Antimalarials during pregnancy: cost-effectiveness analysis
8
Antimalarials during pregnancy: a cost-effectiveness analysis L.J. Schultz,1 R.W. Steketee,2 L. Chitsu10,3 & J.J. Wirima4 Antenatal clinics (ANC) provide an avenue for interventions that promote maternal and infant health. In areas hyperendemic for Plasmodium falciparum, malaria infection during pregnancy contributes to low birth weight (LBW), which is the greatest risk factor for neonatal mortality. Using current data and costs from studies in Malawi, a decision-analysis model was constructed to predict the number of LBW cases prevented by three antimalarial regimens, in an area with a high prevalence of chloroquine (CQ)-resist- ant malaria. Factors considered included local costs of antimalarials, number of ANC visits, compliance with dispensed antimalarials, prevalence of placental malaria, and LBW incidence. For a hypothetical cohort of 10 000 women in their first or second pregnancy, a regimen consisting of one dose of sulfadoxine-pyrimethamine (SP) in the second trimester followed by a second dose at the beginning of the third trimester would prevent 205 cases of LBW at a cost of US$ 9.66 per case of LBW prevented. A regimen using a treatment dose of SP followed by CQ 300 mg (base) weekly would prevent 59 cases of LBW at a cost of $62 per case prevented, compared with only 30 cases of LBW prevented at a cost of $113 per case when the regimen involves initial treatment with CQ (25 mg/kg) followed by CQ 300 mg (base) weekly. In areas hyperendemic for CQ-resistant P. falciparum, a two- dose SP regimen is a cost-effective intervention to reduce LBW incidence and it should be included as part of the antenatal care package. Introduction In rural sub-Saharan Africa, antenatal clinics provide one of the few opportunities for interventions to pro- mote maternal and infant health. A minimum set of services should be provided in the antenatal clinic (ANC), such as assessment and management of maternal or fetal risk factors; completion of relevant history on an antenatal card; immunization with teta- nus toxoid for neonatal tetanus prevention; adminis- tration or dispensing of iron and folate to combat anaemia; testing for syphilis and treatment; and rou- tine administration of antimalarials for prevention of malaria infection (1, 2). Antimalarials are important because, where Plasmodium falciparum transmission is high, women infected with malaria during preg- nancy may develop placental parasitaemia leading to I Epidemiologist, Division of Parasitic Diseases, Mailstop F-22, National Center for Infectious Diseases, Centers for Disease Control and Prevention (CDC), 1600 Clifton Road, Atlanta, GA 30333, USA. Requests for reprints should be sent to this author. 2 Medical Officer, Division of Parasitic Diseases, National Cen- ter for Infectious Diseases, CDC, Atlanta, GA, USA. 3 Officer-in-Charge, Community Health Sciences Unit, Ministry of Health, Lilongwe, Malawi. 4 Professor of Medicine, College of Medicine, University of Mal- awi, Blantyre, Malawi. Reprint No. 5588 decreased fetal nutrition and low-birth-weight (LBW) infants (3-6), and consequent risk of neo- natal and early infant deaths (7, 8). Prevention of ma- laria during pregnancy represents one of the few interventions that can be incorporated into the ante- natal care package to reduce the incidence of low- birth-weight infants and the risk of premature death. When resources are limited, women at greatest risk should be identified and interventions should be delivered selectively to this group. Women in their first pregnancy, and to a lesser extent their second, are more likely to become parasitaemic during the pregnancy (9-11), to have placental infection (3, 5), and to have low-birth-weight babies (8, 12) than women in later pregnancies. Therefore, women in their first or second pregnancies constitute the target group for antimalarial intervention. The factors which must be considered in identi- fying a practical antimalarial regimen for pregnant women in Africa include the efficacy, safety and ease of delivery of the antimalarial to the target pop- ulation, and their compliance with the dosage regi- men. Clearly, the regimen must be efficacious to pre- vent placental parasitaemia. Clinic attendance is essential for the delivery of antimalarials to pregnant women through antenatal clinics. The antimalarial regimen should be acceptable to the pregnant women and the dose schedule simplified to minimize the risk of poor compliance. Finally, the regimen must be Bulletin of the World Health Organization, 1995, 73 (2): 207-214 207
Transcript of Antimalarials during pregnancy: cost-effectiveness analysis

Antimalarials during pregnancy:a cost-effectiveness analysisL.J. Schultz,1 R.W. Steketee,2 L. Chitsu10,3 & J.J. Wirima4
Antenatal clinics (ANC) provide an avenue for interventions that promote maternal and infant health. Inareas hyperendemic for Plasmodium falciparum, malaria infection during pregnancy contributes to lowbirth weight (LBW), which is the greatest risk factor for neonatal mortality. Using current data and costsfrom studies in Malawi, a decision-analysis model was constructed to predict the number of LBW casesprevented by three antimalarial regimens, in an area with a high prevalence of chloroquine (CQ)-resist-ant malaria. Factors considered included local costs of antimalarials, number of ANC visits, compliancewith dispensed antimalarials, prevalence of placental malaria, and LBW incidence.
For a hypothetical cohort of 10 000 women in their first or second pregnancy, a regimen consistingof one dose of sulfadoxine-pyrimethamine (SP) in the second trimester followed by a second dose atthe beginning of the third trimester would prevent 205 cases of LBW at a cost of US$ 9.66 per case ofLBW prevented. A regimen using a treatment dose of SP followed by CQ 300 mg (base) weekly wouldprevent 59 cases of LBW at a cost of $62 per case prevented, compared with only 30 cases of LBWprevented at a cost of $113 per case when the regimen involves initial treatment with CQ (25 mg/kg)followed by CQ 300 mg (base) weekly. In areas hyperendemic for CQ-resistant P. falciparum, a two-dose SP regimen is a cost-effective intervention to reduce LBW incidence and it should be included aspart of the antenatal care package.
IntroductionIn rural sub-Saharan Africa, antenatal clinics provideone of the few opportunities for interventions to pro-mote maternal and infant health. A minimum set ofservices should be provided in the antenatal clinic(ANC), such as assessment and management ofmaternal or fetal risk factors; completion of relevanthistory on an antenatal card; immunization with teta-nus toxoid for neonatal tetanus prevention; adminis-tration or dispensing of iron and folate to combatanaemia; testing for syphilis and treatment; and rou-tine administration of antimalarials for prevention ofmalaria infection (1, 2). Antimalarials are importantbecause, where Plasmodium falciparum transmissionis high, women infected with malaria during preg-nancy may develop placental parasitaemia leading to
I Epidemiologist, Division of Parasitic Diseases, Mailstop F-22,National Center for Infectious Diseases, Centers for DiseaseControl and Prevention (CDC), 1600 Clifton Road, Atlanta, GA30333, USA. Requests for reprints should be sent to this author.2 Medical Officer, Division of Parasitic Diseases, National Cen-ter for Infectious Diseases, CDC, Atlanta, GA, USA.3 Officer-in-Charge, Community Health Sciences Unit, Ministryof Health, Lilongwe, Malawi.4 Professor of Medicine, College of Medicine, University of Mal-awi, Blantyre, Malawi.
Reprint No. 5588
decreased fetal nutrition and low-birth-weight(LBW) infants (3-6), and consequent risk of neo-natal and early infant deaths (7, 8). Prevention of ma-laria during pregnancy represents one of the fewinterventions that can be incorporated into the ante-natal care package to reduce the incidence of low-birth-weight infants and the risk of premature death.
When resources are limited, women at greatestrisk should be identified and interventions should bedelivered selectively to this group. Women in theirfirst pregnancy, and to a lesser extent their second,are more likely to become parasitaemic during thepregnancy (9-11), to have placental infection (3, 5),and to have low-birth-weight babies (8, 12) thanwomen in later pregnancies. Therefore, women intheir first or second pregnancies constitute the targetgroup for antimalarial intervention.
The factors which must be considered in identi-fying a practical antimalarial regimen for pregnantwomen in Africa include the efficacy, safety andease of delivery of the antimalarial to the target pop-ulation, and their compliance with the dosage regi-men. Clearly, the regimen must be efficacious to pre-vent placental parasitaemia. Clinic attendance isessential for the delivery of antimalarials to pregnantwomen through antenatal clinics. The antimalarialregimen should be acceptable to the pregnant womenand the dose schedule simplified to minimize the riskof poor compliance. Finally, the regimen must be
Bulletin of the World Health Organization, 1995, 73 (2): 207-214 207

L.J. Schultz et al.
affordable, whether paid for by the women them-selves or by the government (where ANC servicesare provided free).
In Malawi, ANC attendance is high and thenational malaria policy has recommended thatwomen be given weekly chloroquine (CQ) (300 mgbase) throughout pregnancy. Two major problemsexisted with this regimen. First, there are high levelsof CQ resistance throughout Malawi, and CQ hasbeen documented to be of little benefit in clearingplacental malaria in this setting (13). Second, aweekly CQ regimen relies on women rememberingand self-administering the drug at home each weekduring the pregnancy. For reasons varying fromminor side-effects to sociocultural beliefs, compli-ance with weekly CQ prophylaxis has been extreme-ly poor in many settings (14, 15). Less frequent dos-ing, particularly on-site administration at antenatalclinic visits with a more efficacious drug, would al-leviate compliance problems and increase theregimen's effectiveness. The cost factor must also beconsidered. In Malawi, the cost of antimalarialsdelivered through antenatal clinics is borne by thegovernment, which attempts to direct the limitedavailable resources to those interventions that willgive maximum benefit to the health of Malawians.
The National Malaria Control Committee inMalawi identified the control of malaria during preg-nancy as a health priority for which a practical inter-vention was required. To aid in the selection of anantimalarial intervention for use during pregnancy, astudy was conducted to examine the efficacy of regi-mens containing sulfadoxine-pyrimethamine (SP)and/or CQ (16). This paper examines the cost-effec-tiveness of these regimens when administered towomen in their first and second pregnancy.
MethodsAntimalarial regimens. Based on efficacy, availabili-ty, safety, cost, and dosage, three regimens wereselected as candidates for implementation throughthe national malaria control programme (16). Theseregimens were compared on the basis of the numberof LBW cases prevented and the cost per case ofLBW prevented (cost-effectiveness):(1) SP/SP-an initial single treatment dose of SP (3tablets, 1500 mg sulfadoxine and 75 mg pyrimetha-mine), given at the first antenatal clinic visit (typical-ly, 16th to 22nd week of gestation) and again at thebeginning of the third trimester.(2) SP/CQ-an initial treatment dose of SP at thefirst antenatal clinic visit, followed by CQ chemo-prophylaxis (300 mg base) weekly until delivery.
(3) CQ/CQ-an initial treatment dose of CQ(25 mg/kg, administered as a divided dose over 3days) at the first antenatal clinic visit, followed bychloroquine chemoprophylaxis (300 mg base) week-ly until delivery.
Description of the model. A decision-analysis modelwas constructed to estimate the number of low-birth-weight cases prevented by each of the regimens for ahypothetical cohort of 10 000 women in their first orsecond pregnancy. Critical decision nodes in themodel were the percentage of women attending theantenatal clinic, the expected compliance with week-ly CQ, the expected placental malaria infection rates,and the incidence of LBW deliveries. The 1992 costof antimalarials to the government of Malawi wasused to calculate the projected cost of each regimenper case of LBW prevented.
At the first visit, which was assumed to occur at20 weeks' gestation, women would be placed on oneof the antimalarial regimens (Fig. 1). Women onSP/SP would be given the first dose of SP, womenon SP/CQ would be given an initial treatment doseof SP and a 1-month supply of CQ prophylaxis toself-administer each week at home. Women onCQ/CQ would receive the initial treatment dose ofCQ and a 1-month supply of CQ prophylaxis.Women who return for a second clinic visit wouldthen receive the second dose of SP administered onsite, if the SP/SP regimen was being used. Forwomen on SP/CQ or CQ/CQ, CQ would be dis-pensed for weekly use at home until delivery.Because compliance can be a major limitation to theregimen's effectiveness, the model included expect-ed compliance for women receiving CQ weekly. Theprobability of placental malaria infection amongwomen on the candidate regimens was estimated andthe probability of women delivering a LBW newbornwas predicted based on the woman's malaria infec-tion status.
Probability estimates. Probability estimates used inthe model were derived from several recent studiesconducted in Malawi (Table 1). Results from anational survey showed that 93% of pregnant womenattend the antenatal clinic at least once and thatamong those who attend once, 94% return for one ormore subsequent visits (17). According to nationalpolicy at the time of the study, women who contin-ued attending the clinic were given CQ to be takenweekly at home until delivery. However, only 35%of these women complied with these recommenda-tions (18).
Hospital surveillance data indicate that amongwomen not attending the ANC and not receivingantimalarials during pregnancy, 38% would haveplacental malaria infection at delivery (19). In a
WHO Bulletin OMS. Vol 73 1995208

Cost-effectiveness of antimalarials during pregnancy
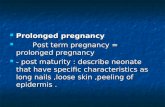
Fig. 1. Decision-analysis model to estimate, for each of three antimalarial regimens, the number of low-birth-weightcases expected for a hypothetical cohort of 10 000 women in their first or second pregnancy. Critical decision nodesinclude the number of women attending the antenatal clinic (ANC) for the first and second visits; expected compliance withweekly CO; placental malaria infection rates at delivery; and the incidence of LBW. Assumptions include: the first visitoccurs at 20 weeks' gestation and the second at 24 weeks, at which time the second dose of SP is administered.
I CQCCQ/CQ SP/CQ SP/SP
yes28%
2274 cases 2245 casesLBW LBW
(30 prevented) (59 prevented)
recent antimalarial efficacy study in which compli-ance was ensured by observed administration of allantimalarials, 9% of the women who received SP/SP,26% of the women who received SP/CQ, and 32% ofthe women who received CQ/CQ had placentalmalaria infection at delivery (16). Among womenscheduled to receive the SP/CQ regimen who were
2099 casesLBW
(205 prevented)WHO 94883
,ompliant with weekly CQ, the incidence of pla-I malaria infection was predicted to be less thanig women who received the full course ofQ. Therefore, we used an intermediate estimate;2% had placental malaria infection at delivery.Len who received one dose of SP but failed toi to the antenatal clinic were analogous to
Table 1: Probability estimates and data sources for specific variables used in the model for the cost-effectivenessof antimalarials used during pregnancy
Probabilityestimate Data source
First ANC visit 93% Malaria knowledge, attitudes, and practices survey, 1992 (17)Return rate for ANC attenders 94% Malaria knowledge, attitudes, and practices survey, 1992 (17)Compliance to CQ 35% Chloroquine compliance study, 1990 (18)Placental malaria infection rate:CO/Co 32% SP and CQ during pregnancy study, 1992 (16)SP/CQ 26% SP and CQ during pregnancy study, 1992 (16)SP/SP 9% SP and CQ during pregnancy study, 1992 (16)No antimalarials 38% Mangochi malaria project, 1987-1991 (19)LBW rate:With placental malaria 28% Mangochi malaria project, 1987-1991(19)No placental malaria 20% Mangochi malaria project, 1987-1991(19)
WHO Bulletin OMS. Vol 73 1995
I a
209

L.J. Schultz et al.
women returning to the clinic, but failing to complywith weekly CQ, so the incidence of placental malar-ia among those women was also estimated to be32%. Among women who received CQ/CQ, non-compliance or failure to attend the antenatal clinicwas estimated to increase the placental malaria infec-tion rate to 35%. Among women who receivedSP/SP but failed to return for the second dose, pla-cental malaria infection rates were estimated at 32%.Since SP/SP was administered on site, compliancewas not included as a determinant of the effective-ness for this regimen.
Data from a large cohort study (19) and ongoinghospital surveillance documented a LBW rate of28% among women in their first or second pregnan-cy who had placental malaria infection at delivery.Among women in their first or second pregnancywho did not have placental malaria infection, a LBWrate of 20% was observed.
Cost estimates. Antimalarial cost was based on thecost to the government in the spring of 1992; the costof a treatment dose was US$ 0.11 for SP and 7.5cents for CQ. The cost incurred at the first visit wasfor the initial treatment dose plus any antimalarialsthat would be dispensed. On the return visit, thecosts included antimalarials given on site for thetwo-dose SP group, or the cost of CQ dispensed foruse at home. The cost-effectiveness (cost per case ofLBW prevented) was then calculated for each regi-men. Finally, univariate and multivariate sensitivityanalysis was performed to test the robustness of thecost-effectiveness analysis.
ResultsEffectiveness and cost-effectiveness. Using thedecision analysis model, we estimated that 2304cases of LBW would occur per 10 000 women intheir first or second pregnancy if no antimalarialswere administered. For the SP/SP, SP/CQ andCQ/CQ regimens, the number of LBW cases expec-ted would be 2098, 2245 and 2274, respectively.Therefore, the number of cases of LBW prevented
by the SP/SP, SP/CQ and CQ/CQ regimens were205, 59 and 30, respectively. The total cost for thecohort of 10 000 women in their first or second preg-nancy was calculated at US$ 1984 for the SP/SPregimen, $3679 for the SP/CQ regimen, and $3353for the CQ/CQ regimen. The cost-effectiveness ofthe regimens (cost per case of LBW prevented) forSP/SP, SP/CQ and CQ/CQ was estimated to be$9.66, $59 and $113, respectively (Table 2).Sensitivity analysis. In the univariate analysis, thecritical variables affecting the regimen's effective-ness were ANC attendance and drug efficacy. Com-pliance was a limiting factor for regimens containingCQ but not for SP/SP. An example of how these fac-tors influence the number of cases of LBW prevent-ed by each of the regimens is shown in Table 3. IfANC attendance decreased to 50% for either the firstor the follow-up visit, or if compliance with weeklyCQ increased to 80%, the relative cost-effectivenessof the three regimens remained similar. The variablesmost affecting costs were the price of the antimalar-ials, the duration of CQ prophylaxis, drug efficacy,and compliance. However, regardless of changes ineach of these factors, the relative cost-effectiveness ofthe regimens did not change substantially (Table 4,see page 212).
Multivariate sensitivity analysis was performedto test further the robustness of the results. The rela-tive cost-effectiveness did not vary significantly withsimultaneous alteration of multiple variables. Thecost-effectiveness of the SP/SP regimen remainedconstant at $10 to $14 per case of LBW prevented,except when the price of SP was changed. With theCQ/CQ regimen, the cost per case of LBW prevent-ed decreased from $113 to $59 when compliancewas increased to 80% and the duration of CQ pro-phylaxis was shortened to 12 weeks. Under the samecircumstances, the cost of SP/SP was only $10 percase of LBW prevented. SP/SP remained most cost-effective, even when the cost of SP/SP was increasedthreefold and the efficacy was reduced such that18% of women receiving SP/SP had placental malar-ia at delivery (Table 4).
Table 2: Overall cost (US$) and the cost per low-birth-weight case prevented using threeantimalarial regimens administered to a hypothetical cohort of 10 000 women in their first orsecond pregnancy
Cost of Cost of No. of CosVfirst visits return visits Total LBW cases LBW case
Regimena (93%) (94%) cost prevented prevented
SP/SP $1023 $962 $1985 205 $9.66SP/CQ $1581 $2098 $3679 59 $62.01CQ/CQ $1256 $2098 $3354 30 $113.05a SP (sulfadoxine-pyrimethamine) cost: $0.1 1/treatment dose (3 tabs). CQ (chloroquine) cost: $0.075/treat-ment dose (25 mg/kg); $0.015/week prophylaxis dose (300 mg base).
WHO Bulletin OMS. Vol 73 1995210

Cost-effectiveness of antimalarials during pregnancy
Table 3: Univariate sensitivity analysis: number of LBW cases prevented for a hypotheticalcohort of 10 000 women in their first or second pregnancy who followed one of three anti-malarial regimensa
No. of LBW cases prevented with:
Placental ImprovedFirst visit Return visit Compliance infection rate: CQ/CQ efficacy:decreased decreased increased SP/SP 18% placental infection
Regimen to 50% to 50% to 80% SP/CQ 29% rate 20%
SP/SP 110 130 205 144 211SP/CQ 32 52 78 67 146CQ/CQ 16 26 39 30 89a Results illustrated in this Table were calculated using the figures for the original model and varying onlythe factor as shown in the column heading. Factors used in the original model were: first visit, 93%; returnvisit, 94%; compliance, 35%; CQ prophylaxis duration, 20 weeks; CQ/CQ placental infection rate, 32%.
The model was applied to settings where therates of placental malaria infection or LBW were dif-ferent from those in rural Malawi. Table 5 illustratesthe cost-effectiveness of the regimens in a settingwhere placental malaria infection rate in untreatedwomen was 25%, and LBW incidence was 20%among women with infected placentas and 15%among women with uninfected placentas. The costper case prevented increased substantially, but SP/SPremained more cost-effective (Table 5). Again, thisrelative cost-effectiveness remained unchanged inboth univariate and multivariate sensitivity analysis.
DiscussionWhen identifying interventions to prevent malariaduring pregnancy, the efficacy of the antimalarial isnecessary but not sufficient by itself for success. Weconstructed a decision-analysis model that incorpora-ted socio-behavioural and biological factors to assessthe relative effectiveness of antimalarial regimens foruse in a national malaria prevention programme inpregnant women. The model identifies drug efficacy,
compliance, and antenatal clinic attendance as majorfactors limiting the regimen's effectiveness. Thecost-effectiveness was most influenced by the drug'sefficacy and cost, the total number of weeks CQ wasadministered, and, to a lesser extent, compliance. Byutilizing a regimen that allows single-dose intermit-tent treatment with a highly efficacious antimalarial,administered on-site in an antenatal clinic, only theclinic attendance remains a potential limiting factorto the regimen's effectiveness.
The costs presented in this analysis aredescribed from the perspective of the Ministry ofHealth, which provides free antenatal services atgovemment health facilities. Programme costs,including fixed costs, were not included in the modelon the assumption that delivery of antimalarialswould be incorporated as one part of the package ofservices delivered to women attending the antenatalclinic. Furthermore, the costs of administering any ofthe three regimens through this system should besimilar and would not alter the relative cost-effectiveness of the regimens. In Malawi, the costof SP/SP would be significantly higher if purchasedby women outside the health care system. Many
Table 5: Multivariate sensitivity analysis: cost (in US$) per LBW case prevented for a hypo-thetical cohort of 10 000 women in their first or second pregnancy who followed one ofthree antimalarial regimens in a setting with lower Incidence of placental malaria and lowbirth weighta
Original model Placental infection:variables for visits, Return visit, Compliance, SP cost, SP/SP 13%
Regimen compliance, and cost 50% 80% $0.33/dose SP/CQ 18%
SP/SP $258 $29 $28 $83 $36SP/CQ $99 $77 $85 $154 $113CQ/CQ $241 $202 $169 $241 $241a Placental parasitaemia rates: untreated, 25%; SP/SP, 9%; SP/CQ, 15%; CQ/CQ, 20%. Low birth weightincidence: 20% with placental infection, 15% with no placental infection. Results illustrated in this Tablewere calculated using the figures for the original model and varying only the factor(s) shown in the columnheading. Factors used in the original model were: first visit, 93%; return visit, 94%; compliance, 35%; SPcost, $0.1 1/treatment dose; CQ prophylaxis duration, 20 weeks.
WHO Bulletin OMS. Vol 73 1995 211

L.J. Schultz et al.
o = .& potential costs were not addressed, including thoseCo
0). °associated with adverse drug reactions or delivery
a 31. 'ao t.- of a LBW infant (e.g., prolonged hospitalization andX s5'9 ° 6§ 6 §E -o
follow-up clinic visits), or with the value of yearsL LO CD ea,)of life lost for LBW infants who die.
B.i , O0 An important consideration with any drug to beX 'a: 80 n _ used during pregnancy is its safety for both the fetus
u) cn- X LCZ 11 and the mother. The major concem with SP during
CZ r CO .o S pregnancy is a theoretical increase in the risk of ker-o bt 5 ° Sg °o n nicterus in the newbom due to competition between
.- bilirubin and sulfadoxine for binding sites on albu-_O C6 3 E offl min. Although an increase in kemicterus was report-
s0° a) LO CO ed in one early study in which sulfonamides were_~ ~<co 6-d A 64 °) administered to newboms (20), subsequent studies._-n D_ 61)* C have not found any increased risk of kemicterus after
E 8 > 3 gadministration of a sulfonamide to the pregnanto E 8 woman (21-23). Therefore, the risk of serious mater-o 0. g2C > CO e co nal or fetal side-effects after a two-dose regimeno ~~~~~~~~cnEo-m=^ o e e o a) administered during the second trimester and early in0c 6-- Xo the third trimester was thought to be insignificantoO
oB S < = (s cfwhen compared with the increased risk of neonatalIt LO Co E ao mortality due to malaria-associated LBW.o °
D 80 oN Further analysis comparing the relative cost ofo < n <w-< O 0 antimalarials delivered through antenatal clinics withX a) a° >3 that of other health interventions (nutritional supple-
co. C mentation, focusing on reduction of low birth weighto- o O B:or neonatal mortality) is required to ascertain the rel-
0. c\( 0 ative economic efficiency of interventions. Within>L) 5 C Co the context of antimalarial interventions, this analy-
O E -o O §o 6c E " sis demonstrates that CQ/CQ, at present used in_Cl) _ O .sc° it many countries with CQ-resistant P. falciparum, isc 0C-.O)-Q neither an effective nor inexpensive intervention to
-0t0 C-O o prevent LBW. A regimen consisting of two-dose SPX=.oa,_cq w X -'o was less costly and prevented significantly more
ffc o cases of LBW, resulting in a relative cost-effective-co En'CXcL UOO ness that remained unchanged even when critical
0a))a) m<,, factors were varied. These results provide furtherm o0) - C argument for replacing the widely recommended
> OYcnCM -co cm(Cp CQ/CQ regimen with a more efficacious antimalarialQ c0.()6 6 E *fi o which can be delivered intermittently under con-
"D en o X n gtrolled circumstances (e.g., in an antenatal clinic) to
: E cQ n O N 5 t reduce malaria-associated LBW. Currently, the Mal-. 5 CZ C 0 awi Ministry of Health has changed the national pol-
E o > icy for malaria control to recommend SP/SP adminis-o )° 3a,,tration to pregnant women and this recommendation
co is widely implemented through govemment antenatal#> CZ 0cmo E COC care programmes.
a)LO LO C
U)(
tg -<- ' Acknowledgementsco'~~~~~oO
. X The authors are grateful to Deborah McFarland for re-
C3 cn (m a)' viewing the model construction and cost analysis andX.O m{L X j u) Gc Laurence Slutsker for reviewing the manuscript.
212WHO Buletin OMD.vol 73 199
212 WHO Bulletin OMS. Vol 73 1995

Cost-effectiveness of antimalarials during pregnancy
ResumeAntipaludiques pendant la grossesse:analyse cout/efficacit6En Afrique subsaharienne rurale, les dispensairesantenatals offrent l'une des rares occasionsd'intervention en faveur de la sante maternelle etinfantile. Le traitement par des antipaludiques doitfigurer parmi les interventions, car I ou la trans-mission de Plasmodium falciparum est intense,l'infection de la mere au cours de la grossessepeut entrainer une parasit6mie placentaire, asso-ciee a un faible poids de naissance chez l'enfantet a un risque de d6ces neonatal ou au cours dela premibre enfance. De plus, la prevention du palu-disme par administration d'antipaludiques repr6-sente l'une des rares interventions qui puisse etreintegree dans les soins antenatals et qui soitcapable de reduire efficacement l'incidence dufaible poids a la naissance.
Cet article examine le rapport co0tGefficacitede trois sch6mas de traitement antipaludiquecontenant de la sulfadoxine-pyrim6thamine (SP)et/ou de la chloroquine (CQ), administres lors dela premibre et de la deuxieme grossesses. Lesschemas retenus ont ete s6lectionnes par le pro-gramme national de lutte contre le paludisme auMalawi d'apres les resultats d'evaluations portantsur l'efficacite, la disponibilite, l'innocuite, le coOtet la facilit6 d'administration des medicaments.
1) SP/SP - une dose unique initiale de SP(3 comprim6s, soit 1500 mg de sulfadoxine et75 mg de pyrim6thamine) lors de la premibre visi-te au dispensaire ant6natal (habituellement entrela seizieme et la vingt-deuxieme semaine de lagrossesse), et de nouveau au d6but du troisiemetrimestre.
2) SP/CQ - une dose initiale de SP lors dela premibre visite au dispensaire ant6natal, puisune chimioprophylaxie par CQ (300 mg de chloro-quine base), une fois par semaine jusqu'a I'accou-chement.
3) CQ/CQ - une dose initiale de CQ(25 mg/kg, r6partie sur 3 jours) lors de la premierevisite au dispensaire ant6natal, puis une chimio-prophylaxie par CQ (300 mg de chloroquine base)une fois par semaine jusqu'a l'accouchement.
D'aprbs les donn6es et coOts r6sultant d'etu-des realisees au Malawi, un modble d'analysedecisionnelle a 6t6 6tabli pour pr6dire le nombrede cas de faible poids a la naissance qui peuventetre evites grace aux trois types de traitementantipaludique, et le rapport cout/efficacite relatif deces derniers dans une region a forte pr6valence
de paludisme chloroquinoresistant. Les d6termi-nants de l'efficacite 6taient la frequence desvisites au dispensaire antenatal, l'observance dutraitement antipaludique, la prevalence du paludis-me placentaire, et l'incidence du faible poids a lanaissance. Dans une cohorte hypothetique de10 000 femmes pendant leur premiere ou leurdeuxieme grossesse, recevant chacun des sch6-mas etudies, il serait ainsi possible d'eviter 205cas de faible poids a la naissance avec le sch6maSP/SP, 59 cas avec le sch6ma SP/CQ et 30 casavec le schema CQ/CQ. Le coOt total pour cettecohorte a e 6valu6 a US$ 1984 pour le schemaSP/SP, US$ 3679 pour le sch6ma SP/CQ, et US$3353 pour le sch6ma CQ/CQ. Le rapport coOt/effi-cacit6 des sch6mas (coOt par cas de faible poidsa la naissance 6vite) pour les schemas SP/SP,SP/CQ et CQ/CQ a 6te evalu6, respectivement, aUS$ 9,66, US$ 59 et US$ 113.
Ces r6sultats d6montrent a nouveau l'int6retdu remplacement du schema CQ/CQ, actuelle-ment largement recommande, par un antipalu-dique plus efficace, qui puisse etre administrep6riodiquement sous surveillance (par exempledans un dispensaire antenatal) pour reduire l'inci-dence du faible poids a la naissance associe aupaludisme. Is montrent que le schema SP/SP estune intervention rentable pour r6duire l'incidencedu faible poids a la naissance dans les r6gions ouP. falciparum chloroquinoresistant est hyperend6-mique, et qu'elle doit figurer dans le programmede soins ant6natals. Le Ministere de la Sante duMalawi a modifie la politique nationale de lutteantipaludique et recommande maintenant I'admi-nistration de SP/SP aux femmes enceintes.
References1. Rooney C. Antenatal care and maternal health: how
effective is it? A review of the evidence. Geneva,World Health Organization, 1992: 10-37.
2. Stanfield JP, Galazka A. Neonatal tetanus in theworld today. Bulletin of the World Health Organiza-tion, 1984, 62: 647-669.
3. Jelliffe EFP. Low birth weight and malaria infectionof the placenta. Bulletin of the World Health Organ-ization, 1968, 38: 69-78.
4. MacGregor JD, Avery JG. Malaria transmissionand fetal growth. British medical journal, 1974, 3:433-436.
5. McGregor IA et al. Malaria infection of the placentain the Gambia, West Africa; its incidence and rela-tionship to stillbirth, birthweight, and placentalweight. Transactions of the Royal Society for Tropi-cal Medicine and Hygiene, 1983, 77: 232-244.
6. Brabin BJ. An analysis of malaria in pregnancy inAfrica. Bulletin of the World Health Organization,1983, 61: 1005-1016.
WHO Bulletin OMS. Vol 73 1995 213

L.J. Schultz et al.
7. McCormick MC. Contribution of low birth weight toinfant mortality and childhood morbidity. New Eng-land journal of medicine, 1985, 312: 82-90.
8. World Health Organization, Division of FamilyHealth. The incidence of low birth weight: a criticalreview of available information. World health statis-tics quarterly, 1980, 33: 197-224.
9. McGregor IA. Epidemiology, malaria and pregnan-cy. American journal of tropical medicine andhygiene, 1984, 33: 517-525.
10. Keuter M et al. Comparison of chloroquine, pyri-methamine and sulfadoxine, and chlorproguanil anddapsone as treatment for falciparum malaria inpregnant and non-pregnant women, Kakamega dis-trict, Kenya. British medical journal, 1990, 301:466-470.
11. Steketee RW et al. Malaria infection in pregnantwomen in Zaire: the effects and the potential forintervention. Annals of tropical medicine and parasi-tology, 1988, 82: 113-120.
12. Kramer MS. Intrauterine growth and gestationalduration determinants. Pediatrics, 1987, 80: 502-511.
13. McDermott JM et al. Efficacy of chemoprophylaxisin preventing Plasmodium falciparum parasitaemiaand placental infection in pregnant women in Mala-wi. Transactions of the Royal Society for TropicalMedicine and Hygiene, 1983, 77: 232-244.
14. MacCormak CP, Lwihula G. Failure to participatein a malaria chemosuppression programme: NorthMara, Tanzania. Journal of tropical medicine andhygiene, 1983, 86: 99-107.
15. Helitzer-Allen DL. Examination of the factors influ-encing utilization of the antenatal malaria chemo-prophylaxis program, Malawi, Central Africa. Balti-more, MD, Johns Hopkins University Press, 1989:86-96.
16. Schultz LJ et al. The efficacy of antimalarial regi-mens containing sulfadoxine-pyrimethamine and/orchloroquine in preventing peripheral and placental
Plasmodium falciparum infection during pregnancy.American journal of tropical medicine and hygiene,1994, 51: 515-522.
17. Schultz LJ et al. Malaria knowledge, attitudes, andpractices among childbearing women in Malawi.Tropical medicine and parasitology, 1994, 45 (suppl.1): 65-69.
18. Heymann DL et al. Antenatal chloroquine chemo-prophylaxis in Malawi: chloroquine resistance, com-pliance, protective efficacy and cost. Transactions ofthe Royal Society for Tropical Medicine andHygiene, 1990, 84: 496-498.
19. Steketee RW et al. Malaria prevention in pregnan-cy. The effects of treatment and chemoprophylaxison placental malaria infection, low birth weight, andfetal, infant, and child survival (African Child Survi-val Initiative - Combatting Childhood Communi-cable Diseases Project Document 099-4048). Atlan-ta, GA, Centers for Disease Control and Prevention,1993.
20. Silverman WA et al. A difference in mortality rateand incidence of kernicterus among prematureinfants allotted to two prophylactic antibacterial regi-mens. Pediatrics, 1956, 18: 614-625.
21. Baskin CG et al. Sulfadiazine and rheumatic feverprophylaxis during pregnancy: does it increase therisk of kernicterus in the newborn? Cardiology,1980, 65: 222-225.
22. Kantor Hi et al. Effect on bilirubin metabolism inthe newborn of sulfisoxazole administered to themother. Obstetrics and gynecology, 1962, 17:494-500.
23. Barbosa JC, Ferreira I. Sulfadoxine-pyrimethamine(Fansidar) in pregnant women with Toxoplasmaantibody titers. In: Siegenthaler W, Luthy R, eds.Current chemotherapy: Proceedings of the 10thInternational Congress of Chemotherapy. Vol. 1.Washington DC, American Society for Microbiology,1978: 134-135.
214 WHO Bulletin OMS. Vol 73 1995