
Antimicrobials in continuous renal replacement therapy ...
42
Antimicrobials in continuous renal replacement therapy (CRRT) Dr Catherine McKenzie PhD FFRPS FRPHARMS Consultant Pharmacist Guys‘and St. Thomas’ NHS Foundation Trust Senior Clinical Lecturer School of Medicine and Pharmacy Kings College London ESCMID 2015 Ferney-Voltaire ESCMID Online Lecture Library © by author
Transcript of Antimicrobials in continuous renal replacement therapy ...

Antimicrobials incontinuous renal replacement therapy (CRRT)
Dr Catherine McKenzie PhD FFRPS FRPHARMSConsultant PharmacistGuys‘and St. Thomas’ NHS Foundation TrustSenior Clinical Lecturer School of Medicine and PharmacyKings College London
ESCMID 2015 Ferney-Voltaire
ESCMID Online Lecture Library
© by author

Challenges
z PK alteration in critical illness superimposedz Different modes have different PK parametersz Much of older literature is out of datez Drug dosing probably requires individualised
approach
ESCMID Online Lecture Library
© by author

Original literature values
Filter UFR (L/hr)
DFR (L/hr)
Dose
Ceftazidime AN69 0.43m2
0.5 1, 2 1g 24hrly Davies 1991
Ciprofloxacin AN69 0.43m2
0.4 1, 2 200mg 12-8hrly
Davies 1992
Fluconazole AN69 0.43m2
- 1 200mg 24hrly
Nicolau 1994
ESCMID Online Lecture Library
© by author

Original literature…..what’s wrong with it
Assumed that RRT was equivalent to severe renal failure
• Rates were never higher than 20ml/minute
• Majority 10ml per minutes
• Does anyone ever run RRT at 10ml per minute
Took no account of critical illness
Little appreciation of resistant bacteria and variable MIC
Recommend once a day. What happens if one miss that dose
• E.g Once daily ceftriaxone in pneumococcal meningitis
ESCMID Online Lecture Library
© by author

Drug Factors
z Protein bindingz Volume of distributionz Method of total body clearance (Cl)z Metabolismz PharmacodynamicsESCMID Online Lectu
re Library
© by author

z Most medicines < 500 Dy MDZ 325 Da, LZP 320Da, Vecuronium 700Da,
Membrane cut - off: 20 -40,000 D
Does medicine size matter
ESCMID Online Lecture Library
© by author

Drug factors protein binding
z The higher the binding the more likely that the antimicrobial is NOT removed by CRRT
z Albumin, 1-acid glycoprotein, lipoproteinz Drug-protein = 50,000 D
z Changes in ICU patients• pH• Albumin (), AAG ()• bilirubin• other drugs
ESCMID Online Lecture Library
© by author

Protein bindingHigh (~90%)
y Ceftriaxone y Teicoplaniny Clindamycin y Amphotericin y Rifampicin
Low (<15%)
y Meropenemy Gentamicin y Fluconazoley Metronidazole y Acicloviry Fluconazolw
ESCMID Online Lecture Library
© by author
Drug factores Volume of distribution (Vd)
Any medicine has to be in the central compartment to be removed by CRRT
Thus small Vd, more likely to be effectively removed by CRRT
In theory !<1L/kg removed>2L/kg unlikely
ESCMID Online Lecture Library
© by author

Vd of antimicrobials commonly prescribed in critical care
z Aciclovir 0.6L/kgz Cefotaxime 0.3L/kgz Colistin 0.34L/kgz Piperacillin 0.18L/kgz Vancomycin 0.7L/kgz Linezolid 0.6L/kgz Gentamicin 0.25 l/kg
z Itraconazole 10L/kgz Moxifloxacin 2L/kgz Voriconazole 4.6L/kgz Tedizolid 1.0-1.1 L/kg
ESCMID Online Lecture Library
© by author

Clearance (Cl)
z Drugs that are largelyExcreted unchanged byGFRz Likely removed by
CRTTz There are exceptions-DigoxinESCMID Online Lectu
re Library
© by author

Total Clearance (ml/min)
= Cl renal + Cl non renal (+ Cl filter)
Cl renal > 25-30%
Pk of Clearance
ESCMID Online Lecture Library
© by author

Renal clearance
High
y Benzylpenicillin (85%)
y Cefuroxime (96%)
y Ceftazidime (84%)
y Gentamicin (95%)
Low (<25%)
y Erythromyciny Clindamyciny Amphotericiny Anidulafunginy Caspofunginy Posaconazole
ESCMID Online Lecture Library
© by author

Is CRRT clearance important?Vd (L/kg) % renal
Meropenem 0.25 70%Gentamicin 0.25 100%Fluconazole 0.7 75%Metronidazole 0.7 10%
Aciclovir 0.7 75%Ganciclovir 0.6 90%
Dose related neutropenia
ESCMID Online Lecture Library
© by author

Is CRRT clearance important?
Protein VdBinding (L/kg)
Benzylpenicillin 60% 0.3
Cefuroxime 33% 0.19
Ceftazidime 21% 0.23
Digoxin 25% 5-8
ESCMID Online Lecture Library
© by author

z Antimicrobials metabolised in liver y Tend to be, lipophilic- high protein biding, larger Vd,
reduced renal Clz Don’t forget ..pro drugs
y Pro drugs………oseltamivir to oseltamivir carbxylate. Active compound is renally excreted.
z Or active metabolites toxicityy Methylflucloxacillin, hepatotoxicity in renal failure
EMC, Kucers and Bennett
Drug Factors…. hepatic metabolism
ESCMID Online Lecture Library
© by author

S = Chf / Cpre-filter
x Haemofiltrationx Protein binding
(Golper 1991)
Absolute Value -Sieving coefficient
ESCMID Online Lecture Library
© by author

Important consideration in drug therapy (especially, antimicrobials)
Early therapy essential, amount often forgotten,
Vd= volume of distribution
Cp= plasma concentration
Loading dose is independent of renal function
A high initial dose may be preferred when treating infection in the intensive care
Vale et al Antibiotic therapy in severe sepsis: does the dose matter? Critical Care 2010)
ESCMID Online Lecture Library
© by author

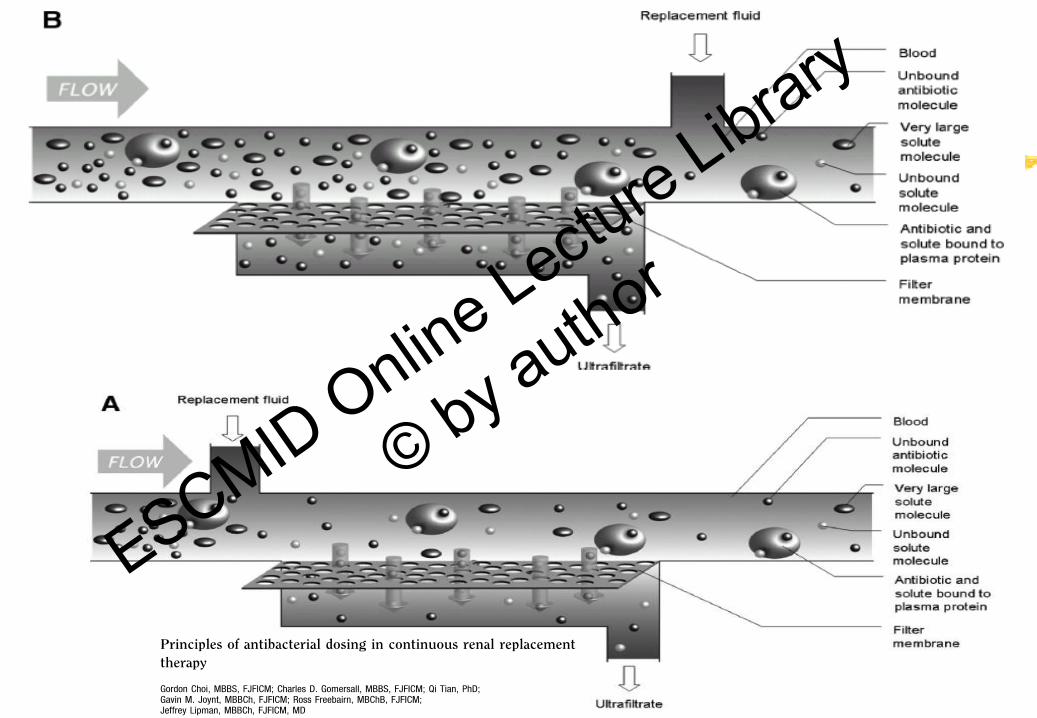
Classification of antibiotic according to their solubility and pharmacokinetic /pharmacodynamic properties
ESCMID Online Lecture Library
© by author

Aminoglycosides, fluoroquinolones, colistin High initial dose required for maximum effect gentamicin, larger peak
greater reduction in mortaility(CID 2000) Ciprofloxacin, Inhibitory ratio , pkarea/MIC
Larger, less frequent dosing can be associated with less adverse events
Aminoglycoside nephrotoxicity, uptake into renal cortex saturable, less dosing less uptake
Begg et al what is the evidence for once daily aminoglycoside
Clinical Pharmacokinetics 2001
ESCMID Online Lecture Library
© by author

Time dependence Beta lactams vancomycin
Achieve the target concentration quickly and maintain it Loading dose or large initial dose still important Optimal effect when time > MIC ?
Increased probability of success with T>MIC at 90 to 100 % of the dosing interval.
In ICU –possibility of lower initial Cp and higher desired MIC
• Roberts J et al Lancet 2015,
• McKenzie CA Antibiotic Dosing in Critical Illness
JAC 2011ESCMID Online Lecture Library
© by author

Aminoglycosides, fluoroquinolones, colistin High initial dose required for maximum effect
gentamicin, larger peak greater reduction
in mortaility(CID 2000) Ciprofloxacin, Inhibitory ratio , pkarea/MIC
Larger, less frequent dosing can also be associated with less adverse events
Aminoglycoside nephrotoxicity, uptake into renal cortex saturable, less dosing less uptake
Begg et al what is the evidence for once daily aminoglycoside Clinical Pharmacokinetics 2001McKenzie CA Antibiotics dosing in critical careJAC 2011
ESCMID Online Lecture Library
© by author

System factors
z Filter typez Haemofiltration ratez Dialysate ratez Membrane Interactions
ESCMID Online Lecture Library
© by author

Renal Replacement Therapy
• RRT = Life support treatment for renal failure• Includes dialysis, filtration and transplantation
• Terms:• PD – peritoneal dialysis (rarely used in ICU)• IHD – intermittent hemodialysis (rarely used in ICU outside USA)• SCUF – slow continuous ultrafiltration• CVVHD – continuous veno-venous hemodialysis• CVVHF – continuous veno-venous hemofiltration• CVVHDF – continuous veno-venous hemodiafiltration
• EDD(-f) – extended daily dialysis (diafiltration)• SLED
• IHD and PD standardised, everything else….
ESCMID Online Lecture Library
© by author

System factorsHaemofiltration rate
z 1 to 4litre per hour , often expressed in ml/kgz Convective transport
z Transmembrane pressurey Blood pump speedy Hydrostatic pressurey Oncotic pressureESCMID Online Lectu
re Library
© by author

System Factors CVVHD rate
z 1 - 4 L/hrz Dosed per ideal body weight (lean IBW)z Diffusive transport
z Blood : Dialysate = 150 : 17-34 ml/min z Maximise concentration gradient
y dialysate rateESCMID Online Lecture Library
© by author
ESCMID Online Lecture Library
© by author

Only UNBOUND drug is filtered
Ultrafiltrate
FLOW
FLOW
Semi-permeable Membrane
RRT: Protein Binding
+/- Dialysate
Bound
Drug
Unbound
Drug
Protein
ESCMID Online Lecture Library
© by author

Extended Dialysis
z In AKI or CKD if patient anuric, NO RENAL CLEARANCE
z Much considerations same as CKDz Give renally cleared drugsz E.g Vancomycin
y Aminoglycosidez Beginning of dialysisz Check serum level at completionObserved from clinical practice
ESCMID Online Lecture Library
© by author

Patient Factors Pragmatic
z CRRT stops, filter clotsz Patients escapes for procedurez Consider omitting dose if lasts greater than 4 hours z Daily review essential by Clinical Pharmacist
Barret NB et al IJPP 20111Shulman RS et al Journal of Critical Care 2015
ESCMID Online Lecture Library
© by author

Patient Factors Volume of distribution (Vd)
z Changes in critically ill patientsInfection !
Severe sepsisVd of many agents can increase as extracellular fluid
increasesx Increase in Vd in severe sepsis
z .y Serum albumin can dropy What happens to drug-albumin binding
Roberts et al Lancet Infect Dis. 2014 Jun; 14(6): 498–509
ESCMID Online Lecture Library
© by author

Patient factors
z Altered PK-Pd of drugs in critical illnessy Effects of heart failurey Effects of liver failure- presence of ascites
z Deep tissue infectionsz Immune system/presence of immunosuppresantsz Co-morbidities, COPD, CVA, tissue burnsAllen JA et al JAC 2014McKenzie CA et al Critical Care 2005ESCMID Online Lectu
re Library
© by author

Patient FactorSepsis changes PK and PD
Extracorporeal circuits (e.g. RRT)
Altered CL andIncreased Vd
? Plasma concentrations
If dosing does not account for these changes – sub-optimal levels!
Sub-optimal patient outcomes
ESCMID Online Lecture Library
© by author

SO Which dose for your patient
z Literature valuez Calculatez Best guessz Conduct study ?z Refer to guidelines (that are up to date)
ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

Literature Values
z Ceftazidime 1 to 2g iv 12 hourly CVVH/HD/HDFz Ciprofloxacin 200 to 400mg iv 12 hourly
y @GSTT 800mg iv 8 hourly in obese patientsz Fluconazole 400mg to 800mg iv/po 24 hourly
y Drug interactions (antipsychotics)
Some now out of date ? For higher MIC
Trotman and colleagues CID 2005;41:1159-66
ESCMID Online Lecture Library
© by author

Aciclovir –for HSV pneumonitis in CRRT
z Vd = 0.7l/kgz Renal eliminationz T half-lifez Neurotoxicity at high dosesz Dose in normal renal function is 10mg/kg 8hourlyz 10mg per kg (weight 50kg)
y Chest penetrationy ImmunocompromisedESCMID Online Lectu
re Library
© by author

Aciclovir…….
z Depends on rate of CRRTz 30ml per kg per hour= 30ml per minutez Mild renal impairmentz I would recommend 10ml per kg 8 hourlyz Serum levelsz Review dose daily
ESCMID Online Lecture Library
© by author

In CONCLUSION
ESCMID Online Lecture Library
© by author

Looking forward………..
Don’t forget the pathogen !
• Rapid diagnosis will help
Point of Care Testing for
antimicrobials
Citrate –longer life circuits
• PKPD studies needed
Ostermannand colleagues Nephron 2015
ESCMID Online Lecture Library
© by author


















