Anticipatory supply of palliative care medications for ... · Version 2.0 Anticipatory Supply of...
26
Version 2: Draft Anticipatory Supply of Palliative Care Medications for Adults Policy Anticipatory Supply of Palliative Care Medications for Adults Policy 8 November 2012 Version 2.0 (Refer to back page for version control record) IMPORTANT NOTICE : If the review date of this policy or procedure has expired staff should seek advice from their clinical lead or manager regarding the appropriate action to be taken. Staff should refer to the POD for the most up to date information.
Transcript of Anticipatory supply of palliative care medications for ... · Version 2.0 Anticipatory Supply of...
Version 2: Draft Anticipatory Supply of Palliative Care Medications for Adults Policy
Anticipatory Supply of Palliative Care
Medications for Adults Policy
8 November 2012
Version 2.0
(Refer to back page for version control record)
IMPORTANT NOTICE : If the review date of this policy or procedure has expired staff should seek advice from their clinical lead or manager regarding the appropriate action to be taken.
Staff should refer to the POD for the most up to date information.
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 2 of 26 Date of Issue: 7
th February 2014
CONTROL RECORD
Title Anticipatory Supply of Palliative Care Medications for Adults Policy
Purpose Guidance for the prescribing ,supply, administration and disposal of anticipatory medications
Audience All Prescribers and community healthcare and nursing staff
Version Version 2.0 Version Date 8 November 2012
Issue 1 Issue Date 7 February 2014
Status Final Review Date 8 November 2014
Author End of Life Care Team and Dr Christina Sharkey
Development group
End of Life Care Team, Dr Christina Sharkey, End of Life Care Implementation Group, Michele Bates, Community nursing and rehabilitation service, Medicines Management Team,
Superseded Documents
Policy for the Anticipatory Supply of Palliative Care Medications for Adults
Associated Documents
Approved by Quality Assurance Forum Date 8 November 2012
Ratified by Patient Safety Committee Date 18 December 2012
Distribution list All Staff within Nottingham CityCare Partnership
Access Rights Nottingham CityCare Partnership
Impact Assessment
How do the changes affect staff
How do the changes affect working practices
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 3 of 26 Date of Issue: 7
th February 2014
Contents
Page
1 Introduction 5
2 Evidence Base 5
3 Purpose 5
4 Scope 6
5 Definitions 6
6 Responsibilities 6
7 Risk Management (Indications and Contra-Indications/ Hazards) 8
8 Equipment List 8
9 The Process 9
9.1 Suitable Patients 9
9.2 Prescribing the Medications 10
9.3 Communication with other Teams 10
9.4 Prescription Requirements 10
9.5 Collection and Delivery arrangements 11
9.6 Storage of Medications 12
9.7 Checking 12
9.8 Checking the contents of the Anticipatory Prescribing Pack 12
9.9 Authorisation and Administration of Medications from the Anticipatory Prescribing Pack
12
9.10 Information Sheets 13
9.11 Anticipatory Prescribing Pack No Longer Required 13
9.12 Review Process 14
10 Audit 14
11 Anticipatory Prescribing Pack in the Care Home Setting 14
12 Interaction with Other Policies and Procedures 15
13 Equality & Diversity Statement 15
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 4 of 26 Date of Issue: 7
th February 2014
14 Monitoring & Review (of this policy) 15
15 Further Guidance 16
16 References 16
Appendix 1 Anticipatory Prescribing Pack Patient Information Leaflet 17
Appendix 2 ‘The Core Four’, FP10 Prescription completed example 18
Appendix 3 Community Pharmacy Palliative Care Drugs Scheme (April 2012) 19
Appendix 4 Anticipatory Prescribing Policy Inventory Card – Weekly Check Card pre First Drug Administration
21
Appendix 5 DNS1 AP - Prescription Record Sheet for Anticipatory Medications 22
Appendix 6 General Practitioner/Community Nurse Information Sheet 23
Appendix 7 Pharmacists Information Sheet 25
Version History 26
Change Control Record 26
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 5 of 26 Date of Issue: 7
th February 2014
Introduction
1.1. Despite the fact that up to 90% of all palliative care occurs in a patient’s home environment and the majority of patients and their carers wish for a home death, a majority of people still die in an institution. Uncontrolled symptoms and lack of anticipatory palliative care are a contributory factor to high hospital death rates and patients being unable to die in their place of choice.
1.2. Often towards the end of life patients cannot swallow oral medication therefore parenteral administration is required via a subcutaneous injection to control symptoms. This medication needs to be available immediately to the doctor and district nurse making the assessment of a patient’s deterioration. Therefore it is recommended that the regular GP prescribes medication in advance of deterioration and that these drugs are left in the patient’s home.
1.3. Anticipatory prescribing is now embedded into practice within Nottingham CityCare Partnership as indicated by the End of Life Care Pathway audit 2010-11. It reported that 73% of known palliative patients had anticipatory medications prescribed (Nottingham CityCare Partnership, 2011).
2. Evidence Base
2.1. The National End of Life Care Strategy (Department of Health (DoH), 2008) identifies the need of effective anticipatory planning and the need for prompt access to additional medications, for example, the use of anticipatory prescribing and palliative care boxes stored at the patient’s home. From a local perspective the Nottinghamshire End of Life Care Pathway for All Diagnoses recommends that Anticipatory Medications are supplied when a patient’s diagnosis is “a few weeks”, to help control any distressing symptoms.
2.2. Securing proper access to medications in the out of hours period recommends prompt and easy access to palliative care medications in the out of hours period (action points 8 and 9, DoH, 2004).
2.3. The Liverpool Care Pathway (LCP) is one of the recognised best practice tools in end of life care. The Core Four medications advised for use in the symptom control guidelines within the LCP are the same as those recommended within this policy.
3. Purpose
3.1. The purpose of this policy is to ensure appropriate and effective prescribing and supply of palliative medications are in place in anticipation of need
3.2. The aim is to provide enough parenteral medication potentially to last for 24 – 72 hour period. This will provide enough medication for a weekend period when a patient’s regular GP is not available.
3.3. To prevent unproductive admissions to hospital for symptom management in end of life care.
3.4. To promote choice as patients might be able to achieve their preferred place of care if they have these medications in place.
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 6 of 26 Date of Issue: 7
th February 2014
4. Scope
4.1. This policy is aimed at all prescribers employed by Nottingham CityCare Partnership
4.2. This policy applies to all registered nurses within Nottingham CityCare Partnership, if appropriate to their role
4.3. Aspects of this policy will be relevant to other community services, for example Community Pharmacy services, General Practitioners (GPs), Nottingham Emergency Medical Services (NEMS) and Palliative Care at Home Services.
5. Definitions
Anticipatory Medications: this refers to the four core medications that are provided in preparation of potential palliative symptoms
Anticipatory Prescribing Pack: this refers to the Grey Box and contents including the medications
GP: General Practitioner
Liverpool Care Pathway: this is a nationally recognised best practice tool. It is a pathway designed to be used in the last days of life
PRN: this is the recognised term for a when required medication
Single Step Range: dose increase from original starting dose to next recognised step up dose, this is usually a 100% increase, e.g. 2.5-5mg
6. Responsibilities
In order to fulfil its responsibilities the following personnel are responsible to ensure Nottingham CityCare Partnership meets its objectives:
6.1. Chief Executive
promoting and supporting the aims and objectives of this policy
providing resources for putting the policy into practice
6.2. Executive Team
Are responsible for implementing and disseminating the policy to all clinical staff within their area of responsibility.
6.3. Medicines Management Team
To offer support and training to all appropriate staff where necessary regarding controlled drugs and medications used in regard to this policy
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 7 of 26 Date of Issue: 7
th February 2014
6.4. Team Managers
To ensure that all appropriate registered nurses have access and awareness of the policy and any subsequent updates.
To ensure all staff are aware of the documentation provided within this policy and any subsequent updates.
To ensure all staff are aware of the their role and responsibility in the use of Anticipatory Medications
6.5. Nottingham CityCare Partnership Staff
6.5.1. All Staff
Are aware of their clinical responsibilities regarding the supply of anticipatory medications
Understand what they have to do regarding every stage of use of the anticipatory medications
To understand and implement responsibilities in accordance to the Controlled Drugs policy
Understand their role in explaining to carers/family in regard to collection, administration and destruction of the anticipatory medications
To ensure they are competent to work with the medications within this policy, for example why they have been prescribed, appropriate doses and when to administer. If additional support is required contact team manager or the End of Life Care Team.
6.5.2. Prescribers (including Non-Medical Prescribers (NMP))
Fully understand the process for prescribing the anticipatory medications
6.5.3. The staff who administer these medications
Ensure the contents of the palliative care pack are correct and up to date
Understand their responsibility to ensure appropriate equipment required is available in order to administer the medications
To check the medications on a regular basis and record in the nursing notes (appendix 4)
6.6. End of Life Care Team
As the current author of this policy the team has responsibility to ensure any relevant updates are amended in a timely manner
Will update the overall policy in the required timeframe
To hold stock of the grey boxes. If replacement or additional boxes are required then please contact the End of Life Care Team.
Will be able to advise registered nurses and GPs regarding the use of the policy and medications within it
To raise awareness of this policy and the medications used within it for new starters. This will be delivered at the Syringe pump training session for new starters.
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 8 of 26 Date of Issue: 7
th February 2014
7. Risk Management (Indications and Contra-Indications/ Hazards)
7.1. All infection control precautions should be followed as per current Infection Prevention and Control Policy (Nottingham CityCare Partnership, 2011).
7.2. Safe disposal of sharps as per the safe handling and disposal of sharps including the prevention of occupational exposure to blood borne viruses policy (Nottingham CityCare Partnership, 2011)
7.3. Safe disposal of medications as per CD Policy (Nottingham CityCare Partnership, 2012).
7.4. As with any procedure involving injections there is a potential risk of sharps injuries, the policy above (7.2) outlines actions to be taken in this scenario
7.5. All registered healthcare professionals are accountable for their actions and omissions.
7.6. In prescribing these medications the prescriber should be aware of individual patient needs, e.g. appropriate doses and dose conversion. See National Patient Safety Agency (2008) Reducing Dosing Errors with Opioid Medicines (NPSA/2008/RRR05).
7.7. In administering any medication individuals must exercise their professional judgment and apply their knowledge and skill in a given situation.
7.8. Patients and/or carers may misinterpret anticipatory prescribing as provision for euthanasia or it may cause increased anxiety that death is near, however clear effective communication and use of patient information leaflet (Appendix 1) should allay these fears.
7.9. It is best practice that all patients who have these medications must be risk assessed for the safety of use of these medications
7.10. As with all drugs, medications supplied in patients’ residence may be open to abuse. It is vital that a risk assessment is completed if there are any known problems. This information must be shared with colleagues, it should be stored in the patient’s notes and documented on SystmOne.
7.11. Refer to the Controlled Drug Policy and Controlled Drug Standard Operating Procedure to fulfil the requirements regarding the use of controlled drugs
8. Equipment List
8.1. Once prescribed and the medications are in the patient’s home, they should be stored in the grey box designed specifically for the task. Within the box there should be:
Patient leaflet (appendix 1)
Laminated copy of the example FP10 (appendix 2)
Community Pharmacy Palliative Care Drugs Scheme (Appendix 3)
Anticipatory Prescribing Policy Inventory Card (appendix 4)
8.2. To ensure that the boxes are utilised to the maximum it is advisable to also include:
Palliative Care Pocketbook
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 9 of 26 Date of Issue: 7
th February 2014
Liverpool Care Pathway
Spare medication documents (DNS1 AP, DNS2, DNS3 etc)
A sample of slip syringes (1ml and 2ml)
Needles for the above
Butterflies (winged infusion sets)
Transparent dressings
8.3. To comply with the Nottingham CityCare Partnership CD policy all partially used controlled drugs ampoules must be destroyed using a denaturing kit the policy states
“In the case of a part ampoule or unfinished syringe pump, the contents should be destroyed in the home in the presence of a witness (where possible). The CD waste should be added to a ‘denaturing kit’* as per container instructions.” (CD Policy, Nottingham CityCare Partnerships, 2012)
8.4. All sharps must be discarded using an appropriate sharps bin
9. The Process
9.1. Suitable Patients
9.1.1. Any appropriate patient must have been referred to the Community Nursing and Rehabilitation Team for a holistic assessment of their palliative care needs. The patient must be registered on SystmOne and there must be written records within the home that are accessible to visiting professionals
9.1.2. A patient is identified as appropriate for the Anticipatory Prescribing Pack by a GP or community nurse. The pack is usually introduced in the last few weeks of life, this can be difficult to diagnose but those who are eligible for Fast Track funding which is equivalent of the amber phase of the Nottinghamshire End of Life Care Pathway would be suitable. For Clinical guidance see the Gold Standards Framework Prognostic Indicator Guidance, available at:
http://www.goldstandardsframework.org.uk/Resources/Gold%20Standards%20Framework/General/Prognostic%20Indicator%20Guidance%20October%202011.pdf
9.1.3. Patients ability to swallow and general condition may vary at the time of initiating the Anticipatory Prescribing Pack, therefore their introduction should be reviewed regularly
9.1.4. A risk assessment must be completed to ensure there are no risks regarding known drug misusers who have access to the patient’s home. Decisions must be made by the multi-disciplinary team if it is appropriate to provide the Anticipatory Prescribing Pack when a known drug misuser has access to a patients home.
9.1.5. The provision of the Anticipatory Prescribing Pack must be discussed with the patient and where possible the family/carer. It is vital they understand why these medications are being prescribed. Give consideration to communication needs (e.g. if an interpreter is required) and the Patient Leaflet (appendix 1) should be left with the most relevant people. If the patient leaflet is given from the pack please replace for next time the pack is used.
9.1.6. Where patients lack capacity to consent and understand the necessity for the Anticipatory Prescribing Pack, then the process of making a best interest decision should be followed, by completing a two stage test and documenting all findings. This would include discussion
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 10 of 26 Date of Issue: 7
th February 2014
with partner, relatives, carers or potentially friends and multidisciplinary team. This is in line with the Mental Capacity Act: Code of Practice (Department of Constitutional Affairs, 2007)
9.2. Prescribing The Medications
9.2.1. The four medications to be prescribed are based on the medications advised for use in the symptom control guidelines of the Liverpool Care Pathway. The four core medications, typical starting doses and quantities to be prescribed are:
Medication Strength Quantity
Morphine Sulphate * 10mg/1ml 5 x 10mg ampoules
Levomepromazine 25mg/1ml 5 x 25mg ampoules
Midazolam 10mg/2ml 5 x 10mg ampoules
Hyoscine Butylbromide 20mg/1ml 5 x 20mg ampoules
Water for Injection 10 x 10ml ampoules
* If patient is already on a opiate based medication then the dose must be individually calculated/converted to ensure correct dose is available for parenteral (subcutaneous) use
9.2.2. If the patient is already taking any of these medications orally or parentally then this should be taken into consideration when deciding the dosage and strength required
9.2.3. Single doses can be prescribed. However, a single step range being prescribed is permissible as per the Liverpool Care Pathway symptom control sheets. Instructions should be clear to give the lower dose first (this is stated on the new DNS AP form) however this then allows a higher dose to be administered next time if the lower dose was ineffective. Typical starting dose ranges for example:
Morphine Sulphate 2.5-5mg Midazolam 2.5mg-5mg
9.2.4. If there are any changes to medication dosage a new prescription DNS1 AP (Appendix 5) must be written.
9.2.5. The medications cannot be administered unless a DNS1 AP has been provided and is in the patients home
9.3. Communication with other teams
9.3.1. Communication with out of hours services is essential to inform them that there are anticipatory medications in the home. This should be communicated via the special patient information section of the NEMS/NHS Direct Special Patient Notes handover form. The NEMS form must be completed by a GP or registered nurse.
9.3.2. The Evening and Night service will require clear communication regarding the Anticipatory Prescribing Pack, to ensure they are aware it is in the home of the patient. This should be done by telephone and/or fax.
9.3.3. If the patient is in receipt of hospice at home services then the presence of anticipatory medications must be communicated to the provider.
9.4. Prescription Requirements
9.4.1. A normal FP10 prescription is generated for the medications contained in the Anticipatory Prescribing Pack and signed by the prescriber (GP or non-medical prescriber) caring for the
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 11 of 26 Date of Issue: 7
th February 2014
patient. The correct dosage must be specified for all medications and they should be written ‘In Anticipation of’ (see Appendix 2)
9.4.2. To complete the DNS1 AP all information must be clearly written, this includes: Name of drug; Indication; Dose to be given; minimal interval; maximum dose in 24 hours; route of administration; name and signature of prescriber. This needs to be completed for each medication prescribed on the form.
9.4.3. Prescriptions for parenteral/subcutaneous Morphine and Midazolam are subject to controlled drugs regulations.
9.4.4. It may be possible for GP practices to create the FP10 into a computer template; taking care to individualise doses and identify any patient specific issues e.g. allergies or interactions.
9.4.5. A prescription (FP10) for the anticipatory medication controlled drug such as Morphine Sulphate should typically contain the following instructions:
Morphine Sulphate 10mg/1ml, 5 (five)x 1ml ampoules. Dose 2.5-5mg subcutaneously in anticipation of pain, at least one hour between doses The dose, strength and number of ampoules need to be individually prescribed to meet the needs of the patient.
A single step dose range (i.e. one step e.g. 2.5-5mg morphine) is permissible and should typically be used in the following circumstances
Where the patients symptoms are not well controlled and there may be a delay in contacting a prescriber to increase the dose to the next level
Where a patient is in their final days of life and the lowest dose in the range has been administered and the pain is not well controlled after one to two hours
The administrator should always start with the lower dose. If the administrator has any concerns regarding the use of ranges they must contact the prescriber or another authorised prescriber for advise and support e.g. out of hours GP.
9.4.6. If the patient has required more than two extra PRN doses in a 24 hour period then consider commencing a syringe pump. If this is the case then calculate the dose for the syringe pump by adding the total of each medication used in the previous 24 hour period. It is essential to review if this is effective, ideally on a daily basis.
9.5. Collection and Delivery Arrangements
9.5.1. The general practitioner is responsible for writing the prescription. Alternatively a non-medical prescriber e.g. Community Nurse Specialist or Community Matron, can write the prescription if competent and this is relevant to their role
9.5.2. On receipt of the prescription the patient/carer is responsible to collect these medications from a community pharmacy. Appendix 3 provides information regarding the pharmacies that have signed up to hold a supply of the regularly used palliative care drugs
9.5.3. The medications should either be collected by the patient or their nominated carer, alternatively where a community pharmacy offers home delivery this can be arranged. A prescription for controlled drugs is valid for 28 days but the patient/carer should be advised to arrange for the medications to be dispensed and collected promptly.
9.5.4. In exceptional circumstances it is permissible for Nottingham CityCare staff to collect these medications from the pharmacy and deliver to the patient’s home (see the Controlled Drug
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 12 of 26 Date of Issue: 7
th February 2014
Standard Operating Procedure (Controlled Drug Policy, Nottingham CityCare Partnership, 2012) for further information).
9.6. Storage of the Medications
9.6.1. The patient’s community registered nurse is responsible for storing the medications in the container provided by Nottingham CityCare Partnership the “Grey Box”. This needs to be rigid with a secure lid, light proof and non–transparent. The authorised CityCare “Grey Box” must be used where available.
9.6.2. The nurse records the contents of the pack on the anticipatory medications inventory card and stores this in the grey box if the drugs are not to be used immediately
9.6.3. The following details should be completed by the nurse on the inventory card when preparing the Anticipatory Prescribing Pack
Patient’s name.
The name of the prescriber
Drug Name
Ampoule Strength
Stock Balance
The batch or lot numbers of the medications.
Expiry dates of the medications
9.6.4. The nurse places the pack in a suitable location within the patient’s home out of reach and sight of children (if there are children present in the house), accessible to the healthcare professionals caring for the patient. The nurse indicates in the community nursing notes where the Anticipatory Prescribing Pack is located and this must also be recorded on SystmOne
9.7. Checking the contents of the Anticipatory Prescribing Pack
9.7.1. It is the responsibility of the attending nurses to check the contents of the pack regularly and this should be recorded in the community nursing notes using the Inventory Card (appendix 4). If the nurses are attending frequently this does not need to be done more than once a week.
9.8. Discrepancies Found when Checking Pack
9.8.1. If medications do not match the details on the inventory card or DNS2/DNS3 and or/if they has not been completed, the practitioner should attempt to identify who accessed the pack by checking the nursing notes or checking with the practice. The documentation should be completed to explain the discrepancy eg. if the DNS2/DNS3 indicates that the medications were administered.
9.8.2. If the healthcare professional finds any discrepancies not resolved by the above measures, the Incident Reporting Policy and Procedure must be followed.
9.9. Authorisation & Administration of Medication from the Anticipatory Prescribing Pack
9.9.1. Drugs from the pack cannot be administered by the community nursing team unless the medications are authorised (prescribed doses, indication, directions, signed and dated) by a prescriber on the DNS1 AP (appendix 5)
9.9.2. Many clinical scenarios in end of life care can be anticipated, such as a patient being unable to swallow. The medications should be ‘written up’ in advance when the pack is organised for the patient e.g. Morphine Sulphate (Dose) mg in anticipation of pain
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 13 of 26 Date of Issue: 7
th February 2014
9.9.3. Only a healthcare professional qualified to administer medication and accountable to Nottingham CityCare Partnership for care of the patient may administer a medication from the Anticipatory Prescribing Pack.
9.9.4. All documentation must be completed at the time of administration of medication. Where possible and if two members of staff are in attendance all administrations must be witnessed and countersigned
9.9.5. Once any medications have been administered for the first time they all should be transferred to the DNS2 or DNS3, and stock levels should be checked against the inventory card. The Inventory card is now not required and should be placed in the patients notes
9.9.6. When a doctor or nurse administers a medication from the pack, the individual must complete the DNS2 or DNS3 to ensure that an accurate running record is available at all times. The amount of drug given and wasted must be documented.
9.9.7. Any discarded or wasted medications should be discarded into the denaturing kit.
9.9.8. Prior to administration patient details must be verified. The name of the medication, batch number and expiry date should be checked in the usual manner.
9.9.9. If the pack is used by the out-of-hours team, the out of hours doctor or community nurse is responsible for informing the community nursing and rehab teams by telephone/fax or computer link the next working day that the pack has been commenced or any medication administered.
9.10. Information Sheets
9.10.1. Medications are provided with the medicinal product’s patient information leaflets and the healthcare professional administering the medications must ensure the patient has access to the relevant leaflet, as well as the Anticipatory Prescribing Pack Patient Information Leaflet (Appendix 1).
9.10.2. Information Sheets are also provided for:
GPs and community nurses (Appendix 6)
Pharmacists (Appendix 7)
9.11. Anticipatory Prescribing Pack No Longer Required
9.11.1. When the patient has died it is the responsibility of the community nurse to collect the Grey Box, the Denaturing Kit and the Sharps Bin. All unused medications should be returned to the pharmacy by the family/carer and this transfer of medications should be recorded clearly on the DNS2/DNS3.
9.11.2. It is the responsibility of the relatives or carer to return any unused medications to a pharmacy and it may be appropriate for the nurse to remind the carer of this. In exceptional circumstances it is appropriate for the RN to return the drugs to the pharmacy (as per CD Standard Operating Procedure, see CD policy)
9.11.3. The completed inventory card must be inserted into the community nursing notes for tracking and audit purposes
9.11.4. The denaturing kit should be disposed of in a green pharmacy bin (available in health centres)
9.11.5. The risk of contamination of the grey box is low, therefore cleaning the returned container with detergent is adequate
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 14 of 26 Date of Issue: 7
th February 2014
9.12. Review Process
9.12.1. It is the responsibility of the nurses using the anticipatory pack, to review the use of the pack on a monthly basis with the prescriber as to whether the pack should be kept or discarded (if no longer appropriate).
10. Audit
10.1. Audit of use of this policy across Nottingham CityCare Partnership will be encompassed in the End of Life Care Pathway Audit by the End of Life Care Team. This will include the number of patients on the district nursing caseloads that have anticipatory medications prescribed. Audits will be completed and reported annually. Reports will be disseminated to the Medicines Management Group and End of Life Care Implementation Group
11. Patient in the Care Home Setting
11.1. If a care home is the patient’s residence the anticipatory medications will not be stored in the Nottingham CityCare authorised container (Grey box)
11.2. The medications will be stored in a secure drugs cupboard as per the policy for the supply, administration, safe handling and storage of medications in the care home.
11.3. Any clinician representing Nottingham CityCare must sign the drugs in and out of the controlled drugs record book that is held as a stock and administration record in the care home setting (usually kept in the clinic room or where drugs are stored). The nurse must also document using the Nottingham CityCare DNS2 and DNS3 held within patient record.
11.4. Care home with nursing staff must sign the drugs in and out of the controlled drugs record book that is held as a stock and administration record. They must also complete the Medication Administration Record (MAR) sheet, the staff at the care home must ensure this is readily available to the nurses.
11.5. All medication remains the property of the patient when they enter a care home. Under care home regulations, care homes are required to retain patients’ own medication (including controlled drugs) for SEVEN days following the death of a resident. In all cases the medication remains the property of the patient, on the death of the patient, the responsibility passes to the family/care home or carer for the patient. Consent must always be sought when any removal and destruction of medication occurs.
11.6. Following the death of a patient, if the medication is being stored in the care home rather than being returned directly to a community pharmacy it is recommended that the attending nurse ‘signs over’ the medication to the home. This is not a legal requirement but is good practice and a risk management recommendation. The responsibility for safe storage of the medication until the appropriate destruction at a community pharmacy then passes to the care home. The residential care home should return the medication to the community pharmacy for destruction after the seven day period. Nursing homes are responsible to destroy their own medications after seven days.
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 15 of 26 Date of Issue: 7
th February 2014
12. Interaction with Other Policies and Procedures
12.1. This Policy should be read in conjunction with:
Equality & Diversity Policy.
Infection prevention and control policy
Medicines Management Policy
The safe handling and disposal of sharps including the prevention of occupational exposure to blood borne viruses Policy
Controlled Drugs Policy
13. Equality & Diversity Statement
13.1. The Organisation will not tolerate the less favourable treatment of anyone on the grounds of their age, disability, gender, marital status, being pregnant or on maternity leave, race/ethnicity, religion or belief, sexual orientation, responsibility for dependents, trade union or political activities, or any other reason which cannot be shown to be justified
14. Monitoring and Review - (of this policy)
14.1. It is the responsibility of each individual prescriber to ensure that the medications within the Anticipatory Prescribing Pack are prescribed appropriately in accordance to relevant Nottingham CityCare Partnership policies
14.2. The monitoring of compliance to this document is the responsibility of team managers to ensure all registered nurses are using the policy appropriately
14.3. The implementation and use of this policy will be monitored by the End of Life Care team. This will entail an audit of the number of anticipatory medications prescribed, this will be achieved through the annual End of Life Care Pathway audit.
14.4. This Policy will be reviewed every two years or where changes are required, by the End of Life Care team
14.5. Any incident regarding the Anticipatory Prescribing Pack must have an incident form completed. These are monitored monthly at the Patient Safety and Infection Prevention and Control Committee and quarterly at the Governance Committee; both committees act to ensure relevant changes required are implemented
14.6. Serious incident root cause analysis reports and actions plans in relation to Anticipatory Prescribing Pack (for example any incident involving medication issues) are monitored by the patient safety and Infection Prevention and Control Committee monthly until all identified actions have been completed
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 16 of 26 Date of Issue: 7
th February 2014
15. Further Guidance
15.1. If you have any concerns or issues with the contents of this policy or have difficulty understanding how this policy relates to you and/or your role, please contact the End of Life Care team
16. References
Department of Constitutional Affairs (2007) Mental Capacity Act 2005: Code of Practice. London: The Stationary Office. Available at: http://www.justice.gov.uk/downloads/protecting-the-vulnerable/mca/mca-code-practice-0509.pdf Department of Health (2004) Delivering the Out-of-Hours Review: Securing Proper Access to Medicines in the Out-of-Hours Period. London: DoH. Available at: http://www.out-of-hours.info/downloads/short_medicines_guidance.pdf
Department of Health (2008) End of Life Care Strategy: Promoting high quality care for all adults at the end of life. London: DoH. Available at: http://www.endoflifecareforadults.nhs.uk/assets/downloads/pubs_EoLC_Strategy_1.pdf
The Gold Standards Framework (2011) The Prognostic Indicator Guidance: 4th Edition. Shrewsbury: The Gold Standards Framework Centre In End of Life Care CIC. Available at: http://www.goldstandardsframework.org.uk/Resources/Gold%20Standards%20Framework/General/Prognostic%20Indicator%20Guidance%20October%202011.pdf Marie Curie Palliative Care Institute Liverpool (2009) The Liverpool Care Pathway for the Dying Patient (LCP): Supporting care in the last hours or days of life. Nottinghamshire LCP, locally adapted from National LCP version 12. National Patient Safety Agency (2008) Reducing Dosing Errors with Opioid Medicines: NPSA/2008/RRR05. National Patient Safety Agency. Available at: http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=60286&type=full&servicetype=Attachment Next Stage Review (NSR) Group for End of Life Care in Nottinghamshire (2008) Nottinghamshire End of Life Care Pathway for All Diagnoses. Nottingham: NHS Nottinghamshire County, NHS Nottingham City, NHS Bassetlaw, and Local Authorities. Available at: http://www.nottinghamcity.nhs.uk/images/stories/Nottinghamshire%20EoL%20Pathway%20Booklet%20for%20Professionals.Final%20version.pdf
Nottingham CityCare Partnership (2011) Palliative Care District Nursing Clinical Audit 2010-2011.
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 17 of 26 Date of Issue: 7
th February 2014
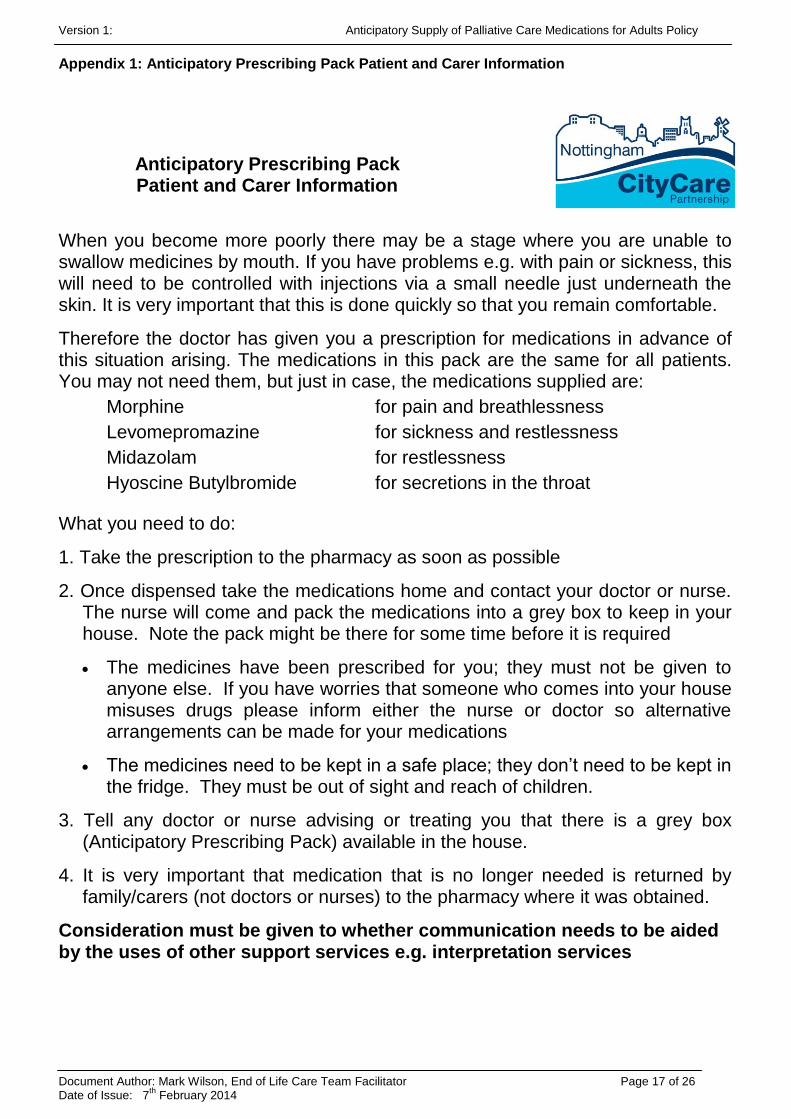
Appendix 1: Anticipatory Prescribing Pack Patient and Carer Information
Anticipatory Prescribing Pack
Patient and Carer Information
When you become more poorly there may be a stage where you are unable to swallow medicines by mouth. If you have problems e.g. with pain or sickness, this will need to be controlled with injections via a small needle just underneath the skin. It is very important that this is done quickly so that you remain comfortable.
Therefore the doctor has given you a prescription for medications in advance of this situation arising. The medications in this pack are the same for all patients. You may not need them, but just in case, the medications supplied are:
Morphine for pain and breathlessness
Levomepromazine for sickness and restlessness
Midazolam for restlessness
Hyoscine Butylbromide for secretions in the throat
What you need to do:
1. Take the prescription to the pharmacy as soon as possible
2. Once dispensed take the medications home and contact your doctor or nurse. The nurse will come and pack the medications into a grey box to keep in your house. Note the pack might be there for some time before it is required
The medicines have been prescribed for you; they must not be given to anyone else. If you have worries that someone who comes into your house misuses drugs please inform either the nurse or doctor so alternative arrangements can be made for your medications
The medicines need to be kept in a safe place; they don’t need to be kept in the fridge. They must be out of sight and reach of children.
3. Tell any doctor or nurse advising or treating you that there is a grey box (Anticipatory Prescribing Pack) available in the house.
4. It is very important that medication that is no longer needed is returned by family/carers (not doctors or nurses) to the pharmacy where it was obtained.
Consideration must be given to whether communication needs to be aided by the uses of other support services e.g. interpretation services
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 18 of 26 Date of Issue: 7
th February 2014
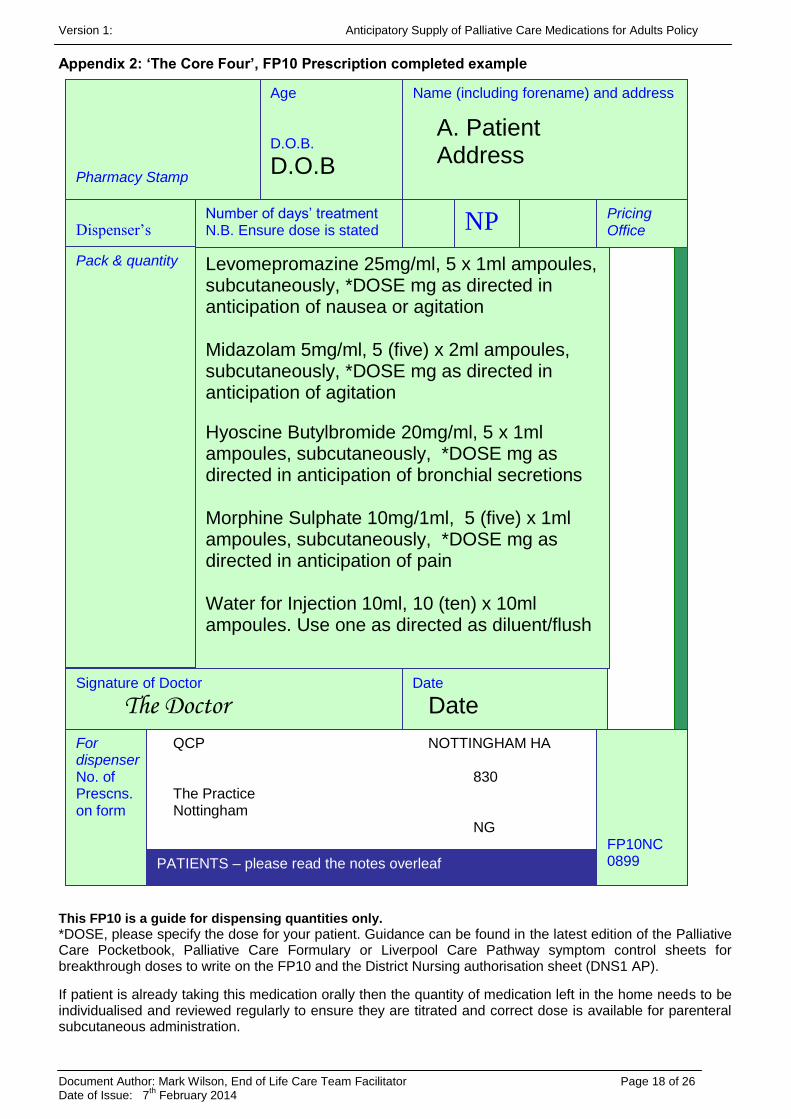
Appendix 2: ‘The Core Four’, FP10 Prescription completed example
This FP10 is a guide for dispensing quantities only.
*DOSE, please specify the dose for your patient. Guidance can be found in the latest edition of the Palliative Care Pocketbook, Palliative Care Formulary or Liverpool Care Pathway symptom control sheets for breakthrough doses to write on the FP10 and the District Nursing authorisation sheet (DNS1 AP).
If patient is already taking this medication orally then the quantity of medication left in the home needs to be individualised and reviewed regularly to ensure they are titrated and correct dose is available for parenteral subcutaneous administration.
Pharmacy Stamp
Name (including forename) and address
A. Patient Address
Dispenser’s
endorsement
Number of days’ treatment N.B. Ensure dose is stated
NP Pricing Office
Pack & quantity
Levomepromazine 25mg/ml, 5 x 1ml ampoules, subcutaneously, *DOSE mg as directed in anticipation of nausea or agitation Midazolam 5mg/ml, 5 (five) x 2ml ampoules, subcutaneously, *DOSE mg as directed in anticipation of agitation
Hyoscine Butylbromide 20mg/ml, 5 x 1ml ampoules, subcutaneously, *DOSE mg as directed in anticipation of bronchial secretions Morphine Sulphate 10mg/1ml, 5 (five) x 1ml ampoules, subcutaneously, *DOSE mg as directed in anticipation of pain Water for Injection 10ml, 10 (ten) x 10ml ampoules. Use one as directed as diluent/flush
Signature of Doctor
The Doctor Date
Date
For dispenser No. of Prescns. on form
QCP NOTTINGHAM HA 830 The Practice Nottingham NG
PATIENTS – please read the notes overleaf
Age D.O.B.
D.O.B
FP10NC 0899
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 19 of 26 Date of Issue: 7
th February 2014
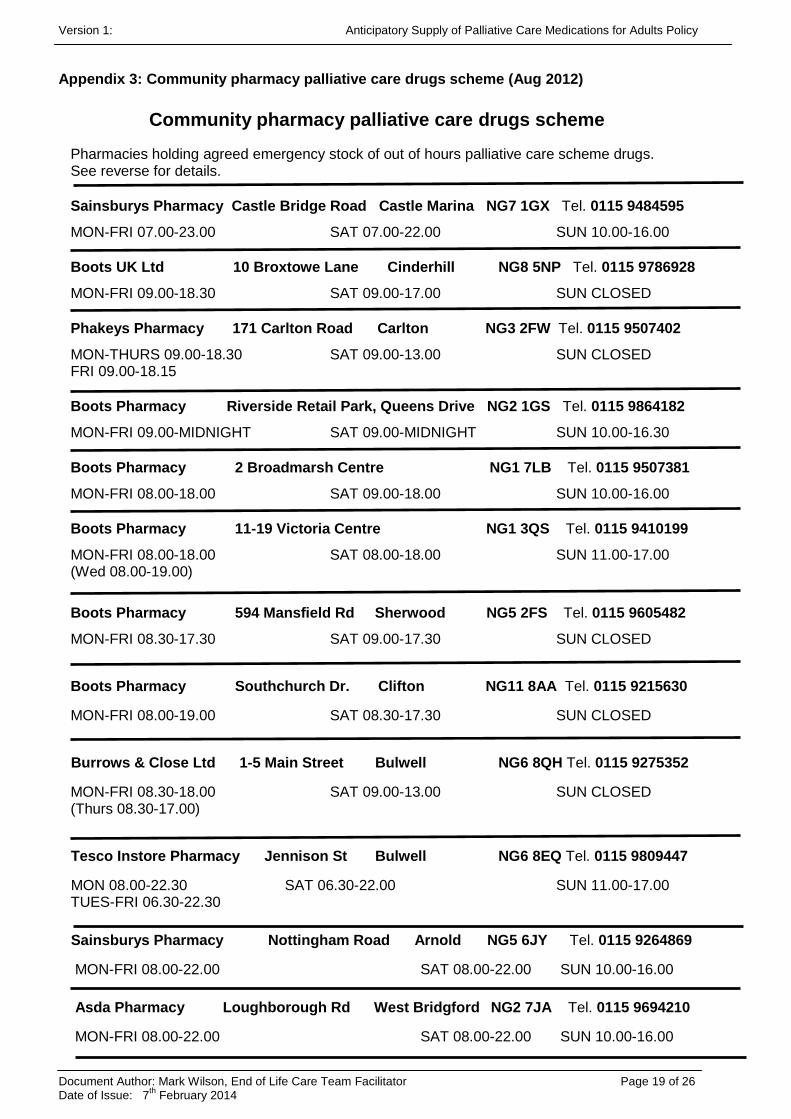
Appendix 3: Community pharmacy palliative care drugs scheme (Aug 2012)
Community pharmacy palliative care drugs scheme
Pharmacies holding agreed emergency stock of out of hours palliative care scheme drugs. See reverse for details.
Sainsburys Pharmacy Castle Bridge Road Castle Marina NG7 1GX Tel. 0115 9484595
MON-FRI 07.00-23.00 SAT 07.00-22.00 SUN 10.00-16.00
Boots UK Ltd 10 Broxtowe Lane Cinderhill NG8 5NP Tel. 0115 9786928
MON-FRI 09.00-18.30 SAT 09.00-17.00 SUN CLOSED
Phakeys Pharmacy 171 Carlton Road Carlton NG3 2FW Tel. 0115 9507402
MON-THURS 09.00-18.30 SAT 09.00-13.00 SUN CLOSED FRI 09.00-18.15
Boots Pharmacy Riverside Retail Park, Queens Drive NG2 1GS Tel. 0115 9864182
MON-FRI 09.00-MIDNIGHT SAT 09.00-MIDNIGHT SUN 10.00-16.30
Boots Pharmacy 2 Broadmarsh Centre NG1 7LB Tel. 0115 9507381
MON-FRI 08.00-18.00 SAT 09.00-18.00 SUN 10.00-16.00
Boots Pharmacy 11-19 Victoria Centre NG1 3QS Tel. 0115 9410199
MON-FRI 08.00-18.00 SAT 08.00-18.00 SUN 11.00-17.00 (Wed 08.00-19.00)
Boots Pharmacy 594 Mansfield Rd Sherwood NG5 2FS Tel. 0115 9605482
MON-FRI 08.30-17.30 SAT 09.00-17.30 SUN CLOSED
Boots Pharmacy Southchurch Dr. Clifton NG11 8AA Tel. 0115 9215630
MON-FRI 08.00-19.00 SAT 08.30-17.30 SUN CLOSED
Burrows & Close Ltd 1-5 Main Street Bulwell NG6 8QH Tel. 0115 9275352
MON-FRI 08.30-18.00 SAT 09.00-13.00 SUN CLOSED (Thurs 08.30-17.00)
Tesco Instore Pharmacy Jennison St Bulwell NG6 8EQ Tel. 0115 9809447
MON 08.00-22.30 SAT 06.30-22.00 SUN 11.00-17.00 TUES-FRI 06.30-22.30
Sainsburys Pharmacy Nottingham Road Arnold NG5 6JY Tel. 0115 9264869
MON-FRI 08.00-22.00 SAT 08.00-22.00 SUN 10.00-16.00
Asda Pharmacy Loughborough Rd West Bridgford NG2 7JA Tel. 0115 9694210
MON-FRI 08.00-22.00 SAT 08.00-22.00 SUN 10.00-16.00
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 20 of 26 Date of Issue: 7
th February 2014
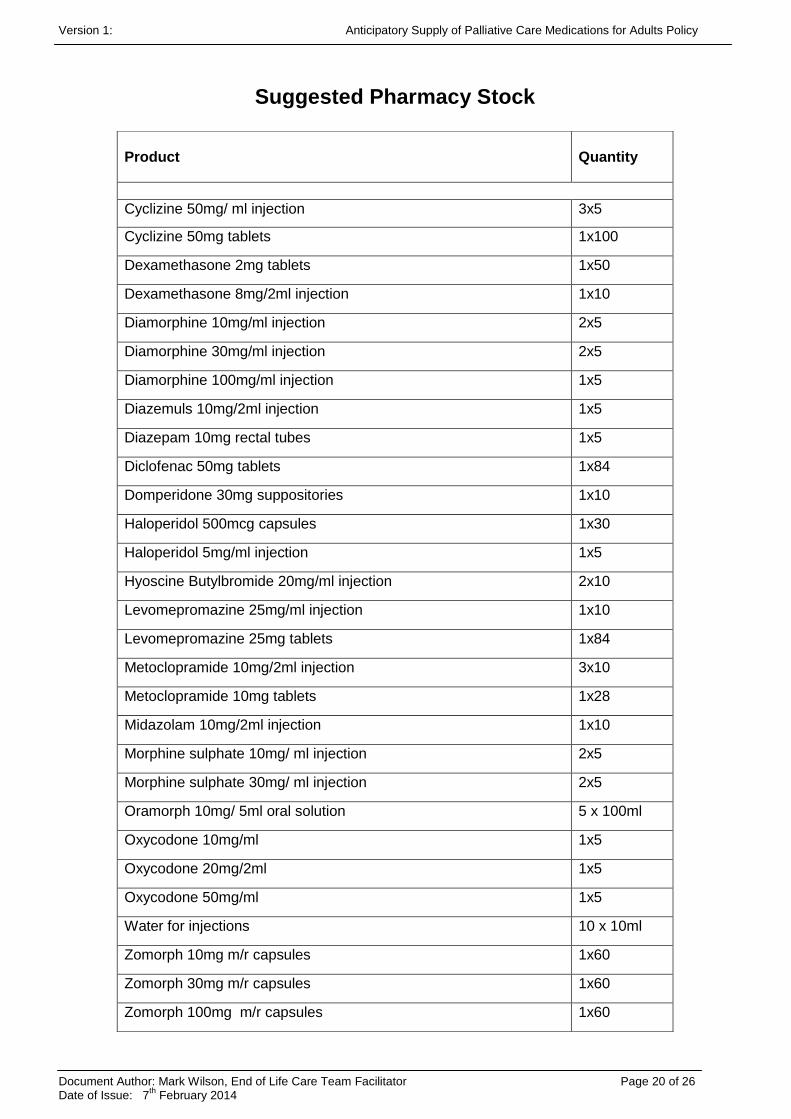
Suggested Pharmacy Stock
Product
Quantity
Cyclizine 50mg/ ml injection 3x5
Cyclizine 50mg tablets 1x100
Dexamethasone 2mg tablets 1x50
Dexamethasone 8mg/2ml injection 1x10
Diamorphine 10mg/ml injection 2x5
Diamorphine 30mg/ml injection 2x5
Diamorphine 100mg/ml injection 1x5
Diazemuls 10mg/2ml injection 1x5
Diazepam 10mg rectal tubes 1x5
Diclofenac 50mg tablets 1x84
Domperidone 30mg suppositories 1x10
Haloperidol 500mcg capsules 1x30
Haloperidol 5mg/ml injection 1x5
Hyoscine Butylbromide 20mg/ml injection 2x10
Levomepromazine 25mg/ml injection 1x10
Levomepromazine 25mg tablets 1x84
Metoclopramide 10mg/2ml injection 3x10
Metoclopramide 10mg tablets 1x28
Midazolam 10mg/2ml injection 1x10
Morphine sulphate 10mg/ ml injection 2x5
Morphine sulphate 30mg/ ml injection 2x5
Oramorph 10mg/ 5ml oral solution 5 x 100ml
Oxycodone 10mg/ml 1x5
Oxycodone 20mg/2ml 1x5
Oxycodone 50mg/ml 1x5
Water for injections 10 x 10ml
Zomorph 10mg m/r capsules 1x60
Zomorph 30mg m/r capsules 1x60
Zomorph 100mg m/r capsules 1x60
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
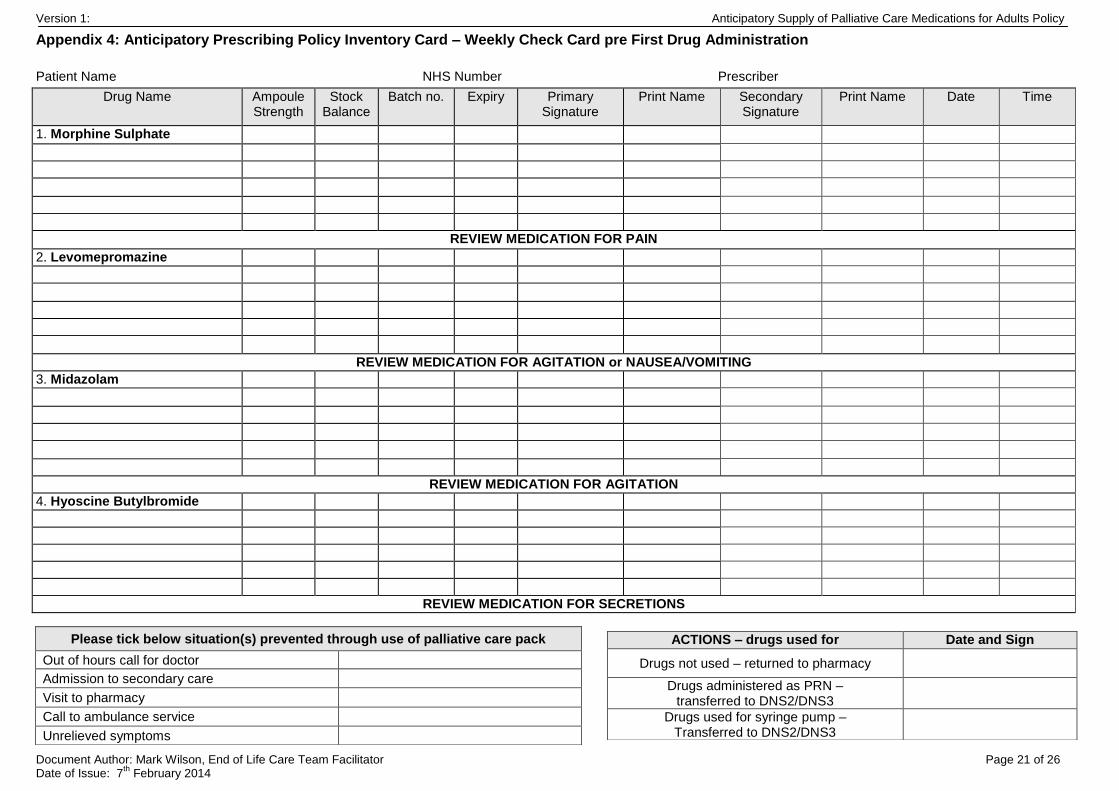
Appendix 4: Anticipatory Prescribing Policy Inventory Card – Weekly Check Card pre First Drug Administration
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 21 of 26 Date of Issue: 7
th February 2014
Patient Name NHS Number Prescriber
Drug Name Ampoule Strength
Stock Balance
Batch no. Expiry Primary Signature
Print Name Secondary Signature
Print Name Date Time
1. Morphine Sulphate
REVIEW MEDICATION FOR PAIN
2. Levomepromazine
REVIEW MEDICATION FOR AGITATION or NAUSEA/VOMITING
3. Midazolam
REVIEW MEDICATION FOR AGITATION
4. Hyoscine Butylbromide
REVIEW MEDICATION FOR SECRETIONS
Please tick below situation(s) prevented through use of palliative care pack
Out of hours call for doctor
Admission to secondary care
Visit to pharmacy
Call to ambulance service
Unrelieved symptoms
ACTIONS – drugs used for Date and Sign
Drugs not used – returned to pharmacy
Drugs administered as PRN – transferred to DNS2/DNS3
Drugs used for syringe pump – Transferred to DNS2/DNS3
Version 1: Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 22 of 26 Date of Issue: 7
th February 2014
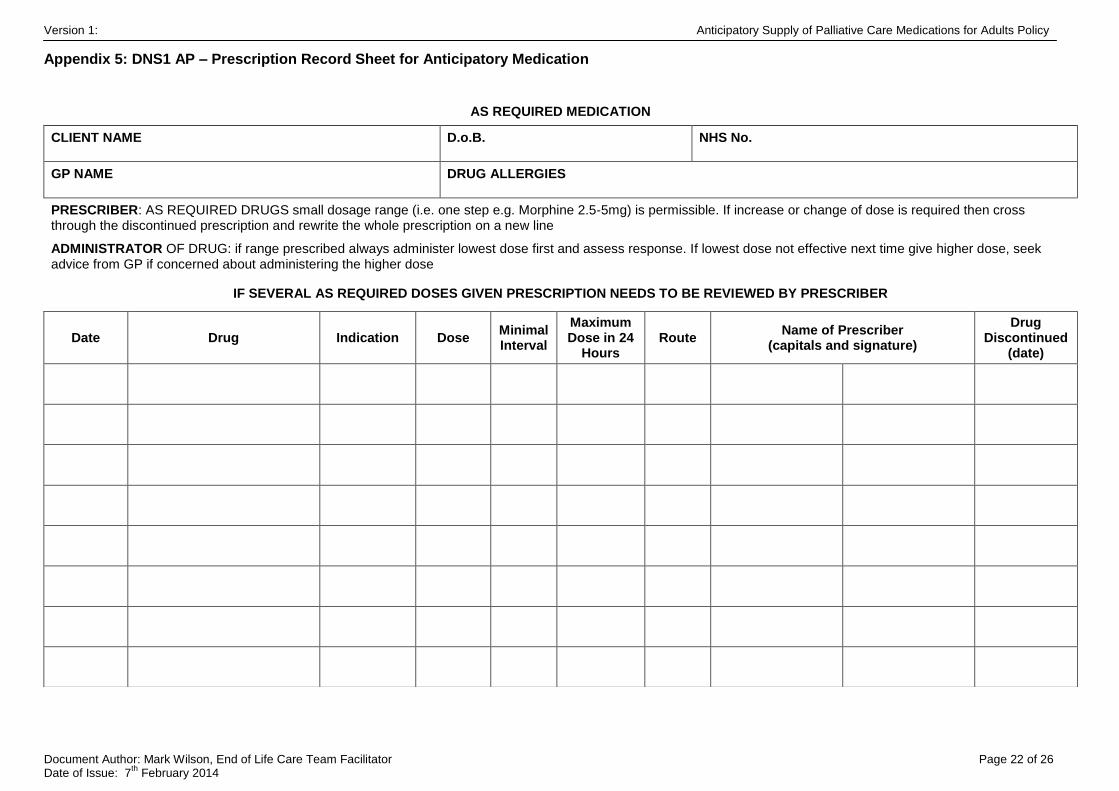
Appendix 5: DNS1 AP – Prescription Record Sheet for Anticipatory Medication
AS REQUIRED MEDICATION
CLIENT NAME D.o.B. NHS No.
GP NAME DRUG ALLERGIES
PRESCRIBER: AS REQUIRED DRUGS small dosage range (i.e. one step e.g. Morphine 2.5-5mg) is permissible. If increase or change of dose is required then cross through the discontinued prescription and rewrite the whole prescription on a new line
ADMINISTRATOR OF DRUG: if range prescribed always administer lowest dose first and assess response. If lowest dose not effective next time give higher dose, seek advice from GP if concerned about administering the higher dose
IF SEVERAL AS REQUIRED DOSES GIVEN PRESCRIPTION NEEDS TO BE REVIEWED BY PRESCRIBER
Date Drug Indication Dose Minimal Interval
Maximum Dose in 24
Hours Route
Name of Prescriber (capitals and signature)
Drug Discontinued
(date)
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 23 of 26 Date of Issue: 7
th February 2014
Appendix 6: General Practitioner/Community Nurse Information Sheet
Anticipatory Supply of Palliative Care Medications General Practitioner/Community Nurse Information
All palliative care patients should be able to achieve a comfortable and dignified death. Often towards the end of life patients cannot swallow oral medication therefore parenteral administration is required via a butterfly as a subcutaneous PRN or syringe pump to control symptoms. This medication needs to be available immediately to the doctor and district nurse making the assessment on a patient’s deterioration. Therefore it is recommended that the regular GP prescribes medication and authorises on the community nursing DNS1 AP form in advance of deterioration and that these drugs are left in the patient’s home.
How do we do this?
1. Write a prescription for the anticipatory palliative medications, that includes:
Morphine Sulphate for pain
Levomepromazine for nausea or agitation
Midazolam for agitation or restlessness
Hyoscine Butylbromide for respiratory secretions
See Anticipatory Supply of Palliative Care Medications policy (appendix 2) for example FP10 prescription for suggested dispensing quantities to last 24-72 hours. This is not a guide for dosages.
2. If patient can no longer swallow oral medications it may be appropriate to stop all oral medications and commence the anticipatory drugs and/or syringe pump as necessary for symptom management
3. If patient is already taking this medication orally then the quantity of medication left in the home needs to be individually converted and reviewed regularly to ensure correct dose available for parenteral subcutaneous administration. For example:
If patient is already on an oral opioid calculate equivalent parenteral subcutaneous quantity and enough for breakthrough doses. Oral Morphine: subcutaneous morphine ratio is 2:1
A PRN dose is approximately 1/6 of the 24 hour daily dose
For example: Oral Morphine Sulphate modified release 60mg BD (120mg/24hr) is approximately equivalent to 60mg Morphine Sulphate injection over 24hr and 10mg Morphine Sulphate injection for each breakthrough dose
4. Breakthrough doses for vomiting, agitation, respiratory secretions and pain need to be written up on the community nursing authorisation sheet DNS1 AP (as the community nurses cannot administer these medications without this documentation)
5. Please ensure Water for Injections are prescribed along with the above medications
6. Please see latest edition of Palliative Care Pocketbook, Palliative Care Formulary or Liverpool Care Pathway symptom control sheets for appropriate doses and dose conversions
7. Explain the purpose of these medications, ask the relatives to collect the medications dispensed and leave them in the house. They should be advised to contact the district nurses as soon as they are in the home of the patient. In exceptional circumstances community staff may collect these medications from the pharmacy
8. Take an Anticipatory Prescribing Pack container (grey box) to the house. The nurse will then check and sign in the medications using the Inventory Card, they should also be written on the DNS2 and DNS3. Please note earliest expiry date of contents to ensure they can be administered when required
9. To ensure the pack is utilised to the maximum it is advisable to include e.g. Palliative Care Pocketbook, Liverpool Care Pathway, Spare medication documents (DNS1 AP, DNS2, DNS3 etc), Butterflies (winged infusion sets), a sample of slip syringes (1ml and 2ml), needles and transparent dressing
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 24 of 26 Date of Issue: 7
th February 2014
10. For all patients Inform out of hours providers: NEMS via the special patient note information form and the Evening and Night service by telephone and/or fax, that anticipatory medications have been prescribed and are in the home of the patient
11. When the medications are required for patient administration, ensure administration and electronic records are updated.
12. Ideally the medications should be reviewed on a monthly basis to ensure: the doses are still appropriate; they are still required and the medications are still in date.
13. After the patient has died, ask the patient’s relatives/carers to return unused medication to the pharmacy, The nurses should collect the grey box for re-use as per the Policy.
Common questions:
Is this not a waste of medication?
The total cost of the initial supply of anticipatory medications in an opioid naive patient is approx. £30. This is a good use of money if it means a patient is able to achieve a dignified and comfortable death at home, if that is their place of choice. The cost of unproductive emergency admissions for dying patients with uncontrolled symptoms outweighs the cost of unused medications.
Will the medication be open to abuse?
A risk assessment must be completed to ensure there are no risks regarding known drug misusers or person with a mental health condition at risk of self harm who have access to the patient’s home. Decisions must be made by the multi-disciplinary team if it is appropriate to provide the Anticipatory Prescribing Pack when a known drug misuser has access to a patient’s home.
Will pharmacists have this medication in stock?
Pharmacists are being educated about anticipatory prescribing. If your local pharmacy is not regularly making this medication available then try one of the dedicated pharmacies that are stocking palliative care medications (see Policy Appendix 3)
What if my patient is well controlled on oral anti-emetic e.g. Cyclizine or Metoclopramide for vomiting do I need to prescribe Levomepromazine instead?
If patient is achieving good symptom relief on a particular medication then yes prescribe parenteral Cyclizine/Metoclopramide in anticipation. However, the situation may arise if parenteral Cyclizine is not controlling symptoms that conversion to Levomepromazine may be necessary.
What conversion ratios should I be using in converting from oral morphine to subcutaneous opioids?
Dose conversions vary between patients and careful monitoring during conversion is required to avoid insufficient or excessive dosing. Please see latest edition of Palliative Care Pocketbook, Palliative Care Formulary for dose conversion details.
Breakthrough (PRN) doses are 1/6 of the total 24h dose of opioid.
What should I do when my patient is on an opioid based transdermal patch?
It is generally difficult to titrate back from a patch to either oral or parenteral opioids, therefore it is advised to continue to transdermal patch as prescribed and supplement with subcutaneous PRN medications as required.
Further Information:
The latest versions of the Palliative Care Formulary and Palliative Care Pocketbook provide the most relevant medication and symptom management guidelines for this policy For further advice contact: Hayward House Specialist Palliative Care (Nottingham City Hospital) 24 hours a day 0115 9627619 Nottingham CityCare End of Life Care Team Monday to Friday office based hours 0115 8834787
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 25 of 26 Date of Issue: 7
th February 2014
Appendix 7: Pharmacist Information Sheet
Anticipatory Supply of Palliative Care Medications
Pharmacist Information
Patients in the last few weeks of may require a subcutaneous medication/syringe pump to control symptoms in their final days. It can be difficult to access parenteral medication quickly. Nottingham CityCare Partnership have an Anticipatory Supply of Palliative Care Medications policy to ensure there is a process for this.
To ensure that patients have their symptoms controlled in a timely manner GPs in the area are prescribing medication in anticipation of a patient’s deterioration. The medication remains in the patient’s home (including care homes) until required.
The Four most common symptoms at the end of life are pain, nausea and vomiting, agitation and respiratory tract secretions. The drugs used to control these symptoms are:
Morphine for pain and breathlessness
Levomepromazine for sickness and restlessness
Midazolam for restlessness
Hyoscine Butylbromide for secretions in the throat
Within the Anticipatory Supply of Palliative Care Medications policy there is an example FP10 (appendix 2) to supply these medications. It is important that these prescriptions are correctly written, please consider the following:
The GP’s have written the exact dose required on the FP10 and they should also state that the medications are ‘in anticipation’ of specific symptom for each of the medications prescribed
Within the update of the policy prescribing of single step ranges is being advocated for Morphine, Levomepromazine and Midazolam
E.g. Morphine Sulphate 2.5-5mg In Anticipation of Pain
The medications cannot be administered without Water for Injection, so an adequate supply needs to be provided with the medications
Patients/carers must tell the District Nursing teams that they have these medications, as they have to check them before they can be used
Please ask relatives/carers to return the medication to the local pharmacy when it is no longer required (nurses will also advocate this practice)
It would be advantageous if this medication is part of pharmacy routine stock so it can be dispensed promptly (see below)
Several pharmacies within Nottingham CityCare have now signed up to the Community pharmacy palliative care drugs scheme. This scheme has been set up to ensure minimum stock levels of the most commonly used palliative care medications. A list of these pharmacies is in the Anticipatory Supply of Palliative Care Medications policy (appendix 3).
Version 2.0 Anticipatory Supply of Palliative Care Medications for Adults Policy
Document Author: Mark Wilson, End of Life Care Team Facilitator Page 26 of 26 Date of Issue: 7
th February 2014
Version History
Version Date Status Comment
Version 1
This was a Citihealth Policy
01.01.2009 Final Policy review date expired. First update of this policy required, changes made to mirror evolvement of practice since initial implementation
D0.1 08.11.2012 Policy been to QAF and changes implemented. Some changes made at request of medicines management team prior to going to Patient Safety
V2.0 18.12.2012 Policy ratified at Patient Safety Committee.
Change Control Record
Date Version Section Changes made







![Akram, Gazala and Corcoran, Emma Dunlop and MacRobbie ... · Palliative care is increasingly delivered in the community setting [1–3]. However a lack of forward or anticipatory](https://static.fdocuments.net/doc/165x107/5ec68c450cb82c436f0419c0/akram-gazala-and-corcoran-emma-dunlop-and-macrobbie-palliative-care-is-increasingly.jpg)