
Appendix 2 - cygnethealth.co.uk · Appendix 2 Mental Health Act Inspection Report (Quarter 3) The...
41
Cygnet Health Care Service Quality Report Quarter 3: Oct – Dec 2015 Appendix 2 Care Quality Commission Mental Health Act Inspection Report (Quarter 3) The following pages contain the inspection report and action plan relating to CQC inspection at Cygnet Hospital Harrow during Quarter 3. Appendix 2 Care Quality Commission Mental Health Act Inspection Report (Quarter 3)
Transcript of Appendix 2 - cygnethealth.co.uk · Appendix 2 Mental Health Act Inspection Report (Quarter 3) The...
Cygnet Health Care Service Quality Report
Quarter 3: Oct – Dec 2015
Appendix 2
Care Quality Commission Mental Health Act Inspection Report
(Quarter 3)
The following pages contain the inspection report and action plan relating to CQC inspection at
Cygnet Hospital Harrow during Quarter 3.
Appendix 2 Care Quality Commission
Mental Health Act Inspection Report
(Quarter 3)

This report describes our judgement of the quality of care at this location. It is based on a combination of what wefound when we inspected and a review of all information available to CQC including information given to us frompatients, the public and other organisations
Ratings
Overall rating for this location Good –––
Are services safe? Good –––
Are services effective? Requires improvement –––
Are services caring? Good –––
Are services responsive? Good –––
Are services well-led? Good –––
Mental Health Act responsibilities and Mental Capacity Act and Deprivation of LibertySafeguardsWe include our assessment of the provider’s compliance with the Mental Capacity Act and, where relevant, MentalHealth Act in our overall inspection of the service.
We do not give a rating for Mental Capacity Act or Mental Health Act, however we do use our findings to determine theoverall rating for the service.
Further information about findings in relation to the Mental Capacity Act and Mental Health Act can be found later inthis report.
CCygneygnett HospitHospitalal HarrHarrowowQuality Report
London Road, Harrow on the HillMiddlesex HA1 3KlTel: 020 8996 7000Website: www.cygnethealth.co.uk
Date of inspection visit: 13 – 14 October 2015Date of publication: This is auto-populated when thereport is published
1 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Overall summary
We rated Cygnet Hospital Harrow as good because:
• Byron ward and Springs wing were clean and wellfurnished.
• The provider was refurbishing the wards to addressligature risks.
• Patients could access regular one-to-one time withtheir named nurse and staff rarely cancelled activitiesand leave.
• Patients said they felt safe on the wards.• The provider used regular bank workers to cover
vacancies and was actively recruiting to fill posts.• Staff completed patients’ risk assessments on
admission and reviewed them regularly.• Most staff were up to date with mandatory training
and there were systems in place to monitor this.• Staff completed patients’ assessments on admission
and most care records were complete, up to date andpersonalised to the individual patient’s needs.
• Patients had access to a range of psychologicaltherapies recommended by the National Institute forHealth and Care Excellence (NICE) guidelines.
• The wards had good multidisciplinary input andrespected all staff’s clinical backgrounds within teams.
• External stakeholders spoke positively about therelationship they had with the hospital, whichprovided regular updates on patients.
• Staff understood how to use the Mental Health Act(MHA) and completed MHA paperwork accurately.
• We observed kind and caring interactions betweenstaff and patients on all three wards. Patients’ familyand carers were involved with their care whereappropriate.
• The provider had regular integrated governancemeetings and fed this information back to staff teams.
• Staff were positive about their teams, managers andfelt respected.
However,
• There were some environmental concerns on Springsunit, including the nature of the environment, layoutof the ward, lack of visual signs and the way it servedthe needs of patients with autism.
• Staff on Springs wing and Springs unit had notcompleted specialist training in autism. This meantthat staff were not adequately trained to understandand manage patients’ needs.
• Staff did not always address patients’ physical healthneeds in a timely manner.
• Information stored in patients’ paper files was notalways easily accessible.
• Staff on Byron ward had not had regular supervision inthe last three months.
• Patients admitted to the wards informally did not haveclear information about their rights to leave the ward.
• Staff’s knowledge on the use and application of theMCA varied across the wards.
Summary of findings
2 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Contents
PageSummary of this inspectionBackground to Cygnet Hospital Harrow 5
Our inspection team 5
Why we carried out this inspection 5
How we carried out this inspection 5
What people who use the service say 6
The five questions we ask about services and what we found 7
Detailed findings from this inspectionMental Health Act responsibilities 10
Mental Capacity Act and Deprivation of Liberty Safeguards 10
Outstanding practice 37
Areas for improvement 37
Action we have told the provider to take 38
Summary of findings
3 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Location name here
Services we looked at
Acute wards for adults of working age and psychiatric intensive care units; Forensic inpatient/secure wards; Longstay/rehabilitation mental health wards for working-age adults
Locationnamehere
Good –––
4 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Background to Cygnet Hospital Harrow
Cygnet Hospital Harrow is provided by Cygnet HealthCare and registered with CQC on 15 November 2010.
Cygnet Hospital Harrow is a 44-bed service over threewards:
Byron ward – 18 beds, mixed acute psychiatric serviceprovides assessment, diagnosis and treatment for a widerange of psychological and emotional problems,including addictions.
Springs unit – 16 beds, low-secure ward for males withautism spectrum disorder, Asperger’s syndrome or highfunctioning autism.
Springs wing – 10 beds, open rehabilitation ward formales with an autism spectrum condition.
We have inspected Cygnet Hospital Harrow four timessince 2010, and published the most recent report inSeptember 2014. At the last inspection, Cygnet HospitalHarrow was meeting essential standards, now known asfundamental standards.
Cygnet Hospital Harrow is registered for the followingregulated activities:
Treatment of disease, disorder or injury
Assessment or medical treatment of persons detainedunder the Mental Health Act 1983
Registered Manager – Seamus Quigley
Accountable Officer – Seamus Quigley
Our inspection team
Team leader: Heather Mah The team that inspected the service included aconsultant psychiatrist, a CQC inspection assistant, a CQCinspection manager, three CQC inspectors, an expert byexperience, a Mental Health Act reviewer and apharmacist inspector.
Why we carried out this inspection
We inspected this service as part of our ongoingcomprehensive mental health inspection programme.
How we carried out this inspection
To fully understand the experience of people who useservices, we always ask the following five questions ofevery service and provider:
• Is it safe?• Is it effective?• Is it caring?• Is it responsive to people’s needs?• Is it well-led?
Before the inspection visit, we reviewed information thatwe held about the location, asked a range of otherorganisations for information.
During the inspection visit, the inspection team:
• Visited all three wards, looked at the quality of theward’s environment and observed how staff cared forpatients.
Summaryofthisinspection
Summary of this inspection
5 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Spoke with 18 patients who were using the service andtheir family/carers and collected feedback from threepatients using comment cards.
• Spoke with the hospital manager, clinical managerand quality assurance manager
• Spoke with the ward managers for each of the wards.• Spoke with 32 other staff members, including assistant
psychologists, catering staff, doctors, domestic staff,healthcare support workers, human resources, nurses,occupational therapists, a psychotherapist and atraining coordinator.
• Received feedback about the service from threeexternal stakeholders.
• Spoke with an independent advocate.• Attended and observed one ward round, one
community meeting and one multidisciplinarymeeting.
• Looked at 21 care and treatment records of patients.• Reviewed records of restraint and seclusion.• Looked at records regarding incidents, training, team
meetings, complaints, staffing levels and communitymeetings.
• Carried out a specific check of the medicationmanagement on all wards.
• Looked at a range of policies, procedures and otherdocuments relating to the running of the service.
What people who use the service say
Patients said they felt safe on the wards. Patients saidthat staff were kind and polite, and treated them withrespect. Patients knew how to make a complaint andcould raise concerns in the weekly community meetings.Patients spoke positively about the therapy and activities
on the wards and in the community, although they wouldlike more to do in the evenings and at weekends. Patientssaid they were involved in their care plans, whichincluded their family/carers where appropriate.
Summaryofthisinspection
Summary of this inspection
6 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

The five questions we ask about services and what we found
We always ask the following five questions of services.
Are services safe?We rated safe as good because:
• Byron ward and Springs wing were clean and well furnished.• The provider was refurbishing the wards to address ligature
risks.• Patients could access regular one-to-one time with their named
nurse and staff rarely cancelled activities and leave.• Patients said they felt safe on the wards.• The provider used regular bank workers to cover vacancies and
was actively recruiting to fill posts.• Staff completed risk assessments for patients on admission and
reviewed them regularly.• Most staff were up to date with mandatory training.
However,
• There were some environmental concerns on Springs unit.
Good –––
Are services effective?We rated effective as requires improvement because:
• Staff on Springs wing and Springs unit had not completedspecialist training in autism. The provider had not adequatelytrained staff to understand and manage patients’ needs.
• Staff did not always address patients’ physical health needs in atimely manner.
• Information stored in patients’ paper files was not always easilyaccessible.
• Staff on Byron ward had not had regular supervision in the lastthree months.
• Patients who were admitted to the wards informally did nothave clear information about their rights to leave the ward.
• Staff’s knowledge on the use and application of the MCA variedacross the wards.
However,
• Staff completed patient assessments on admission and mostcare records were complete, up to date and personalised toindividual patients’ needs.
• Patients had access to a range of psychological therapiesrecommended by NICE guidelines.
• The wards had good multidisciplinary input and respected allstaff’s clinical backgrounds within teams.
Requires improvement –––
Summaryofthisinspection
Summary of this inspection
7 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• External stakeholders spoke positively about the relationshipthey had with the hospital, which provided regular updates onpatients to them.
• Staff understanding and use of the Mental Health Act (MHA) wasgood and paperwork was completed accurately.
Are services caring?We rated caring as good because:
• We observed kind and caring interactions between staff andpatients on all three wards.
• Patients’ family and carers were involved with their care whereappropriate.
• Staff discussed patients respectfully during ward rounds.• The wards had regular community meetings where patients
could provide feedback and report any concerns.• Care records showed staff worked to engage patients in care
planning.• Patients received an information guide and introduction to the
ward on admission.• Patients had access to a range of activities at the hospital and in
the community, although some told us they would like more todo during the evenings and weekends.
Good –––
Are services responsive?We rated responsive as good because:
• The hospital had well-equipped occupational therapy rooms, alaundry room, gym, multi-faith room and large garden.
• Staff and patients said the food was generally good.• Staff could access interpreters when needed.• Patients knew how to raise a complaint and staff managed
these appropriately.
However,
• Patients’ confidentiality was not always maintained on Springsunit, as the ward board was visible from the ward.
• The environment of Springs unit was not autism friendly. It didnot have visual signs and the lay out made it difficult to reducenoise.
Good –––
Are services well-led?We rated well-led as good because:
• The provider had good systems in place to monitor mandatorytraining.
Good –––
Summaryofthisinspection
Summary of this inspection
8 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• The provider had regular integrated governance meetings andfed this information back to staff teams.
• The provider completed regular audits and ensured actionswere completed.
• Staff were positive about their teams, managers and feltrespected. Staff could report any concerns to their managers.
• The provider was committed to improving the quality of care onan on-going basis.
Summaryofthisinspection
Summary of this inspection
9 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Mental Health Act responsibilities
We do not rate responsibilities under the Mental HealthAct 1983 (MHA). We use our findings to help us determinean overall judgement about the Provider.
• Eighty nine percent of Cygnet Harrow staff hadcompleted training in the MHA. Staff said they feltconfident in using the MHA and were familiar with itscode of practice.
• There was a clear MHA process flowchart in the wardoffice. Staff said their MHA administrator was helpful.The MHA administrator could provide additionalmentoring and support to staff for any queries regardingthe MHA.
• Staff said they informed all patients of their rights underthe MHA and documented this in patients’ files.However, the three files we inspected on Springs wingdid not all contain a record of patients being told theirrights, although one of these patients confirmed stafftold them their rights.
• On Springs wing, staff ensured patients understoodthe provisions of the MHA that applied to them andtheir right to appeal to the tribunal when they wereplaced under the MHA and when their section wasrenewed. We did not find evidence that this wascarried out on other occasions. Patients had regularaccess to an advocate who visited the wards regularly.The advocate confirmed that staff were supportive ofadvocacy and regularly referred patients requiringsupport to the advocacy service.
• Staff filled detention paperwork correctly. All patientshad their legal status and dates for renewal recorded.The treatment forms were with patients’ medicationcharts as required.
• On Springs unit, staff made referrals tosecond-opinion appointed doctors where appropriate.However, one patient on Springs wing was waiting fora medication change to be authorised by asecond-opinion appointed doctor. The requiredpaperwork was not completed in a way, whichcomplied with the MHA.
• Assessments of capacity to consent to treatment werenot carried out on a regular, systematic basis.
• Information in a leaflet given to informal patientsregarding their right to leave the hospital showed thatinformal patients might not be fully aware of their rightsto leave the hospital at will. This leaflet stated thatinformal patients could only leave the hospital grounds‘with the consent and agreement of the nursing staff/responsible Clinician’. In addition, the board in Byronward’s office indicated a leave status of “Leave NotRecommended” for all informal patients on the wardwhich possibly compromised their freedom ofmovement.
• Cygnet Hospital Harrow maintained a database onpatients’ MHA details including their MHA status, date ofsection and expiry, consent to treatment and dates oftribunals and hearings. The provider had an integratedgovernance and integrated audit meetings every othermonth that included monitoring MHA compliance. All ofCygnet’s MHA administrators met at MHA governancemeetings twice a year to evaluate current practices anddiscuss updates to the MHA.
Mental Capacity Act and Deprivation of Liberty Safeguards
• Although most staff across the wards completed trainingin the Mental Capacity Act (MCA), their knowledge of theMCA was variable. It was not always clear how they weresupporting patients to make relevant decisions. Staff onSprings unit did not always record that they hadassessed an individual’s capacity to make a decision
when it was necessary to do so. Staff on the Springswing knew of the policy developed by Cygnet relating tothe MCA. Reading the MCA policy is part of theirmandatory training. It was also available for staff to readon the staff database. The provider reviewed this policy
Detailed findings from this inspection
10 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

in September 2015. However, when we looked at thepolicy, the provider had not updated it to reflectimportant legal changes effective from April 2014regarding DOLS.
• The ward doctor usually completed the consent totreatment part of the psychiatric assessment form uponadmission. However, staff did not regularly follow up onconsent and capacity issues.
• Staff said they had never considered the use ofDeprivation of Liberty Safeguards (DOLS) on Byron ward.The staff on Springs wing had not made anyapplications for DoLS in the past 12 months. There wereno patients subject to DoLS at the time of ourinspection.
• Springs unit staff assessed the capacity of patients tobudget and manage their own money.
Detailed findings from this inspection
11 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Safe Good –––
Effective Good –––
Caring Good –––
Responsive Good –––
Well-led Good –––
Are acute wards for adults of workingage and psychiatric instensive care unitservices safe?
Good –––
Safe and clean environment
• Byron ward was clean with all rooms en-suite except forthe three observation rooms behind the nursing station.The ward had spacious and well-decorated loungeareas and a well- kept garden.
• The wards did not have clear sight lines throughout, butthe observations process and the use of CCTV camerasmitigated this. There was no seclusion room on theward.
• The ward had ligature anchor points on the handles ofbedroom doors and in the ensuite bathrooms. However,a works programme was underway to replace these.Two rooms at a time were being worked on withapproximately nine weeks of work left to complete onthe ward. Staff mitigated these through regularobservation of the ward.
• The ward was mixed gender, but adhered to guidelineson same sex accommodation through careful allocationof rooms following risk assessments. The threeobservation rooms were never mixed gender becausethey shared a communal bathroom. There was afemale-only lounge.
• The observation rooms had transparent walls to enablestaff to see the areas around it and were located behindthe nursing station so that other patients could not see
into them. Patients with increased levels of risk weretransferred to these observation rooms and staff rapidlymoved patients into ensuite bedrooms once the level ofrisk diminished.
• All staff had fobs with alarms. The ward had a radiocommunications system on the unit and staffcompleted health and safety assessments on a quarterlybasis.
• The clinic room was small and cramped with no sink orcouch. However, the medication was neatly ordered andthere was a separate controlled drugs cabinet. Thechecklists and stock lists for all the drugs and ordering/disposal procedures were up to date and clear. Thefridge was clean and in good working order with fridgeand room temperatures logged on a daily basis. Staffknew what action to take if the temperatures fell out ofthe acceptable range.
• Stocks of medication were full and staff orderedmedication online, which would arrive by courier thesame day if ordered by 10am.
• The ward kept a resuscitation grab bag in the nursingstation. This included oxygen, defibrillator equipment,airways suction equipment and emergency medication.Staff regularly checked the bag for contents andfunction.
• There was easy access up the stairways to the Springswing from Byron ward, enabling patients from bothlocations to move freely between wards. Some Springswing patients had their own fobs, which may haveaffected the security of Byron ward. There had recentlybeen an incident when staff found a patient from theSprings wing in the room of a patient on Byron ward.Following our visit, the hospital manager provided
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
12 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

proposed refurbishment plans that involved relocatingSprings wing to a new unit on the hospital site andwould allow separate entrances for each ward. Therefurbishment work is due to start in the spring of 2016with an aim to be completed in July 2017.
• The entrance to the ward had hand gel dispensers.However, we observed five members of staff enteringthe ward without using the gel.
• The garden fence had only been in place for a year.There had been fewer patients going absent withoutleave as a result but patients were able to climb over thefence quite easily. In the 21 incident reports wereviewed, three involved a patient going absent withoutleave.
Safe staffing
• The senior nursing team on Byron ward comprised award manager, and three charge nurse team leaders.There was one vacancy for a qualified nurse and onevacancy for a healthcare support worker. There was afull-time occupational therapy vacancy at the time ofour visit.
• Medical input consisted of two consultant psychiatristswho dealt with a maximum of nine patients each. Bothhad private admission rights. There was a ward doctorworking three days a week, with a locum ward doctorfor the remaining two days. A duty doctor rota systemoperated from 5pm to 9am and at weekends. Dutydoctors could generally get to the ward within 20minutes.
• There was an easily accessible Cygnet bank workersystem for qualified and unqualified staff. The wardoften needed bank workers because of observationlevels. Bank workers were usually well known havingworked on the ward before. On rare occasions it wasnecessary to use agency staff. The ward providedagency staff with a basic induction. The hospital invitedthe agency to send staff to Cygnet training sessions sothey would know Cygnet policies and procedures whenthe time comes.
• The staff matrix system allowed for a minimum of twoqualified nurses and two healthcare support workers at
any one time. Once the number of patients rose to 17patients this increased to three and five respectively.The ward could use additional staff for one to oneobservation requirements.
• The ward manager said that recruitment was not aproblem but that retention was an issue especially forhealthcare support workers. Seven substantive staff,including five healthcare support workers left the wardbetween 1 September 2014 and 31 August 2015. Theward did not have a strategy in place to address staffretention.
• Staff said that they very rarely cancelled leave becauseof staffing issues. Patients said they could usually taketheir leave.
• Sickness levels on Byron ward from 1 September 2014 to31 August 2015 was 2.3%.
• Staff at Cygnet Harrow were 88% compliant withmandatory training in September 2015. A trainingcoordinator managed training completion using amonthly training report and training matrix.
Assessing and managing risk to patients and staff
• There was no seclusion room on the ward and noreported incidents of seclusion in the past 12 months.The clinical manager said they did not use seclusion onthe ward and they assessed patients based on risk, pasthistory and current presentation and did not admitpatients assessed as being too acutely unwell and whomay require seclusion. Staff managed patients whobecame acutely unwell by using various approachesincluding verbal de-escalation, PRN “as needed”medication and/or increasing the patient’s observationlevel. Staff said they tried to use verbal de-escalationand that there was always a prevention andmanagement of violence and aggression (PMVA)instructor on shift. If a patient required seclusionfacilities, staff liaised with their referring trust to transferthe patient psychiatric intensive care unit (PICU) bedwithin the trust or a private bed. The five patients wespoke with on the ward had not been secluded duringtheir admission.
• Staff said that if necessary they would try to restrain inthe patients’ rooms. If staff had to restrain in a commonaccess area, staff said they would try to lead otherpatients away. Figures provided by the hospital
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
13 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

indicated there were 15 incidents of restraint in the pastsix months, seven prone, of which five required rapidtranquilisation. Observations would always beincreased after restraint and there would be debriefs forstaff. After incidents, staff completed restraint and rapidtranquilisation forms. Restraint records showed thatdoctors completed all necessary observations and thatthey did not last for long periods.
• The ward had a clear a screening process for newreferrals. Staff completed short term assessment of riskand treatability (START) risk assessments on all newpatients.
• The ward had restrictions on bringing illegal drugs andalcohol onto the ward. Staff checked patients’ propertyon arrival. Staff did not remove mobile phones unlessthere was a distinct reason such as patients takingphotos or making nuisance calls. Staff treated laptopcomputers the same way. However, staff did not permitpatients to keep their own chargers.
• Staff said they had a good relationship with the Harrowsafeguarding team. Safeguarding was part of mandatorytraining. Staff said they often did not get to know theoutcome of safeguarding concerns they had raised withoriginating trusts because patients returned to thetrusts.
• Staff responded to emergencies on other wards whenthe alarms were set off. If involved in incidents on theother wards those staff were invited to have a debriefabout the incident.
• Staff used the board in the nursing office to rate patientson a red, amber and green risk basis.
• The provider had appropriate arrangements in place forobtaining medicines. Staff told us how medicines andsupplies were available so patients could have theirmedicines when they needed them. We checked themedicines for 33 patients and saw no medicines wereout of stock.
• The provider stored medication securely. Medicinesrequiring cool storage where stored appropriately andrecords showed that they were kept at the correcttemperature, and so would be fit for use.
• The provider stored and managed controlled drugsappropriately. It was the provider’s policy to store andrecord the use of all benzodiazepines in its register ofdrugs liable for misuse.
• The provider had appropriate arrangements in place forrecording the administration of medicines. Theserecords were clear and fully completed. The recordsshowed patients were getting their medicines whenthey needed them, there were no gaps on theadministration records and any reasons for not givingpatients their medicines were recorded.
• The provider had weekly visits by a pharmacist whochecked staff gave medicines safely to patients andrecorded the administration of medicines correctly. Staffchecked Mental Health Act (MHA) compliance,prescription writing and patient details.
• Medicines in the emergency resuscitation packs were fitfor use. However, none of the wards had any flumazenilinjection available, which is used to reverse the centralsedative effects of benzodiazepines. As lorazepaminjection was used for rapid tranquilisation a riskassessment is required to determine if this should beavailable to treat patients if they experienced respiratorydepression. Staff on Byron ward and Springs unit told usthey would order some from pharmacy that day.
Track record on safety
• The ward manager said that the ward had one seriousassault of a nurse by a patient last year. There were noserious incidents recorded for Byron ward in the last 12months.
Reporting incidents and learning from when things gowrong
• The ward had incident forms, restraint forms and rapidtranquilisation forms readily available for any staffmember to complete. We saw the ward managerchecked these after completion, signed them off andthen monitored by clinical management.
• Cygnet had an internal bulletin on serious incidentsfrom across the wider Cygnet group and also acorporate lessons learned log. The ward managerinvited staff to read serious incident investigationreports and sometimes discussed them in the reflectivepractice group.
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
14 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• We reviewed 21 incident reports going back to May 2015.The ward had seven restraints (four on the samepatient), four prone with one resulting in rapidtranquilisation. The records all matched across thethree books: incidents, restraint records, rapidtranquilisation records. No seclusion was recorded.Three incident forms recorded patients jumping overthe fence and leaving the hospital.
Are acute wards for adults of workingage and psychiatric intensive care unitservices effective?(for example, treatment is effective)
Good –––
Assessment of needs and planning of care
• Patients had a full physical health assessment uponadmission, as evidenced by the care records and staffcontacted the GP for medication reconciliation. Staff cutshort many physical health interventions due topatients being recalled to their home services.
• Sometimes staff had to transfer patients to NorthwickPark Hospital A&E. For example, a patient with breathingproblems was recently taken there. This showed staffaddressed patients’ physical health needsappropriately.
• The ward had a nursing handover at 7.15am and 7.15pmand a multidisciplinary meeting at 9am every weekday.The ward also had a reflective practice group onTuesdays and a community meeting for patients andstaff on Wednesdays. All patients had access to theconsultant psychiatrists twice a week.
• We reviewed nine care records. All had a psychiatricassessment including a brief statement of capacity.Each record contained a START risk assessment butthese often did not contain much information orformulation. All the records contained a medical historyand physical health examination completed inconsiderable detail as well as health of the nationoutcome scale scores. Three of the records includedpatient health questionnaire-9 (PHQ-9) and alcoholproblems questionnaires.
• All the records contained mental health recovery andproblem behaviour care plans. Most of the interventionslisted were common to all the care plans. Thecontinuous written records were legible and detailedand made constant reference to the care plans,providing information about progress towards recoverygoals. In two of the records, staff had not completed theconsent for information sharing form.
• We saw that in one record where there was potential toconsider safeguarding procedures, this was not done.Only two of the care records seemed to contain weeklysummaries or typed ward round notes which could besent to the originating trusts.
• The provider kept all of the patients’ records in paperfiles and not electronically. This meant that informationwas not always easily accessible. Staff said that theywould find an electronic care record more helpful thanthe current hand written system.
Best practice in treatment and care
• A wide range of NICE compliant therapies was availableto patients on the ward. Four psychotherapists offeredsessions including cognitive behaviour therapy (CBT),resourcing, coping strategies work and EMDR (eyemovement desensitisation and reprogramming).
• Staff provided therapy in groups and in one to onesessions.
• The psychotherapist said the discipline was valued andrespected by colleagues. They said that MDT discussionsabout de-escalation and psychological interventionshad led to a reduction in the use of PRN medication onthe ward.
• The psychotherapist facilitated the reflective practicegroup on the ward. This was an open forum for anyonein the team to come and explore issues and shareinformation. For example, the meaning of leastrestrictive practice.
• Staff confirmed that all patients, regardless of whichpart of the country they had come from, were registeredto the local GP.
• The wards completed various audits including patientsatisfaction, health and safety, clinical records,medicines management, infection control, physicalhealthcare and health and safety.
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
15 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published
Skilled staff to deliver care
• The ward had medical, nursing and healthcare supportworker input on the ward. There was very goodpsychology input offering a range of different therapies.
• Staff said that the ward really needed an occupationaltherapist and recruitment was underway for this vacantpost. One patient said that since the OT recently left thatthe ward was quieter during evenings and weekends.
• The ward did not have a social worker and some staffthought it would be useful to have one to help withliaison with community teams as well as taking a leadon safeguarding and mental capacity.
• The ward had a supervision tree and it was clear whosupervised whom. Supervision was supposed to be on amonthly basis and the ward manager said there wasalso a lot of informal supervision. Regular bank workerswere also offered supervision. Although all staff had asigned supervision contract records showed that nostaff had had three supervision sessions during the pastthree months, leaving the ward 100% non- compliantwith the target.
• Nurses and healthcare support worker’s appraisals weresupposed to take place on a yearly basis but many ofthese were overdue for the year.
• A training coordinator created a yearly training plan forclinical and non-clinical staff that included specialistand mandatory training courses.
• Specialty doctors completed annual mandatory trainingan well as in-house training programmes including therecovery star, START assessment. Each doctorcompleted annual appraisals with their supervisingconsultant and regular supervision. Cygnet’s groupmedical director manages the revalidation processcentrally.
Multidisciplinary and inter-agency team work
• We observed an MDT review/ward round. Staffdiscussed five patients in detail. There was an informeddiscussion with good input from all disciplines.
• There were two consultants on the ward and a warddoctor three times a week that provided constant coverduring the week.
• The ward had three psychotherapists and one CBTpsychologist who gave input into the ward and Springswing.
• All staff, including a student nurse and the supportworkers said that the ward operated in amultidisciplinary way and that all clinical backgroundswere respected. All staff said they felt valued membersof an effective team.
• External stakeholders spoke positively about therelationship they had with the hospital, which providedregular updates on patients to them. They told us staffwere professional, communicated effectively andincluded both patients and their family/carers in theirtreatment pathway.
Adherence to the MHA and the MHA Code of Practice
• Eighty nine percent of staff at Cygnet had completedMHA training. The MHA administrator could provideadditional mentoring and support to staff for anyqueries regarding the MHA.
• Staff said they felt confident in using the MHA and werefamiliar with the code of practice.
• There was a clear MHA process flow chart in the wardoffice. Staff said MHA administrator was helpful.
• The board in the ward office indicated a leave status of“Leave Not Recommended” for all informal patients onthe ward which may have impacted upon the way inwhich informal patients’ rights were perceived by staff.
• The T2 and T3 forms were not attached to the drugcharts and were not kept on the ward, which meant thatinformation relating to consent to treatment was notready to hand for staff.
• Sometimes there were disagreements between theHarrow approved mental health practitioner (AMHP)team and the local AMHP teams over who should takeresponsibility for completing patients’ mental healthassessments under the MHA. This had not led topatients being illegally detained, but it did mean thatsome patients were assessed near the end of section 2and section 5.2 time limits.
Good practice in applying the MCA
• Staff said that they felt less confident in the applicationof the Mental Capacity Act (MCA) than the MHA.
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
16 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• One of the consultants said that the ward staff neededmore training on capacity.
• The ward doctor usually completed the consent totreatment part of the psychiatric assessment form uponadmission. However, staff did not regularly follow up onconsent and capacity issues.
• Staff said they had never considered the use ofdeprivation of liberty safeguards (DoLS) on the ward.There were no patients subject to DoLS at the time ofour inspection.
• Staff said that they could obtain advice and guidance onthe MCA from Cygnet’s company solicitors. They alsosaid that the same solicitors provided their MCA training.
Are acute wards for adults of workingage and psychiatric intensive care unitservices caring?
Good –––
Kindness, dignity, respect and support
• We observed several interactions between staff andpatients on the ward and in each case the staff membershowed courtesy and kindness towards the patient. Forexample, a nurse skilfully comforted a patient on one toone observation when she became upset at not beingallowed to leave the ward.
• We observed a community meeting for patients andstaff on Byron ward. During this meeting staff interactedwith patients in a kind and respectful manner, givingthem encouragement and support in articulatingdifficult feelings. Staff showed considerable patienceand an ability to calm an angry patient and offerreassurance.
• All five patients we spoke with said staff were kind,caring and respectful. One patient’s daughter told usthey could call the nursing station anytime to speak withthem. Another patients; family who lived outside ofLondon had come to visit.
The involvement of people in the care they receive
• Patients had access to a Mind advocate once a week onThursdays and staff noted advocacy appointments onthe board in the staff office.
• The regular community meetings afforded patients theopportunity to give feedback about the care they werereceiving and to report any concerns they had withpractical or maintenance issues. Staff made every effortto ensure that these issues were addressed swiftly andthe manager responsible for the upkeep of the buildingattended the community meeting.
• Care plans indicated that staff had made efforts in eachcase to get patient input into the planning process.Sometimes they were not successful but the continuouswritten records detailed attempts to engage the patientsin care planning.
• Patients said staff told them about their medication andwere positive about the activities they accessed. Somepatients were unsure about their discharge plans.
Are acute wards for adults of workingage and psychiatric intensive care unitservices responsive to people’s needs?(for example, to feedback?)
Good –––
Access and discharge
• Byron ward staff tried to respond to all referrals withinone hour. Referrals came through at any time and fromall over the country.
• Demand for beds on Byron was high but patients couldreturn at any time to the referring trust. This led to somedisruption and to staff feeling they were not able tocomplete the recovery journey with patients.
• At the time of our inspection there were ten patients onthe ward. Patients came from trusts around the countryincluding Nottingham, Birmingham, Avon and Wiltshire,Bedfordshire, Cornwall and South London.
• The average length of stay was seven to 10 days.
• Staff expressed some frustration at the frequency withwhich patients were recalled. This meant that recoveryand discharge planning was often cut short by thesudden return of a patient to a bed in their local area.
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
17 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Staff had regular communication with the patients’referring home trust and liaised with bed managers,care coordinators and home treatment teams tomanage discharge. Relatives, carers and carecoordinators were invited to ward round meetings andoccasional staff from the patient’s home Trust’sdischarge team also attended. Staff from the patient’shome Trust’s crisis or home treatment teamcommunicated with the patient prior to discharge. Theward staff faxed discharge notifications to the crisis orhome treatment team and patient’s GP before thepatient was discharged including information abouttheir medication.
The facilities promote recovery, comfort, dignity andconfidentiality
• The ward was clean and comfortable with newfurnishings in evidence.
• There were well-equipped OT rooms, a laundry roomand a multi-faith room just outside the ward.
• The hospital provided meals in the restaurant with tableservice and a choice of food. The kitchen could providefor any dietary requirements. Staff and patients said thefood quality was generally good.
• The ward had a ward pay phone, and patients couldalso ask to use the phone at the nursing station. Therewere also phones in the bedrooms.
Meeting the needs of all people who use the service
• The ward had disabled access including wheelchairaccess.
• Interpreters were readily available, for example aHungarian interpreter was booked for a mental healthtribunal during our inspection.
• Most staff completed training on equality, diversity anddisability.
• Staff said they could help patients to access imams,rabbis and other religious ministers.
Listening to and learning from concerns andcomplaints
• In the past 12 months there had been six complaintsrelating to Byron ward, two of these were upheld.
• There was a complaints leaflet in the folder that staffgave to all new patients. The ward manager said that helooked at all complaints initially and would try toresolve matters swiftly. For example, when a patientwho felt one of the nurses on nights was making toomuch noise, the manager spoke to the nurse and thepatient was satisfied.
• Patients said they knew how to make a complaint andcould raise any concerns in the weekly communitymeetings.
Are acute wards for adults of workingage and psychiatric intensive care unitservices well-led?
Good –––
Vision and values
• Staff were aware that the Cygnet group had recentlybeen taken over by a larger company. They said they feltthe values of the organisation would stay the same andthat they thought these values were about providing ahigh quality and personalised service to all patients.
• Staff said they identified with the hospital more than thewider Cygnet group They did not know the names ofsenior managers in the Cygnet group.
Good governance
• The medical secretaries updated the mandatorytraining record and the ward manager was given amonthly update.
• The hospital’s combined record showed low completionrate for Clozapine Dose Titration, Prescription Writingand Administration Standards and Rapid Tranquilizationcourses.
• The service had an integrated governance meetingevery two months. The agenda for these meetings hadchanged recently. The regular agenda now includedmedication management, risks, restraints, physicalinterventions, security and recent audits.
• Each ward had a recently implemented overarchinglocal action plan (OLAP) that included health and safety,quality network reviews and the service environment.These areas were red, amber and green (RAG) rated,
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
18 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

updated monthly and included recommendations, theaccountable person, resources required and actionplans. Some actions were also allocated to the local riskregister. The hospital manager trained the heads ofdepartments on using the OLAP to ensure informationfiltered down to team meetings.
• Cygnet’s main office completed recruitment includinginterviewing and employment checks. The hospitalmanager could set criteria for shortlisting andparticipated on interview panels. Staff records were upto date including occupational health, references, workpermits, proof of identification and professionalmemberships.
• Cygnet Harrow’s hospital manager reported to theoperations manager, who reported to the organisationschief operating officer. The hospital manager attendedregular meetings with other Cygnet hospital managersfrom other sites for information sharing.
• The quality assurance manager acted as a link betweenthe local governance and corporate governance andcovered eight Cygnet sites across the south west andsouth east of the country.
• Cygnet had an internal bulletin on serious incidentsfrom across the wider Cygnet group and also acorporate lessons learned log. The ward managerinvited staff to read serious incident investigationreports and sometimes discussed them in the reflectivepractice group.
Leadership, morale and staff engagement
• All the staff we spoke with said that they enjoyedworking on the ward and that the team was supportiveand cohesive.
• The morale on the ward was high and all staff felt thatthe team respected them and listened to their views.
• Staff said that they felt they could report any concernsto their managers without fear and that the hospital wascommitted to improving the quality of care on anon-going basis.
• Some staff favourably compared the intimate and familytype atmosphere in the hospital with their experiencesin larger institutions.
• Staff spoke highly of their line managers.
Commitment to quality improvement and innovation
• Therapy staff said they hoped to further develop therange of therapies offered to patients to make Byronward sought after for non-medical interventions.
• Byron ward deferred their AIMS accreditation followingpeer review in November 2014 due to recommendationsmade regarding the fabric of the building, particularlyaround the ligature points. The board approved thisimprovement programme and was currently in progress.
Acutewardsforadultsofworkingageandpsychiatricintensivecareunits
Acute wards for adults of workingage and psychiatric intensivecare units
Good –––
19 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Safe Good –––
Effective Requires improvement –––
Caring Good –––
Responsive Good –––
Well-led Good –––
Are forensic inpatient/secure wards safe?
Good –––
Safe and clean environment
• The Springs unit was over two floors. Staff in the upstairsof the ward, where the bedrooms and lounge werelocated, could observe patients from the nursing stationpositioned to allow observation of the two corridors.The stairwell area was kept locked. The service hadpositioned convex mirrors to allow staff to observe blindspots under the stairs. The service was in the process ofinstalling CCTV. At the time of the inspection, it did notcover all areas of the ward. Staff kept the gym andoccupational therapy room downstairs locked. Staffsupervised patients when they had access to theseareas.
• Staff had completed a ligature audit of the unit inFebruary 2015. The service had been undertaking workto reduce ligatures on the unit. All but one bedroom hadbeen refurbished with new doors and ligature free wetrooms. The service had not refurbished the final room toallow continuity for the patient whose room it was.
• The sensory room had a number of hazards, includingplugs and light fittings. This room was only accessed bypatients under staff supervision.
• The ward had a fully equipped clinic room. Theresuscitation equipment and emergency drugs werekept in a bag in the ward office, which was kept locked.
The bag included two types of ligature cutters. Staffknew where the equipment was kept. Staff checked theequipment regularly and recorded that they had doneso.
• The ward had a seclusion room, which was located atthe end of the main bedroom corridor. It had beenrecently renovated. The room allowed for clearobservation, two-way communication and had toiletfacilities and a clock.
• The service had regular cleaning staff. We sawcompleted daily cleaning checklists completed by stafffor the hospital areas. However, on the day of theinspection there was a strong smell of urine in thesensory room and upstairs corridor.
• Some areas of the ward were cluttered. For example, inthe occupational therapy room there was a wheelchairbeing stored. Staff told us this was for the use of apatient who had been discharged. The gym containedsome unusable items of equipment, including anexercise bike without a seat. The garden contained anumber of deflated footballs.
• Staff completed training in infection control andunderstood their role. 96% of staff had completed themandatory training.
• Cygnet Hospital Harrow was awarded a Food HygieneRating of 5 (Very Good) by London Borough of Harrowon 3 March 2015.
• An anti-bacterial gel dispenser was available outside theentrance to the ward.
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
20 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• At the time of our inspection, the service was in theprocess of installing new doors to ensure it met withguidance following a recent inspection by the LondonFire Brigade.
• All staff and visitors carried personal alarms while on theward.
• The service had completed an audit to ensure that itmet guidance for the security required on a low-secureunit. The ward had a secure perimeter including a fencearound the garden. Everyone entering and leaving theward though the door entered through an air lock. Onemember of staff on all shifts was the designated securitymember of staff.
Safe staffing
• The ward had seven members of nursing staff on a dayshift: three qualified nurses and four healthcareassistants. At night there were four members of nursingstaff: two qualified nurses and two healthcareassistants. In addition to this there was a member ofstaff in charge of security at all times. If one patientrequired enhanced one-to-one observations, this wouldbe done using the set numbers. Should more than onepatient require enhanced one-to-one observations theward would have access to extra staff.
• Between 1 September 2014 and 31 August 2015 theward had a vacancy rate of 11.5%. In August 2015 theward had three registered nurses vacancies. The wardwas using bank workers to cover the vacancies. Between12 May 2014 to 12 August 2015, bank workers covered352 shifts. The unit used bank workers that were familiarwith the ward whenever possible.
• Escorted leave or ward activities were rarely cancelledbecause there were too few staff. Patients told us theycould usually take their leave.
• The ward doctor worked on the ward from Monday toFriday. The consultant visited once a week for the wardround. The ward had an on call rota system for medicalcover at nights and weekends.
• Staff had received appropriate mandatory training,which included training in safeguarding, fire awareness,the recovery approach STAR, and equality and diversity.Most staff were up to date in most courses. The servicehad 87% of staff or more up to date in each course.
Assessing and managing risk to patients and staff
• Staff discussed and updated the risk of patients at dailyhandover. Staff checked patients’ risk prior to accessingleave in the community.
• Staff carried out random patient and room searches.These usually involved asking patients to empty theirpockets and allow staff to see what was in their bags.Staff completed random room checks each week. Theseusually were environmental checks and carried out withthe patient.
• The service updated its policy for ‘The prevention andmanagement of violence and aggression’ in August 2015to reflect recent changes to guidance.
• Staff completed training in using prevention andmanagement of violence and aggression. Staff receivedtraining in promoting safer therapeutic services (PSTS)by Cygnet in-house instructors who are trained underthe auspices, professional codes of practice for WestLondon Mental Health Trust. 100% of staff were up todate with PSTS training.
• Staff documented incidents of restraint in the wardrestraint book. Restraint records were detailed andincluded information on the type of restraint andduration.
• The hospital used the seclusion room for patients fromthe Springs wing that patients accessed through aconnecting door located at the back of Springs unit.
• The service completed monthly audits of restraint whichstaff discussed at their clinical governance meeting.
• Between January and June 2015, staff restrainedpatients 53 times. Five of these incidents had been inthe prone position.
• The provider was ware of recent guidance on reducingthe use of prone restraint and had reviewed this inrecent audits.
• Staff recorded incidents of seclusion in a seclusionbook. Staff had fully completed three out of four recordswe reviewed. One record did not have the time theseclusion finished recorded. Between February and July2015, the ward reported 13 incidents of seclusion. Therewere no incidents of long term segregation reported.
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
21 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Staff completed safeguarding training and most knewhow to raise concerns, although two members of staffwe spoke with were not clear in their answers. 87% ofstaff were up to date with safeguarding adultsmandatory training. The service had raised safeguardingreferrals appropriately with the local authority and CQC.
• The service kept patients’ money locked in the securityroom. Staff recorded all transactions in a book.
• The provider had appropriate arrangements in place forobtaining medicines. Staff told us how medicines theyobtained and supplies were available to enable patientsto have their medicines when they needed them. Wechecked the medicines for 33 patients and saw nomedicines were out of stock.
• The provider stored medication securely. Medicinesrequiring cool storage where stored appropriately andrecords showed that they were kept at the correcttemperature, and so would be fit for use.
• The provider stored and managed controlled drugsappropriately. It was the provider’s policy to store andrecord the use of all benzodiazepines in its register ofdrugs liable for misuse.
• The provider had appropriate arrangements in place forrecording the administration of medicines. Theserecords were clear and fully completed .The recordsshowed patients were getting their medicines whenthey needed them, there were no gaps on theadministration records and any reasons for not givingpatients their medicines were recorded.
• The provider had weekly visits by a pharmacist whochecked staff gave medicines safely to patients andrecorded the administration of medicines correctly. Staffchecked MHA compliance, prescription writing andpatient details.
• Medicines in the emergency resuscitation packs were fitfor use. However, none of the wards had any flumazenilinjection available which is used to reverse the centralsedative effects of benzodiazepines. As lorazepaminjection was used for rapid tranquilisation a riskassessment is required to determine if this should beavailable to treat patients if they experienced respiratorydepression. Staff on Byron ward and Springs unit told usthey would order some from pharmacy that day.
• Patients who staff recorded as being administeredlorazepam injection for rapid tranquillisation hadappropriate documentation on their rapidtranquillisation observation records.
• Children were not allowed onto the ward to visit. If achild visited a patient, they would meet in the meetingrooms elsewhere in the hospital.
• Staff undertook gatekeeping assessments of patientsprior to admission to see whether they meet the criteriafor the unit.
• The ward had some patients with high needs, who werepresenting with difficult to manage behaviours. Anumber of staff raised concerns with us regarding theability of the unit, as a low-secure unit, to meet theneeds of these patients without impacting on otherpatients on the ward.
• Staff undertook risk assessments using the HCR-20V3(Historical clinical risk management–20, version 3) andSTART risk assessment tool. Staff had completed andupdated these assessments in all six files we reviewed.Staff had completed risk assessments in all six patientfiles we reviewed.
• The psychology department took the lead on HCR-20V3risk of interpersonal violence assessment reports uponpatient admission. Staff updated these whenever anincident occurs, other than that they are reviewed everysix months in line with patients’ care programmeapproach (CPA).
• Patients had regular set times when they would have acigarette. Staff closed the downstairs of the wardfollowing the final break at 10pm.
• Patients could use mobile phones on the ward.
Track record on safety
• The ward had two serious incidents requiringinvestigation in the last 12 months. One of these waswith regards to an allegation by one patient againstanother and the other with regards to violence on theward.
Reporting incidents and learning from when things gowrong
• All staff knew how to report an incident using theservice’s incident reporting system. Most staff knew of
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
22 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

what constituted a reportable incident. However, somestaff were not clear on what constituted a reportableincident. Some staff referred to incidents involvingpatients, which they had not reported. For example,when a patient locked a member of staff in their room.
• After staff completed an incident form, they entered itonto the corporate computer system. In the threemonths from 1 July 2015 to 30 September 2015 therehad been 32 incidents reported on the Springs Unit.
• Staff were aware of the need to be open and transparentand explain to patients when things went wrong.
• Staff received feedback form incidents in monthly teammeetings. Overviews and clinical governance meetingminutes were also available on the shared drive.
• Staff were offered feedback after incidents and met todebrief. However, some staff noted that following arecent incident on Springs wing, this had not takenplace for a week.
Are forensic inpatient/secure wardseffective?(for example, treatment is effective)
Requires improvement –––
Assessment of needs and planning of care
• Staff completed appropriate assessments on physicaland mental health after admission. Followingadmission, staff completed an initial nursingassessment and more detailed care plans.
• Occupational therapists completed occupationalself-assessment (OSA) and Model of human occupationscreening tool (MOHOST). Where appropriate, theywould also complete kitchen, road safety and sensoryassessments.
• If a patient did not have a formal medical diagnosis,staff completed ‘Autism Diagnostic ObservationSchedule’ and ‘Autism Diagnostic Interview-Revised’assessments.
• Staff had not completed some records monitoringpatients’ weight and vital observations. Staff told us thiswas due to patients not being available or refusing. On
one record, staff had not updated monitoring a patient’sweight since July. Prior to this they had refused. Noassessment had been made of their capacity to makethis decision.
• Staff produced a range of care plans for each patientcovering the holistic needs of patients. This includedcare plans for ‘my mental health problems’,’ stopping myproblem behaviours’, ‘getting insight’, ‘my life skills’, ‘myrelationships’, and ‘staying healthy’.
• All six care records we reviewed were personalised tothe individual patient’s needs.
• Five out of the six care records were up to date andshowed a range of care plans to meet identified needs.However, for one person the plans were not clear whatthe goal of the admission was and how they weresupporting the person’s recovery.
• Each patient had an identified keyworker. The servicehad an expectation that the keyworker would meet thepatient for a one-to-one discussion at least weekly andrecord this in the patients care files. In all the care fileswe reviewed there were few records of formalone-to-ones. For example, one patient only had tworecorded and another had none.
• The provider stored patients’ care records in paper filesand locked these in the ward office. Some staff told usthey found it difficult to locate information on the paperfiles. When staff updated care plans, they printed a copyand placed it in the patient’s file.
Best practice in treatment and care
• Staff offered a range of psychological therapiesrecommended by NICE guidelines including cognitivebehavioural therapy (CBT), mindfulness and dialecticalbehavioural therapy (DBT).
• The patients had access to health checks. Where ahealth check identified that a patient required physicalhealthcare the patient was then referred to the local GP.Staff confirmed that all patients, regardless of whichpart of the country they had come from, were registeredto the local GP. Staff made appropriate referrals tophysical health specialists.
• Staff completed health of the nation outcome scales forpatients upon and throughout admission to measureoutcomes.
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
23 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• The wards completed various audits including patientsatisfaction, health and safety, clinical records,medicines management, infection control, physicalhealthcare and health and safety.
Skilled staff to deliver care
• The ward had a range of mental health disciplinesproviding input. This included a ward doctor, anoccupational therapist, nursing staff and assistantpsychologists. A clinical psychologist, a consultantpsychiatrist and a pharmacist also spent time on theward.
• The ward did not have a social worker and was in theprocess of recruiting for a vacant gym instructorposition.
• Staff received regular supervision. The manager told usthey aimed to have formal supervision every four weeks.Ninety three percent of staff had received formalsupervision in the month before the inspection.
• Ninety-three percent of staff had received a formalappraisal in the previous year.
• The ward had staff meetings. The ward aimed to havethese once a month, although staff had no teammeeting in July and August 2015.
• Staff had only received limited specialist training inlearning disabilities, autistic spectrum disorder andautism. The clinical psychologist had recently provideda half-day session on autistic spectrum disorderawareness and management to improve staffknowledge. However, five members of staff told us theydid not feel the training was sufficient for staff withoutprior experience or knowledge. Bank staff said they hadnot completed any autism training. Some staff hadcompleted autism diagnostic observation schedule(ADOS) training externally. However, the majority ofthese staff included doctors, OTs and psychologists.Only one qualified nurse completed this training.Previous autism training records were dated from 2007 –2010.
• Specialty doctors completed annual mandatory trainingan well as in-house training programmes including therecovery star, START assessment. Each doctorcompleted annual appraisals with their supervisingconsultant and regular supervision. Cygnet’s groupmedical director manages the revalidation processcentrally.
Multidisciplinary and inter-agency team work
• Staff from all professional backgrounds felt othermembers of the team respected their views.
• The ward held a weekly ward round when the MDT metto discuss patients. Staff from a range of professionalbackgrounds attended this. In the meeting we observedall staff could offer their professional perspective andview.
• Staff conducted a handover between shifts, which theyrecorded. Some staff told us they felt thatcommunication could be improved between the team.
• External stakeholders spoke positively about therelationship they had with the hospital, who providedregular updates on patients. They told us staff wereprofessional, communicated effectively and includedboth patients and their family/carers in their treatmentpathway.
Adherence to the MHA and the MHA Code of Practice
• Eighty seven percent of the staff on the ward hadcompleted their training in the MHA. The MHAadministrator could provide additional mentoring andsupport to staff for any queries regarding the MHA.
• Staff completed consent to medication forms.• Staff recorded dates for patients S132 rights to ensure
staff remembered when to repeat them.• Staff filled in detention paperwork correctly. All patients
had their legal status, and dates for renewal, recorded.• Staff made referrals to second opinion appointed
doctors where appropriate.• An advocate visited the ward every Thursday, or at other
times if requested.• Cygnet Hospital Harrow maintained a database on
patients’ MHA details including their MHA status, date ofsection and expiry, consent to treatment and dates oftribunals and hearings. The provider had an integratedgovernance and integrated audit meetings every othermonth that included monitoring MHA compliance. All ofCygnet’s MHA administrators met at MHA governancemeetings twice a year to evaluate current practices anddiscuss updates to the MHA.
Good practice in applying the MCA
• Although staff completed training in the MCA, theirknowledge of the MCA was variable. It was not always
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
24 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

clear how they were supporting patients to makerelevant decisions. Staff had not always recorded thatthey had assessed an individual’s capacity to make adecision when it had been necessary to do so.
• We saw a completed capacity assessment for a patientregarding budgeting and managing their own money.
• Staff said that they could obtain advice and guidance onthe MCA from Cygnet’s company solicitors. They alsosaid that the same solicitors provided their MCA training.
Are forensic inpatient/secure wardscaring?
Good –––
Kindness, dignity, respect and support
• Staff discussed patients in a respectful manner, forexample during the MDT ward round which weobserved.
• We observed staff interacting in a friendly andprofessional way with patients.
• The six patient we spoke with said that staff were politeand kind and that they felt happy on the ward and withthe activities they accessed in the community.
The involvement of people in the care they receive
• Patients received an information guide when theyarrived on the ward.
• Staff invited patients to attend ward round meetings.• Staff sought to involve patients in developing care plans.
All six care files showed some patient involvement intheir development. Most patients had signed their careplans.
• The ward had a carer’s group that met on a quarterlybasis. Carers of patients on the ward were positiveabout the care the patients received and the staffing.Most felt involved in the patient’s care, although onecarer said that communication from staffing could beimproved.
• Where appropriate, staff involved families and carers inpatients’ care. For example, during the MDT ward roundstaff contacted a relative of a patient who was involvedin their care.
• The ward held regular community meetings everyMonday morning. The most recent meeting gavepatients an opportunity to discuss advocacy, cateringand housekeeping.
• Staff involved patients in devising new menus anddecisions regarding the decoration on the wardincluding the sensory room.
Are forensic inpatient/secure wardsresponsive to people’s needs?(for example, to feedback?)
Good –––
Access and discharge
• NHS England place patients in the unit. The placementscame from all over southern England, including Kent,London, Devon and Wessex areas. Following a referral tothe Unit staff completed a gatekeeping assessmentwithin two weeks to see whether the person wasappropriate for the unit. However, four members of stafftold us they felt that some patients had too high needsfor the unit. They told us this affected their ability tomeet the needs of the patients. For example, staff hadbeen required to maintain one-to-one observations forone patient for over two months.
• Of the 14 patients on the ward, three had been admittedto the ward in 2011 or earlier. The Unit had admitted 10patients since 2014. Staff completed CPA reviews anddiscussed discharge planning at MDT reviews.
• When the service had agreed funding with a person’slocal clinical commissioning group (who fund non-lowsecure care) and it was appropriate, patients had movedto the less-restrictive Springs Wing. Other patientsmoved to units nearer their home area.
• In the six months prior to the inspection there was onedelayed discharge from the unit. This was due to lack ofsuitable local community facility for the patient.
• The bed occupancy on the unit was 100%.• Staff had regular communication with the patients’
referring home trust and liaised with bed managers,care coordinators and home treatment teams tomanage discharge. Relatives, carers and carecoordinators were invited to ward round meetings andoccasional staff from the patient’s home Trust’sdischarge team also attended. Staff from the patient’s
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
25 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

home Trust’s crisis or home treatment teamcommunicated with the patient prior to discharge. Theward staff faxed discharge notifications to the crisis orhome treatment team and patient’s GP before thepatient was discharged including information abouttheir medication.
The facilities promote recovery, comfort, dignity andconfidentiality
• The main entrance to the upstairs of the ward wasthrough the main bedroom corridor. At the time of theinspection, one patient was being nursed on one-to-oneobservations. This meant staff sat outside his door. Thisdid not allow for privacy or dignity as other patients andvisitors to the ward had to pass the open door.
• The ward board, displaying the names of patients andother details regarding them was in the ward office.However, other patients could view patients’ detailsthrough the door.
• The ward was not autism friendly. The ward did nothave visual signs to help people around the ward. Therewas one small sensory room, which had someequipment. Staff told us they found it difficult to supportsome patients with autistic spectrum disorder becausethe layout of the ward made it difficult to reduce noise.
• The ward had an occupational therapy room, whichincluded a kitchen. The ward also had a sensory roomand two other rooms were patients could meet peoplein privacy.
• The ward had an activity room, which was also the gym.This room contained a pool table and some gymequipment. However, at the time of the inspection theroom was not fully in use due to ward renovations.
• There was a computer room with two computers, whichpatients could access with staff for supervised internetaccess.
• The ward had a telephone that patients could use.• The patients had access to a large garden to the rear of
the ward.• Most patients told us they felt the food was good.• Patients could personalise their bedrooms with their
own possessions.• The ward had a central locked cupboard where patients
could store their possessions. securely. Patients alsohad their own lockers. Staff risk assessed whetherpatients could have their own key to lock theirbedrooms. Staff could lock their bedroom doors.
• Patients had access to a range of therapeutic activitiesincluding daily relaxation sessions, art club once aweek, pet therapy twice a week and library trips. Somepatients also completed one-to-one cooking sessionsand swimming sessions.
• Four members of staff told us they felt the main way theward could improve would be by offering moreeducational opportunities for the patients.
Meeting the needs of all people who use the service
• The service had produced some information inaccessible formats. For example, one patient had apictorial plan regarding his expressed plan of movingon.
• The service could provide food that met religious needs,such as being halal.
• The ward had a prayer room. Staff completed a careplan regarding the spiritual needs of patients. A chaplainwould visit the ward if requested.
Listening to and learning from concerns andcomplaints
• Patients knew of how to complain and give feedback.Staff responded to minor individual concernsappropriately.
• In the last year, the Springs unit had received twocomplaints. Staff had investigated and responded tothese appropriately.
Are forensic inpatient/secure wardswell-led?
Good –––
Vision and values
• Staff identified ‘helpful, respect, empathetic’ as valueswhich are in line with organisation’s values.
Good governance
• The ward completed regular audits in case notes andcare plans.
• The service had an integrated governance meetingevery two months. The agenda for these had changedrecently. The regular agenda now included medicationmanagement, risks, restraints, physical interventions,security and recent audits.
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
26 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Each ward had a recently implemented overarchinglocal action plan (OLAP) that included health and safety,quality network reviews and the service environment.These areas were red, amber and green (RAG) rated,updated monthly and included recommendations, theaccountable person, resources required and actionplans. Some actions were also allocated to the local riskregister. The hospital manager trained the heads ofdepartments on using the OLAP to ensure informationfiltered down to team meetings.
• Cygnet’s main office completed recruitment includinginterviewing and employment checks. The hospitalmanager could set criteria for shortlisting andparticipated on interview panels. Staff records were upto date including occupational health, references, workpermits, proof of identification and professionalmemberships. The ward had experienced a highturnover of staff in the previous year and did not have astrategy in place to address staff retention.
• Cygnet Harrow’s hospital manager reported to theoperations manager, who reported to the organisationschief operating officer. The hospital manager attendedregular meetings with other Cygnet hospital managersfrom other sites for information sharing.
• The quality assurance manager acted as a link betweenthe local governance and corporate governance andcovered eight Cygnet sites across the south west andsouth east of the country.
Leadership, morale and staff engagement
• Staff felt well supported by management and felt thatthe ward team worked well together. They felt respectedby other staff members. Most staff told us that they feltthe morale of the team was good.
• Staff felt they would be able to raise a concern shouldthey have one.
• The Springs unit had a sickness rate of 1.5% between 01September 2014 and 31 August 2015.
• Staff were able to feed their views back through thesurvey of staff conducted by the provider.
• The hospital had a whistleblowing policy and “speakout” helpline staff could access. One incident of bullyinghad been investigated appropriately.
Commitment to quality improvement and innovation
• The Springs unit is a member of the Royal College ofPsychiatry Quality Network for forensic mental healthservices.
Forensicinpatient/securewards
Forensic inpatient/secure wards
Good –––
27 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published
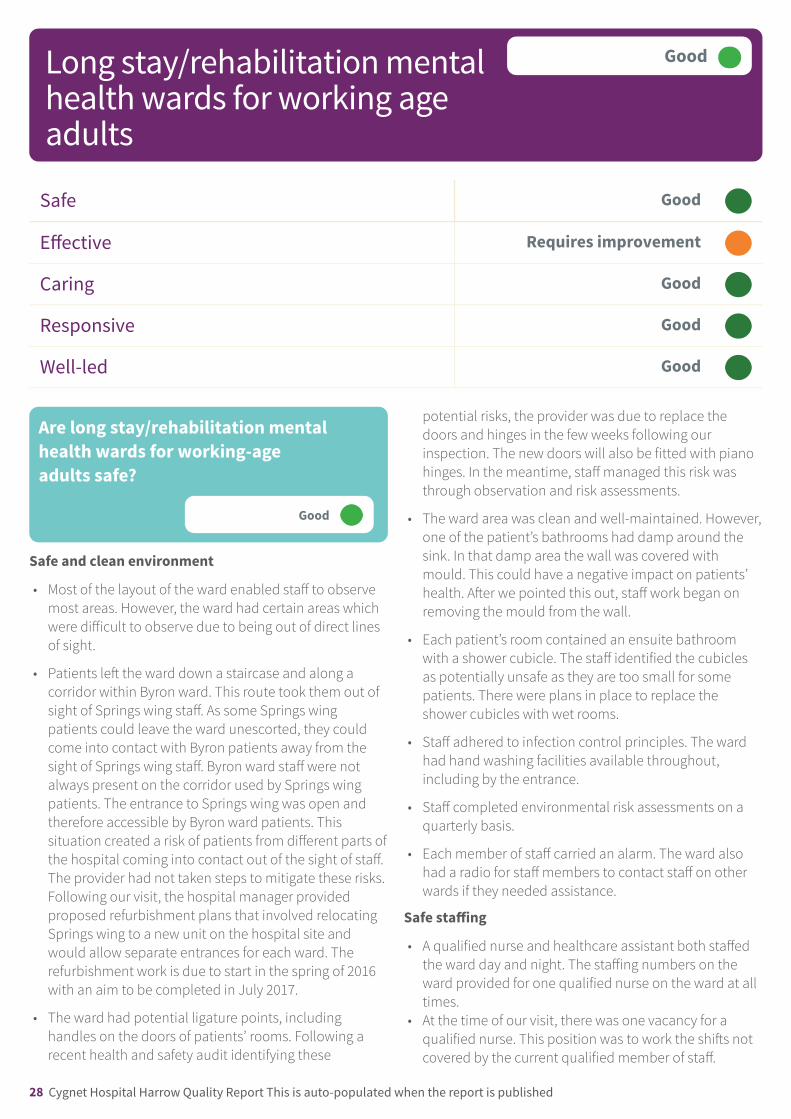
Safe Good –––
Effective Requires improvement –––
Caring Good –––
Responsive Good –––
Well-led Good –––
Are long stay/rehabilitation mentalhealth wards for working-ageadults safe?
Good –––
Safe and clean environment
• Most of the layout of the ward enabled staff to observemost areas. However, the ward had certain areas whichwere difficult to observe due to being out of direct linesof sight.
• Patients left the ward down a staircase and along acorridor within Byron ward. This route took them out ofsight of Springs wing staff. As some Springs wingpatients could leave the ward unescorted, they couldcome into contact with Byron patients away from thesight of Springs wing staff. Byron ward staff were notalways present on the corridor used by Springs wingpatients. The entrance to Springs wing was open andtherefore accessible by Byron ward patients. Thissituation created a risk of patients from different parts ofthe hospital coming into contact out of the sight of staff.The provider had not taken steps to mitigate these risks.Following our visit, the hospital manager providedproposed refurbishment plans that involved relocatingSprings wing to a new unit on the hospital site andwould allow separate entrances for each ward. Therefurbishment work is due to start in the spring of 2016with an aim to be completed in July 2017.
• The ward had potential ligature points, includinghandles on the doors of patients’ rooms. Following arecent health and safety audit identifying these
potential risks, the provider was due to replace thedoors and hinges in the few weeks following ourinspection. The new doors will also be fitted with pianohinges. In the meantime, staff managed this risk wasthrough observation and risk assessments.
• The ward area was clean and well-maintained. However,one of the patient’s bathrooms had damp around thesink. In that damp area the wall was covered withmould. This could have a negative impact on patients’health. After we pointed this out, staff work began onremoving the mould from the wall.
• Each patient’s room contained an ensuite bathroomwith a shower cubicle. The staff identified the cubiclesas potentially unsafe as they are too small for somepatients. There were plans in place to replace theshower cubicles with wet rooms.
• Staff adhered to infection control principles. The wardhad hand washing facilities available throughout,including by the entrance.
• Staff completed environmental risk assessments on aquarterly basis.
• Each member of staff carried an alarm. The ward alsohad a radio for staff members to contact staff on otherwards if they needed assistance.
Safe staffing
• A qualified nurse and healthcare assistant both staffedthe ward day and night. The staffing numbers on theward provided for one qualified nurse on the ward at alltimes.
• At the time of our visit, there was one vacancy for aqualified nurse. This position was to work the shifts notcovered by the current qualified member of staff.
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
28 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• In order to maintain one qualified member of staff onthe ward, the ward regularly employed a qualified banknurse. The ward never used agency staff. In the eventthat management could not obtain a qualified banknurse, they would move a qualified nurse to the wingfrom another part of the hospital.
• In the previous 12 months the sickness rate for qualifiednurses was 8.5%. For unqualified staff the sickness ratewas 5%. In the previous 12 months one staff memberhad left the ward.
• The provider calculated staffing levels according to whathad been historically used on the ward and used astaffing matrix based on patient numbers.
• The ward employed bank workers wherever possiblethat had worked on the ward before to ensurecontinuity of care for patients.
• The ward manager was also the manager for Springsunit. This meant they could adjust staffing levels asrequired by moving the staff between the two wards.This was sometimes necessary where extra staff wererequired on the wing to facilitate activities such asescorting patients out into the community. Staffplanned these activities to ensure the manager couldmake the necessary staff adjustments. However,another staff member told us that it was common forplanned activities to be cancelled because there werenot always enough staff to escort patients from the wardout into the community. There was no informationavailable as to how many activities the ward cancelled.However one staff member said this was a commonoccurrence. Planned activities are an important part ofpatients’ rehabilitation. Therefore frequent cancellationof activities could potentially undermine patients’rehabilitation. Patients told us that their leave was notcancelled because of staff shortage, although the timeof was sometimes changed for this reason. Howevermost leave from the wing was unescorted.
• A qualified nurse was often present in the communalareas of the wing, but this was not the case at all times.This was because staff were sometimes involved inother duties.
• Staff told us that there were enough staff on the wing toensure that patients had regular 1:1 time with theirnamed nurse. Patients confirmed they regularly spenttime with their nurse.
• If physical interventions were required on the ward, staffused the panic alarm system to summon assistancefrom other wards of the hospital. All staff on the ward,including the manager, had completed physicalrestraint training.
• Out of 26 mandatory training courses, staff hadcompleted 24. In the remaining two courses forClozapine Dose Titration and Prescription Writing thecompletion rate was 50% for one member of staff.
Assessing and managing risk to patients and staff
• In the past six months, no patients had been inlong-term segregation or seclusion. During this time,staff restrained four patients. None of these restraintswas in the prone position. Staff had not used rapidtranquilisation. There was no seclusion unit on theward. If a patient experienced a significant deteriorationin their mental health, they could be transferred to thelow-secure unit adjacent to the ward.
• Staff completed risk assessments after every incidentand updated the patient’s risk profile.
• Staff used two recognised risk assessment tools. Thefirst was the short term assessment of risk andtreatability (START) risk assessment. Staff used this toolto assess all the patients on the ward. In the eight riskassessments we looked at, all were fully completed andthe information carried over into each patient’s careplan. This was in order to plan how to manage anddecrease the risk for each patient. For example, one riskassessment identified that a patient was at risk of self-neglect. Staff recorded this risk in the patients’ care planalong with steps as to how staff would support greaterinsight and self-care. The second risk assessment toolthat staff used was historical, clinical risk assessment(HCR-20). This was not used in every case and onlywhere patients had a history of violence and aggression.These were properly completed and the informationtranslated to the patients’ care plans.
• Staff told us that informal patients were free to leave atwill. Informal patients confirmed this. Staff also gaveinformal patients a leaflet detailing their rights and howstaff would treat them while on the wing. The patientand a nurse signed this leaflet. The leaflet said thatinformal patients could only leave the hospital grounds‘with the consent and agreement of the nursing staff/responsible Clinician’. There was a risk that by providinginformation in this form, informal patients may not befully aware of their rights to leave the hospital at will
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
29 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Staff used verbal de-escalation techniques prior torestraining patients.
• In the past 12 months, staff had not put any patientsinto seclusion or given any patients rapidtranquilization.
• Staff training records showed that all staff members hadcompleted their mandatory safeguarding training andwere up to date with mandatory refresher courses. Staffdemonstrated a good knowledge of safeguardingprocedures.
• The ward did not permit child visitors. Patients couldsee child visitors away from the ward in another part ofthe building.
• The provider had appropriate arrangements in place forobtaining medicines. Staff told us how medicines theyobtained and supplies were available to enable patientsto have their medicines when they needed them. Wechecked the medicines for 33 patients and saw nomedicines were out of stock.
• The provider stored medication securely. Medicinesrequiring cool storage where stored appropriately andrecords showed that they were kept at the correcttemperature, and so would be fit for use.
• The provider stored and managed controlled drugsappropriately. It was the provider’s policy to store andrecord the use of all benzodiazepines in its register ofdrugs liable for misuse.
• The provider had appropriate arrangements in place forrecording the administration of medicines. Theserecords were clear and fully completed .The recordsshowed patients were getting their medicines whenthey needed them, there were no gaps on theadministration records and any reasons for not givingpatients their medicines were recorded.
• The provider had weekly visits by a pharmacist whochecked staff gave medicines safely to patients andrecorded the administration of medicines correctly. Staffchecked MHA compliance, prescription writing andpatient details.
• On Springs wing, the ward manager said nursing stafflabelled and dispensed to take away medicines for
patients to use on weekend. This did not comply withthe provider’s medication management policy whichstated all leave medicines from should be ordered fromthe pharmacy.
• Medicines in the emergency resuscitation packs were fitfor use. However, none of the wards had any flumazenilinjection available, which is used to reverse the centralsedative effects of benzodiazepines. As lorazepaminjection was used for rapid tranquilisation a riskassessment is required to determine if this should beavailable to treat patients if they experienced respiratorydepression. Staff on Byron ward and Springs unit told usthey would order some from pharmacy that day.
• Patients who staff recorded as being administeredlorazepam injection for rapid tranquillisation hadappropriate records on their rapid tranquillisationobservation charts.
Track record on safety
• There were no serious incidents recorded on the wing inthe past 12 months. Staff recorded one adverse eventwhen a patient had gone absent without leave.
Reporting incidents and learning from when things gowrong
• Staff demonstrated a good knowledge of how to reportincidents that took place on the ward. We saw oneexample of this where a detained patient had left theward without permission, before returning two hourslater with police. Staff had fully documented thisincident with action plans put in place to prevent afurther occurrence.
• Management on the wing told us that they gave staffinformation from incidents handovers, ward rounds anddebriefings following incidents. Staff we spoke toconfirmed this happened. However, staff also said that areflective practice meeting that used to take place overa year ago no longer happened.
Are long stay/rehabilitation mentalhealth wards for working-ageadults effective?(for example, treatment is effective)
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
30 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Requires improvement –––
Assessment of needs and planning of care
• Staff told us that they assessed each patient for risk andtheir care needs upon admission to the wing. However,it was not always possible to see what actions had takenplace on a patient’s admission as staff archived oldercare plans. Of the eight patient files we saw allcontained risk assessments that staff completed uponthe admission of the patient.
• We looked at eight patients’ records. Staff recordedwhere they had examined patients’ physical health.However, staff had not done this in a systematic orregular way. Staff said that all patients received aphysical examination on a weekly basis by the warddoctor. In three of the eight records there was noindication that this had happened.
• Patient care plans were detailed with multipleobjectives with a recovery focus. All the plans that wesaw had indications of patient involvement. Suchobjectives included addressing mental health recovery,making feasible plans, developing relationships andstaying physically healthy. For example one care plan ofa patient with a history of shouting and biting detailedhow staff planned to speak softly and calmly at all timesto encourage calmer behaviour. The plan also detailedhow staff planned to remove the patient from othersduring incidents of anxiety and offer therapies at thesame time.
• The ward kept patient files on paper but notelectronically. These paper files did not hold all theinformation about the patient. This was because fromtime to time staff removed and archived older records.The archived files were held in a different part of thebuilding.
Best practice in treatment and care
• The patients had limited access to health checks. Wherea health check identified that a patient requiredphysical healthcare the patient was then referred to thelocal GP. Staff confirmed that all patients, regardless ofwhich part of the country they had come from, wereregistered to the local GP. However, staff admitted thatthey did not automatically address health concerns
raised by health checks. They gave two examples. In thefirst they referred a patient with repeated very highblood pressure a local GP who declined to prescribe anytreatment. In this case, staff decided that they wouldwrite to the GP to raise their continuing concerns, butwould not give any physical health treatmentthemselves. In the second case, a patient withcontinuing high cholesterol was similarly referred to aGP because the ward doctor was not confident inprescribing any treatment.
• Psychology sessions aimed to give patients an insightinto their illness and strategies for coping with theirsymptoms. Psychology also provided sessions in angermanagement and cognitive behavioural therapy.
• The wards completed various audits including patientsatisfaction, health and safety, clinical records,medicines management, infection control, physicalhealthcare and health and safety.
Skilled staff to deliver care
• A range of professionals were available to supportpatients on the wing. This comprised of a qualifiednurse, an occupational therapist and a ward doctor whoworked solely on the wing. In addition a psychologist, asocial worker and a pharmacist visited the wing toprovide additional support.
• Staff confirmed that they received supervision every fourto six weeks and described this as helpful andsupportive. Staff also received clinical supervision whenrequired and a yearly appraisal. However, reflectivepractice was not currently available for staff. A reflectivepractice meeting has not taken place for staff on thewing for over a year. The minutes of the staff meeting inSeptember showed that they mostly discussed staffadministration.
• The nurses and healthcare support workers did nothave a specialist background in autism. The clinicalpsychologist had recently provided a half-day sessionon autism spectrum disorder awareness andmanagement to improve staff knowledge. The nursereceived this training only after two and a half years onthe ward, although during this period receivedmentorship from a nurse experienced in autism. Somehospital staff had completed autism diagnosticobservation schedule (ADOS) training externally.
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
31 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

However, the majority of these staff included doctors,OTs and psychologists. Only one nurse completed thistraining. Previous autism training records were datedfrom 2007 – 2010.
• Specialty doctors completed annual mandatory trainingan well as in-house training programmes including therecovery star, START assessment. Each doctorcompleted annual appraisals with their supervisingconsultant and regular supervision. Cygnet’s groupmedical director manages the revalidation processcentrally.
Multidisciplinary and inter-agency team work
• Daily handovers took place between day and night staff.Information passed between the staff concerning thepatients was detailed in the patients’ notes.
• Staff described that they work effectively with theoutside agencies, including the local authority, policeand GP services to support patients on the wing.However, there was no available evidence to indicatethe effectiveness or otherwise of such relationships.
• External stakeholders spoke positively about therelationship they had with the hospital, which providedregular updates on patients to them. They told us staffwere professional, communicated effectively andincluded both patients and their family/carers in theirtreatment pathway.
Adherence to the Mental Health Act (MHA) and theMHA Code of Practice
• 100% of the staff on the ward had completed theirtraining in the MHA. However, the information leafletgiven to informal patients regarding their right to leavethe hospital showed that informal patients may not befully aware of their right to do so.
• We found staff ensured patients understood theprovisions of the MHA that applied to them and theirrights to appeal to the tribunal when under the MHA andwhen their section was renewed. We did not findevidence that this was carried out on other occasions.
• Staff said they informed all patients of their rights underthe MHA and documented this in patients’ files.However, the three files we inspected did not all containa record of patients being given their rights. One patientwe spoke to confirmed staff told them their rights.
• Patients had access to an advocate who visited the wardregularly. The advocate confirmed that staff weresupportive of advocacy and regularly referred patientsrequiring support to the advocacy service.
• We found that assessments of capacity to consent totreatment were not carried out on a regular, systematicbasis.
• There was a patient whose medication change waswaiting to be authorised by a second-opinion appointeddoctor. The required paperwork was not completed in away that complied with the MHA.
• The MHA administrator could provide additionalmentoring and support to staff for any queries regardingthe MHA.
• Cygnet Hospital Harrow maintained a database onpatients’ MHA details including their MHA status, date ofsection and expiry, consent to treatment and dates oftribunals and hearings. The provider had an integratedgovernance and integrated audit meetings every othermonth that included monitoring MHA compliance. All ofCygnet’s MHA administrators met at MHA governancemeetings twice a year to evaluate current practices anddiscuss updates to the MHA.
Good practice in applying the MCA
• All staff completed training in the MCA and coulddescribe the five principles of the MCA.
• The staff had not made any applications for Deprivationof Liberty Safeguards in the past 12 months.
• Staff on the ward knew of the policy developed byCygnet relating to the MCA. Reading the MCA is part oftheir mandatory training. It was also available for staff toread on the staff database.
• Staff said that they could obtain advice and guidance onthe MCA from Cygnet’s company solicitors. They alsosaid that the same solicitors provided their MCA training.
Are long stay/rehabilitation mentalhealth wards for working-ageadults caring?
Good –––
Kindness, dignity, respect and support
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
32 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Staff treated patients in a kind and respectful manner.For example, one nurse spoke at length with a patientabout their future education and career plans andproviding advice as to how to reach those goals.
• Patients said that staff treated them in a respectful wayand cared for their health and dignity. Patient spokepositively about their experiences of being on the ward.
• Staff showed an understanding of how they shouldspeak to and care for patients. Each patient’s file had acommunication protocol detailing how staff shouldinteract with patients.
The involvement of people in the care they receive
• The patients received a detailed booklet uponadmission to the ward describing the support theycould receive as well as summarising their rights. Theguide included information about the purpose androutines of the ward, who the key members of staffwere, details of the treatment that is offered, a list ofactivities available, and details of how to complainabout the service and how to contact the CQC.
• The majority of care plans evidence patient involvementand gave clear indications of patient desires andconcerns. The two patients we spoke to confirmed thatthey had regular involvement in their care planning.
• The ward advertised the mental health advocacy serviceon the patient notice board on the ward. The advocateconfirmed that they regularly supported patients with arange of issues on the ward. This included attendingward rounds where they supported patients to ask forleave or to raise issues in relation to discharge. Onepatient said he was frustrated by the difficulties theyhad contacting their social worker and commissioningauthority to progress the arrangements for his dischargeand return to his home area.
• The ward held a weekly community meeting for patientsto discuss issues of concern and to receive informationfrom staff. The patients confirmed this meeting could beuseful and said that staff always reminded patients inthese meetings that they could make a complaint.
• Patients told us about groups and activities includingcookery, art groups, creative writing groups and acultural awareness group. One patient said that he hadleave each week to attend a college where he wasstudying a maths course with a view to going to
university. One patient said that he would like there tobe more activities at weekends because there was a lotof sitting around and that time went very slowly whenthere was nothing to do.
• Patients spoke positively about leave to the community.They told us about regular trips with small groups ofpatients to the local shops and trips out for coffee. Onepatient enjoyed going bowling.
• Patients felt involved in decisions about their care andtreatment which mainly took place through discussionswith their doctor at ward rounds. Patients also felt thatthe care and treatment they received was helpful tothem in managing the effects of their autistic spectrumdisorder. One patient said that staff prompted him tohave a shower and to shave, which he would oftenforget to do. Another patient said that their discussionswith their psychologist had given them a much betterunderstanding
Are long stay/rehabilitation mentalhealth wards for working-ageadults responsive to people’s needs?(for example, to feedback?)
Good –––
Access and discharge
• The average bed occupancy rate in the past six monthswas 90%.
• Either the NHS or the local Clinical CommissioningGroup funded all beds on the wards. None of the bedswere privately funded or were contracted out at the timeof our visit.
• A bed was always available for a patient when theyreturned from leave. This was because of therehabilitation nature of the ward. Staff always plannedadmissions well in advance so there were never anycases of a lack of beds. The ward did not provide foremergency admissions.
• Staff did not move patients between wards onadmission. With rehabilitation the plan was always toadmit the patient and remain on the ward until theywere ready for discharge.
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
33 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• Staff always planned discharges well in advance as partof a patient’s transition plan, to take place during theday.
• Emergency beds were available in other parts of thelocation in the event of a patient becoming unwell.
• Discharge for some patients on the ward was sometimesdelayed, mostly because of housing problems. Theaverage delay for this reason was two months.
• A typical length of stay on the ward was about two years.Patients were usually discharged to supported living inthe community.
The facilities promote recovery, comfort, dignity andconfidentiality
• The ward had a variety of facilities for patients. Thisincluded a therapy room, an occupational therapyroom, a lounge, a kitchen with patient washing facilitiesand a computer area. The kitchen was fully equippedand patients were encouraged to do their own washing.In the lounge there was a television, a DVD player withDVDs and a games console with games. The ward had acomputer with a printer for the patients to use. Allequipment was in working order.
• There was no dedicated room on the wing for patientsto meet visitors. Private rooms were available on theground floor for this purpose.
• Patients could keep and use their own mobile phoneson the ward for making private calls.
• The hospital had two gardens for patients to use. Theone beside the ward was relatively large andwell-maintained with plants and seating areas.
• The kitchen area on the ward was for the patients’ use.They could make hot and cold drinks whenever theywanted and there was also a water dispenser. Patientssaid that the quality of the food was variable. Onepatient said that the portions could be bigger. The wardmanager said that consideration had been given to thiscomment and, following discussions with the kitchenand a dietician, the food portions for that patient wereincreased.
• Patients’ bedrooms were personalised with personalitems such as book and games and musicalinstruments. Some patients also had their own bedding.Each room had storage space for patients’ possessions.
Meeting the needs of all people who use the service
• Access to the ward was via a set of stairs only and thestaff were aware of the impact for patients who werereferred with reduced mobility.
• The ward displayed a range of information for patients.This included details about an advocacy clinic, themeeting minutes for the last patient communitymeeting, multi-faith pastoral care and a charterdescribing what patients could expect from the service.
• We did not see leaflets on the ward in other languages.Staff said that they had access to translation servicesincluding staff at the location who could speak a rangeof community languages.
• There was a reasonable range of food available forpatients. Patients said that the quality and choice offood was generally good. However, one patient said thathe would like to have more vegetables. The staff saidthat that a range of alternative food was available forreligious and ethnic groups as well as gluten-free meals.At the time of our visit, such food was not on the menu,although staff said it could be prepared at patients’request.
• In a communal area outside of the ward there were faithrooms for patients to use where they could receiveappropriate spiritual support. These rooms alsocontained religious and spiritual reading material fromdifferent faiths. One of these rooms was also used as anadvocacy office where patients could meet the advocatein private.
Listening to and learning from concerns andcomplaints
• The patients we spoke to confirmed that they knew howto make a complaint if they needed to. One patient saidthat staff repeated how to do this every Monday at thepatients’ community meeting.
• Staff said that complaints on the ward were very rareand that no patients on the ward had made a formalcomplaint for over the last year. The patients we spoketo confirmed that they had not made any complaintsand did not know of any others being made. Theadvocate also said that they were not aware of anyformal complaints on the wing for a very long time. Theadvocate said that occasionally patients were not happyabout the scheduling of their leave and asked for theirsupport to request it being moved. The advocate said
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
34 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

that staff usually agreed to these requests. A patientalso confirmed that staff had responded positively totheir request to move their scheduled leave times toaccommodate his needs.
• Staff said that feedback was given to staff and patientsfollowing an investigation into a patient’s complaint.However, no patient records displayed any suchfeedback.
Are long stay/rehabilitation mentalhealth wards for working-ageadults well-led?
Good –––
Vision and values
• It was evident that the staff knew who the seniormanagers of the ward were and these managers wereon the ward throughout our inspection. The managersworked in offices adjacent to the ward and were clearlyaccessible to staff.
Good governance
• Records indicated that staff were mostly up to date withtheir mandatory training and that they received regularsupervision. Although staff had not received significanttraining in working with an autistic client group.
• Staff said that they learned from incidents through staffmeetings, handovers and ward rounds. However, thereflective practice meeting was stopped over a year ago.The minutes of the staff meeting in September detailedonly discussions on administrative issues. There was nodiscussion of cases, how staff worked with patients,patients’ needs or reflective practice.
• Staff did not have the ability to submit items directly tothe trust risk register. Staff gave details of incidents to asecurity manager, who had the responsibility ofupdating the register. It was not clear who had thisresponsibility in the absence of the security manager.
• Each ward had a recently implemented overarchinglocal action plan (OLAP) that included health and safety,quality network reviews and the service environment.These areas were red, amber and green (RAG) rated,updated monthly and included recommendations, theaccountable person, resources required and action
plans. Some actions were also allocated to the local riskregister. The hospital manager trained the heads ofdepartments on using the OLAP to ensure informationfiltered down to team meetings.
• The clinical manager chaired a monthly clinicalgovernance meeting that discussed topics such as acorporate learning log, incidents, complaints, andpharmacy. Doctors, nurses, the pharmacist, qualityassurance manager and medical director attendedthese meetings.
• Cygnet’s main office completed recruitment includinginterviewing and employment checks. The hospitalmanager could set criteria for shortlisting andparticipated on interview panels. Staff records were upto date including occupational health, references, workpermits, proof of identification and professionalmemberships.
• Cygnet Harrow’s hospital manager reported to theoperations manager, who reported to the organisationschief operating officer. The hospital manager attendedregular meetings with other Cygnet hospital managersfrom other sites for information sharing.
• The quality assurance manager acted as a link betweenthe local governance and corporate governance andcovered eight Cygnet sites across the south west andsouth east of the country.
Leadership, morale and staff engagement
• The ward did not have any bullying or harassment casesin the past 12 months.
• Staff said that they felt confident that they could raiseconcerns about their work with management.
• Staff said they enjoyed working on the ward and theirmorale was good. One staff member said thatmanagement had been very supportive of staff, givingthe example of management agreement to staffrequests for flexible working.
• One staff member said that management were verysupportive in staff ideas for new patient activities. Oneof these ideas was for a patient swimming group, whichwas shortly to be implemented.
Commitment to quality improvement and innovation
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
35 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

• The consultants said a lot of work had gone into tryingto get AIMS accreditation but they had been let down bythe environment. Work was currently underway on thewards to address the recommendations and improvethe environment.
Longstay/rehabilitationmentalhealthwardsforworkingageadults
Long stay/rehabilitation mentalhealth wards for working ageadults
Good –––
36 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Areas for improvement
Action the provider MUST take to improve
• The provider must ensure that all staff on Springs wingand Springs unit complete specialist autism training tobetter understand the needs of patients.
Action the provider SHOULD take to improve
• The provider should ensure that it considers the risksof the shared entrance between Byron ward andSprings wing by putting measures in place to ensurepatients’ safety and effectively manage risks.
• The provider should review Springs unit wardenvironment to ensure it meets the needs of peoplewith autism and/or learning disabilities.
• The provider should ensure that the ward boardcannot be viewed from the ward on Springs unit.
• The provider should ensure that all areas of the wardare kept tidy and clear of broken or unused items ofequipment at all times.
• The provider should ensure that blind spots onSprings wing are addressed and staff mitigateassociated risks.
• The provider should ensure that staff follow handhygiene procedures.
• The provider should ensure that they complete a riskassessment to determine if flumazenil should beavailable to treat patients if they experiencedrespiratory depression.
• The provider should ensure that staff report allincidents.
• The provider should ensure they give informal patientsaccurate information regarding their rights to leave theward.
• The provider should ensure that staff assess thecapacity of patients to make individual decisions inrelation to the MCA.
• The provider should proactively review whether it ismeeting the needs of patients who have been on theunit for more than five years.
• The provider should ensure that supervision on Byronward takes place each month for all staff and that thisis recorded clearly.
• The provider should ensure that patients’ informationin their files is easily accessible, including archivedinformation.
• The provider should ensure that patients’ health needsare adequately addressed.
Outstandingpracticeandareasforimprovement
Outstanding practice and areasfor improvement
37 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published

Action we have told the provider to takeThe table below shows the legal requirements that were not being met. The provider must send CQC a report that sayswhat action they are going to take to meet these requirements.
Regulated activity
Assessment or medical treatment for persons detainedunder the Mental Health Act 1983
Treatment of disease, disorder or injury
Regulation 18 HSCA (RA) Regulations 2014 Staffing
The provider had not ensured that all staff on Springsunit and Springs wing had completed specialist autismtraining. This meant that staff were not adequatelytrained to understand and manage patients’ needs.
This was a breach of regulation 18 (2)(a)
Regulation
This section is primarily information for the provider
Requirement noticesRequirementnotices
38 Cygnet Hospital Harrow Quality Report This is auto-populated when the report is published
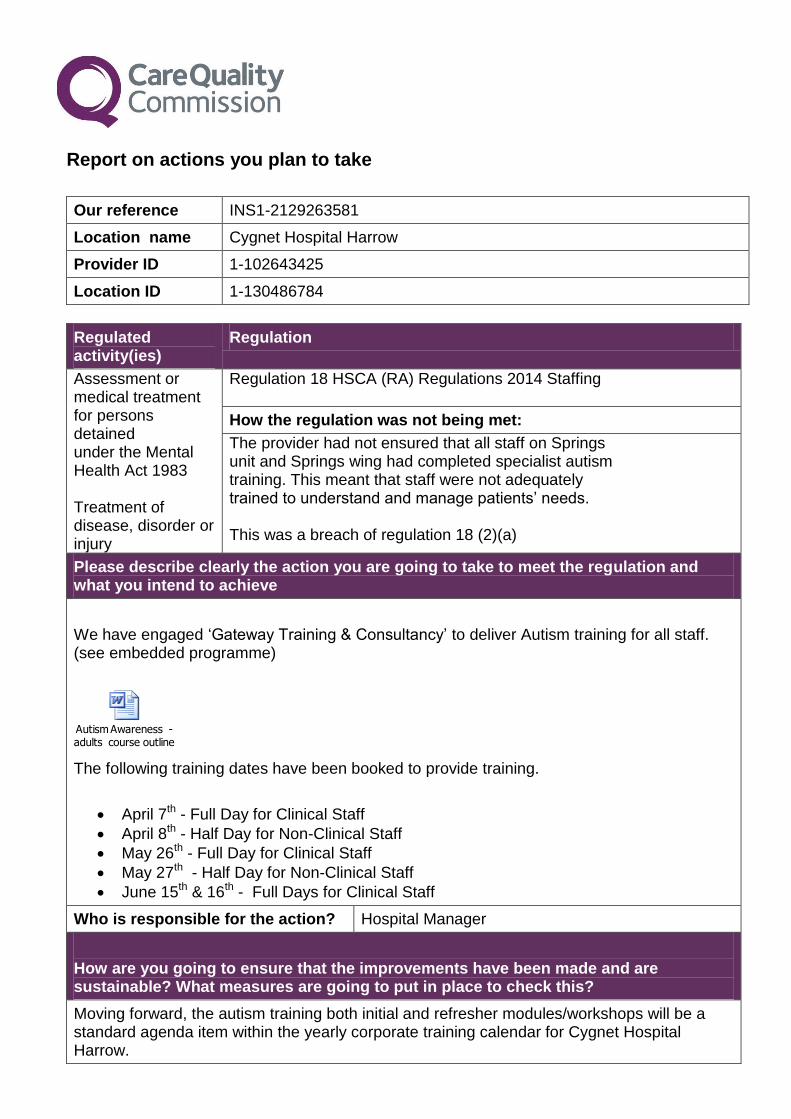
Report on actions you plan to take
Our reference INS1-2129263581
Location name Cygnet Hospital Harrow
Provider ID 1-102643425
Location ID 1-130486784
Regulated activity(ies)
Regulation
Assessment or medical treatment for persons detained under the Mental Health Act 1983 Treatment of disease, disorder or injury
Regulation 18 HSCA (RA) Regulations 2014 Staffing
How the regulation was not being met:
The provider had not ensured that all staff on Springs unit and Springs wing had completed specialist autism training. This meant that staff were not adequately trained to understand and manage patients’ needs. This was a breach of regulation 18 (2)(a)
Please describe clearly the action you are going to take to meet the regulation and what you intend to achieve
We have engaged ‘Gateway Training & Consultancy’ to deliver Autism training for all staff. (see embedded programme)
Autism Awareness - adults course outline .doc
The following training dates have been booked to provide training.
April 7th - Full Day for Clinical Staff
April 8th - Half Day for Non-Clinical Staff
May 26th - Full Day for Clinical Staff
May 27th - Half Day for Non-Clinical Staff
June 15th & 16th - Full Days for Clinical Staff
Who is responsible for the action? Hospital Manager
How are you going to ensure that the improvements have been made and are sustainable? What measures are going to put in place to check this?
Moving forward, the autism training both initial and refresher modules/workshops will be a standard agenda item within the yearly corporate training calendar for Cygnet Hospital Harrow.
2
Who is responsible? Hospital Manager / Training Coordinator
What resources (if any) are needed to implement the change(s) and are these resources available?
Planned sessions: To be delivered at Cygnet Hospital Harrow.
April 7th & 8th
May 26th & 27th
June 15th & 16th
Date actions will be completed: June 2016 & on-going
How will people who use the service(s) be affected by you not meeting this regulation until this date?
Our in-house Consultant Clinical Psychologist has to date run ASD Awareness sessions for staff both clinical and non-clinical. There are two additional sessions booked for 23rd Feb & 8th March 2016.
In addition, reflective practice (facilitated by our Consultant Clinical Psychologist) will continue on an on-going basis.
Autism Presentation_1.pptx
Completed by:
(please state name(s) in full)
S.P. Quigley
Position(s):
Hospital Manager
Date: 15th February 2016


















