Antiviral Chemotherapy Discovery of antiviral drugs Targets of antiviral drugs.
Upload
sifuma-andrew-njengaCategory
view
351download
0
PHB60057
1PCOL305 ANTIVIRAL AND ANTINEOPLASTIC AGENTS
COURSEWORK 2009
Amplification of ALU repeats in the chromosome 16 PV92 region
WRITE - UP
In this lab class you have amplified a DNA repeat sequence. The same technology that you have used is utilised to investigate other repeat sequences which are of greater significance to cancer formation.
Answer the following questions:
Explain why in PCR the precise length target DNA sequence doesn’t get amplified until the third PCR cycle. (10)
The precise length target DNA sequence doesn’t get amplified until the third PCR cycle because it is at this cycle that the DNA primers serve as the beginning and ends of the amplified region.In the first cycle of PCR, after denaturation of the original DNA molecule, the primer anneals to the unzipped DNA strand and a new complementary DNA strand is synthesized onto said primer. Taq polymerase extends the new strand way beyond the target sequence to be amplified to the “flanking region” so the new strand thus contains forward and reverse primers and is much longer than the precise target sequence

PHB60057
Fig 1. Cycle 1 of PCRIn the second cycle therefore, there are 2 types of template, the original DNA strand and the newly synthesised DNA strands that have the target DNA fragment and flanking region on the 3’ end of the DNA strand but at the beginning of this cycle they are annealed together and so need to be denatured to separate them, and after this the primers anneal to the original DNA strand again, as well as the newly synthesized strand made in the 1st cycle. When new strands are synthesized they make a small number of target DNA sequences and hybrid sequences
Fig 2. Cycle 3 of PCR
In the third cycle of PCR the target sequence DNA now acts as a template for polymerisation. The original DNA sequence is still present but the specific target DNA exhibits dominance when being primed or polymerised. The newly synthesized target sequence is then reprimed forward and back and Taq polymerase synthesizes copies of target DNA, copied exponentially for however many cycles the PCR is set to

PHB60057
Fig 3. Cycle 3 of PCR What kind of controls were run in this experiment? Why are they important? Could
others be used? (10)
The controls run in the experiment were an MMR DNA standard, a control that was (++) homozygous for the ALU PV92 repeat, a homozygous (--) control, and a heterozygous (+-) control.Controls are important in laboratory experiments because they give the scientist working the experiment a standard to compare their sample results to, as well as showing whether the methods used to conduct the experiment have worked properly.For example in this experiment these controls can be used to figure out which students sample exhibit which genotype e.g. if a student has the homozygous ++ genotype, the band formed on the agarose gel after electrophoresis will be at the same position as that of the ++ control. The controls shown so far are positive controls and are used to help find a resultOther controls that could be used in this experiment are negative controls such as to add a tube with a mix of master mix, nuclease free water and water(instead of cheek cells) and this should be added to the PCR and ran with the other samples all the way to the electrophoresis. This should show a negative result and should not show bands on the gel picture. If a result is shown there is contamination of reagents with DNA.
Why in this lab class, using your DNA, have we investigated the number of ALU repeat sequences in PV92 rather than a disease-associated repeat sequence? What was your genotype ?(10)In this lab class we tried to identify the Alu element in the PV92 region of chromosome 16 within our own cheek cells. The ALU PV92 element is a short

PHB60057
interspersed element (SINE), making it an intron (region of DNA not serving any function in the body) this particular Alu element is dimorphic, and is present in some individuals and not others. Some people have the insert in one copy of chromosome 16 (one allele), others may have the insert in both copies of chromosome 16 (two alleles), while some may not have the insert on either copy of the chromosome. The presence or absence of this insert can be detected using PCR followed by agarose gel electrophoresis.Genetic testing has developed to a point whereby certain disease states caused by genes as well as the possibility of screening people for drug metabolism. Certain disease states can be assessed by doing neonatal tests e.g. in the UK DNA testing is done in neonates for sickle cell anaemia and cystic fibrosis. In the USA breast cancer patients are screened for metabolism of tamoxifen and this screening leads to whether the patient will be prescribed tamoxifen or not.Although it would have been possible to amplify a disease related DNA fragment, this was not done because of various ethical issues associated with gene screening used for diagnosis.The first reason for this is that if we were testing for a disease related gene it would be legally necessary to draw up informed consent forms and get all of those in the lab class to go through them and decide whether they want to give consent. Because of this some people may not be comfortable giving their consent because of the results they might get that would tell them their possible risk of contracting cancer. This could possibly reduce the sample size significantly.The next issue with screening for a cancer related gene would be that of confidentiality. This is because if we had been testing for the presence of a cancer related gene the lab class would essentially making a medical diagnosis and this would require a medical practitioner to be present, and revealing any results obtained would be the choice of the “patients” which could also cause problems with population size as well as running the risk of the results being given out to third parties and this may cause stigmatization along with discrimination e.g. when applying for health insurance.If we were to have done screening for a disease related gene and any patients were to end up having the disease causing genotype it would cause unnecessary lifelong psychosocial and psychological issues and would require counselling that the invigilators in the lab may not be trained for.In a nutshell, it is very unlikely that people would want to have themselves screened for a potentially cancer causing gene because of the “ticking time bomb” effect the results that may show a increased neoplastic risk in later life may give them, and if it were to be done more formalities would have to be gone through before conducting the experiment.

PHB60057
Describe screening for microsatellite instability as a diagnostic and prognostic marker for certain cancers, citing hereditary colorectal cancer (HNPCC) as an example (20)
Microsatellite instability is described by the national cancer institute as a change that occurs in the DNA of certain cells in which the number of repeats of microsatellites (short repeats of DNA) are not the same number as when the DNA was inherited. Microsatellite instability is thought to be caused by DNA mismatch repair gene (MMR) not working properly on certain genes.Many studies have been conducted to evaluate the role of high levels of MSI as a prognostic marker and predictor of risk of certain kinds of cancer, as well as an indicator of the success of chemotherapy in these patients.An example of this is in hereditary non polyp colorectal cancer. HNPCC is also known as Lynch syndrome, after Henry T Lynch who first characterised it in 1966. It is known to cause an early onset of cancers of the lower GI tract as well as those of the reproductive system. In HNPCC the cause of MSI is a germline mutation in a mismatch repair enzyme and alterations of the MutS homologue 2 and MutL homologue 1 mismatch repair genes account for 90%. Microsatellites that had changed in length are found in all HNPCCs, not only in the critical genetic region but virtually everywhere in the genome of tumours tested.Testing for microsatellite instability in colorectal cancer is done using polymerase chain reaction and it is the most straightforward method of doing so: DNA from a tumour and from normal tissue are tested. Mutations that alter microsatellite lengths are visualised as band shifts on electrophoresis gel. The choice of microsatellite markers is important for MSI testing. The 1997 Bethesda guidelines proposed a panel of five microsatellite markers for uniform analysis in HNPCC. These included two mononucleotide (BAT-25 and BAT-26) and three dinucleotide (D5S346, D2S123 and D17S250) repeats. The Bethesda guidelines have since been revised as the use of dinucleotide repeats may cause underestimation and overestimation of instability status. The revision mainly recommends the use of more mononucleotide markers especially in dinucleotide-unstable cases. Screening using the revised Bethesda MSI markers is now performed in trials for detection of HNPCC but diagnostic yield and costs cause an issue so even though screening in this way is feasible, the option of screening all patients with colorectal cancer with MSI should wait for more evidence of its clinical value and therapeutic influence of information gained.
How can the number of repeat sequences at the ends of chromosomes be modulated and is this important in neoplastic disease? (20)Repeat sequences at the end of chromosomes are known as telomeres and their function is to prevent the end of chromosomes from destruction. Telomeres are

PHB60057
modulated by the enzyme telomerase, which is a reverse transcriptase enzyme as DNA polymerase can only prime in the 5’ to 3’ direction and so cannot copy extreme end sequences of linear DNA.Telomerase carries its own template of RNA (TERC) which is complementary to telomere repeat sequences. This allows telomerase to create multiple copies of telomere repeat sequences without needing a DNA template to direct synthesis. A defect in telomerase proficiency causes abnormal maintenance of telomeres and this is associated with some disease states. In somatic cells the telomeres shorten with every cell division, and this may cause cell aging or cell growth arrest. Disease associated with this have links to premature aging where there is a major loss of telomeres whereas in cancer cells there is an excess production of telomerase, which allows cells to grow indefinitely.This is important in neoplastic disease as one will be able to test for high levels of telomerase and check for an increase in telomeres present within a patients DNA using bioassays. Telomerase inhibitors are a valuable new method used for cancer therapy. Their effectiveness however may be variable firstly because of slow response due to time needed for telomeres in cancer cells to undergo apoptosis, and so long term therapy used in combination with either radiotherapy or surgery would be necessary. There have also been concerned that inhibiting telomerase may lead to an increase in malignancy as it would cause genomic instability. These findings have emerged from studies on gene knockout mice.When using drugs that target telomeres and telomerase there are several taget sites that have been studied and can be manipulated. The RNA component can be targeted by the antisense oligodeoxynucleotides and the hammerhead ribozymes. The catalytic(hTERT) component can be targeted by reverse transcriptase inhibitors, and immunotherapy. There have also been studies conducting using small molecules tested using NCI-COMPARE system. They’re mechanism of action is not fully known but it is thought that they disrupt the anchoring of the telomerase to the enzyme or
What impact does CA repeat sequence in intron 1 of the EGFR have on neoplasia? (20)Epidermal growth factor(EGF) along with its complementary receptor tyrosine kinases are important in understanding how signals from growth factors can be used in a cell in order to modulate gene expression and cause cell proliferation and subsequently replication. EGFR(epidermal growth factor receptor), the first of its kind to be discovered is involved in cell growth and gene expression, however gene expression happens within the nucleus, and EGFR is an extracellular receptor so to get a signal from it to the nucleus certain pathways must be activated such as binding of the growth factor by a ligand, receptor demonization, Autophosphorylation, activation of signal transducers(intracellular), cascading of

PHB60057
kinases and regulation of transcription factors used for gene expression. All of these steps can be used as targets by therapeutic agents.Cancer cells have malfunctioning DNA and so grow and replicate exponentially and so it is known that growth factors and growth factor receptors play a critical role in tumour progression, and it is thought that the length of the CA repeat of intron 1 in the EGFR gene is correlated with the expression of the EGFR receptor in our cells. It has been found that EGFR is over expressed in a number of solid tumours and is linked to resistance to clinical strategies including hormone replacement therapy, chemotherapy and radiotherapy. This over expression is also linked to poor prognosis of cancer in patients that have it. Recent in vivo and in vitro studies have shown conclusive evidence that there is a decrease in gene transcription with an increase in CA repeats on intron 1 and vice versa. In breast cancer shorter CA repeats have been found and in these tumours EGFR over expression was noted.EGFR is a good target for neoplastic disease and there are currently several drugs that affect signal transduction. The anti-EGFR drugs are kinase inhibitor drugs that have their mode of action directed against kinase activity on members of the EGFR super family examples of the drugs are Tarceva, and Iressa. Another target used is the extra-cellular domain of EGFR receptor and monoclonal antibodies are used. An example is the drug Herceptin which causes receptor degradation, recruitment of immune cells causing cellular toxicity, as well as inhibition of angiogenesis of cancer cells.
What do you see as the clinical benefit to studying DNA repeat sequences in carcinogenesis? (10).
Carcinogenesis, the formation of cancer, can be caused by spontaneous mutation, which disrupts the cell cycle and causes uncontrolled cell proliferation. Carcinogenesis may also be caused by other factors such as chemicals (carcinogens) which involve DNA damage which is unable to repair itself causing mutated DNA resulting in carcinogenesis. Radiation (for example UV radiation causing skin cancer) can also cause carcinogenesis as radiation will penetrate skin and cause mutation of DNA.
DNA repeated sequences can be found all across the genome and vary in length and number in different people. In some cases; the number of repeats can help the development or maybe even cause certain conditions.
Thus the study of these repeated sequences can help in the treatment and prevention of some disorders, such as cancer. Studying repeat sequences has certain benefits such as giving an early prognosis of cancer, maybe even years before cancers start to develop. Early prognosis results in higher survival rates and in the USA there has been a major decrease in deaths caused by cancer in the past 2 years . the study of repeat sequences and the genome can also give details of drug

PHB60057
metabolism and this will give clues of what therapy is the best to use in a certain patient. There could also be some financial advantages involved as early detection will allow treatment to start earlier, decreasing the need for more costly treatments in later stages of disorders. Thus the study and research of DNA repeat sequences may be highly beneficial in cancer therapy.
Results
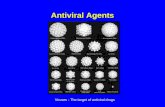
+/+ +/- -/- No result
Frequency 1 16 10 11
Percentage(f/38) 2.63% 42.11% 26.32% 28.95%
Fig 4. Pie chart of percentage frequency of different gene combinations for ALU PV92

PHB60057
REFERENCES
http://irc.igd.cornell.edu/MolecularMarkers/PCR%20basics.pdf
http://individual.utoronto.ca/myancheva/ESC102-BME-Lab-Report-Final.pdf
http://scientificinquiry.suite101.com/article.cfm/scientific_method_uses_experiments_and_controls
http://www.patient.co.uk/doctor/Newborn-Screening.htm
http://www.nci.nih.gov/dictionary/?CdrID=285933
http://www.promega.com/catalog/catalogproducts.aspx?categoryname=productleaf_1628&ckt=1
www.cancerresearchuk.org
http://www.ncbi.nlm.nih.gov/pubmed/9563488
http://www.genetichealth.com/CRC_HNPCC_Microsatellite_Instability_Testing.shtml
http://clincancerres.aacrjournals.org/content/11/23/8332.full.pdf