BioVLAB-Microarray: Microarray Data Analysis in Virtual Environment

Early Cancer Detection
Dr O H [email protected]
01.07.2016 Nottingham Pathology 2016 1
CEAC: Centre of Excellence for Autoimmunity in Cancer

01.07.2016Nottingham Pathology 2016
2

• Within a 30 year period (2000 – 2030), cancer is predicted to double in incidence worldwide, with a concurrent doubling in number of deaths/year.
01.07.2016 Nottingham Pathology 2016 3
• For many types of cancer the outlook has changed little in the last 30 years.– Lung cancer – <10% have surgery in UK and 5%-10% alive at 5 years– Pancreatic cancer – 1% alive at 5 year
• Most people are diagnosed only when there is a late ‘presentation’ of the cancer; impaired survival, major forms of therapy, major operation, chemotherapy and radiotherapy.

Early detection and treatment has been shown to significantly reduce mortality:
Randomised trials (‘Level 1’ evidence)• Breast Cancer - Mammography (50-74yrs)
– 23% reduction in deaths from breast cancer– [NB: only ~1/3rd of BCs occur between 50-74]
• Lung Cancer – CT scans (55-74yrs, >30 pys)– 20% reduction in deaths from lung cancer– [NB: Only ~1/3rd LCs occur in NLST trial]
• Colon Cancer – faecal occult blood test + colonoscopy (>50yrs)– 16% reduction in deaths from colon cancer– [NB: Only ~1/3rd individuals accept colon screening]
01.07.2016 Nottingham Pathology 2016 4

Our solution is to provide a blood test that will:• Improve public acceptability.• Provide improved sensitivity & specificity compared to other screening
methods.• This will significantly improve clinical outcomes (improved survival
rates) and cost-effectiveness.
01.07.2016 Nottingham Pathology 2016 5

01.07.2016 Nottingham Pathology 2016 6

01.07.2016 Nottingham Pathology 2016 7
q The immune system, which protects us from microbes, also mounts a response to very small amounts of aberrant protein overproduced and released by cancer cells within a tumour.
q This response includes the generation of autoantibodies (AAbs) to these tumour-associated molecules/antigens (TAAs).
q Autoantibodies directed against TAAs were shown to be relevant tumour biomarkers and can be detected up to 5 years before the tumour is overt clinically.
Immune response to cancer cells

01.07.2016 Nottingham Pathology 2016 8
1- Lung Cancer.
2- Colorectal Carcinoma.
3- Breast Cancer.

01.07.2016 Nottingham Pathology 2016 9

01.07.2016 Nottingham Pathology 2016 10
q Prof Robertson and his team in collaboration with oncimmune have already developed a blood test which has moved from the 'bench to the bedside' enabling the early detection of lung cancer. This test is called Early CDT-Lung.
q The test is currently in clinical use and has already shown that within high risk populations that cancers can be detected early whilst they are still treatable with the potential for increased patient survival and indeed in some cases cure.
Stage 1A Lung Cancer – curable!

2010
2011
2014
2012
Auditoftheautoantibodytest,EarlyCDT®-Lung,in1600patients:Anevaluationofitsperformanceinroutineclinicalpractice _
JamesJett,LauraPeek,LynnFredericks,WilliamJewell,WilliamPingleton,JohnF.R.RobertsonLungCancer2014;83:51–55
01.07.2016
Nottingham Pathology 2016 11

Early Cancer Detection Test –Lung Cancer Scotland
01.07.2016
Nottingham Pathology 2016 12

01.07.2016 Nottingham Pathology 2016 13

Background• Colorectal cancer (CRC) is the 2nd highest cause of cancer mortality in the
Western world.
• Key to better survival is early diagnosis (>90% survival if detected early).
• Current early diagnostic methods (ie Faecal sampling) have low takeup(57%:Uk, 34% EU). Alternative investigations are invasive (iesigmoidoscopy, colonoscopy) and have equally poor patient acceptability.
01.07.2016 Nottingham Pathology 2016 14

01.07.2016 Nottingham Pathology 2016
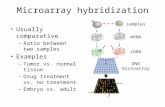
Antigen-based protein microarrays:q TAAs are arrayed (spotted) as a regular
pattern (a microarray) onto an activated surface. A single array can have multiple TAAs, each at separate location.
q A 5x5mm array can accommodate up to 150+ individual features.
q Immobilized TAAs are exposed to a patient serum sample.
q Autoantibodies binding to any of the TAAs can be detected fluorescently and measured

Antigen-based protein microarrays
Advantages including:
• High throughput, much increased capacity for multiplexing detection of a range of specific AABs.
• Reduced requirements for TAAs, serum and reagents;
• Increased assay robustness; better sensitivity and specificity than that achievable by ELISA-based assays.
01.07.2016 Nottingham Pathology 2016 16

Serum samples: sera from 3 different cohorts; 200 sera from Pittsburgh,USA (100 CRC and 100 controls), 42 sera (21 CRC and 21 matched controls)from New York, USA, and 20 sera from Dundee, UK (10 CRC and 10 controls)were tested.A panel of multiple tumour-associated antigens (TAAs) using anoptimised multiplex microarray system. Tumour-associated antigen selection:a panel of 32 TAAs (non-glycosylated recombinant proteins expressed inE.coli) were included: P53, SOX2, NY-ESO-1, GBU, MAGE A4, HuD, AFP,Gankyrin, GRP78, HCC1, HDGF, H-Ras1, IMP, p62, RalA, MUC1, CEA, AnnexinA1, rhUteroglobulin (CCSP1), K-Ras, APC1, APC2 blocking peptide, SDCCAG8(NY-CO-8), TDRD6 (NY-CO-45), vWFA2 (CCSP2), ErbB2, RAF1, SCGB1A1,CA19-9, UTP14A (NY-CO-16), K-RAS-Q61H and APC-N.
Pilot study
01.07.2016 Nottingham Pathology 2016 17

01.07.2016 Nottingham Pathology 2016 18

1- Quality assessment of the antigens
Antigen Quality
A representative analysis of a selection of TAAs by Western blot (WB) and Silver stain.
A)Printing New Antigens
Evaluation of the optimal concentration to print the new antigens
ERBB2
100 ug
50 ug
25 ug
B)
01.07.2016Nottingham Pathology 2016 19

2- Internal QC measures on Microarray
Serial dilution of purified human IgG to verify function of the detection system and provide a standard curve of human IgG against which AAb responses could be calibrated.
Nottingham Pathology 2016

3- Cohort results associated with TAA responses:
Nottingham Pathology 2016 21

4- Sensitivity and Specificity of the assay.Antigen/Panel Sensitivity (%) Specificity
(%)AFP 27 95
P53 26 95
K Ras 27 96
NY-CO-16 41 95
RAF1 18 95
Annexin 29 94
A panel of the 6 TAAs
61.1% 80.9%
Sensitivity and specificity of individual TAAs and panels of TAAs were calculated to establish the best combinations of this test set of TAAs that would provide good discrimination between cancer-positive
and normal serum samples.
Results

5- Sensitivity of CRC sample set by stage (A) and site (B).
The sensitivity is not a stage dependent. The data also show no difference in AAb detection by CRC location (76% sensitivity for left side CRCs and 72% for right side CRCs).

01.07.2016Nottingham Pathology 2016 24
Human blood autoantibodies in the detection of colorectal cancer
OlaHNegm,MohamedRHamed,RobertESchoen,RichardLWhelan,RobertJSteele,JohnScholefield,ElizabethMDilnot,ShanthaKumara,JohnFRRobertson,HerbertFSewell.
PLOS one- June 2016

01.07.2016 Nottingham Pathology 2016 25

01.07.2016 Nottingham Pathology 2016 26
Pilot Study for Early Detection of breast cancer
q The preliminary data confirmed that BC also induces autoantibodies (AAbs) againstthe small number of specific tumour associated antigens (TAAs) used in this pilotstudy.
q These pilot results showed positive autoantibody signal was detectable across all ageranges (ie <50yrs, 50-70 years and >70 years) and that the positive tests were asfrequent in early stage cancer (stages 1 & 2) as in late stage disease. The resultsshowed that 90% of positive samples for the autoantibody test were hormonereceptor positive (HR +ve).
q Initial proof of principle studies have been run to confirm our hypothesis.
q Breast cancer serum samples included 300 invasive BC, (approx. 50% being stage 1/2) and 300 age and gender matched controls.

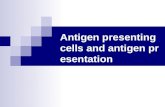
Plots of reactivity to four individual TAAs: BRCA1 (A), EPCAM (B), MUC1 (C) and MAGE A4 (D) probed with breast cancer (BC)and normal control (Con) sera. Each graph shows side-by-side comparisons of AAb responses to the TAA antigens for clinicallyconfirmed BC (white circles) and control (grey circles).
Reactivity of selected TAAs to sera from breast cancer patients and normal controls

Proven preventative treatments:potential to prevent ~35% of all breast cancer cases
01.07.2016 Nottingham Pathology 2016 28
70% of all breast cancers
are stimulated to grow by estrogen
50% Prevented by drugs
like tamoxifen
~35% of cases could be
prevented
X =
Blood test to identify at early stage

What will be achievedEarly detection of all types of solid cancers will mean:• More people have a greater chance of survival • Improved survival rates and life expectancy• Less aggressive treatments• Less money spent on treatment.• Worldwide impact– applicable to low & medium income countries too
Within 5 years• Can get 3 common cancers (eg breast, colon & primary liver cancer),
through to market and available for clinical use in the UK. • Tests for other cancers would be at various stages of development.
01.07.2016 Nottingham Pathology 2016 29

Acknowledgment
Prof John Robertson Prof Herb Sewell
30