Antiphospholipid antibody syndrome due to interferon treatment for hepatitis C
11
Antiphospholipid antibody syndrome due to interferon treatment for hepatitis C Michi Shinohara, MD Pacific Dermatologic Association August 10, 2008
description
Antiphospholipid antibody syndrome due to interferon treatment for hepatitis C. Michi Shinohara, MD Pacific Dermatologic Association August 10, 2008. Case presentation. 53 yo woman with 3 week history of progressive superficial cutaneous thrombosis - PowerPoint PPT Presentation
Transcript of Antiphospholipid antibody syndrome due to interferon treatment for hepatitis C
Antiphospholipid antibody syndrome due to interferon
treatment for hepatitis C
Michi Shinohara, MDPacific Dermatologic Association
August 10, 2008
Case presentation
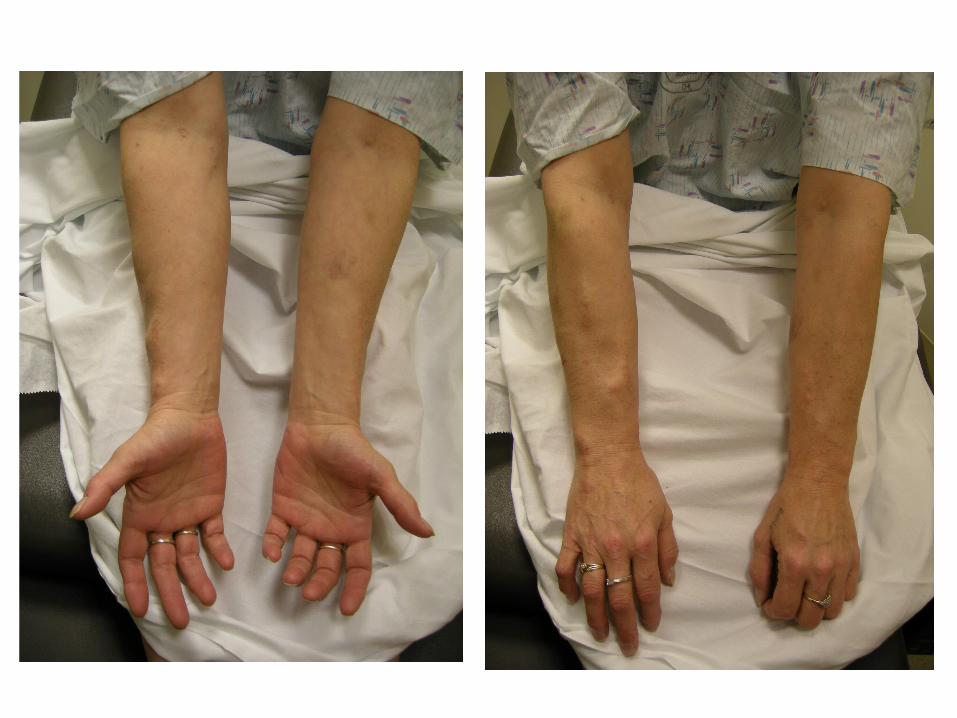
• 53 yo woman with 3 week history of progressive superficial cutaneous thrombosis
• History of Hep C with cryoglobulinemia and cutaneous vasculitis, s/p IFN and ribavarin
• IVDU > 10y ago, current skin lesions in areas of prior injection
• Health otherwise stable, no dyspnea, chest pain or leg edema

Work up• Upper extremity duplex confirmed superficial
clot; no DVT• Assessed for hypercoaguable state
– Anticardiolipin antibodies, lupus anticoagulant, inherited thrombophilias, cryoglobulins negative
2 glycoprotein-1 Ab (2-GP-1) titer >99th percentile
• Referred to hematology, initiated on anticoagulation for antiphospholipid antibody syndrome (APS)
Antiphospholipid antibody syndrome
• Primary or secondary (SLE)• Diagnosis based on antiphospholipid
antibodies “aPL Abs” (LA, aCL, 2-GP-1) and clinical features (thrombosis, fetal loss)
• Pathogenesis due to aPL Ab binding to phospholipid associated proteins, especially 2-GP-1– Main antigenic target of aPL Abs– Clotting inhibitor required for binding of aCL with
cardiolipin
Autoantibodies and hepatitis C• Development of autoantibodies in setting of
hepatitis C is common - RF– APL Abs including aCL1, LA2 reported in up to
46% of those with hepatitis C
• APS in hepatitis C rare, incidence not increased in setting of hepatitis C1,2
– aPL Abs due to infection “cofactor independent”, nonthrombogenic
– No increased incidence of 2-GP-1 antibodies
1. Ordi-Ros et al, (2000) Clin and Diag Lab Immuno 7:241-2442. Amin, N (2008) Hematol Oncol Clin N Am 22:131-143
Antiphospholipid antibody syndrome and interferon
• Autoantibodies and immune phenomenon common during IFN therapy– Thyroid antibodies in 22%– Appearance or exacerbation of SLE, sarcoidosis1
• Our patient had mildly elevated 2-GP-1 antibodies prior to therapy (22 SGU, ref range 0-9) which rose markedly after IFN
• Also developed sarcoidosis in tattoo
1. Hauschild et al (2008) J Deutschem Dermatol ISSN: 1610-0387 (Online)

Conclusions
• Numerous autoimmune phenomena attributable to hepatitis C as well as immunomodulatory treatment
• Although development of APS is rare, consider screening for aPL Abs in patients with thrombosis in setting of hepatitis C or interferon treatment
Thank youDr John Olerud, Division head; Claudia Davis ARNP, and the Pacific Derm Association