
Appendices - Shodhganga : a reservoir of Indian theses...
50
Appendices
Transcript of Appendices - Shodhganga : a reservoir of Indian theses...

Appendices

A. Consent Form
Title of the study: “A study on effect of music therapy and meditation on performance in
professional shooters”.
Invitation to Participation;
You are invited to participate in this research study investigating the efficacy of music therapy
and meditation on performance in professional shooters.
Basis for Subject selection;
You are eligible to participate in this study because you fulfill all the inclusion and exclusion
criteria required for the study. You will be one of the approximately 200 professional shooters to
participate in this study.
Procedure;
You will undergo a non-invasive evaluation procedure and will be asked to undergo the training
protocol allotted to you. It is anticipated that your time commitment will be 5 days /week for 5
weeks from the time of your participation.
Potential risks;
There are minimal perceivable risks associated with your involvement in this research study.
However, you may ask about any doubts regarding the study, if any while you are participating.
Potential benefits;
The potential benefits to you for participating in this research study are-
This study may show increase in overall shooting performance, increase activeness and decrease
pre competition stress/anxiety.
Guarantee of Confidentiality;
All the information about you would be kept confidential and limited to me and my project
supervisors and will not be shared with person who is not a part of this research. At no time will
your name appear on any materials or reports of the research findings (including web-site
postings of the results, conference presentations, or professional publications). Your signed
consent form will be stored separately from your data to insure complete confidentiality.
Withdrawal from Participation;
Participation in this study is voluntary. If you decide to dropout, you are free to withdraw your
consent and to discontinue your participation at any time with impunity.
Offer to Answer Any Questions;
If you have any questions about the procedures at any time, please do not hesitate to ask. If you
think of questions later, please feel free to contact Shaji John (+91 9560223344,
[email protected]). All questions about the procedures and this study in general will be
answered. However, some questions may not be answered until after you have completed the
procedures to insure that your responses will not be affected by your knowledge of the research.

Participant’s Statement;
I am voluntarily making the decision to participate, and I am at least eighteen years of age. My
signature certifies that I have read and understood the aforementioned information. My signature
also certifies that I have had an adequate opportunity to discuss this study with the research
investigator and have had all my questions answered to my satisfaction. I understand that by
signing this document, I waive no legal rights. I also know that I shall receive a copy of this
consent form for my records.
Participant’s Name:……………………….………………Signature/Date: ……………….
Confidential Code:………Address:.........................................................................................
Contact no: ……………………e-mail: ……………………………………………………..
Research Investigator’s Statement;
In my judgment, the aforementioned participant is voluntarily and knowingly giving informed
consent and possesses the legal capacity to do so.
Research Investigator’s Name: Shaji John Signature/Date………………………
Contact No: +91-9560223344, e-mail: [email protected]

B. Subjective Data Form
Group: - A B C D
Demographic data;
1. Conf. Code: ……………………………..Age/Sex: ……yrs./M: F: Date:…./..…/……..
2. Weight (kg): ……………. Height (cm): ……………. BMI: ……………
3. HR:……./ bpm RR:……../ rpm BP: ……/…… mm of Hg
Shooting History;
4. Level of shooters: International: National: State: District: Recreational:
5. Participation in competitive shooting for: <1 yr: <2 yrs: <5 yrs: >10 yrs:
6. Categories of shooting: Pistol: Rifle: Specification:……………………..
7. For pistol shooters specify range: 10m: 25m 50m:
8. Average duration of shooting training / practice:… …….. hrs/day …...………. days/week
9. Average duration for fitness training:…….…………….. hrs/day……………….days/week
Medical History;
10. Have you been diagnosed of any medical problem last 6 months: Yes: No:
11. Are you on any medication: Yes: No:
12. If ‘Yes’ for 10 and 11 specify in detail:.………………………………………………………
13. Do you feel stressed during: Training: : Yes: No: Pre-competition: Yes: No:
Competition Yes: No: Post-competition: Yes: No: Always Yes: No:
Intervention Specific;
14. Are you interested in listening to music: Yes: No:
15. If ‘Yes’ type of music: Classical: Hindi Film: Western: Instrumental:
Fast: Melodious: Any: Specification: …………………………………...
16. Have you listened to any music daily more than 10 minutes in last 1 week:
Yes: No:
17. Are you interested in meditation: Yes: No:
18. Are you practicing any form of Meditation for last 6 months: Yes: No:
19. Have you ever practiced any form of relaxation therapies? Yes: ..………..…… No:
Personal History;
20. Are you alcoholic: Yes: No: Daily: <week: <month: occasional:
21. Are you a Smoker: Yes: No: Daily: <week: <month: occasional:
22. Do you feel it is necessary during Training, Pre-competition, Competition: Yes:No:
23. Are you able to follow the instructions given to you till the end of the study: Yes:No:

Subject Data Chart
S# Variables 0 Days / Pre test 29 days / Post Test 36 Days / Follow up
2
SDNNi
5
nHF
6
nLF
8
S. Cortisol
9
P. Score

C. Songs Table
1 Ab Kahan Jayen Ham
Ujala 1959 Darbari
Kanada
Kaherava
Shankar Jaikishan Manna Dey
2 Ab Mori Vinti Suno
Bhagwaan
Taj 1956 Darbari
Kanada
Kaherava
Hemant Kumar
Mohd. Rafi
3 Agar Mujhse Muhobbat Hai,
Mujhe Sab Apne Gam De
Do
Aap Ki Parchhaiyan 1964 Darbari
Kanada
Dadra
Madan Mohan Lata Mangeshkar
4 Basti Basti Parbat Parbat
Railway Platform 1955 Darbari
Kanada
Kaherava
Madan Mohan Mohd. Rafi
5 Chandi Ki Divar Na Todi
Vishvaas 1969 Darbari
Kanada
Kaherava Kalyanji, Anandji Mukesh
6 Aiya Re Daiya Laj Mohe
Lage
Leader 1964 Darbari
Kanada
Kaherava Naushad Asha Bhosle
7 Dekha Hai Pehli Baar
Saajan 1991
Darbari
Kanada
Dadra Laxmikant, Pyarelal Alka Yagnik,
S.P.
Balsubramaniam
8 Dil Jalta Hai To Jalane De Pahli Nazar
1945 Darbari
Kanada
Kaherava
Anil Biswas
Mukesh
9 Duniya Badal Gayi
Babul 1950 Darbari
Kanada
Dadra
Naushad Talat Mehmood,
Shamshad
Begum
10 Ghoonghat Ke Pat Khol Re Jogan 1950 Darbari Kanada
Kaherava
Bulo C Rani Geeta Roy
11 Guzre Hain Aaj Ishq Men,
Dil Diya Dard Liya
1966 Darbari
Kanada
Dadra
Naushad
Mohd. Rafi
12 Ham Tujh Se Muhabbat Kar Ke
Awara 1951
Darbari Kanada
Kaherava
Shankar Jaikishan Mukesh
13 Ham Tum Se Juda Ho Ke Ek Sapera Ek
Lutera
1965
Darbari
Kanada
Kaherava
Usha Khanna Mohd. Rafi
14 Hangama Hai Kyon Barpa
non-film song 1994 Darbari
Kanada
Kaherava
Ghulam Ali
Ghulam Ali
15 Jhanak Jhanak Tori Baje Payeliya
Mere Huzur
1968
Darbari Kanada
Tintal
Shankar, Jaikishan Manna Dey
16 Jogi Aaya Black & White
2008 Darbari
Kanada
Kaherava Sukhwinder Singh
Sukhwinder
Singh
17 Kabhi Dil Dil Se Takarata
To Hoga
Anokhi Ada
1948 Darbari
Kanada
Kaherava Naushad
Shamshad
Begum
18 Kitna Hasin Hai Mausam
Azad
1955 Darbari
Kanada
Kaherava C. Ramchandra Lata
Mangeshkar, C. Ramchandra
19 Koi Matwala Ayaa Mere
Dware
Love In Tokyo 1966 Darbari
Kanada
Sitarkhani Shankar, Jaikishan Lata Mangeshkar
20 Main Nigahen Tere Chehare
se Hataun Kaise
Aap ki Parchaiyyan 1964 Darbari
Kanada
Dadra
Madan Mohan Mohd. Rafi
21 Mere Mehboob Shayad Aaj Kuchh
Kitne Paas Kitne Door
1976 Darbari Kanada
Kaherava Chand Pardesi
Chandrani Mukherji
22 Mitava Laut Aye Ri
Sangeet Samrat Tansen
1962
Darbari Kanada
-- S.N. Tripathi
Manna Dey
23 Muhabbat Ki Jhuthi Kahani
Pe Roye
Mughal-e-Azam
1960
Darbari
Kanada
Kaherava Naushad
Lata Mangeshkar
24 Mujhe Tum Se Kuch Bhi Na
Chahie
Kanhaiya 1959 Darbari
Kanada
Rupaktal Shankar, Jaikishan Mukesh
25
Nain Se Nain Milaye
Rakhne Ko
Waada
1957 Darbari
Kanada
Ektal Rashid Atre Ustad Fateh Ali
Khan and Zahida

R
a
g
a
D
a
r
b
a
r
i
b
a
s
e
d
m
u
s
i
c
u
s
e
d
f
o
r
M
usic Therapy (www.chandrakantha.com)
Perveen
26 Nainheen Ko Raah Dikha Prabhu
Bhakta Surdaas
1942 Darbari Kanada
Kaherava Gyan Dutt
K.L. Saigal
27 O Duniya Ke Rakhavale
Baiju Bawra
1952 Darbari
Kanada
Kaherava Naushad
Mohd. Rafi
28 Pag Ghoongroo Bandh
Meera Naachi Thi
Namak Halal
1982 Darbari
Kanada
Kaherava Bappi Lahari Kishore Kumar
29 Pyar Ki Aag Men Tan
Badan
Ziddi 1964 Darbari
Kanada
Kaherava S.D. Burman Manna Dey
30 Raha Gardishon Men
Haradam
Do Badan
1966 Darbari
Kanada
Kaherava Ravi Mohd. Rafi
31 Sarfaroshi Ki Tammana Shaheed
1965 Darbari
Kanada
Dadra Prem Dhawan
Mohd. Rafi,
Manna Dey,
Rajendra Mehta
32 Satyam Shivam Sundaram
Satyam Shivam Sundaram
1978 Darbari Kanada
Kaherava Laxmikant, Pyarelal
Lata Mangeshkar
33 Shairana Si Hai Zindagi Ki Faza
Phir Teri Kahani Yaad Ayi
1993 Darbari Kanada
Dadra Anu Malik Alka Yagnik
34 Suhani Chaandni Raaten
Hamen Sone Nahin Deti
Mukti 1977 Darbari
Kanada
Dadra R.D. Burman Mukesh
35 Tere Dar Pe Ayaa Hun,
Kuchh Karke Jaunga
Laila Majnu
1976 Darbari
Kanada
Kaherava Madan Mohan Mohd. Rafi
36 Teri Duniya Mein Dil Lagta
Nahin
Baware Nain 1950 Darbari
Kanada
Kaherava Roshan Mukesh
37 Tora Man Darpan Kahalay
Kaajal
1965 Darbari
Kanada
Kaherava Ravi Asha Bhosle
38 Woh Mohabbat Woh Wafaayen
Noor Jahan
1967 Darbari Kanada
Dadra Roshan Mohd. Rafi
39 Tu Jo Nahin Hai to Kuch Bhi Nahin Hai
Wo Lamhe
2006 Darbari Kanada
Kaherava Pritam Glenn John
40 Tu Pyar Ka Sagar Hai
Seema 1955 Darbari Kanada
Kaherava Shankar Jaikishan Manna Dey
41 Tumhe Zindagi Ke Ujale
Mubarak
Poornima 1965 Darbari
Kanada
Jhaptal Kalyanji, Anandji Mukesh
42 Tumse Hi Ghar Ghar
Kahalaya
Bhabhi Ki
Chudiyaan
1961 Darbari
Kanada
Kaherava Sudhir Phadke
Mukesh
43 Tuthe Hue Khvabon Ne
Madhumati
1958 Darbari
Kanada
Kaherava Salil Chowdhury Mohd. Rafi
44 Ud Ja Bhanwar Maya Kamal
Ka
Rani Roopmati 1959 Rupaktal S.N. Tripathi Manna Dey


D. Abstract
A STUDY ON EFFECT OF MUSIC THERAPY AND MEDITATION ON
PERFORMANCE IN PROFESSIONAL SHOOTERS Shaji John
1, S. K Verma
2, G. L Khanna
3
1PhD Scholar, Punjabi University, India,
2Supervisor, Department of Sports Sciences, Punjabi University, India,
3Co-Supervisor, Faculty of Applied Medical Sciences, Manav Rachna International University, India.
E-mail:[email protected], Tel.: +919560223344
Background: Little has been known about the Hypothalamic Pituitary Adrenal (HPA) axis
response and Autonomic Nervous System (ANS) activity to Pre-Competition Stress (PCS) and
its response to relaxation therapies such as of Music Therapy (MT) and Mindfulness Meditation
Therapy (MMT) on sports population. Studies have been performed on the psychophysiological
responses of music and meditation on normal and diseased persons, but little has been done on
its combination and individual responses on sports population especially in shooters.
Objective: The purpose of this study was to estimate the contribution of MT, MMT and its
Combination Therapy (CT) on PCS, by psychophysiological basis and its effect on Shooting
Performance.
Methods: 200 professional elite male shooters with mean age of 29.5 ± 4.3years were examined
in four groups (n= 50 ±3) in each group. Group A, B, C and D; MT, MMT, CT and as a Control
(C) groups respectively. Total duration of the study was 5weeks, 4weeks of interventional and
1week study to determine the follow-up effect. Pre, post and follow-up data of quantitative
phenotypic markers of ANS activity by Heart Rate Variability (HRV), HPA- Axis by Salivary
Cortisol (SC) and Performance Score (PS) were analyzed.
Results: All three interventional groups have shown positive correlation, but CT group has
shown highly significant (p<0.0001) post-intervention and in follow-up (p<0.0001) in SDNNi,
nHF, nLF, SC and in PS. Ultimately resulted in reduction of PCS level and increase in PS.
Comparatively MT and MMT, MT group shown marginal improvement than MMT. Whereas
the control group has been shown non-significant result compare to interventional groups
(p<0.05).
Conclusions: It is concluded that relaxation therapies such as MT and MMT interventions along
with routine sports specific training may decrease PCS and will enhance PS and found CT is
more effective than MT and MMT alone and also found MT has been shown better effectiveness
than MMT in four weeks of training.
Key words: ANS, HPA, HRV, Cortisol, Pre competition Stress, Music, Meditation, Shooting.

Manuscript
Introduction:
In shooting the requirement of good physical and psychological condition as well as
technical perfection is highly demanded. The important use of vision for shooting necessitates,
leading to compensation through subconscious postural mechanisms based on proprioceptive and
vestibular information, such as a less elevation of pre-shot heart rate and blood pressure, a lower
sweating and a more appropriate preparatory brain activity (Tremayne and Barry, 2001). Pistol
shooting is a static activity requiring a strict control of body segments and posture to align the
rear sight aperture and the foresight through proprioceptive feedback and gaze fixation either on
the target directly or between the target and the weapon and, therefore, to increase precision of
the shot (Mononen et al., 2007). Air pistol shooting is an Olympic sport requiring extreme
mental concentration and movement precision for success. Compared to that of rifle shooting,
there are very little literatures related to pistol shooting. In this work, we investigated pistol
shooting and several of the psychophysiological factors that affect the shooting performance.
While a number of studies have examined both psychological and physiological factors related to
shooting performance, to our knowledge, this is the first study to determine the efficacy of MT
and MMT on HRV and SC in professional shooters.
Stress is most often used to describe an unpleasant emotional state or condition which is
characterized by subjective feelings of tension, apprehension, and worry. In sports context it is
commonly known as PCS or anxiety. Further, researches indicated that anxiety has a negative effect
on these sport outcomes (Terry and Slade, 1995). Research on how athletes cope with sport-related
stress has been recognized for both its practical and its theoretical importance because of the
debilitating effects that stress may have on athletic performance (Smith et al., 1998). Stephen et
al., (2009), findings suggest that, prior to competing, sport performers encounter more stressors
pertinent to performance, these observations highlight that all the athletes should be considered
when preparing and implementing interventions to manage competition stress. PCS is a widely
prevalent condition that exists among athletes of all levels and within every sport. Its relationship
to performance has been studied both in and out of the sport context through test anxiety research
and anxiety research with athletes (Chamberlain and Hale, 2007; Kais and Raudsepp, 2005).
Despite the large body of research on pre-competition anxiety, our understanding of its

relationship to performance remains elusive. Researchers have been conducted to discover or
identify the sources of stress in various competitive sports, including basketball (Madden et al.,
2004), figure skating (Scanlan et al., 1989), college baseball (Anshel et al., 1978), golf (Cohn,
1990), and wrestling (Gould et al., 1988). Anxiety and stress decreases the concentration and
performance level of sports persons (Solberg and Bergulund,, 1996). A recent meta-analysis
examined the effects of competitive anxiety and self-confidence on athletic performance (Craft et
al., 2003), it is concluded that a weak relationship appears to exist between competitive anxiety,
self-confidence, and athletic performance. Pre competition and during competition stress rises in
today’s sports world.
Research findings comparing the physiological and psychological markers of stress have
been equivocal (Filaire et al., 2001). Acute stress may affect cardiac function by shifting
autonomic cardiac regulation in favor of the sympathetic nervous system. Environmental
conditions that evoke behavioral or physiological responses may be considered stressors.
Neurobiological responses are stressor-specific (Pacak and Palkovits, 2001) thus, it is important
to study responses to relevant stressors.
Cortisol is a hormonal response to acute stress and has been measured to be higher before
competition than at resting conditions (Salvador et al., 2003). Researchers have found that
athletes produce higher levels of Cortisol before games than before non-competition situations
(Filaire et al., 2007; Filaire et al., 2001; Haneishi et al., 2007; Salvador et al., 2003). The result
supports previous findings that athletes are more anxious before games than during off days,
because Cortisol is secreted as a result of a threatening stimulus, and sports competition is
considered an anxiety-arousing situation (Salvador et al., 2003).
Decreased HRV has often been reported during physically or emotionally stressful
events. The majority of the studies concluded that the reduction in overall variability is induced
by the withdrawal of the highly frequent vagal activity. High vagal tone has been linked to
efficient autonomic regulatory activity which allows an organism to enhance its sensitivity and
response to physiological and environmental challenges (Friedman and Thayer, 1998). In
previous research, HRV was found to serve as a physiological index of self-regulatory strength
(Segerstrom and Solberg, 2007). Empirical evidence strongly supports these assumptions,
indicating that HRV co varies with processes that are involved in self regulation, such as emotion
regulation (Appelhans and Luecken, 2006), constructive coping (Fabes and Eisenberg, 1997),

and the pursuit of goals (Geisler and Kubiak, 2009). More specifically, researches have indicated
that HRV is associated with behaviors that require executive functioning.
In applied sport psychology, its efforts to enhance the competitive performance of
athletes, has traditionally utilized cognitive behavioral methods and techniques with an emphasis
on developing self-control of internal states, commonly referred to as psychological skills
training (Whelan et al., 1991). Relaxation techniques have been used in sports primarily to
enhance recovery from training and competition, manage anxiety and improve performance
(Solberg et al., 1996).
Studies support previous researches that found music to be an effective tool for
improving athletic performance (Copeland and Franks, 1991; Ferguson et al., 1994;
Karageorghis et al., 1996). Evidence for the positive effect of music on performance demon-
strated that karate players attained superior performances with the use of asynchronous
background music during performance (Ferguson et al., 1994). Likewise, performance
improvements were observed in treadmill running tasks under conditions of asynchronous music
(Copeland and Franks, 1991). Additionally, Studies that have investigated the stimulative or
energising effects of music have also noted benefits in the performance of physical tasks
(Karageorghis et al., 1996) Furthermore, (Jackson et al., 1992) reported that pre-performance
mood was a key antecedent of flow among elite figure skaters.
The techniques of MMT which focus on awareness to develop a detached observation of
the contents of consciousness may represent a powerful cognitive behavioural coping strategy
for transforming the ways in which we respond to life events (Astin, 1997). Even though many
studies on MMPs have been criticized for the lack of scientific rigor, including the lack of high
quality randomized controlled studies designed to differentiate between the specific (i.e.
specifically related to repeated sitting meditation practice) and the non specific (i.e. related to
benefits' expectations) effects of such practices (Chiesa and Serretti, 2010). The frequent use of
self report instruments as measures of clinical improvements following mindfulness training
(Chambers, et al, 2008); overall available studies provide preliminary evidence for the clinical
usefulness of such interventions. Further, as it has been suggested that the use of mindfulness
techniques may lead to the development of greater self-awareness, habitual ways of responding
to external cues can be more easily identified, which may result in enhanced behavioural

flexibility in response to athletic demands. Mindfulness-Based Cognitive Therapy for use with
an athletic population.
The present study focused on the relation of physiological response to skilled sport
performance, and investigated the relevance of relaxation therapies in PCS. For this purpose,
physiological variables, including Heart Rate Variability (HRV) and Salivary Cortisol (SC) were
recorded during the pre and post-competition and follow-up phases of real shooting competition.
Materials and Methods
Subjects: A total of 220 healthy male elite level shooters with mean age of (29.5±4.3years)
voluntarily recruited from Indian shooting team were selected for the present study; permission
was obtained from chief coach and officials. Questionnaires administered prior to the experiment
were indicated that no volunteers are included as per exclusion criteria such as any physical or
mental illness, hearing impairment, and have been undergoing neither meditation nor music
therapies for last 3 months. All subjects were nonsmokers, medication-free and not habitual
drinkers. The procedures involved and potential risks of the study were explained to the subjects,
and the written consent was obtained prior to the study.
The program consisted of three primary components: (1) Music Therapy (MT) (2)
Mindfulness Meditation Therapy (MMT), and (3) Combination of both (CT). 220 Participants
were randomly allocated into four groups, 55 in each group; MT, MMT, CT, and Control (C)
groups by multiple blocked randomization, after the dropout 200 (50±3) subjects could complete
the study. Heart Rate (70±3bpm), Respiratory Rate (15±2rpm), BMI (24±1.04kg/cm2) and Blood
Pressure (119±4/79±4 mm of Hg) were the mean values of recruited in this study. Intervention
trial was conducted to the respective subjects 1week prior to the study. Concerning impediments
to effective practice, subjects were monitored by the researcher and experts during the
interventions. The interventions were provided over the course of 4 weeks and 1week follow-up,
group sessions with a maximum of 8 participants each, 20 minutes session per day, 6 days a
week and one day was off. Participants were asked not to consume caffeine or alcoholic
beverages for 12 h, and not to exercise for 12 h prior to the experiment especially during testing.
They were requested to refrain from eating and drinking for at least 3 h prior to the experiment.
Procedure: The all participants of each batch reported to the laboratory at 08:00AM, each
session conducted in the morning (between 8 AM and 10 AM) and The subject changed into

loose fitting clothing, and shoes removed then the participants were instructed to lie in the supine
position on the floor mat in a quiet, light-attenuated room with the temperature between 24 and
28 °C with their eyes closed.
Interventions:
Music Therapy: CD of 30-40 music of Raga Darbari based Hindi songs given to the subject (in
MT and CT Groups) one week prior to the study and asked them to select 5-10 songs according
to their choice from 40 songs given , After selection of music, made separate folder for each
subjects. This music was delivered on SonyTM
MP3 player by headphone with volume of 60-70
dB, 60 to 70 beats per minute. The MT group was encouraged to assume a comfortable position
in supine position on a floor mat during delivery of the music intervention, Advised subjects to
clear their minds and allow their muscles to relax throughout the training session. The
participants left the room after 20 minutes of session.
Mind Fullness Meditation Therapy: The first step in performing a meditation is to adopt a
posture that ensures an erect spine and shoulder resting on the mat, with the hands should be
placed on the upper position of the abdomen, the position of head kept slightly foreword with the
support of small towel roll. The eyes closed, and were given 1 minutes of adaptation period. As a
meditation condition progress, subjects were asked to undergo 3 minutes for stabilization by
Shavasana, For Shavasana training the technique recommended by (Coulter, 2001) was used.
The subjects were asked to relax, performed meditation comprising a Pranayam for 4 min while
situated as in the control condition (in the supine position with the eyes closed and respiration at
a constant frequency of 0.2 Hz in tempo with the sound of a metronome (i.e., 5 breaths/min for 4
min)). Then the participants were instructed mindfulness by body scan i.e. focusing attention on
various joints of body by simply focuses on the way each part of body feels without labeling the
sensations as either “good” or “bad” in a sequence from distal to proximal and for 4 minutes
Pranayam. Finally ended with 3 minutes of Shavasana again.
Due to inexperience, drowsiness might cause during the performance of the meditation,
therefore tried to eliminate drowsiness by checking the participant’s eye movement and
respiration rates. Subjects were informed to raise their hands during any discomfort while doing
meditation and if so they were asked to immediately stop the session. Subsequently, the
participants left the room after 20 minutes of session.

Combination Therapy: This group was given a combination of both music and
meditation. Started with posture stabilization done by subjects during 1 minutes of adaptation
period, The music was delivered on MP3 player by headphone for 10 minutes of individual
choice and after the music session in same supine position meditation training started, they
performed meditation comprising all steps as MMTgroup, but the duration has been reduced to
10 minutes consists of Adaptation period for 1minutes, Shavasana for 1 minutes, Pranayam for 2
minutes, mind fullness for 3 minutes, 2 minutes of Pranayam and finally ended with Shavasana
for 1 minute. Subsequently, the participants left the room after 20 minutes of session.
Testing: The testing sessions were conducted between 8 am and 12 pm and the same researcher
tested all subjects. Measurement day scheduled one day prior to beginning the 1st week, 29
th day
and 36th
day, subjects were assessed for pre-test, post-test and follow-up data respectively,
except Performance Test, in a quiet controlled room with ambient temperature (24–280C). The
performance score calculated by pre-scheduled a competition in a internationally standard
shooting range on one day prior to beginning the 1st week, and on 29
th day, subjects were
assessed for pre-test, post-test Performance Score respectively.
All Participants were instructed to avoid consuming stimulant beverages, tea, and coffee;
exercising, in the 12 hours previous to the examination. The all participants of each batch
reported to the laboratory at 08:00AM, measurement procedure started between 09:00 am and
12:00 pm, to control as much as possible for circadian variations. Prior to testing, Participants
attended a detailed briefing session where they received full verbal instructions regarding the
procedures of the testing. SC samples were taken between 9:00 am -10:00 am. And HRV data
were taken between 10:00 am-12:00pm, all subjects were tested individually.
Salivary Cortisol; For obtaining the free, unbound, biologically active moiety of cortisol,
saliva samples were collected. To rid the mouth of contaminates, subjects rinsed thoroughly with
water ten minutes before saliva collection. Subjects sat in a comfortable chair with lumbar
support, Subjects were then allowed to relax for five minutes, the experimenter then began each
test session and collected minimum of 2 ml of saliva by tilting the head forward, allowing the
saliva to pool on the floor of the mouth, then passing the saliva through a short straw into a
polypropylene vial. The Salivary samples were labelled and sealed and refrigerated in an ice box
within 30 minutes. After all procedures the sealed sample sends to the laboratory on the same
day by 2:00 h to store under-15 degree centigrade to the laboratory for later analysis,

Free cortisol level data from the samples of saliva were analyzed in the laboratory by
using SalimetricsTM
salivary cortisol kit. On day of assay, samples brought at room temperature
and thaw completely, and centrifuge at 1500 x g (@3000 rpm for 15 minutes before adding to
assay plate and cortisol was assessed in via enzyme-linked immunosorbent assay as per
manufacturer (SalimetricsTM
) instructions.
Heart Rate Variability; For HRV testing, after fixation of equipments, subjects were then
instructed to lie down on the lounge for 5 minutes as an adaptation period, then the participants
were instructed to lie in the supine position on the floor mat with their eyes closed and the
subjects were asked to remain awake and relaxed, but the depth and rate of breathing were not
controlled. A continuous 5-minute resting data were collected and saved for HRV analysis.
HRV data were obtained using a cardio-recorder (i.e. Polar RS 800 CX ®—Polar electro Oy,
Kempele, Finland). For the Polar monitor, the series were automatically recorded by a receptor
belt and captured and stored by a wrist sensor unit, and this individual files containing normal
HRV data were transferred and saved to the computer via Infra Red port. Stored data processed
on a computer to calculate the following time and frequency domain indices of HRV according
to the recommendations of the Task Force of the European Society of Cardiology and the North
American Society of Pacing and Electrophysiology (1996); by dedicated software analyzed with
the polar HRV software (Polar Precision Performance TM
Software). Heart rate variability was
assessed in two ways: (1) time domain analysis and (2) frequency domain analysis, the power
was divided into two components: low frequency (LF, 0.04 Hz-0.15 Hz), and high frequency
(HF, 0.15-0.40 Hz).
In time domain analysis Standard Deviation of all R-R intervals (SDNNi) was obtained.
In frequency domain analysis, HF (is a marker of solely parasympathetic activity) and LF (is
mainly a measure of sympathetic activity with some influence from the parasympathetic nervous
system) were obtained. All these components were expressed in ms2
and then converted to
normalised units (n.u) (i.e. nHF, nLF), as recommended by the Task Force of European Society
of Cardiology (Task-Force, 1996).
Performance score: Measure of shooting accuracy, shooting score was calculated from the
standard shooting scoring board and the final result of competition obtained from the chief coach
after the completion of competition, in order to test shooting performance.
Data Obtained: Descriptive statistics (mean and SD) were used to describe all the study (Age,
BMI, HR, RR, BPD, BPS) and outcome variables (HRV (SDNNi, nHF, nLF), SC, PS). The
within group comparison of mean values of outcome variables (SDNNi, nHF, nLF, and SC) at
the baseline, 29th
day and at 36th
day was done using one-way analysis of variance followed by
Tukey’s post hoc multiple comparison tests and between 4 groups (MT, MMT, CT, C)
comparison of study and outcome variables was also carried out similar statistical tests (Table-10
and 11). And the main outcome variable performance score was compared before and after
intervention by using student’s t-test for paired samples. The 95% confidence intervals were
calculated for difference of mean of all outcome variables.
Result:
The comparison of base line mean values of study variables (Table-1) and outcome
variables (Table-2-5) among the 4 study groups, that is shooters who had interventions: as MT,
MMT, CT and C, showed a statistically non-significant difference in the mean values of Age( F=
1.15; p= 0.332), HR( F= 0.10;p=0.961), RR(F=2.44;p=0.066),BPD(F=0.42;p=0.736), and BPS
(F=1.11;p=0.347) among these groups. But there is a statistically significant difference in the
mean values of BMI (F= 3.57; p=0.015). In outcome variables showed a statistically non-
significant difference in the mean values in SDNNi (F= 0.29; p = 0.829), nHF (F= 1.68; p =
0.172), SC (F= 0.02; p = 0.995), PS (F= 0.40; p = 0.756). But there is a statistically significant
difference in the mean values of nLF (F= 10.18; p <0.0001) among these groups.
SDNNi: There is highly statistically significant difference in the mean values of SDNNi across
the 4 study groups at 29th
day (F= 905.76; p <0.0001) and at 36th
day (F= 796.73; p <0.0001).
The pair wise comparison of mean values indicates the group CT subjects mean values of
SDNNi were statistically significantly higher at 29th
day and 36th
day ( 56.78; 55.57) when
compared the mean values of study subjects of MT group at 29th
day and 36th
day (54.48; 53.87),
of MMT group (52.91; 52.70) and of C group ( 48.03; 48.20). Among the 4 groups the mean
values of SDNNi at 29th
and 36th
day were statistically significantly lower in C group i.e.
shooters who did not had any intervention. And among the 3 intervention groups, the mean
values of MMT group were significantly lower than the mean values of MT group and CT group.
nHF: Analysis showed a highly statistically significant difference in the mean values of nHF
across the 4 study groups at 29th
day (F= 3.26; p <0.0001) and at 36th
day (F= 2.16; p <0.0001).

The pair wise comparison of mean values indicates the CT group subjects mean values of nHF
were statistically significantly higher at 29th
day and 36th
day ( 45.53;44.44) when compared the
mean values of study subjects of MT group at 29th
day and 36th
day (43.42;41.56), of MMT
group (44.53;42.24) and of C group ( 33;33.95). Among the 4 groups the mean values of nHF at
29th
and 36th
day were statistically significantly lower in control group. And among the 3
intervention groups, the mean values of MT group were significantly lower than the mean values
of MMT group and CT group.
nLF: The pair wise comparison of mean values indicates the CT group subjects mean values of
nLF were statistically significantly lower at 29th
day and 36th
day ( 54.47; 55.56) when compared
the mean values of study subjects of MT group at 29th
day and 36th
day (56.58;58.44), of MMT
group (55.47;57.76) and of C group ( 70;66.05). Among the 4 groups the mean values of nLF at
29th
and 36th
day were statistically significantly higher in control group. And among the 3
intervention groups, the mean values of MT group were significantly higher than the mean
values of MMT and CT groups.
SC: Analysis showed a highly statistically significant difference in the mean values of SCO
across the 4 study groups at 29th day (F= 5.25; p <0.0001) and at 36th
day (F= 986.7; p <0.0001).
The pair wise comparison of mean values indicates the CT group subjects mean values of SCO
were statistically significantly lower at 29th
day and 36th
day ( 0.33;0.45) when compared the
mean values of study subjects of MT group at 29th
day and 36th
day (0.53;0.91), of MMT group
(0.66;0.93) and of C group ( 1.95;1.60). Among the 4 groups the mean values of SCO at 29th
and
36th
day were statistically significantly higher in control group. And among the 3 intervention
groups, the mean values of MMT group were significantly higher than the mean values of MT
and CT groups.
PS: Analysis showed a highly statistically significant difference in the mean values of
performance score across the 4 study groups at 29th
day (F= 13.69; p <0.0001) .The pair wise
comparison of mean values indicates the CT group subjects mean values of performance score
were statistically significantly higher at 29th
day (549.72) when compared the mean values
performance score of study subjects of MT group (544.31), of MMT group (541.69) and of C
group (518.04) at 29th
day. Among the 4 groups the mean values of PS at 29th
day was
statistically significantly lower in control group. And among the 3 intervention groups, the mean

values of PS of MMT group were significantly lower than the mean values of MT and CT
groups.
Discussion:
In the current study, used Heart Rate Variability (HRV) and Salivary Cortisol (SC) as
two physiological markers and Performance Score (PS) as one subjective marker to assess the
changes with different interventions in three groups and also assessed changes in control group
during the same duration. These parameters are very much reliable to provide true picture of
changes in pre competition anxiety or stress. This fact is supported by (Filarie et al., 2007 and
Hanesishi et al., 2007) and also supported by research findings comparing the physiological and
psychological markers of stress have been equivocal (Filaire et al., 2001). Since the salivary
cortisol assay has been proposed as the method of choice for assessing adrenocortical
(endocrine) function and responses to competitive stress, autonomic nervous system requires a
complex a dynamic interplay between SNS and PNS, Thus in this study also included HRV as a
physiological marker.
Time Component (SDNNi): The result of study showed that in HRV, SDNNi component value
from 0-29 day (Pre and Post Intervention) demonstrated significant difference in all groups
(F=905.76; p<0.0001) and also in 29th
- 36th
day (Follow-up) (F=796.73; p<0.0001). When
comparing in groups CT group (Combination) has shown 13.2% increase (56.78) during post
interventions and a follow up difference of 2.4% (55.57). When compared to MT and MMT (i.e.
Music and Meditation alone), Both groups also have been showed an increase in SDNNi value,
but MT group showed more increase of SDNNi than MMT group in post intervention i.e. 8.3%
(54.48) and 5.7 % (52.91) and a follow up effect of 1.2 % (53.87) and .4% (52.70) respectively.
These values showed there is an increase in SDNNi value in all groups where as CT group is
more than MT and MT group is more than MMT group. But in C group showed decrease of
4.5% (48.03) and 0.3% (48.20) during pre and post competition (Table-6).
Frequency Component (nHF): The result of this study showed that in nHF component of HRV
from 0-29 day (pre and Post Intervention) demonstrated significant difference in all groups
(F=3.26; p<0.0001) and also in 29th
- 36th
day (Follow-up) (F=2.16; p<0.0001). Pair wise
comparison of mean values indicates CT has shown 24% increase (45.53) during post
interventions and a follow up difference of 3% (44.44). MMT showed increase of 24% (44.53)

and follow up effect of 6% (42.24). In MT showed an increase of 18% (43.42) during
intervention and 5% (41.56) of increase during follow up effect. This result indicates MT has
less value of intervention effect in comparison with CT and MMT groups. But comparing CT
and MMT groups, MMT showed more follow up effect than CT and MT groups. Whereas C
group showed a decrease of 10% (33) during pre competition and 3% (33.95) of decrease during
post competition (Table-7).
Frequency Component (nLF): The result of the current study also supported the previous
researches, showed during intervention the nLF component decreased in all three groups of
intervention and follow up (F=3.26; p<.001; F=2.16; p<0.001). CT group decreased 14% (54.47)
during intervention and follow up decrease of 2% (55.56), MMT group decreased 12% (55.47)
and 4% (57.76) during intervention and follow up respectively. But in MT group there is a
decrease of 11% (56.58) and 3% (58.44) during intervention and follow up respectively. These
results showed that during intervention CT group is showed more decrease than MMT and MT
groups, and MMT group showed more follow up effect than both group MT and CT, whereas C
group showed an increase of 11% (70) and 6% (66.05) during pre and post competition period
(Table-8).
Salivary Cortisol: Result have been proved, during intervention of relaxation therapies, the
cortisol level in saliva decreased in all three groups of intervention and follow up (F=5.25;
p<0.0001 ; F=986.7; p<0.0001). In our result CT group has shown more decrease during
intervention and MT group showed more carryover effect in comparison with CT and MMT, and
there is decrease in pre competition. Whereas CT 75% (.33), MT 60% (.53) and MMT 50% (.66)
and as follow up carry over decrease MT 29% (.91), MMT 20% (.93) and CT 9% (.45) groups
respectively. Whereas C group showed an increase of 47% 1.95 and 26% 1.60 pre-competition
and post competition respectively (Table-9).
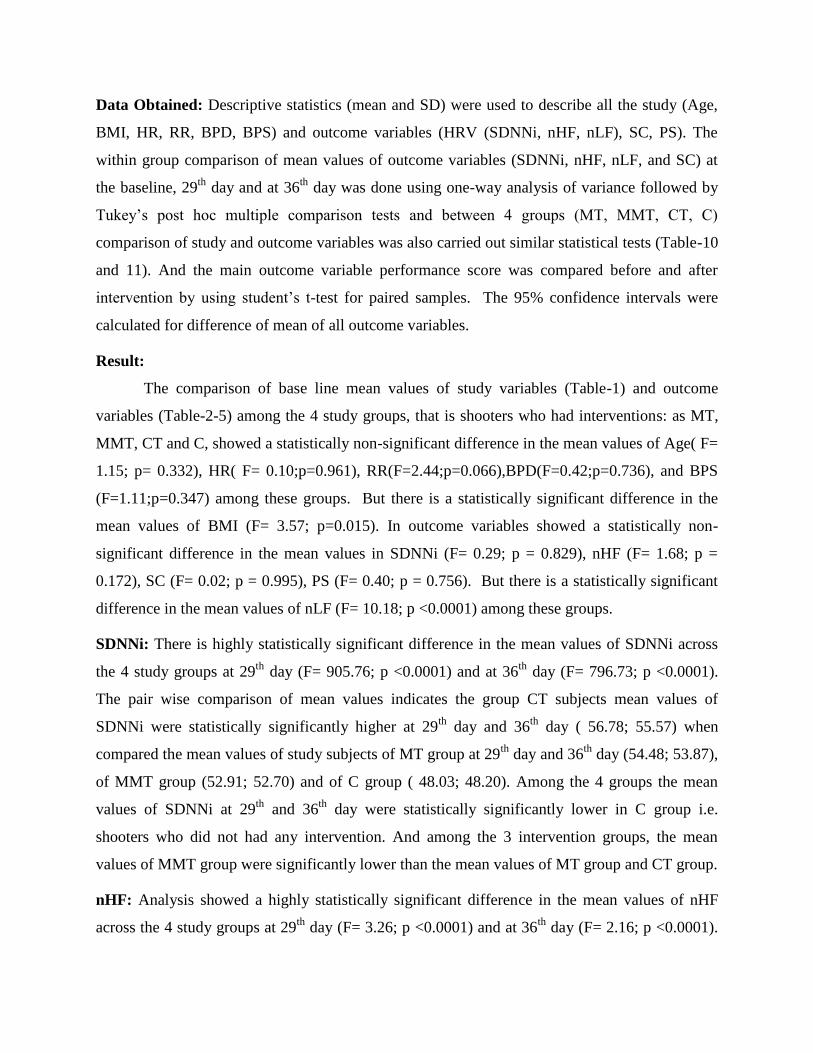
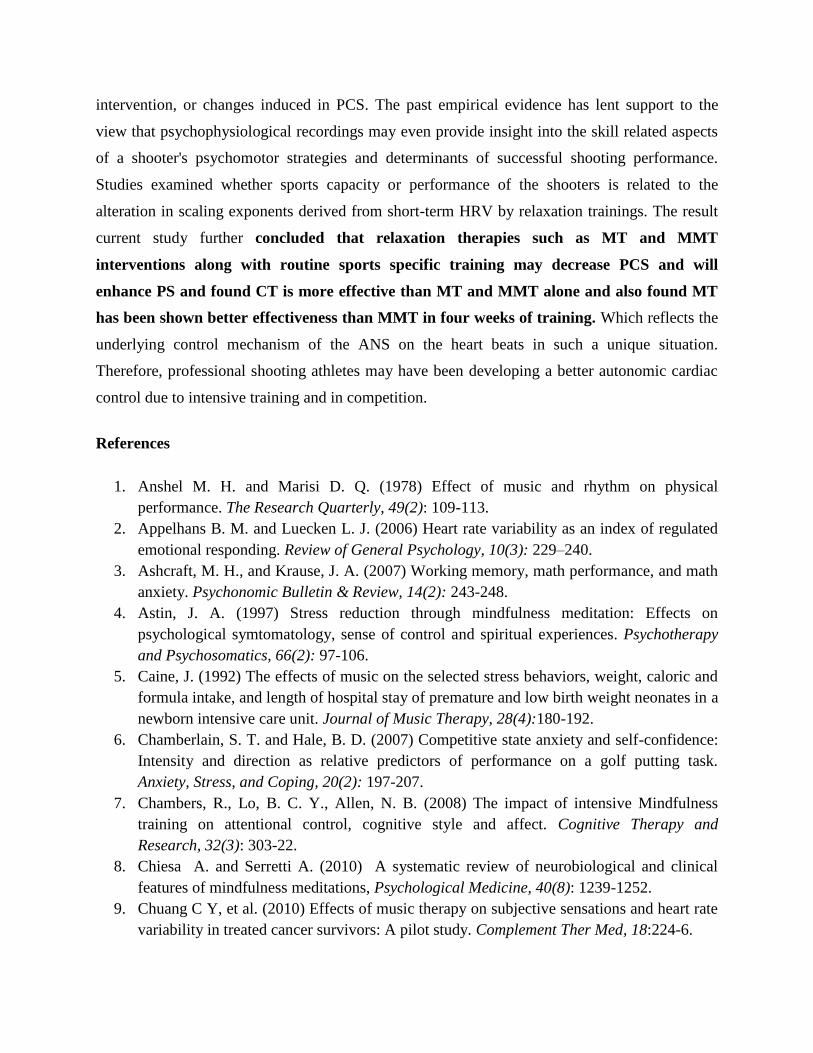
Performance Score: This study showed the pre and post competition PS of all three
interventions were increased (F=13.69; p<000.0001) whereas C group showed a decrease of PS.
In Group CT has shown more increase of PS in comparison with MT and MMT groups, whereas
MT showed an increase of PS than Group B. percentage values are 3%(544), 2.6% (542), 4.5%
(550) and 0.9% (518) for Groups A, B ,C, and D respectively (Graph1-4).

The result of the study indicated that there is an increase in post-intervention and follow-
up values in all interventional groups and combination was showing more effective, whereas the
control groups it was highly insignificant result. The reason for these changes might be
supported by studies on competition stress have been observed (Stephen et. al., 2009), supported
that, prior to competing, sport performers encounter more stressors pertinent to performance. The
level of anxiety automatically narrows perception restricting the focus of attention (Ashcraft and
Krause, 2007). Thus result of this study indicated that there is a decrease in control group and
increase in post intervention PS in all interventional groups; the reason for these changes might
be due to decrease in PCS.
Acute stress may affect cardiac function by shifting autonomic cardiac regulation in favor
of the sympathetic nervous system (Pacak and Palkovits 2001) thus during stress or anxiety the
nLF component of HRV increases. Cortisol is a hormonal response to acute stress and has been
measured to be higher before competition than at resting conditions (Salvador et al., 2003). SC
has been shown to reliably reflect levels of unbound cortisol in the blood and raised levels have
been found to be associated with stress in normal subjects (Kirschbaum and Hellhammer, 1994).
supported by studies on competition stress have been observed to decrease HRV, and alter the
power spectrum by decreasing the high frequency (HF) component, increasing the low frequency
(LF) component (Isowa et al. 2006). Based on these facts if any intervention is effective to
reduce competition stress then we observed the reversibility in behaviour of these markers that
will get an increase in HF and decrease in LF components of HRV and increase in SDNNi
component of HRV. The same phenomena observed with three different interventional groups
after receiving interventions.
Further, suggesting that relative increases in sympathetic nervous system activity during
stressful events (Sloan et al. 1994). It is also proved that there is an increase in parasympathetic
activity due to interventions of this study. Malfatto et al., (1996) explained the results regarding
elevation of SDNNi, the strongest prognostic HRV markers, have been supported with an
explanation. Thus in this study SDNNi component showed elevation from their baseline values
after interventions. McCraty et al., (1995) also supported that the positive emotions resulting
from relaxation therapies may significantly augment the HF component of a power spectrum
whereas the opposite occurs with negative emotions that happens with competition stress.
Therefore, HRV analysis provides a means of assessing the rhythmical changes that occur in

instantaneous heart rate (R-R intervals) in response to alterations in sympathovagal balance. By
relaxing music increases in parasympathetic activity decrease heart rate and increase HRV
(White, 1999). Current study also supports the increase of nHF and decrease of nLF in all music
interventional groups.
Music affects a reduction in sympathetic nervous control and therefore a reduction in
heart and respiration rates, metabolism, oxygen consumption, muscle tension, (Lee et al., 2005).
Reduced heart and respiration rates lead to less anxiety and can promote relaxation. These
studies support the reduction of nLF component in groups involved with music.
Listening to classical music increases heart rate variability, whereas listening to noise or
rock music decreases heart rate variability (reflecting greater stress) (Chuang et al., 2010).
Current study also given music therapy based on classical music that might have increased HRV
in groups which have under gone music interventions.
As repeated listening to music affects people's preference for it as well as their
physiological responses to it (Knight and Rickard, 2001), the HF component of HRV might be
increased with repeated listening. Music appears to exert direct physiological effects through the
autonomic nervous system. In the current study have given 20 minutes session for 4 weeks this
could supports the more effect of meditation in frequency components than music.
During guided relaxation, there was a reduction in the power of the low-frequency (LF)
component of the HRV spectrum and an increase in the power of the high-frequency (HF)
component, which suggested a reduction in sympathetic nervous system activity (Vempati and
Telles, 2002). HRV can be influenced by different patterns of breathing, breathing patterns
investigated in parallel to HR to determine the role of lengthening or shortening R-R interval in
the decision making process to pull the trigger. Thus in our study we included meditation
training. One of the aims of this experiment was to show the effects of paced breathing at 0.2 Hz
in meditation, compared to uncontrolled breathing, on time and frequency domain measures of
heart rate variability. The results showed a significant trend for paced breathing at 0.2 Hz to
increase HRV in the time domain, measured by SDNNi, and to shift sympathovagal balance,
measured by LF/HF spectral power, toward greater sympathetic activity. Because of the
respiration-related variability (respiratory sinus arrhythmia) of electrocardiogram inter-beat (RR)
intervals, the necessity of controlling respiratory frequency during measurements of HRV has
been demonstrated, several mechanisms have been attributed to this observation, e.g., the

respiratory sinus arrhythmia might be amplified due to increased tidal volume (De Meersman et
al. 1995). Tidal volume is also reported to be a modulator of the heart rate variability spectrum
by increasing high frequency power (Grossman et al. 2004) and 0.2 Hz paced breathing usually
increases tidal volume (Pinna et al. 2006). The activity of the vagal nerve endings increases
during exhalation, and the activity of sympathetic fibers increases during inhalation, causing the
“respiratory modulation” (RM) or “sinus arrhythmia”, i.e., during inhalation the heartbeat
intervals shorten and during exhalation they stretch. The oscillation in vagal action is responsible
for most of the RM, because it is faster than the sympathetic action. In summary, these factors
could have been helped to enhance further improvement nHF and nLF component of HRV in
MMT than MT alone training.
The combination effect supported by MT studies also indicate that music and
progressive muscle relaxation has effective outcomes in controlling muscle tension, anxiety,
sleep quality, and reducing stress (Hernandez-Ruiz, 2005). In addition, lower anxiety is expected
to promote psychological well being by decreasing plasma norepinephrine and cortisol (Mockel
et al., 1994) and enhancing relaxation and calmness. Therefore, soothing music was expected to
have a therapeutic effect on relaxation.
Meditation has been shown to decrease cortisol levels in populations of healthy
volunteers, but the effect of MMT program in PCS and release of SC levels has not previously
been evaluated in sports population. However, there has been some investigation of the effects of
psychosocial intervention on cortisol levels in normal and patient population. Tang et al., (2007)
supported by participants who meditated had better attentional processing on alerting function as
well as better mood, lower cortisol, and better immune function, allowing to conclude that
randomly assigned short-term intensive meditation causes immediate benefits. Studies reported
long-term endocrinologic changes in cortisol in subjects practicing transcendental meditation
(TM). Walton et al., (1995) found low concentrations of the blood levels of cortisol in TM
practitioners, in comparison with nonpracticing subjects. Music listening may influence
cognitive functioning via alternate pathways by helping to better organize cortical brain
transmissions (Rauscher et al., 1993), this might have improved performance.
These observations highlight that all the demands faced by athletes should be considered
when preparing and implementing interventions to manage competition stress. Result of the
current study showed all interventional groups have been shown some amount of follow up
effects even after one week of intervention this is supported by studies such as, (Caine, 1992)

found evidence that playing recorded music for infants in the neonatal intensive care unit
increased weight gain and shortened lengths of stay. Moreover, a follow-up study of the infants
that participated in Caine's music listening study indicated that infants who participated in the
music intervention were rated as calmer by their mothers at 6 months of age compared to infants
without music intervention. The results concerning the affective component of symptom changes
showed that the effect of music therapy was sustained. One week after the discontinuation of
sessions. Crocker et al., (1988) found evidence that post meditation there was significant com-
petitive performance improvements, and these improvements were maintained at 6-month
follow-up.
Future Research
The neuroendocrine scientific studies of music and meditation is clearly still in its
infancy, but the initial findings reviewed earlier promise both to reveal the mechanisms by which
such training might exert its effects on relaxation that underlie complex regulatory mental
functions. It seems that music and meditation can exert physiological effects through the
autonomic nervous system, but the factors directly involved are still unknown. These findings
will need to be supplemented with more data, most crucially from longitudinal studies examining
changes over time within the same individuals randomized either to music or meditation training
or to an active control group. The impact of relaxation or mental training on peripheral biological
processes that are important for physical health and illness is not yet clear. Although several
clinical studies have reported changes in, there are no data that mechanistically link changes in
the brain that might be produced by music or meditation, and alterations in peripheral processes,
further study is required to enable music and meditation related interventions to be accepted by
the sports science community on the basis of strong empirical evidence. Specifically, now that
the benefits of music and meditation have been repeatedly demonstrated in laboratory settings,
more ecologically valid and group-based research methods would serve to bolster the knowledge
base. Further work is needed to investigate subjects, measurement indicators, and experimental
conditions to clarify the relationship between physiological changes and emotional responses
produced by music or meditation.
Conclusion
To our knowledge, the HRV and SC have been little evaluated in young athletes and, in
such conditions of pre-competitive stress and post relaxation therapies. This work was made
possible to find out the changes on the neuroendocrine (ANS and HPA axis) activity during
intervention, or changes induced in PCS. The past empirical evidence has lent support to the
view that psychophysiological recordings may even provide insight into the skill related aspects
of a shooter's psychomotor strategies and determinants of successful shooting performance.
Studies examined whether sports capacity or performance of the shooters is related to the
alteration in scaling exponents derived from short-term HRV by relaxation trainings. The result
current study further concluded that relaxation therapies such as MT and MMT
interventions along with routine sports specific training may decrease PCS and will
enhance PS and found CT is more effective than MT and MMT alone and also found MT
has been shown better effectiveness than MMT in four weeks of training. Which reflects the
underlying control mechanism of the ANS on the heart beats in such a unique situation.
Therefore, professional shooting athletes may have been developing a better autonomic cardiac
control due to intensive training and in competition.
References
1. Anshel M. H. and Marisi D. Q. (1978) Effect of music and rhythm on physical
performance. The Research Quarterly, 49(2): 109-113.
2. Appelhans B. M. and Luecken L. J. (2006) Heart rate variability as an index of regulated
emotional responding. Review of General Psychology, 10(3): 229–240.
3. Ashcraft, M. H., and Krause, J. A. (2007) Working memory, math performance, and math
anxiety. Psychonomic Bulletin & Review, 14(2): 243-248.
4. Astin, J. A. (1997) Stress reduction through mindfulness meditation: Effects on
psychological symtomatology, sense of control and spiritual experiences. Psychotherapy
and Psychosomatics, 66(2): 97-106.
5. Caine, J. (1992) The effects of music on the selected stress behaviors, weight, caloric and
formula intake, and length of hospital stay of premature and low birth weight neonates in a
newborn intensive care unit. Journal of Music Therapy, 28(4):180-192.
6. Chamberlain, S. T. and Hale, B. D. (2007) Competitive state anxiety and self-confidence:
Intensity and direction as relative predictors of performance on a golf putting task.
Anxiety, Stress, and Coping, 20(2): 197-207.
7. Chambers, R., Lo, B. C. Y., Allen, N. B. (2008) The impact of intensive Mindfulness
training on attentional control, cognitive style and affect. Cognitive Therapy and
Research, 32(3): 303-22.
8. Chiesa A. and Serretti A. (2010) A systematic review of neurobiological and clinical
features of mindfulness meditations, Psychological Medicine, 40(8): 1239-1252.
9. Chuang C Y, et al. (2010) Effects of music therapy on subjective sensations and heart rate
variability in treated cancer survivors: A pilot study. Complement Ther Med, 18:224-6.

10. Cohn, P. J. (1990) An exploratory study on sources of stress and athlete burnout in youth
golf. The Sport Psychologist, 4(2): 95-106.
11. Copeland, B. L. and Franks, B. D. (1991) Effects of types and intensities of background
music on treadmill endurance. The Journal of Sports Medicine and Physical Fitness,
15(1):100-103.
12. Coulter, H.D. (Ed.) (2001) Relaxation and meditation. In: Anatomy of Hatha Yoga: Body
and Breath, first ed. Inc. Honesdale, pp. 547–557.
13. Craft, L. L., Magyar, M., Beaker, B. J., Feltz, D. L. (2003) The relationship between the
Competitive State Anxiety Inventory-2 and sport performance: A meta-analysis. Journal
of Sport and Exercise Psychology, 25: 44-65.
14. Crocker, R R. E, Alderman, R. B., Smith, M. R. (1988) Cognitive-affective stress
management training with high performance youth volleyball players: Effects on affect,
cognition, and performance. Journal of Sport and Exercise Psychology, 10:448-460.
15. De Meersman, R.E., Reisman, S.S., Daum, M., Zorowitz, R., Leifer M, Findley, T. (1995)
Influence of respiration on metabolic, hemodynamic, psychometric, and R–R interval
power spectral parameters. American Journal of Physiology, 269 (4Pt2): 1437–1440.
16. Fabes, R. A., and Eisenberg, N. (1997) Regulatory control and adults’ stress-related
responses to daily life events. Journal of Personality and Social Psychology, 73(5): 1107–
1117.
17. Ferguson, A. R., Carbonneau, M. R., Chambliss, C. (1994) Effects of positive and
negative music on performance of a karate drill. Perceptual and Motor Skills, 78 (3 Pt 2):
1217–1218.
18. Filaire, E., Alix, D., Rouveix, M., Le Scanff, C. (2007) Motivation, stress, anxiety, and
Cortisol responses in elite paragliders. Perceptual and Motor Skills, 104(3 Pt 2): 1271-
1281.
19. Filaire, E., Sagnol, M., Ferrand, C, Maso, F., Lac, G. (2001) Psychophysiological stress in
judo athletes during competitions. Journal of Sports Medicine and Physical Fitness, 41(2):
263-268.
20. Friedman, B.H., Thayer, J.F. (1998) Autonomic balance revisited: panic anxiety and heart
rate variability. J. Psychosom. Res., 44(1): 133–151.
21. Geisler, F. C. M. and Kubiak, T. (2009) Heart rate variability predicts self-control in goal
pursuit. European Journal of Personality, 23: 623–633.
22. Gould, Eklund and Jackson. (1988) U.S. Olympic wrestling excellence: I. mental
preparation, precompetitive cognition, and affect, The Sport Psychologist, 6(4): 358 - 382.
23. Grossman P, Wilhelm FH, Spoerle M. (2004) Respiratory sinus arrhythmia, cardiac vagal
control, and daily activity. American Journal of Physiology Heart and Circulatory
Physiology 287 (2):728–734.
24. Haneishi, K., Fry, A. C, Moore, C. A., Schilling, B. K., Li, Y. (2007) Cortisol and stress
responses during a game and practice in female collegiate soccer players. Journal of
Strength and Conditioning Research, 21: 583-588.
25. Hernández-Ruiz E. (2005) Effect of music therapy on the anxiety levels and sleep patterns
of abused women in shelters. J Music Ther. Summer, 42(2):140-58.
26. Isowa T, Ohira H, Murashima S. (2006) Immune, endocrine and cardiovascular responses
to controllable and uncontrollable acute stress. Biol Psychol., 71:202-213.
27. Jackson, S. A. and Roberts, G. C. (1992) Positive performance states of athletes: Towards
a conceptual understanding of peak performance. The Sport Psychologist, 6: 156-171.
28. Kais, K. and Raudsepp, L. (2005) Intensity and direction of competitive state anxiety, self-
confidence and athletic performance. Kinesiology, 37: 13-20.
29. Karageorghis, C. I., Drew, K. M., & Terry, P. C. (1996). Effects of pretest stimulative and
sedative music on grip strength. Perceptual and Motor Skills, 83, 1347–1352.
30. Kirschbaum C. and Hellhammer, D H. (1994) Salivary cortisol in psychoneuroendocrine
research: recent developments and applications. Psychoneuroendocrinology, 19(4): 313-
333.
31. Knight WEJ. and Rickard NS. (2001) Relaxing music prevents stress-induced increases in
subjective anxiety, systolic blood pressure and heart rate in healthy males and females.
Journal of Music Therapy, 38(4):254-272.
32. Lee OK et al., (2005) Music and its effect on physiological and anxiety levels of patients
receiving mechanical ventilation: a pilot study. Journal of Clinical Nursing, 14(5): 609-
620.
33. Maddan, Summers. and Brown. (2004) Coping behavior and susceptibility to chocking.
Journal of sports Behavior, 2: 7-23.
34. Malfatto G, Facchini M, Bragato R, Branzi G, Sala L, Leonetti G.( 1996) Short and long
term effects of exercise training on the tonic autonomic modulation of heart rate
variability after myocardial infarction. Eur Heart J, 17:532–8.
35. McCraty, R., Atkinson, M., Tiller, W.A., Rein, G., Watkins, A.D. (1995) The effects of
emotions on short-term power spectrum analysis of heart rate variability. Am. J. Cardiol.
76: 1089–1093.
36. Mockel M, Rocker L, Stork T, et al., (1994) Immediate physiological responses of healthy
volunteers to different types of music: cardiovascular, hormonal and mental changes. Eur
J Appl Physiol Occup Physiol, 68:451-9.
37. Mononen K, Konttinen N, Viitasalo J, Era P. (2007) Relationships between postural
balance, rifle stability and shooting accuracy among novice rifle shooters. Scand J Med
Sci Sports, 17:180–5.
38. Pacak K, Palkovits M, (2001) Stressor specificity of central neuroendocrine responses:
implications for stress-related disorders. Endocr Rev 22:502–548.
39. Pinna GD, Maestri R, La Rovere MT, Gobbi E, Fanfulla F. (2006) Effect of paced
breathing on ventilatory and cardiovascular variability parameters during short-term
investigations of autonomic function. American Journal of Physiology. Heart and
Circulatory Physiology 290 (1): 424–433.

40. Rauscher FH, Shaw GL, Ky KN. (1993) Music and spatial task performance. Nature
365:611.
41. Salvador, A., Suay, F., Gonzalez-Bono, E., Serrano, M. A. (2003) Anticipatory Cortisol,
testosterone and psychological responses to judo competition in young men.
Psychoneuroendocrinology, 28: 264-375.
42. Scanlan, Ravizza. and Stein. (1989) An in-depth study of Former Elite Figure Skaters: II.
sources of enjoyment. Journal of Sport & Exercise Psychology 11(1): 65 - 83.
43. Segerstrom, S. C. and Solberg Nes, L. (2007) Heart rate variability reflects self regulatory
strength, effort, and fatigue. Psychological Science, 18: 275–281.
44. Sloan RP, Shapiro PA, Bagiella E, Myers MM, Bigger JT, Steinman R C. (1994) Brief
interval heart period variability by different methods of analysis correlates highly with 24-
h analyses in normals. Bio- Psychol., 38(2–3):133–42.
45. Smith. R. E., Smoll, F. L., Weichinan, S. A. (1998) Measurement of trait anxiety in sport.
In J. L Duda (Ed.), Advances in Sport and Exercise Psychology Measurement, pp.105-
128.
46. Solberg, E. E. and Bergulund, K A. (1996) The effect of meditation on shooting
performance. British Journal of Sports Medicine, 30(4):342-346.
47. Stephen D Mellalieu, Richard Neil, Sheldon Hanton, David Fletcher. (2009) Competition
stress in sport performers: Stressors experienced in the competition environment. J Sports
Sci., 27(7):729-44.
48. Tang, Y., Ma, Y., Wang, J., Feng, S., Yu, Q., Rothbart, M. K., et al., (2007) Short-term
meditation training improves attention and self- regulation. PNAS Proceedings of the
National Academy of Sciences of the United States of America, 104:17152–17156.
49. Terry, P. C. and Slade, A. (1995) Discriminate effectiveness of psychological state
measures in predicting performance outcome in karate competition. Perceptual and Motor
Skills, 81(1): 275-286.
50. Tremayne, P. and Barry, R. J. (2001) Elite pistol shooters: Physiological patterning of best
vs. worst shots. International Journal of Psychophysiology, 41: 19–29.
51. Vempati, R.P. and Telles, S. (2002) Yoga-based guided relaxation reduces sympathetic
activity judged from baseline levels. Psychological Reports 90 (2): 487–494.
52. Walton KG, Pugh ND, Gelderloos P and Macrae P. (1995) Stress reduction and
preventing hypertension: preliminary support for a psychoneuroendocrine mechanism.
Journal of Alternative Complementary Therapy; 1(3): 263-283.
53. Whelan, J. P., Mahoney, M. J., Meyers, A. W. (1991) Performance enhancement in sport:
A cognitive behavioral domain. Behavior Therapy, 22: 307-327.
54. White J M. (1999) Effects of relaxing music on cardiac autonomic balance and anxiety
after acute myocardial infarction, Am J Crit Care 8(4): 220-230.
Graphs and Tables
Graph 1: Bland and Altman plot—Comparison of pre and post performance values of
study subjects who had MT as intervention
350 400 450 500 550 600
8
6
4
2
0
-2
-4
-6
AVERAGE of Score29 and Score0
(Sco
re2
9 -
Sco
re0
) /
Ave
rag
e %
Mean
2.9
-1.96 SD
-1.3
+1.96 SD
7.2
460 480 500 520 540 560 580 600
10
8
6
4
2
0
-2
-4
-6
-8
-10
AVERAGE of Score29 and Score0
(Sco
re2
9 -
Sco
re0
) /
Ave
rag
e %
Mean
2.6
-1.96 SD
-2.4
+1.96 SD
7.6

Graph 2: Bland and Altman plot—Comparison of pre and post performance values of
study subjects who had MMT as intervention
Graph 3: Bland and Altman plot—Comparison of pre and post performance values of
study subjects who had combination of CT as intervention
480 500 520 540 560 580 600
20
15
10
5
0
-5
AVERAGE of Score29 and Score0
(Sco
re2
9 -
Sco
re0
) /
Ave
rag
e %
Mean
4.5
-1.96 SD
-2.5
+1.96 SD
11.5
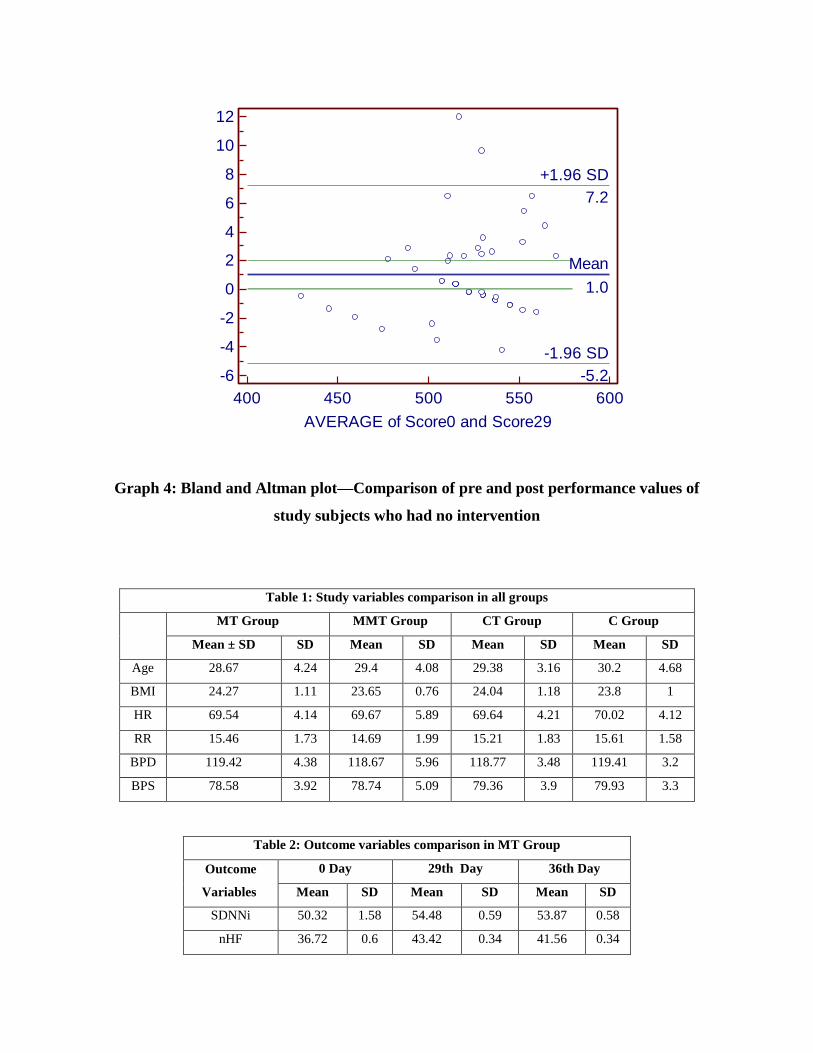
Graph 4: Bland and Altman plot—Comparison of pre and post performance values of
study subjects who had no intervention
Table 1: Study variables comparison in all groups
MT Group MMT Group CT Group C Group
Mean ± SD SD Mean SD Mean SD Mean SD
Age 28.67 4.24 29.4 4.08 29.38 3.16 30.2 4.68
BMI 24.27 1.11 23.65 0.76 24.04 1.18 23.8 1
HR 69.54 4.14 69.67 5.89 69.64 4.21 70.02 4.12
RR 15.46 1.73 14.69 1.99 15.21 1.83 15.61 1.58
BPD 119.42 4.38 118.67 5.96 118.77 3.48 119.41 3.2
BPS 78.58 3.92 78.74 5.09 79.36 3.9 79.93 3.3
Table 2: Outcome variables comparison in MT Group
Outcome
Variables
0 Day 29th Day 36th Day
Mean SD Mean SD Mean SD
SDNNi 50.32 1.58 54.48 0.59 53.87 0.58
nHF 36.72 0.6 43.42 0.34 41.56 0.34
400 450 500 550 600
12
10
8
6
4
2
0
-2
-4
-6
AVERAGE of Score0 and Score29
(Sco
re0
- S
co
re2
9)
/ A
ve
rag
e %
Mean
1.0
-1.96 SD
-5.2
+1.96 SD
7.2

nLF 63.44 0.26 56.58 0.34 58.44 0.34
SC 1.33 0.06 0.53 0.07 0.91 0.11
PS 528.52 29.1 544.31 30.64
Table 3: Outcome variables comparison in MMT Group
Outcome
Variables
0 Day 29th Day 36th Day
Mean SD Mean SD Mean SD
SDNNi 50.05 1.42 52.91 0.56 52.7 0.3
nHF 35.79 4.85 44.53 0.15 42.24 0.12
nLF 63.33 0.27 55.47 0.15 57.76 0.12
SC 1.33 0.06 0.66 0.07 0.93 0.11
PS 528.04 25.26 541.69 25.11
Table 4: Outcome variables comparison in CT Group
Outcome
Variables 0 Day 29th Day 36th Day
Mean SD Mean SD Mean SD
SDNNi 50.15 0.57 56.78 1.21 55.57 1.16
nHF 36.74 1.1 45.53 0.01 44.44 0.21
nLF 63.02 0.68 54.47 0.01 55.56 0.21
SC 1.33 0.15 0.33 0.07 0.45 0.08
PS 525.87 25.89 549.72 18.66
Table 5: Outcome variables comparison in C Group
Outcome
Variables
0 Day 29th Day 36th Day
Mean SD Mean SD Mean SD
SDNNi 50.28 2.38 48.03 0.89 48.2 0.76
nHF 36.67 0.21 33 0.25 33.95 0.05
nLF 63.33 0.21 70 0.25 66.05 0.05
SC 1.33 0.06 1.95 0.08 1.6 0.11
PS 522.96 31.14 518.04 28.1
Table 6: Outcome variable-SDNNi comparison in all Groups
SDNNi
Variable
MT Group MMT Group CT Group C Group
Mean SD Mean SD Mean SD Mean SD

SDNNi-0 50.32 1.58 50.05 1.42 50.15 0.57 50.28 2.38
SDNNi-29 54.48 0.59 52.91 0.56 56.78 1.21 48.03 0.89
SDNNi-36 53.87 0.58 52.7 0.3 55.57 1.16 48.2 0.76
Table 7: Outcome variable-nHF comparison in all Groups
nHF
Variable
MT Group MMT Group CT Group C Group
Mean SD Mean SD Mean SD Mean SD
nHF-0 36.72 0.6 35.79 4.85 36.74 1.1 36.67 0.21
nHF-29 43.42 0.34 44.53 0.15 45.53 0.01 33 0.25
nHF-36 41.56 0.34 42.24 0.12 44.44 0.21 33.95 0.05
Table 8: Outcome variable-nLF comparison in all Groups
nLF
Variable
MT Group MMT Group CT Group C Group
Mean SD Mean SD Mean SD Mean SD
nLF-0 63.44 0.26 63.33 0.27 63.02 0.68 63.33 0.21
nLF-29 56.58 0.34 55.47 0.15 54.47 0.01 70 0.25
nLF-36 58.44 0.34 57.76 0.12 55.56 0.21 66.05 0.05
Table 9: Outcome variable-SC comparison in all Groups
SC
Variable
MT Group MMT Group CT Group C Group
Mean SD Mean SD Mean SD Mean SD
SC-0 1.33 0.06 1.33 0.06 1.33 0.15 1.33 0.06
SC-29 0.53 0.07 0.66 0.07 0.33 0.07 1.95 0.08
SC-36 0.91 0.11 0.93 0.11 0.45 0.08 1.6 0.11
One way Analysis of Variance
Table 10: Comparison of mean values of study variables at 3 stages in male shooters among
the 4 study groups
Sum of
Squares
df Mean Square F Sig.

Age- Between Groups
Within Groups
Total
56.59
3208.61
3265.21
3
195
198
18.86
16.45
1.15
.332
BMI- Between Groups
Within Groups
Total
11.12
202.37
213.50
3
195
198
3.71
1.04
3.57 .015
HR- Between Groups
Within Groups
Total
6.34
4190.76
4197.10
3
195
198
2.11
21.49
.10 .961
RR- Between Groups
Within Groups
Total
23.51
626.91
650.42
3
195
198
7.84
3.22
2.44 .066
BPD- Between Groups
Within Groups
Total
24.36
3737.79
3762.15
3
195
198
8.12
19.17
.42 .736
BPS- Between Groups
Within Groups
Total
55.93
3280.06
3335.99
3
195
198
18.64
16.82
1.11 .347

One way Analysis of Variance
Table 11: Comparison of mean values of outcome variables at 3 stages in male shooters of 4 study
groups
Sum of Squares df Mean Square F Sig.
SDNNi 0- Between Groups
Within Groups Total
2.27
493.97 496.24
3
195 198
.76
2.53
.29 .827
SDNNi 29- Between Groups
Within Groups
Total
1998.61
143.43
2142.04
3
195
198
666.20
.74
905.76 .000
SDNNi 36- Between Groups
Within Groups
Total
1435.73
117.13
1552.86
3
195
198
478.58
.601
796.73 .000
nHF 0- Between Groups
Within Groups
Total
30.76
1187.33
1218.09
3
195
198
10.25
6.09
1.68 .172
nHF 29- Between Groups
Within Groups
Total
4790.12
9.57
4799.69
3
195
198
1596.71
.05
3.26 .000
nHF 36- Between Groups
Within Groups
Total
2989.13
9.00
2998.13
3
195
198
996.38
.05
2.16 .000
nLF 0- Between Groups
Within Groups
Total
5.19
33.15
38.34
3
195
198
1.73
.17
10.18 .000
nLF 29- Between Groups
Within Groups
Total
4790.12
9.57
4799.69
3
195
198
1596.71
.05
3.26 .000
nLF 36- Between Groups
Within Groups
Total
2989.13
9.00
2998.13
3
195
198
996.38
.05
2.16 .000
SC 0- Between Groups
Within Groups
Total
.00
1.65
1.65
3
195
198
.000
.008
.02 .995
SC 29- Between Groups
Within Groups
Total
76.74
.95
77.69
3
195
198
25.58
.01
5.25 .000
SC 36- Between Groups
Within Groups
Total
32.81
2.16
34.97
3
195
198
10.94
.01
986.67 .000
PS 0- Between Groups
Within Groups
Total
923.33
151648.89
152572.21
3
195
198
307.78
777.69
.40 .756
PS 29- Between Groups
Within Groups
Total
28100.54
133436.06
161536.59
3
195
198
9366.85
684.29
13.69 .000

Mindfulness Meditation on HPA-Axis
The Effect of Mindfulness Meditation on HPA-Axis in Pre-Competition Stress in Sports Performance of Elite Shooters
Dr. Shaji John*, Dr. S. K Verma**, Dr. G. L Khanna***
*Researcher, College of Applied Medical Sciences, King Saud University, KSA, **Professor, Department of Sports Sciences, Punjabi University, India, ***Professor, Faculty of Applied Medical Sciences, Manav Rachna International University, India.
Abstracts: Background: Little has been known about the Hypothalamic Pituitary Adrenal (HPA) axis response to pre-competition stress (PCS) and its response to relaxation therapies such as of Mindfulness Meditation Therapy (MMT) on sports population. In shooting sports good physical as well as psychological condition is highly demanded. Researchers have been performed on the psychophysiological responses of MMT on normal and diseased persons, but little has been done on sports population especially in shooters. Objective: The purpose of current study was to estimate the contribution of MMT on Salivary Cortisol (SC), a reliable physiological marker of HPA- axis response in reducing PCS, and its effect on shooting performance (PS). Methods: 96 male elite Shooters, with mean age of 29.5±4.3years were examined as in experimental and control (48 in each). Total duration of the study was five weeks, four weeks of experimental and one week study to determine the follow-up effect. Pre, post and follow-up data of quantitative phenotypic markers of HPA-Axis activity by analysis of SC and PS were analyzed. Results: Compare to control, experimental group has shown significant result, post-intervention (p<0.001) and in follow-up (p<0.001) in SC and in PS. Resulted in reduction of PCS level and increase in PS, whereas the control group has been shown non-significant result (p<0.05).Conclusions: Results indicated that relaxation therapies such as MMT may decrease PCS and will enhance PS. It is concluded that in four weeks of MMT has an effect on HPA-Axis by decreasing the level of SC as a reliable physiological marker of PCS. [ John S NJIRM 2011; 2(3) : 15-21] Key Words: HPA, Cortisol, Pre competition Stress, Meditation, Shooting.
Author for correspondence: Shaji John, Researcher, College of Applied Medical Sciences, King Saud University, P O Box;10219, Riyadh 11433, KSA., E-mail:[email protected]
Introduction: Air pistol shooting is an Olympic sport requiring extreme mental concentration and movement precision for success. Pistol shooting is a static activity requiring a strict control of body segments and posture to align the rear sight aperture and the foresight through proprioceptive feedback and gaze fixation either on the target directly or between the target and the weapon and, therefore, to increase precision of the shot1. Compared to that for rifle shooting, there is very little literature related to pistol shooting. In this work, we investigated pistol shooting.
Stress is most often used to describe an unpleasant emotional state or condition which is characterized by subjective feelings of tension, apprehension, and worry. In sports context it is commonly known as pre-competition stress or anxiety. Further, research indicated that anxiety has a negative effect on these sport outcomes2. Research findings suggest that, prior to competing; sport performers encounter more stressors pertinent to
NJIRM 2011; Vol. 2(3). July- September
performance3. These observations highlight that all the demands faced by athletes should be considered when preparing and implementing interventions to manage competition stress. Pre-competition anxiety is a widely prevalent condition that exists among athletes of all levels and within every sport 4 , 5 , 6. Despite the large body of research on pre-competition anxiety, our understanding of its relationship to performance remains elusive.
Cortisol is a hormonal response to acute stress and has been measured to be higher before competition than at resting conditions7. Some researchers have found that athletes produce higher levels of Cortisol before games than before non-competition situations 8 , 9 , 1 0 , 7. The results support previous findings that athletes are more anxious before games than during off days1 1. Research findings comparing the physiological and psychological markers of stress have been equivocal9.
eISSN: 0975-9840 pISSN: 2230 - 9969 I 15
Mindfulness Meditation on HPA-Axis
Relaxation techniques have been used in sports primarily to enhance recovery from training and competition, manage anxiety and improve performance12. The techniques of mindfulness meditation which focus on awareness to develop a detached observation of the contents of consciousness may represent a powerful cognitive behavioural coping strategy for transforming the ways in which we respond to life events1 3. Even though many studies on MMT have been criticized for the lack of scientific rigor, including the lack of high quality randomized controlled studies designed to differentiate between the specific (i.e. specifically related to repeated sitting meditation practice) and the non specific (i.e. related to benefits' expectations) effects of such practices14, and the frequent use of self report instruments as measures of clinical improvements following MMT 1 5 .
The present study focused on examining the relation of physiological response to skilled sport performance, and investigating the relevance of MMT in pre-competition anxiety. For this purpose, Salivary Cortisol (SC) were recorded during the training and pre-competition phase of actual shooting.
Material and Methods: Subjects: A total of 110 healthy male elite level shooters with mean age of (29.5±4.3years) selected for the study. Subjects were voluntarily recruited from national shooting team; permission was obtained from officials. Questionnaires administered prior to the experiment were indicated that no volunteers are included as per exclusion criteria such as any physical or mental illness, hearing impairment, and have been undergoing meditation therapies for last 3 months. All subjects were nonsmokers, medication-free and not habitual drinkers. The aims of the present study, the procedures involved and potential risks of the study were explained carefully to subjects, and the written consent was obtained prior to the study. The study and all protocols were approved by research ethical committee of Punjabi University.
Participants were randomly allocated into two groups; experimental (MMT) and Control by multiple blocked random sampling of 55 in each
NJIRM 2011; Vol. 2(3). July- September
group, after the dropout 96 subjects could complete the study in each group. The baseline values of Heart Rate (70±3bpm), Respiratory Rate (15±2rpm), BMI (24±1.04kg/cm2) and Blood Pressure (119±4/79±4 mm of Hg) were documented. For the better understanding of Interventions a sample trial was conducted to the experimental subjects one week prior to the study. Concerning impediments to effective practice, subjects were monitored by the researcher and experts during the interventions. The intervention was provided over the course of four weeks and one week follow-up, group sessions with a maximum of 8 participants each, 20 minutes session per day, 6 days a week and one day was off per week. Participants were asked not to consume caffeine or alcoholic beverages for 12 h, and not to exercise for 12 h prior to the experiment especially during testing.
Procedure: The all participants of each batch reported to the laboratory at 08:00AM, each session conducted in the morning (between 8 AM and 10 AM) and The subject changed into loose fitting clothing, and shoes removed then the participants were instructed to lie in the supine position on the floor mat in a quiet, light-attenuated electrically shielded room with the temperature between 24 and 28 °C with their eyes closed.
Interventions; Mindfulness Meditation Therapy (MMT): The first step in performing a MMT is to adopt a posture that ensures an erect spine and shoulder resting on the mat, with the hands should be placed on the upper position of the abdomen, the position of head kept slightly foreword with the support of small towel roll. The eyes may be fully closed, or the upper lids may be dropped and was given 1 minutes of adaptation period. As a meditation condition progress, subjects were asked to undergo 3 minutes for stabilization by Shavasana, For Shavasana training the technique recommended by Coulter was used 2 8. The subject was asked to relax , after this, they performed meditation comprising a Pranayam for 4 min while situated as in the control condition (in the supine position with the eyes closed and respiration at a constant frequency of 0.2 Hz in tempo with the sound of a metronome (i.e., 5 breaths/min for 4
eISSN: 0975-9840 pISSN: 2230 - 9969 I 16

Mindfulness Meditation on HPA-Axis
min)). Then the participants were instructed mindfulness by body scan i.e. focusing attention on various joints of body by focuses on the each joint from proximal to distal as described and feels without labeling the sensations as either "good" or "bad" in a sequence from distal to proximal. Once they completes again for 4 minutes Pranayam at a constant frequency of 0.2 Hz in tempo with the sound of a metronome and ended with 3 minutes of Shavasana. Subjects were informed to raise their hands during any discomfort while doing meditation and if so they were asked to immediately stop the session. Subsequently, the participants left the room after 20 minutes of session.
Testing; The testing sessions were conducted between 8 am and 10 am and the same researcher tested all subjects. Measurement day scheduled one day prior to beginning the 1 s t week, 29 t h day and 36 t h day, subjects were assessed for pre-test, post-test and follow-up data respectively, except Performance Test, in a quiet controlled room with ambient temperature (24-280C). The performance score calculated by pre-scheduled a competition in a internationally standard shooting range on one day prior to beginning the 1 s t week, and on 29 t h
day, subjects were assessed for pre-test, post-test Performance score respectively.
All Participants were instructed to avoid consuming stimulant beverages, tea, and coffee; exercising, in the 12 hours previous to the examination. The all participants of each batch reported to the laboratory at 08:00AM, measurement procedure started between 09:00 am and 10:00 am, to control as much as possible for time of day, to avoid circadian variations. Prior to testing, Participants attended a detailed briefing session where they received full verbal instructions regarding the procedures of the study. SC samples were taken been 9:00 am -10:00 am to minimize time of day effects. All subjects were tested individually.
Salivary Cortisol; For obtaining the free, unbound, biologically active moiety of cortisol, saliva samples were collected. To rid the mouth of contaminates, subjects rinsed thoroughly with water ten minutes before saliva collection. Subjects sat unrestrained
NJIRM 2011; Vol. 2(3). July- September
in a comfortable chair with lumbar support, Subjects were then allowed to relax for five minutes, the experimenter then began each test session and collected minimum of 2 ml of saliva by tilting the head forward, allowing the saliva to pool on the floor of the mouth, then passing the saliva through a short straw into a polypropylene vial. The Salivary samples were labeled and sealed and refrigerated in an ice box within 30 minutes. After all procedures the sealed sample sends to the laboratory on the same day by 2:00 h to store under-15 degree centigrade to the laboratory for later analysis,
Free cortisol level data from the samples of saliva were analyzed in the laboratory by using Salimetric s T M salivary cortisol kit. On day of assay, samples brought at room temperature and thaw completely, vortex, and centrifuge at 1500 x g (@3000 rpm) for15 minutes before adding to assay plate and cortisol was assessed in via enzyme-linked immunosorbent assay as per manufacturer (SalimetricsTM) instructions.
Performance score; Measure of shooting accuracy or shooting score was calculated from the standard shooting scoring board and the final result of competition obtained from the chief coach after the completion of competition, in order to test shooting performance.
Result: Descriptive statistics of study and outcome variables measured in 48 subjects each in experimental and control group. The comparison of base line mean values of study variables (Table-1) and outcome variables (Table-2 ) among the 2 study groups, that is male shooters who had interventions: as MMT and control, shows a non statistically significant difference in the mean values of Age( F= 1.15; p= 0.332), BMI (F= 3.57; p=0.015), heart rate (HR)( F= 0.10;p=0.961), respiratory rate (RR)(F=2.44;p=0.066), diastolic blood pressure (BPD)(F=0.42;p=0.736), and systolic blood pressure (BPS) (F=1.11;p=0.347) and SC(F= 0.02; p = 0.995),,PS (F= 0.40; p = 0.756).
In MMT group, the mean values of Salivary Cortisol (SC) had statistically significantly decreased from the baseline value of 1.33 to 0.66 at 29 t h day and 0.93 at 36 t h day which is statistically significant
eISSN: 0975-9840 pISSN: 2230 - 9969 I 1 7

Mindfulness Meditation on HPA-Axis
(F=834.6;p<0.001).The post hoc pair wise comparison of these values indicates highly statistically significant difference among the values. From this it can be infer that the effect of meditation in this group has decreased the SC values significantly from their base line values. The mean value of performance score has statistically significantly increased from 528 to 544(t-value=-6.85, p<0.001) (Graph-1).
Table:1 Mean values of Study variables in comparison between MMT and Control groups
Study Variables
MMT Control Study Variables Mean ±SD Mean ±SD
Age 29.40 4.08 30.2 4.68
BMI 24 .8 24 1
HR 70 6 70 4
RR 15 2 16 2
BPD 119 6 119 3
BPS 79 5 80 3
Table:2 : Comparison of mean values of outcom variables at 3 stages in male shooters of study
Outcome Variable
MM T Group Control Group Outcome Variable Mean ±SD Mean ±SD
SC-0Day 1.33 0.06 1.33 0.06
SC-29th Day 0.66 0.07 1.95 0.08
SC-36th Day 0.93 0.11 1.6 0.11
PS-0Day 528 13 524 2
PS-29th Day 542 13 518 16
Graph- 1: Bland and Altman plot—Comparison of pre and post performance values of study subjects who had meditation as intervention
10
8
6
4
2
0
-2
-4
-6
-8
-10
O O Q O O O O C
7.6
Mean 2.6
-1.96 SD -2.4
460 480 500 520 540 560 580 A V E R A G E of Score29 and Score0
600
In control group, the mean values of Salivary Cortisol (SC) had statistically significantly increased
NJIRM 2011; Vol. 2(3). July- September
from the baseline value of 1.33 to 1.95 at 29 t h day and 1.60 at 36 t h day which is statistically significant (F=577.48;p<0.001).The post hoc pair wise comparison of values indicates highly statistically significant difference among the values. From this it can be infer that the effect of no meditation intervention in this group has increased the SC values significantly from their base line values. The mean value of performance score has statistically significantly decreased from 524 to 522 (t-value=0.65, p<0.001)(Graph-2).
Graph-2: Bland and Altman plot—Comparison of pre and post performance values of study subjects who had no intervention
-5.2,
450 500 550
A V E R A G E of Sco re0 and Score29
eISSN:
Discussion: In the current study, used Salivary Cortisol (SC) as physiological marker and Performance Score (PS) as subjective marker to assess the changes in groups. These parameters are very much reliable to provide true picture of changes and also susceptible for changes in pre competition anxiety or stress. This fact is supported by 8 , 1 0 and also supported by research findings comparing the physiological and psychological markers of stress have been equivocal9. Since the salivary cortisol assay has been proposed as the method of choice for assessing adrenocortical (endocrine) function. Thus in this study included SC as a physiological marker.
The result of the study indicated that there is an increase in post intervention and follow up values in MMT group whereas the control group, it was highly insignificant result. In MMT group, the cortisol level in saliva decreased in post-intervention and follow up. i.e. 50% (.66) and as follow up carry over decrease of 20% (.93). Whereas control group showed an increase of 47% (1.95) and 26% (1.60) pre-competition and post
0975-9840 pISSN: 2230 - 9969 I 18
+1.96 S D 7.2
Mean
1.0
-1.96 S D
400 600
+1.96 SD

Mindfulness Meditation on HPA-Axis
competition respectively. In performance score experimental group showed an increase of 2.6% (542) from base line (528), whereas control group showed decrease of 0.9% (518) from base line (524). The reason for these changes supported by studies on competition stress, supported that, prior to competing, sport performers encounter more stressors pertinent to performance3. The level of anxiety automatically narrows perception restricting the focus of attention 1 6 , 1 7 , 1 8 , 1 9 . Thus result of this study indicated that there is an decrease in control group and increase in post intervention performance score in all interventional groups; the reason for these changes might be due to decrease in pre competition anxiety.
Cortisol is a hormonal response to acute stress and has been measured to be higher before competition than at resting conditions7. In recent years, however, salivary cortisol has been shown to reliably reflect levels of unbound cortisol in the blood and raised levels have been found to be associated with stress in normal subjects20. Based on these facts if any intervention is effective to reduce competition stress then we observed the reversibility in behaviour of this marker. These observations highlight that all the demands faced by athletes should be considered when preparing and implementing interventions to manage competition stress.
Meditation has been shown to decrease cortisol levels in populations of healthy volunteers21 , but the effect of meditation training program in pre competition stress and release of cortisol levels has not previously been evaluated in Sports population. However, there has been some investigation of the effects of psychosocial intervention on cortisol levels in normal and patient population. Study supported by participants who meditated had better attentional processing on alerting function as well as better mood, lower cortisol, and better immune function, allowing to conclude that randomly assigned short-term intensive meditation causes immediate benefits. This might have improved performance22.
Result of the current study showed intervention group has been shown some amount of follow up
NJIRM 2011; Vol. 2(3). July- September
effects even after one week of intervention this is supported by studies such as, found evidence that post meditation there was significant competitive performance improvements, and these improvements were maintained at 6-month follow-up 2 3.
Conclusion: The past empirical evidence has lent support to the view that psychophysiological recordings may even provide insight into the skill related aspects of a shooter's psychomotor strategies and determinants of successful shooting performance. Results of this study showed positive correlation in MMT than controlled group in one month duration training. It has shown improvement in dependent variables such as decrease salivary cortisol and Performance score of individual shooter. As previous studies the long term training may enhance the further in experimental group. It is suggested that the intensity of improvement and follow-up effect shall be analyzed and compared in long duration interventional training i.e. more than a month. To our knowledge until HPA- Axis has been little evaluated in young athletes, especially in such conditions of pre-competitive stress and efficacy of post relaxation therapies. This work was made possible to find out the changes on the endocrine (HPA axis) activity during intervention, or changes induced in pre-competition stress. Although short-term activations of the HPA axis are adaptive and necessary for everyday functioning, extreme, frequent or chronic activation of this system are associated with negative health outcomes. Existing research has implicated the HPA axis in the development of a variety of sub-clinical and clinical conditions including metabolic syndrome2 4, depression2 5, risk for cardiovascular disease26 and cognitive decline2 7.
References: 1. Mononen K, Konttinen N, Viitasalo J, Era P.
Relationships between postural balance, rifle stability and shooting accuracy among novice rifle shooters. Scand J Med Sci Sports. 2007; 17:180-5.
2. Terry, P. C., & Slade, A. Discriminate effectiveness of psychological state measures in predicting performance outcome in karate
eISSN: 0975-9840 pISSN: 2230 - 9969 I 19

Mindfulness Meditation on HPA-Axis
competition. Perceptual and Motor Skills. 1995; 81(i): 275-286.
3. Stephen D Mellalieu, Richard Neil, Sheldon Hanton, David Fletcher. Competition stress in sport performers: Stressors experienced in the competition environment. Psychology of sport and exercise. 2009; 27 (7): 729-736.
4. Chamberlain, S. T., & Hale, B. D. Competitive state anxiety and self-confidence: Intensity and direction as relative predictors of performance on a golf putting task. Anxiety, Stress, and Coping. 2007; 20: 197-207.
5. Kais, K., & Raudsepp, L. Intensity and direction of competitive state anxiety, self-confidence and athletic performance. Kinesiology. 2005; 37: 13-20.
6. Swain, A., & Jones, G. Explaining performance variance: The relative contribution of intensity and direction dimensions of competitive state anxiety. Anxiety, Stress, and Coping. 1996; 9: 1¬18.
7. Salvador, A., Suay, F., Gonzalez-Bono, E., & Serrano, M. A. Anticipatory Cortisol, testosterone and psychological responses to judo competition in young men. Psychoneuroendocrinology. 2003; 28: 264-375.
8. Filaire, E., Alix, D., Rouveix, M., & Le Scanff, C. Motivation, stress, anxiety, and Cortisol responses in elite paragliders. Perceptual and Motor Skills. 2007; 104: 1271-1281.
9. Filaire, E., Sagnol, M., Ferrand, C, Maso, F., & Lac, G. Psychophysiological stress in judo athletes during competitions. Journal of Sports Medicine and Physical Fitness. 2001; 41: 263¬268.
10. Haneishi, K., Fry, A. C, Moore, C. A., Schilling, B. K., & Li, Y. Cortisol and stress responses during a game and practice in female collegiate soccer players. Journal of Strength and Conditioning Research. 2007; 21: 583-588.
11. Filaire, E., Alix, D., Ferrand, C, Verger, M. Psychophysiological stress in tennis players during the first single match of a tournament. Psychoneuroendocrinology. 2009; 34 (1):150-7.
12. E E Solberg, F Ingjer, A Holen. Reviews of the literature, Recovery from a standardized exercise bout: a study on 31 runners practicing relaxation technique. British Journal of Sports Medicine. 2000; 34:268-272.
13. Astin JA. Stress reduction through mindfulness meditation: Effects on psychological symtomatology, sense of control and spiritual expe-riences. Psychotherapy and Psychosomatics. 1997; 66(2): 97-106.
14. Chiesa A and A. Serretti. A systematic review of neurobiological and clinical features of mindfulness meditations, Psychological Medicine. 2010; 40: 1239-1252.
15. Chambers, R., Lo, B. C. Y., & Allen, N. B. The impact of intensive Mindfulness training on attentional control, cognitive style and affect. Cognitive Therapy & Research. 2008; 32: 303¬22.
16. Ashcraft, M . H. , & Krause, J. A . Working memory, math performance, and math anxiety. Psychonomic Bulletin & Review. 2007; 14: 243-248.
17. Curry, D. G., Meyer, J. E., & McKnney, J. M. Seeing versus perceiving: What you see isn't always what you get. Professional Safety. 2006; 57(6): 28-34.
18. Fredrickson, B. L., & Branigan, C. Positive emotions broaden the scope of attention and thought-action repertoires. Cognition & Emotion. 2005; 19(3): 313-332.
19. Most, S. B., Scholl, B. J., Clifford, E. R., & Simons, D. J. What you see is what you set: Sustained in attentional blindness and the capture of awareness. Psychological Review. 2005; 112(1): 217-242.
20. Kirschbaum C & Hellhammer DH. Salivary cortisol in psychoneuroendocrine research: recent developments and applications. Psychoneuroendocrinology. 1994; 19: 313-333.
21. MacLean, C.R., Walton, K.G., Wenneberg, S.R., Levitsky, D.K., Mandarino, J.P., Waziri, R., Schneider, R.H. Altered responses of cortisol, GH, TSH and testosterone to acute stress after four months' practice of transcendental meditation (TM). Ann. N. Y. Acad. Sci. 1994; 746: 381-384.
22. Tang, Y., Ma, Y., Wang, J., Feng, S., Yu, Q., Rothbart, M. K., et al. Short-term meditation training improves attention and self-regulation. PNAS Proceedings of the National Academy of Sciences of the United States of America. 2007 ; 104: 17152-17156.
23. Crocker, R R. E, Alderman, R. B., & Smith, M. R. Cognitive-affective stress management training
NJIRM 2011; Vol. 2(3). July- September eISSN: 0975-9840 pISSN: 2230 - 9969 I 20

Mindfulness Meditation on HPA-Axis
with high performance youth volleyball players: Effects on affect, cognition, and performance. Journal of Sport and Exercise Psychology. 1988; 10:448-460.
24. Brunner, E.J., Hemingway, H., Walker, B.R., Page, M., Clarke, P., Juneja, M., Shipley, M.J., Kumari, M., Andrew, R., Seckl, J.R., Papadopoulos, A., Checkley, S., Rumley, A., Lowe, G.D.O., Stansfeld, S.A., Marmot, M.G. Adrenocortical, autonomic, and inflammatory causes of the metabolic syndrome. Circulation. 2002; 106: 2659—2665.
25. Belmaker R.H., Agam G. Major depressive disorder. N. Engl. J. Med. 2008; 358: 55- 68.
26. Smith, G.D., Ben-Shlomo, Y., Beswick, A., Yarnell, J., Lightman, S., Elwood, P. Cortisol, testosterone, and coronary heart disease: prospective evidence from the Caerphilly study. Circulation. 2005; 112: 332—340.
27. Seeman, T.E., McEwen, B.S., Singer, B.H., Albert, M.S., Rowe, J.W. Increase in urinary cortisol excretion and memory declines: MacArthur studies of successful aging. J. Clin. Endocrinol. Metab. 1997;82: 2458—2465.
28. Coulter, H.D. (Ed.).Relaxation and meditation. In: Anatomy of Hatha Yoga: Body and Breath, first ed. Inc. Honesdale, 2001; 547-557.
NJIRM 2011; Vol. 2(3). July- September eISSN: 0975-9840 pISSN: 2230 - 9969 21

Journal of Exercise Science and Physiotherapy, Vol. 6, No. 2: 70-77, 2010
70
The Effect of Music Therapy on Salivary Cortisol as a Reliable
Marker of Pre Competition Stress in Shooting Performance
John1, S., Verma
2, S. K., Khanna
3, G. L.
1Department of Sports Sciences, Punjabi University, Patiala, Punjab, India, email:[email protected],
2Professor,
Department of Sports Sciences, Punjabi University, Patiala, Punjab, India, Email: [email protected]
3Professor & Dean,
Faculty of Applied Medical Sciences, Manav Rachna International University, Faridabad, Haryana, India.
Introduction
In shooting the requirement of
good physical and psychological condition as well as technical perfection is
highly demanded (Antal et al., 1994).
Pistol shooting is a static activity requiring a strict control of body segments
and posture to align the rear sight aperture
and the foresight through proprioceptive
feedback and gaze fixation either on the target directly or between the target and
the weapon and, therefore, to increase
precision of the shot (Mononen et al., 2007). Air pistol shooting is an Olympic
sport requiring extreme mental
concentration and movement precision for success. Compared to that for rifle
shooting, there is very little literature
related to pistol shooting. To our
knowledge, this is the first study to
determine the efficacy of Music Therapy
(MT) on Salivary Cortisol (SC) in professional shooters. Stress is most often
used to describe an unpleasant emotional
state or condition which is characterized by subjective feelings of tension,
apprehension, and worry. In sports
context it is commonly known as pre-
competition stress or anxiety. Further, researches indicate that anxiety has a
negative effect on these sport outcomes
(Terry & Slade, 1995). Research on how athletes cope with sport-related stress has
been recognized for both its practical and
its theoretical importance because of the debilitating effects that stress may have
on athletic performance (Smith et al.,
1998). Findings of Mellalieu et al (2009)
Abstract
Studies have been performed on the psychophysiological responses of Music Therapy (MT) in
normal and diseased, but little has been done on pre-competition stress (PCS) and Hypothalamic
Pituitary Adrenal (HPA) axis response on sports population. The purpose of the current study was to estimate the contribution of MT on Salivary Cortisol (SC) in reducing PCS, and its effect
on shooting performance (PS). One hundred male shooters between the age range of
29.5±4.3years were examined as experimental (N=50, MT along with the routine sports specific
training) and control (N=50, only with the routine sports specific training). Duration of the study
was 5 weeks, 4 weeks of interventional and 1 week study to determine the follow-up effect. Pre,
post and follow-up data of quantitative phenotypic markers of HPA-Axis by SC and PS were
analyzed. Compared to the control, experimental group has shown significant result, post-
intervention (p<0.001) and in follow-up (p<0.001) in SC and in PS. Experimental group
demonstrated in reduction of PCS level and increase in PS, whereas the control group showed
non-significant result. Results indicated that relaxation therapies such as MT may decrease PCS
and therefore enhance PS. It is concluded that four weeks of MT has an effect on HPA-Axis by
decreasing the level of SC as a reliable physiological marker of PCS.
Key Words: HPA, Cortisol, Pre competition Stress, Music, Shooting.

The Effect of Music Therapy on Salivary Cortisol as a Reliable Marker of Pre Competition Stress in Shooting Performance
– John, S. et al
71
suggest that, prior to competing; sport performers encounter more stressors
pertinent to performance. These
observations highlight that all the
demands faced by the athletes should be considered when preparing and
implementing interventions to manage
competition stress. Pre-competition anxiety is a widely prevalent condition
that exists among athletes of all levels and
within every sport. Its relationship to
performance has been studied both in and out of the sport context through test
anxiety research (Liebert & Morris, 1967)
and anxiety research with athletes (Swain & Jones, 1996; Kais & Raudsepp, 2005;
Chamberlain & Hale, 2007). Despite the
large body of research on pre-competition anxiety, our understanding of its
relationship to performance remains
elusive.
Cortisol is a hormonal response to acute stress and has been measured to be
higher before competition than at resting
conditions (Salvador et al., 2003). Some researchers have found that athletes
produce higher levels of cortisol before
games than before non-competition situations (Salvador et al., 2003; Filaire
et al., 2007; Haneishi et al.,2007). The
results support previous findings of
Filaire et al (2009) that athletes are more anxious before games than during off
days. Because cortisol is secreted as a
result of a threatening stimulus, and sports competition is considered an anxiety-
arousing situation (Salvador et al., 2003).
Research findings comparing the
physiological and psychological markers of stress have been equivocal (Filaire et
al., 2001).
Applied sport psychology, in its efforts to enhance the competitive perfor-
mance of athletes, has traditionally
utilized cognitive behavioral methods and techniques with an emphasis on
developing self-control of internal states,
commonly referred to as psychological
skills training (Whelan et al., 1991). Relaxation techniques have been used in
sports primarily to enhance recovery from
training and competition, manage anxiety and improve performance (Solberg et al.,
2000). One mechanism through which
music may impact on flow is by
enhancing pre-performance mood. Indeed, in a recent review, presented a strong case
for the mood-enhancing effects of music
in a sport context. (Vlachopoulos et al., 2000). Studies support previous research
that found music to be an effective tool
for improving athletic performance ( Karageorghis et al., 1996).
The present study focused on
examining the relation of physiological
response to skilled sport performance, and investigating the relevance of music
therapy in pre-competition stress. For this
purpose, physiological variable such as Salivary Cortisol (SC) were recorded
during the training and pre-competition
phase of actual shooting.
Materials and Methods
Subjects: A total of 110 healthy
male elite level shooters aged
(29.5±4.3years) selected for the study. Subjects were voluntarily recruited from
national shooting team; permission was
obtained from officials. Questionnaires administered prior to the experiment were
indicated that no volunteers are included
as per exclusion criteria such as any
physical or mental illness, hearing impairment, and have been under going
music therapies for last 3 months. All
subjects were nonsmokers, medication-free and not habitual drinkers. The aims
of the present study, the procedures

Journal of Exercise Science and Physiotherapy, Vol. 6, No. 2: 70-77, 2010
72
involved and potential risks of the study were explained carefully to subjects, and
the written consent was obtained prior to
the study. The study and all protocols
were approved by research ethical committee of Punjabi University.
Participants were randomly
allocated into two groups; experimental (Music Therapy) and Control by multiple
blocked random sampling of 55 in each
group, after the dropout 100 (50±3)
subjects could complete the study in each group. Heart Rate (70±3bpm),
Respiratory Rate (15±2rpm), BMI
(24±1.04kg/cm2) and Blood Pressure
(119±4/79±4 mm of Hg) were recruited to
participate in this study. Intervention trial
was conducted to the experimental subjects one week prior to the study.
Concerning impediments to effective
practice, subjects were monitored by the
researcher and experts during the interventions. The intervention was
provided over the course of four weeks
and one week follow-up, group sessions with a maximum of 8 participants each,
20 minutes session per day, 6 days a week
and one day was off per week. Participants were asked not to consume
caffeine or alcoholic beverages for 12 h,
and not to exercise for 12 h prior to the
experiment especially during testing.
Procedure: The all participants of
each batch reported to the laboratory at
08:00AM, each session conducted in the morning (between 8 AM and 10 AM) and
The subject changed into loose fitting
clothing, and shoes removed then the
participants were instructed to lie in the supine position on the floor mat in a quiet,
light-attenuated electrically shielded room
with the temperature between 24 and 28 °C with their eyes closed.
Interventions:
Music Therapy: CD of 30-40 music of Raga Darbari based Hindi songs
given to the experimental subjects one
week prior to the study and asked them to
select 5-10 songs according to their choice from the songs given, after
selection of individual choice of music
made separate folder for each subjects. The music was delivered on Sony
TM MP3
player by headphone with volume of 60-
70 dB, 60 to 70 beats per minute.
The music therapy group was encouraged to assume a comfortable
position in supine position on a floor mat
during delivery of the music intervention, Advised subjects to clear their minds and
allow their muscles to relax throughout
the training session. The participants left the room after 20 minutes of session.
Experimental group underwent music
therapy along with the routine sports
specific training and control group only with the routine sports specific training.
Testing: The testing sessions were
conducted between 8 am and 10 am and the same researcher tested all subjects.
Measurement day scheduled one day prior
to beginning the 1st week, 29
th day and
36th day, subjects were assessed for pre-
test, post-test and follow-up data
respectively, except Performance Test, in
a quiet controlled room with ambient temperature (24–28
0C). The performance
score calculated by pre-scheduled a
competition in a internationally standard shooting range on one day prior to
beginning the 1st week, and on 29
th day,
subjects were assessed for pre-test, post-
test Performance score respectively.
All the participants were
instructed to avoid consuming stimulant
beverages, tea, and coffee; exercising, in the 12 hours previous to the examination.
All the participants of each batch reported
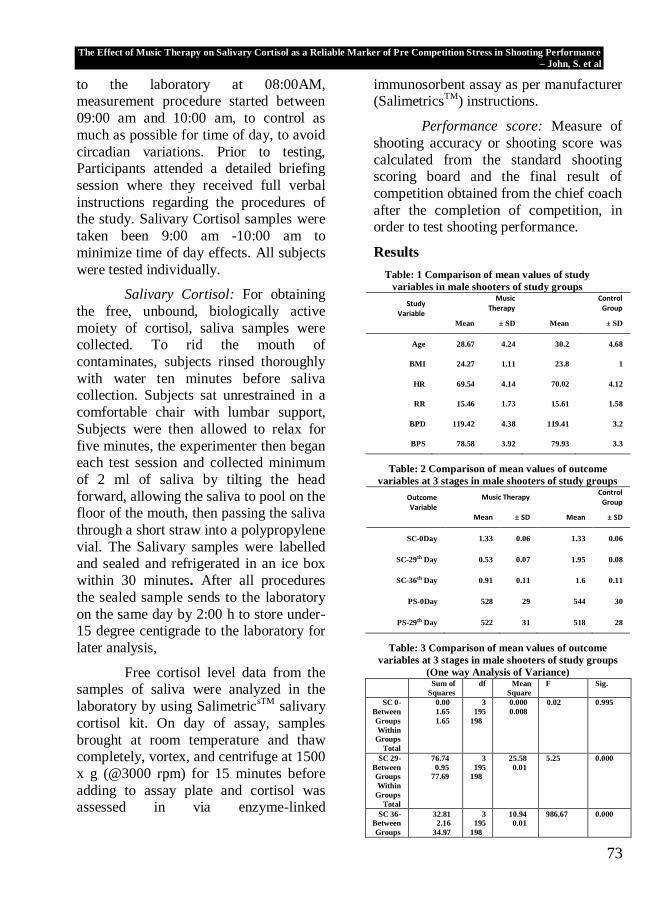
The Effect of Music Therapy on Salivary Cortisol as a Reliable Marker of Pre Competition Stress in Shooting Performance
– John, S. et al
73
to the laboratory at 08:00AM, measurement procedure started between
09:00 am and 10:00 am, to control as
much as possible for time of day, to avoid
circadian variations. Prior to testing, Participants attended a detailed briefing
session where they received full verbal
instructions regarding the procedures of the study. Salivary Cortisol samples were
taken been 9:00 am -10:00 am to
minimize time of day effects. All subjects
were tested individually.
Salivary Cortisol: For obtaining
the free, unbound, biologically active
moiety of cortisol, saliva samples were collected. To rid the mouth of
contaminates, subjects rinsed thoroughly
with water ten minutes before saliva collection. Subjects sat unrestrained in a
comfortable chair with lumbar support,
Subjects were then allowed to relax for
five minutes, the experimenter then began each test session and collected minimum
of 2 ml of saliva by tilting the head
forward, allowing the saliva to pool on the floor of the mouth, then passing the saliva
through a short straw into a polypropylene
vial. The Salivary samples were labelled and sealed and refrigerated in an ice box
within 30 minutes. After all procedures
the sealed sample sends to the laboratory
on the same day by 2:00 h to store under-15 degree centigrade to the laboratory for
later analysis,
Free cortisol level data from the samples of saliva were analyzed in the
laboratory by using SalimetricsTM
salivary
cortisol kit. On day of assay, samples
brought at room temperature and thaw completely, vortex, and centrifuge at 1500
x g (@3000 rpm) for 15 minutes before
adding to assay plate and cortisol was assessed in via enzyme-linked
immunosorbent assay as per manufacturer (Salimetrics
TM) instructions.
Performance score: Measure of
shooting accuracy or shooting score was
calculated from the standard shooting scoring board and the final result of
competition obtained from the chief coach
after the completion of competition, in order to test shooting performance.
Results
Table: 1 Comparison of mean values of study
variables in male shooters of study groups
Study Variable
Music Therapy
Control Group
Mean ± SD Mean ± SD
Age 28.67 4.24 30.2 4.68
BMI 24.27 1.11 23.8 1
HR 69.54 4.14 70.02 4.12
RR 15.46 1.73 15.61 1.58
BPD 119.42 4.38 119.41 3.2
BPS 78.58 3.92 79.93 3.3
Table: 2 Comparison of mean values of outcome
variables at 3 stages in male shooters of study groups
Outcome Variable
Music Therapy Control
Group
Mean ± SD Mean ± SD
SC-0Day 1.33 0.06 1.33 0.06
SC-29th Day 0.53 0.07 1.95 0.08
SC-36th Day 0.91 0.11 1.6 0.11
PS-0Day 528 29 544 30
PS-29th Day 522 31 518 28
Table: 3 Comparison of mean values of outcome
variables at 3 stages in male shooters of study groups
(One way Analysis of Variance) Sum of
Squares
df Mean
Square
F Sig.
SC 0-
Between
Groups
Within
Groups
Total
0.00
1.65
1.65
3
195
198
0.000
0.008
0.02 0.995
SC 29-
Between
Groups
Within
Groups
Total
76.74
0.95
77.69
3
195
198
25.58
0.01
5.25 0.000
SC 36-
Between
Groups
32.81
2.16
34.97
3
195
198
10.94
0.01
986.67 0.000

Journal of Exercise Science and Physiotherapy, Vol. 6, No. 2: 70-77, 2010
74
Within
Groups
Total
PS 0-
Between
Groups
Within
Groups
Total
923.33
151648.89
152572.21
3
195
198
307.78
777.69
0.40 0.756
PS 29-
Between
Groups
Within
Groups
Total
28100.54
133436.06
161536.59
3
195
198
9366.85
684.29
13.69 0.000
Descriptive statistics of study and
outcome variables measured in 52 and 48 subjects in experimental and control
group respectively. The comparison of
base line mean values of study variables
(Table-1) and outcome variables (Table-2 ) among the two study groups, that is
male shooters who had interventions: as
music and control, shows a non statistically significant difference in the
mean values of Age (F= 1.15; p= 0.33),
BMI (F= 3.57; p=0.02), heart rate (HR) ( F=0.10; p=0.96), respiratory rate (RR)
(F=2.44;p=0.07), diastolic blood pressure
(BPD) (F=0.42; p=0.74), and systolic
blood pressure (BPS) (F=1.11; p=0.35) and SC(F=0.02; p=0.99), PS (F=0.40; p=
0.756).
In Experimental group, the mean values of Salivary Cortisol (SC) had
statistically significantly decreased from
the baseline value of 1.33 to 0.53 at 29th
day and 0.91 at 36th day which is
statistically significant (F=1.20;p<0.001).
The post hoc pair wise comparison of
these three values indicates highly statistically significant difference among
the three values. From this it can be infer
that the effect of music in this group has decreased the SC values significantly
from their base line values. The mean
value of performance score has
statistically significantly increased from 528 to 544(t-value=-9.67, p<0.001).
In control group, the mean values of Salivary Cortisol (SC) had statistically
significantly increased from the baseline
value of 1.33 to 1.95 at 29th day and 1.60
at 36th day which is statistically
significant (F=577.48; p<0.001). The post
hoc pair wise comparison of these three
values indicates highly statistically significant difference among the three
values. From this it can be infer that the
effect of no music intervention in this
group has increased the SC values significantly from their base line values.
The mean value of performance score has
statistically significantly decreased from 524 to 522 (t-value=0.65, p<0.001).
Discussion
In the current study, used Salivary Cortisol (SC) as physiological markers
and Performance Score (PS) as one
subjective marker to assess the changes
with music intervention group and also assessed changes in control group during
the same duration. These parameters are
very much reliable to provide true picture of changes and they are also very much
susceptible for changes in pre competition
anxiety or stress. This fact is supported by (Filarie et al., 2007 and Hanesishi et al.,
2004) and also supported by research
findings comparing the physiological and
psychological markers of stress have been equivocal (Filaire et al., 2001). Since the
salivary cortisol assay has been proposed
as the method of choice for assessing adrenocortical (endocrine) function and
responses to competitive stress Thus in
this study also included SC as a
physiological marker.
Result have been proved, during
intervention of music therapy, the cortisol
level in saliva decreased in music group post-intervention 60% (.53) and follow-up
29% (.91). Whereas control group showed

The Effect of Music Therapy on Salivary Cortisol as a Reliable Marker of Pre Competition Stress in Shooting Performance
– John, S. et al
75
an increase of 47% 1.95 and 26% 1.60 pre-competition and post competition
respectively. Study also showed the pre
and post competition performance score
of experimental group has increased 3% (544) whereas control group showed a
decrease of performance score 0.9%
(518).
The result of the study indicated
that there is an increase in post
intervention and follow up values in
experimental group was showing more effective whereas the control groups it
was highly insignificant result. The reason
for these changes might be supported by studies on competition stress have been
observed (Stephen D Mellalieu et. al.,
2009), supported that, prior to competing, sport performers encounter more stressors
pertinent to performance. The level of
anxiety automatically narrows perception
restricting the focus of attention (Fredrickson & Branigan, 2005; Most et
al., 2005; Curry et al., 2006; Ashcraft &
Krause, 2007). Thus result of this study indicated that there is an decrease in
control group and increase in post
intervention performance score in music therapy group; the reason for these
changes might be due to decrease in pre
competition stress.
supported by studies on cortisol have been observed, Cortisol is a
hormonal response to acute stress and has
been measured to be higher before competition than at resting conditions
(Salvador et al., 2003). In recent years,
however, salivary cortisol has been shown
to reliably reflect levels of unbound cortisol in the blood and raised levels
have been found to be associated with
stress in normal subjects (Kirschbaum and Hellhammer, 1994).
Music affects a reduction in sympathetic nervous control and therefore
a reduction in heart and respiration rates,
metabolism, oxygen consumption, muscle
tension, (Lee et al 2005). Listening to classical music increases heart rate
variability helps in stress reduction,
whereas listening to noise or rock music decreases heart rate variability (reflecting
greater stress) (Chuang et al., 2010).
Also supported by reductions in
autonomic activity and self-reported tension and improved performance of
surgeons (Allen and Blaskovich, 1994). In
the current study music therapy has also been given based on classical music that
might have increased relaxation in groups
which have under gone music interventions.
As repeated listening to music
affects people's preference for it as well as
their physiological responses to it (Knight and Rickard, 2001), Music appears to
exert direct physiological effects through
the autonomic nervous system (Rakel et. al., 2003). In our study we have given 20
minutes session for 4 weeks this could
supports the more effect of music. In addition, lower anxiety is expected to
promote psychological well being by
decreasing plasma norepinephrine and
cortisol (Mockel et al., 1994) and enhancing relaxation and calmness.
Therefore, soothing music was expected
to have a therapeutic effect on relaxation.
Result of the current study
showed in experimental group have been
shown some amount of follow up effects
even after one week of intervention this is supported by studies such as, (Caine,
1992) found evidence that playing
recorded music for infants in the neonatal intensive care unit increased weight gain
and shortened lengths of stay. Moreover,

Journal of Exercise Science and Physiotherapy, Vol. 6, No. 2: 70-77, 2010
76
a follow-up study of the infants that participated in Caine's music listening
study indicated that infants who
participated in the music intervention
were rated as calmer by their mothers at 6 months of age compared to infants
without music intervention. The results
concerning the affective component of symptom changes showed that the effect
of music therapy was sustained. One
week after the discontinuation of sessions
(Guetin et al., 2009).
Conclusion
The neuroendocrine scientific
studies of music is clearly still in its infancy, but the initial findings reviewed
earlier promise both to reveal the
mechanisms by which such training might exert its effects on relaxation that
underlie complex regulatory mental
functions. Results of this study indicated
that relaxation therapies such as music therapy may decrease pre-competition
stress and will enhance sports
performance. It is concluded that in four weeks of music training has an effect on
HPA-Axis by decreasing the level of
salivary cortisol as a reliable physiological marker of pre-competition
stress.
The past empirical evidence has
lent support to the view that psychophysiological recordings may even
provide insight into the skill related
aspects of a shooter's psychomotor strategies and determinants of successful
shooting performance.
To our knowledge, the salivary
cortisol has been little evaluated in young athletes and, in such conditions of pre-
competitive stress and post relaxation
therapies. This work was made possible to find out the changes on the
neuroendocrine (ANS and HPA axis) activity during intervention, or changes
induced in pre-competition stress.
Although short-term activations of the
HPA axis are adaptive and necessary for everyday functioning, extreme, frequent
or chronic activation of this system are
associated with negative health outcomes. Existing research has implicated the HPA
axis in the development of a variety of
sub-clinical and clinical conditions
including metabolic syndrome (Brunner et al., 2002), depression (Belmaker and
Agam, 2008), risk for cardiovascular
disease (Smith et al., 2005) and cognitive decline (Seeman et al., 1997).
References
Allen, K., Blascovich, J. 1994. Effects of music on cardiovascular reactivity among surgeons. JAMA 272: 882-884.
Antal, L., Shankar, R. 1994. Theory and Methodology of Training, Pistol Shooting. Psychonomic Bulletin & Review, 14(2): 243-248.
Ashcraft, M. H., & Krause, J. A. 2007. Working
memory, math performance, and math anxiety. Psychonomic Bulletin & Review, 14(2): 243-248.
Caine, J. 1992. The effects of music on the selected stress behaviors, weight, caloric and formula intake, and length of hospital stay of premature and low birth weight neonates in a newborn intensive care unit. J. Music Ther. 28: 180-192.
Chamberlain, S. T., & Hale, B. D. 2007. Competitive state anxiety and self-confidence: Intensity and direction as relative predictors of performance on a golf putting task. Anxiety, Stress, and Coping, 20: 197-207.
Chuang, C. Y., Han, W. R. Lie, P. C. et al. 2010. Effects of music therapy on subjective
sensations and heart rate variability in treated cancer survivors: A pilot study. Compl. Ther. Med., doi:10.1016/j.ctim. 2010.08.003.
Curry, D. G., Meyer, J. E., & McKnney, J. M. 2006. Seeing versus perceiving: What you see isn't always what you get. Prof. Safety, 57(6): 28-34.

The Effect of Music Therapy on Salivary Cortisol as a Reliable Marker of Pre Competition Stress in Shooting Performance
– John, S. et al
77
Solberg, E. E., Bergulund, K. A. 1996. The effect of meditation on shooting performance. Brit. J. Sports Med., 30: 342-346.
Filaire, E., Alix, D., Rouveix, M., & Le Scanff, C. 2007. Motivation, stress, anxiety, and Cortisol responses in elite paragliders.
Percep. and Motor Skills, 104: 1271-1281.
Filaire, E., Sagnol, M., Ferrand, C., Maso, F., & Lac, G. 2001. Psychophysiological stress in judo athletes during competitions. J. Sports Med. and Phy. Fit., 41: 263-268.
Fredrickson, B. L., & Branigan, C. 2005. Positive emotions broaden the scope of attention and thought-action repertoires. Cogn. &
Emot., 19(3): 313-332. Haneishi, K., Fry, A. C, Moore, C. A., Schilling, B.
K., & Li, Y., 2007. Cortisol and stress responses during a game and practice in female collegiate soccer players. J. Str. Res., 21: 583-588.
Kais, K., & Raudsepp, L. 2005. Intensity and direction of competitive state anxiety,
self-confidence and athletic performance. Kinesiology, 37: 13-20.
Karageorghis, C. I., Drew, K. M., & Terry, P. C. 1996. Effects of pretest stimulative and sedative music on grip strength. Percep. and Motor Skills, 83: 1347–1352.
Kirschbaum, C. & Hellhammer, D.H., 1994. Salivary cortisol in
psychoneuroendocrine research: recent developments and applications. Psychoneuroendocrinology, 19: 313-333.
Knight, W.E.J., Rickard, N.S. 2001. Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure and heart rate in healthy males and females. J. Music Ther., 38: 254-272.
Lee, O.K. et al., 2005. Music and its effect on physiological and anxiety levels of patients receiving mechanical ventilation: a pilot study. J. Clin. Nurs. 14(5): 609-620.
Mockel, M., Rocker, L., Stork, T. et al., 1994. Immediate physiological responses of healthy volunteers to different types of music: cardiovascular, hormonal and
mental changes. Eur. J. Appl. Physiol. Occup. Physiol., 68: 451-9.
Mononen, K., Konttinen, N., Viitasalo, J., Era, P. 2007. Relationships between postural balance, rifle stability and shooting accuracy among novice rifle shooters. Scand. J. Med. Sci. Sports, 17:180–5.
Most, S. B., Scholl, B. J., Clifford, E. R., &
Simons, D. J., 2005. What you see is what you set: Sustained in attentional blindness and the capture of awareness. Psych. Rev., 112(1): 217-242.
Guetin, S., Soua, B., Voiriot, M.C., Picot, C., Herisson, C. 2009. The effect of music therapy on mood and anxiety-depression: An observational study in institutionalised patients with traumatic
brain injury Ann. Phys. Rehab. Med. 52: 30-40.
Salvador, A., Suay, F., Gonzalez-Bono, E., & Serrano, M. A. 2003. Anticipatory Cortisol, testosterone and psychological responses to judo competition in young men. Psychoneuroendocrinology, 28, 264-375.
Smith. R. E., Smoll, F. L., & Weichinan, S. A. 1998. Measurement of trait anxiety in sport. In: Advances in Sport and Exercise Psychology Measurement, Ed: Duda, J. L pp.105-128.
Stephen, D., Mellalieu, R. N., Sheldon, H., Fletcher. D. 2009. Competition stress in sport performers: Stressors experienced
in the competition environment. 27(7): 729.
Swain, A., & Jones, G. 1996. Explaining performance variance: The relative contribution of intensity and direction dimensions of competitive state anxiety. Anxiety, Stress, and Coping, 9, 1-18.
Terry, P. C., & Slade, A. 1995. Discriminate
effectiveness of psychological state measures in predicting performance outcome in karate competition. Percep. and Motor Skills, 81(i): 275-286.
Vlachopoulos, S.P., Karageorghis, C.I. and Terry, P.C. 2000. Motivation profiles in sport: A self-determination theory perspective. Res. Quart. Exer. Sport, 71: 387-397.
Whelan, J. P., Mahoney, M. J., & Meyers, A. W.
1991. Performance enhancement in sport: A cognitive behavioral domain. Behav. Therap., 22, 307-327.


















