ANTIPHOSPHOLIPID ANTIBODY SYNDROME By Dr. Arvind Mishra M.D.

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 9 , N O . 1 8 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 2 . 0 5 8
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Antiphospholipid SyndromeRole of Vascular Endothelial Cells and Implications forRisk Stratification and Targeted Therapeutics
Michel T. Corban, MD,a Ali Duarte-Garcia, MD,b Robert D. McBane, MD,a Eric L. Matteson, MD, MPH,b,c
Lilach O. Lerman, MD, PHD,a,d Amir Lerman, MDa
ABSTRACT
Fro
of
Ep
the
Mi
au
Ma
Antiphospholipid syndrome (APS) is an autoimmune disease characterized by venous thromboembolism, arterial thrombosis,
and obstetric morbidities in the setting of persistently positive levels of antiphospholipid antibodies measured on 2 different
occasions 12 weeks apart. Patients with APS are at increased risk for accelerated atherosclerosis, myocardial infarction,
stroke, and valvular heart disease. Vascular endothelial cell dysfunction mediated by antiphospholipid antibodies and sub-
sequent complement systemactivation play a cardinal role in APS pathogenesis. Improved understanding of their pathogenic
function could help in the risk stratification of patients with APS and provide new molecular therapeutic targets.
(J Am Coll Cardiol 2017;69:2317–30) © 2017 by the American College of Cardiology Foundation.
T he term antiphospholipid syndrome (APS) wascoined in the 1980s to describe a conditionof autoantibody-induced thrombophilia (1).
This autoimmune prothrombotic condition is charac-terized by venous thromboembolism, arterial throm-bosis, and pregnancy morbidity in the setting oflaboratory evidence of elevated levels of antiphos-pholipid antibodies (aPLs). aPLs can be identified by1 of 3 assay platforms, namely, clot-based assaysto identify lupus anticoagulant, or enzyme-linkedimmunosorbent assays to identify anticardiolipin(aCL) or anti–b2-glycoprotein 1 (b2-GP1) antibodies(immunoglobulin G or immunoglobulin M). Regard-less of the assay, this class of antibodies targetsantiphospholipid-bound proteins. The prevalence ofaPLs in a random sample of 552 healthy blooddonors was found to be 6.5% and 9.4% for aCL immu-noglobulin G and immunoglobulin M antibodies,respectively. None of those normal subjects with
m the aDepartment of Cardiovascular Diseases, Mayo Clinic College of Me
Rheumatology, Department of Medicine, Mayo Clinic College of Medici
idemiology, Department of Health Sciences Research, Mayo Clinic CollegedDivision of Nephrology and Hypertension, Department of Medicine, May
nnesota. Dr. McBane has a research grant from Bristol-Myers Squibb. Dr.
thors have reported that they have no relationships relevant to the conte
nuscript received January 2, 2017; revised manuscript received February
positive aPLs developed thrombotic events at 1-yearfollow-up (2).
A definite diagnosis of APS requires the presence ofat least 1 clinical and 1 laboratory criterion. Clinicalcriteria may include objectively confirmed venous,arterial, or small-vessel thrombosis or pregnancymorbidity attributable to placental insufficiency,including pregnancy loss or premature birth. Labo-ratory criteria encompass persistently positive testresults for at least 1 of these 3 aPLs measures on 2 ormore occasions 12 weeks apart. The 12-week testinginterval is particularly important, given that someinfections and medications can cause transientaPL-positive testing (3,4).
APS typically presents in the fourth decade of lifeand is classified as either a primary disease or sec-ondary to another underlying autoimmune disease,solid tumor, or hematologic disorder. Approximately10% to 40% of patients with systemic lupus
dicine and Science, Rochester, Minnesota; bDivision
ne and Science, Rochester, Minnesota; cDivision of
of Medicine and Science, Rochester, Minnesota; and
o Clinic College of Medicine and Science, Rochester,
Leman is a consultant for Itamar Medical. All other
nts of this paper to disclose.
21, 2017, accepted February 28, 2017.

ABBR EV I A T I ON S
AND ACRONYMS
aCL = anticardiolipin antibody
aPL = antiphospholipid
antibody
apoER2 = apolipoprotein E
receptor 2
APS = antiphospholipid
syndrome
b2-GP1 = b2-glycoprotein 1
CAPS = catastrophic
antiphospholipid syndrome
eNOS = endothelial nitric oxide
synthase
HCQ = hydroxychloroquine
INR = international normalized
ratio
mTORC = mammalian target of
rapamycin complex
NO = nitric oxide
NOAC = new oral
anticoagulant agents
SLE = systemic lupus
erythematosus
Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2318
erythematosus (SLE) (5) and up to 20% ofpatients with rheumatoid arthritis (6) havepositive aPL serologies. Moreover, patientswith SLE who have positive lupus anticoagu-lant have a 50% chance of developing venousor arterial thrombotic events within a 20-yearfollow-up period (5). APS can affect any bodyorgan, and patients with APS have increasedrisk for thrombosis, accelerated atheroscle-rosis, myocardial infarction, and stroke (7,8).In a large prospective cohort study of 1,000patients with APS followed over a 10-yearperiod, deep vein thrombosis was the mostcommon presenting clinical manifestation(39%), followed by thrombocytopenia (30%),livedo reticularis (24%), stroke (20%), pul-monary embolism (14%), and myocardialinfarction (6%). In that study, thromboticevents occurred in 16.6% of patients duringthe first 5-year period and in 14.4% during thesecond 5-year period; 90.7% of patients werestill alive at 10 years (9). Despite high survivalrates, these data reflect a substantial diseaseburden and morbidity in patients with APS oncurrent treatment.
Obstetric morbidities in APS are thought to besecondary to placental vascular insufficiencies,with early (<10 weeks) and late ($10 weeks) mis-carriages being the most common obstetric manifes-tations (35% vs. 17%, respectively) of APS, followedby premature labor (11%), pre-eclampsia and/oreclampsia (5%), and intrauterine growth restriction(2%) (9).
A recent meta-analysis demonstrated that APS isassociated not only with clinical adverse cardiovas-cular events but also with subclinical cardiovascularrisk factors associated with endothelial cell dysfunc-tion, such as increased carotid artery intima-mediathickness and lower flow-mediated dilation, higherfrequency of carotid plaques, and increased preva-lence of pathological ankle-brachial indexes (10). Therenal vasculature may also be affected in APS, leadingto nephropathy, renal vein thrombosis, renal arterystenosis, thrombotic microangiopathy, hypertension,kidney infarction, and ultimately end-stage kidneydisease (11,12). The most severe, yet fortunatelyinfrequent form of APS is catastrophic APS (CAPS).CAPS, with an incidence of 0.9% (9) and mortality>50% (9,13), is defined as small-vessel thrombosisinvolving $3 organs, organ systems, and/or tissues,occurring simultaneously or in <1 week, along withpositive laboratory evidence of aPLs and no alterna-tive diagnosis (13).
PATHOGENESIS
THE CARDINAL ROLE OF ENDOTHELIAL CELLS. Thefact that normal healthy subjects with circulating aCLantibodies remained free of thrombotic events at1-year follow-up on one hand and the important directrole of aPLs in the pathogenesis of APS on the otherhand imply that additional underlying host suscepti-bility characteristics are necessary for the develop-ment of the disease. More than a decade ago, it wassuggested that endothelial cells play a central role inAPS pathogenesis and may represent the commonpathway through which autoimmunity and inflam-mation participate in APS (14). Although circulatingaPLs and underlying endothelial dysfunction are anecessary “first hit” for thrombosis in APS, an inflam-matory “second hit” is needed to precipitate a throm-botic event (15–17). Although elevated levels of aPLshave been associated with both vascular thrombosisand pregnancy morbidity in patients with APS (18,19),human aPLs injected into mice did not promotethrombosis in the absence of endothelial injury (20,21).Growing evidence demonstrates that endothelial celldysfunction, mediated by aPLs binding to endothelialcell b2-GP1 receptors, results in increased risk forthrombosis, accelerated atherosclerosis, myocardialinfarction, and stroke in patients with APS (7). Simi-larly, a recent in vitro study associated obstetricmorbidity in APS to placental inflammatory responsemediated by binding of aPLs to b2-GP1 receptors on thesurface of placental trophoblasts (22). Moreover, aninflammatory insult secondary to surgery, trauma, orinfection has been demonstrated to up-regulateexpression of b2-GP1 receptors on the endothelial cellsurface (Figure 1A) (15,17).Endothe l ia l n i t r i c ox ide synthase inh ib i t ion andthrombos is . Endothelium-derived nitric oxide (NO),produced by endothelial NO synthase (eNOS), isimportant for normal endothelial function andvascular health (23–25). Patients with APS have lowerplasma nitrite levels and an impaired endothelium-dependent vascular response, suggestive ofimpaired eNOS activity and reduced NO productionand endothelial function (26,27). The antithromboticeffects of eNOS and NO secreted from endothelialcells and platelets have been demonstrated in multi-ple animal and human studies. Indeed, eNOS-knockout mice demonstrated enhanced plateletaggregation (28) and increased predisposition tothrombosis, stroke, and atherosclerosis (29–32), anddecreased endogenous NO production in humanshas also been associated with increased risk forthrombosis (33–35).

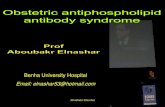
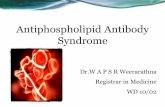
FIGURE 1 Antiphospholipid Syndrome Pathogenesis
(A) Up-regulation of beta-2 glycoprotein 1 (b2-GP1) receptors on endothelial cells following a “second hit” inflammatory insult. (B) Antiphospholipid antibody
(aPL)–mediated endothelial nitric oxide synthase (eNOS) inhibition, impaired nitric oxide (NO) production and release, and endothelial dysfunction. “First hit.”
(C) aPL-mediated endothelial cell proliferation, intimal hyperplasia, and nonatherosclerotic vascular stenosis. (D) Antiphospholipid syndrome (APS)–associated
accelerated atherosclerosis. (E) aPL-mediated platelet cell activation, aggregation, and thrombosis. (F) Complement system activation and thrombosis.
apoER2 ¼ apolipoprotein E receptor 2; C5a ¼ complement component 5a fragment; C5aR ¼ complement component 5a fragment receptor; C5b ¼ complement
component 5b fragment; C5bR ¼ complement component 5b fragment receptor; DI ¼ domain I of b2-GP1 receptor; DV ¼ domain V of b2-GP1 receptor;
LDL ¼ low-density lipoprotein; MAC ¼ membrane attack complex; mTORC ¼ mammalian target of rapamycin complex; PI3K-AKT ¼ phosphatidylinositol 3-kinase–AKT
pathway; PP2A ¼ protein phosphatase 2 A; VCAM ¼ vascular cell adhesion molecule.
J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2319
Recent elegant in vitro and animal studies havedemonstrated that aPL-mediated eNOS inhibition isthe molecular basis of endothelial dysfunction,increased leukocyte–endothelial cell adhesion, andthrombus formation in patients with APS (36,37).Binding of circulating aPLs to domain I of the b2-GP1receptor on endothelial cells induces b2-GP1 dimer-ization (38,39). Subsequent interaction betweendomain V of dimerized b2-GP1 and low-densitylipoprotein–binding domain 1 of apolipoprotein Ereceptor 2 (apoER2) mediates aPL-induced eNOSinhibition, up-regulation of adhesion molecule
expression, and increased production of endothelin-1and tissue factor, ultimately leading to thrombusformation (37,38,40–44). It was recently shown thatthe intracellular pathway of aPL-induced eNOS inhi-bition following aPL, b2-GP1, and apoER2 interactionis mediated by protein phosphatase 2 A dephosphor-ylation of a critical serine residue (Ser1177) ofeNOS (Figure 1B) (37,45,46). Thus, circulatingaPL-associated NO-dependent endothelial dysfunc-tion, mediated by inhibitory dephosphorylation ofeNOS, plays an important role in the pathogenesis ofAPS-related thrombosis.

Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2320
Endothel ia l ce l l dysfunct ion and vascu lopathy .Circulating aPL-induced endothelial cell dysfunctionmay also lead to vasculopathy. Steps to aPL-mediatedvasculopathy include diffuse intimal hyperplasia,accelerated atherosclerosis, and microvasculardysfunction.Endothelial cell proliferation and intimal
hyperplasia. Patients with APS have significantlyincreased carotid intima-media thickness andsmaller carotid luminal diameter in the absenceof atherosclerotic disease (47,48). Moreover,pathological specimens of patients with APSnephropathy show evidence of vascular cellularinfiltrates, severe intimal hyperplasia, and fibrosisof the intima and media (49–51).
Interestingly, the pathogenesis of acute peripheralarterial occlusion (49) and ischemic cerebrovascularevents (52,53) in patients with APS has been associ-ated primarily with severe concentric intimal andmedial hyperplasia and fibrous occlusions with vari-able evidence of thrombosis and thrombus stages.Two important recent studies by Canaud et al. (54,55)have demonstrated that aPLs, specifically aCL andanti-b2-GP1 antibodies, induce endothelial cell pro-liferation and intimal hyperplasia through activationof the phosphatidylinositol 3-kinase–AKT pathwayand, subsequently, the mammalian target of rapa-mycin complex (mTORC) (Figure 1C). Moreover,mTORC pathway activation in endothelial cellscorrelated with aPL titers, and an mTORC pathwayinhibitor (sirolimus) prevented recurrent renal allo-graft vasculopathy in patients with APS (54,55).Endothelial cell dysfunction and accelerated
atherosclerosis. Endothelial dysfunction is theearliest detectable stage of atherosclerosis (56–59).Circulating aPL-mediated endothelial dysfunction isassociated with accelerated peripheral and coronaryatherosclerosis (60–66) relative to the generalpopulation with comparable risk factors (67).Circulating aCL and anti-b2-GP1 antibodies mediateinternalization of oxidized low-density lipoprotein–b2-GP1 complexes into macrophages to formfoam cells, which leads to the development ofatherosclerotic lesions (Figure 1D) (68–70).
Multiple clinical studies have demonstrated astrong correlation between circulating aPLs andsystemic atherosclerosis in humans, including pe-ripheral arterial disease, coronary artery disease,acute myocardial infarction, and ischemic stroke(8,66,71–76). Moreover, aPL levels have been associ-ated with increased mortality rates due to coronaryartery disease (73). Premature atherosclerosis inthese patients has been linked to localized proin-flammatory nontraditional immunopathological risk
factors mediated by circulating aPLs. Aggressivecontrol of traditional cardiovascular risk factors istherefore recommended to prevent further endothe-lial injury.
Interestingly, recurrent thrombosis was recentlysuggested to be a potential mechanism for coronaryplaque progression in cardiac allograft transplantvasculopathy (77). Taking into account a similaritybetween these 2 features of accelerated atheroscle-rosis, the association between recurrent clinical orsubclinical thrombosis and accelerated atheroscle-rosis in patients with APS warrants furtherinvestigation.Endothelial cell dysfunction and coronary microvascular
obstruction. Coronary microvascular endothelialdysfunction in APS has also been associated withischemic heart disease. Cardiac magnetic resonancestudies of these patients with otherwise low pre-testprobability for coronary artery disease revealed ahigher than anticipated incidence of late myocardialgadolinium enhancement consistent with subclinicalcoronary microvascular dysfunction (78). Similarly,60% of asymptomatic patients with APS and noknown systemic risk factors had subclinicalmyocardial perfusion abnormalities (23% exerciseinduced and 42% persistent) on single-positronemission computed tomography (technetium-99msestamibi) imaging, suggestive of endothelialdysfunction and associated thrombosis in coronarymicrovasculature (79). In both studies, the level ofcirculating aPLs positively correlated with detectedmyocardial perfusion defects.
THROMBOSIS: ACTIVATION OF PLATELETS AND
COMPLEMENT SYSTEM. Binding of circulating aPLsto domain I of b2-GP1 receptors on platelets inducesvenous and/or arterial thrombosis through increasedproduction of thromboxane B2. Thromboxane A2, apotent platelet activator, results in enhanced adhe-sion of platelets to collagen and increased plateletaggregation before being degraded to thromboxane B2
(Figure 1E) (80). Indeed, a strong correlation has beenreported between the level of anti-b2-GP1 domain 1aPLs and adverse clinical outcomes in patients withAPS (81,82).
In addition to eNOS inhibition and platelet aggre-gation, the thrombogenic effects of aPLs also involveactivation of the classical complement system(21,83,84). Complement activation and depositionhave been associated with placental injury in femalepatients with APS experiencing obstetric complica-tions (85).
Girardi et al. (86) suggested that heparin preventedobstetric complications by blocking complement

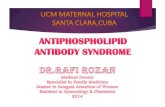
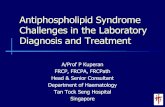
FIGURE 2 Libman-Sacks Endocarditis
Transthoracic echocardiographic (TTE) and transesophageal echocardiographic (TEE) images of a 33-year-old woman who presented with
acute-onset shortness of breath secondary to flash pulmonary edema in the setting of new diagnosis of antiphospholipid syndrome (strongly
positive anticardiolipin immunoglobulin G antibody, >100 GPL), Libman-Sacks endocarditis, and moderate-to-severe mitral regurgitation.
(A) TTE parasternal long-axis view of the mitral valve with thickened anterior and posterior leaflets and adherent deposits on the leaflets
coaptation point. (B) TEE images demonstrating mitral valve vegetations on the atrial aspect of both leaflets tips consistent with
Libman-Sacks endocarditis. (C) Moderate-to-severe mitral valve regurgitation associated with incomplete coaptation of mitral valve leaflets
secondary to Libman-Sacks endocarditis lesions.
J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2321
activation, rather than by directly preventingplacental thrombosis. In mice, C3 and C5 activationwas required for aPL-induced thrombosis andincreased leukocyte adhesion to endothelium (84,87).In addition, interaction between C5a and C5aR wasrequired for aPL-induced pregnancy loss (88).Furthermore, C5a binding to endothelial cells resul-ted in increased neutrophil adhesion, tissue factorexpression, and release of other procoagulant sub-stances (89,90). C5b-initiated assembly of the mem-brane attack complex subsequently triggersproinflammatory signaling pathways and promotesthrombus formation (Figure 1F) (91). In contrast, C3convertase inhibitor and anti-C5 mouse antibodiesblocked aPL-induced thrombus formation in thismodel (84,87). Similarly, blockade of C5aR preventedthrombus formation in a rat model of antibody-mediated thrombotic glomerulonephritis (92). Eculi-zumab, a C5 inhibitor, prevented APS-associatedthrombotic microangiopathy in a post–renal trans-plantation patient with CAPS and in other patientswith recurrent CAPS (93,94).
VALVULAR HEART DISEASE IN APS
Between 15% and 30% of patients with APS havevalvular heart disease, known as Libman-Sacksendocarditis or nonbacterial thrombotic endocarditis(9,95). The reported incidence rate is 5% over a10-year period (9). Although the revised classification
criteria for definite APS diagnosis do not includevalvular heart disease, the international consensusstatement defines aPL-associated cardiac valve dis-ease as the coexistence of aPLs and echocardio-graphic evidence of mitral or aortic valve lesions.These criteria include valve thickness >3 mm, local-ized thickening of the proximal or middle portion ofthe valve leaflet, irregular nodules on the atrial aspectof the mitral valve or the vascular surface of the aorticvalve, and/or moderate-to-severe valvular regurgita-tion or stenosis (Figure 2). Infective endocarditisand rheumatic heart disease history are importantexclusions (4).
Histologically, Libman-Sacks endocarditis lesionsare small (up to 3 to 4 mm), sterile, fibrinous vege-tations with varying fibroblastic organization, neo-revascularization, and mononuclear inflammatorycell infiltration. Fibrous plaque formation, scarring,and focal calcifications may be seen in advancedstages (96).
Although the risk for valvular heart disease is 3-foldhigher in patients with circulating aPLs (97), its precisepathophysiology remains unclear. Ziporen et al. (98)demonstrated deposits of aPLs and complementon deformed heart valves of patients with APS.Blank et al. (99) identified target epitopes of anti-b2-GP1 antibodies on valvular endothelial cell b2-GP1receptors. These findings suggest that the pathogen-esis could include aPL-mediated valvular endothelialcell activation with complement fixation, similar to

TABLE 1 Primary Thromboprophylaxis in
Antiphospholipid Syndrome
General measures for allantiphospholipid-positive patients
� Assessment and management oftraditional cardiovascular risk factors
� In high-risk situations (puerperium,surgery, prolonged immobilization),use usual doses of LMWH forthromboprophylaxis
Antiphospholipid-positivenon-SLE patients(obstetric APS andasymptomatic carriers)
� Low-dose aspirin (75–100 mg/day) inthose with a high-risk aPL profile,especially in the presence of otherthrombotic risk factors
Patients with SLE andpositive aPLs
� Hydroxychloroquine (200–400 mg/day)þ low-dose aspirin (75–100 mg/day)
aPL ¼ antiphospholipid antibody; APS ¼ antiphospholipid syndrome;LMWH ¼ low–molecular weight heparin; SLE ¼ systemic lupus erythematosus.
Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2322
endothelial cell injury in other vascular beds. It isunclear whether antithrombotic therapy limits thedevelopment of valvular injury in this setting.
RISK STRATIFICATION: INCREMENTAL
VALUE OF ENDOTHELIAL FUNCTION TESTING
AND CLINICAL IMPLICATIONS
Tools capable of early and reliable identification ofthe high-risk APS patient population would be clini-cally useful. Known thrombotic risk variables includea “triple-positive” aPL profile (positive for lupusanticoagulant, aCL, and anti-b2-GP1 antibodies)(100,101), high mean platelet volumes as a surrogatefor increased platelet activation (102), and decreasedplasminogen and elevated plasminogen activator in-hibitor-1 levels (103). The Global APS Score, a novel,promising risk assessment tool, may be useful for thispurpose. The tool, on the basis of prospective studiesin primary and secondary APS (104,105), uses the aPLprofile, hypertension, dyslipidemia, diabetes melli-tus, and the presence of other autoimmune anti-bodies, namely, antinuclear antibodies, extractablenuclear antibodies (anti-Ro, La, Smith, ribonucleo-protein, scleroderma-70, Jo-1 antibodies), anddouble-stranded deoxyribonucleic acid antibodies topredict thrombosis risk (106).
Measures of endothelial cell dysfunction are notincluded in this risk assessment tool. Other importantrisk factors, including obesity and cigarette smoking,are also not used. Given the central role of endothelialdysfunction in APS, future risk stratification toolsmight benefit from incorporating either invasive ornoninvasive measures of endothelial function, suchas intracoronary acetylcholine challenge testing, orbrachial reactivity and plethysmography finger arte-rial pulsatile volume changes (EndoPAT, ItamarMedical, Caesarea, Israel). On the basis of the growingbody of evidence that endothelial dysfunction is apredictor of adverse cardiovascular events indepen-dently of traditional risk factors (107), the role ofendothelial function assessment for risk stratificationand potential therapeutic implications in APS needsfurther investigation. Moreover, the benefit of theassessment of APS score in individuals with unex-plained endothelial dysfunction and acceleratedatherosclerosis may be explored.
PHARMACOLOGICAL THERAPY: CURRENT
RECOMMENDATIONS, EMERGING THERAPIES,
AND POTENTIALLY PROMISING
TARGETED THERAPIES
PRIMARY THROMBOPROPHYLAXIS. Thrombophiliaremains the hallmark of APS, and thrombosis
prevention is a major goal of therapy. Asymptomaticpatients with positive APS-related antibodies maydevelop thrombotic events at a rate of 0% to 4% peryear, especially in the setting of SLE (108). Althoughthromboembolic risk stratification tools for patientswith APS are limited, contemporary recommenda-tions for primary thromboprophylaxis in high-riskSLE and non-SLE patients with positive aPL serologyhave been proposed (Table 1).
The 13th International Congress on Anti-phospholipid Antibodies Prevention and Manage-ment Task Force recommended evaluation and tightcontrol of traditional cardiovascular risk factors aspart of primary prophylaxis in APS (108). Althoughhypertension has been associated with thrombosis inaPL-positive patients, hypertriglyceridemia, lowhigh-density lipoprotein levels, and central obesityare the most common cardiovascular risk factorsassociated with primary APS (109). Control of tradi-tional cardiovascular risk factors is indeed importantto help prevent additional insult to the vascularendothelium in patients with APS. The task force alsorecommended that all aPL-positive patients receiveappropriate thromboprophylaxis with heparin inhigh-risk situations, such as surgery, postpartum, andprolonged immobilization (108).
Two recent meta-analyses have suggested that therisk for first thrombotic event was significantlydecreased by low-dose aspirin among asymptomaticaPL-positive subjects, patients with SLE, and patientswith obstetric APS (110,111). A recent open-labelrandomized trial showed no incremental primarythromboprophylaxis benefit in adding anticoagu-lation with warfarin to low-dose aspirin alone (112).As such, primary prophylaxis with anticoagulantagents is not recommended in otherwise healthyambulatory patients with no prior thrombotic history.Currently, guidelines recommend the use of low-dose

TABLE 2 Secondary Thromboprophylaxis in
Antiphospholipid Syndrome
Definite APS and a firstvenous event
� Indefinite oral anticoagulant therapyto a target INR of 2.0–3.0
Definite APS and arterialthrombosis
� Indefinite oral anticoagulant therapyto a target INR >3.0 or combinedantiaggregant-anticoagulant (INR2.0–3.0) therapy
Patients with venous orarterial thrombosiswho do not fulfillcriteria for APS
� Treatment as per usual recommen-dations for arterial or venousthrombosis
APS ¼ antiphospholipid syndrome; INR ¼ international normalized ratio.
J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2323
aspirin in aPL-positive patients, with or without SLE,with a high-risk aPL profile and/or additional throm-botic risk factors (108).
Hydroxychloroquine (HCQ) is an antimalarial usedextensively in autoimmune disease that has immu-nomodulatory and possibly antithrombotic proper-ties. HCQ has been shown to reduce thrombus sizeand platelet aggregation in mouse models (113,114).The antithrombotic efficacy of HCQ in humans hasbeen shown during its use for deep vein thrombosisprophylaxis after hip surgery (115). HCQ is widelyused in SLE for its disease-modifying effects (116),and its use in asymptomatic patients with positiveaPL serologies resulted in a reduction of thrombo-embolic events (117). In patients with obstetric APS,HCQ has been considered after failure of standardtreatment with heparin and aspirin (118). Currentguidelines recommend the use of HCQ in addition tolow-dose aspirin only in aPL-positive patients withSLE (108). There are no recommendations regardingthe use of HCQ for primary thrombosis prevention inother aPL-positive populations.
SECONDARY THROMBOPROPHYLAXIS. Anticoagulationis the mainstay therapy for secondary thrombopro-phylaxis in patients with APS. Current guidelines forsecondary thromboprophylaxis, summarized inTable 2, recommend consideration of whether thefirst thrombotic event was venous or arterial (108). Ifthe initial event was venous thromboembolism, it isrecommended that moderate-intensity warfarintherapy targeting international normalized ratio (INR)values of 2.0 to 3.0 be initiated, with heparinbridging. Two systematic reviews have confirmedboth the efficacy and safety of this approach in pre-venting recurrent venous thrombosis (119,120).
In comparison, management of arterial thromboticevents has been less well studied and more contro-versial, with 2 approaches proposed: moderate in-tensity (INR goal 2 to 3) versus high-intensity (INR >3)warfarin anticoagulation. A systematic review ofobservational studies concluded that the rate ofrecurrent arterial thrombosis was significantly lowerwith INR>3 (3.8%) versus INR<3 (23%) (120). AlthoughAPASS (Antiphospholipid Antibodies and StrokeStudy), a large prospective cohort study of 1,770 pa-tients, found no difference in recurrent stroke anddeath in patients treated with moderate-intensitywarfarin (INR 1.4 to 2.8) versus those treated withhigh-dose aspirin (325 mg/day) (121), a small random-ized controlled trial of 20 patients with APS andischemic stroke showed that patients treated with acombination of low-dose aspirin (100 mg/day) andmoderate-intensity warfarin (INR 2.0 to 3.0) had a
significantly lower incidence of recurrent strokecompared with those treated with low-dose aspirinalone (122). However, it is important to note that noneof the patients included in the APASS study met thecurrently accepted diagnostic criteria for APS. Thetask force of the 13th International Congress onAntiphospholipid Antibodies recommended high-intensity warfarin (INR >3.0) or combined moderate-intensity warfarin (INR 2.0 to 3.0) therapy and anantiplatelet agent for secondary thromboprophylaxisin patients with APS with arterial thrombotic events(108); however, this recommendation did not reachpanel consensus. Importantly, patients with venous orarterial thrombosis who do not fulfill criteria for aconclusive APS diagnosis should be treated the sameas aPL-negative patients with similar venous or arte-rial thrombotic event presentation (108).
Secondary thromboprophylaxis, whether forvenous or arterial thrombosis, should be continuedindefinitely (108). A retrospective study revealed asignificant increase (relative risk: 4.55 [95% confi-dence interval: 2.67 to 7.43] vs. 0.36 [95% confidenceinterval: 0.24 to 0.53] on any treatment, p < 0.001 forboth) in recurrent thrombosis soon after stopping oralanticoagulant agents (123). Elevated titers of aCL an-tibodies predict recurrent thrombosis and death inthe 6-month period following the initial episode ofvenous thromboembolism (124).
NEW ORAL ANTICOAGULANT AGENTS. The efficacyof the new oral anticoagulants (NOACs), the directthrombin inhibitor dabigatran, and direct anti–factorXa inhibitors rivaroxaban, apixaban, and edoxaban,in APS remains unclear, and is largely on the basis ofcase reports and case series. A recent systematic re-view showed that approximately 20% of patients withAPS on NOACs developed vascular events during amean follow-up period of 12 months (125), whereasone-third of patients developed recurrent eventsduring 2 years of follow-up (126).

TABLE 3 Alternative and Adjunctive Therapeutic Options for Specific Clinical
Scenarios in Antiphospholipid Syndrome
Known warfarin allergy,warfarin intolerance, orpoor anticoagulant controlon warfarin despitetherapeutic target (as perTable 2)
� Treatment with, or addition of, NOAC: directthrombin inhibitor dabigatran or direct anti–factor Xa inhibitors rivaroxaban, apixaban, oredoxaban
Heparin-inducedthrombocytopenia
� Treatment with fondaparinux or argatroban
Refractory APS despiteadequate anticoagulation(as per Table 2)
� Consider starting statin therapy� Consider adding rituximab therapy� Consider adding glucocorticosteroids and
IVIG þ plasma exchange
CAPS � Heparin anticoagulation þ glucocorticosteroids þIVIG and/or plasma exchange reduces mortality
� Eculizumab reduces mortality
Renal transplantation patientswith APS
� Sirolimus decreases recurrent vascular lesionsand vascular proliferation
� Eculizumab for treatment and prevention ofthrombotic microangiopathy in patients withhistory of CAPS
Obstetric APS � Heparin (unfractionated or LMWH) þ lowdose aspirin (75–100 mg/day)
� Patients on warfarin should be switched toheparin (unfractionated or LMWH) immedi-ately upon pregnancy confirmation to avoidteratogenicity
� Extended thromboprophylaxis (up to 6 weeksafter delivery) for high-risk patients
� Indefinite anticoagulation for APS patientswith prior thrombotic events
CAPS ¼ catastrophic antiphospholipid syndrome; IVIG ¼ intravenous immunoglobulin;NOAC ¼ new oral anticoagulant; other abbreviations as in Table 1.
Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2324
The RAPS (Rivaroxaban Versus Warfarin to TreatPatients With Thrombotic Antiphospholipid Syn-drome, With or without Systemic Lupus Erythema-tosus) trial enrolled only patients with venousthrombotic events, and a laboratory surrogateoutcome measure (endogenous thrombin potential)was the primary outcome. Rivaroxaban did not reachthe noninferiority threshold from the laboratory sur-rogate standpoint, but there was no increase inthrombotic risk compared with standard-intensitywarfarin (127).
Two currently ongoing randomized controlledclinical trials, ASTRO-APS (Apixaban for the Second-ary Prevention of Thromboembolism Among PatientsWith the Antiphospholipid Syndrome; NCT02295475)and TRAPS (Rivaroxaban in Thrombotic Anti-phospholipid Syndrome; NCT02157272), will helpclarify the role of NOACs in the management of APS.Currently, the 14th International Congress on Anti-phospholipid Antibodies task force recommends theuse of NOACs only when there is a known warfarinallergy, warfarin intolerance, or poor anticoagulationcontrol (Table 3) (128).
OTHER ANTICOAGULANT AGENTS. The evidencebase for the use of other anticoagulant agents, such as
fondaparinux or argatroban, in APS is also limited tocase reports and case series and is predominantly inthe setting of heparin-induced thrombocytopenia(129,130). The 14th International Congress on Anti-phospholipid Antibodies task force recommends theuse of these anticoagulant agents only in the settingof heparin-induced thrombocytopenia in APS(Table 3) (128).
STATINS. The immunomodulatory and anti-inflammatory properties of statins can be beneficialin APS (131). Simvastatin and fluvastatin suppressanti-b2GPI antibody–mediated endothelial activation(132), and fluvastatin also reduced up-regulation oftissue factor expression by aPLs on endothelial cells(133). Moreover, patients with APS treated with flu-vastatin showed decreases in multiple inflammatoryand prothrombotic biomarkers, including interleukin1b, vascular endothelial growth factor, tumor necrosisfactor–a, inducible protein–10, soluble CD40 ligand,and soluble tissue factor (134). To date, there are noformal recommendations for the use of statins inpatients with APS who have normal lipid profiles;however, statins can be considered in patients withrefractory APS despite adequate anticoagulation(Table 3) (128). Furthermore, we submit that endo-thelial function assessment may play a role in iden-tifying patients with APS and normal lipid profileswho might benefit from statin therapy.
mTOR INHIBITORS. Patients with APS nephropathywho required transplantation and were receivingsirolimus had no recurrence of vascular lesions and adecrease in vascular proliferation on biopsycompared with patients with aPLs who were not onsirolimus (Table 3) (54). Although the mTOR pathwaymay represent potential future therapeutic targets fortreatment of APS vasculopathy, the prothromboticeffects of mTOR inhibitors might limit their efficacyin this syndrome (135–138).
CELL DEPLETION THERAPY. Rituximab, a chimericmonoclonal antibody targeting CD20 cells, has beeneffectively used in cases of CAPS, anticoagulationfailure, recurrent thrombosis, and thrombocytopenia(139). In a retrospective single-center study, ritux-imab decreased thrombotic events (average follow-upperiod 40 months) in patients with SLE-associatedAPS with recurrent thrombosis despite adequatewarfarin therapy or life-threatening active diseaserefractory to conventional therapy (140). It is impor-tant to note that immunosuppression was added toongoing anticoagulation therapy (141).
Moreover, rituximab therapy was associated withclinical response in non-thrombosis-related APSmanifestations, including thrombocytopenia, cardiac

J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2325
valve disease, skin ulcers, nephropathy, and cogni-tive dysfunction, in a small pilot open-label phase2 trial of 20 patients with APS. Interestingly, therewas no significant variation in the aPL titers atfollow-up (142).
Although the role of rituximab in APS is not yetclearly defined, anti-CD20 antibodies may be animportant future tool in the management of hema-tologic and microangiopathic manifestations, aswell as thrombotic cases of APS refractory to anti-coagulation therapy (Table 3) (128).
COMPLEMENT INHIBITION. Complement systemactivation plays an important role in pathogenesisand thrombus formation in APS. Eculizumab is amonoclonal antibody that binds the C5 protein,inhibiting its cleavage into C5a and C5b. By blockingthe complement cascade, the formation of themembrane attack complex is inhibited. A smallnumber of case reports and case series have reportedsuccessful use of eculizumab in acute CAPS, aswell as in treatment and prevention of thromboticmicroangiopathy following renal transplantation inpatients with CAPS (Table 3) (93,94,143). Currently,there are no recommendations for the global useof eculizumab in APS; however, selective treatmentin refractory cases remains an attractive tool forthe expanding tool box for these complicatedpatients (128).
GLUCOCORTICOSTEROIDS, PLASMA EXCHANGE,
AND INTRAVENOUS IMMUNOGLOBULINS. The use ofglucocorticosteroids, plasma exchange, and intrave-nous immunoglobulins in APS is limited to refractorycases of recurrent thrombosis despite adequateanticoagulation (144,145) and CAPS (Table 3). Thecombination of heparin anticoagulation, glucocorti-costeroids, and plasma exchange, intravenous im-munoglobulins, or both reduced mortality comparedwith other treatment strategies in patients withCAPS (146).
MANAGEMENT OF OBSTETRIC APS. The ninthedition of the American College of Chest Physiciansevidence-based clinical practice guidelines and the14th International Congress on AntiphospholipidAntibodies task force report on obstetric APS recom-mend treatment of women with obstetric APS with acombination of heparin, either unfractionated orlow–molecular weight heparin, and low-dose aspirin(75 to 100 mg/day) (Table 3) (147,148). Although2 randomized controlled trials reported a higher rateof live births with the addition of unfractionatedheparin to low-dose aspirin (149,150), these resultswere not confirmed in 2 additional randomizedcontrolled trials (151,152). Pooled data of all available
randomized controlled trials showed a beneficialeffect on live births with unfractionated heparin andlow-dose aspirin, whereas data on the efficacy of low–
molecular weight heparin and low-dose aspirin wereinconclusive (148).
For patients already receiving warfarin, therapyshould be transitioned to either low–molecularweight heparin or unfractionated heparin andlow-dose aspirin. This transition should occurimmediately upon pregnancy confirmation to avoidteratogenicity. The risk for warfarin-induced fetaleffects is highest during the first 6 weeks, especiallyfor patients requiring more than 5 mg of warfarindaily. For selected high-risk patients in whom sig-nificant risk factors persist following delivery, inter-national guidelines suggest extended prophylaxis(up to 6 weeks after delivery) following dischargefrom the hospital (108,147). For patients with APSwith prior thrombotic events, anticoagulant agentsshould be continued indefinitely. Importantly,maternal warfarin therapy is safe for nursing infants.
b2-GP1 DOMAINS I AND V ANTAGONISTS. Thebinding of aPLs to domain I of b2-GP1 receptors onendothelial cells induces a conformational change inthe receptor and promotes binding of domain V toapoER2. This binding results in eNOS inhibition-mediated endothelial cell dysfunction and ulti-mately thrombosis (Figure 1). Similarly, binding ofaPLs to domain I of the b2-GP1 receptor on plateletsinduces thrombus formation because of increasedthromboxane B2 secretion, enhanced adhesionof platelets to collagen, and increased plateletaggregation.
To date, only a handful of in vitro and mousestudies investigated potential b2-GP1 antagonists.Ioannou et al. (153) demonstrated that the mutateddomain I of b2-GP1 receptors was associated withreduced binding to aPLs in vitro, and that therecombinant antigenic target peptide domain I ofb2-GP1 inhibited venous thrombotic events anddecreased vascular cell adhesion molecule–1 expres-sion on aortic endothelial cells in mice injected withhuman aPLs (154). Moreover, Ostertag et al. (155)demonstrated that TIFI, a 20–amino acid syntheticpeptide with conformational similarities to domain Vof b2-GP1, inhibited APS-induced thrombosis in mice.Similarly, Kolyada et al. (156) demonstrated that theA1-A1 molecule, which inhibits binding of apoER2 todomain V of b2-GP1, reduced arterial thrombus size inAPS mice. These studies support the pursuit ofunique targets, possibly within the b2-GP1 receptor,for future drug development beyond simple antico-agulant therapy.

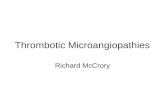
CENTRAL ILLUSTRATION Antiphospholipid Syndrome Pathogenesis
Corban, M.T. et al. J Am Coll Cardiol. 2017;69(18):2317–30.
Pathogenesis of antiphospholipid syndrome and recommended areas for research: “first hit” circulating antiphospholipid antibodies (aPLs) and underlying endothelial
dysfunction and “second hit” inflammatory insult result in impaired nitric oxide (NO)–dependent endothelial function, accelerated atherosclerosis, nonatherosclerotic
vasculopathy, platelet activation and aggregation, and complement system activation. Research in aPL and beta-2 glycoprotein 1 receptor (b2-GP1) interaction,
b2-GP1 and apolipoprotein E receptor 2 (apoER2) interaction, and complement system activation is recommended. C5a ¼ complement component 5a fragment;
C5b ¼ complement component 5b fragment.
Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2326
CONCLUSIONS
APS is an autoimmune disease characterized bythrombophilia, adverse obstetric events and recur-rent miscarriages, accelerated atherosclerosis,increased risk for myocardial infarction and stroke,and valvular heart disease. Morbidity and mortalityin APS is strongly associated with aPL-mediatedvascular endothelial cell dysfunction and comple-ment system activation. Although thrombophilia isthe hallmark of APS, accurate identification of pa-tients at increased risk for thrombosis remains achallenge.
To date, therapeutic efforts have focused mostlyon preventing recurrent thrombotic events in
patients with APS, with only limited research directedtoward new therapies for primary prevention.Although anticoagulation is the mainstay therapy forsecondary thromboprophylaxis in patients with APS,a significant number of those patients developrecurrent thrombosis despite conventional thera-peutic anticoagulation targets. Simply increasing thedoses of anticoagulant agents comes at the expense ofincreased risk for bleeding. Indeed, hemorrhageremains the most common cause of death (23%) inpatients with primary APS (9).
The cardinal role of vascular endothelial dysfunc-tion in APS pathogenesis (summarized in the CentralIllustration) calls for more focused researchregarding aPLs and b2-GP1 interaction, b2-GP1 and

J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2327
apoER2 interaction, and associated intracellularsignaling pathways. Large prospective cohort studiesand randomized clinical trials are warranted to studythe role of endothelial function testing in therisk stratification of patients with APS, investigatethe association between recurrent thrombosis andaccelerated atherosclerosis in patients with APS, andevaluate targeted therapies against endothelialdysfunction-mediated APS thrombophilia and vas-culopathy. A paradigm shift aimed at investigatingnew therapeutic targets is of the utmost importanceand is potentially highly rewarding and timely
for reducing morbidity and mortality in patientswith APS.
ACKNOWLEDGMENTS The authors thank Mr. KevinYouel for his artistic contribution to the Figure 1 andthe Mayo Clinic Echocardiography Laboratory forproviding the echocardiographic images in Figure 2.
ADDRESS FOR CORRESPONDENCE: Dr. AmirLerman, Mayo Clinic, Department of CardiovascularDiseases, 200 First Street SW, Rochester,Minnesota 55905. E-mail: [email protected].
RE F E RENCE S
1. Hughes GR. The antiphospholipid syndrome: tenyears on. Lancet 1993;342:341–4.
2. Vila P, Hernández MC, López-Fernández MF,Batlle J. Prevalence, follow-up and clinical sig-nificance of the anticardiolipin antibodies innormal subjects. Thromb Haemost 1994;72:209–13.
3. Lim W. Antiphospholipid syndrome. Hematolo-gy Am Soc Hematol Educ Program 2013;2013:675–80.
4. Miyakis S, Lockshin MD, Atsumi T, et al. Inter-national consensus statement on an update of theclassification criteria for definite antiphospholipidsyndrome (APS). J Thromb Haemost 2006;4:295–306.
5. Petri M. Epidemiology of the antiphospholipidantibody syndrome. J Autoimmun 2000;15:145–51.
6. Olech E, Merrill JT. The prevalence and clinicalsignificance of antiphospholipid antibodies inrheumatoid arthritis. Curr Rheumatol Rep 2006;8:100–8.
7. Mineo C. Inhibition of nitric oxide and anti-phospholipid antibody-mediated thrombosis. CurrRheumatol Rep 2013;15:324.
8. Soltész P, Szekanecz Z, Kiss E, Shoenfeld Y.Cardiac manifestations in antiphospholipid syn-drome. Autoimmun Rev 2007;6:379–86.
9. Cervera R, Serrano R, Pons-Estel GJ, et al., forthe Euro-Phospholipid Project Group (EuropeanForum on Antiphospholipid Antibodies). Morbidityand mortality in the antiphospholipid syndromeduring a 10-year period: a multicentre prospectivestudy of 1000 patients. Ann Rheum Dis 2015;74:1011–8.
10. Ambrosino P, Lupoli R, Di Minno A, Iervolino S,Peluso R, Di Minno MN. Markers of cardiovascularrisk in patients with antiphospholipid syndrome: ameta-analysis of literature studies. Ann Med 2014;46:693–702.
11. Amigo MC. Kidney disease in antiphospholipidsyndrome. Rheum Dis Clin North Am 2006;32:509–22.
12. Sciascia S, Cuadrado MJ, Khamashta M,Roccatello D. Renal involvement in anti-phospholipid syndrome. Nat Rev Nephrol 2014;10:279–89.
13. Asherson RA, Cervera R, de Groot PG, et al., forthe Catastrophic Antiphospholipid SyndromeRegistry Project Group. Catastrophic anti-phospholipid syndrome: international consensusstatement on classification criteria and treatmentguidelines. Lupus 2003;12:530–4.
14. Blum A, Simsolo C. The antiphospholipid syn-drome and endothelial function. Isr Med Assoc J2004;6:556–8.
15. Agostinis C, Biffi S, Garrovo C, et al. In vivodistribution of b2 glycoprotein I under variouspathophysiologic conditions. Blood 2011;118:4231–8.
16. Meroni PL. Anti-beta-2 glycoprotein I epitopespecificity: from experimental models to diag-nostic tools. Lupus 2016;25:905–10.
17. Meroni PL, Borghi MO, Raschi E, Tedesco F.Pathogenesis of antiphospholipid syndrome: un-derstanding the antibodies. Nat Rev Rheumatol2011;7:330–9.
18. Galli M, Luciani D, Bertolini G, Barbui T. Anti-b2-glycoprotein I, antiprothrombin antibodies, andthe risk of thrombosis in the antiphospholipidsyndrome. Blood 2003;102:2717–23.
19. Miyakis S, Giannakopoulos B, Krilis SA. Beta 2glycoprotein I—function in health and disease.Thromb Res 2004;114:335–46.
20. Arad A, Proulle V, Furie RA, Furie BC, Furie B.b2-Glycoprotein-1 autoantibodies from patientswith antiphospholipid syndrome are sufficient topotentiate arterial thrombus formation in a mousemodel. Blood 2011;117:3453–9.
21. Fischetti F, Durigutto P, Pellis V, et al.Thrombus formation induced by antibodies to b2-glycoprotein I is complement dependent and re-quires a priming factor. Blood 2005;106:2340–6.
22. Mulla MJ, Brosens JJ, Chamley LW, et al.Antiphospholipid antibodies induce a pro-inflammatory response in first trimester tropho-blast via the TLR4/MyD88 pathway. Am J ReprodImmunol 2009;62:96–111.
23. De Caterina R, Libby P, Peng HB, et al. Nitricoxide decreases cytokine-induced endothelialactivation. Nitric oxide selectively reduces endo-thelial expression of adhesion molecules andproinflammatory cytokines. J Clin Invest 1995;96:60–8.
24. Palmer RM, Ferrige AG, Moncada S. Nitricoxide release accounts for the biological activity ofendothelium-derived relaxing factor. Nature 1987;327:524–6.
25. Radomski MW, Palmer RM, Moncada S.Endogenous nitric oxide inhibits human plateletadhesion to vascular endothelium. Lancet 1987;2:1057–8.
26. Ames PR, Batuca JR, Ciampa A, Iannaccone L,Delgado Alves J. Clinical relevance of nitric oxidemetabolites and nitrative stress in thromboticprimary antiphospholipid syndrome. J Rheumatol2010;37:2523–30.
27. Charakida M, Besler C, Batuca JR, et al.Vascular abnormalities, paraoxonase activity, anddysfunctional HDL in primary antiphospholipidsyndrome. JAMA 2009;302:1210–7.
28. Freedman JE, Sauter R, Battinelli EM, et al.Deficient platelet-derived nitric oxide andenhanced hemostasis in mice lacking the NOSIIIgene. Circ Res 1999;84:1416–21.
29. Atochin DN, Wang A, Liu VW, et al. Thephosphorylation state of eNOS modulates vascularreactivity and outcome of cerebral ischemiain vivo. J Clin Invest 2007;117:1961–7.
30. Huang Z, Huang PL, Ma J, et al. Enlarged in-farcts in endothelial nitric oxide synthaseknockout mice are attenuated by nitro-L-arginine.J Cereb Blood Flow Metab 1996;16:981–7.
31. Kuhlencordt PJ, Rosel E, Gerszten RE, et al.Role of endothelial nitric oxide synthase in endo-thelial activation: insights from eNOS knockoutendothelial cells. Am J Physiol Cell Physiol 2004;286:C1195–202.
32. Lefer DJ, Jones SP, Girod WG, et al. Leukocyte-endothelial cell interactions in nitric oxidesynthase-deficient mice. Am J Physiol 1999;276:H1943–50.
33. Freedman JE. Oxidative stress and platelets.Arterioscler Thromb Vasc Biol 2008;28:s11–6.
34. Freedman JE, Loscalzo J. Nitric oxide and itsrelationship to thrombotic disorders. J ThrombHaemost 2003;1:1183–8.
35. Prasad M, McBane R, Reriani M, Lerman LO,Lerman A. Coronary endothelial dysfunction isassociated with increased risk of venous throm-boembolism. Thromb Res 2016;139:17–21.

Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2328
36. Mineo C, Shaul PW. New insights into themolecular basis of the antiphospholipid syndrome.Drug Discov Today Dis Mech 2011;8:e47–52.
37. Ramesh S, Morrell CN, Tarango C, et al. Anti-phospholipid antibodies promote leukocyte-endothelial cell adhesion and thrombosis in miceby antagonizing eNOS via b2GPI and apoER2. J ClinInvest 2011;121:120–31.
38. de Groot PG, van Lummel M, Pennings M,et al. b2-Glycoprotein I and LDL-receptor familymembers. Thromb Res 2004;114:455–9.
39. Ninivaggi M, Kelchtermans H, Lindhout T, deLaat B. Conformation of beta2glycoprotein I andits effect on coagulation. Thromb Res 2012;130Suppl 1:S33–6.
40. Jankowski M, Vreys I, Wittevrongel C, et al.Thrombogenicity of b2-glycoprotein I-dependentantiphospholipid antibodies in a photochemicallyinduced thrombosis model in the hamster. Blood2003;101:157–62.
41. Pierangeli SS, Chen PP, Raschi E, et al. Anti-phospholipid antibodies and the antiphospholipidsyndrome: pathogenic mechanisms. SeminThromb Hemost 2008;34:236–50.
42. Pierangeli SS, Vega-Ostertag M, Harris EN.Intracellular signaling triggered by anti-phospholipid antibodies in platelets and endo-thelial cells: a pathway to targeted therapies.Thromb Res 2004;114:467–76.
43. Romay-Penabad Z, Aguilar-Valenzuela R,Urbanus RT, et al. Apolipoprotein E receptor 2 isinvolved in the thrombotic complications in amurine model of the antiphospholipid syndrome.Blood 2011;117:1408–14.
44. Urbanus RT, Pennings MT, Derksen RH, deGroot PG. Platelet activation by dimeric b2-glycoprotein I requires signaling via both glyco-protein Iba and apolipoprotein E receptor 20 .J Thromb Haemost 2008;6:1405–12.
45. Greif DM, Kou R, Michel T. Site-specificdephosphorylation of endothelial nitric oxidesynthase by protein phosphatase 2A: evidence forcrosstalk between phosphorylation sites.Biochemistry 2002;41:15845–53.
46. Michell BJ, Chen ZP, Tiganis T, et al. Coordi-nated control of endothelial nitric-oxide synthasephosphorylation by protein kinase C and thecAMP-dependent protein kinase. J Biol Chem2001;276:17625–8.
47. Der H, Kerekes G, Veres K, et al. Impairedendothelial function and increased carotid intima-media thickness in association with elevated vonWillebrand antigen level in primary anti-phospholipid syndrome. Lupus 2007;16:497–503.
48. Medina G, Casaos D, Jara LJ, et al. Increasedcarotid artery intima-media thickness may beassociated with stroke in primary antiphospholipidsyndrome. Ann Rheum Dis 2003;62:607–10.
49. Alarcón-Segovia D, Cardiel MH, Reyes E.Antiphospholipid arterial vasculopathy.J Rheumatol 1989;16:762–7.
50. Hughson MD, McCarty GA, Brumback RA.Spectrum of vascular pathology affecting patientswith the antiphospholipid syndrome. Hum Pathol1995;26:716–24.
51. Long BR, Leya F. The role of antiphospholipidsyndrome in cardiovascular disease. HematolOncol Clin North Am 2008;22:79–94.
52. Hughson MD, McCarty GA, Sholer CM,Brumback RA. Thrombotic cerebral arteriopathy inpatients with the antiphospholipid syndrome. ModPathol 1993;6:644–53.
53. Westerman EM, Miles JM, Backonja M,Sundstrom WR. Neuropathologic findings in multi-infarct dementia associated with anticardiolipinantibody. Evidence for endothelial injury as theprimary event. Arthritis Rheum 1992;35:1038–41.
54. Canaud G, Bienaimé F, Tabarin F, et al. Inhi-bition of the mTORC pathway in the anti-phospholipid syndrome. N Engl J Med 2014;371:303–12.
55. Canaud G, Legendre C, Terzi F. AKT/mTORCpathway in antiphospholipid-related vasculop-athy: a new player in the game. Lupus 2015;24:227–30.
56. Gimbrone MA Jr., García-Cardeña G. Vascularendothelium, hemodynamics, and the pathobi-ology of atherosclerosis. Cardiovasc Pathol 2013;22:9–15.
57. Gimbrone MA Jr., García-Cardeña G. Endo-thelial cell dysfunction and the pathobiology ofatherosclerosis. Circ Res 2016;118:620–36.
58. Stary HC. Natural history and histologicalclassification of atherosclerotic lesions: an update.Arterioscler Thromb Vasc Biol 2000;20:1177–8.
59. Virmani R, Kolodgie FD, Burke AP, Farb A,Schwartz SM. Lessons from sudden coronarydeath: a comprehensive morphological classifica-tion scheme for atherosclerotic lesions. Arte-rioscler Thromb Vasc Biol 2000;20:1262–75.
60. Ames PR, Margarita A, Alves JD. Anti-phospholipid antibodies and atherosclerosis: in-sights from systemic lupus erythematosus andprimary antiphospholipid syndrome. Clin Rev Al-lergy Immunol 2009;37:29–35.
61. Belizna CC, Richard V, Primard E, et al. Earlyatheroma in primary and secondary anti-phospholipid syndrome: an intrinsic finding. SeminArthritis Rheum 2008;37:373–80.
62. Cervera R, Boffa MC, Khamashta MA,Hughes GR. The Euro-Phospholipid project:epidemiology of the antiphospholipid syndrome inEurope. Lupus 2009;18:889–93.
63. Matsuura E, Koike T. Accelerated atheromaand anti-beta2-glycoprotein I antibodies. Lupus2000;9:210–6.
64. Petri M. Detection of coronary artery diseaseand the role of traditional risk factors in theHopkins Lupus Cohort. Lupus 2000;9:170–5.
65. Shoenfeld Y, Gerli R, Doria A, et al. Acceler-ated atherosclerosis in autoimmune rheumaticdiseases. Circulation 2005;112:3337–47.
66. Vaarala O. Antiphospholipid antibodies andatherosclerosis. Lupus 1996;5:442–7.
67. Jara LJ, Medina G, Vera-Lastra O, Shoenfeld Y.Atherosclerosis and antiphospholipid syndrome.Clin Rev Allergy Immunol 2003;25:79–88.
68. Hasunuma Y, Matsuura E, Makita Z, Katahira T,Nishi S, Koike T. Involvement of b2-glycoprotein Iand anticardiolipin antibodies in oxidatively
modified low-density lipoprotein uptake by mac-rophages. Clin Exp Immunol 1997;107:569–73.
69. Kobayashi K, Matsuura E, Liu Q, et al.A specific ligand for b2-glycoprotein I mediatesautoantibody-dependent uptake of oxidized lowdensity lipoprotein by macrophages. J Lipid Res2001;42:697–709.
70. Liu Q, Kobayashi K, Furukawa J, et al.u-Carboxyl variants of 7-ketocholesteryl estersare ligands for b2-glycoprotein I and mediateantibody-dependent uptake of oxidized LDL bymacrophages. J Lipid Res 2002;43:1486–95.
71. Adler Y, Finkelstein Y, Zandeman-Goddard G,et al. The presence of antiphospholipid antibodiesin acute myocardial infarction. Lupus 1995;4:309–13.
72. Erkkilä AT, Närvänen O, Lehto S, Uusitupa MI,Ylä-Herttuala S. Autoantibodies against oxidizedlow-density lipoprotein and cardiolipin in patientswith coronary heart disease. Arterioscler ThrombVasc Biol 2000;20:204–9.
73. Erkkilä AT, Närvänen O, Lehto S, Uusitupa MI,Ylä-Herttuala S. Antibodies against oxidized LDLand cardiolipin and mortality in patients withcoronary heart disease. Atherosclerosis 2005;183:157–62.
74. Sherer Y, Shoenfeld Y. Mechanisms of disease:atherosclerosis in autoimmune diseases. Nat ClinPract Rheumatol 2006;2:99–106.
75. Shoenfeld Y, Sherer Y, George J, Harats D.Autoantibodies associated with atherosclerosis.Ann Med 2000;32 Suppl 1:37–40.
76. Veres K, Lakos G, Kerényi A, et al. Anti-phospholipid antibodies in acute coronary syn-drome. Lupus 2004;13:423–7.
77. Matsuo Y, Cassar A, Li J, et al. Repeated epi-sodes of thrombosis as a potential mechanism ofplaque progression in cardiac allograft vasculop-athy. Eur Heart J 2013;34:2905–15.
78. Sacré K, Brihaye B, Hyafil F, et al. Asymp-tomatic myocardial ischemic disease in anti-phospholipid syndrome: a controlled cardiacmagnetic resonance imaging study. ArthritisRheum 2010;62:2093–100.
79. Padjas A, Płazak W, Celi�nska-Lowenhoff M,et al. Myocardial ischaemia, coronary atheroscle-rosis and pulmonary pressure elevation in anti-phospholipid syndrome patients. Adv Clin ExpMed 2016;25:1199–205.
80. Urbanus RT, Derksen RH, de Groot PG.Platelets and the antiphospholipid syndrome.Lupus 2008;17:888–94.
81. de Laat B, de Groot PG. Autoantibodiesdirected against domain I of beta2-glycoprotein I.Curr Rheumatol Rep 2011;13:70–6.
82. de Laat B, Pengo V, Pabinger I, et al. The as-sociation between circulating antibodies againstdomain I of beta2-glycoprotein I and thrombosis:an international multicenter study. J ThrombHaemost 2009;7:1767–73.
83. Giannakopoulos B, Krilis SA. The pathogenesisof the antiphospholipid syndrome. N Engl J Med2013;368:1033–44.
84. Pierangeli SS, Girardi G, Vega-Ostertag M,Liu X, Espinola RG, Salmon J. Requirement of

J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7 Corban et al.M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0 Antiphospholipid Syndrome
2329
activation of complement C3 and C5 for anti-phospholipid antibody-mediated thrombophilia.Arthritis Rheum 2005;52:2120–4.
85. Shamonki JM, Salmon JE, Hyjek E,Baergen RN. Excessive complement activation isassociated with placental injury in patients withantiphospholipid antibodies. Am J Obstet Gynecol2007;196:167.e1–5.
86. Girardi G, Redecha P, Salmon JE. Heparinprevents antiphospholipid antibody-induced fetalloss by inhibiting complement activation. Nat Med2004;10:1222–6.
87. Holers VM, Girardi G, Mo L, et al. ComplementC3 activation is required for antiphospholipidantibody-induced fetal loss. J Exp Med 2002;195:211–20.
88. Girardi G, Berman J, Redecha P, et al. Com-plement C5a receptors and neutrophils mediatefetal injury in the antiphospholipid syndrome[published correction appears in J Clin Invest2004;113:646]. J Clin Invest 2003;112:1644–54.
89. Davis WD, Brey RL. Antiphospholipid anti-bodies and complement activation in patients withcerebral ischemia. Clin Exp Rheumatol 1992;10:455–60.
90. Wojta J, Kaun C, Zorn G, et al. C5a stimulatesproduction of plasminogen activator inhibitor-1 inhuman mast cells and basophils. Blood 2002;100:517–23.
91. Wetsel RA. Structure, function and cellularexpression of complement anaphylatoxin re-ceptors. Curr Opin Immunol 1995;7:48–53.
92. Kondo C, Mizuno M, Nishikawa K, Yuzawa Y,Hotta N, Matsuo S. The role of C5a in the devel-opment of thrombotic glomerulonephritis in rats.Clin Exp Immunol 2001;124:323–9.
93. Lonze BE, Singer AL, Montgomery RA. Eculi-zumab and renal transplantation in a patient withCAPS. N Engl J Med 2010;362:1744–5.
94. Shapira I, Andrade D, Allen SL, Salmon JE.Brief report: induction of sustained remission inrecurrent catastrophic antiphospholipid syndromevia inhibition of terminal complement with eculi-zumab. Arthritis Rheum 2012;64:2719–23.
95. Zuily S, Huttin O, Mohamed S, Marie PY,Selton-Suty C, Wahl D. Valvular heart disease inantiphospholipid syndrome. Curr Rheumatol Rep2013;15:320.
96. Hojnik M, George J, Ziporen L, Shoenfeld Y.Heart valve involvement (Libman-Sacks endo-carditis) in the antiphospholipid syndrome. Circu-lation 1996;93:1579–87.
97. Zuily S, Regnault V, Selton-Suty C, et al.Increased risk for heart valve disease associatedwith antiphospholipid antibodies in patients withsystemic lupus erythematosus: meta-analysis ofechocardiographic studies. Circulation 2011;124:215–24.
98. Ziporen L, Goldberg I, Arad M, et al. Libman-Sacks endocarditis in the antiphospholipid syn-drome: immunopathologic findings in deformedheart valves. Lupus 1996;5:196–205.
99. Blank M, Shani A, Goldberg I, et al. Libman-Sacks endocarditis associated with anti-phospholipid syndrome and infection. Thromb Res2004;114:589–92.
100. Hernández-Molina G, Espericueta-Arriola G,Cabral AR. The role of lupus anticoagulant andtriple marker positivity as risk factors forrethrombosis in patients with primary anti-phospholipid syndrome. Clin Exp Rheumatol 2013;31:382–8.
101. Pengo V, Ruffatti A, Legnani C, et al. Clinicalcourse of high-risk patients diagnosed with anti-phospholipid syndrome. J Thromb Haemost 2010;8:237–42.
102. Rupa-Matysek J, Gil L, Wojtasi�nska E,Ciepłuch K, Lewandowska M, Komarnicki M. Therelationship between mean platelet volume andthrombosis recurrence in patients diagnosed withantiphospholipid syndrome. Rheumatol Int 2014;34:1599–605.
103. Aĭsina RB, Mukhametova LI, Ostriakova EV,et al. [Polymorphism of the plasminogen activatorinhibitor type 1 gene, plasminogen level andthrombosis in patients with antiphospholipid syn-drome]. Biomed Khim 2014;60:72–93.
104. Sciascia S, Cuadrado MJ, Sanna G, et al.Thrombotic risk assessment in systemic lupus er-ythematosus: validation of the global anti-phospholipid syndrome score in a prospectivecohort. Arthritis Care Res (Hoboken) 2014;66:1915–20.
105. Sciascia S, Sanna G, Murru V, Roccatello D,Khamashta MA, Bertolaccini ML. The global anti-phospholipid syndrome score in primary APS.Rheumatology (Oxford) 2015;54:134–8.
106. Sciascia S, Bertolaccini ML. Thrombotic riskassessment in APS: the Global APS Score (GAPSS).Lupus 2014;23:1286–7.
107. Matsuzawa Y, Kwon TG, Lennon RJ,Lerman LO, Lerman A. Prognostic value of flow-mediated vasodilation in brachial artery andfingertip artery for cardiovascular events: a sys-tematic review and meta-analysis. J Am HeartAssoc 2015;4:e002270.
108. Ruiz-Irastorza G, Cuadrado MJ, Ruiz-Arruza I,et al. Evidence-based recommendations for theprevention and long-term management ofthrombosis in antiphospholipid antibody-positivepatients: report of a task force at the 13th Inter-national Congress on antiphospholipid antibodies.Lupus 2011;20:206–18.
109. Medina G, Gutiérrez-Moreno AL, Vera-Lastra O, Saavedra MA, Jara LJ. Prevalence ofmetabolic syndrome in primary antiphospholipidsyndrome patients. Autoimmun Rev 2011;10:214–7.
110. Arnaud L, Mathian A, Devilliers H, et al. Pa-tient-level analysis of five international cohortsfurther confirms the efficacy of aspirin for theprimary prevention of thrombosis in patients withantiphospholipid antibodies. Autoimmun Rev2015;14:192–200.
111. Arnaud L, Mathian A, Ruffatti A, et al. Efficacyof aspirin for the primary prevention of thrombosisin patients with antiphospholipid antibodies: aninternational and collaborative meta-analysis.Autoimmun Rev 2014;13:281–91.
112. Cuadrado MJ, Bertolaccini ML, Seed PT, et al.Low-dose aspirin vs low-dose aspirin plus low-intensity warfarin in thromboprophylaxis: a pro-spective, multicentre, randomized, open,
controlled trial in patients positive for anti-phospholipid antibodies (ALIWAPAS). Rheuma-tology (Oxford) 2014;53:275–84.
113. Edwards MH, Pierangeli S, Liu X, Barker JH,Anderson G, Harris EN. Hydroxychloroquine re-verses thrombogenic properties of anti-phospholipid antibodies in mice. Circulation 1997;96:4380–4.
114. Espinola RG, Pierangeli SS, Gharavi AE,Harris EN. Hydroxychloroquine reverses plateletactivation induced by human IgG antiphospholipidantibodies [published correction appears inThromb Haemost 2002;87:IX]. Thromb Haemost2002;87:518–22.
115. Loudon JR. Hydroxychloroquine and post-operative thromboembolism after total hipreplacement. Am J Med 1988;85:57–61.
116. Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy and sideeffects of antimalarials in systemic lupus erythe-matosus: a systematic review. Ann Rheum Dis2010;69:20–8.
117. Erkan D, Yazici Y, Peterson MG,Sammaritano L, Lockshin MD. A cross-sectionalstudy of clinical thrombotic risk factors and pre-ventive treatments in antiphospholipid syndrome.Rheumatology (Oxford) 2002;41:924–9.
118. Sciascia S, Branch DW, Levy RA, et al. Theefficacy of hydroxychloroquine in altering preg-nancy outcome in women with antiphospholipidantibodies. Evidence and clinical judgment.Thromb Haemost 2016;115:285–90.
119. Lim W, Crowther MA, Eikelboom JW. Man-agement of antiphospholipid antibody syndrome:a systematic review. JAMA 2006;295:1050–7.
120. Ruiz-Irastorza G, Hunt BJ, Khamashta MA.A systematic review of secondary thrombopro-phylaxis in patients with antiphospholipid anti-bodies. Arthritis Rheum 2007;57:1487–95.
121. Levine SR, Brey RL, Tilley BC, et al., for theAPASS Investigators. Antiphospholipid antibodiesand subsequent thrombo-occlusive events in pa-tients with ischemic stroke. JAMA 2004;291:576–84.
122. Okuma H, Kitagawa Y, Yasuda T, Tokuoka K,Takagi S. Comparison between single antiplatelettherapy and combination of antiplatelet and anti-coagulation therapy for secondary prevention inischemic stroke patients with antiphospholipidsyndrome. Int J Med Sci 2009;7:15–8.
123. Khamashta MA, Cuadrado MJ, Mujic F,Taub NA, Hunt BJ, Hughes GR. The managementof thrombosis in the antiphospholipid-antibodysyndrome. N Engl J Med 1995;332:993–7.
124. Schulman S, Svenungsson E, Granqvist S, forthe Duration of Anticoagulation Study Group.Anticardiolipin antibodies predict early recurrenceof thromboembolism and death among patientswith venous thromboembolism following antico-agulant therapy. Am J Med 1998;104:332–8.
125. Yazici A, Unlu O, Erkan D. A systematic reviewof direct oral anticoagulant use in anti-phospholipid syndrome. Presented at: 15th Inter-national Congress on Antiphospholipid Antibodies;September 21–24, 2016; Istanbul, Turkey (Relo-cated to North Cyprus).

Corban et al. J A C C V O L . 6 9 , N O . 1 8 , 2 0 1 7
Antiphospholipid Syndrome M A Y 9 , 2 0 1 7 : 2 3 1 7 – 3 0
2330
126. Unlu O, Cohen H, Cuadrado M, et al. Anti-phospholipid Syndrome Alliance for Clinical Trialsand International Networking (APS ACTION) Clin-ical Database and Repository Analysis: direct oralanticoagulant use among antiphospholipid syn-drome patients. Presented at: 15th InternationalCongress on Antiphospholipid Antibodies;September 21–24, 2016; Istanbul, Turkey (Relo-cated to North Cyprus).
127. Cohen H, Hunt BJ, Efthymiou M, et al., for theRAPS Trial Investigators. Rivaroxaban versuswarfarin to treat patients with thrombotic anti-phospholipid syndrome, with or without systemiclupus erythematosus (RAPS): a randomised,controlled, open-label, phase 2/3, non-inferioritytrial. Lancet Haematol 2016;3:e426–36.
128. Erkan D, Aguiar CL, Andrade D, et al. 14thInternational Congress on Antiphospholipid Anti-bodies: task force report on antiphospholipidsyndrome treatment trends. Autoimmun Rev2014;13:685–96.
129. Holtan SG, Knox SK, Tefferi A. Use of fon-daparinux in a patient with antiphospholipid anti-body syndrome and heparin-associatedthrombocytopenia. J Thromb Haemost 2006;4:1632–4.
130. Pendleton R, Wheeler MM, Rodgers GM.Argatroban dosing of patients with heparin-induced thrombocytopenia and an elevated aPTTdue to antiphospholipid antibody syndrome[published correction appears in Ann Pharmac-other 2006;40:1477]. Ann Pharmacother 2006;40:972–6.
131. Danesh FR, Anel RL, Zeng L, Lomasney J,Sahai A, Kanwar YS. Immunomodulatory effects ofHMG-CoA reductase inhibitors. Arch Immunol TherExp (Warsz) 2003;51:139–48.
132. Meroni PL, Raschi E, Testoni C, et al. Statinsprevent endothelial cell activation induced byantiphospholipid (anti-beta2-glycoprotein I) anti-bodies: effect on the proadhesive and proin-flammatory phenotype. Arthritis Rheum 2001;44:2870–8.
133. Ferrara DE, Swerlick R, Casper K, et al. Flu-vastatin inhibits up-regulation of tissue factorexpression by antiphospholipid antibodies onendothelial cells. J Thromb Haemost 2004;2:1558–63.
134. Erkan D, Willis R, Murthy VL, et al.A prospective open-label pilot study of fluvastatinon proinflammatory and prothrombotic bio-markers in antiphospholipid antibody positive pa-tients. Ann Rheum Dis 2014;73:1176–80.
135. Ahya VN, McShane PJ, Baz MA, et al.Increased risk of venous thromboembolism with asirolimus-based immunosuppression regimen inlung transplantation. J Heart Lung Transplant2011;30:175–81.
136. Austin SK, Starke RD, Lawrie AS, Cohen H,Machin SJ, Mackie IJ. The VWF/ADAMTS13 axis inthe antiphospholipid syndrome: ADAMTS13 anti-bodies and ADAMTS13 dysfunction. Br J Haematol2008;141:536–44.
137. Hidalgo LG. Inhibition of the mTORC pathwayin the antiphospholipid syndrome. N Engl J Med2014;371:1554.
138. Verhave JC, Tagalakis V, Suissa S, Madore F,Hébert MJ, Cardinal H. The risk of thromboembolicevents in kidney transplant patients. Kidney Int2014;85:1454–60.
139. Berman H, Rodríguez-Pintó I, Cervera R,et al., for the Catastrophic Antiphospholipid Syn-drome (CAPS) Registry Project Group (EuropeanForum on Antiphospholipid Antibodies). Rituximabuse in the catastrophic antiphospholipid syn-drome: descriptive analysis of the CAPS registrypatients receiving rituximab. Autoimmun Rev2013;12:1085–90.
140. Wang CR, Liu MF. Rituximab usage in sys-temic lupus erythematosus-associated anti-phospholipid syndrome: a single-centerexperience. Semin Arthritis Rheum 2016;46:102–8.
141. Bakshi J, Stevens R. Rituximab therapy forrecurrent thromboembolic disease in anti-phospholipid syndrome. Lupus 2013;22:865–7.
142. Erkan D, Vega J, Ramón G, Kozora E,Lockshin MD. A pilot open-label phase II trial ofrituximab for non-criteria manifestations of anti-phospholipid syndrome. Arthritis Rheum 2013;65:464–71.
143. Canaud G, Kamar N, Anglicheau D, et al.Eculizumab improves posttransplant thromboticmicroangiopathy due to antiphospholipid syn-drome recurrence but fails to prevent chronicvascular changes. Am J Transplant 2013;13:2179–85.
144. Sciascia S, Giachino O, Roccatello D. Pre-vention of thrombosis relapse in antiphospholipidsyndrome patients refractory to conventionaltherapy using intravenous immunoglobulin. ClinExp Rheumatol 2012;30:409–13.
145. Sherer Y, Levy Y, Shoenfeld Y. Intravenousimmunoglobulin therapy of antiphospholipid syn-drome. Rheumatology (Oxford) 2000;39:421–6.
146. Cervera R, Rodríguez-Pintó I,Colafrancesco S, et al. 14th International Congresson Antiphospholipid Antibodies Task Force Reporton Catastrophic Antiphospholipid Syndrome.Autoimmun Rev 2014;13:699–707.
147. Bates SM, Greer IA, Middeldorp S,Veenstra DL, Prabulos AM, Vandvik PO. VTE,thrombophilia, antithrombotic therapy, andpregnancy: antithrombotic therapy and pre-vention of thrombosis, 9th ed: American
College of Chest Physicians evidence-basedclinical practice guidelines. Chest 2012;141:e691S–736S.
148. de Jesus GR, Agmon-Levin N, Andrade CA,et al. 14th International Congress on Anti-phospholipid Antibodies task force report on ob-stetric antiphospholipid syndrome. AutoimmunRev 2014;13:795–813.
149. Kutteh WH. Antiphospholipid antibody-associated recurrent pregnancy loss: treatmentwith heparin and low-dose aspirin is superior tolow-dose aspirin alone. Am J Obstet Gynecol1996;174:1584–9.
150. Rai R, Cohen H, Dave M, Regan L. Rando-mised controlled trial of aspirin and aspirin plusheparin in pregnant women with recurrentmiscarriage associated with phospholipid anti-bodies (or antiphospholipid antibodies). BMJ1997;314:253–7.
151. Farquharson RG, Quenby S, Greaves M.Antiphospholipid syndrome in pregnancy: arandomized, controlled trial of treatment[published correction appears in ObstetGynecol 2002;100:1361]. Obstet Gynecol2002;100:408–13.
152. Laskin CA, Spitzer KA, Clark CA, et al. Lowmolecular weight heparin and aspirin for recurrentpregnancy loss: results from the randomized,controlled HepASA Trial. J Rheumatol 2009;36:279–87.
153. Ioannou Y, Pericleous C, Giles I, Latchman DS,Isenberg DA, Rahman A. Binding of anti-phospholipid antibodies to discontinuous epitopeson domain I of human b2-glycoprotein I: mutationstudies including residues R39 to R43. ArthritisRheum 2007;56:280–90.
154. Ioannou Y, Romay-Penabad Z, Pericleous C,et al. In vivo inhibition of antiphospholipidantibody-induced pathogenicity utilizing the anti-genic target peptide domain I of b2-glycoprotein I:proof of concept. J Thromb Haemost 2009;7:833–42.
155. Ostertag MV, Liu X, Henderson V,Pierangeli SS. A peptide that mimics the Vth re-gion of beta-2-glycoprotein I reversesantiphospholipid-mediated thrombosis in mice.Lupus 2006;15:358–65.
156. Kolyada A, Porter A, Beglova N. Inhibition ofthrombotic properties of persistent autoimmuneanti-b2GPI antibodies in the mouse model ofantiphospholipid syndrome. Blood 2014;123:1090–7.
KEY WORDS antiphospholipid antibodies,atherosclerosis, epidemiology,thrombophilia, vascular endothelium,warfarin