Antidepressant. Management of psychological disorders Medical treatment Psychotherapy Support...
41
Antidepressant
-
Upload
james-golden -
Category
Documents
-
view
223 -
download
0
Transcript of Antidepressant. Management of psychological disorders Medical treatment Psychotherapy Support...
Antidepressant
Management of psychological disorders
• Medical treatment
• Psychotherapy
• Support groups

Depression
• Point prevalence – 5-6 %
• Life time prevalence – 10 %
• Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)



Amine hypothesis of mood
Major depressive disorders results from functional deficiencies of norepinephrine or serotonin
• Most antidepressant drugs enhance the action of NE and serotonin (5-HT)
Drawbacks of amine hypothesis
• Postmortem studies do not reveal any decrease in NE or 5-HT
• Actions within hours effects within weeks
• Bupropion has minimal effects on NE or 5-HT







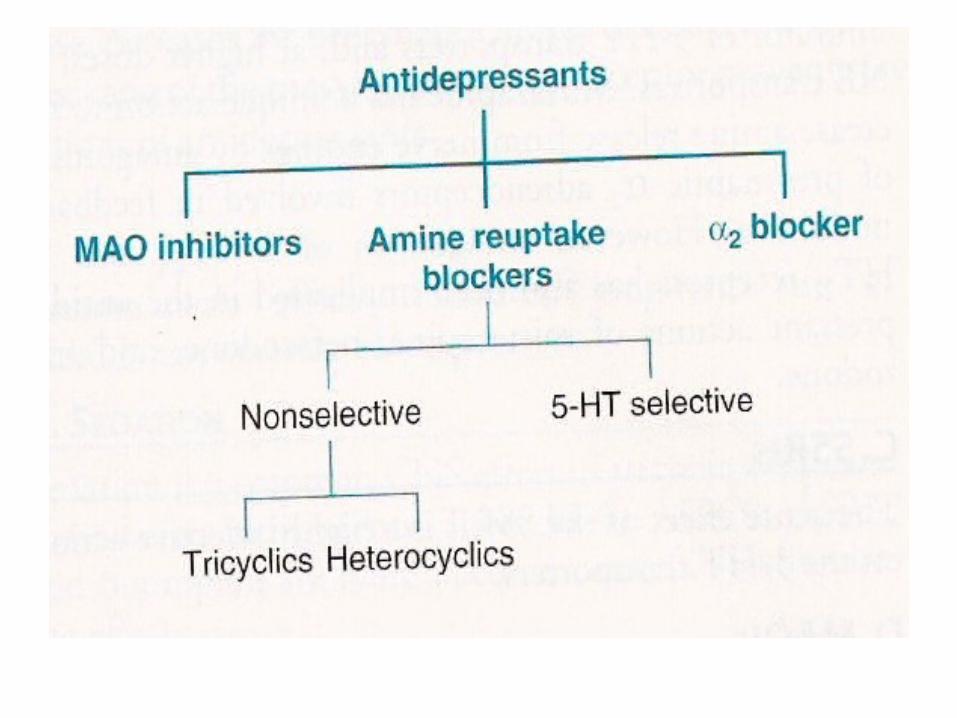


Antidepressants
• Little difference in efficacy
Choice depends on– Presence of concomitant disease– Existent therapy – Suicidal risk– Response to previous therapy

Depression
• Major depressive episodes (endogenous)
• Tricyclic and SSRIs
• Popularity due to well tolerance
• For severe inpatient – Tricyclic antidepressant
• Electroconvulsion therapy (ECT)







Hyponatraemia and antidepressant therapy
• Hyponatraemia (usually in the elderly and possibly due to inappropriate secretion of antidiuretic hormone) has been associated with all types of antidepressants
• However, it has been reported more frequently with SSRIs than with other antidepressants.
The CSM has advised that hyponatraemia should be considered in all patients who develop
– drowsiness, confusion, or convulsions while taking an antidepressant.
Suicidal behaviour and antidepressant therapy
• The use of antidepressants has been linked with suicidal thoughts and behaviour
• children, young adults, and patients with a history of suicidal behaviour are particularly at risk.
• Where necessary patients should be monitored for suicidal behaviour, self-harm, or hostility,
• Particularly at the beginning of treatment or if the dose is changed.
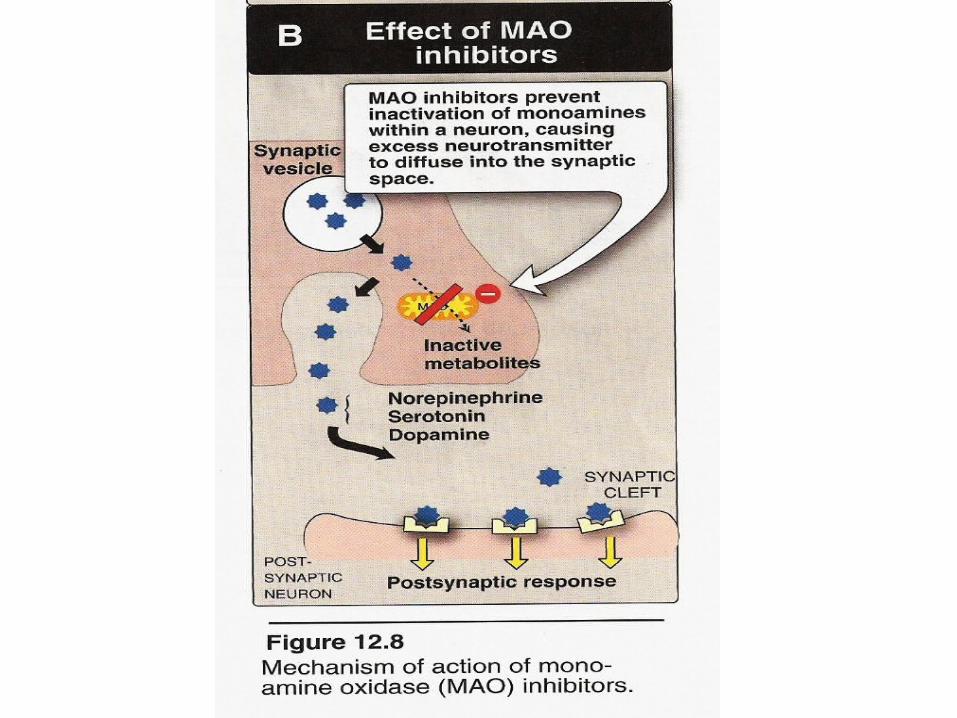
MAO inhibitors
• Drug interactions
• MAO and tyramine
• Cheese, chicken liver, beer and red wine – Headache – Tachycardia– Nausea – Arrythmia

St John's wort
• Hypericum perforatum
• Unlicensed indication
• Mild depression
• Active ingredient
• Drug interaction
Depression
• Major depressive episodes (endogenous)
• Tricyclic and SSRIs
• Popularity due to well tolerance
• For severe inpatient – Tricyclic antidepressant
• Electroconvulsion therapy (ECT)

Depression
• MAO inhibitors and atypical depression– Labile mood, rejection sensetivity, appetite
disorders
• 4-6 weeks before change treatment
• Drug washout

Panic disorders and phobias
• Antidepressant are generally used
• Imipramine and MAOIs
• SSRIs
• Benzodiazepines

Obsessive-compulsive disorders
• SSRIs are especially effective– Fluoxetine – Fluvaxamine
• Clomipramine – SNRIs

Enuresis
• Tricyclic antidepressant
• Imipramine
• Not preferred approach
Chronic pain
• Tricyclic is clinically useful
• SNRIs– Venalafaxine– Duloxetine
• SSRIs are not effective

Unresponsive patients
5 Ds

Diagnosis
Drug
Dose
Duration of treatment
Different treatment