Antianginal Drug Class Review - Utah Medicaid 1. Antianginal Therapies ... Sublingual nitroglycerin...
22
Drug Class Review Antianginal Agents 24:12.08 Nitrates and Nitrites 24:04.92 Cardiac Drugs, Miscellaneous Amyl Nitrite Isosorbide Dinitrate (IsoDitrate ER®, others) Isosorbide Mononitrate (Imdur®) Nitroglycerin (Minitran®, Nitrostat®, others) Ranolazine (Ranexa®) Final Report May 2015 Review prepared by: Melissa Archer, PharmD, Clinical Pharmacist Carin Steinvoort, PharmD, Clinical Pharmacist Gary Oderda, PharmD, MPH, Professor University of Utah College of Pharmacy Copyright © 2015 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved.
Transcript of Antianginal Drug Class Review - Utah Medicaid 1. Antianginal Therapies ... Sublingual nitroglycerin...
Drug Class Review
Antianginal Agents 24:12.08 Nitrates and Nitrites
24:04.92 Cardiac Drugs, Miscellaneous
Amyl Nitrite Isosorbide Dinitrate (IsoDitrate ER®, others)
Isosorbide Mononitrate (Imdur®) Nitroglycerin (Minitran®, Nitrostat®, others)
Ranolazine (Ranexa®)
Final Report May 2015
Review prepared by: Melissa Archer, PharmD, Clinical Pharmacist Carin Steinvoort, PharmD, Clinical Pharmacist Gary Oderda, PharmD, MPH, Professor University of Utah College of Pharmacy Copyright © 2015 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved.

2
Table of Contents
Executive Summary ......................................................................................................................... 3 Introduction .................................................................................................................................... 4 Table 1. Antianginal Therapies .............................................................................................. 4 Table 2. Summary of Agents .................................................................................................. 5 Disease Overview ........................................................................................................................ 8 Table 3. Summary of Current Clinical Practice Guidelines .................................................... 9 Pharmacology ............................................................................................................................... 10 Table 4. Pharmacokinetic Properties of the Antianginal Agents ......................................... 11 Methods ........................................................................................................................................ 13 Clinical Efficacy .............................................................................................................................. 13 Adverse Drug Reactions ................................................................................................................ 14 Table 5. Drug‐Drug Interactions Reported with the Antianginal Therapies ........................ 14 Table 6. Adverse Events Reported with Antianginal Therapies ........................................... 15 References .................................................................................................................................... 17

3
Executive Summary
Introduction: A number of therapies are available for the treatment of angina, including:
beta-blockers, calcium channel blockers, nitrates and a number of miscellaneous vasodilation agents. Four nitrates are currently available for use in the United States: amyl nitrite, isosorbide dinitrate, isosorbide mononitrate and nitroglycerin. Ranolazine is a newer agent with a unique mechanism of action which may also be used in the treatment and prevention of chronic angina. Sublingual nitroglycerin is used to treat an angina attack and the long-acting nitrates (transdermal and extended release nitroglycerin, isosorbide mononitrate, isosorbide dinitrate) are used for prophylaxis of angina.
Ischemic heart disease is one of the most frequently reported cardiovascular diseases in
the US and angina pectoris is the most common symptom of ischemic heart disease. ACCF/AHA Guidelines for patients with Stable Ischemic Heart Disease recommend beta-blockers with or without short-acting sublingual nitroglycerin as first-line treatment. The long-acting nitrates and ranolazine may be considered second-line or add-on options in patients who are not able to tolerate beta-blockers or who require additional therapy to control angina. The nitrates and ranolazine may also be used in the treatment of unstable angina and angina associated with heart failure or myocardial infarction.
Clinical Efficacy: No comparative clinical evidence is available for the antianginal therapies. When compared to placebo, the agents demonstrate efficacy in reducing the severity and frequency of angina episodes. Clinical evidence comparing the agents to other therapies (such as beta-blockers and calcium channel blockers) suggests the agents have similar rates of safety and efficacy.
Adverse Drug Reactions: The most common adverse events reported with nitrate therapy are headache and flushing. Nitrate tolerance may develop with continuous nitrate therapy and can be avoided or overcome with daily nitrate-free intervals ranging from 12-14 hours, depending on dosage form. Ranolazine is not associated with the development of tolerance. The most common adverse events reported with ranolazine therapy are dizziness, headache and gastrointestinal upset. Ranolazine is also associated with dose-related increases in the QT interval and should not be used in patients who are at an increased risk of developing QT prolongation.
Summary: In general, the antianginal agents appear to have similar rates of efficacy and are generally well tolerated. Development of tolerance and dosing recommendations vary between the agents. Pharmacokinetic factors, in addition to guideline recommendations, should be used when selecting an agent and mode of therapy with the antianginal therapies.

4
Introduction
A number of therapies are available for the treatment of angina, including: beta-blockers, calcium channel blockers, nitrates and a number of miscellaneous vasodilation agents. This report will include a review of the nitrates currently available for use in the United States: amyl nitrite, isosorbide dinitrate, isosorbide mononitrate, nitroglycerin and ranolazine. The agents included in this review are available in oral, inhalation and injectable formulations and are used variably, depending on severity of disease and concurrent pharmacotherapies. Table 1 provides a summary of all therapies used in the treatment of angina and Table 2 provides a summary of the agents included in this drug class review. Table 1. Antianginal Therapies1,2 Drug Class Indicated
Products Route of Administration
Labeled Uses Generic Available
Beta‐blockers Atenolol Metoprolol Nadolol Propranolol
IntravenousOral
All agents: Treatment of hypertension, alone or in combination with other agents; management of angina pectoris. Atenolol, Metoprolol, Propranolol: Secondary prevention postmyocardial infarction. Propranolol: Management of pheochromocytoma; essential tremor; supraventricular arrhythmias, ventricular tachycardias; migraine headache prophylaxis; hypertrophic subaortic stenosis; proliferating infantile hemangioma.
Yes
Calcium Channel Blockers
Amlodipine Diltiazem Nicardipine Nifedipine Verapamil
IntravenousOral
All agents: Treatment of hypertension; angina pectoris Verapamil: Treatment of supraventricular tachyarrhythmia (PSVT, atrial fibrillation/flutter [rate control])
Yes
Nitrates Amyl Nitrite Isosorbide Dinitrate Isosorbide Mononitrate Nitroglycerin
InhalationIntravenous Oral Rectal Topical
Treatment of angina pectoris
Yes
Miscellaneous Vasodilator
Ranolazine Oral Treatment of chronic angina No

5
Table 2. Summary of Agents1,2 Drug Class Available
Formulations Uses Dose Range, Adult Dose Range,
Pediatric Clinical Notes Generic
Available
Amyl Nitrite Liquid, for inhalation: USP: 85%‐103% (0.3 mL)
Labeled: Coronary vasodilator in angina pectoris Off‐label: Cyanide toxicity; Production of changes in the intensity of heart murmurs; Provocation of latent left ventricular outflow tract (LVOT) gradient during echocardiography in patients with hypertrophic cardiomyopathy (HCM)
Angina: 2‐6 nasal inhalations from 1 crushed ampule; may repeat in 3‐5 minutes Cyanide toxicity (off‐label use): 0.3 mL ampule crushed into a gauze pad and placed in front of the patient’s mouth to inhale over 15‐30 seconds; repeat every minute until sodium nitrite can be administered
Not currently labeled for use in pediatric patients Cyanide toxicity (off‐label use): Refer to adult dosing
Given the widespread use of newer nitrate compounds, the use of amyl nitrite for patients experiencing angina pectoris has fallen out of favor
Yes
Isosorbide Dinitrate (Dilatrate‐SR; IsoDitrate ER; Isordil Titradose)
Oral Capsule, ER (Dilatrate‐SR®): 40 mg Oral Tablet (generic): 5 mg, 10 mg, 20 mg, 30 mg Oral Tablet, ER (generic): 40 mg Oral Tablet, sublingual (generic): 2.5 mg [DSC]
Labeled: Prevention of angina pectoris Off‐label: Heart failure with reduced ejection fraction; Esophageal spastic disorders
Immediate release: Initial: 5‐20 mg 2‐3 times daily; Maintenance: 10‐40 mg 2‐3 times daily or 5‐80 mg 2‐3 times daily Sustained release: 40‐160 mg/day with nitrate free interval of >18 hours is recommended or 40 mg 1‐2 times daily; Maximum dose: 160 mg/day Sublingual: 5‐10 mg every 2‐4 hours for prophylaxis of acute angina; may supplement with 5‐10 mg prior to activities which may provoke an anginal episode
Not currently labeled for use in pediatric patients
Due to slower onset of action, not the drug of choice for acute anginal episode
Product dependent
Isosorbide Mononitrate (Imdur)
Oral Tablet (generic): 10 mg, 20 mg Oral Tablet, ER (generic): 30mg, 60 mg, 120 mg
Prevention of angina pectoris Immediate release: 5‐20 mg twice daily with the 2 doses given 7 hours apart (eg, 8 AM and 3 PM) to decrease tolerance development Extended release: 30‐60 mg given once daily in the morning; titrate upward as needed, giving at least 3 days between increases; maximum daily single dose: 240 mg
Not currently labeled for use in pediatric patients
Tolerance to nitrate effects develops with chronic exposure; dose escalation does not overcome this effect, tolerance can only be overcome by short periods of nitrate absence from the body
Yes
6
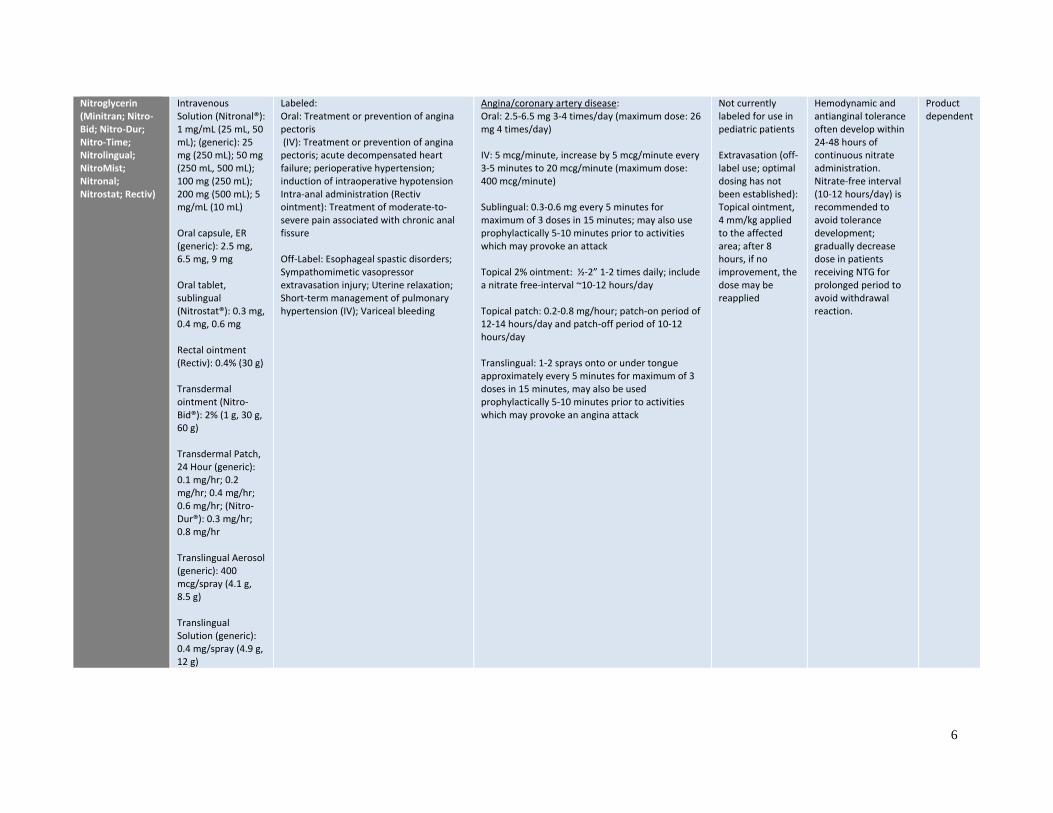
Nitroglycerin (Minitran; Nitro‐Bid; Nitro‐Dur; Nitro‐Time; Nitrolingual; NitroMist; Nitronal; Nitrostat; Rectiv)
Intravenous Solution (Nitronal®): 1 mg/mL (25 mL, 50 mL); (generic): 25 mg (250 mL); 50 mg (250 mL, 500 mL); 100 mg (250 mL); 200 mg (500 mL); 5 mg/mL (10 mL) Oral capsule, ER (generic): 2.5 mg, 6.5 mg, 9 mg Oral tablet, sublingual (Nitrostat®): 0.3 mg, 0.4 mg, 0.6 mg Rectal ointment (Rectiv): 0.4% (30 g) Transdermal ointment (Nitro‐Bid®): 2% (1 g, 30 g, 60 g) Transdermal Patch, 24 Hour (generic): 0.1 mg/hr; 0.2 mg/hr; 0.4 mg/hr; 0.6 mg/hr; (Nitro‐Dur®): 0.3 mg/hr; 0.8 mg/hr Translingual Aerosol (generic): 400 mcg/spray (4.1 g, 8.5 g) Translingual Solution (generic): 0.4 mg/spray (4.9 g, 12 g)
Labeled: Oral: Treatment or prevention of angina pectoris (IV): Treatment or prevention of angina pectoris; acute decompensated heart failure; perioperative hypertension; induction of intraoperative hypotension Intra‐anal administration (Rectiv ointment): Treatment of moderate‐to‐severe pain associated with chronic anal fissure Off‐Label: Esophageal spastic disorders; Sympathomimetic vasopressor extravasation injury; Uterine relaxation; Short‐term management of pulmonary hypertension (IV); Variceal bleeding
Angina/coronary artery disease: Oral: 2.5‐6.5 mg 3‐4 times/day (maximum dose: 26 mg 4 times/day) IV: 5 mcg/minute, increase by 5 mcg/minute every 3‐5 minutes to 20 mcg/minute (maximum dose: 400 mcg/minute) Sublingual: 0.3‐0.6 mg every 5 minutes for maximum of 3 doses in 15 minutes; may also use prophylactically 5‐10 minutes prior to activities which may provoke an attack Topical 2% ointment: ½‐2” 1‐2 times daily; include a nitrate free‐interval ~10‐12 hours/day Topical patch: 0.2‐0.8 mg/hour; patch‐on period of 12‐14 hours/day and patch‐off period of 10‐12 hours/day Translingual: 1‐2 sprays onto or under tongue approximately every 5 minutes for maximum of 3 doses in 15 minutes, may also be used prophylactically 5‐10 minutes prior to activities which may provoke an angina attack
Not currently labeled for use in pediatric patients Extravasation (off‐label use; optimal dosing has not been established): Topical ointment, 4 mm/kg applied to the affected area; after 8 hours, if no improvement, the dose may be reapplied
Hemodynamic and antianginal tolerance often develop within 24‐48 hours of continuous nitrate administration. Nitrate‐free interval (10‐12 hours/day) is recommended to avoid tolerance development; gradually decrease dose in patients receiving NTG for prolonged period to avoid withdrawal reaction.
Product dependent

7
Ranolazine (Ranexa®)
Oral Tablet ER, 12 Hour: 500 mg, 1000 mg
Treatment of chronic angina 500 mg twice daily; may increase to 1000 mg twice daily as needed; maximum: 1000 mg twice daily
Not currently labeled for use in pediatric patients
Ranolazine dose should not exceed 500 mg twice daily when given concurrently with diltiazem, erythromycin, fluconazole, verapamil and other moderate CYP3A inhibitors Ranolazine dose should be titrated to clinical response when used concurrently with P‐glycoprotein inhibitors (eg, cyclosporine)
No
Key: ER = extended release, DSC = discontinued, IV = intravenous
8
Disease Overview
Cardiovascular diseases are the most common causes of death in the United States and are rapidly growing problems throughout the world.3-12 Diseases included in this category are hypertension, congestive heart failure, ischemic heart disease, stroke and peripheral arterial disease. A sedentary lifestyle, unhealthy diet, tobacco use and alcohol abuse are some of the risk factors for developing a cardiovascular disease. According to the American Heart Association, each day over 2000 Americans will die of a cardiovascular disease (averaging one death every 39 seconds) and each year nearly 800,000 Americans will experience a stroke (averaging one cerebrovascular accident every 40 seconds). Therapeutic approaches to prevent cardiovascular disease include lifestyle modification (weight reduction, physical activity, smoking cessation), blood pressure control, fluid management, lipid-lowering treatment, and use of antiplatelet and antithrombotic agents.3-9
Ischemic heart disease is a condition defined as a reduced blood supply to the
heart.13-15 Cardiac ischemia is caused by atherosclerosis, or hardening of the arteries, and can result in angina, heart attack and death. In developed countries, ischemic heart disease is one of the most frequently reported cardiovascular diseases and causes of death. Angina pectoris is the most common symptom of ischemic heart disease and is characterized as chest pain which results from an imbalance in the coronary vessels where the oxygen demand in the heart is greater than the oxygen supplied to the heart. The pain may be mild or intense and feel like a crushing, burning, or squeezing discomfort that can spread to the neck or arms. Typically, the pain lasts for 5-10 minutes and is relieved with sublingual nitroglycerin. Angina pectoris is divided into three types: secondary angina, or effort angina, wherein inadequate blood flow during exercise or times of stress results in chest pain; primary angina, or variant angina, wherein the ischemia causes spasm of the coronary vessels and chest pain without increases in cardiac demand; and unstable angina wherein a sudden worsening of the patients chronic angina occurs.13-15 All types of angina demonstrate the same characteristic chest pains and are relieved with the administration of nitroglycerin.
As mentioned, nitroglycerin is commonly used to treat chest pain associated with
ischemic heart disease. Nitroglycerin is an organic nitrate and considered the standard treatment for immediate relief of angina. Overall, three drug classes are typically used in the treatment and prevention of angina: organic nitrates, calcium channel blockers and beta-blockers.14,15 Each of these therapeutic drug classes reduce myocardial oxygen requirements by decreasing heart rate, blood pressure and/or contractility. Sublingual nitroglycerin is used to treat an angina attack. Calcium channel blockers, beta-blockers and long-acting nitrates (transdermal and extended release nitroglycerin, isosorbide mononitrate, isosorbide dinitrate) are used for prophylaxis of angina. Ranolazine is a newer agent with a unique mechanism of action which may also be used in the treatment and prevention of chronic angina. According to the 2012 Guidelines for Patients with Stable Ischemic Heart Disease16, beta-blockers with or without short-acting sublingual nitroglycerin is recommended as first-line treatment.16 The long-acting nitrates, calcium channel blockers and ranolazine are considered second-line or add-on options in patients

9
who are not able to tolerate beta-blockers or who require additional therapy to control angina.16 The nitrates and ranolazine may also be used in the treatment of unstable angina and angina associated with heart failure or myocardial infarction. Table 3 provides a summary of the current clinical guideline recommendations for treatment of angina.
Table 3. Summary of Current Clinical Practice Guidelines
Guideline Treatment Recommendations
ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 201216
Recommendations: First‐line: β‐blockers + short‐acting sublingual nitrates prn Second‐line: long‐acting nitrates, calcium channel blockers, ranolazine Add‐on: β‐blockers + long‐acting nitrates, calcium channel blockers, ranolazine
Institute for Clinical Systems Improvement (ICSI): Stable Coronary Artery Disease, 201317
Recommendations: Daily aspirin (81‐162 mg) Patients with mild, stable CAD and angina: First‐line: β‐blockers + short‐acting sublingual nitrates prn Second‐line: long‐acting nitrates Third‐line: calcium channel blockers Last line: ranolazine Add‐on: β‐blockers + long‐acting nitrates Second‐line add‐on: β‐blockers + calcium channel blockers
ACCF/AHA Guideline for the Management of Heart Failure, 201318
African Americans with NYHA class III–IV HFrEF: Combination of hydralazine and isosorbide dinitrate with ACE inhibitors and beta blockers
ACCF/AHA guideline for the management of ST‐elevation myocardial infarction, 201319
Intravenous nitroglycerin may be useful to treat patients with STEMI and hypertension or heart failure There is no role for the routine use of oral nitrates in the convalescent phase of STEMI
Guidelines for the Management of Patients With Unstable Angina/Non–ST‐Elevation Myocardial Infarction, 201220
Patients with UA/NSTEMI: First‐line: beta‐blocker and ace inhibitor Second‐line or add‐on: calcium channel blocker, angiotensin receptor blocker Patients with UA/NSTEMI and ongoing ischemic discomfort: sublingual NTG (0.4 mg) every 5 min for a total of 3 doses intravenous NTG is indicated in the first 48 h for treatment of persistent ischemia, heart failure or hypertension
AHA/ACC Guideline for the Management of Patients With Non–ST‐Elevation Acute Coronary Syndromes, 201421
Patients with NSTE‐ACS: First‐line: aspirin, beta‐blocker (sustained‐release metoprolol succinate, carvedilol or bisoprolol, ace inhibitor, high‐intensity statin, anticoagulation Second‐line: calcium channel blocker (verapamil or diltiazem), clopidogrel or ticagrelor Patients with NSTE‐ACS continuing ischemic pain: sublingual nitroglycerin (0.3‐0.4 mg) every 5 minutes for up to 3 doses intravenous nitroglycerin for patients with persistent ischemia, heart failure or hypertension
Key: prn‐ as needed; CAD‐ coronary artery disease; HFrEF ‐ heart failure with reduced ejection fraction; STEMI ‐ ST segment elevation myocardial infarction; NTG ‐ nitroglycerin; UA/NSTEMI ‐ Unstable Angina/Non‐ST‐ Segment Elevation myocardial infarction; NSTE‐ACS ‐ non–ST‐elevation acute coronary syndromes
10
Pharmacology
Organic nitrates are simple nitric and nitrous acid esters of polyalcohols.2,22,23 Nitroglycerin is considered the prototype but all of the agents have a similar mechanism of action.14,15 Nitrates form a free radical, nitric oxide, which activates guanylate cyclase in smooth muscle and causes myosin (MYLK) dephosphorylation, resulting in:
Relaxation of smooth muscle Vasodilation of the peripheral veins (primarily) and arteries Dilation of coronary arteries Reduction of cardiac oxygen demand by decreasing preload (left ventricular end-diastolic
pressure) Modest reduction of afterload Improvement of collateral flow to ischemic regions
Tolerance may develop with continuous nitrate therapy.14,15 The development of nitrate
tolerance is not fully understood but may result from activation of a neurohormonal mechanism, expansion of plasma volume, production of super oxide, from abnormalities in biotransformations of nitrates or nitric oxide signaling mechanisms. Nitrate tolerance may be avoided or overcome by daily nitrate-free intervals ranging from 12-14 hours for most long-acting nitrates, depending on the dosage form. The addition of hydralazine to the nitrate product may help to improve efficacy and reduce the development of tolerance.14,15
Amyl Nitrate: With the widespread use and proven efficacy for nitroglycerin and isosorbide,
the use of amyl nitrite for angina pectoris is not generally recommended. Amyl nitrate may be used in the treatment of cyanide poisoning and works by binding to the cyanide ion to form cyanomethemoglobin which results in release of the cytochrome oxidase and allows aerobic metabolism to continue.2,22
Isosorbide: The isosorbide agents are indicated in the prevention of angina pectoris and are not generally the agent of choice for acute angina episodes due to the slower onset of action (30-60 minutes). Isosorbide is available in a dinitrate or mononitrate formulation, which is simply the active metabolite of isosorbide dinitrate. Both formulations are given once daily (with the extended release agents) or 2-3 times daily (with the immediate release formulations). Tolerance can be avoided by short periods of nitrate-free intervals (10-12 hours/day).2,22
Nitroglycerin: The conventional sublingual tablet form of nitroglycerin offers relief within 1-5 minutes and should not be chewed, crushed, or swallowed as the onset of action is quicker when absorbed through the lining of the mouth. The sublingual tablets are stored in tightly closed glass containers as the tablets can lose potency through volatilization and adsorption to plastic surfaces. Nitroglycerin is also available as an translingual spray and IV formulation for immediate relief as well as an extended release tablet and transdermal patch for prevention of angina. To avoid the development of tolerance, the transdermal patch requires a daily 10 hour nitrate-free period and the extended release product should be dosed with an 18 hour nitrate-free period daily. When used in the treatment of rectal fissures, topical nitroglycerin cream works by decreasing sphincter tone and intra-anal pressure.2,22
11
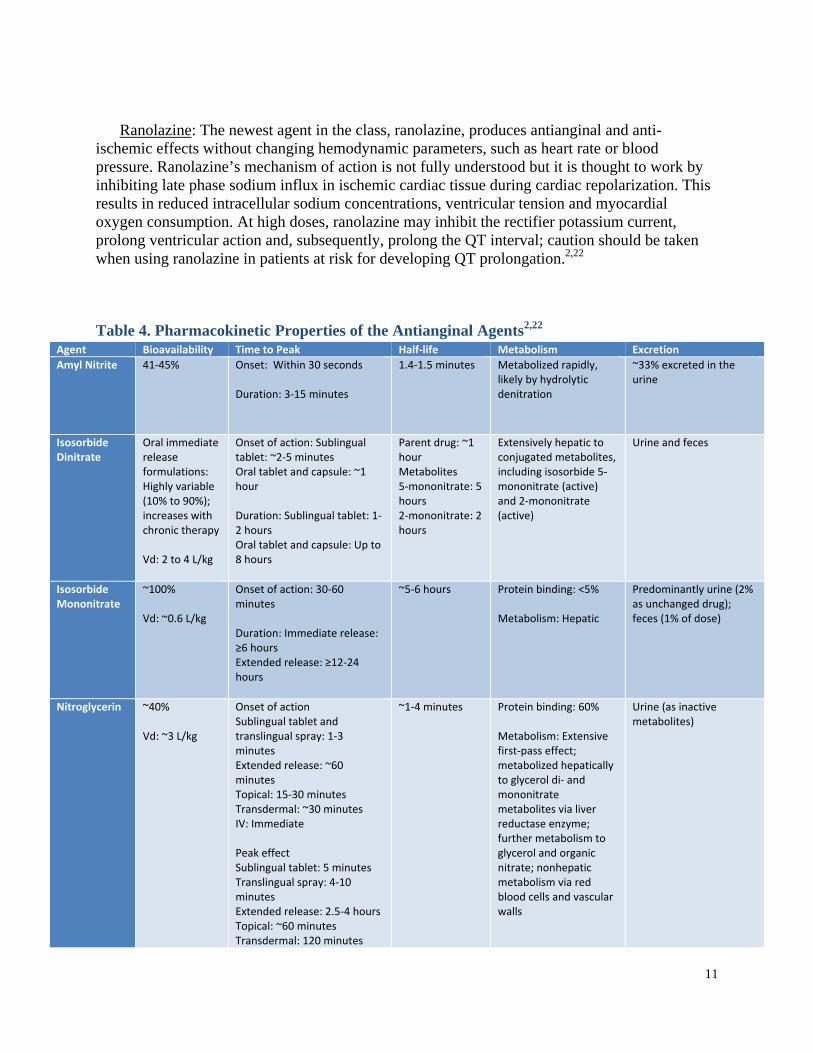
Ranolazine: The newest agent in the class, ranolazine, produces antianginal and anti-ischemic effects without changing hemodynamic parameters, such as heart rate or blood pressure. Ranolazine’s mechanism of action is not fully understood but it is thought to work by inhibiting late phase sodium influx in ischemic cardiac tissue during cardiac repolarization. This results in reduced intracellular sodium concentrations, ventricular tension and myocardial oxygen consumption. At high doses, ranolazine may inhibit the rectifier potassium current, prolong ventricular action and, subsequently, prolong the QT interval; caution should be taken when using ranolazine in patients at risk for developing QT prolongation.2,22
Table 4. Pharmacokinetic Properties of the Antianginal Agents2,22 Agent Bioavailability Time to Peak Half‐life Metabolism Excretion
Amyl Nitrite
41‐45% Onset: Within 30 seconds Duration: 3‐15 minutes
1.4‐1.5 minutes Metabolized rapidly, likely by hydrolytic denitration
~33% excreted in the urine
Isosorbide Dinitrate
Oral immediate release formulations: Highly variable (10% to 90%); increases with chronic therapy Vd: 2 to 4 L/kg
Onset of action: Sublingual tablet: ~2‐5 minutes Oral tablet and capsule: ~1 hour Duration: Sublingual tablet: 1‐2 hours Oral tablet and capsule: Up to 8 hours
Parent drug: ~1 hour Metabolites 5‐mononitrate: 5 hours 2‐mononitrate: 2 hours
Extensively hepatic to conjugated metabolites, including isosorbide 5‐mononitrate (active) and 2‐mononitrate (active)
Urine and feces
Isosorbide Mononitrate
~100% Vd: ~0.6 L/kg
Onset of action: 30‐60 minutes Duration: Immediate release: ≥6 hours Extended release: ≥12‐24 hours
~5‐6 hours Protein binding: <5% Metabolism: Hepatic
Predominantly urine (2% as unchanged drug); feces (1% of dose)
Nitroglycerin ~40% Vd: ~3 L/kg
Onset of action Sublingual tablet and translingual spray: 1‐3 minutes Extended release: ~60 minutes Topical: 15‐30 minutes Transdermal: ~30 minutes IV: Immediate Peak effect Sublingual tablet: 5 minutes Translingual spray: 4‐10 minutes Extended release: 2.5‐4 hours Topical: ~60 minutes Transdermal: 120 minutes
~1‐4 minutes Protein binding: 60% Metabolism: Extensive first‐pass effect; metabolized hepatically to glycerol di‐ and mononitrate metabolites via liver reductase enzyme; further metabolism to glycerol and organic nitrate; nonhepatic metabolism via red blood cells and vascular walls
Urine (as inactive metabolites)

12
Key: IV‐intravenous, HTN‐ hypertension, CYP‐ cytochrome P450
IV: Immediate Duration Sublingual tablet and translingual spray: >25 minutes Extended release: 4‐8 hours Topical: 7 hours Transdermal: 10‐12 hours IV: 3‐5 minutes
Ranolazine 76% Time to peak: 2‐5 hours 7 hours Metabolites (activity undefined): 6‐22 hours
Protein binding: ~62% Metabolism: Extensive; Hepatic via CYP3A (major) and 2D6 (minor); intestines
Primarily urine (75% mostly as metabolites; <5% as unchanged drug); feces (25% mostly as metabolites; <5% as unchanged drug)
13
Methods
A literature search was conducted to identify articles evaluating the antianginal agents,
searching the MEDLINE database (1950 – 2014), the Cochrane Library, and reference lists of review articles. For the clinical efficacy section, only clinical trials published in English, evaluating the comparative efficacy of the antianginal agents are included. Trials evaluating the agents as monotherapy or combination therapy where adjunctive medications remained constant throughout the trial are included. Noncomparative trials and trials comparing monotherapy with combination regimens are excluded. The following reports were excluded (note: some were excluded for more than 1 reason):24-31
Individual clinical trials which evaluated endpoints other than reduction of symptoms, such
as pharmacokinetics, pharmacodynamics, pharmacoeconomics or other outcomes unrelated to reduction of symptoms.32-42
Individual trials comparing the agents in dose-finding43-51 and placebo-controlled studies51-55 or in healthy volunteers.39,56
Individual clinical trials evaluating agents or formulations not currently available in the US or clinical trials without access to the full article.57-63
Clinical Efficacy
The efficacy of the antianginal agents has not been directly compared in any comparative clinical trials or meta-analyses. The agents have been studied in the prevention or treatment of angina in a number of placebo-controlled trials. Trials comparing the safety and efficacy of the agents with other therapies, including beta-blockers and calcium channel blockers, are also available. In a recent review of nitrates for acute heart failure syndromes (2013)64, no significant differences in efficacy were reported between nitrate vasodilator therapy and alternative interventions (furosemide and morphine, furosemide alone, hydralazine, beta-blockers, intravenous nesiritide and placebo). According to the systemic review, nitrate therapy may be associated with a lower incidence of adverse effects but no differences in symptom relief or hemodynamic variables were demonstrated. Ranolazine has been directly compared to calcium channel blocking therapy (amlodipine), beta-blocker therapy (atenolol) and placebo and demonstrated statistically significant improvements in exercise stress test parameters, reduced angina frequency and nitroglycerin use compared with placebo.65,66 In general, the antianginal agents demonstrate efficacy in reducing the severity and frequency of angina episodes.

14
Adverse Drug Reactions
The antianginal agents are generally well-tolerated. The most common adverse events reported with nitrate therapy include headache and flushing.2,22 Hypotension may also occur and should be used with caution in elderly patients. Tolerance may develop with chronic antianginal therapy and nitrate-free intervals are recommended and vary depending on agent and dosage form. Nitrate therapy is contraindicated in patients with hypertrophic cardiomyopathy or suspected right ventricular infarction and nitrates should not be given to patients with hypotension, aortic stenosis, volume depletion or moderate-severe bradycardia/tachycardia. Nitrates are also contraindicated in patients with 5'phosphodiesterase inhibitor use within the previous 24-48 hours due to risk of severe hypotension.19 Table 5 provides a summary of important drug interactions associated with these agents.
The most common adverse events reported with ranolazine therapy are dizziness, constipation, headache and nausea.2,22 Ranolazine is not associated with the development of tolerance, as seen with standard nitrate therapy. Ranolazine does produce a dose-dependent increase in the QT interval and is contraindicated in patients with preexisting QT interval prolongation or hepatic disease and in patients taking other drugs that prolong the QT interval. Table 6 provides a list of the most frequent adverse events reported with each of the agents, according to package labeling.
Table 5. Drug-Drug Interactions Reported with the Antianginal Therapies2,22,67
Medication Interaction Description
Organic nitrates & Ranolazine
Avanafil*; Sildenafil*; Tadalafil*; Vardenafil*
Clinical studies with each of the phosphodiesterase 5 (PDE5) inhibitors have found evidence that these agents potentiate the hypotensive effects of nitrates. Concurrent use of phosphodiesterase 5 (PDE5) inhibitors with an organic nitrate is contraindicated; this includes both regular and intermittent nitrate use. No safe interval between use of any PDE5 inhibitor and a nitrate has been identified. Based on the elimination half‐lives of the PDE5 inhibitors, nitrate doses should not be given within at least 24 hours of sildenafil or vardenafil, and nitrates should not be given within at least 48 hours of tadalafil. Avanafil US prescribing information states that in a life‐threatening situation where a nitrate is desired in a patient who has taken avanafil, a nitrate may be administered at least 12 hours after the last avanafil dose was ingested, but only with close medical supervision and monitoring.
Bromocriptine; Cabergoline; Dihydroergotamine; Ergoloid Mesylates; Ergonovine; Ergotamine*; Methylergonovine
Ergot alkaloids are known precipitants of angina and would be expected to oppose the antianginal effects of nitroglycerin.1 Additionally, nitroglycerin increases the bioavailability of dihydroergotamine and could thereby increase the risk of adverse effects (e.g., ergotism).1,2 It is unknown whether the bioavailability of ergot derivatives other than dihydroergotamine would be similarly affected.
Conivaptan, Fusidic Acid, Idelalisib, others
Are strong CYP3A inhibitor and likely inhibited the metabolism of these agents, and it is expected that conivaptan would have similar effects on other CYP3A4 substrates. As a result, the conivaptan prescribing information recommends avoiding concurrent use with drugs metabolized primarily via CYP3A.1 Also, initiation of treatment with any drug metabolized primarily via CYP3A should be delayed for at least 7 days following discontinuation of conivaptan.
Ranolazine only
Amiodarone; Cisapride; Citalopram; Dofetilide; Domperidone; Paliperidone; Pimozide; Procainamide; QUEtiapine; QuiNIDine; others
Moderate Risk QTc‐Prolonging Agents may enhance the QTc‐prolonging effect of Highest Risk QTc‐Prolonging Agents.The concomitant use of highest risk QTc‐prolonging agents with any other QTc‐prolonging agent should be avoided. Many such combinations are listed contraindications for these drugs. Concomitant use is expected to substantially increase the risk for serious toxicities, including the development of torsades de pointes (TdP) or other significant ventricular tachyarrhythmias. Patients with other risk factors present (e.g., older age, female sex, bradycardia, hypokalemia, hypomagnesemia, heart disease, and higher drug concentrations), would be at an even higher risk for these potentially life‐threatening toxicities.

15
Table 6. Adverse Events Reported with Antianginal Therapies2,22,67 Agent Cardiovascular Central Nervous
System Dermatologic Gastrointestinal Neuromuscular
& Skeletal Miscellaneous
Amyl Nitrite
Cerebral ischemia, facial flushing, hypotension, orthostatic
hypotension, pallor, shock, syncope, tachycardia, vasodilation
Dizziness, headache, intracranial pressure increased, restlessness
Dermatitis, irritation
Fecal incontinence,
nausea, vomiting
Weakness Urinary incontinence, Hemolytic anemia,
methemoglobinemia, Intraocular pressure increased, irritation,
Diaphoresis
Isosorbide Dinitrate
Crescendo angina (uncommon), hypotension, orthostatic
hypotension, rebound hypertension
(uncommon), syncope (uncommon)
Headache (most common),
lightheadedness (related to blood
pressure changes)
‐‐ ‐‐ ‐ Methemoglobinemia (rare, overdose)
Isosorbide Mononitrate
Angina (≤2%), flushing (≤2%), arrhythmia, bradycardia, edema, hyper‐/hypo‐tension,
orthostatic hypotension, pallor,
palpitation, tachycardia
Headache (13% to 35%),
Dizziness (≤4%), fatigue (≤4%), pain (≤4%), emotional
lability (≤2%), anxiety,
concentration impaired, depression, insomnia,
nervousness, nightmares, paresthesia, restlessness,
tremor, vertigo
Pruritus (≤2%), rash
(≤2%)
Nausea (≤3%), abdominal pain (≤2%), diarrhea (≤2%), anorexia, dyspepsia, taste disturbance,
thirst, vomiting, xerostomia
Back pain, muscle cramps,
neck pain
Upper respiratory infection (≤4%), cough increased (≤2%), Allergic
reaction (≤2%), Amblyopia, asthma, diaphoresis, dyspnea, methemoglobinemia (rare; overdose), prostatic disorder,
sinusitis
Nitroglycerin Bradycardia, flushing, hypotension, orthostatic hypotension,
peripheral edema, syncope, tachycardia,
cardiovascular collapse, crescendo angina, palpitation,
rebound hypertension
Headache (common), dizziness,
lightheadedness, blurred vision, restlessness,
vertigo
Pallor, rash Nausea, vomiting, xerostomia
Paresthesia, weakness
Dyspnea, pharyngitis, rhinitis, Diaphoresis, Allergic reactions,
anaphylactoid reaction, application site irritation
(patch), contact dermatitis (ointment, patch), exfoliative
dermatitis, fixed drug eruption (ointment,
patch), methemoglobinemia (rare; overdose), shock
Ranolazine Bradycardia (≤4%), hypotension (≤4%),
orthostatic hypotension (≤4%), palpitation (≤4%), peripheral edema
(≤4%), prolonged QT interval on ECG (>500 msec: ≤1%), torsade de pointes (case report [Morrow,
2007])
Headache (≤6%), dizziness (1% to 6%), confusion (≤4%), vertigo (≤4%), syncope (≤4%), ataxia, hallucination, paresthesia
Hyperhidrosis (≤4%), pruritus
Constipation (5%), abdominal
pain (≤4%), anorexia (≤4%), dyspepsia (≤4%), nausea (≤4%; dose related), vomiting (≤4%), xerostomia
(≤4%)
Weakness (≤4%)
Hematuria (≤4%), blurred vision (≤4%),
tinnitus (≤4%), dyspnea (≤4%), angioedema,
decreased glycosylated hemoglobin, dysuria, eosinophilia, increased blood urea nitrogen, increased serum
creatinine, leukopenia, pancytopenia, renal
failure, thrombocytopenia

16
Summary
Ischemic heart disease is one of the most frequently reported cardiovascular diseases in the US and angina pectoris is the most common symptom of ischemic heart disease. A number of therapies are available for the treatment of angina, including: beta-blockers, calcium channel blockers, nitrates and a number of miscellaneous vasodilation agents. Sublingual nitroglycerin is used to treat an angina attack and long-acting nitrates (transdermal and extended release nitroglycerin, isosorbide mononitrate, isosorbide dinitrate) are used for prophylaxis of angina. Ranolazine is a newer agent with a unique mechanism of action which may also be used in the treatment and prevention of chronic angina. ACCF/AHA Guidelines for patients with Stable Ischemic Heart Disease recommend beta-blockers with or without as needed short-acting sublingual nitroglycerin as first-line treatment. The long-acting nitrates, calcium channel blockers and ranolazine may be considered second-line or add-on options in patients who are not able to tolerate beta-blockers or who require additional therapy to control angina. The nitrates and ranolazine may also be used in the treatment of unstable angina and angina associated with heart failure or myocardial infarction.
The nitrate agents work by relaxing smooth muscle, reducing cardiac oxygen demand and
improving collateral flow to ischemic regions. Ranolazine works by inhibiting late phase sodium influx in ischemic cardiac tissue and reducing myocardial oxygen consumption. Nitrate tolerance may develop with continuous nitrate therapy and can be avoided or overcome with daily nitrate-free intervals ranging from 12-14 hours, depending on dosage form. Ranolazine is not associated with the development of tolerance. No comparative clinical evidence is available for the antianginal therapies. Clinical evidence comparing the agents to other therapies (like beta-blockers and calcium channel blockers) suggests the agents have similar rates of safety and efficacy. The most common adverse events reported with nitrate therapy are headache and flushing and the most common adverse events reported with ranolazine therapy are dizziness, headache and gastrointestinal upset. Ranolazine is also associated with dose-related QT prolongation. In general, the antianginal agents appear to have similar rates of efficacy and are generally well tolerated but development of tolerance and dosing recommendations vary between the agents. Pharmacokinetic factors, in addition to guideline recommendations, should be used when selecting an agent and mode of therapy with the antianginal therapies.

References
1. AHFS Drug Information, ed AHFS 2014 Drug Information. Bethesda, MD: American Society of Health-
System Pharmacists; 2014. 2. Lexi-Comp I, ed Drug Information Handbook. 21st ed. Hudson, OH: Lexi-Comp; 2014. 3. Wilson PW. Prediction of cardiovascular disease events. Cardiol Clin. Feb;29(1):1-13. 4. Srikanth S, Deedwania P. Primary and secondary prevention strategy for cardiovascular disease in diabetes
mellitus. Cardiol Clin. Feb;29(1):47-70. 5. Lardizabal JA, Deedwania P. Lipid-lowering therapy with statins for the primary and secondary prevention
of cardiovascular disease. Cardiol Clin. Feb;29(1):87-103. 6. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the
United States: a policy statement from the American Heart Association. Circulation. Mar 1;123(8):933-944.
7. Gupta R, Deedwania P. Interventions for cardiovascular disease prevention. Cardiol Clin. Feb;29(1):15-34. 8. Franco M, Cooper RS, Bilal U, Fuster V. Challenges and opportunities for cardiovascular disease
prevention. Am J Med. Feb;124(2):95-102. 9. Ketchum K, Peterson K, Thakurta S, Low A, McDonagh MS. Drug class review: Newer Antiplatelet
Agents. Update 2. Oregon Health and Science University; 2011. 10. De Lemos JA, O'Rourke RA, Harrington R. Chapter 59. Unstable Angina and Non-ST-Segment Elevation
Myocardial Infarction. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst's the heart. 13th ed. New York: McGraw-Hill; 2011.
11. Weitz JI. Chapter 30. Blood Coagulation and Anticoagulant, Fibrinolytic, and Antiplatelet Drugs. In: Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2011.
12. Weitz JI. Chapter 118. Antiplatelet, Anticoagulant, and Fibrinolytic Drugs. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medecine. 18th ed. New York: McGraw-Hill; 2012.
13. Katzung BG. Vasodilators & the Treatment of Angina Pectoris. In: Katzung BG, Trevor AJ, eds. Basic & Clinical Pharmacology. 13th ed. New York, NY: McGraw-Hill; 2015.
14. Michel T, Hoffman BB. Chapter 27. Treatment of Myocardial Ischemia and Hypertension. . In: Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York, NY: McGraw-Hill; 2011.
15. Depre C, Vatner SF, Gross GJ. Chapter 54. Coronary Blood Flow and Myocardial Ischemia. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst's The Heart. 13th ed. New York, NY: McGraw-Hill; 2011.
16. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: executive summary: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. Dec 18 2012;126(25):3097-3137.
17. Goblirsch G, Bershow S, Cummings K, et al. Stable Coronary Artery Disease.: Institute for Clinical Systems Improvement; 2013.
18. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. Oct 15 2013;62(16):e147-239.
19. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. Jan 29 2013;127(4):e362-425.
20. Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. Jun 11 2013;127(23):e663-828.
21. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of
18
Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. Dec 23 2014;130(25):e344-426.
22. McEvoy GK, Snow EK, Kester L, Litvak K, Miller J, Welsh OH, eds. AHFS 2014 Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2014.
23. Bogaert MG. Clinical pharmacokinetics of nitrates. Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy. Oct 1994;8(5):693-699.
24. Ninomiya Y, Hamasaki S, Saihara K, et al. Comparison of effect between nitrates and calcium channel antagonist on vascular function in patients with normal or mildly diseased coronary arteries. Heart and vessels. Mar 2008;23(2):83-90.
25. Kaplan K, Davison R, Parker M, Przybylek J, Teagarden JR, Lesch M. Intravenous nitroglycerin for the treatment of angina at rest unresponsive to standard nitrate therapy. The American journal of cardiology. Mar 1 1983;51(5):694-698.
26. Hall R, Chong C. A double-blind, parallel-group study of amlodipine versus long-acting nitrate in the management of elderly patients with stable angina. Cardiology. 2001;96(2):72-77.
27. Shapira OM, Alkon JD, Macron DS, et al. Nitroglycerin is preferable to diltiazem for prevention of coronary bypass conduit spasm. The Annals of thoracic surgery. Sep 2000;70(3):883-888; discussion 888-889.
28. Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA : the journal of the American Medical Association. May 26 1999;281(20):1927-1936.
29. Raddino R, Caretta G, Bonadei I, Teli M, Vizzardi E, Cas LD. Differences between nitrates: role of isosorbide 2-mononitrate. Journal of cardiovascular medicine (Hagerstown, Md.). Jul 2010;11(7):486-492.
30. Is isosorbide mononitrate better than the dinitrate? Drug and therapeutics bulletin. Jan 27 1984;22(2):7-8. 31. Ankier SI, Fay L, Warrington SJ, Woodings DF. A multicentre open comparison of isosorbide-5-
mononitrate and nifedipine given prophylactically to general practice patients with chronic stable angina pectoris. J Int Med Res. Mar-Apr 1989;17(2):172-178.
32. Macedo PG, Asirvatham SJ, Maia L, et al. Comparison of a shortened isosorbide dinitrate-potentiated head-up tilt testing with the conventional protocol: tolerance and diagnostic accuracy. Pacing and clinical electrophysiology : PACE. Aug 2012;35(8):1005-1011.
33. Holmes AS, Chirkov YY, Willoughby SR, Poropat S, Pereira J, Horowitz JD. Preservation of platelet responsiveness to nitroglycerine despite development of vascular nitrate tolerance. Br J Clin Pharmacol. Oct 2005;60(4):355-363.
34. Kosmicki MA, Szwed H, Sadowski Z. Anti-ischaemic response to sublingual nitroglycerin during oral administration of isosorbide dinitrate in patients with stable angina pectoris: when does cross-tolerance occur? Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy. Jan 2004;18(1):47-55.
35. Khanlari B, Linder L, Haefeli WE. Local effect of transdermal isosorbide dinitrate ointment on hand vein diameter. European journal of clinical pharmacology. Dec 2001;57(10):701-704.
36. Nino J, Villar JC, Tahvanainen KU, Kahonen M, Kuusela TA, Morillo CA. Vasovagal susceptibility to nitrate or isoproterenol head-up tilt. The American journal of cardiology. Dec 1 2001;88(11):1326-1330.
37. Webb DJ, Muirhead GJ, Wulff M, Sutton JA, Levi R, Dinsmore WW. Sildenafil citrate potentiates the hypotensive effects of nitric oxide donor drugs in male patients with stable angina. Journal of the American College of Cardiology. Jul 2000;36(1):25-31.
38. Pfister M, Seiler C, Fleisch M, Gobel H, Luscher T, Meier B. Nitrate induced coronary vasodilatation: differential effects of sublingual application by capsule or spray. Heart. Oct 1998;80(4):365-369.
39. Wallen NH, Larsson PT, Broijersen A, Andersson A, Hjemdahl P. Effects of an oral dose of isosorbide dinitrate on platelet function and fibrinolysis in healthy volunteers. Br J Clin Pharmacol. Feb 1993;35(2):143-151.
40. Atanassova R, Spassov G, Balansky R, Boev K. Effects of isosorbide-5-mononitrate and isosorbide-2-mononitrate on the contractile and electrical activity and on the content of cyclic nucleotides in isolated heart muscles of the guinea-pig and dog. The Journal of pharmacy and pharmacology. Aug 1992;44(8):663-666.
41. De Caterina R, Giannessi D, Bernini W, Lazzerini G, Mazzone A, Lombardi M. In vivo actions of organic nitrates on platelet function in humans. Zeitschrift fur Kardiologie. 1989;78 Suppl 2:56-60; discussion 64-57.

19
42. Mukerjee N, Pietruszko R. Inactivation of human aldehyde dehydrogenase by isosorbide dinitrate. The Journal of biological chemistry. Aug 26 1994;269(34):21664-21669.
43. Parker JO. Eccentric dosing with isosorbide-5-mononitrate in angina pectoris. The American journal of cardiology. Oct 15 1993;72(12):871-876.
44. Thadani U, Maranda CR, Amsterdam E, et al. Lack of pharmacologic tolerance and rebound angina pectoris during twice-daily therapy with isosorbide-5-mononitrate. Annals of internal medicine. Mar 1 1994;120(5):353-359.
45. Chrysant SG, Glasser SP, Bittar N, et al. Efficacy and safety of extended-release isosorbide mononitrate for stable effort angina pectoris. The American journal of cardiology. Dec 1 1993;72(17):1249-1256.
46. DeMots H, Glasser SP. Intermittent transdermal nitroglycerin therapy in the treatment of chronic stable angina. Journal of the American College of Cardiology. Mar 15 1989;13(4):786-795.
47. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. The New England journal of medicine. Nov 11 2004;351(20):2049-2057.
48. Anand IS, Tam SW, Rector TS, et al. Influence of blood pressure on the effectiveness of a fixed-dose combination of isosorbide dinitrate and hydralazine in the African-American Heart Failure Trial. Journal of the American College of Cardiology. Jan 2 2007;49(1):32-39.
49. Cohn JN, Tam SW, Anand IS, et al. Isosorbide dinitrate and hydralazine in a fixed-dose combination produces further regression of left ventricular remodeling in a well-treated black population with heart failure: results from A-HeFT. Journal of cardiac failure. Jun 2007;13(5):331-339.
50. Colvin-Adams M, Taylor AL. Isosorbide dinitrate-hydralazine improves outcomes in African Americans with heart failure. Cleveland Clinic journal of medicine. Mar 2007;74(3):227-234.
51. Taylor AL, Ziesche S, Yancy CW, et al. Early and sustained benefit on event-free survival and heart failure hospitalization from fixed-dose combination of isosorbide dinitrate/hydralazine: consistency across subgroups in the African-American Heart Failure Trial. Circulation. Apr 3 2007;115(13):1747-1753.
52. Thadani U, Ezekowitz M, Fenney L, Chiang YK. Double-blind efficacy and safety study of a novel anti-ischemic agent, ranolazine, versus placebo in patients with chronic stable angina pectoris. Ranolazine Study Group. Circulation. Aug 1994;90(2):726-734.
53. Thadani U, Opie LH. Nitrates for unstable angina. Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy. Oct 1994;8(5):719-726.
54. Karlberg KE, Saldeen T, Wallin R, Henriksson P, Nyquist O, Sylven C. Intravenous nitroglycerin reduces ischaemia in unstable angina pectoris: a double-blind placebo-controlled study. Journal of internal medicine. Jan 1998;243(1):25-31.
55. Yancy CW, Ghali JK, Braman VM, et al. Evidence for the continued safety and tolerability of fixed-dose isosorbide dinitrate/hydralazine in patients with chronic heart failure (the extension to African-American Heart Failure Trial). The American journal of cardiology. Aug 15 2007;100(4):684-689.
56. Hutt V, Theodor R, Pabst G, Lutz D, Bonn R, Fritschi E. Bioavailability and pharmacokinetics of a new isosorbide dinitrate spray preparation in healthy volunteers. Arzneimittel-Forschung. Aug 1993;43(8):842-846.
57. Bray CL, Jain S, Faragher EB, et al. A comparison of buccal nitroglycerin and sublingual nitroglycerin in the prophylaxis and treatment of exertional (situation-provoked) angina pectoris. European heart journal. May 1991;12 Suppl A:16-20.
58. Ryden L, Schaffrath R. Buccal versus sublingual nitroglycerin administration in the treatment of angina pectoris: a multicentre study. European heart journal. Sep 1987;8(9):995-1001.
59. Dellborg M, Gustafsson G, Swedberg K. Buccal versus intravenous nitroglycerin in unstable angina pectoris. European journal of clinical pharmacology. 1991;41(1):5-9.
60. Tankova L, Yoncheva K, Kovatchki D, Doytchinova I. Topical anal fissure treatment: placebo-controlled study of mononitrate and trinitrate therapies. International journal of colorectal disease. Apr 2009;24(4):461-464.
61. Dragoni S, Gori T, Lisi M, et al. Pentaerythrityl tetranitrate and nitroglycerin, but not isosorbide mononitrate, prevent endothelial dysfunction induced by ischemia and reperfusion. Arteriosclerosis, thrombosis, and vascular biology. Sep 2007;27(9):1955-1959.
62. Zhu WL, Shan YD, Guo JX, et al. Double-blind, multicenter, active-controlled, randomized clinical trial to assess the safety and efficacy of orally administered nicorandil in patients with stable angina pectoris in China. Circulation journal : official journal of the Japanese Circulation Society. Jun 2007;71(6):826-833.
63. Rayman G, Baker NR, Krishnan ST. Glyceryl trinitrate patches as an alternative to isosorbide dinitrate spray in the treatment of chronic painful diabetic neuropathy. Diabetes care. Sep 2003;26(9):2697-2698.
20
64. Wakai A, McCabe A, Kidney R, et al. Nitrates for acute heart failure syndromes. Cochrane Database Syst Rev. 2013;8:Cd005151.
65. Banon D, Filion KB, Budlovsky T, Franck C, Eisenberg MJ. The usefulness of ranolazine for the treatment of refractory chronic stable angina pectoris as determined from a systematic review of randomized controlled trials. The American journal of cardiology. Mar 15 2014;113(6):1075-1082.
66. Savarese G, Rosano G, D'Amore C, et al. Effects of ranolazine in symptomatic patients with stable coronary artery disease. A systematic review and meta-analysis. International journal of cardiology. Nov 15 2013;169(4):262-270.
67. Ives HE. Chapter 15. Diuretic Agents. In: Katzung BG, Masters SB, Trevor AJ, eds. Basic & Clinical Pharmacology. 12th ed. New York, NY: McGraw Hill; 2012.
1. AHFS Drug Information, ed AHFS 2014 Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2014.
2. Lexi-Comp I, ed Drug Information Handbook. 21st ed. Hudson, OH: Lexi-Comp; 2014. 3. Wilson PW. Prediction of cardiovascular disease events. Cardiol Clin. Feb;29(1):1-13. 4. Srikanth S, Deedwania P. Primary and secondary prevention strategy for cardiovascular disease in diabetes
mellitus. Cardiol Clin. Feb;29(1):47-70. 5. Lardizabal JA, Deedwania P. Lipid-lowering therapy with statins for the primary and secondary prevention
of cardiovascular disease. Cardiol Clin. Feb;29(1):87-103. 6. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the
United States: a policy statement from the American Heart Association. Circulation. Mar 1;123(8):933-944.
7. Gupta R, Deedwania P. Interventions for cardiovascular disease prevention. Cardiol Clin. Feb;29(1):15-34. 8. Franco M, Cooper RS, Bilal U, Fuster V. Challenges and opportunities for cardiovascular disease
prevention. Am J Med. Feb;124(2):95-102. 9. Ketchum K, Peterson K, Thakurta S, Low A, McDonagh MS. Drug class review: Newer Antiplatelet
Agents. Update 2. Oregon Health and Science University; 2011. 10. De Lemos JA, O'Rourke RA, Harrington R. Chapter 59. Unstable Angina and Non-ST-Segment Elevation
Myocardial Infarction. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst's the heart. 13th ed. New York: McGraw-Hill; 2011.
11. Weitz JI. Chapter 30. Blood Coagulation and Anticoagulant, Fibrinolytic, and Antiplatelet Drugs. In: Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2011.
12. Weitz JI. Chapter 118. Antiplatelet, Anticoagulant, and Fibrinolytic Drugs. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medecine. 18th ed. New York: McGraw-Hill; 2012.
13. Katzung BG. Vasodilators & the Treatment of Angina Pectoris. In: Katzung BG, Trevor AJ, eds. Basic & Clinical Pharmacology. 13th ed. New York, NY: McGraw-Hill; 2015.
14. Michel T, Hoffman BB. Chapter 27. Treatment of Myocardial Ischemia and Hypertension. . In: Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York, NY: McGraw-Hill; 2011.
15. Depre C, Vatner SF, Gross GJ. Chapter 54. Coronary Blood Flow and Myocardial Ischemia. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst's The Heart. 13th ed. New York, NY: McGraw-Hill; 2011.
16. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: executive summary: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. Dec 18 2012;126(25):3097-3137.
17. Goblirsch G, Bershow S, Cummings K, et al. Stable Coronary Artery Disease.: Institute for Clinical Systems Improvement; 2013.
18. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. Oct 15 2013;62(16):e147-239.
19. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. Jan 29 2013;127(4):e362-425.

21
20. Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. Jun 11 2013;127(23):e663-828.
21. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. Dec 23 2014;130(25):e344-426.
22. McEvoy GK, Snow EK, Kester L, Litvak K, Miller J, Welsh OH, eds. AHFS 2014 Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2014.
23. Ninomiya Y, Hamasaki S, Saihara K, et al. Comparison of effect between nitrates and calcium channel antagonist on vascular function in patients with normal or mildly diseased coronary arteries. Heart and vessels. Mar 2008;23(2):83-90.
24. Kaplan K, Davison R, Parker M, Przybylek J, Teagarden JR, Lesch M. Intravenous nitroglycerin for the treatment of angina at rest unresponsive to standard nitrate therapy. The American journal of cardiology. Mar 1 1983;51(5):694-698.
25. Hall R, Chong C. A double-blind, parallel-group study of amlodipine versus long-acting nitrate in the management of elderly patients with stable angina. Cardiology. 2001;96(2):72-77.
26. Shapira OM, Alkon JD, Macron DS, et al. Nitroglycerin is preferable to diltiazem for prevention of coronary bypass conduit spasm. The Annals of thoracic surgery. Sep 2000;70(3):883-888; discussion 888-889.
27. Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA : the journal of the American Medical Association. May 26 1999;281(20):1927-1936.
28. Macedo PG, Asirvatham SJ, Maia L, et al. Comparison of a shortened isosorbide dinitrate-potentiated head-up tilt testing with the conventional protocol: tolerance and diagnostic accuracy. Pacing and clinical electrophysiology : PACE. Aug 2012;35(8):1005-1011.
29. Holmes AS, Chirkov YY, Willoughby SR, Poropat S, Pereira J, Horowitz JD. Preservation of platelet responsiveness to nitroglycerine despite development of vascular nitrate tolerance. Br J Clin Pharmacol. Oct 2005;60(4):355-363.
30. Kosmicki MA, Szwed H, Sadowski Z. Anti-ischaemic response to sublingual nitroglycerin during oral administration of isosorbide dinitrate in patients with stable angina pectoris: when does cross-tolerance occur? Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy. Jan 2004;18(1):47-55.
31. Khanlari B, Linder L, Haefeli WE. Local effect of transdermal isosorbide dinitrate ointment on hand vein diameter. European journal of clinical pharmacology. Dec 2001;57(10):701-704.
32. Nino J, Villar JC, Tahvanainen KU, Kahonen M, Kuusela TA, Morillo CA. Vasovagal susceptibility to nitrate or isoproterenol head-up tilt. The American journal of cardiology. Dec 1 2001;88(11):1326-1330.
33. Webb DJ, Muirhead GJ, Wulff M, Sutton JA, Levi R, Dinsmore WW. Sildenafil citrate potentiates the hypotensive effects of nitric oxide donor drugs in male patients with stable angina. Journal of the American College of Cardiology. Jul 2000;36(1):25-31.
34. Pfister M, Seiler C, Fleisch M, Gobel H, Luscher T, Meier B. Nitrate induced coronary vasodilatation: differential effects of sublingual application by capsule or spray. Heart. Oct 1998;80(4):365-369.
35. Parker JO. Eccentric dosing with isosorbide-5-mononitrate in angina pectoris. The American journal of cardiology. Oct 15 1993;72(12):871-876.
36. Thadani U, Maranda CR, Amsterdam E, et al. Lack of pharmacologic tolerance and rebound angina pectoris during twice-daily therapy with isosorbide-5-mononitrate. Annals of internal medicine. Mar 1 1994;120(5):353-359.
37. Chrysant SG, Glasser SP, Bittar N, et al. Efficacy and safety of extended-release isosorbide mononitrate for stable effort angina pectoris. The American journal of cardiology. Dec 1 1993;72(17):1249-1256.
38. DeMots H, Glasser SP. Intermittent transdermal nitroglycerin therapy in the treatment of chronic stable angina. Journal of the American College of Cardiology. Mar 15 1989;13(4):786-795.
39. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. The New England journal of medicine. Nov 11 2004;351(20):2049-2057.

22
40. Anand IS, Tam SW, Rector TS, et al. Influence of blood pressure on the effectiveness of a fixed-dose combination of isosorbide dinitrate and hydralazine in the African-American Heart Failure Trial. Journal of the American College of Cardiology. Jan 2 2007;49(1):32-39.
41. Cohn JN, Tam SW, Anand IS, et al. Isosorbide dinitrate and hydralazine in a fixed-dose combination produces further regression of left ventricular remodeling in a well-treated black population with heart failure: results from A-HeFT. Journal of cardiac failure. Jun 2007;13(5):331-339.
42. Colvin-Adams M, Taylor AL. Isosorbide dinitrate-hydralazine improves outcomes in African Americans with heart failure. Cleveland Clinic journal of medicine. Mar 2007;74(3):227-234.
43. Taylor AL, Ziesche S, Yancy CW, et al. Early and sustained benefit on event-free survival and heart failure hospitalization from fixed-dose combination of isosorbide dinitrate/hydralazine: consistency across subgroups in the African-American Heart Failure Trial. Circulation. Apr 3 2007;115(13):1747-1753.
44. Thadani U, Ezekowitz M, Fenney L, Chiang YK. Double-blind efficacy and safety study of a novel anti-ischemic agent, ranolazine, versus placebo in patients with chronic stable angina pectoris. Ranolazine Study Group. Circulation. Aug 1994;90(2):726-734.
45. Thadani U, Opie LH. Nitrates for unstable angina. Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy. Oct 1994;8(5):719-726.
46. Karlberg KE, Saldeen T, Wallin R, Henriksson P, Nyquist O, Sylven C. Intravenous nitroglycerin reduces ischaemia in unstable angina pectoris: a double-blind placebo-controlled study. Journal of internal medicine. Jan 1998;243(1):25-31.
47. Yancy CW, Ghali JK, Braman VM, et al. Evidence for the continued safety and tolerability of fixed-dose isosorbide dinitrate/hydralazine in patients with chronic heart failure (the extension to African-American Heart Failure Trial). The American journal of cardiology. Aug 15 2007;100(4):684-689.
48. Bray CL, Jain S, Faragher EB, et al. A comparison of buccal nitroglycerin and sublingual nitroglycerin in the prophylaxis and treatment of exertional (situation-provoked) angina pectoris. European heart journal. May 1991;12 Suppl A:16-20.
49. Ryden L, Schaffrath R. Buccal versus sublingual nitroglycerin administration in the treatment of angina pectoris: a multicentre study. European heart journal. Sep 1987;8(9):995-1001.
50. Dellborg M, Gustafsson G, Swedberg K. Buccal versus intravenous nitroglycerin in unstable angina pectoris. European journal of clinical pharmacology. 1991;41(1):5-9.
51. Tankova L, Yoncheva K, Kovatchki D, Doytchinova I. Topical anal fissure treatment: placebo-controlled study of mononitrate and trinitrate therapies. International journal of colorectal disease. Apr 2009;24(4):461-464.
52. Dragoni S, Gori T, Lisi M, et al. Pentaerythrityl tetranitrate and nitroglycerin, but not isosorbide mononitrate, prevent endothelial dysfunction induced by ischemia and reperfusion. Arteriosclerosis, thrombosis, and vascular biology. Sep 2007;27(9):1955-1959.
53. Zhu WL, Shan YD, Guo JX, et al. Double-blind, multicenter, active-controlled, randomized clinical trial to assess the safety and efficacy of orally administered nicorandil in patients with stable angina pectoris in China. Circulation journal : official journal of the Japanese Circulation Society. Jun 2007;71(6):826-833.
54. Rayman G, Baker NR, Krishnan ST. Glyceryl trinitrate patches as an alternative to isosorbide dinitrate spray in the treatment of chronic painful diabetic neuropathy. Diabetes care. Sep 2003;26(9):2697-2698.
55. Banon D, Filion KB, Budlovsky T, Franck C, Eisenberg MJ. The usefulness of ranolazine for the treatment of refractory chronic stable angina pectoris as determined from a systematic review of randomized controlled trials. The American journal of cardiology. Mar 15 2014;113(6):1075-1082.
56. Ives HE. Chapter 15. Diuretic Agents. In: Katzung BG, Masters SB, Trevor AJ, eds. Basic & Clinical Pharmacology. 12th ed. New York, NY: McGraw Hill; 2012.