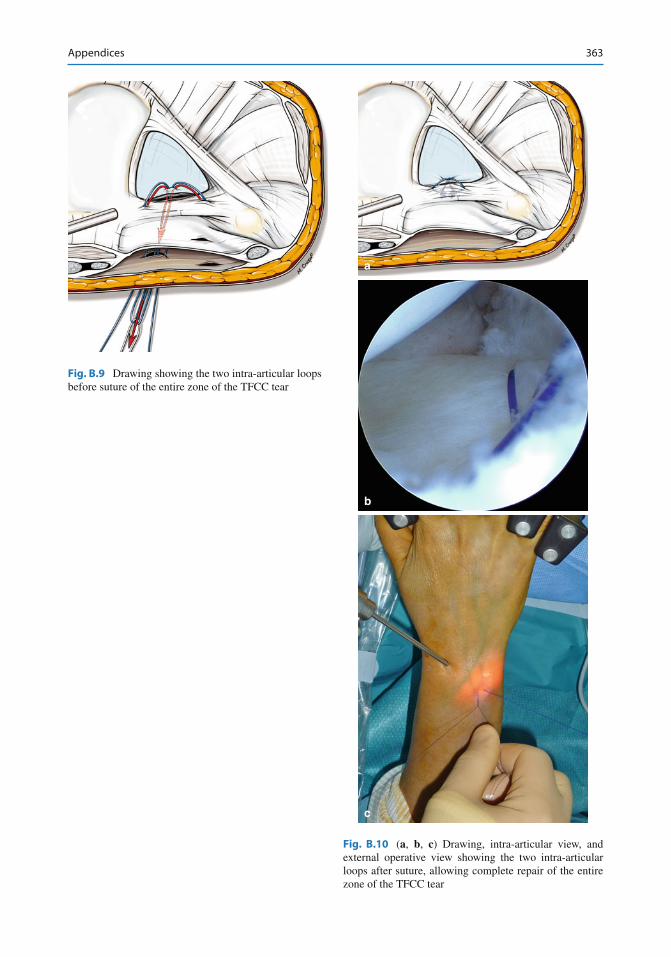
AT this stage, we have two intra-articular loops, allowing a complete suture of the entire zone of the TFCC tear (Fig. B.10a, b, c ).
The wrist traction is relieved, the wrist is posi-tioned in slight extension and ulnar inclination, and the sutures at the DRU level are then tied. An anterior palmar splint is used to maintain this position for 6 weeks. Physiotherapy is started at 6 weeks in all cases.
a
b
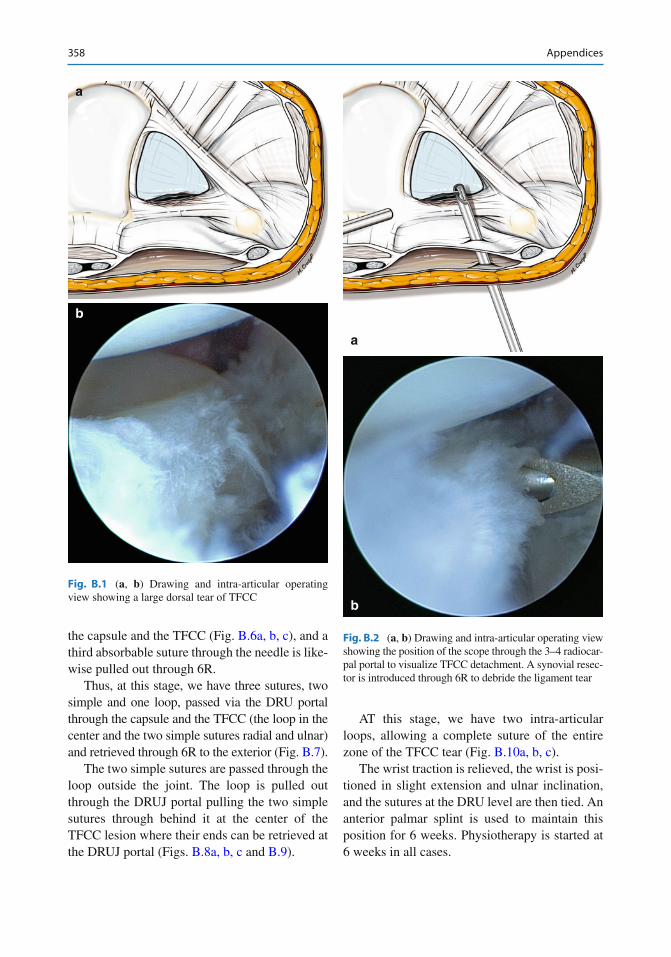
Fig. B.1 ( a , b ) Drawing and intra-articular operating view showing a large dorsal tear of TFCC
a
b
Fig. B.2 ( a , b ) Drawing and intra-articular operating view showing the position of the scope through the 3–4 radiocar-pal portal to visualize TFCC detachment. A synovial resec-tor is introduced through 6R to debride the ligament tear
359Appendices
Discussion
The TFCC is more complex than it appears. Wrist arthroscopy allows a better understanding of the different insertions of this complex proxi-mally and distally and detection of its lesions. Appropriate treatment of these lesions avoids the failures of classic arthroscopic reattachment and their associated persistent radioulnar insta-bility since the problem had been only partially
addressed. Numerous arthroscopic techniques of suturing the TFCC dorsal capsule have been proposed with the advantage of a direct suture of the distal medial portion of the TFCC lesions and often produce good results. In proximal TFCC lesions with clinical distal radioulnar instability, traditional arthroscopic suture techniques can-not restore stability, as reinsertion of the foveal attachment of this ligament is not possible. Open surgical technique has been recommended so far to achieve transosseous reinsertion of the TFCC. Despite the good results often reported, this operation often resulted in stiffness and limita-tion of pronosupination. With the advances in arthroscopy, this operation can be done with bet-ter results [4, 6].
The healing potential of the TFCC depends mainly on its blood supply – mainly, branches of the ulnar artery and palmar and dorsal branches of the anterior interosseous artery. Poor vascular-ization limits the possibility of a good quality repair as often seen in old TFCC lesions with retraction (stage 4). Blood supply is sometimes altered in some congenital malformations as, for example, styloid hypoplasia. Good quality carti-lage is a condition (sine qua non) for TFCC repair. The classi fi cation proposed by Atzei under EWAS has shown the possibility of existence of isolated proximal lesions, formerly undetected [2]. Recent studies analyzing arthroscopic repair by the Hong Kong team [3] have shown that 51 % of their 35 patients could not be appropriated by the Palmer classi fi cation. With an average follow-up of 39 months, they had 26 % bad results. In 45 % cases, these bad results were due to DRUJ instability. More recently, the Mayo Clinic team has published a comparative study of results of the classic arthroscopic repair techniques and open surgery. In the arthroscopic series, there were 17 % reoperations for persistent DRUJ instability [1].
Extensive distal peripheral tears involving the entire dorsal insertion of the TFCC do exist in reality, even if rare. Simple peripheral suture techniques do not achieve good repair in this case. Double loop sutures using the “in-and-out” principle allow excellent healing.
b
a
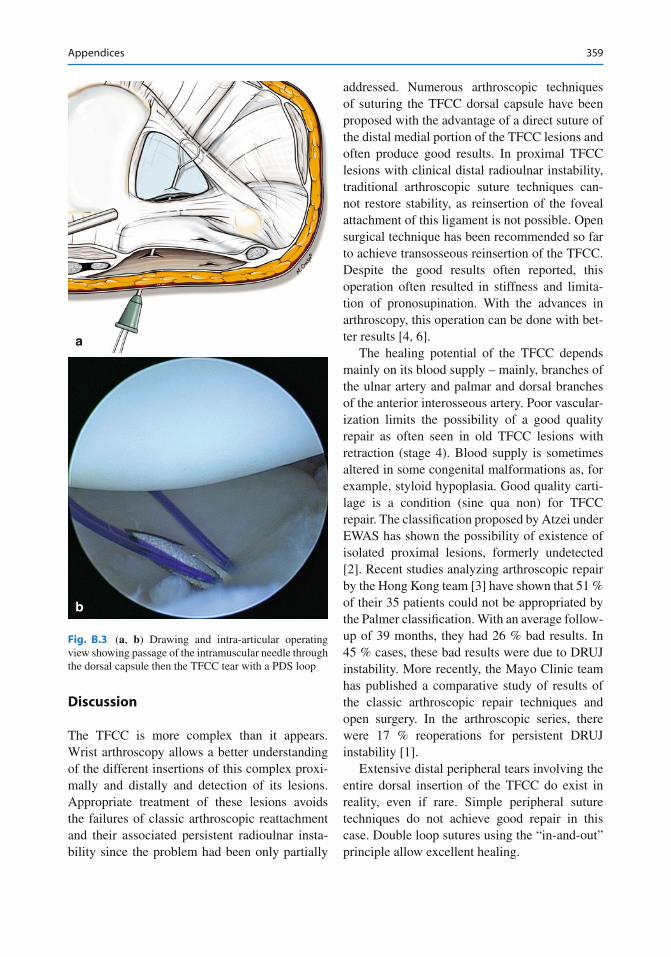
Fig. B.3 ( a , b ) Drawing and intra-articular operating view showing passage of the intramuscular needle through the dorsal capsule then the TFCC tear with a PDS loop

360 Appendices
b
c
a
Fig. B.4 ( a , b , c ) Drawing, intra -articular operating view, and external operative view of the PDS loop retrieved using a forceps through 6R portal
361Appendices
b
a
Fig. B.5 ( a , b ) Drawing and intra-articular operating view showing the passage of the second suture beside the fi rst and similarly retrieved through 6R
b
c
a
Fig. B.6 ( a , b , c ) Drawing, intra-articular operating view, and external operative view showing the passage of the third suture beside the others and similarly retrieved through 6R
362 Appendices
b
c
a
Fig. B.8 ( a , b , c ) Drawing, intra-articular operating view, and external operative view showing the trick to place the second and third single suture in the fi rst loop, which is pulled through the DRUJ leading the sutures through with it, thereby leaving two single loops inside the joint at the end
Fig. B.7 Operative view showing the three sutures, two simple and one loop, passed via the RUP through the cap-sule and the TFCC (the loop in the center and the two simple sutures radial and ulnar) and retrieved through 6R to the exterior
363Appendices
Fig. B.9 Drawing showing the two intra-articular loops before suture of the entire zone of the TFCC tear
b
c
a
Fig. B.10 ( a , b , c ) Drawing, intra-articular view, and external operative view showing the two intra-articular loops after suture, allowing complete repair of the entire zone of the TFCC tear

364 Appendices
Conclusion
Arthroscopic analysis of the radiocarpal and distal radioulnar joints has allowed better appreciation and understanding of the com-plexity of the TFCC. It has shown the impor-tance of the proximal component and the foveal insertion for the stability of the DRUJ. Complete tears of the dorsal insertion of the TFCC are an example. The double loop suture allows simple ef fi cient repair of these lesions. It allows healing for most patients, especially sports persons who can thereby regain a func-tional painless wrist.
References
1. Anderson LM et al (2008) Clinical comparison of arthroscopic versus open repair of triangular fi brocartilage complex tears. J Hand Surg 33A:675–682
2. Atzei A et al (2008) Arthroscopic foveal repair of trian-gular fi brocartilage complex peripheral lesion with dis-tal radioulnar joint instability. Tech Hand Up Extrem Surg 12(4):226–235
3. Estrella PE et al (2007) Arthroscopic repair of triangular fi brocartilage complex tears. Arthroscopy 23:729–737
4. Fulcher S, Poehling G (1998) The role of operative arthroscopy for the diagnosis and treatment of lesions about the distal ulna. Hand Clin 14:285–296
5. Palmer AK, Werner FW (1981) The triangular fi brocartilage complex of the wristVanatomy and func-tion. J Hand Surg Am 6:153–162
6. Pederzini L, Luchetti R, Soragni O et al (1992) Evaluation of the triangular fi brocartilage complex tears by arthroscopy, arthrography, and magnetic reso-nance imaging. Arthroscopy 8:191–197
365F. del Piñal et al. (eds.), Arthroscopic Management of Ulnar Pain, DOI 10.1007/978-3-642-30544-3, © Springer-Verlag Berlin Heidelberg 2012
Index
A Acute injuries treatment, LT tears
conservative , 223 debridement , 223 pin fi xation, LT interval ( see Pin fi xation, LT interval) plication ( see Plication, LT tears)
All-inside repair techniques dorsal capsular tears, TFC , 349 epidural needle , 355 reattachment, TFC , 355 suture materials , 353 variant 1 variant 2 water in fi ltrates , 352
Arthroscopy axial section , 121–122 cannula , 124–125 dorsal portal , 122–123 hamate impingement , 191–192, 194 instruments , 121, 123 LT ligament
classi fi cation , 218, 221 integrity , 218 location, size, extent and ligament injuries , 217 MCR and MCU portal, lunate type II , 218, 222 portal visualization , 217–218
partial resection, distal ulna , 175, 178, 179 resection , 180 surgeons
CT and MR arthrography , 63–64 description , 61–62 intra-articular injuries ( see Intra-articular injuries) MR imaging , 62–63 radiography , 61, 62 tendinous injuries , 78–82 ulnar nerve neuropathy , 82–83 ultrasound , 61, 62 vascular injuries , 83–84
techniques lunate drilling ( see Lunate drilling) radiographic changes , 258 revascularization, drilling , 258–259 scaphocapitate fusion ( see Scaphocapitate fusion)
shell removal, lunate cartilage , 258 treatment
midcarpal instability ( see Midcarpal instability) ulnocarpal abutment ( see Ulnocarpal abutment)
ulnar styloidectomy , 187–190 ulnolunate con fl ict , 174 volar portal , 123–124 working con fi guration , 124, 125
B Bag worms sign, 258 Ballottement test
de fi ned , 215 and gliding , 30 joint manipulation , 215, 217
1B constellation capsule
anterior detachments , 90, 94 hypertrophic synovium and scarred tissue , 94, 95 partial detachment , 94 ulno-lunate , 94, 95
horizontal tears , 95, 96 TFCC ( see Triangular fl brocartilaginous complex
(TFCC)) ulnar styloid
fovea , 88–89 impingement , 89 motocross racer , 88–91 non-united styloid , 89, 92 stable , 88
Biomechanics, TFCC eccentric dorsal fi bers , 19 RUL , 17–18 TFC , 19
C Capitohamate (CH) axial carpal instability, wrist
anatomy and biomechanics , 275, 277, 278 bone scan , 278, 280 diagnosis , 279 punching mechanism , 277
366 Index
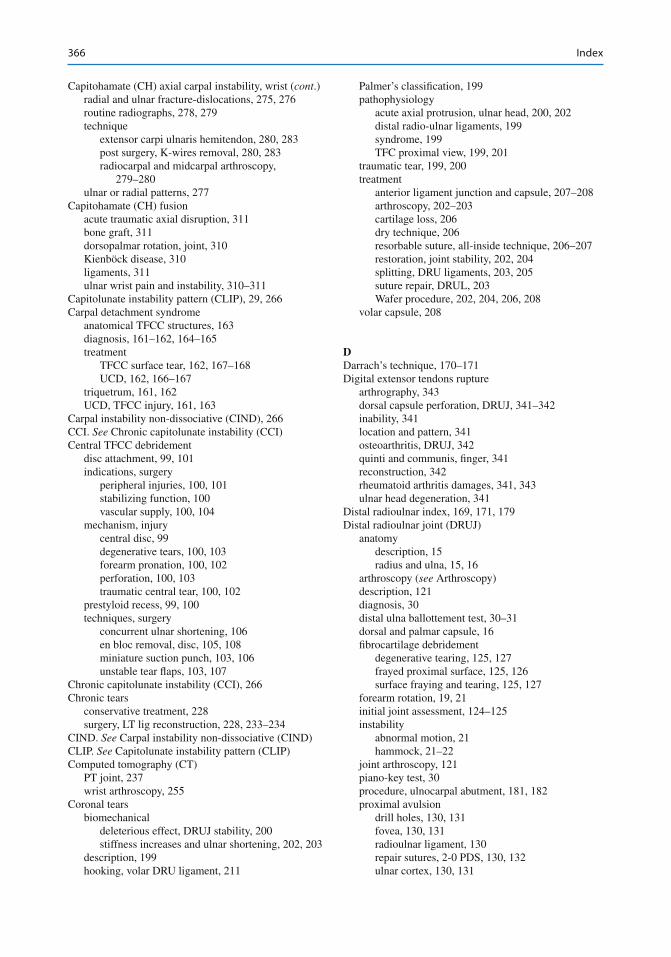
Capitohamate (CH) axial carpal instability, wrist ( cont .) radial and ulnar fracture-dislocations , 275, 276 routine radiographs , 278, 279 technique
extensor carpi ulnaris hemitendon , 280, 283 post surgery, K-wires removal , 280, 283 radiocarpal and midcarpal arthroscopy ,
279–280 ulnar or radial patterns , 277
Capitohamate (CH) fusion acute traumatic axial disruption , 311 bone graft , 311 dorsopalmar rotation, joint , 310 Kienböck disease , 310 ligaments , 311 ulnar wrist pain and instability , 310–311
Capitolunate instability pattern (CLIP) , 29, 266 Carpal detachment syndrome
anatomical TFCC structures , 163 diagnosis , 161–162, 164–165 treatment
TFCC surface tear , 162, 167–168 UCD , 162, 166–167
triquetrum , 161, 162 UCD, TFCC injury , 161, 163
Carpal instability non-dissociative (CIND) , 266 CCI. See Chronic capitolunate instability (CCI) Central TFCC debridement
disc attachment , 99, 101 indications, surgery
peripheral injuries , 100, 101 stabilizing function , 100 vascular supply , 100, 104
mechanism, injury central disc , 99 degenerative tears , 100, 103 forearm pronation , 100, 102 perforation , 100, 103 traumatic central tear , 100, 102
prestyloid recess , 99, 100 techniques, surgery
concurrent ulnar shortening , 106 en bloc removal, disc , 105, 108 miniature suction punch , 103, 106 unstable tear fl aps , 103, 107
Chronic capitolunate instability (CCI) , 266 Chronic tears
conservative treatment , 228 surgery, LT lig reconstruction , 228, 233–234
CIND. See Carpal instability non-dissociative (CIND) CLIP. See Capitolunate instability pattern (CLIP) Computed tomography (CT)
PT joint , 237 wrist arthroscopy , 255
Coronal tears biomechanical
deleterious effect, DRUJ stability , 200 stiffness increases and ulnar shortening , 202, 203
description , 199 hooking, volar DRU ligament , 211
Palmer’s classi fi cation , 199 pathophysiology
acute axial protrusion, ulnar head , 200, 202 distal radio-ulnar ligaments , 199 syndrome , 199 TFC proximal view , 199, 201
traumatic tear , 199, 200 treatment
anterior ligament junction and capsule , 207–208 arthroscopy , 202–203 cartilage loss , 206 dry technique , 206 resorbable suture, all-inside technique , 206–207 restoration, joint stability , 202, 204 splitting, DRU ligaments , 203, 205 suture repair, DRUL , 203 Wafer procedure , 202, 204, 206, 208
volar capsule , 208
D Darrach’s technique , 170–171 Digital extensor tendons rupture
arthrography , 343 dorsal capsule perforation, DRUJ , 341–342 inability , 341 location and pattern , 341 osteoarthritis, DRUJ , 342 quinti and communis, fi nger , 341 reconstruction , 342 rheumatoid arthritis damages , 341, 343 ulnar head degeneration , 341
Distal radioulnar index , 169, 171, 179 Distal radioulnar joint (DRUJ)
anatomy description , 15 radius and ulna , 15, 16
arthroscopy ( see Arthroscopy) description , 121 diagnosis , 30 distal ulna ballottement test , 30–31 dorsal and palmar capsule , 16 fi brocartilage debridement
degenerative tearing , 125, 127 frayed proximal surface , 125, 126 surface fraying and tearing , 125, 127
forearm rotation , 19, 21 initial joint assessment , 124–125 instability
abnormal motion , 21 hammock , 21–22
joint arthroscopy , 121 piano-key test , 30 procedure, ulnocarpal abutment , 181, 182 proximal avulsion
drill holes , 130, 131 fovea , 130, 131 radioulnar ligament , 130 repair sutures, 2-0 PDS , 130, 132 ulnar cortex , 130, 131
367Index
stability, coronal tears , 200 TFCC ( see Triangular fl brocartilaginous complex
(TFCC)) wafer resection con fi ne
distal ulna , 127–128 sigmoid notch and fovea , 128, 129 ulnocarpal impaction , 128
Dorsal distal radioulnar (DRUJ) arthroscopy , 53 determination , 53 dorsal and volar , 48 TFCC , 56 volar ulnar aspect , 54
Dorsal portals 3–4 portals , 48–49 4–5 portals , 49 6R and 6U portals , 49
Double loop technique, TFCC rupture advantage, direct suture , 359 arthroscopic analysis , 357 cartilage quality , 359 classi fi cation , 357 complete suture , 358, 363 distal peripheral tears , 359 extensive peripheral lesion , 357 “in-and-out” principle , 359 intra-articular loops before suture , 358, 363 intramuscular needle passing, PDS loop ,
357, 359 intramuscular needle places , 358, 361 large dorsal tear , 357, 358 loop pushes, DRUJ portal , 358, 362 Palmer classi fi cation , 359 PDS loop retrieve, 6R radiocarpal portal , 357 physiotherapy , 358 radioulnar portal , 357 RUP , 357 saline injection , 357 surgery, arm tourniquet , 357 sutures passes, DRU portal , 358, 362 synovial resector, ligament tear , 357, 358 treatment , 359 vascularization limits , 359 wrist arthroscopy , 359 wrist traction , 358
Drawer’s test , 34 DRUJ. See Distal radioulnar joint (DRUJ); Osteoarthritis,
DRUJ
E ECU. See Extensor carpi ulnaris (ECU) EDM. See Extensor digiti minimi (EDM) Extensor carpi ulnaris (ECU)
anatomy , 5–6 description , 78 factors , 286 hemiresection, ulnar head , 170, 174 imaging diagnosis
luxation , 80–81
radiography , 80 tenodinosis and partial tear , 80, 81
instability capsular fl ap raises and ECU tendon ,
337, 339–340 dorso-ulnar approach, fi fth compartment ,
337, 341–342 fi bro-osseous sheath , 336 Innoue distribution , 337–339 osteophytes and suture anchors , 337 retinaculum , 336 sand scoop test and surgical repair , 337
nonrheumatoid ruptures , 80 palmer 1B tear , 289 pathology , 78, 81 subluxation , 79, 287 subsheath injury , 289 synergy test , 38 tendinopathy
conservative and surgical treatment , 336 ECU instability , 335–336 in fl ammation, proliferation
and maturation , 335 symptoms , 336 tendinosis , 335 TFCC tear diagnosis , 335, 336
tendon subluxation test , 36, 38 Extensor digiti minimi (EDM)
hemiresection, ulnar head , 170 slip, tendon , 350, 351
Extra-articular ulnar-side pain causes , 335 diagnosis , 335 digital extensor tendons ( see Digital extensor tendons
rupture) ECU
instability , 336–340 tendinopathy , 335–336
fl exor carpi ulnaris tendinopathy , 340–341 hamate fracture and non-union hook , 346–347 hypothenar hammer syndrome ( see Hypothenar
hammer syndrome) neurogenic , 343–345
F FCU. See Flexor carpi ulnaris (FCU) Flexor carpi radialis (FCR) , 48, 51, 153 Flexor carpi ulnaris (FCU)
imaging diagnosis , 82 injuries , 82
Flexor carpi ulnaris tendinopathy , 340–342 Four corners fusion
arthroscopic , 302 capitate reduction , 305 cartilage shell, burring , 303 chronic pathology , 301 clinical impact , 301–302 MCU and MCR portal , 303, 304 partial wrist and mid-carpal , 302
368 Index
Four corners fusion ( cont. ) pathology , 301 scaphoid
excision , 304 removal , 301
SNAC/SLAC wrist , 301 triquetrohamate arthrodesis , 302
Foveal detachment, TFCC arthrogram , 137, 138 arthroscopic transosseous repair , 142, 143 diagnosis , 137–138 DRUJ arthroscopy fi ndings , 138–139 indication , 139 MRI , 137, 138 radioulnar ligament tear , 139, 140 suture anchor/screw , 141 ulnar nerve , 139, 141
G Gliding test , 30 Gripping rotatory impaction test (GRIT) , 29 GRIT. See Gripping rotatory impaction test (GRIT)
H Hamate impingement
arthritis , 191 arthroscopy , 191–192, 194 clinical features , 191 description , 191 distinction , 191 plain radiographs , 191, 193 radiological survey , 191 shapes , 191, 192 surgical technique
MRI, proximal pole , 193, 195 procedures , 192 triquetro-hamate (T-H), UMC swapping portal ,
196 swelling, UMC portal , 191, 192 treatment , 192
Hook hamate fracture and non-union acute internal fi xation , 346–347 carpal bone , 346 CT , 346, 347 diagnosis , 346 pain resisted fl exion, little fi nger , 346
Hook of the hamate pull test , 42–43 Hook test, 150 Hypothenar hammer syndrome
description , 83 imaging diagnosis , 83–84 intimal hyperplasia , 83
I Intra-articular injuries
ligamentous LT , 74, 75
MCI , 74 lunotriquetral coalition , 78–80 osseous
fractures ( see Osseous injuries, fractures) Kienböck disease , 76–77 Pseudo-Kienböck , 76–77, 79
TFCC ( see Triangular fl brocartilaginous complex (TFCC))
ulnar-sided wrist impaction syndromes ( see Ulnar-sided wrist impaction syndromes)
K Kienböck’s disease. See also Wrist arthroscopy
classi fi cation , 77 description , 76–77 symptoms , 77
L Ligament reconstruction, arthroscopy
ballottement test , 149 diagnostic imaging , 150 hypoplasia , 150 indications , 151 outcomes and complications , 158–159 painful wrist , 149 postoperative treatment , 158 radiocarpal , 150 radioulnar translation , 149–150 surgical technique
DETG , 156, 157 diagnostic wrist arthroscopy , 152 PETG , 155, 156 tendon graft harvest and radial
tunnel , 152–154 ulnar tunnel , 154–155
tensioning and fi xation, tendon graft , 157, 158 TFCC , 147
Loaded pronosupination test , 36, 37 Lunate and triquetrum (LT lig) tears and repair
anatomy and biomechanics meniscal projection , 213 proximal row movement , 213–214
arthrography , 216, 221 CT , 217 description , 213 diagnosis , 215
Ballottement test , 215, 217 examination, ulnar side wrist and LT
interval , 215, 216 proximal row squeeze (PRS)
test , 215, 219 shear test , 215, 218 ulnar snuffbox , 215
injury , 214–215 MRI , 217, 221 pathomechanics , 214 radiography , 216, 220 staging , 222
369Index
treatment acute injuries ( see Acute injuries) chronic tears ( see Chronic tears) modalities , 223
video fl uoroscopy , 217 Lunate drilling
capabilities , 260 debridement , 259–260 fl uoroscopy and surgical planning , 259 large, free- fl oating, osteochondral lunate
fragment , 260 loose removal and necrotic lunate , 260 midcarpal joint , 259 procedures , 260–261
Lunotriquetral palmar region , 53 SLIL , 48–49
Lunotriquetral compression test , 39, 41 Lunotriquetral (LT) fusion
burring , 308–309 cannulated screw insertion , 310 description , 308 intercarpal arthrodesis , 308 midcarpal arthroscopic approach , 308 minimal scarring, surgical wounds , 310, 311 open procedure , 308 shortening osteotomy , 308 X-ray and Geissler grade 3 , 308, 309
Lunotriquetral (LTq) joint ballottement test , 32–33 Derby test , 32, 35 shear test or shuck test , 32, 34
M Magnetic resonance imaging (MRI)
LT lig injury , 217, 221 proximal pole, hamate impingement , 193, 195 PT joint , 237 ulnocarpal abutment , 169, 172 wrist arthroscopy , 254–255
MCI. See Midcarpal instability (MCI) MCS. See Midcarpal space (MCS) Meniscus homologue
description , 3 TFC , 4
Midcarpal instability (MCI) abnormal movements , 267–268 anterior drawer test , 267 arthroscopic-assisted reconstructions , 269 arthroscopic thermal shrinkage , 269 collagen fi brils , 269 complications , 272 description , 265 fl exion loss, capsular shrinkage , 272, 273 fl uoroscopy , 268 gyroscopic spinball, strengthening , 268 imaging techniques , 267 kinematics
CCI, CIND and CLIP , 266 dorsal wrist ligaments , 266 volar wrist ligaments , 266 wrist motion , 265
partial wrist fusion , 268 posterior drawer test , 267 post-operative rehabilitation , 272 severity , 268 soft tissue reconstructions , 268–269 symptomatic giving way , 266 technique
Midcarpal portals dorsal , 50 TH , 50, 51
Midcarpal shift test , 41–42, 267
N Neurogenic ulnar-sided wrist pain
dorsal sensory , 344 Guyon’s canal/tunnel , 343–344 irritation , 344 MRI, cervical spine cord , 344, 346 TOS , 344
O Open ulnar styloidectomy
disadvantages , 187 dorsal approach , 185 DRUJ capsule , 185 ligamentous repair , 187
Osseous injuries, fractures fi fth metacarpal base , 76 hamate , 75–76 imaging diagnosis , 75 psiform , 76 stress reactions , 75 triquetrum , 76, 77 ulnar styloid , 75
Osteoarthritis, DRUJ anatomic alignment , 315 arthroscopy , 315 complications , 319 Darrach procedure , 315 description , 315 ECU tendon , 332 evaluation, pre-and postoperative , 321, 324 indications , 316 open surgery , 315 post-traumatic and LT instability , 321 rigidity , 321 S-K procedure ( see Sauvé-Kapandji (S-K) procedure)
P Palpation
anatomical landmarks , 27–29 description , 26
370 Index
Partial wrist fusion, instability and arthritis arthroscopy , 296 autogenous bone grafting
arthroscopic cannula , 300 control and monitor , 300, 301 de fi nition , 299 impaction, blunt trocar , 300 injection and small chips , 300 vascularity and quality , 299 wide bore needle , 300
carpal fusion , 299 cartilage denudation
blade rotation and oscillating mode , 298 burring , 298–299 excessive cartilage and subchondral bone
removal , 298 punctate bleeding, subchondral
bone , 298, 299 contraindications , 296–297 de fi nitive fi xation , 301 description , 295 DRUJ , 296 pisotriquetral , 296 primary osteoarthritis , 296 setup and instrumentation , 297 severe posttraumatic , 296 surveillance
hemostasis effect, lignocaine , 297, 298 inspection , 297 intra-articular injection , 297 midcarpal joint , 298 synovial growth , 298
technique and rehabilitation capitohamate , 310–311 four corners , 301–308 lunotriquetral , 308–310 pisotriquetral fusion , 312 triquetrohamate , 312
techniques , 297 wrist arthritis , 296
PETG. See Palmer end of the tendon graft (PETG) Piano-key test , 30 Pin fi xation, LT interval
fi brodesis creation and joint stabilize , 224, 226 fl uoroscope , 224 K-wires , 224 LT instability , 226 reduce and stabilize , 224, 225 scope MCR portal , 224 TFCC tears and DRUJ instability , 226 unstable LT dislocation reduction , 224, 227
Piso-triquetral (PT) fusion , 312 Piso-triquetral (PT) joint
anaesthetic injections , 245 anatomy
carpal and sesamoid bone , 238 communication types , 239, 240 FCU and acts , 238 radial and ulnar stabilisers , 238, 239
ulnar-sided cutaneous nerves , 239 variations, radio-carpal joint , 239, 240 wrists connections , 239
biomechanics/kinematics , 239, 240 carpus , 243 diagnosis , 237 differential diagnosis , 243 examination , 243–245 FCU , 237 imaging
CT , 247 MRI scanning , 247 plain x-rays , 246 radiology , 235, 246 SPECT , 247–248
osteoarthritis , 237 palpate, painful structures , 243, 245 pathology
loose bodies , 243 osteoarthritis , 240–241 pisiform , 243 post-traumatic , 243 suffers , 240 wear patterns , 241–243
pisiformectomy , 237–238 proximity , 237 site pain and pinpoint , 243 super fi cial volar stabiliser , 238 therapy, arthroscope , 249–250 visualisation
clockwise rotation , 248–249 dilatation and arthroscopic excision , 249 3/4 portal view , 248 standard radio-carpal portals , 248
X-rays, MRI and CT , 237 Plication, LT tears
complications , 228 establishment, volar 6U portal , 227, 228 forearm immobilization , 227–228 outside volar 6U portal and RC joint , 227, 232 pinning , 226 suture passes, volar 6U portal , 227, 229–231 UC lig performance , 226
Portals CMC , 56 contraindications , 46 description , 45 dorsal anatomy , 46–47 DRUJ ( see Dorsal distal radioulnar (DRUJ)) equipment and implants , 57 FCR , 48 fracture dislocation, metacarpal , 58–59 indications
DRUJ , 46 midcarpal arthroscopy , 45 VR , 45 VRM , 46 VU , 46
metacarpal , 57
371Index
methodology dorsal ( see Dorsal portals) midcarpal ( see Midcarpal portals) scaphotrapezial , 50–51 SLIL and LTIL , 48–49 volar , 51–53 VRM , 53
TFCC ( see Triangular fl brocartilaginous complex (TFCC))
VDRU , 54 Proximal row squeeze (PRS) test , 215, 219 Pseudo-Kienböck lesions
description , 77 MR imaging , 77, 79
PT joint. See Piso-triquetral (PT) joint
R Radial midcarpal (RMC) portal , 193 Radioulnar compression test , 36, 37 Radioulnar ligament (RUL)
dorsal and palmar , 18 fovea , 22 and TFC , 17 TFCC , 17
RMC portal. See Radial midcarpal (RMC) portal
S Sauvé-Kapandji (S-K) procedure
advantages , 332 burrs sizes , 318 cannulated screw insert , 318, 322 conventional open surgery , 319–320 dry arthroscopy , 317–318 end procedure, DRUJ fi xation , 318, 325 K-wire insertion , 318, 321 osteotomy and K-wire position , 318, 322 pronosupination wrist motion, end procedure ,
318, 324 rehabilitation and physical therapy , 320 remnant cartilage removal, 6R portal ,
317, 318 screw tightening, after resection , 318, 323 severe chondral damage and sub-chondral
bone expose , 317 synovectomy , 317 ulnocarpal impaction syndrome,
DRUJ surgery , 316, 317 Wafer resection , 317, 318 wrist rotation and pronation pushing ,
318, 319 ulnar head resection , 328, 333
Scaphocapitate fusion evaluation, probing , 261 fi nal fi xation , 261, 262 loose bodies removal , 261 midcarpal joint and resection , 261, 262 radio and midcarpal joints , 261
Scapholunate (SLIL) and LTIL , 48–49 VRM portal , 53
Scaphotrapezial portals STT-P portal , 50 STT-R portal , 50, 52 STT-U portal , 50
Scaphotrapezial-trapezoidal (STT) cadaver dissections , 50 chondral damage , 271
STT. See Scaphotrapezial-trapezoidal (STT) Suturing techniques
all-inside repair techniques ( see All-inside repair techniques)
double loop technique ( see Double loop technique, TFCC rupture)
T Tendinous injuries
ECU ( see Extensor carpi ulnaris (ECU)) FCU ( see Flexor carpi ulnaris (FCU))
TFC. See Triangular fi brocartilage (TFC) TFCC. See Triangular fl brocartilaginous complex
(TFCC) Thoracic outlet syndrome (TOS) , 344, 345 TILT. See Triangular impingement ligament
tear (TILT) TOS. See Thoracic outlet syndrome (TOS) Traumatic injuries, TFCC
avascular disc central slit , 64 carpal detachment , 66, 67 distal radius fracture , 64–65 foveal insertion , 64, 65 IB foveal tear , 64, 66 ID lesion , 64, 66 imaging diagnosis , 66, 67 Palmer’s classi fi cation , 66, 67 styloid insertion , 64, 65 ulnar insertion , 64
Triangular fi brocartilage (TFC) arthroscopic suture technique Atzei’s classi fi cation , 111, 112 capsular sutures , 120 diagnosis and indications , 111, 113 diagnostic arthroscopy , 113 disc proper , 162, 167 distal extension , 4 fl ap tear , 162 junctional portion , 199, 201 and meniscus homologue , 17 orthesis , 120 RUL , 17 shape , 19 surface , 162, 166
Triangular fl brocartilaginous complex (TFCC). See also Central TFCC debridement
anatomy , 54 arthroscopic assessment , 53
372 Index
Triangular fl brocartilaginous complex (TFCC) ( cont. ) Atzei’s class , 290 biomechanics , 17–19 calcium deposition , 151 capsule anterior , 271–272 carpal attachment and bones , 161 carpal detachment , 162, 165 chronic massive peripheral tear , 150, 151 classi fi cation, peripheral tears , 147 con fi gurations types , 161 coronal tears ( see Coronal tears) degenerative processes , 293 distal rupture , 87–88 dorsal UT ligament , 293 DRUJ ( see Distal radioulnar joint (DRUJ)) exposed, covered and attachment type ,
161, 163 foveal avulsion , 11–12 foveal detachment ( see Foveal detachment,
TFCC) ligaments , 147, 149 lunate-triquetrum ligament , 292 MRI , 286, 290 proximity , 87 radial and ulnar deviation stresses , 161–162, 164 radial insertion , 49 radiocarpal joint , 163 radioulnar ligament , 16 and radius , 17, 19 stability , 287 stress test , 161 surface tear, carpal detachment ,
162, 165 three-dimensional structure , 17 traumatic tears , 64–67 triquetrum, articular surface , 161 ulnar corner, periphery , 272 ulnar-sided pain. , 161, 293 ulnar styloid , 17, 18 ulnolunate con fl ict ( see Ulnocarpal abutment)
Triangular impingement ligament tear (TILT) soft tissue lesion, wrist , 163 triquetral fi brous tissue , 163
Triquetro-hamate (TH) fusion , 312 portal , 50, 51, 196
U UCD. See Ulnocarpal detachment (UCD) Ulnar head hemiresection
closed extensor retinaculum and dorsal capsule , 170, 174
description , 170 ECU roll , 170, 174 EDM , 170 Fernandez principle , 170, 173 immobilization and physiotherapy , 170 TFCC and half ECU harvesting , 170, 173
Ulnar head resection advantages , 333 anatomical conditions , 333 Bowers procedure , 325 complication , 328, 332 description , 325 ECU/FCU tendons , 333 open surgery , 328 S-K procedure , 333 surgical technique
dry arthroscopy , 328 exposed, TFCC , 317, 328 foveal insertion, secondary DRUJ instability , 328 intraoperative images , 328–331 position changes, burr , 328 S-K procedure , 328 synovectomy , 328 Wafer resection , 328
Ulnar injuries, distal radius fractures acute and chronic setting , 285–286 degenerative processes , 293 description , 285 distal radius fracture , 289–290 ECU
pathology , 292 subsheath, tear , 286, 289
impaction, osteoarthritis and lunate-triquetrum ligament injury , 286, 288
negative bone scan , 286, 289 osteoarthritic changes, bone scan , 287, 290 positive variance, impaction , 292 schematic drawing, palmer 1B tear , 292–293 stable and unstable, pain , 286, 289 styloid fracture , 286, 288, 293 technique
ballottement and hook test , 289 “satisfaction of search” , 287 TFC complex assessment , 289–291 traction , 287 wrist probe , 288
TFCC tears, MR imaging , 291 ulnar-sided wrist pain, diagnoses , 286–287
Ulnar midcarpal (UMC) portal , 193 Ulnar nerve neuropathy
anatomy , 82 imaging diagnosis , 83
Ulnar shortening osteotomy (USO) , 170, 173 Ulnar-sided painful wrist
clinical condition , 25 clinical examination
ballottement and gliding tests , 30 carpometacarpal joint , 34 DRUJ ( see Distal radioulnar joint (DRUJ)) ECU ( see Extensor carpi ulnaris (ECU)) hook of the hamate pull test , 42–43 loaded pronosupination test , 36, 37 LTq joint , 32–35 lunocapitate joint , 34, 36 lunotriquetral compression test , 39, 41
373Index
midcarpal shift test , 42–43 palpation ( see Palpation) pisotriquetral joint , 32, 35 provocative maneuvers , 34, 36 radioulnar compression test , 36, 37 range of motion and grip strength
determination , 29–30 TFC grind test , 38, 39 triquetral shift maneuver , 40, 41 triquetrohamate joint , 33–35 ulnocarpal joint , 31–32 ulnocarpal meniscoid test , 40, 41 USTI , 39, 40
description , 25–26 history , 26 inspection , 26
Ulnar-sided wrist impaction syndromes chronic impaction , 68 clinical manifestation , 68 hamatolunate
articulation , 73 imaging diagnosis , 73–74
imaging diagnosis IIC and IID lesion , 69 radiography , 68
impingement cardinal features , 69–70 clinical manifestation , 70 imaging diagnosis , 70–71
pathologic conditions , 68 styloid
imaging diagnosis , 72–73 subtypes , 71–72 triquetrum bone and soft tissues , 70, 71 USPI , 70–71
Ulnar styloidectomy articular damage , 188 CT, non-united ulnar styloid fracture , 189, 190 eburnated bone , 188, 189 fl uoroscopy , 187 open ulnar styloidectomy ( see Open ulnar
styloidectomy) pituitary rongeur and 6R portal removal , 189, 190 postoperative recovery , 187 preservation, dorsal branch , 187 procedure and modi fi cations , 187 removal, non-union prior , 189, 190 resection , 188 syndrome ( see Ulnar styloid impaction syndrome)
Ulnar styloid impaction syndrome aetiology , 183–184 characterization , 183 clinical features , 184 imaging
3D CT , 185 de fi nition, long ulnar styloid process , 184–185 echo coronal , 185, 186 plain posteroanterior radiograph , 185 SCR , 185, 186
USPI , 185, 186 pathology , 183 treatment , 185
Ulnar styloid process index (USPI) fractures , 70–71 relative ulnar styloid length determination , 185, 186
Ulnar styloid triquetral impaction (USTI) test axial load, palm , 39, 40 description , 39
Ulnocarpal abutment arthroscopy, ulnolunate con fl ict , 174, 179 clinical and paraclinical assessment
evaluation, functional disability , 169 MRI , 169, 172 neutral pronation position , 169, 172 radial deviation, ulnolunate con fl ict , 169, 172 symptoms , 169
de fi nition , 169 description , 169 distal radioulnar index , 169, 171, 179 mobility , 180 partial resection technique, distal ulna
arthroscopic control , 178–179 chondropathy , 175 DRUJ procedure , 181, 182 intra-articular view, osteotomy , 178–179, 181 pronation-supination movements , 178, 180–181 TFCC central perforation , 175, 178
postoperative hematomas , 180 relationship, ulna and radius , 169, 170 treatment
hemiresection, ulnar head , 170, 173, 174 Sauvé-Kapandji technique , 174, 176 ulnar head prosthesis , 174 ulnar head total resection , 170, 171, 173,
174, 175 USO and Milch’s ulnar shortening , 170, 173
ulnar variance , 179–180 ulnolunate con fl ict after distal radius fracture ,
180, 182 Ulnocarpal compartment
anatomy , 1 distal radioulnar and ulnocarpal joint , 6 ECU ( see Extensor carpi ulnaris (ECU)) kinematics
fi xed-point concept , 7, 9 ligament , 8 ligament paths , 9, 10 TFCC foveal avulsion , 11–12 ulnar fovea sign test , 13
ligaments ulnocapitate , 1, 2 ulnolunate ( see Ulnolunate ligament) ulnotriquetral ( see Ulnotriquetral ligaments)
meniscus homologue ( see Meniscus homologue) prestyloid recess , 5 ulnar nerve
dorsal branch , 7 Kaplan’s accessory branches , 7, 8
374 Index
Ulnocarpal detachment (UCD) carpal bone and TFC , 162, 167 cartilage defect , 163 dorsal carpal bone (DC) and TFC disc , 162, 166 fi brocartilage tissue , 162 hypertrophic synovium , 162, 166 mechanism , 162, 164 TFCC injuries , 161, 162, 165 ulnar deviation stress , 161
Ulnocarpal meniscoid test , 40, 41 Ulnolunate ligament
apes wrist , 2, 4 and ulnotriquetral , 2
Ulnotriquetral ligaments anatomy , 2, 3 description , 1–2 ulnocarpal and radioulnar , 2, 4
UMC portal. See Ulnar midcarpal portal USO. See Ulnar shortening osteotomy (USO) USPI. See Ulnar styloid process index (USPI)
V Vacant fovea, 129–130 Vascular injuries
CT , 62 hypothenar hammer syndrome , 83–84
Volar portals SLIL and DRCL , 53
surface anatomy , 51, 52 ulnar , 53 VRM , 53
Volar radial midcarpal (VRM) portal portal , 53 SLIL , 53
Volar radial (VR) portal. See VR portal Volar ulnar (VU) portal
VDRU , 54 VR and , 52
VRM portal. See Volar radial midcarpal portal
VR portal FCR , 48 SLIL and DRCL , 48 and VU portals , 52
VU portal. See Volar ulnar portal
W Wafer procedure
coronal tears , 202, 204, 206, 208 positive ulnar variance , 106
Wafer resection DRUJ , 317, 318 ulnar head resection , 328
Waiter’s test. See Ulnocarpal meniscoid test Wrist clunk , 286
















![[XLS]didefth.grdidefth.gr/new/wp-content/uploads/30544-s-ΠΕ02.xlsx · Web view29 37 38 41 45 74 79 80 83 84 112 126 132 236 243 276 296 335 337 361 417 421 428 431 443 448 449 457](https://static.fdocuments.net/doc/165x107/5abd5c857f8b9ad8278bb4f5/xls-02xlsxweb-view29-37-38-41-45-74-79-80-83-84-112-126-132-236-243-276-296.jpg)

