
Anticoagulation 2013 for NSTEMI and STEMI · zBivalirudin for STEMI, Fondaparinux for NSTE ACS,...
28
Anticoagulation 2013 for NSTEMI and STEMI Manesh R. Patel, MD
Transcript of Anticoagulation 2013 for NSTEMI and STEMI · zBivalirudin for STEMI, Fondaparinux for NSTE ACS,...

Anticoagulation 2013 for NSTEMI and STEMI
Manesh R. Patel, MD

DisclosuresDisclosures
Research fundingResearch fundingResearch fundingResearch fundingAstraZeneca, Johnson and Johnson, NHLBI, AHRQAstraZeneca, Johnson and Johnson, NHLBI, AHRQ
ConsultantConsultantJansen, Bayer, Genzyme, OtsukaJansen, Bayer, Genzyme, Otsuka
OffOff--label uses of drugs or devices may be discussedlabel uses of drugs or devices may be discussed
Bivalirudin for STEMI, Fondaparinux for NSTE ACS, Bivalirudin for STEMI, Fondaparinux for NSTE ACS, Coronary stents for ACSCoronary stents for ACS
“Every system is perfectly Every system is perfectly designed to get the results it
”gets”
Dr. Paul BataldenDartmouth College

ACS Management: what are our goals and ACS Management: what are our goals and priorities?priorities?
GoalsGoals PrioritiesPriorities
Treat SxTreat Sx
Attenuate myocardial Attenuate myocardial
Rapid treatmentRapid treatmentRisk stratificationRisk stratificationyy
damagedamage
Reduce the risk ofReduce the risk of
Balance risk of Balance risk of thrombosis with risk of thrombosis with risk of bleedingbleedingReduce the risk of Reduce the risk of
recurrent ischemic recurrent ischemic eventsevents
bleedingbleedingIntegrate strategies into Integrate strategies into invasive or conservative invasive or conservative
ShortShort--term (interm (in--hospital)hospital)
LongLong--termterm
managementmanagementRecognize duration of Recognize duration of treatment coursetreatment course
Reduce LOS/CostsReduce LOS/Costs

ACS Management: StateACS Management: State--ofof--thethe--artart
NSTENSTE--ACSACS STEMISTEMI
Management optionsManagement optionsIndividualized therapy vs. Individualized therapy vs.
STEMI NetworksSTEMI NetworksPharmacotherapyPharmacotherapy
oneone--sizesize--fitsfits--allall
Risk stratificationRisk stratification
pypyStent typeStent typeVascular access*Vascular access*
Initial triage*Initial triage*
Invasive vs. conservativeInvasive vs. conservative

Management options Management options –– NSTE ACSNSTE ACSNSTE ACSNSTE ACSO2, NTG, ASA
Clopidogrel Ticagrelor Prasugrel
UFH Enoxaparin Fondaparinux Bivalirudin
Invasive Conservative
DES
CABG PCIRadial
Femoral
DES
BMS

ACS Management in 2012 and beyond…ACS Management in 2012 and beyond…
The old…The old… The new…The new…

Risk scores and the guidelinesRisk scores and the guidelines

ESC guidelines:ESC guidelines:BleedingBleeding complications?complications?Bleeding Bleeding complications?complications?
Assessment of bleeding risk is an important part of Assessment of bleeding risk is an important part of the decisionthe decision--making process and should be taken making process and should be taken into account when deciding on a treatment strategy into account when deciding on a treatment strategy (I(I--B)B)Minor bleeding should be managed without interruption Minor bleeding should be managed without interruption of active Rx (Iof active Rx (I--C)C)M j bl di i i t ti / t li ti fM j bl di i i t ti / t li ti fMajor bleeding requires interruption/neutralization of Major bleeding requires interruption/neutralization of antithrombotic Rx unless it can be adequately controlled antithrombotic Rx unless it can be adequately controlled (I(I--C)C)The decision to transfuse should be made individually The decision to transfuse should be made individually but withheld in stable patients with Hct > 25% or Hgb > but withheld in stable patients with Hct > 25% or Hgb > 8g/dl (I8g/dl (I--C)C)
Bassand JP. Bassand JP. European Heart JournalEuropean Heart Journal 20072007Bassand JP. Bassand JP. European Heart JournalEuropean Heart Journal 20072007

GRACE Risk ScoreGRACE Risk Score
http://www.outcomes-umassmed.org/grace/
Arch Intern Med 2003;163:2345-2353
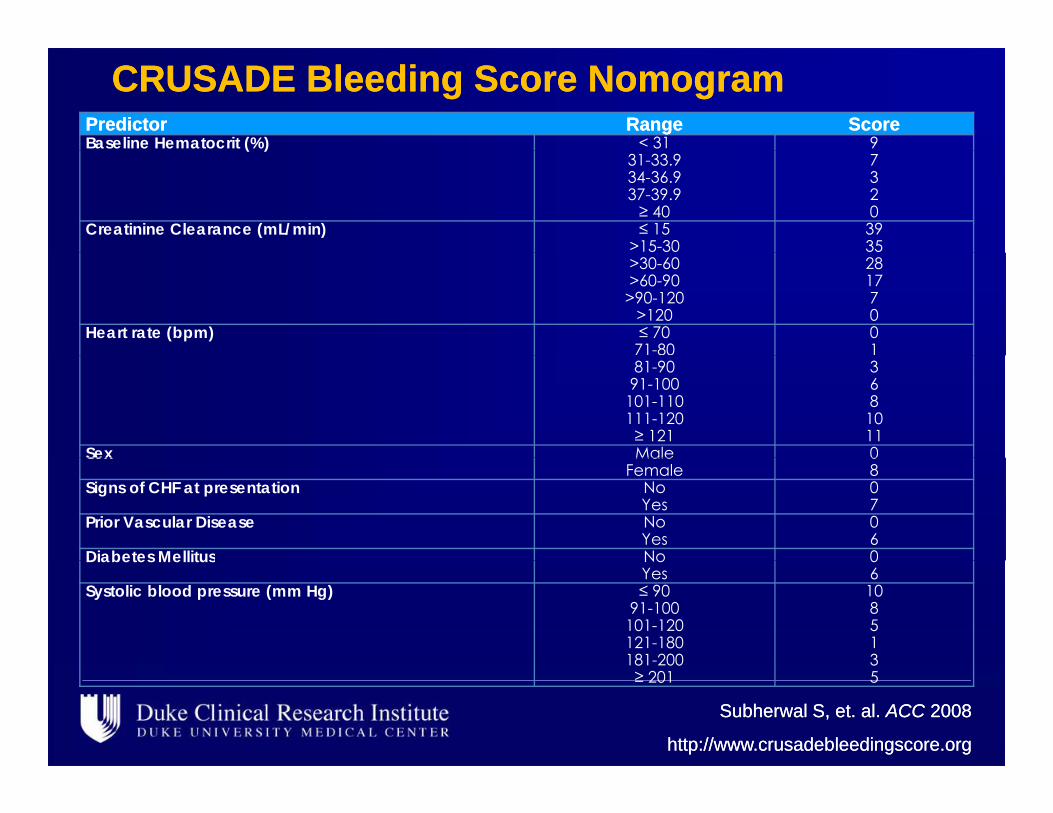
CRUSADE Bleeding Score NomogramCRUSADE Bleeding Score NomogramPredictorPredictor RangeRange ScoreScoreBaseline Hematocrit (%) < 31 9( )
31-33.934-36.937-39.9≥ 40
7320
Creatinine Clearance (mL/min) ≤ 15>15-30
3935
>30-60>60-90
>90-120>120
281770
Heart rate (bpm) ≤ 7071-80
01
81-9091-100
101-110111-120≥ 121
3681011
Sex Male 0Sex MaleFemale
08
Signs of CHF at presentation NoYes
07
Prior Vascular Disease NoYes
06
Diabetes Mellitus No 0Diabetes Mellitus NoYes
06
Systolic blood pressure (mm Hg) ≤ 9091-100
101-120121-180181-200
108513
Subherwal S, et. al. Subherwal S, et. al. ACCACC 20082008
http://www.crusadebleedingscore.orghttp://www.crusadebleedingscore.org
181 200≥ 201
35

CRUSADE Bleeding Risk ScoreCRUSADE Bleeding Risk Score
Patients were categorized into quintiles of risk Patients were categorized into quintiles of risk groups based on their CRUSADE Bleeding groups based on their CRUSADE Bleeding ScoreScore
Risk N Min Score Max Score Bleedingg
Very low 19,486 1 20 3.1%
Low 12 545 21 30 5 5%Low 12,545 21 30 5.5%
Moderate 11,530 31 40 8.6%
High 10,961 41 50 11.9%g
Very High 15,210 51 91 19.5%
Subherwal S, et. al. Subherwal S, et. al. ACCACC 20082008

TIMACS Trial TIMACS Trial N=3031 ACS patients randomized to early or delayed angiographyN=3031 ACS patients randomized to early or delayed angiography
End point HR (95% CI) pp ( % ) p
Death, MI, stroke* 0.85 (0.68–1.06) 0.15
Death MI refractory 0 72 (0 58 0 89) 0 002Death, MI, refractory ischemia
0.72 (0.58–0.89) 0.002
Death, MI, stroke, refractory 0.84 (0.71–0.99) 0.039, , , yischemia, repeat intervention
( )
Refractory ischemia 0.30 (0.17–0.53) <0.00001
*Primary end point; Reference is delayed angiography
Mehta SR et al NEJM 2009

TIMACS Trial TIMACS Trial N=3031 ACS patients randomized to early or delayed angiographyN=3031 ACS patients randomized to early or delayed angiography
Mehta SR et al NEJM 2009

TIMACSTIMACSRates of death, MI, or stroke within six months according to GRACE risk level Rates of death, MI, or stroke within six months according to GRACE risk level and HR (95% CI)and HR (95% CI)and HR (95% CI)and HR (95% CI)
Risk level by GRACE score*
Early (%) Delayed (%) HR (95% CI) p
Low/ 7 7 6 7 1 14 (0 82 1 58) 0 43Low/intermediate
(n=2070)
7.7 6.7 1.14 (0.82–1.58) 0.43
*Low/intermediate risk=GRACE score <140
High (n=961) 14.1 21.6 0.65 (0.48–0.88) 0.005
High risk=GRACE score >140
Mehta SR et al NEJM 2009

pain-free low–mod risk pain-free low–mod risk
Symptoms of Acute IschemiaSymptoms of Acute IschemiaDuke ACS Duke ACS AlgorithmAlgorithmDuke ACS Duke ACS AlgorithmAlgorithm N T i d ECG ithi 10 i tN T i d ECG ithi 10 i t
ST ↑, LBBBST ↑, LBBB
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
Chest Chest
AlgorithmAlgorithmAlgorithmAlgorithmEnroll in TrialsEnroll in Trials
Nurse Triage and ECG within 10 minutesNurse Triage and ECG within 10 minutes
≥ 12h Sx≥ 12h Sx non ST ↑ ACS, mod–high risknon ST ↑ ACS, mod–high risk
Chest Chest Pain UnitPain UnitASA ASA 325 mg initial dose; 325 mg initial dose;
81 mg 81 mg qDqD until/at DCuntil/at DC< 12h Sx< 12h Sx
Primary PCIPrimary PCIA i h b i RA i h b i RAntithrombotic RxAntithrombotic Rx
Ticagrelor Ticagrelor or or ClopidogrelClopidogrel 600 mg load; 150 mg qD for 7d or until DC (if PCI)600 mg load; 150 mg qD for 7d or until DC (if PCI)
TicagrelorTicagrelor or or PrasugrelPrasugrel**
NSSTT Δs,neg. cardiac markersNSSTT Δs,neg. cardiac markers
ClopidogrelClopidogrel 600 mg load; 150 mg qD for 7d or until DC (if PCI)600 mg load; 150 mg qD for 7d or until DC (if PCI)Dynamic STΔs , pos. cardiac markersDynamic STΔs , pos. cardiac markers
BivalirudinBivalirudin or or UFH/GP IIb/IIIaUFH/GP IIb/IIIa
cath in 12hcath in 12hno cath in 12hno cath in 12h
Anticoagulant RxAnticoagulant RxCath <24 hrsCath <24 hrs Cath >24 hrsCath >24 hrs No or delayed cathNo or delayed cath
FondaparinuxFondaparinux or enoxaparinor enoxaparinUFHUFH ††
FondaFonda UFHUFHOr Or bivalirudinbivalirudin*****Prasugrel for primary PCI (if no h/o TIA or stroke); *Prasugrel for primary PCI (if no h/o TIA or stroke); ††GP IIb/IIIa at time of PCI or if refractory ischemia; **Consider bivalirudin for GP IIb/IIIa at time of PCI or if refractory ischemia; **Consider bivalirudin for cath <12 hourscath <12 hours

Duke ACS AlgorithmDuke ACS Algorithm
Symptoms of Acute Ischemia
Consider for Clinical TrialsConsider for Clinical Trials
Nurse Triage and ECG within 10 minutesNurse Triage and ECG within 10 minutes
ST ↑ LBBBST ↑ LBBB pain-free low–mod risk pain-free low–mod risk ASAASA 325 mg initial dose; 325 mg initial dose;
81 mg qD until DC81 mg qD until DC
Consider for Clinical TrialsConsider for Clinical Trials
ST ↑, LBBBST ↑, LBBB
< 12 h Sx< 12 h Sx
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
≥ 12 h Sx≥ 12 h Sx non ST ↑ ACS, mod–high risknon ST ↑ ACS, mod–high risk
81 mg qD until DC81 mg qD until DC
Reperfusion RxReperfusion Rx Chest Pain UnitChest Pain Unit
gg
Antithrombotic RxAntithrombotic Rx

Duke ACS Algorithm: STEMIDuke ACS Algorithm: STEMIDuke ACS Algorithm: STEMIDuke ACS Algorithm: STEMIReperfusion RxReperfusion Rx
Activate ICC Express/AMI HotlineActivate ICC Express/AMI Hotline
1st door-to-balloon > 90 min1st door-to-balloon > 90 min 1st door1st door--toto--balloon < 90 minballoon < 90 min1st door1st door--toto--balloon < 90 minballoon < 90 min
Primary PCIPrimary PCI
Cr unknown or Cr unknown or Known Cr > 2.5 Known Cr > 2.5 UFH b lUFH b l
Upstream of labUpstream of labUpstream of labUpstream of lab
TT TT (TNK)(TNK) + clopidogrel+ clopidogrel
Ti lTi l
UFHUFH Enoxaparin Enoxaparin (Dose adjust to 0.75 mg/kg q 12 (Dose adjust to 0.75 mg/kg q 12
<2.5 mg/dL<2.5 mg/dLmg/dLmg/dL UFH bolusUFH bolus TicagrelorTicagrelor or or clopidogrelclopidogrel
In labIn labIn labIn lab( j g g q( j g g qhours with no bolus if ≥ 75 years) hours with no bolus if ≥ 75 years) BivalirudinBivalirudin or or
UFH/GP IIb/IIIaUFH/GP IIb/IIIaTicagrelorTicagrelor or or PrasugrelPrasugrel* * or or clopidogrelclopidogrel
*Presentation to Duke ED (no h/o TIA or stroke) and for clopidogrel failure; transferring *Presentation to Duke ED (no h/o TIA or stroke) and for clopidogrel failure; transferring RACE ERs will give clopidogrel; decision in lab if thienopyridine not administered RACE ERs will give clopidogrel; decision in lab if thienopyridine not administered
upstreamupstream

Duke ACS AlgorithmDuke ACS Algorithm
Symptoms of Acute Ischemia
Consider for Clinical TrialsConsider for Clinical Trials
Nurse Triage and ECG within 10 minutesNurse Triage and ECG within 10 minutes
ST ↑ LBBBST ↑ LBBB pain-free low–mod risk pain-free low–mod risk ASAASA 325 mg initial dose; 325 mg initial dose;
81 mg qD until DC81 mg qD until DC
Consider for Clinical TrialsConsider for Clinical Trials
ST ↑, LBBBST ↑, LBBB
< 12 h Sx< 12 h Sx
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
pain free, low mod risk, neg or nonspecific ECGneg. CK-MB, TnT/I
≥ 12 h Sx≥ 12 h Sx non ST ↑ ACS, mod–high risknon ST ↑ ACS, mod–high risk
81 mg qD until DC81 mg qD until DC
Reperfusion RxReperfusion Rx Chest Pain UnitChest Pain Unit
gg
Antithrombotic RxAntithrombotic Rx

Duke ACS Algorithm: NSTE ACSDuke ACS Algorithm: NSTE ACSDuke ACS Algorithm: NSTE ACSDuke ACS Algorithm: NSTE ACS
Antithrombotic RxAntithrombotic Rx
NSSTT Δs,NSSTT Δs,Dynamic STΔs, Dynamic STΔs,
Ticagrelor Ticagrelor 180 mg load; 90 mg twice daily 180 mg load; 90 mg twice daily or Clopidogrelor Clopidogrel 600 mg load; 150 mg qD for 7d or until DC (if PCI)*600 mg load; 150 mg qD for 7d or until DC (if PCI)*
NSSTT Δs,neg. cardiac markersNSSTT Δs,neg. cardiac markers
Dynamic STΔs, pos. cardiac markersDynamic STΔs, pos. cardiac markers
cath in 12 hcath in 12 hno cath in 12 hno cath in 12 h
Anticoagulant RxAnticoagulant RxCath <24 hrsCath <24 hrs Cath >24 hrsCath >24 hrs No or delayed cathNo or delayed cath
Fondaparinux Fondaparinux or enoxaparinor enoxaparinUFH UFH ††
FondaFonda UFHUFH
in 12 hin 12 hOr bivalirudin**Or bivalirudin**
*Unless high bleeding risk; decrease to 75 mg qD at DC; 75 mg qD if no PCI *Unless high bleeding risk; decrease to 75 mg qD at DC; 75 mg qD if no PCI ††GP IIb/IIIa at time of PCI or if refractory ischemiaGP IIb/IIIa at time of PCI or if refractory ischemia
**Consider bivalirudin for cath <12 hours**Consider bivalirudin for cath <12 hours

Factors in Choosing Which AnticoagulantFactors in Choosing Which AnticoagulantFactors in Choosing Which AnticoagulantFactors in Choosing Which Anticoagulant
ConditionCondition UFHUFH LMWHLMWH FondaFonda BivalBivalConditionCondition UFHUFH LMWHLMWH FondaFonda BivalBival
Severe renal insuff.Severe renal insuff. cautioncaution avoidavoid avoidavoid bestbest
↑↑ bleeding riskbleeding risk neutralneutral avoidavoid yesyes yesyes
Severe renal insuff.Severe renal insuff. cautioncaution avoidavoid avoidavoid bestbest
↑↑ bleeding riskbleeding risk neutralneutral avoidavoid yesyes yesyes↑↑ bleeding riskbleeding risk neutralneutral avoidavoid yesyes yesyes
ThrombocytopeniaThrombocytopenia worstworst betterbetter betterbetter bestbest
↑↑ bleeding riskbleeding risk neutralneutral avoidavoid yesyes yesyes
ThrombocytopeniaThrombocytopenia worstworst betterbetter betterbetter bestbest
Early cath strategyEarly cath strategy yesyes generallygenerally avoidavoid yesyesavoidavoid
Early cath strategyEarly cath strategy yesyes generallygenerally avoidavoid yesyesavoidavoid
Continue anticoagulant until (effective) revascularization or day 7/hospital discharge,
Continue anticoagulant until (effective) revascularization or day 7/hospital discharge, y p g ,
whichever comes firsty p g ,
whichever comes first

What would she want from a cardiac procedure?What would she want from a cardiac procedure?
The real voyage of discovery consists of not in seeking new landscapes,but in having new eyes Marcel Proustbut in having new eyes. Marcel Proust
- Marcel Proust

Radial vs. Femoral in STEMIRadial vs. Femoral in STEMIN=3347 pts from randomized, caseN=3347 pts from randomized, case--control, and cohort studies incl. RIVALcontrol, and cohort studies incl. RIVAL
MortalityMortality
Bleeding
Procedure time (min)
Joyal D, et. al. AJC 2012

ESC Updated STEMI GuidelinesESC Updated STEMI Guidelines
The guidelines also support the use of transradial The guidelines also support the use of transradial primary PCI over the use of transfemoral, but primary PCI over the use of transfemoral, but only only i th h d f i d ti th h d f i d tin the hands of experienced operators…in the hands of experienced operators…
Steg PG, James SK, Atar D, et. al. EHJ 2012

ACS: StateACS: State--ofof--thethe--art art Accelerated developments in ACS management makeAccelerated developments in ACS management makeAccelerated developments in ACS management make Accelerated developments in ACS management make the the ““optimaloptimal”” strategy a constantly moving targetstrategy a constantly moving target
The benefitThe benefit--risk ratio of the chosen strategy may be influenced risk ratio of the chosen strategy may be influenced by the patientby the patient’’s baseline risks baseline riskby the patientby the patient s baseline risks baseline risk
Nomograms to assess a patientNomograms to assess a patient’’s risk of death, s risk of death, death/MI, and bleeding in the shortdeath/MI, and bleeding in the short-- and intermediateand intermediate--, g, gterm are availableterm are availableSTEMI care has improved significantlySTEMI care has improved significantly
The future is to reduce complications (bleeding, vascular), The future is to reduce complications (bleeding, vascular), develop networks, STEdevelop networks, STE--NoMI?NoMI?
Radial approach supported by trials, observational data, Radial approach supported by trials, observational data, pp pp y , ,pp pp y , ,and guidelinesand guidelines
No D2B consistently reported, mechanism of benefit unclearNo D2B consistently reported, mechanism of benefit unclearNeed a large multicenter trial that reports clinical outcomes andNeed a large multicenter trial that reports clinical outcomes andNeed a large multicenter trial that reports clinical outcomes and Need a large multicenter trial that reports clinical outcomes and D2BD2B

““Every system is perfectly designed to get the results it gets”to get the results it gets
Dr. Paul BataldenDartmouth CollegeDartmouth College
“C i th t ?”Can we improve the system?

Questions
All Rights Reserved, Duke Medicine 2008


















