Aortic Stenosis: Tips DISCLOSURE: Sunil Mankad …...7/26/2016 1 Aortic Stenosis: Tips for Primary...
15
7/26/2016 1 Aortic Stenosis: Tips for Primary Care and Newer Treatment Options Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo Clinic, Rochester, MN [email protected] @MDMankad DISCLOSURE: Sunil Mankad Relevant Financial Relationship(s) None Off Label Usage None • Canadians: Please divert your course 15 degrees to the South to avoid collision. • United States: Recommend you divert your course 15 degrees to the North to avoid a collision. This is a transcript of an actual radio conversation between a US Naval ship and Canadian authorities off the coast of Newfoundland in October, 1995. Radio conversation released by the Chief of Naval Operations 10/10/95 • Canadians: Negative. We insist that you divert your course 15 degrees to the South to avoid a collision. • United States: This is the Captain of a US Navy Ship. I say again, divert YOUR course. • Canadians: No. I say again, you divert YOUR course. • United States: This is the aircraft carrier USS Lincoln, the second largest ship in the United States’ Atlantic Fleet. We are accompanied by three destroyers, three cruisers, and numerous support vessels. I demand that you change your course 15 degrees North! I say again, that’s one five degrees North or counter- measures will be undertaken to ensure the safety of this ship. • Canadians: This is a lighthouse. Your call. Photo by Lynn Botterman
Transcript of Aortic Stenosis: Tips DISCLOSURE: Sunil Mankad …...7/26/2016 1 Aortic Stenosis: Tips for Primary...

7/26/2016
1
Aortic Stenosis: Tips
for Primary Care and
Newer Treatment
Options Sunil Mankad, MD, FACC, FCCP, FASE
Associate Professor of Medicine
Mayo Clinic College of Medicine
Director, Transesophageal Echocardiography
Associate Director, Cardiology Fellowship
Mayo Clinic, Rochester, MN
@MDMankad
DISCLOSURE: Sunil Mankad
Relevant Financial Relationship(s)
None
Off Label Usage
None
• Canadians: Please divert your course 15 degrees to the South to avoid collision.
• United States: Recommend you divert your course 15 degrees to the North to avoid a collision.
This is a transcript of an actual radio conversation between a US Naval ship and Canadian authorities off the coast of Newfoundland in October, 1995. Radio conversation released by the Chief of Naval Operations 10/10/95
• Canadians: Negative. We insist that you divert your course 15 degrees to the South to avoid a collision.
• United States: This is the Captain of a US Navy Ship. I say again, divert YOUR course.
• Canadians: No. I say again, you divert YOUR course.
• United States: This is the aircraft carrier USS Lincoln, the second largest ship in the United States’ Atlantic Fleet. We are accompanied by three destroyers, three cruisers, and numerous support vessels. I demand that you change your course 15 degrees North! I say again, that’s one five degrees North or counter-measures will be undertaken to ensure the safety of this ship.
• Canadians: This is a lighthouse. Your call.
Photo by Lynn Botterman

7/26/2016
2
Aortic Valve Disease: Stenosis
• Epidemiology, Pathophysiology, and Natural History of Aortic Stenosis
• Assessment of Severity
• Imaging
• Hemodynamics
• Role of Stress Testing
• Timing of Intervention
• Transcatheter Aortic Valve Replacement (TAVR)
2014 AHA/ACC Guideline for the
Management of Patients With
Valvular Heart Disease
Developed in Collaboration with the American Association for Thoracic Surgery,
American Society of Echocardiography, Society for Cardiovascular Angiography and
Interventions, Society of Cardiovascular Anesthesiologists, and Society of Thoracic
Surgeons
© American College of Cardiology Foundation and American Heart Association
Circulation. 2014 Jun 10;129(23):e521-643
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O'Gara PT, Ruiz
CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD; ACC/AHA Task Force Members.
Frequency of Echocardiograms in Asymptomatic Patients With VHD and Normal Left Ventricular Function
Valve Lesion
Stage Aortic Stenosis Aortic
Regurgitation Mitral Stenosis
Mitral
Regurgitation
Progressive
(stage B)
Every 3–5 y
(mild severity
Vmax 2.0–2.9 m/s)
Every 1–2 y
(moderate
severity
Vmax 3.0–3.9 m/s)
Every 3-5 y
(mild severity)
Every 1-2 y
(moderate
severity)
Every 3–5 y
(MVA >1.5 cm2)
Every 3–5 y
(mild severity)
Every 1–2 y
(moderate
severity)
Severe
(stage C)
Every 1 y
(Vmax ≥4 m/s)
Every 1 y
Dilating LV–
more frequent
Every 1–2 y
(MVA 1.0–1.5 cm2)
Every 1 y
(MVA <1 cm2)
Every 6 months
to 1 y
Dilating LV–
more frequent
Circulation. 2014 Jun 10;129(23):e521-643
A Parisian Shoemaker named Carolus Rayger died suddenly (1672)
- reported by Bonetus in 1679 - “Sepulchretum” – aortic valves of “bone”
Aortic Stenosis: Background
• Aortic stenosis (AS) is the 3rd most common cardiovascular disorder in the US, trailing only HTN and CAD
• Most common valvular lesion
• Prevlalence increases with age
• Severe AS affects 3-4% of persons >75 yrs old
• Most common reason for valve replacement

7/26/2016
3
Normal Aortic Valve A B
L
R
N
N L
R
N = non-coronary cusp; L = left coronary cusp; R = right coronary cusp
Michelena HI, Mankad S, Sarano ME. Atlas of Echocardiography, 2009
• Normal Valve Area = 3 to 4 cm2
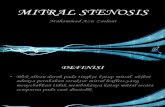
Calcific Aortic Stenosis
Michelena HI, Mankad S, Sarano ME. Atlas of Echocardiography, 2009
Causes of Aortic Stenosis
Passik CS, et al: Mayo Clin Proc 62:119, 1987
< 70 years old (n=324) > 71 years old (n=324)
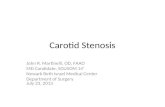
Timing of peak
Single
Component S2
Duration S4
S1 S2 S1
Aortic Stenosis
Distinguishing AS vs HOCM
Image from Healio.com
Risk Factors for Aortic Stenosis • Similar to atherosclerosis
• Hypertension • Hypercholesterolemia • Smoking • Male • Lp(a) • Diabetes
• Autopsy studies have revealed that initial lesion of AS resembles that of coronary artery plaque
• Rajamannan et al (Circulation 2003) showed that calcific aortic valves obtained at time of AVR exhibited dynamic calcification, similar to that of skeletal bone formation
Otto CM. Aortic stenosis: Clinical evaluation and optimal timing of surgery.Cardiology Clinics 1998;16:353.

7/26/2016
4
Aortic Sclerosis • Aortic sclerosis and aortic stenosis most
likely represent different stages in the same disease process
Olsen MH... Devereaux RB; LIFE substudy. Am J Cardiol 2005;95:132-6.
Aortic Stenosis: Medical Therapy
Recommendations COR LOE
Statin therapy is not indicated for prevention of
hemodynamic progression of AS in patients
with mild-to-moderate calcific valve disease
(stages B to D)
III: No
Benefit A
Nishimura RA et al. Circulation. 2014 Jun 10;129(23):e521-643
Aortic Stenosis: Pathophysiology
• Pressure overload of the LV
• As obstruction progresses, LV adapts in an attempt to keep wall stress normal
• Laplace’s law → LV Hypertrophy • Wall stress = LV systolic pressure x radius/ 2 x wall thickness
• If LV does not hypertrophy adequately to maintain normal wall stress, “afterload mismatch” will occur
• Diastolic function abnormal diastolic stiffness and subsequent LVEDP
• LV performance is subsequently impaired • Decline in LV ejection fraction
Boudoulas H, Gravanis MB: Valvular heart disease. In Gravanis MB: Cardiovascular Disorders: Pathogenesis and Pathophysiology. 1993, p 64.)
Aortic Stenosis LV Pressure Hypertrophy
Long-Axis View
LA
LV
RV
Ao
Courtesy of W. Edwards
Aortic Stenosis: LV Hypertrophy
HITHERTO unsettled problem of the pathologic physiology of the
circulation has been the in vivo estimation of degrees of valvular stenosis.
Because of the essentially fixed nature of the rings of the cardiac valves
when disease, an attempt has been made to apply the hydraulic principles
and formulas of fixed orifices to these stenotic valves.
A
American Heart Journal
Original Communications
HYDRAULIC FORMULA FOR CALCULATION OF
THE AREA OF THE STENOTIC VALVES
R. GORLIN, M.D., AND S.G. GORLIN, M.E.
BOSTON, MASS.
VOL. 41 JANUARY, 1951 No. 1
“in vivo estimation of degrees of
valvular stenosis.”
“……to apply the hydraulic
principles and formulas of fixed
orifices to these stenotic valves.”

7/26/2016
5
AVA = Forward flow rate
44.3C mean grad
CO ÷ [SEP HR]
44.3C mean grad =
Gorlin formula
Hakki formula
CO
mean grad AVA =
*co-existent regurgitation AVA underestimation
LVOT TVI LVOT area
AV area
=
x
AV TVI
% of Aortic Stenosis Pts Undergoing Invasive Hemodynamics, After Doppler
Exam, Prior to Valve Replacement Mayo Clinic
Roger et al. Mayo Clinic Proc 1996;71:141-149
Early 1980s
95
13 13
98 99
Pt underg
oin
g invasiv
e
hem
odynam
ics (
%)
Year
1990 91 92 93 94 (122) (149) (152) (160) (145)
54
40 35
29 23
0
20
40
60
80
100
Severity of Aortic Stenosis
Echo/Doppler
Parameter
Mild Moderate Severe
Velocity
(meters/sec)
< 3.0 3.0 - 4.0 > 4.0
Mean Gradient
(mmHg)
< 25 25 - 40 > 40
Valve Area (cm2) > 1.5 1.0 - 1.5 < 1.0
Valve Area Index
(cm2/m2)
< 0.6
Aortic Valve Area Equivalents
(cm2)
2.5 1.2 0.95 0.5 0.5
• 622 patients with severe AS
• Peak velocity ≥ 4 m/sec
• Mean Age = 72 ±11 yrs
• Mean FU = 5.4 ± 4.0 yrs
• Sudden death without preceding symptoms occurred in 1% per year of unoperated pts
Circulation 2005;111:3290-3295

7/26/2016
6
Years No. at risk 397 265 185 128 80 47 25 15 9 6
Survival free of
symptoms (%)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
Survival Free of Symptoms of Severe AS Censored at AV Surgery
Pellikka, Circulation 111:2005: 3290-5
• AS is Progressive
• Average peak velocity increases 0.3 m/sec per year
• Average AVA decreases 0.1 cm2 per year
Otto et al Circulation. 1997;95:2262
Survival in Asymptomatic Severe AS
Su
rviv
al
(%)
Time (yrs) after Dx asymptomatic severe AS
Brown ML, et al J Thorac Cardiovasc Surg 2008
No Symptoms: AVR
Symptoms : AVR
No Symptoms:
ØAVR
Symptoms: ØAVR
n = 622
Kaplan-Meier Survival Curves Comparing Asymptomatic Severe Aortic Stenosis Patients
with and without Aortic Valve Replacement
Cum survival
Pai et al: Ann Thorac Surg 82:2116, 2006
Years
No. at risk 99 87 78 71 64 55 46 35 25 20 11 (AVR)
239 140 104 86 68 57 38 28 18 14 6 (no AVR)
Survival 1 yr 2 yr 5 yr AVR 94% 93% 90% No AVR 67% 56% 38%
P<0.0001
No AVR (n=239)
AVR (n=99)
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12
Aortic Stenosis: Timing of Intervention
Recommendations COR LOE AVR is recommended with severe high-gradient
AS who have symptoms by history or on exercise
testing
I B
AVR is recommended for asymptomatic patients
with severe AS and LVEF <50% I B
AVR is indicated for patients with severe AS when
undergoing other cardiac surgery I B
Nishimura RA et al. Circulation. 2014 Jun 10;129(23):e521-643
Aortic Stenosis: Timing of Intervention (cont.) Recommendations COR LOE
AVR is reasonable for asymptomatic patients with
very severe AS (mean gradient ≥ 60 mm Hg)
and low surgical risk
IIa B
AVR is reasonable in symptomatic patients with
low-flow/low-gradient severe AS with reduced
LVEF when a low-dose dobutamine stress study
that shows an aortic velocity 4 m/s (or mean
pressure gradient 40 mm Hg) with a valve area
1.0 cm2 at any dobutamine dose
IIa B
AVR is reasonable in symptomatic patients who
have low-flow/low-gradient severe AS who are
normotensive and have an LVEF ≥ 50% if clinical,
hemodynamic, and anatomic data support valve
obstruction as the most likely cause of symptoms
IIa C
Case
• 82 year old male
• “Asymptomatic” aortic stenosis • Swims ½ hour several times/week
• Slow pace
• Episode of severe dyspnea on 1 occasion
• NYHA functional class I
• HTN, Hyperlipidemia, Glucose intolerance, Glaucoma

7/26/2016
7
Medications • Allopurinol
• Losartan
• ASA
• Centrum Silver
• Xalatan eye drops
• Flonase
• Rosuvastatin
Labs
• BNP 62 pg/ml
• LDL 41 mg/dl
• Otherwise WNL
EKG
CXR Echocardiogram
• LA volume index 36 cc/m2 (mildly dilated)
• Grade I diastolic dysfunction (impaired relaxation)
• E/e’ 10 (at rest)
• Normal LV mass index
• LV EF 60%
Severe Aortic Stenosis
• Mean Gradient 45 mmHg
• AVA 0.81 cm2
What would you recommend?
1. Yearly follow-up in valve clinic with serial echo
2. Stress test
3. Referral for AVR

7/26/2016
8
What would you recommend?
1. Yearly follow-up in valve clinic with serial echo
2. Stress test
3. Referral for AVR
Supine Bike Stress Echo
• Patient reached 125 Watts
• Fall in BP
• Pre-peak 178/84 mmHg
• Peak 148/84 mmHg
• Dyspnea, no angina
• Drop in EF
• Baseline – 60%
• Peak – 45%
Supine Bike Echo
Stress
Baseline Catheterization
• No significant CAD
Underwent AVR
Doing well
Am J Cardiol 2009;104:972–977
•No significant complications with stress testing
Sudden Cardiac Death
Rafique et al. Am J Cardiol 2009;104:972–977
• 0/179 patients with normal stress test had SCD
• 9/183 patients with abnormal stress test had SCD

7/26/2016
9
Aortic Stenosis: Diagnosis and Follow-Up
Recommendations COR LOE
Exercise testing is reasonable to assess
physiological changes with exercise and to confirm
the absence of symptoms in asymptomatic
patients with a calcified aortic valve and an aortic
velocity 4.0 m per second or greater or mean
pressure gradient 40 mm Hg or higher (stage C)
IIa B
Exercise testing should not be performed in
symptomatic patients with AS when the aortic
velocity is 4.0 m per second or greater or mean
pressure gradient is 40 mm Hg or higher (stage D)
III:
Harm B
New Technology
CP1298669-51
Dismal Prognosis in Symptomatic Severe AS Without AVR
Ross J, Braunwald E. Aortic Stenosis. Circulation1968; 38(suppl5);61-7
Aortic Stenosis: Natural History
Schwarz et al Circulation 1982
Carabello and Paulus Lancet 2009
87 Year Old Man with NYHA Class IV Dyspnea
• Physical Exam
•BP 96/67 HR 60
•JVP: elevated
•Carotids: tardus and parvus
•Heart: Single component S2, 3/6 late-peaking SEM, 2/6 HSM at apex
•Lungs: bibasilar crackles
•Ext: 2+ edema
• Past Medical History
•CABG: age 69
•Redo CABG: age 81
•Atrial Fibrillation
•HTN
•Hyperlipidemia
•OSA
•CKD (baseline Cr 2.5)
•Remote tobacco use
•Mild cognitive impairment

7/26/2016
10
• Meds:
• Statin
• ACE-I
• Beta Blocker
• Diuretic
• Nitrate
• Coumadin
• PPI
• Abnormal Labs:
•Hgb: 11.3 g/dl
•Cr: 2.6 mg/dl
•INR: 2.5
•BNP 1655 pg/ml
87 Year Old Man with NYHA Class IV Dyspnea
EKG
CXR Echocardiogram
• LV Ejection Fraction = 20-25%
• Aortic valve area = 0.58 cm2
• Mean aortic valve gradient = 65 mmHg
• Moderate to Severe MR
• Moderate TR
Aortic Valve – Long-axis View Aortic Valve – Short-axis View
Cardiac Catheterization
• LIMA – LAD patent
• SVG – R-PDA patent
• 100% occluded LAD, LCX, and RCA
• Nothing to revascularize
Summary
• 87 year old man
• Severe AS with Class IV symptoms, LV dysfunction, and multiple co-morbidities
• 2 prior CABG operations
• Creatinine = 2.6 mg/dl
• Options?
• What is the risk of surgery?

7/26/2016
11
Online STS Risk Calculator
Risk of Mortality = 20.1%
Risk of Morbidity or Mortality = 68.9%
Risk of Long Length of Stay = 39.4%
Risk of Permanent Stroke = 8.1%
Risk of Renal Failure = 31.3%
Assessment of Frailty (Frailty Index Data Collection Form)
To be considered frail, a patient must fail 3 out of 4 categories. Here is the criteria for each category:
• Albumin < 3.5 g/dl = failure in this category
• Grip strength < that recommended grip strength based on BMI
• ADL’s - a total score of 4 or less is failure in this category
• 15 foot/5 meter walk – based on height, walk time greater than or equal to 6-7 seconds (depending on height) is failure in this category
Activities
Points 1 or 0
Independence:
1 Point – No supervision, direction, or
personal assistance
Dependence:
0 Points – With supervision,
direction, personal assistance, or
total care
Bathing ____
1 Point – Bathes self completely or needs help
in bathing only a single part of the body such
as the back, genital area, or disabled extremity
0 Points – Needs help with bathing
more than one part of the body,
getting in or out of the tub/shower
Requires total bathing
Dressing ____
1 Point – Gets clothes from closets and
drawers and puts on clothes and outer
garments complete with fasteners. May have
help tying shoes
0 Points – Needs help dressing self
or needs to be completely dressed
Toileting _____
1 Point – Goes to toilet, gets on and off,
arranges clothes, cleans genital area without
help
0 Points – Needs help transferring
to the toilet, cleaning self or uses
bedpan or commode
Transferring ____
1 Point – Moves in and out of bed or chair
unassisted. Mechanical transfer aids are
acceptable
0 Points – Needs help in moving
from bed to chair or requires
complete transfer
Continence ____
1 Point – Exercises complete self -control over
urination and defecation
0 Points – Is partially or totally
incontinent of bowel or bladder
Feeding ____
1 Point – Gets food from plate into mouth
without help. Preparation of food may be done
by another person.
0 Points – Needs partial or total help
with feeding or requires parenteral
feeding.
Total Points ____
Screening For Vascular Access
Transfemoral Transapical
Transfemoral and Transapical

7/26/2016
12
Deploying the Valve Rapid Ventricular Pacing
Pre-AVR Post-AVR MG=65 mmHg, AVA=0.5cm2 MG=9mmHg, AVA=2.1cm2
Our Patient
N = 179
N = 358 Inoperable
Standard
Therapy
ASSESSMENT:
Transfemoral
Access
Not In Study
TF TAVR
Primary Endpoint: All-Cause Mortality
Over Length of Trial (Superiority)
Co-Primary Endpoint: Composite of All-Cause Mortality
and Repeat Hospitalization (Superiority)
1:1 Randomization
VS
Yes No
N = 179
TF TAVR AVR
Primary Endpoint: All-Cause Mortality at 1 yr
(Non-inferiority)
TA TAVR AVR VS
VS
N = 248 N = 104 N = 103 N = 244
PARTNER Study Design (High Risk Patients: STS score > 8%)
Symptomatic Severe Aortic Stenosis
ASSESSMENT: High-Risk AVR Candidate
3,105 Total Patients Screened
Total = 1,057 patients
2 Parallel Trials:
Individually Powered
N = 699 High Risk
ASSESSMENT:
Transfemoral
Access
Transapical (TA) Transfemoral (TF)
1:1 Randomization 1:1 Randomization
Yes No
Presented by Michael Mack, MD at ACC 2015
Presented by Michael Mack, MD at ACC 2015

7/26/2016
13
ACC 2015
ACC 2015
Primary Endpoint: All-Cause Mortality or Disabling Stroke at Two Years
Randomized Patients
n = 2032
Symptomatic Severe Aortic Stenosis
ASSESSMENT by Heart Valve Team
Operable (STS ≥ 4%)
The PARTNER 2A Trial Study Design
TF TAVR
(n = 775)
Surgical AVR
(n = 775) VS. VS.
ASSESSMENT:
Transfemoral Access
Transapical (TA) / TransAortic (TAo) Transfemoral (TF)
1:1 Randomization (n = 482) 1:1 Randomization (n = 1550)
TA/TAo TAVR
(n = 236) Surgical AVR
(n = 246)
Yes No
N Engl J Med 2016; 374:1609-1620
1
1011 918 901 870 842 825 811 801 774
1021 838 812 783 770 747 735 717 695
Number at risk:
TAVR
Surgery
p (log rank) = 0.253
HR [95% CI] = 0.89 [0.73, 1.09]
TAVR
Surgery
0
10
20
30
40
50
19.3%
21.1%
14.5%
16.4%
0 3 6 9 12 15 18 21 24
6.1%
8.0%
Primary Endpoint (ITT) All-Cause Mortality or Disabling Stroke
Months from Procedure
All
-Ca
us
e M
ort
ali
ty o
r D
isa
bli
ng
Str
ok
e (
%)
1
762 717 708 685 663 652 644 634 612
722 636 624 600 591 573 565 555 537
p (log rank) = 0.04
HR: 0.78 [95% CI: 0.61, 0.99]
16.3%
20.0%
0 0 3 6 9 12 15 18 21 24
0
10
20
30
40
50
15.8%
7.5%
11.7%
4.5%
TF Primary Endpoint (AT) All-Cause Mortality or Disabling Stroke
All
-Ca
us
e M
ort
ali
ty o
r D
isa
bli
ng
Str
ok
e (
%)
TF TAVR
TF Surgery
Months from Procedure Number at risk:
TF TAVR
TF Surgery Self Expandable Balloon Expandable
Sapien Valve CoreValve

7/26/2016
14
2-Year All-cause Mortality
ACC 2014 All Stroke
Conclusions
• Valvular Heart Disease is becoming more prevalent in the elderly
• Important to know when to intervene in severe aortic stenosis
• Novel technologies provide potential answers to treatment gaps in higher risk patients
“Your vision will become clear only when you can look into your own heart -
He who looks outside, dreams
He who looks inside, awakens” Carl Gustav Jung (1875-1961)
“Dream every night as if you will live forever, but live everyday as
if it could be your last”
James Dean
Thank You! [email protected]

7/26/2016
15
Text GEFPEB to (507) 200-3010 to record your attendance today.
48 Hours to Text Attendance
For questions, Andrea Cocker/[email protected]
CME Record of Attendance