The Application of the Risdon Approach for Mandibular Condyle Fracture
Upload
tomoaki-imaiCategory
view
212download
0
b
ob
0
d
J Oral Maxillofac Surg69:1046-1051, 2011
Anterior Dislocation of theIntact Mandibular Condyle Caused
by Fracture of the Articular Eminence:An Unusual Fracture of the
Temporomandibular Joint ApparatusTomoaki Imai, DDS, PhD,* Masahiro Michizawa, DDS, PhD,†
and Makoto Kobayashi, MD, PhD‡
itdt
Maxillofacial injuries often involve fractures of thetemporomandibular joint (TMJ) apparatus, which oc-cur predominantly in the condylar process of themandible.1,2 Fractures of the temporal bone portionof the TMJ, such as the glenoid fossa or articulareminence, are another important group of injuriesdealt with by maxillofacial specialists.3 Fractures ofthe glenoid fossa are occasionally revealed by imagingfor serious head injuries or mandibular trauma.3,4 Anotable manifestation of glenoid fossa fractures isdislocation of the mandibular condyle into the middlecranial fossa,5-7 of which approximately 50 cases have
een reported.8,9
Reports on articular eminence fractures are scarce,10-13
however, possibly because of their rare occurrence oroften-obscured presentation in the presence of othermore serious injuries. Reported cases have beentreated conservatively12,13 or by surgical interventiononly after an incidental finding during operativewound repair.10 This report presents an unusual type
f articular eminence fracture exhibiting a distur-ance of mouth closing and anterior dislocation of the
*Clinical Fellow, Department of Oral and Maxillofacial Surgery,
Saiseikai Senri Hospital, Suita, Osaka, and the Department of Oral
and Maxillofacial Surgery II, Osaka University Graduate School of
Dentistry, Suita, Osaka, Japan.
†Head, Department of Oral and Maxillofacial Surgery, Saiseikai
Senri Hospital, Suita, Osaka, Japan.
‡Head, Intensive Care Unit, Senri Critical Care Medical Center,
Saiseikai Senri Hospital, Suita, Osaka, and Director, Tajima Emer-
gency and Critical Care Medical Center, Toyooka Hospital,
Toyooka, Hyogo, Japan.
Address correspondence and reprint requests to Dr Imai: De-
partment of Oral and Maxillofacial Surgery II, Osaka University
Graduate School of Dentistry, 1-8 Yamadaoka, Suita, Osaka 565–
0871, Japan; e-mail: [email protected]
© 2011 American Association of Oral and Maxillofacial Surgeons
278-2391/11/6904-0022$36.00/0
oi:10.1016/j.joms.2010.02.051
1046
ntact mandibular condyle caused by a fragment ofhe eminence lodged in the glenoid fossa. We alsoiscuss the causative mechanisms of this fracture pat-ern and its management.
Report of a Case
A 23-year-old man was transferred under paramedic careto the emergency department at our institution after suffer-ing a significant laceration to the right preauricular region ina motorbike accident. On primary survey, his airway waspatent, but he exhibited weak thoracic motion and reducedlung sounds. He had a reduced level of consciousness witha Glasgow Coma Scale score of 8 (E2V1M5). He was subse-quently orally intubated, ventilated, and sedated, and amassive fluid infusion was commenced. A chest radiographshowed right pulmonary contusion. On secondary survey,computed tomography (CT) revealed traumatic subarach-noid hemorrhage and facial bone fractures. Neither cere-brospinal fluid otorrhea nor rhinorrhea was evident. Cranialnerves could not be assessed because of the severe headinjuries. On the right side of the patient’s face, there was apreauricular contused-lacerated wound approximately 7 cmin length that extended horizontally to the zygoma acrossthe zygomatic arch. The wound communicated with theexternal auditory meatus but not the oral cavity. Bleedingfrom small vessels was halted and the wound irrigated withnormal saline solution before the laceration was sutured.The patient received a blood transfusion and was thentransferred while intubated to the intensive care unit.
The following day, a subsequent head CT showed nosigns of deterioration in the intracranial hemorrhage, andthe patient was referred to the Department of Oral andMaxillofacial Surgery for consultation. Facial CT showed aslightly laterally rotated fracture of the zygomaticomaxillarycomplex and comminuted fractures of the zygomatic archand articular eminence (Fig 1). The orbital floor, the man-dibular bone including the condylar process, and the pe-trous part of the temporal bone were all intact. A fragmentof the articular eminence was impacted posteriorly into theglenoid fossa, resulting in persistent anterior dislocation ofthe mandibular condyle. Although malocclusion was antic-ipated, occlusal examination was impossible because of oralintubation. On the fourth day, a chest radiograph showedclear lung fields, and the patient was extubated and subse-
quently maintained a stable respiratory status. We were
ilrwioptsctmt
uoftrgnoalslfommatwtt
bdadoatdmotTfo
IMAI ET AL 1047
then able to observe that the midline of the mandible wasdeviated to the left, and there was severe restriction ofmandibular opening and closing (Fig 2). By day 9, a gradualmprovement in the patient’s level of consciousness al-owed us to apply maxillomandibular fixation (MMF) toeposition the condyle into the glenoid fossa; however, thisas ineffective because of the eminence fragment interfer-
ng with the condyle in the fossa. Ophthalmologic andtorhinolaryngologic examinations detected no visual com-lications, taste disturbances, or hearing deficits. The pa-ient’s face was symmetrical at rest with a nonflattenedhape to the malar eminence. The eyes were able to closeompletely, there was no eyelid droop, and the angles ofhe mouth moved symmetrically; however, there was nootor function in the right forehead. There was no pares-
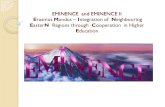
FIGURE 1. Computed tomography images showing fractures ofthe articular eminence, zygomatic arch, and zygomaticomaxillarycomplex: the superficial free fragment derived from the articulareminence including the tubercle (star) and the deeper fragment(arrow) derived from the other part of the eminence, which was themain contributor to obstructing condylar movement. A, Axial imageshowing 2 fragments of the articular eminence dislocated posteri-orly with external rotation. The zygomatic body is also fracturedwith slight external rotation. B, Three-dimensional computed tomog-raphy image showing the articular eminence fragment lodged inthe glenoid fossa and anterior dislocation of the intact mandibularcondyle.
Imai et al. Unusual Fracture of the Articular Eminence. J OralMaxillofac Surg 2010.
hesia of the infraorbital area.
Consequently, on day 11, we performed open surgerynder general anesthesia with nasal intubation. After re-pening the sutured wound, we first found an isolated boneragment of the articular eminence including the articularubercle, situated superficial to the TMJ. On deeper explo-ation, we subsequently identified another fragment in thelenoid fossa, along with obliteration of the articular emi-ence (Fig 3). The TMJ capsule was ruptured with exposuref the upper joint space. The former fragment was notttached to the periosteum and was therefore removed. Theatter fragment was reduced from the fossa without exces-ive bleeding or intracranial perforation. The anteriorly dis-ocated condyle could therefore be repositioned into theossa with manipulation of the mandible, and the normalcclusal position was eventually restored. The deeper frag-ent of the articular eminence and the comminuted frag-ents of the zygomatic arch were fixated with a miniplate
nd stabilized with absorbable sutures. The likely transectedemporal branch of the facial nerve could not be identifiedith a nerve stimulator among the contused subcutaneous
issues. The ruptured articular ligament was sutured, andhe wound was subsequently closed.
Postoperatively, the mandibular deviation relapsed slightlyecause of swelling of the TMJ, but additional maxilloman-ibular fixation was not necessary because the patient wasble to induce his mandible to the occlusal position. Near-aily jaw exercises commenced, and the degree of mouthpening gradually increased to 45 mm with maintenance ofstable occlusal position (Fig 4). Postoperative complica-
ions of taste disturbance or hearing deficit were not evi-ent. Six months later, the patient achieved sufficient jawotion without pain around the TMJ, showed no evidence
f additional complications, and was not concerned abouthe right forehead paralysis. Follow-up lateral panoramicMJ projections revealed normal condylar position in the
ossa on jaw closing and sufficient condylar movement onpening (Fig 5).
Discussion
To our knowledge, only a few reports in Englishhave described fractures of the temporal bone artic-
FIGURE 2. Preoperative malocclusion. The mandible was devi-ated to the left because of anterior dislocation of the right condyle,with disturbance of mouth opening and closing.
Imai et al. Unusual Fracture of the Articular Eminence. J Oral
Maxillofac Surg 2010.
oit
act
IM
1048 UNUSUAL FRACTURE OF THE ARTICULAR EMINENCE
ular eminence (Table 1). The case described here isunique among these in that the mandibular condylewas anteriorly dislocated and unable to restitute intothe glenoid fossa because of obstruction by a frag-ment of the fractured articular eminence. Four of the5 reported cases, including the present case, wereaccompanied by a large ipsilateral preauricular lacer-ation, indicating that this type of fracture may mostoften be caused by a direct lateral force impacting onor near the articular eminence, which is more protu-berant than the glenoid fossa and mandibular con-dyle. This contrasts with condylar fractures, whichexemplify fractures incurred by an indirect force.
Fractures of the TMJ apparatus can vary in patternand severity according to the condylar position and
FIGURE 3. Intraoperative view of preauricular laceration andfractured articular eminence. A, View of the opened wound show-ing anteriorly dislocated condyle with ruptured articular capsule(white arrow). The superficial fragment (star) was subsequentlyremoved and the deeper fragment (black arrowhead) was re-duced. B, View of relocated condyle in the fossa showing exposureof the upper joint cavity with no apparent injury to the articular disk(white arrowhead).
Imai et al. Unusual Fracture of the Articular Eminence. J Oral
Maxillofac Surg 2010.individual morphostructural variations of the TMJ, aswell as the size and direction of the external force.For example, there is a predisposition in childhood tointracranial dislocation of the intact condyle becauseof a relatively smaller and more rounded condylarhead and thinner roof of the glenoid fossa.6,14 More-
ver, a wide mouth opening at the instant of impacts thought to increase the risk of intracranial disloca-ion of the intact condyle7 or condylar fracture,15
whereas fractures incurred while the mouth is closedshow a predilection for the subcondylar region.15 Inddition, mouth opening on impact seemed to be aontributing factor in superolateral condylar disloca-ion into the temporal fossa.16
When fracture fragments of the articular eminenceare displaced, they may normally move inferiorly oranteriorly because there are bony structures posteri-orly and superiorly—namely, the mandibular condyleand the zygomatic process of the temporal bone,respectively. In the present case, however, there wasan anterior-posterior positional interchange betweenthe eminence fragments and condyle. Because thispattern was unlikely to occur as long as the condyleremained in the glenoid fossa, we believe that themost likely causative mechanism of this injury is asfollows: at the moment of impact of the face with theroad surface, the patient opened his mouth widely interror, moving the condyle anteriorly out of the fossa.The direct anterolateral force tore the preauricularsoft tissue, comminuted the zygomatic arch, and frac-tured and slightly laterally rotated the zygomatico-maxillary complex. Concomitantly, the articular emi-nence was also fractured into 2 fragments, and one ofthem slid backward into the vacant fossa, impedingthe restitution of the condyle. Allowing for the ex-
FIGURE 4. Postoperative re-established occlusion.
mai et al. Unusual Fracture of the Articular Eminence. J Oralaxillofac Surg 2010.
traordinary sequence of events required for such an

ct
axillo
IMAI ET AL 1049
outcome, we emphasize its dependence on the man-dibular position at the time of impact.
Management of articular eminence fractures de-pends primarily on the patient’s overall medical statusand more specifically on the degree and pattern ofeminence fracture. Because of the high-energy natureof the causative force, major displacement of theeminence fragment may occur concomitant to life-threatening injuries, such as serious temporal bonefractures or intracranial complications, in which casemaxillofacial specialists commonly have no choiceother than conservative management.3 Here, our pa-tient, who initially had an impaired level of conscious-ness, underwent surgical reduction of the articulareminence fragment that was mechanically impedingcondylar movement. Although rare but generallyknown, there are instances in which open reduction
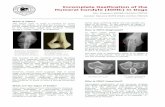
FIGURE 5. Six-month postoperative panoramic temporomandibcontralateral (C and D) sides. A and C, On jaw closing, condylarcondylar movement on the ipsilateral side (B) is sufficient with slighindicate the titanium plate.
Imai et al. Unusual Fracture of the Articular Eminence. J Oral M
of a condylar fracture is indicated when fragments w
from any fracture obstruct movement at the TMJ.1 Toour knowledge, however, this is the first case reportdescribing the surgical treatment of an articular emi-nence fracture based on the preoperative assessmentof a displaced fragment in the glenoid fossa.
Keith et al10 described surrounding soft tissue inju-ries that may be concomitant with articular eminencefractures, including damage of the TMJ capsule result-ing in condylar dysmobility secondary to scarring,chorda tympani injury leading to loss of taste, andstretch injury of the anterior malleolar ligament lead-ing to tearing of the tympanic membrane and conse-quent hearing impairment. Fortunately, neither the 3previously reported cases with established out-comes10,12,13 nor the present case had any of theseomplications. Further, this case illustrates some ofhe issues regarding management of facial lacerations
nt projections for lateral views of the ipsilateral (A and B) andns in the fossa are normal bilaterally. B and D, On jaw opening,inferior movement because of flattening of the eminence. Arrows
fac Surg 2010.
ular joipositiotly less
ith restricted medical resources, particularly those

twatfbartbb
able
1.REP
ORTE
DCA
SES
OF
ARTI
CU
LAR
EMIN
ENCE
FRA
CTU
RE
Rep
ort
Pat
ien
tA
ge(y
rs)
and
Gen
der
Tra
um
atic
Even
tP
reau
ricu
lar
Lace
rati
on
(Len
gth
)D
efin
itiv
eIm
agin
gfo
rD
iagn
osi
sD
islo
cati
on
of
Co
nd
yle
Po
siti
on
of
Frag
men
tO
ther
Cra
nio
faci
alFr
actu
res
Tre
atm
ent
thet
al1
0(1
990)
19,m
ale
Rea
r-se
atp
asse
nge
rin
car
acci
den
tV
erti
cal
(7cm
)N
on
e(i
ntr
aop
erat
ivel
yd
iagn
ose
d)
No
ne
An
teri
or
toco
nd
yle*
Man
dib
le(c
on
tral
ater
alp
aras
ymp
hys
ial
regi
on
and
ipsi
late
ral
ram
us)
Stab
iliza
tio
no
fth
efr
actu
red
emin
ence
frag
men
tw
ith
sutu
res,
follo
wed
by
MM
Ffo
r5
wee
ksec
kian
dW
olf
11
1990
)32
,mal
eA
ssau
ltw
ith
ah
atch
etH
ori
zon
tal
(10
cm)
Pan
ora
mic
x-r
ayN
on
eIn
feri
or
dis
pla
cem
ent
No
ne
No
td
escr
ibed
and
Pec
k12
2001
)31
,mal
eFa
llfr
om
3rd
flo
or
Ver
tica
l(8
cm)
Pan
ora
mic
x-r
ayN
on
eN
od
isp
lace
men
tN
on
eC
on
serv
ativ
etr
eatm
ent
on
lyw
ith
ou
tM
MF
auch
iet
al1
3
2006
)24
,mal
eSt
ruck
on
chin
by
stee
rin
gw
hee
lin
aca
rac
cid
ent
No
ne
MR
Ian
dax
ial
CT
No
ne
No
dis
pla
cem
ent
Gle
no
idfo
ssa
Co
nse
rvat
ive
trea
tmen
to
nly
wit
ho
ut
MM
F
sen
tca
se23
,mal
eM
oto
rbik
eac
cid
ent
Ho
rizo
nta
l(7
cm)
CT
An
teri
or
Gle
no
idfo
ssa
Zyg
om
atic
om
axill
ary
com
ple
xan
dzy
gom
atic
arch
Rem
ova
lo
fin
terf
erin
gfr
agm
ent
tore
po
siti
on
con
dyl
ein
tofo
ssa
bre
viat
ion
s:C
T,
com
pu
ted
tom
ogr
aph
y;M
MF,
max
illo
man
dib
ula
rfi
xat
ion
;M
RI,
mag
net
icre
son
ance
imag
ing.
Deg
ree
of
dis
pla
cem
ent
un
clea
r.
ai
eta
l.U
nu
sua
lFr
act
ure
of
the
Art
icu
lar
Em
inen
ce.J
Ora
lM
axi
llofa
cSu
rg2
01
0.
1050 UNUSUAL FRACTURE OF THE ARTICULAR EMINENCE
related to a traumatic swollen face in a patient ob-tunded because of severe head injuries. Emergencyphysicians rightly prioritize lifesaving treatment dur-ing primary care, which may, however, hamper eval-uation of facial nerve injury, identification of the tran-sected branches, and neurorrhaphy.
Temporal bone fractures are traditionally classifiedinto 2 prominent patterns, longitudinal and transversetypes.3,17 The former typically results from a directlateral blow to the skull, and the fracture line runsthrough the external auditory canal, parallel to thepetrous ridge and to the foramen ovale, whereas thelatter is commonly caused by an anteroposterior blowto the skull resulting in a fracture line perpendicularto the petrous ridge and is accompanied by a poorerprognosis. Ort et al18 reported that both types ofemporal bone fractures can occur in conjunctionith fractures of the TMJ portion in childhood, and
lthough the portion of the TMJ apparatus involved inhese fractures was not classified, they likely involvedracture of the articular eminence, glenoid fossa, oroth. Articulator eminence fractures may be associ-ted with longitudinal fractures because both canesult from a lateral blow, whereas glenoid fossa frac-ures may be associated with either type of temporalone fracture because either a lateral or occipitallow can be transmitted throughout the skull base,3
which includes the glenoid fossa.In conclusion, management of atypical fractures
involving the TMJ are a challenging responsibilityoften falling to maxillofacial specialists, who musttake account of potential concomitant temporal bonefractures and intracranial complications in coopera-tion with emergency physicians, otorhinolaryngolo-gists, and neuro specialists. In any fracture of the TMJapparatus, surgical intervention followed by postop-erative exercises should be carefully considered, par-ticularly when fracture fragments impede condylarmovement.
References1. Chacon GE, Larsen PE: Principles of management of mandibu-
lar fractures, in Miloro M, Ghali GE, Larsen PE, et al (eds):Peterson’s Principals of Oral and Maxillofacial Surgery, Hamil-ton, Canada, BC Decker, 2004, pp 401-433
2. Zachariades N, Mezitis M, Mourouzis C, et al: Fractures of themandibular condyle: A review of 466 cases. Literature review,reflections on treatment and proposals. J Craniomaxillofac Surg34:421, 2006
3. Gladwell M, Viozzi C: Temporal bone fractures: A review forthe oral and maxillofacial surgeon. J Oral Maxillofac Surg 66:513, 2008
4. Iannetti G, Martucci E: Fracture of glenoid fossa followingmandibular trauma. Oral Surg Oral Med Oral Pathol 49:405,1980
5. Barron RP, Kainulainen VT, Gusenbauer AW, et al: Fracture ofglenoid fossa and traumatic dislocation of mandibular condyleinto middle cranial fossa. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 93:640, 2002T
Kei
Rad
(T
ay(
Miy (
Pre Ab *
Im

IMAI ET AL 1051
6. Cillo JE, Sinn DP, Ellis E 3rd: Traumatic dislocation of themandibular condyle into the middle cranial fossa treated withimmediate reconstruction: A case report. J Oral Maxillofac Surg63:859, 2005
7. Musgrove BT: Dislocation of the mandibular condyle into themiddle cranial fossa. Br J Oral Maxillofac Surg 24:22, 1986
8. Barron RP, Kainulainen VT, Gusenbauer AW, et al: Manage-ment of traumatic dislocation of the mandibular condyle intothe middle cranial fossa. J Can Dent Assoc 68:676, 2002
9. Ohura N, Ichioka S, Sudo T, et al: Dislocation of the bilateralmandibular condyle into the middle cranial fossa: Review ofthe literature and clinical experience. J Oral Maxillofac Surg64:1165, 2006
10. Keith O, Jones GM, Shepherd JP: Fracture of the articulareminence. Report of a case. Int J Oral Maxillofac Surg 19:79,1990
11. Radecki CA, Wolf SM: Solitary fracture of the articular emi-nence. Oral Surg Oral Med Oral Pathol 69:768, 1990
12. Tay AB, Peck RH: Solitary fracture of the articular eminence: Acase report. J Oral Maxillofac Surg 59:808, 2001
13. Miyauchi K, Sano K, Nagai M, et al: Occult fractures of articulareminence and glenoid fossa presenting as temporomandibulardisorder: A case report. Oral Surg Oral Med Oral Pathol OralRadiol Endod 101:e101, 2006
14. da Fonseca GD: Experimental study on fractures of the man-dibular condylar process (mandibular condylar process frac-tures). Int J Oral Surg 3:89, 1974
15. Petzel JR, Bulles G: Experimental studies of the fracture behav-iour of the mandibular condylar process. J Maxillofac Surg9:211, 1981
16. Bu SS, Jin SL, Yin L: Superolateral dislocation of the intactmandibular condyle into the temporal fossa: Review of theliterature and report of a case. Oral Surg Oral Med Oral PatholOral Radiol Endod 103:185, 2007
17. Johnson F, Semaan MT, Megerian CA: Temporal bone fracture:Evaluation and management in the modern era. OtolaryngolClin North Am 41:597, 2008
18. Ort S, Beus K, Isaacson J: Pediatric temporal bone fractures
in a rural population. Otolaryngol Head Neck Surg 131:433,2004