Anterior Cruciate Ligament Injuries Intrinsic Risk Factors –Structural differences –Quadriceps...
348
Anterior Cruciate Ligament Injuries Intrinsic Risk Factors – Structural differences – Quadriceps Femoris angle – Femoral Notch – Joint Laxity and Flexibility – Hormonal Influence Extrinsic Risk Factors – Muscular Strength and muscular activation patterns – Knee Stiffness – Jumping and Landing Characteristics
-
Upload
victoria-evans -
Category
Documents
-
view
216 -
download
1
Transcript of Anterior Cruciate Ligament Injuries Intrinsic Risk Factors –Structural differences –Quadriceps...

Anterior Cruciate Ligament Injuries
Intrinsic Risk Factors– Structural differences– Quadriceps Femoris
angle– Femoral Notch– Joint Laxity and Flexibility– Hormonal Influence
Extrinsic Risk Factors– Muscular Strength and
muscular activation patterns
– Knee Stiffness– Jumping and Landing
Characteristics

Structural Differences
Pelvic Width
Tibiofemoral angle
Magnitude of the Q angle
Width of the femoral notch
Quadriceps Femoris Angle(Q Angle)
Average male and female = 8-17 degrees Women avg. at high end; contributes to wide pelvic base and
shorter femoral length resulting in more lateral proximal reference point
Q angles greater than 20 degrees for women are abnormal Inc. lateral pull on quadriceps femoris muscle on the patella and
put medial stress on the knee Lower extremity alignment cannot be altered, but the dynamic
position of the tibia can be improved with internal rotation exercise of the tibia(medial hamstring)

Femoral Notch
Early as 1938, postulated that the dimensions of the intercondylar notch (height, width, ratio of height to width, and overall shape) contribute to anterior cruciate injuries
A narrowed anterior or posterior notch width increases the risk
CT testing necessary A-shaped notch

Joint Laxity and Flexibility
Inherent in the individual
Support by strengthening the quadriceps, hamstrings, gastrocnemius
Caution in attempt to increase flexibility Nutritional support
Hormonal Influence
Estrogen affects soft tissue strength, muscle function, CNS Relaxin can drastically diminish collagen tension Estrogen and progesterone receptor sites have been found in
the ACL More non-contact ACL injuries during the ovulatory phase of
menstrual cycle(day 10-14) During this time there is an estrogen surge and relaxin peak at
day 14 and again midway through the luteal phase PMS influence BCP: hormonal stability

Muscular Strength and Activation Patterns
In response to anterior tibial translation females prefer to recruit the quadriceps whereas the male athlete first contract the hamstrings
Adequate strength and reaction time of the hamstrings is critical in knee stability
Coactivation of the hamstrings with quadriceps is necessary to aid the dynamic component of joint stability, to equalize articular surface pressure distribution, and to regulate the joint’s mechanical impedance.
Plyometrics and agility-type exercises, running through cones, tires, and figure eights to improve muscle reaction time
Knee Stiffness
Intrinsic component is the number of active actin-myosin cross-bridges in the muscles at a specified point(1st point of protection)
Extrinsic component is dependent on the excitation provided by the alpha and gamma motoneurons (potential of protection is greater)
Varus and Valgus stiffness Functional training program that emphasizes the hamstring and
gastrocnemius muscle groups
Jumping and Landing
High percentage of ACL injuries occur when athlete is landing from a jump
More knee extension on landing produces greater maximum impact force
Women perform with less knee flexion, more knee valgus, and less hop flexion.(Orthopedic Society for Sports Medicine Specialty Day, 1999)
Specific Jump and Landing training program is recommended for women who participate in sports that require jumping and pivoting (Hewett 1996)
Rehabilitation of ACL injuries
Early Phase– Weight-bearing and proprioceptive exercises to provide
neuromuscular reeducation and improve functional knee stability
Return-to-Activity Phase– Dynamic exercises involving jumping and pivoting to retrain
the athlete for high impact loading of the knee joint
Follow-through Phase– Continuation of the thrusting leg into a position of full hip and
knee extension. This position causes a valgus force at the knee and tibial external rotation
Back Injuries in the Young Athlete
Acute Injuries
Fractures– T/L spine compression fx occur with axial loading
in a flexed or vertical posture Acute Disc Herniation
– Usually without sciatica– May present with back spasm, neurogenic
scoliosis, hamstring tightness, buttock pain Contusions, Strains, and Subluxations
– Adolescent growth spurt may predispose to an acute apophyseal avulsion of at the lumbodorsal fascia to the apophysis of the iliac crest or spinous process

Overuse Injuries
Risk Factors– Growth Cartilage- immature ossification
centers are often the weakest link of force transfer
– Biomechanics• Kinematics: body motion• Kinetics: force to mass and its motion
– Intrinsic-musculo tendinous inflexibility– Extrinsic-collision and ground reactive forces
– Nutrition- may result in irreversible osteopenia and stress fractures such as spondylolysis
Extension Injuries
Spondylolysis and spondylolisthesis
Lordotic Low Back Pain
Transitional Vertebrae
Facet Syndrome and Sacroilitis
Spondylolysis
Stress fracture of the pars interarticularis Repetitive flexion and extension AP/Lat films Symptomatic fracture treated with anti-
lordotic lumbosacral orthosis(Boston brace), PT modalities, restricted activities
Return to sport after there is demonstrated union, pain-free and manifests a full range of motion

Spondylolisthesis
A forward slippage that occurs with one vertebral body over the inferior vertebral body.
The isthmic type is concern for athlete. Graded by degree of slippage(0-25% grade 1). Athletes are at low risk for progression Progression is associated with rapid growth and
is symptomatic Above Grade 3(>50% slippage); risk for
progression and surgical candidate

Lordotic Low Back Pain
Tight thoracolumbar fascia is a consequence of rapid growth.
Presents as hyperlordosis with a flat mid-back and thoracic kyphosis
Several pain syndromes may ensue– Traction apophysitis at the iliac crest, spinous process,
anterior vertebral ring– Pseudarthrosis (Baastrup’s syndrome)
Transitional Vertebrae
Incomplete segmentation of the lower lumbar and upper sacral vertebrae
Pseudarthrosis may form b/t a bony lumbar extension to the sacral ala or iliac wing
Rapid flexion/extension may cause severe inflammation(Bertolotti’s syndrome) which may mimic a spondylolysis
Treatment to quiet inflammation and stabilize surrounding structures
Facet Syndrome and Sacroiliitis
Flexion Injuries
Scheuermann’s Kyphosis Disc degeneration Internal disc derangement Non traumatic Causes of Back Pain
Scheuermann’s Kyphosis
Three consecutive anterior vertebral bodies wedged at least 5% each
Vertebral end plate changes Schmorl’s nodes Apophyseal ring fractures Upper trunk and postural exercises Atypical Scheuermann’s is associated with the lower
T/L spine due to rapid flexion/extension Aggressive thoracolumbar fascia stretching and
spinal stability

Disc Degeneration
In the young athlete it is usually due to microtraumatic overuse.
Internal Disc Derangement
Radial tear of the inner anulus. The nucleus pulposus is irritating to the outer annulus. The tear is contained and pressure increases with any lumbar flexion. Notably sitting.
Non-traumatic Causes of Back Pain
Consideration must be given from the beginning. Rule out infections with discitis and osteomyelitis, tumors , juvenile RA, and other collagen vascular diseases
Breast Conditions
Breast Cancer Lymph edema Fibro adenoma Fibrocystic Breast Changes Breast Augmentation Mastitis

Breast Cancer
Malignant neoplasm– Classified: in situ (contained) invasive (infiltrated
surrounding tissue)
Several types: – Two most common:
• ductal carcinoma (epithelial cells lining the ducts)
• lobular carcinoma (milk-secreting glands of the breast)

Ductal Carcinoma
Most common of all breast cancers “Ductal carcinoma in situ” has the
highest cure rate of all the cancers Growth Patterns:
– Micropapillary– Cribriform– Solid– Comedo (most aggressive)

Who Gets It?
20-20y/o… 1:2000 30-40y/o… 1:250 40-50y/o… 1:67 50-60y/o… 1:35 60-70y/o… 1:28 Lifetime…. 1:8
Etiology and Risk Factors
Personal and family history of Breast cancer Hormonal influences:
– high/sustained estrogen levels – HRT – BCP(high estrogen)
Exposure: – Foods treated with hormones
• Xeno estrogens
Genes: BRCA 1 BRCA 2 – 50-85% lifetime risk of breast ca, ovarian ca, both.
Signs and Symptoms
Silent Mass-typically not movable “orange-peel” appearance of breast Dilated venous pattern Mass in armpit Nipple discharge Non-healing sore on breast or nipple Swelling in arm or hand Back (bone) pain
Stages of Breast Cancer
Stage O: In situ ductal carcinoma in situ (DCIS)
Stage I: Tumor < 2cm, no spread Stage II(A,B): Tumor 2-5cm, with/without
spread to axillary lymphnodes Stage III(A,B): Tumor >5, spread to axillary
lymphnodes or penetrated the wall to the skin or chest wall
Stage IV: Metastasized
Dietary Support
Indole 3-carbinol: liver metabolism of estrogen to 2-hydroxy estrogen derivative cruciferous vegetables broccoli, kale, cauliflower, cabbage, bok choy
Lignans Green tea catecins Lycopene (tomatoes, red peppers,
grapefruit) Eliminate xenoestrogens (eat organic)
Nutritional Supplementation
Calcium D-glucarate: aid in elimination of xenoestrogens, assist intestinal flora
Coenzyme Q10 300mg/day Selenium 60 mcg/day Vitamin C 5000 mg/day Vitamin E 400 IU/day Folate Vitamin B6 50-100mg/day

Lymphedema
Complication of procedures to treat breast cancer
Accumulation of lymph fluid that accumulates in the arm resulting in swelling.
Etiology– Removal of lymph channels– Compromised immune system
Management
Avoid excessive heat to arm, lifting heavy objects, restrictive clothing, strenuous activity
Compression sleeves Pneumatic pumps Lymphatic drainage massage Mild range of motion exercise

Fibroadenoma What is it?
– Benign tumor of the breast Who gets it?
– Women in their menstruating years, most common breast tumor in adolescent girls
What causes it? – Unknown
Signs and Symptoms: – Movable tumor – Non-tender – Not attached to skin – Clearly delineated
How is it diagnosed? – Signs and symptoms, biopsy, mammography, ultrasound
Fibrocystic Breast Changes
Aka: Cyclic Mastalgia: An exaggerated response of the breast tissue to hormonal changes.
Etiology: Unknown Signs and Symptoms:
– Lumpy breasts– Breast pain and tenderness– Swelling of breasts (feeling of fullness)– Soft, movable lumps– Symptoms progressively worsen after ovulation
and improve after menses
Management
Decrease caffeine Trans fats excess salt hormonal treated foods
Exercise
Breast Augmentation: Risks and Complications
Anesthesia Rxn Asymmetry Bleeding Breast droop Capsular
Contracture Deflation(7%) Displacement Hematoma(3-4%) Impact leak
Infection Nerve damage Pain Permanent
numbness(15%) Rupture of implant Skin irregularities Slow healing Symmastia(merge
into one) Visable scar
Sensation Loss/Change
15% risk of having permanently numb nipples
Implants placed above the muscle have greater risk.
All incisions have a risk of diminished sensation

Capsular Contracture
Scar tissue hardens around the implant Less common and less severe with
saline implants vs. silicone implants Baker Grade I - IV Studies suggest 17% saline implants
have some lasting problem
Rupture or Leak
Rupture of Saline Implants: deflates and the salt water is absorbed by the body.
Rupture of Silicone-Gel implants: pain, tingling, swelling, burning. According to FDA, 69% have at least one rupture.
Mastitis What is it?
– Inflammation/Infection of the milk ducts in the breast Who gets it?
– Women who are breast-feeding. If non-breast feeding, look for CA.
Etiology? – Improper drainage of the milk ducts.
Signs and Symptoms:– Triangular flush: redness on the underside of breast– Swelling, Pain, Tenderness of breast– Flulike symptoms– Fever– Sensation of heat on breast

Prevention/Management
Nurse infant on demand Adequate rest Frequent nursing Support bra Hot packs/massage Drink fluids ** Chaste berry (cyclic mastalgia)
contraindicated b/c prolactin-lowering abilities
Cardiovascular Disease
Any disease of the heart and blood vessels, including CAD, atherosclerosis, DVT, varicose veins, strokes, aneurysms, stenosis
Women affected after age 55. Men-45 y/o
Leading cause of death in women, regardless of race.
Cholesterol(a fat) plays a major role– LDL: bad– HDL: good
Cholesterol
Necessary for variety of functions, primarily the production of hormones
It is not soluble in the blood, must bind to a protein that forms a lipoprotein– LDL: not good because it moves away from the
liver to target tissues, such as the heart– HDL: the protein removes cholesterol from the
target tissue and blood vessels and returns to the liver, for preparation for excretion.
The role of Estrogen
Estrogen raises HDL and lowers LDL Prevents oxidation, making the LDL’
less harmful in the blood vessels. Decreases at menopause
– Women in perimenopause typically have total cholesterol 200-240 with desirable HDL and LDL levels.
Lifestyle changes
Smoking cessation– 4800 chemical substances: many can
damage heart and blood vessels• Nicotine-constricts blood vessels, increase HR
and blood pressure
• Carbon monoxide in smoke- replaces oxygen in the blood, increasing blood pressure, heart has to work harder to get oxygen to tissue
• Women who smoke and take birthcontrol pills are 20-30x greater risk of having stroke or heart attack
Exercise alone reduces CVD by 30-50% Diet: decrease saturated fats Vitamin C: 2000mg/day Folate, B12, B6: decreases homocysteine
levels Homocysteine: Amino acid that, in excess,
damage coronary arteries and make it easier for platelet aggregation, predisposing to heart attack and stroke
Omega-3 fatty acids Manage weight
Female Organ Conditions
Fibroids Polycystic Ovary Syndrome(PCOS) Pelvic Inflammatory Disease(PID) Reproductive Tract Malignancies

Fibroids What is it?
– Noncancerous tumors of the uterus. Who Gets it?
– Women during their reproductive years. Silent in 20’s, symptomatic mid-30’s.
Etiology: – Heredity– Estrogen/Progesterone Imbalance:
• growth is dependent on high estrogen. – Grow during high estrogen times-pregnancy, use of BCP,
insulin resistance. – Shrink with low estrogen times-menopause, progesterone
only BCP
Signs and Symptoms
Feeling of hardness in lower abdomen
Frequent urination Menorrhagia Anemia Blood clots Asymptomatic
Dysmenorrhea Dyspareurnia Mittelschmerz Reproductive
problems-miscarriage and infertility
Low Back Pain
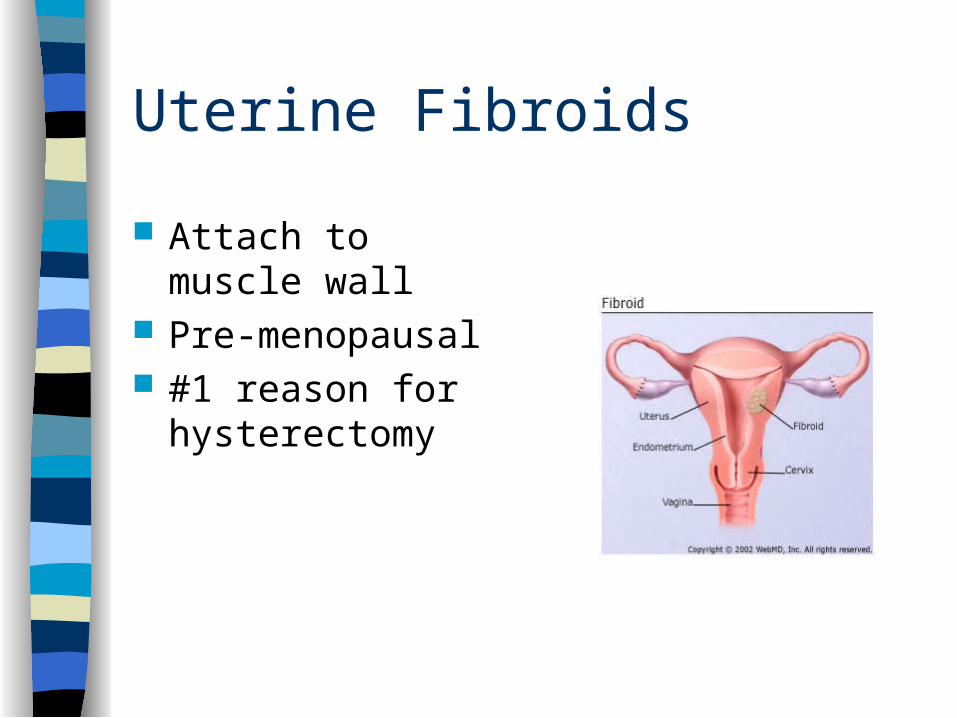
Uterine Fibroids
Attach to muscle wall
Pre-menopausal #1 reason for
hysterectomy
Diagnosis
Uterus appears lumpy on pelvic exam Pelvic ultrasound MRI CT Laparoscopy Hysterosalpingogram Dilation and curettage

Management
Manage insulin resistance: – Can increase estrogen and occurs in times of
prolonged stress. Eliminate Caffeine Increase Phyto estrogens: cruciferous vegetables
Anti-inflammatory Diet Calcium, magnesium, potassium
– decrease muscle/menstrual cramps
Fiber: – Food types provide B vitamins that help body’s
synthesis anti-inflammatory prostaglandins
Psycosocial factors: – Stress causes a rise in cortisol, affects other hormones
Acupressure/Acupuncture Spinal manipulation:
– Uterus and Ovaries T12-L5
Pain control: massage
Vaginal depletion packs-suppositories containing vitamins, minerals, herbs– Improve circulation of the pelvic organs– Draw fluid and infectious exudates out– Inhibit local bacteria growth– Stimulate slough off abnormal cervical cells– Promote lymphatic drainage

Surgery
Myomectomy or Hysterectomy Uterine artery Embolization
– Excessive bleeding– Risk of hemorrhage– Inability to tell if tumor is benign– Familial hx of reproductive tract cancer

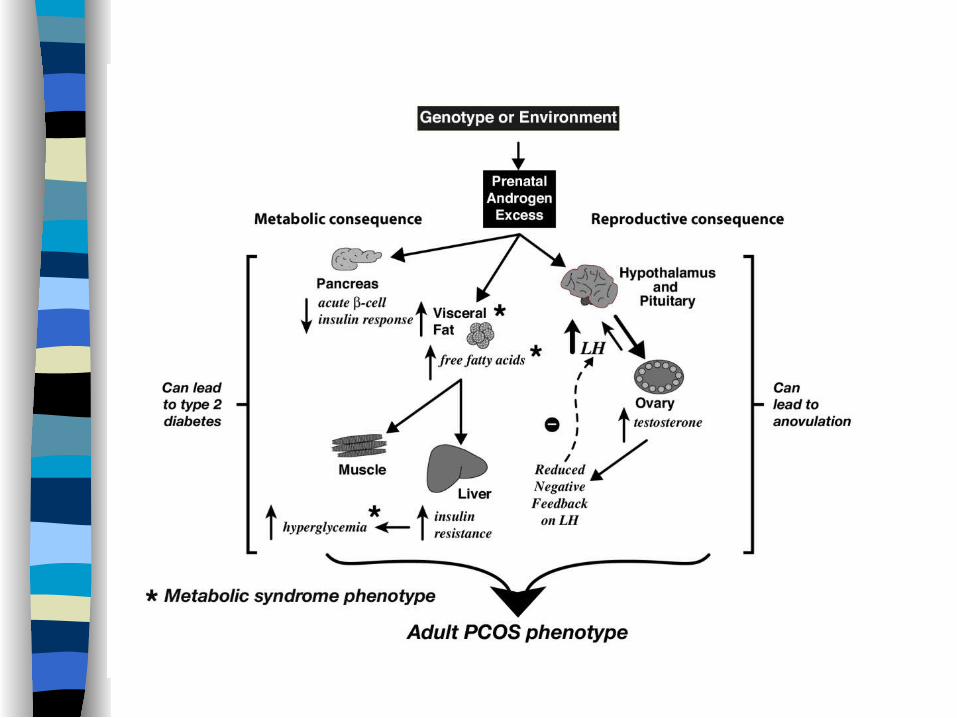
Polycystic Ovary Syndrome(PCOS)
Umbrella term used to label a group of symptoms that all appear to be connected to the menstrual cycle and to have a strong correlation with insulin sensitivity

PCOS
Most common hormonal disorder in women of reproductive age in US (5-10%)
Commonly diagnosed in 20’s but begins during adolescence.
Etiology of PCOS
Ovarian Failure: Follicles mature but do not release an egg, resulting in cyst formation on and around the ovaries, which subsequently cause infertility and amenorrhea
Insulin Resistance: Direct relationship
Insulin Resistance
Cells do not respond to stimulus from insulin…
Blood sugar levels rise, pancreas accelerates insulin production…
Blood sugar floods into cells… Blood sugar levels fall… Hypoglycemic state DIABETES
INSULIN RESISTANCE IS MARKED BY ELEVATED BLOOD SUGAR LEVELS AND BLOOD INSULIN!
Glucose from sugars is converted to energy in cells; in the absence of this critical source of energy, fatigue and food cravings result
The liver responds to elevated Blood sugar levels by rapidly converting excess sugar to fat.
The excess fat results in increased hormone load; more estrogen is stored in fatty tissue and synthesized by the aromatase enzyme.
Aromatase enzyme synthesizes estrogen via the androstenedione pathway…excess testosterone
Signs and Symptoms
Amenorrhea Obesity Infertility Acne Hirsutism Polycystic ovaries Pelvic pain Thinning Hair
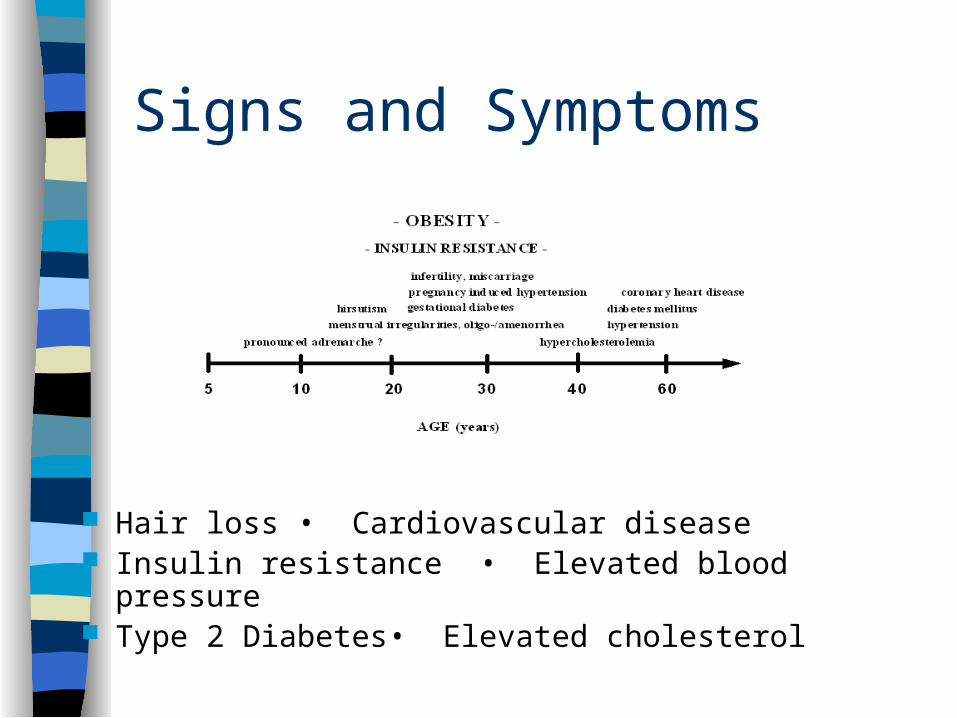
Signs and Symptoms
Hair loss • Cardiovascular disease Insulin resistance • Elevated blood pressure Type 2 Diabetes • Elevated cholesterol
Diagnosis
Gynecologic history Vaginal/abdominal ultrasound Blood chemistries
– Elevated LH– Low FSH– Elevated glucose– Hyperandrogenism– Elevated blood lipids

Management
Dietary: Ingesting simple carbohydrates and high glycemic index foods can compound the problem b/c
they cause a rapid rise in blood sugars. Exercise: Mild to moderate aerobic activity;
intense activity may increase symptoms.
Restore monthly Bleeding:– Progesterone cream during luteal phase– Spinal manipulation to ovaries innervations– Muscle stripping: adductors
Pelvic Inflammatory Disease (PID)
Infection of the uterus, fallopian tubes, or other reproductive organs
Common complication of STD: Chlamydia and gonorrhea Organisms migrate from vagina and cervix into uterus and
pelvis 10% PID are iatrogenically induced: abortion, IUD, D&C Diagnosis:
– Signs & Symptoms
– Differential Diagnosis
– Ectopic pregnancy
– Appendicitis tests immediately following menstruation
Acute PID– Presenting complaint is dull lower abdominal pain;
exacerbated by movement or sexual intercourse– Fever or chills– Rebound tenderness– Procedures that involve dilation of the cervical canal:
miscarriage, abortion, IUD
• Subacute PID• Low back pain• Acute PID
• Chronic PID• Constant/intermittent low back pain• Low grade fever/infection
Reproductive Organ Malignancies
Vulvar cancer: rare form that primarily affects the labia Vaginal cancer:vaginal bleeding in 60% cases Cervical cancer:arises from unmanaged cervical
dysplasia Ovarian cancer: BRCA1 & BRCA 2 Fallopian tube cancer: mild but chronic lower
abdominal or pelvic pain Uterine cancer(endometrial ca):75% post-
menopause; primary cause is unopposed or excess estrogen.
Physiology of the female reproductive system
1. Different periods of Female
Neonatal period : 4 weeks childhood: 4 weeks to age of 12 adolescence: menarche, age of 12-17 sexual maturity: begain 18, maintains for 30
years peri-menopausal period:begain 40,
maintains for 10-20 years pre-menopause, menopause(last time of
menorrhae), post-menopause senility
2.The definition of menstruationMenarche: the onset of the first
menses
occurs about two years after the onset of pubert
occurs between 13 and 15 years of age
anovulatory for first two years
The first day of menstrual bleeding is considered day 1 of the menstrual cycle
The length of menstrual cycle is 28 –30 days
The duration of flow is 2-7 daysThe volume of menstrual blood loss
is 30ml-50mL(<80mL),darkness and nonclotting.
The Founction of ovary
Produce oocyte Endocrine: produce female
hormone

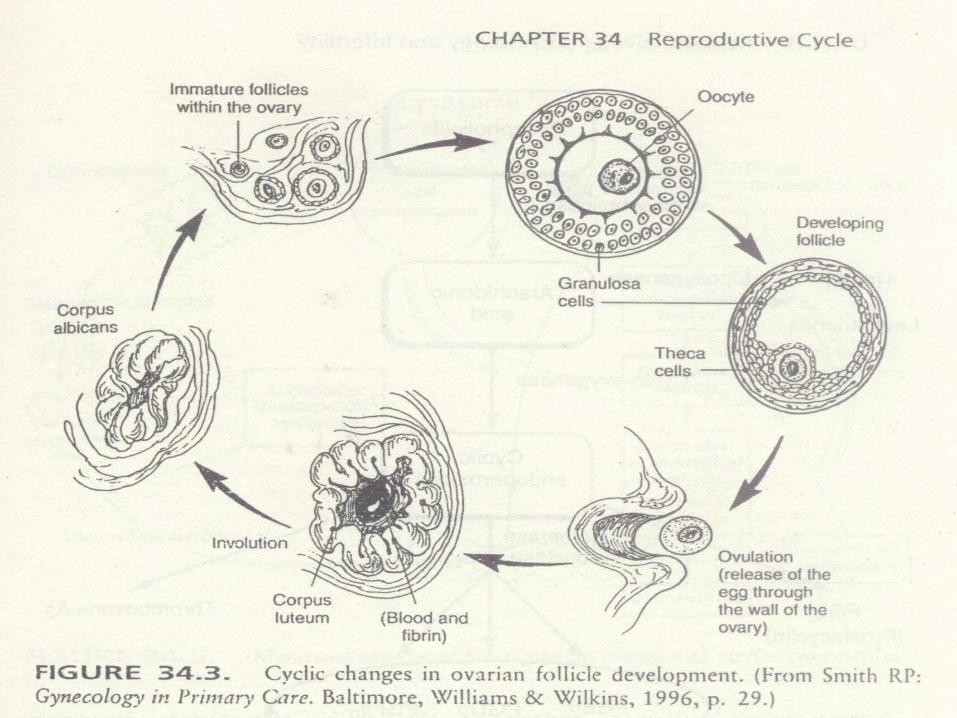
3.Reproductive cycleDevided into 3 phasesMenstruation: 1-4days the follicular phase:5-14 days a number of follicles developing, only one dominant follicle others become atretic ovulation:14th, releasing oocyte luteal phase: 15-28 days unless pregnancy
occurs

1) Development of ovaryOvarian cycle is divided into four phases
Development of follicles primitive folliclesprimary follicles secondary follicles antrun/ developing follicles maturity follicles ovulation corpus luteum corpus albican

2)Ovarian steroid hormones
Estrogens rise in plasma by 4th day of cycle from granulosa cells and theca
cellsnegative feedback to FSHpositve feedback to LH
Progesterone: from corpus luteum maximal production occurs 3-4 days
after ovulation and maintained for 11 days
negative feedback on FSH and LH
4.Clinical manifestations of hormone changes
1)Endometrium be sloughed to a basal level in menstruation proliferative phase: 5-14 days (stroma thickens,gland elongated) in follicular
phase, a maximal thickness in ovulation Secretory phase :15-28 days (stroma loose, edematous, vesseltwisted, gland tortous) in corpus
luteum
Menstrual phase:1-4 days Endomitrium is sloughed and bleeding
onset
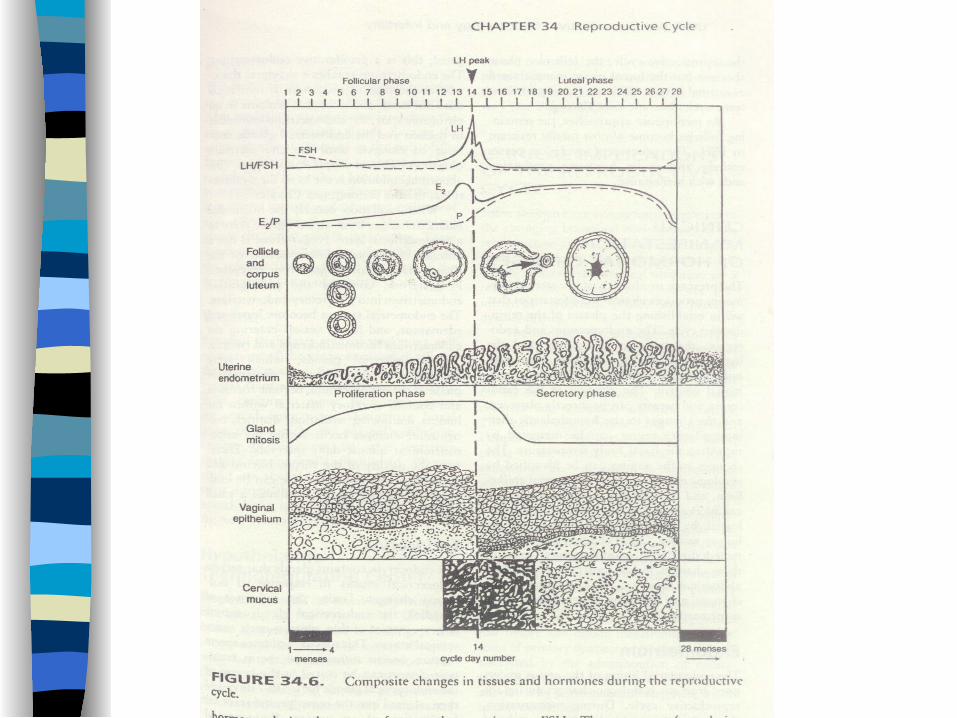

2)endocervix
Cervical also changes in response to the reproductive cycle
Cervical gland secrete thin,clear,watery,mucus in follicular phase
maximal in ovulation
Mucus becomes thick,opaque,tenacious in corpus luteum phase
3)vaginaThickening and maturation of the
surface epithelial cells responed to E2 in follicular phase
thickening and secretory changes of vaginal epithelium in corpus luteum phase
4)Hypothalamic thermoregulating centerProgesterone shifts the Basal body
temperature upward(BBT)
BBT record is a useful tool to evaluate the reproductive cycle
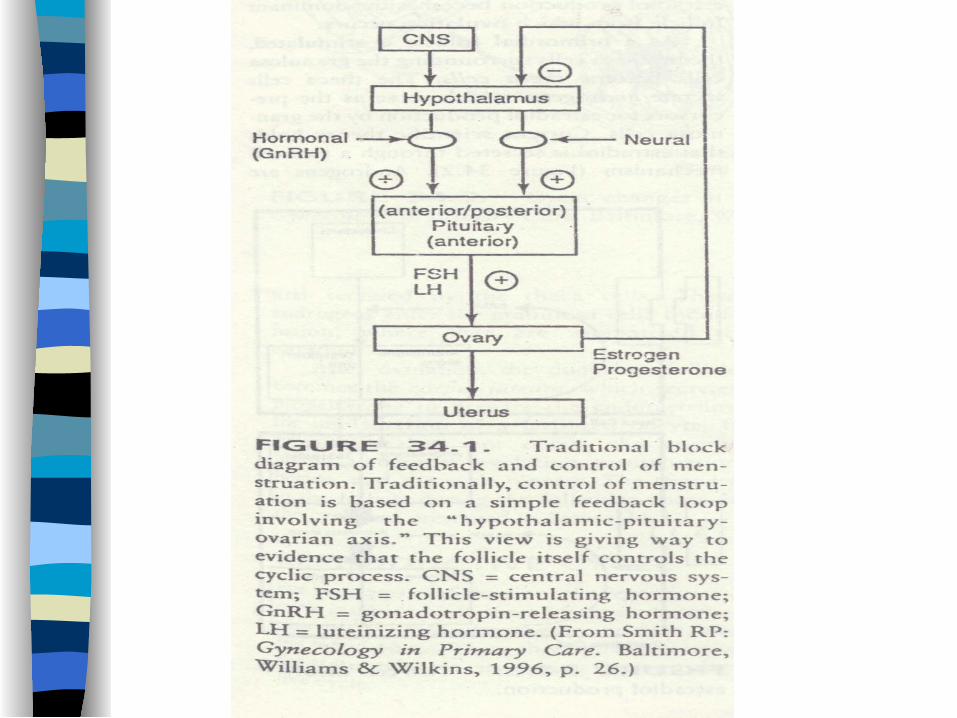
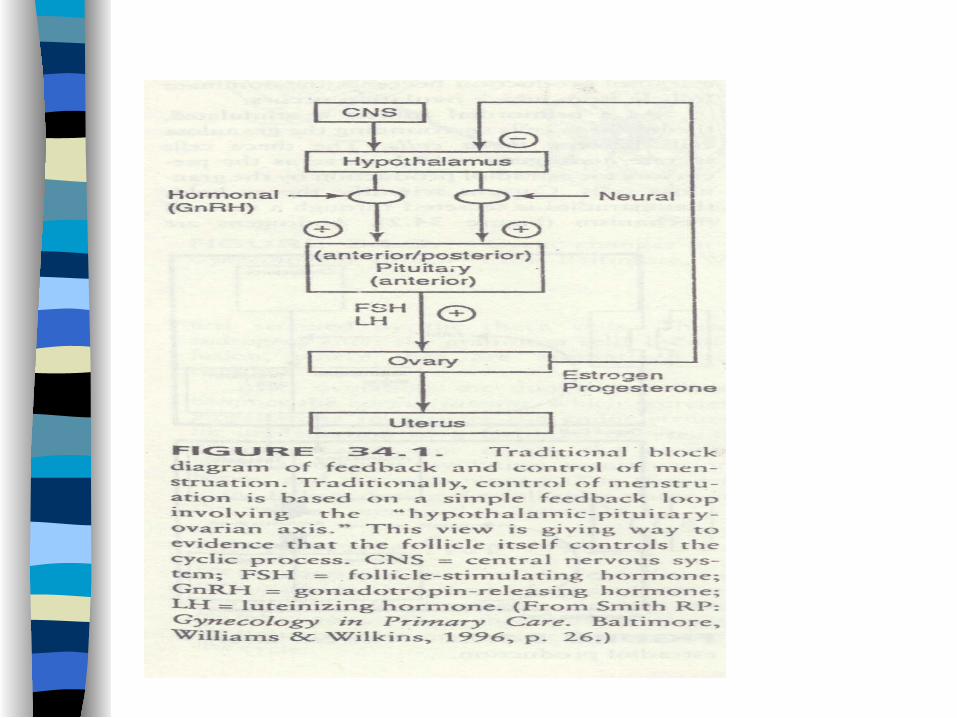
5.H-P-O axis The control of menstruation is
based on a feedback loop of H-P-O axis
Hypothalamus Producing GnRH(gonadotropin-releasing
hormone) be secreted in a pulsatile manner be a pulse generator of cycle be influenced by E and neurotransmitters
PituitaryProducing Gonadotropins follicle-stimulating hormone(FSH) luteinizing hormone(LH)be protein hormones secreted by the
anterior pituitary glandbe pulsatile mannerbe influenced by E,P, and other factors
Ovaries ovarian sex steroid hormones
estradiol (E), progesterone(P)
Feedback of H-P-O axis
Concept of feedback
the magnitude and the rate of GnRH, FSH, LH are determined by E, P,
negative feedback : resulting in decreased secretion ofGnRH FSH,LH
positive feedback: resulting in increased secretion of LH,which triggers ovulation

Key words
reproductive cycle menstruation ovarian cycle H-P-O axis feedback
Fibromyalgia
Aka fibrositis or fibromyositis Most common cause of widespread
muscular pain Affects 2% of all Americans Women 10:1 20-60 y/o; peak at 35 y/o

Etiologies
Sleep disturbances
Lack of exercise
Micro-trauma
Emotional State
Viral Infection
Chemical Imbalance– GH, Serotonin– Low cortisol levels– Elevated substance
P
Autoimmune(RA)

Clinical Diagnosis of Fibromyalgia: American College of Rheumatology 1990
History of Widespread pain– Left side of body– Right side of body– Above waist– Below waist– Axial skeletal(C-T-L)
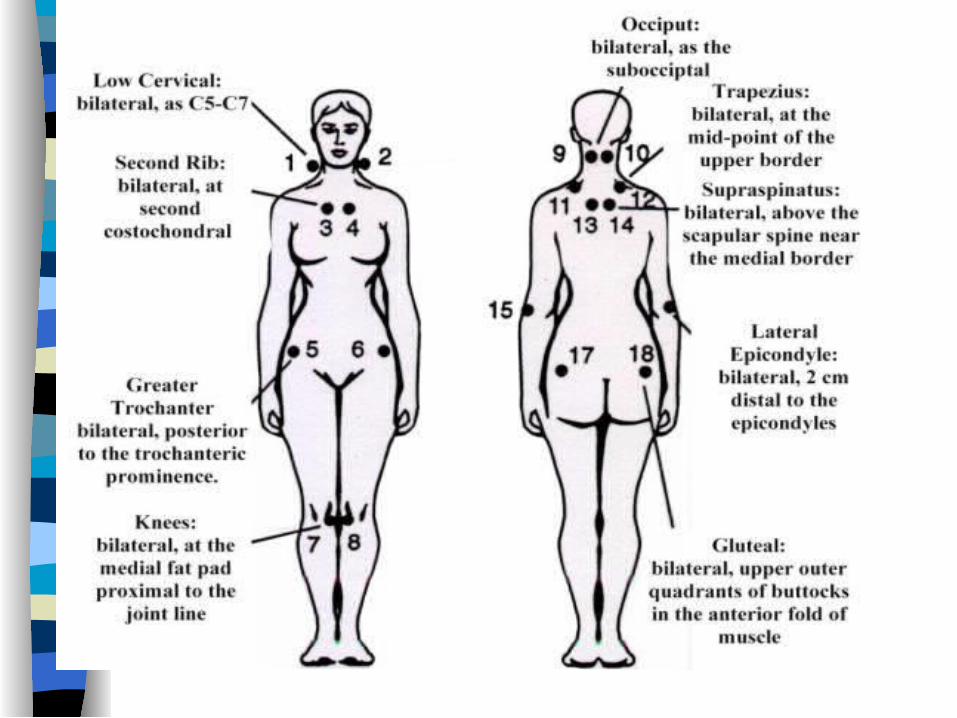
Pain in 11/18 tender point sites on digital palpation
– Occiput– Lower cervical– Trapezium– Supraspinatus– Second rib– Lateral epicondyle– Gluteal Greater
trochanter– Knee
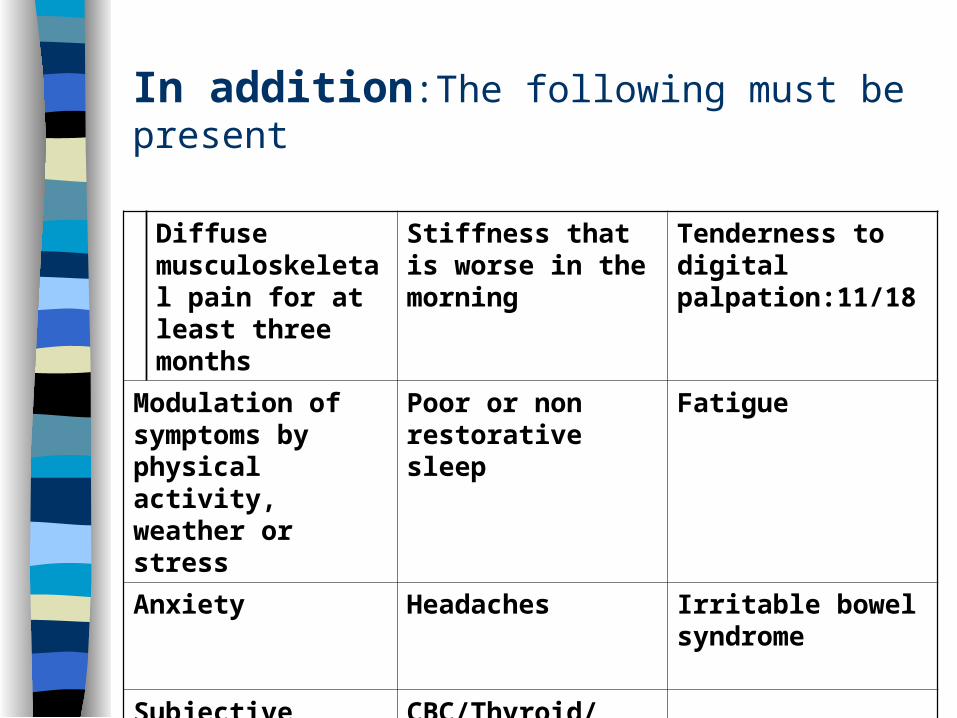
In addition:The following must be present
Diffuse musculoskeletal pain for at least three months
Stiffness that is worse in the morning
Tenderness to digital palpation:11/18
Modulation of symptoms by physical activity, weather or stress
Poor or non restorative sleep
Fatigue
Anxiety Headaches Irritable bowel syndrome
Subjective swelling and numbness
CBC/Thyroid/Anemia/Antibody negative

Fibromyalgia vs. Myofascial Pain
Metabolic Causes vs. Musculoskeletal Injury
Mitochondria damage in muscle cells Disruption of glycolysis: Energy crisis Small blood vessel distortion in muscle during
contraction: tissue hypoxia Decrease cortisol/DHEA: anxiety Leaky gut syndrome: bacteria, fungi, parasites, toxins,
undigested protein, fat and waste
Underactive Liver: free radicals not eliminated-inflammation

Prognosis
Prognosis if favorable with Integrated/supportive treatment
Treatment Protocol
Manipulation/gentle distraction Exercise regime Physical Modalities Sleep Homeopathy/medicine Nutrition Bio behavioral therapies
Liver Detoxification Normalizing intestinal flora Boost immune system Decrease
– Fat consumption– Refined carbohydrates– High protein-increase uric acid levels
Weather Sensitivity
Increase Humidity Decrease barometric pressure +temperature Women 67% ; Men 37% Fibromyalgia 80%(cold,damp) Migraines not affected Ligamentous type of pain syndrome assoc.
with DJD Reactive Depression
Chronic Fatigue Syndrome
Sudden onset of flu-like illness Post-exertional malaise: pain and
weakness of muscles or exacerbation of “systemic” symptoms
Night sweats- 50% patients– Dramatic-associated with chronic infection
CFS vs. Fibromyalgia
Persistant fatigue that does not resolve with bed rest and severe enough to decrease ADL 50% for 6 months
R/O chronic clinical conditions Epstein-Barr antibodies History of viral infection
CFS symptoms
Achy muscles/joints Anxiety Depression Cognitive changes Fever Headaches Intestinal problems Irritability
Muscle spasms URI Sensitivity to
light/heat Sleep disturbances Sore throat Swollen lymph
glands

Treatment
Liver Detoxification Normalizing intestinal flora Boost immune system Decrease
– Fat consumption– Refined carbohydrates– High protein-increase uric acid levels
Iliotibial Band Syndrome
ITB is continuation of the tendinous portion of the TFL Indirectly attaches to the gluteus medius, maximus, and
vastus lateralis muscles The inter-muscular septum connects the ITB to the linea
aspera femoris until just proximal to the lateral epicondyle of the femur
Distally, the ITB spans out and inserts on the lateral border of the patella, lateral patellar retinaculum, and tubercle of the tibia
Assists the TFL in abduction of the thigh and controls and decelerates adduction of the thigh
Anterolateral stabilizer of the knee by moving anterior to the epicondyle as the knee extends and slides posteriorly as the knee flexes, remaining tense in both positions

What Causes ITBS?
Runners mileage Knee Flexion/extension weakness Excessive pronation Hip abductor weakness

The Female Athlete
Title IX: Prohibites sexual discrimination in any federally funded educational institution 1972
Health Concerns Unique to the Female Athlete
Musculoskeletal
Gynecological
Psychological
Nutritional
Musculoskeletal Issues
Osteoarthritis
Spinal injuries
Anterior Cruciate ligament
Stress Fractures
Ilio-tibial Band friction syndrome
Patellar Tracking disorders
Sport Specific Injuries
Female Athlete Triad
Disordered eating: 15-62% female college athletes have self-reported eating disorders. – Anorexia/ Bulimia
Amenorrhea: 66% – Primary, Secondary, Oligomenorrhea
Osteoporosis
Decrease in performance may not be seen for some time, thinking the habits are harmless
Complications include depression, fluid/electrolyte imbalances and changes in endocrine/thermoregulatory systems
Factors contributing include enviromental, mood, performance pressures
Disordered Eating
Amenorrhoea
Altered rhythemic secretions of (GnRH) leads to decreased levels of FSH and LH leads to decreased levels of Estrogen and progesterone
Results in Amenorrhea
Amenorrhea
Primary: Absence of spontaneous uterine bleeding by 14 Y/O; w/o secondary sexual characteristics or by 16y/o with normal development
Secondary: Six-month absence of menstrual bleeding with
Oligomenorrhea Infrequent menses
Osteoporosis
BMD loss is a silent process 95% peak BMD by 18 y/o Puberty accompanied by deposition of 60% of final bone
mass: any nutritional inadequacy and high exercise intensities may more severely alter bone formation
Moderate exercise is beneficial, extreme loads may be detrimental to bone health
Primary function of estrogen is to inhibit osteoclastic activity.
– Hypoestrogenic state, osteoclast-mediated bone resorption in uninhibited, resulting in osteoporosis
Etiology of Female Athlete Triad
Sports or Activities that emphasis lean physique or a specific body weight such as gymnastics, ballet, distant running, diving, swimming
Mental and psychosocial issues: low self-esteem Parents and coaches who place undue
expectations on the athlete Misinformation about nutrition Societal pressure to be thin Physical, sexual, or substance abuse

Signs and Symptoms
Recurrent stress fractures Amenorrhea/
Oligomenorrhea(<9 cycles/yr) Erosion of the tooth enamel
from gastric acids: recurrent vomiting
Very thin Recurring muscle injury Parotid swelling as a result
form frequent stimulation of salivary glands: vomiting
Tooth marks on hand from induced vomiting
Fatigue/decreased ability to concentrate
Sensitivity to cold Heart irregularities Chest pain Endothelial dysfunction Reduced cardiovascular
dilation response to exercise
Eating alone Frequent trips to bathroom
after meals
Diagnosis
History– Menstrual history
• Delayed onset of menarche• Hormonal therapy use
– Diet history• Diet diary• List forbidden foods• Questions about weight• Diet pills/laxatives
– Exercise history• Patterns• Training intensity• Fractures• Overuse injuries
Examination Height/weight/BMI Sexual maturity rating Scoliosis Neglect/abuse screening Blood pressure BMD Labs
– Anemia
– Serum electrolytes
– Enzymes: amylase lipase
Treatment
Diet– Decrease High-phosphate substances (diet soda)– High protein diets cause increase calcium excretion,
potential for bone loss– Decrease red meat: uric acid from protein synthesis
Vitamin and Mineral Supplementation– Calcium– Vitamin D– Vitamin C– Folic Acid




Peri-Menopause Treatment Protocols
Vasomotor(hot flashes, night sweats)
Spinal adjustments: L1/2 ovarian function C0/1 and L5/S1 parasympathetic function
Acupuncture/pressure Bioidentical hormones: Estrogen, testosterone,
progesterone and DHEA. Black cohosh: 500-1000mg dry (20-40mg
extract)/day. Isoflavones (45-50mg/day) Vitamin E (400-800 IU/day) HRT: estrogen; progesterone; est. + prog.

Genitourinary Atrophy/Prolapse
Correcting leg length deficiencies Avoid medication that cause mucosal dryness:
antihistamines and decongestants Chaste berry 150-500mg/day, Black cohosh Zinc 15 mg/day, magnesium, vitamin C Exercises
– Kegal– Knee-chest pulls on slant board– Gluteal contractions– Pelvic rock with pillow between knees
Psychosocial/Psychological
Sleep: aids the function of pineal gland that is responsible for melatonin synthesis.
Melatonin is needed for sleep Diet: omega-3, isoflavones, lignans Exercise St. John’s Wort: inhibit serotonin uptake in brain and
inhibit the enzyme catechol-O-methyltransferase, which degrades the neurotransmitter dopamine.
Manage adrenal fatigue– DHEA: CAREFUL(testosterone-estrogen)– Licorice root

Management of Pregnant Patients
Established patients that become pregnantNew Patients for management of pregnancyNew patients with conditions associated with pregnancy
Activities of Daily Living
Biomechanics: neuro-musculo-skeleton Balance: center of gravity Nutrition Sleep Exercise Stress Ergonomics
Established patients
Treatment schedule – 1st trimester: 12 weeks
• Regular schedule– Fatigue, nausea and vomiting, general malaise– Headaches– Constipation– Hemorroids– Varicosities of legs and vulva– Breast changes– Menstrual like cramping

2nd trimester No more than bimonthly
– Weight gain, greater fatigue, fluid retention– Backache– Indigestion– Food cravings– Light headedness(syncope)– Muscle cramps– Ligament pain– Excessive salivation, Pica, change taste and smell
3rd Trimester 1-2x/wk
– Braxton-Hicks contractions, indigestion– Difficulty breathing, sleeping– Low back pain, groin pain, symphysis pubis pain– Edema– Anxiety, depression, emotional– Joint ache and pain– Dyspepsia
New Pts-pregnancy management
1st trimester: 1x/wk– Establish good alignment and repore
• 2nd trimester: 1x/2wksLess osseous adjusting
• 3rd trimester: 1x/wk Decrease symptoms Prepare for delivery
• Post-partumligamentus stabilityalignmentNutritionbehaviors
NP’s w/ Assoc. Conditions
No xrays Treat with normal protocols Modify technique for comfort Understand that the condition will likely
resolve at end of pregnancy

1st Trimester
Nausea/Vomiting: Ginger, carbonated beverages, acupressure(seabands), cold compress(throat,gastric sphincter)
Fatigue/general malaise: Nutritional counseling, food diary, prenatal vitamin, decrease stress, sleep, readjust to a new schedule
Headaches: Vascular-inc. circulatory volume & vasodilation responding to high progesterone, caffiene-withdrawl, stress, low blood sugar, muscle spasm.
– They may resolve in second trimester. Introduce stress-reduction activities, massage, heat/cold, adjustments
– Fatigue: Educate that she may have to alter daily activities such as• Move away from aerobic activity to isometric activity• Stress reduction technique• Nutritional balance

2nd Trimester
Backache: Center of gravity change resulting in muscle strain. High levels of circulating progesterone softens cartilage and loosens once-stable joints
Upper back pain: Increase breast size– Pelvic tilt exercises, core muscle strengthening,
balance exercises(theraball)– Decrease walking, girdle– Sleeping postures– Heat/cold– Massage/relaxation

Muscles cramp: phosphorus/calcium ratio, pressure on pelvic nerves and blood vessels
– R/O DVT, dehydration
– Ligament Pain: Stretching of pelvic ligaments
• Avoid twisting
• Upper Extremity discomfort: May report pain,
numbness, tingling due to postural changes and fluid retention. CTS symptoms are frequent
– Exercises: balance, core stabilizers, – Wrist splint if necessary– Educate on sleeping postures

Constipation: large amounts of progesterone cause dec. contractibility of GI tract & large intestine compressed by uterus. Bulk forming, nonnutritive laxatives, water, exercise, food suggestions, prenatal vitamins( every 2days)
Cramping: increases vascular congestion in pelvis, stretching of round ligaments, pressure from presenting fetal part.
R/O: ectopic pregnancy, miscarriage, GI problems, UTI
Varicose veins: Legs and Vulva- vasodilation from hormones
– Support hose, legs up for venous drainage-2x/day, girdle, decrease prolong standing and sitting, crossing legs
– R/O: Deep vein thrombosis
Third Trimester
Braxton-Hicks contractions: differentiate from labor contractions-grow longer, stronger, closer together at regular intervals
Edema: Sleeping on left side, Rest 2-3x/day, isometric contractions, do not wear constrictive clothing, TAKE BP EVERY VISIT
R/O: pregnancy induced hypertension
Joint aches/pains: Hormonal changes increase mobility of all joints
– SI, Sacrococcygeal, pubic, increase size of pelvis for delivery– More prone to injury
Childbirth Preparation
Three philosophies:– Grantly Dick-Read: education and relaxation
techniques to reduce fear-tension-pain cycle– Bradley: exercise to prepare muscles, relaxation
techniques, inward focusing with deep abdominal breathing to achieve labor and delivery w/o medications
– Lamaze: relaxation techniques and breathing, outward focusing, and conditioned response to relax during labor.
Postpartum
Period from delivery of the placenta and membranes to the return of the woman’s reproductive organs to their non-pregnant state.
Approx. 6 weeks Assessment: 4-6 weeks

Assessment
Ligament stability and joint alignment – Until hormones are stable– Neuro-musculo-skeletal systems are pre-pregnancy state
• Behavior• ADL: eating, sleeping, grooming• Interaction with baby
• Complications: Gestational diabetes, mastitis, thyroiditis, postpartum eclampsia or hemorrhage

Exercise guidelines
Regular routine: not sporatically Hydration: 2x normal amount Avoid high impact, excessive spinal
curve, stretch adductors Do not lie on back for more than 5 min. Toning and stretching exercises
recommended
Prohibited sports
Snow or water skiing Scuba diving Horseback riding surfing High altitude, oxygen deprivation
Exercises:– Stretching: cat/cow, side bow, standing-triangle, cow face, etc.
– Core: one arm/leg, tree, theraball
– Breathing: belly breathing, alternate nostril, legs up the wall
Adjustment options
Sleeping options
Reflexology
Vibrational therapy
Heat/ice
massage

Specific Sport-related Injury
Soccer
Most frequently added women’s sport among intercollegiate institutions
Heading– Avg six times a game– 5250 headers over a 15yr career– This repetitive impact to the skull accounts
for 4-22% all soccer injuries– Clinical manifestations range from
headache to brain damage

Types of Headers
Clearing : ball is to be projected high into the air over a long distance
Shooting: sufficient speed to elude the goalkeeper
Passing: advances the ball over a small distance
Jumping: approach by running and great accelerated force into the neck musculature
Cervical Spine Musculature
Just before impact, the muscles of the neck must stabilize the head to dissipate the effects of the contact with the ball
During execution, the head is accelerated forward by the neck musculature to generate momentum that can be transferred to the ball
Sternocleidomastoids become active before contact with the ball to generate the forward velocity of the head
Trapezius muscles remain active following impact to stabilize the head and neck system
Figure Skating
50% traumatic injuries 50% overuse injuries
– Women more frequently to the lower extremities
– Causes include inflexibility, inadequate or asymmetric strength, inappropriate warm-up or cool-down, poor diet, fatigue, overuse
Basketball(netball)
Women have 25-60% more ankle and knee injuries
Lumbar spine injuries are usually causes by contact with another player
Achilles tendon injuries due to inappropiate landing techniques
Field Hockey
One of the most common team sports in the world next to soccer
Swimming
Shoulder Impingement Syndrome Lumbar Hyperextension Injuires Cervical overuse syndromes Breaststroke: Medial collateral ligament

Specific Sport-related Injury
Soccer
Most frequently added women’s sport among intercollegiate institutions
Heading– Avg six times a game– 5250 headers over a 15yr career– This repetitive impact to the skull accounts
for 4-22% all soccer injuries– Clinical manifestations range from
headache to brain damage
Types of Headers
Clearing : ball is to be projected high into the air over a long distance
Shooting: sufficient speed to elude the goalkeeper
Passing: advances the ball over a small distance
Jumping: approach by running and great accelerated force into the neck musculature
Cervical Spine Musculature
Just before impact, the muscles of the neck must stabilize the head to dissipate the effects of the contact with the ball
During execution, the head is accelerated forward by the neck musculature to generate momentum that can be transferred to the ball
Sternocleidomastoids become active before contact with the ball to generate the forward velocity of the head
Trapezius muscles remain active following impact to stabilize the head and neck system
Figure Skating
50% traumatic injuries 50% overuse injuries
– Women more frequently to the lower extremities
– Causes include inflexibility, inadequate or asymmetric strength, inappropriate warm-up or cool-down, poor diet, fatigue, overuse
Basketball(netball)
Women have 25-60% more ankle and knee injuries
Lumbar spine injuries are usually causes by contact with another player
Achilles tendon injuries due to inappropiate landing techniques
Field Hockey
One of the most common team sports in the world next to soccer
Swimming
Shoulder Impingement Syndrome Lumbar Hyperextension Injuries Cervical overuse syndromes Breaststroke: Medial collateral ligament
Adolescence and Puberty
Adolescence: the time period from puberty to adulthood: physical, psychological, social, cognitive and emotional changes
Puberty: phase of physical development of sexual maturation and child is capable of reproduction
Puberty (Pubescence)
Physical Transformation– Breast development– Pubic hair growth– Growth spurt– Menarche– Achievement of fertility

Phases of Puberty
1. Adrenarche• Begins about 8 y/o and continues
until appox. 16 y/o.• Increased adrenal activity• DHEA/DHEAS• Secondary sexual characteristics:
responsible for pubic and axillary hair
2. Gonadarche• Begins approx. 8 y/o• Hypothalamus-Pituitary-Ovarian Axis• Primary sexual characteristics: Increased
gonadal stimulation

3. MenarcheThe first menstrual period
17% body fat necessary
22% body fat needed for ovulation
2-21/2 years after breast development

HPO Axis: Biphasic feedback system(a positive feedback mechanism)
Hypothalamus: synthesis and release of gonadotropin releasing hormone(GnRH); – Aka: luteinizing hormone releasing hormone(LHRH)
• Pituitary: GnRH(LHRH) stimulates the Pituitary to synthesize and release gonadotropins, FSH and LH
• Ovaries: FSH and LH stimulate the ovary • Results in germ cell maturation and hormone synthesis
Normal Pubertal Growth
Principal factor:
Insulin-like growth factor-I (IGF-I)GH exerts its action through this mediator.
Concerted action between GH, IGF-I, Estrogen, progesterone, and other sex hormones
** GH directly stimulates epiphyseal cartilage growth
Puberty (Pubescence)
Physical Transformation– Breast development– Pubic/Axillary hair growth– Growth spurt– Menarche– Achievement of fertility
Breast development
Budding occurs with rising levels of estrogen
1st sign of sexual development May be unilateral, often tender < 8 y/o: precocious > 13 y/o: delayed
Pubic/Axillary hair growth
Lags breast development by about 6 mths Appears late in puberty
– If first sign of puberty, may cause Hirsutism and menstrual irregularities
Growth spurts
Starts with breast development Average growth: 2-5 in/yr Sex steroids and GH contribute Increase weight: 8-20 lbs. Higher percentage of fat
Tanner Developmental Scale Sexual maturity rating, Tanner staging Pediatrics A system for objectively determining sexual maturity, which correlates chronologic age with a group of anatomic parameters, determining the degree of adolescent maturation; the most commonly used system was delineated by Tanner; in ♀, 5 stages of maturation are recorded for pubic hair and breast development; in ♂, 5 stages are recorded for pubic hair, growth of penis and testicles.
McGraw-Hill Concise Dictionary of Modern Medicine. ゥ 2002 by The McGraw-Hill Companies, Inc.
Menarche
Single most emblematic event in the transition to womanhood
Lack of menses by 16-17 y/o merits evaluation– Primary Amenorrhea– Hypothalamic immaturity (20%)– HPO axis

Achievement of fertility
Occur approx. 2-21/2 years after menses Anovulatory cycles until HPO axis matures. Secretions of GnRH are pulsatile; every 90 min FSH and LH are augmented in peaks As puberty progresses, the ovaries amplify the message
from the gonadotropins and release a greater amount of estrogen.
This cycle begins only during sleep. As the HPO axis becomes regulated, adds in the uterus in the communication link, the young adolescent will begin ovulating healthy follicles.
Ovarian Follicles
Birth: 600,000 Puberty: 300,000 Menopause: 30,000
Full maturation of one dominant follicle depends on development of support follicles, which secrete hormones such as estradiol, inhibin, and androgens, necessary for healthy HPO-U axis
Common Female Adolescence Problems
• Musculoskeletal
nutritional
Endocrine system• Dysmenorrhea
• Dysfunctional Uterine Bleeding• Eating Disorders
• Psychosocial Issues
Musculoskeletal
Rapid Growth demands– Scoliosis evaluation– “growing pains”: joint instability– Nutritional
• 2200 kcal/day(11-14y/o), 2400 kcal/day(15-18)• Protein/Calcium/Potassium/Zinc• Iron: Increased Blood volume• 1:10 overweight

Endocrine influence on musculoskeletal system– Thyroxine, insulin, corticosteroid=promote
skeletal growth– Parathyroid hormone, calcitonin, Vitamin D
• Skeletal mineralization
Parasympathetic/Sympathetic
Parasympathetic– Uterus via inferior mesenteric plexus:
sacral plexus– None to ovaries
Sympathetic– Uterus and ovaries via thoraco-lumbar
spine– Breasts via Upper - mid thoracic spine
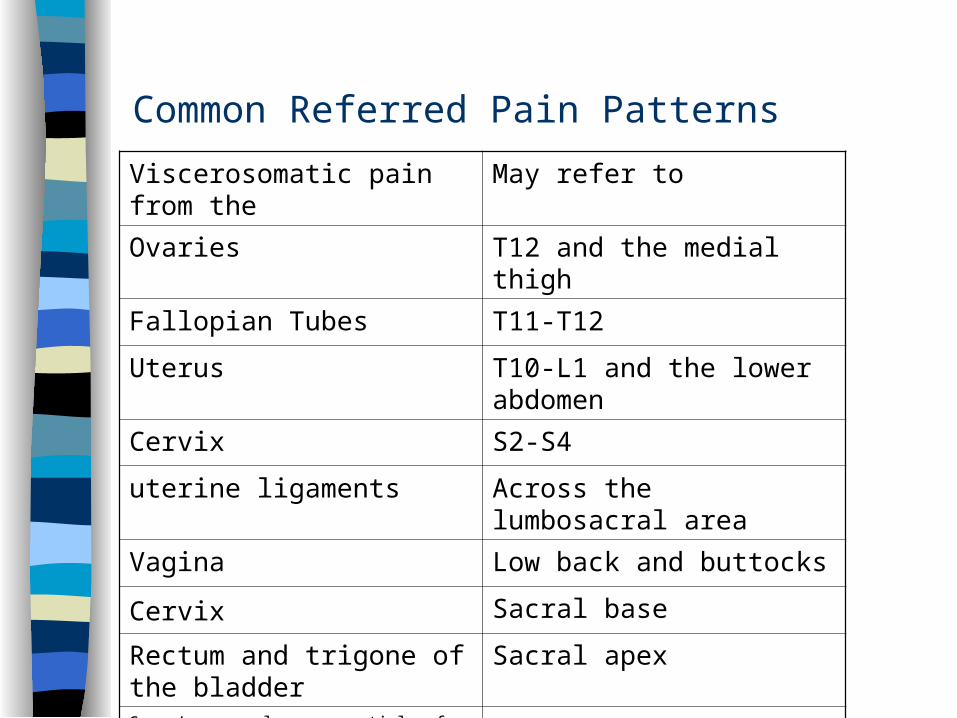
Common Referred Pain Patterns
Viscerosomatic pain from the May refer to
Ovaries T12 and the medial thigh
Fallopian Tubes T11-T12
Uterus T10-L1 and the lower abdomen
Cervix S2-S4
uterine ligaments Across the lumbosacral area
Vagina Low back and buttocks
Cervix Sacral base
Rectum and trigone of the bladder
Sacral apex
Green’s gynecology: essentials of Clinical practice, 1990

Dysmenorrhea
Severe pain or cramps in the lower abdomen during menstruation– Primary: painful menses that is not related to any
definable pelvic lesion. Primary dysmenorrhea begins with the first ovulatory cycles in women under 20
– Secondary: Painful menses that is related to the presence of pelvic lesions or pelvic disease(ie: endometriosis, fibroids, PID)

Who Gets it?
Most female adolescents and young adults
Most common reason for absences from school or work
Causes of Primary Dysmenorrhea
Increased uterine activity/forceful contractions Excessive production of vaspression Overproduction of prostaglandins(E) Cervical Stenosis Misalignment of pelvic girdle(sacrum and ilium) Ligament imbalance: Broad, Round, Uterosacral T12-L4, S2-S4 nerve intervention Other factors: diabetes, anemia, stress, low pain
threshold, increase sensitivity to pain
Causes of Secondary Dysmenorrhea Post-surgical adhesions: C-section,
episiotomy, or tears with birth Cervical stenosis due to surgery on cervix IUD cause irritation Endometriosis Fibroids PID IBS
Signs and Symptoms- Primary
Dull, midline, cramping or spasmodic lower abdominal pain
Shortly before of at the onset of menses Radiate to the lower back and inner
thighs Ancillary symptoms: nausea, diarrhea,
vomiting, headache, anxiety, fatigue
Risk Factors
Earlier age at menarche Long menstrual periods Smoking Obesity Alcohol consumption High simple-sugar diet

Treatment/Therapies for Dysmenorrhea Manipulation Massage Exercise: Stretching Rest Acupuncture Herbs: Bromelain, tumeric, cumin TENS/ IST Heat NSAIDS Dietary changes
Dietary
Omega-3 fatty acids Thiamine (vitamin B1) Calcium: 1200-1800 mg/day
– leafy veg, broccoli, sardines
Magnesium: 500 mg/day– Leafy veg, molasses, soybeans, nuts, seeds
Red Raspberry tea, chamomile
Decrease consumption:– Red meat and dairy: precursors to the
inflammatory prostaglandins via arachidonic acid
– Alcohol: liver stressor and interfere with detoxification pathways
– Caffeine: a sympathetic NS stimulator that can intensify smooth muscle contraction
– Sugar: depletes body of Ca, K, Mg, Mn

Abnormal Uterine Bleeding
Menorrhagia- abnormally heavy or prolonged bleeding during menstruation; longer than 7 days
Metorrhagia- irregular bleeding or bleeding in between cycles
Amenorrhea-absence of menses for at least 6 months
Oligomenorrhea- Infrequent menses; > 35 days Polymenorrhea- Menses occurring with abnormal
frequency
Causes of DUB: Adolescence
Immature HPO axis Anemia Eating Disorders Pregnancy

Eating Disorders
Epidemic proportions in Western Countries
9:10 are women 1.2 million women in America affected
by eating disorders The end point of social, biologic, and
individual factors Mortality rate of anorexia 8-18%
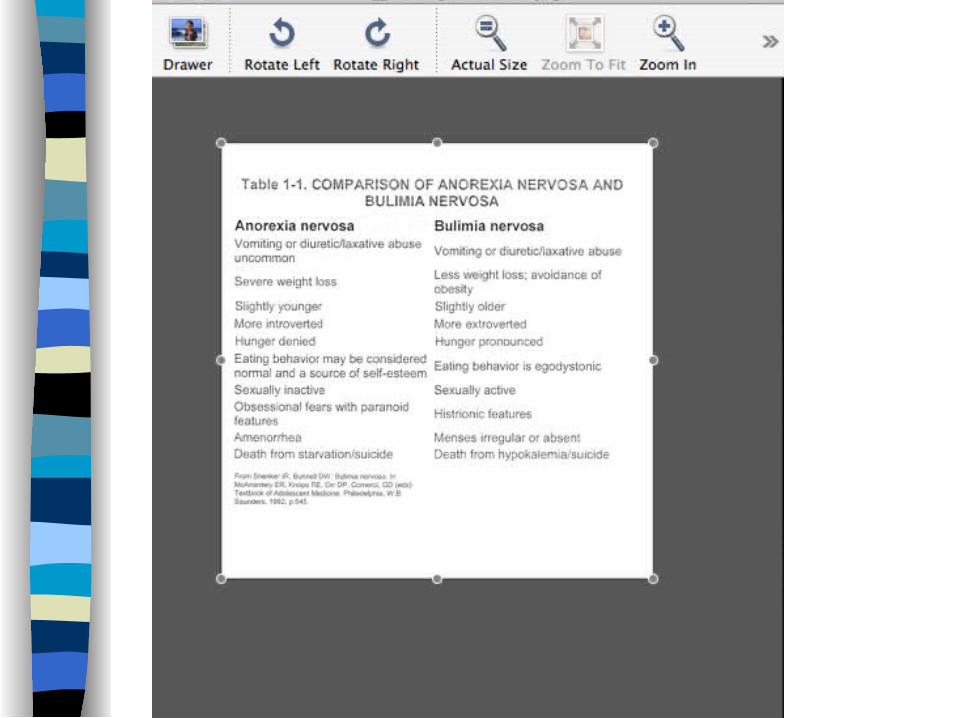
Anorexia Nervosa
Refusal to maintain body weight Body weight less than 85% of expected for
height and weight Intense fear of gaining weight Self evaluation of one’s body altered Two main clinical forms:
– Food restriction: 50% OCD– Binge/Purge: worse addictive behaviors– BOTH EXERCISE EXCESSIVELY– Peak age 14-18: stressful life event
Bulimia Nervosa
Recurrence of Binge eating– 2x/wk for 3 months = diagnosis
Purging/Non-purging Recurring compensatory behavior to prevent
weight gain– Laxatives, diuretics, excessive exercise, fasting,
vomiting Peak age 18 y/o: after diet
Etiology of Eating Disorders
Psychological factors that cause addiction to food as source of comfort
Family difficulties Irregularity in neurohormonal systems
– Serotonin Struggle with body image and sense of
identity

Anorexia, Bulimia, Obesity and Gynecological Health
Nutrition plays a key role in the growth and development of adolescents
Growth spurts: achieve 25% of adult height and 50% of adult weight
Achievement of fertility Menstrual abnormalities reflect abnormal nutrition Anorexia: hypothalamic suppression and amenorrhea;
high risk of osteoporosis Bulimia: 50% hypothalamic dysfunction and irregular
menses; less risk of osteoporosis Obesity: Anovulation and hyperandrogenism(Polycystic
ovary disease)
Pathophysiology of Eating Disorders
Anorexia– Severe caloric restriction suppresses the HPO
axis– Risk of osteopenia and osteoporosis is high
Bulimia– 50% lose their menstrual cycle– Oligomenorrhea does not appear to impact bone
density
The Adolescent Partnership
Communication– Listening skills: open “psychological” ears– Repetition and patience– Non-judgmental, motivate and inspire– Be a good role-model
Evaluation– Keep in mind the adolescent’s perspective on her health
within the context of her developmental state– At 12 y/o: adult brain is only 5% developed– Cultural issues of race, ethnicity, class, community and past
experiences

Meet the Parents
Balance the needs of the adolescent and needs of the parents
Begin Hx with parent and adolescent Find an opportunity for the parents to present
concerns away from the adolescent. Do patient education and treatment programs with
the parent and child together Find many opportunities to discuss treatment and
education with adolescent alone. At the end of every session, ask the adolescent if
there are any unanswered questions or concerns
EndometriosisEstimate 20 million women
Complications:
Pelvic Pain
Cramps
Bladder Disorders
Infertility
“Retrograde Menstrual Bleeding”
John A. Sampson, Albany NY
named disease in 1927
explained how, not why
HYSTERIAGreek for hystero = uterus
Complaints from menstrual cramps were once considered a form of hysteria
Seven Early Warning Symptoms of Endometriosis Menstrual cramps that increase in severity
over time. Intermenstrual pain, or mittelschmerz. Dyspareunia, or painful intercourse Infertility of unknown origin Bladder infections Pelvic pain History of ovarian cysts
Prostaglandins
1935. First discovered by Dr. U.S. von Euler at the Karvlinska Institute in Stockholm originally thought produced solely by prostate gland in males. Hence their name.
1957. Dr. V.R. Pickles, British physiologist at University of Sheffield studied the function of these amino-acid like hormones. He found them in uterine tissue which was a medical milestone in menstrual cramps.

F2 or (F2 Alpha)Usually kept in control by the pregnancy hormone, progesterone. If conception occurred progesterone continues to be produced and F2 is not released.
COMPLAINTS
Dysmenorrhea: painful menstruation
Dyspareunia: Painful intercourse ‘cul de sac’
Rectal bleeding: Urinate frequently, blood in urine during menstruation
FOUR BASIC CAUSES OF ENDOMETRIOSIS
Hereditary factorsImmune system stress
Hormone levelsThe embryonic theory
Before prostaglandin inhibitors were developed, it was not unusual to hear of women who became addicted to Laudanum -
tincture of opium- to relieve their pain.
Others tried Sweat baths with massage “Salt glow” rubdown of the abdominal cavity to
stimulate blood flow. ‘Galvanism’ less fearsome cousin to shock treatment Liniments, douches, decorations, poultice, brews Hemlock tea “tones uterus” (leaves and inner bark.
Now use everything from TENS unit to acupuncture.
Alternative Therapies
AcupunctureHerbs
Chinese MedicineYoga
Magnesium
100:1 with calcium in bone 3x magnesium in muscle Insomnia, nervousness, rapid heartbeat,
mm cramping Regulate body temp-last through
perspiration Cramping-Ca2+ and Mg 2+ 2:1
Potassium and Iron
RBC and muscle tissue contraction of mm,
heartbeat, nerve impulse, and body fluids
electrolyte minimum daily required
40eg kidney or cardiovascular
disorders
RBC and hemoglobin RBC lives 100 days women store=250mg men store=830 mg Ferrus gluconate ferrus sulfate
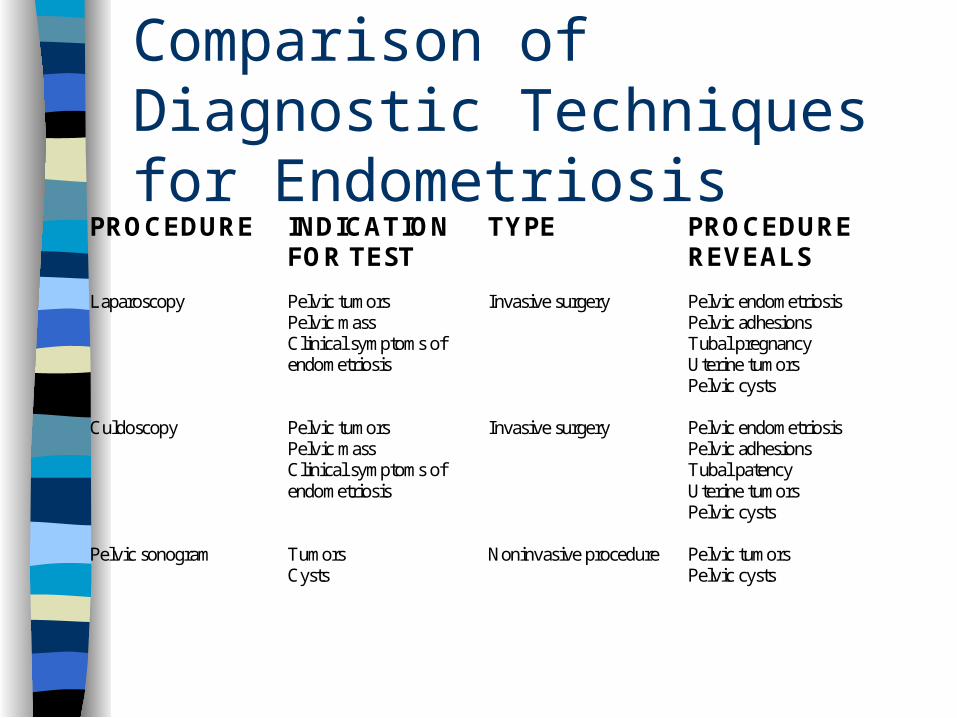
Comparison of Diagnostic Techniques for Endometriosis
PROCEDURE INDICATIONFOR TEST
TYPE PROCEDUREREVEALS
Laparoscopy Pelvic tumorsPelvic massClinical symptoms ofendometriosis
Invasive surgery Pelvic endometriosisPelvic adhesionsTubal pregnancyUterine tumorsPelvic cysts
Culdoscopy Pelvic tumorsPelvic massClinical symptoms ofendometriosis
Invasive surgery Pelvic endometriosisPelvic adhesionsTubal patencyUterine tumorsPelvic cysts
Pelvic sonogram TumorsCysts
Noninvasive procedure Pelvic tumorsPelvic cysts

Side Effects of Danocrine
Weight gain Fatigue DizzinessHeadaches Acne Mild
HirsutismDepression Rash Inc. AllergiesOily skin Bleeding Pelvic painBreasttenderness
Vaginitis Dec. Breastsize
Back pain Breast lumps Neck achesHot flashes
INFERTILITY
•After a couple has been trying to conceive over one year. (over 35 years old - 6 months). •$1 billion a year market

CAUSES OF FEMALE INFERTILITY
Pre-existing endometriosis Underactive thyroid gland Nutritional deficiencies Inappropriate body fat ratio Hormonal Imbalances Use of addictive substances Depression and stress
PREEXISTING ENDOMETRIOSIS
Alfa - v/beta 3 protein Blocks fallopian tubes or ovaries w/scar tissue Tissue produces prostaglandins , the
hormone that interferes with the release of eggs
Affects mechanism between fimbriae and the ovary
Inadequate luteal phase
HYPOTHYROIDISM
Excess Estrogen
Autoimmune processIncrease risk of
miscarriage
NUTRITIONAL SUPPORT OF THYROID
Iodine rich foods: 25 - 1,000 mcg(fish, kelp, seaweed)
Zinc: 20-60 mg(beef, oatmeal, nuts, chicken, seafood, liver, dried beans)
Copper: 2 -3 mg(liver, eggs, yeast, legumes, nuts, raisins)
Tyrosine: 300-1000mg(soy,beef, chicken, fish) B complex: 25-50mg Magnesium: up to 400mg

The Big Picture
Under weight or obesitychronic anemiaLow energy intakelow immunity
Inappropriate Body Fat Ratio
85% < or equal to ideal weight > to 120%
athleteseating disordersamenorrhea

Diet & SupplementsWomen with fertility problems should eat a whole foods diet, avoid highly processed and refined foods, and eliminate excess caffeine which can contribute to infertility.
•Vitamin C: 1,000 mg three times daily•Zinc: 20-60 mg three times daily•Magnesium: at least 400 mg daily•Vitamin B complex: 25-50 mg daily•Beta Carotene: 6mg daily•Omega 3 EFA: 3000 mg•Borage oil: 200-300 mg of gamma linolenic acid daily•Vitamin B6: 50 mg daily•Vitamin E: 400 IU daily•Folic Acid: 500mg
Hormonal Imbalances
Xenoestrogen - laden pesticides “greenhouse gases”
Detoxification protocols (liver channel flows through reproductive organs)
Birth control pills
OTHERS
Use of addictive substances
Depression & stress

Infertility Workup Barnes Basal temp test pelvic exam pap smear laparoscopy (if indicated) hysterosalpingogram progesterone test antisperm antibody test
HERBAL REMEDIES
Chastetree Berry (vitex angus - castus)
Dong quai (Angelica Sinensis)
Licorice (Glycyrrhiza glabra)
Siberian ginseng (Eleutherococcus senticosus)
PREMENSTRUAL SYNDROME (PMS)
PREMENSTRUAL DYSPHORIC DISORDER(PMDD)
Premenstrual Syndrome(PMS)
Umbrella term for a broad range of symptoms that begin after ovulation, peak before menstruation, and diminish after menses.
Premenstrual Dysphoric Disorder(PMDD)Classified in the Diagnostic and Statistical Manual of Mental Disordersas a psychiatric disorder.
Classification of SymptomsClassification of Symptoms
Somatic: water retention, pimples, intestinal disturbance, low back pain, migraines,TMJ, cold soresCognitive: lack of motor coordination, social impairment, dysphoriaEmotional: anxiety, irritability, depression, fatigue, eating habits, mood swings
CAUSES OF PMS
poor diet estrogen dominance
Under active thyroid gland exhausted adrenal glands
Food sensitivities or allergies Stress: sleep disorders nutritional deficiencies
Altered serotonin and dopamine levels
POOR DIET
•low levels of magnesium •higher percentage of total dietary calories derived from fat•Imbalance of Blood sugar
ESTROGEN DOMINANCE
bloating, weight gain, headaches, backache
diet high in estrogenic foodschronic stressPeri menopauseUnder active thyroid
UNDERACTIVE THYROID GLAND ‘HYPOTHYROIDISM’
low production of progesteroneTRH (Thyrotrophin-releasing
hormone)TSH (thyroid-stimulating
hormone) produced by pituitary gland

EXHAUSTED ADRENAL GLANDS
Chronic stress or hypothyroidism
Produce adrenaline & nor-adrenaline
Progesterone used to produce adrenal hormones
NUTRITIONAL DEFICIENCIES B6 hinders liver’s ability to metabolize
Estrogen Magnesium - chronic stress promotes
magnesium excretion, which in turn leads to fluid and sodium retention
Fiber, protein & fat
Food Sensitivities

Environmental sensitivities

stress
sleep disorders
caffeine
lack of sunlight
lack of exercise
DIETARY RECOMMENDATIONS Consume a high-complex carbohydrate diet Limit sugar to less than 10% total calories Limit protein to 15% of total calories & limit or
avoid protein from animal sources For chocolate cravers, choose moderate amounts
of low-fat chocolate foods such as cocoa made with nonfat milk & chocolate cake with no frosting
Reduce fat intake to no more than 30% of calories
DIETARY RECOMMENDATIONS (CON’T) REDUCE SATURATED FAT TO LESS THAN 10% OF
CALORIES INCLUDE ONE TO TWO TBS OF SAFFLOWER OIL IN
THE DAILY DIET. LIMIT SALT TO MINIMIZE FLUID RETENTION AND
SWELLING CONSUME SEVERAL SERVINGS DAILY OF FIBER-
RICH FOODS TO ENSURE A FIBER INTAKE RANGING BETWEEN 20 - 40 g.
AVOID CAFFEINE, ESPECIALLY WHEN ANXIETY AND BREAST TENDERNESS ARE PROBLEMS
DIETARY RECOMMENDATIONS (CON’T) Vitamin B6 supplementation (50-150mg/day)
started on day ten of the menstrual cycle and continued through day three of the next cycle has produced positive results in some women. The RDA for Vitamin B6 is 1.6 mg per day. Vitamin B6 in doses greater than 100 mg a day should be taken only with the supervision of a physician.
DIETARY RECOMMENDATIONS (CON’T) Consume at least RDA levels of
Magnesium, Iron, and the B-Complex Vitamins, and no more than 300 IU of Vitamin E (RDA is 12 IU).
Vitamin D (700 IU/day)and Calcium(1200mg/day)
L-tryptophan
WHAT YOU CAN DO TO GET RELIEF
learn stress reduction techniquesget natural lightantidepressants- st. john’s wortExerciseVitamin E (400-800 IU)Magnesium “anti stress mineral”
ALTERNATIVE MEDICINE THERAPIES FOR PMS
acupressure aromatherapy
ayurvedic medicine Yoga/stretching detoxification
Herbal remedies
PMT-Cator
Clincial measurements of symptoms
The Guy Abrahams PMS classification chart identifies four subgroups of Premenstrual Tension
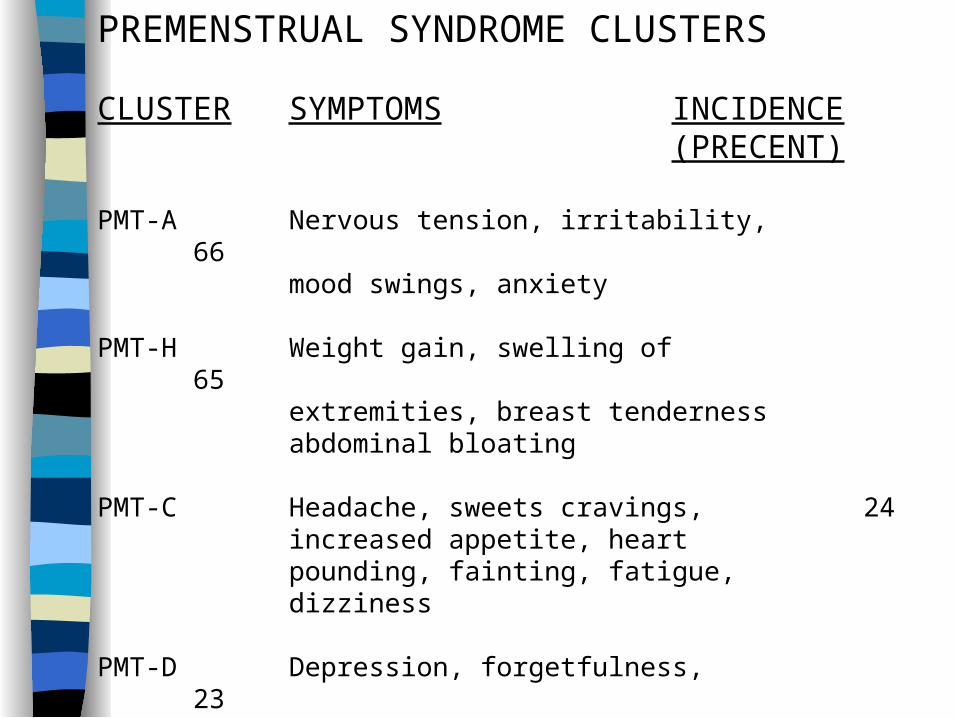
PREMENSTRUAL SYNDROME CLUSTERS
CLUSTER SYMPTOMS INCIDENCE(PRECENT)
PMT-A Nervous tension, irritability, 66mood swings, anxiety
PMT-H Weight gain, swelling of 65extremities, breast tendernessabdominal bloating
PMT-C Headache, sweets cravings, 24increased appetite, heart pounding, fainting, fatigue, dizziness
PMT-D Depression, forgetfulness, 23confusion, crying, insomnia
PMT-A
Anxiety Irritability Insomnia Hormonal Imbalance
– Estrogen is CNS stimulant– Progesterone is CNS depressant

PMT-A
Basic Dietary guidelinesB6(pyridoxine):50-100mg
Fiber: 20-40G
Reduce caffeine
Lower dairy and refined sugar
PMT - H
Hyper hydration
Breast tenderness
Abdominal bloating
Edema of face and hands
PMT-HDietary Guidelines Ginkgo Biloba 40 mg(3 times a day) Vitamin A and B6 Magnesium 200mg/day Vitamin E 150-400IU/day Decrease Sodium

PMT - C
Cravings for sweets Increased appetite Headaches Fatigue Glucose Intolerance

PMT-CMagnesium: 430 mg
B6: 100 mg lower salt and simple
carbohydratesDecrease salts and simple
carbohydratesVitamin A 200,000 - 300,000 IU
PMT - D
Depression Forgetfulness Confusion Lethargy Possible excess progesterone
PMS-D
Amino Acid L - Typtophan: 6gTyrosine 3 - 6 g
B6 Magnesium
Treatment Protocol
Adjustments Nutrition Exercise
Acupuncture Lifestyle
Homeopathic
Chiropractic Adjustments
T11 – S3: sympathetic/parasympathetic L2 produced marked decrease in
symptoms(Hubbs 1986) ROM of femur at hip joint. Adductor
and psoas major muscle hypertonic SI joints
Mosby’s Recommendation
Cramps/LBP: L2-L4 Breast tenderness: T5-T7 Fluid Retention and weight gain: T12-L1 Anxiety: T3-T7
Nutrition-Dietary Changes
• Reduce hypoglycemia: small, frequent meals
• Decrease serotonin synthesis: Eat protein
with carbohydrates
• Limit Arachidonic acid: precursor to
Prostaglandin E

• Eliminate caffeine• Limit high sugar foods
• Screen for excessive yeast• Limit salt
• Increase dietary fiber• Increase water consumption
• Limit alcohol • Increase fish oils
Supplemental Support
B complex
Vitamin B6
Magnesium
Calcium
Vitamin E
Vitamin C
Lecithin
Zinc
Flaxseed or Fish oil
Exercise
Regular Aerobic: Endorphin release
Yoga: Especially inversions and sacral region
Specific strengthening: Keigel
Homeopathic
Evening Primrose oil: lessens uterine contractions & pain, 500-1000mg/3x day
Black Cohosh: regulates hormone production, can delay onset,1-2 capsules/ 3-4hrs
Valerian: reduce anxiety, mild sedative, 1-2 capsules/ 3-4 hrs Chaste Tree Berry: helps balance estrogen/progesterone, 40
drops/day for PMS or amenorrhea Cramp bark: eases cramps,useful in cases of excessive
bleeding, 1 capsule/3-4 hrs for cramping
(dosage recommendations from Women’s Encyclopedia of Natural Health by Tori Hudson)

Lifestyle changes
Stress reduction: “relaxation response”, yoga, biofeedback
Adequate rest Schedule activities with PMS in mind No Smoking Get natural light
AYURVEDIC MEDICINEBALANCE THE DOSHAS : bodily humors (energies)
Vata - blood flow and the endometrial lining (movement)
Pitta - menstruation for hormonal changes (metabolism)
Kapha - contents of menstrual flow (structure)

•On the first day of menstruation, have a liquid diet (blended soups, juices) to aid digestion.•Avoid eggs and fermented, spicy, or sour foods.•Eat foods that are warm and easy to digest.•Eat less than usual, especially in the evening.•Avoid cheese, yogurt, red meat, fried foods, and chocolate.•Avoid carbonated beverages and cold drinks.•If you crave salt, satisfy the desire minimally, but try to resist the sugar craving or find natural substitutes such as whipped cream with honey rather than ice cream.•Take a hot shower rather than a bath.•Budget time for resting.•Reduce your exercise schedule.•Spend some time turning inward.
TRY FISH OILS FOR RELIEF OF CRAMPS
Taking as little as 6g of fish oil daily during the time of menstrual cramping can significantly reduce the pain. When 42 young women, 15 to 18 years old, took 6g of fish oil (omega-3 essential fatty acid) daily for two months for relief of menstrual pain, pain reduction was rated at 37%. The women also managed on 53% less conventional pain medication (ibuprofen) for their cramps.
AcupunctureReflexology
Pregnancy

Important Factors
Mechanical stress variations Hormonal Considerations
– Relaxin, pregnanediol and estriol Patient comfort Boundary Issues Nutritional Support

Musculoskeletal Conditions
Low back pain Tension cephalgia Altered gait Chronic neck and back
fatigue Intercostal neuralgia Groin Pain Thoracic Outlet
Syndrome Symphasis Pubis Pain
Sciatic neuralgia Coccygodynia Herniated IVD Carpal tunnel syndrome DeQuervian
tenosynovitis Osteonecrosis of
femoral head
Common Complaints
Bleeding Gums Dehydration Breathing Difficulties Diastasis Recti Abdominis Dizziness/Light-headedness Fluid Retention Symptom Heartburn In Utero Constraint (Webster technique) Morning Sickness Tipped Uterus (Buckled Sacrum Maneuver) Snoring
Serious Issues
Gestational Diabetes Pre-eclampsia/Toxemia Premature Contractions Rhesus Factor Spontaneous Abortion(Miscarriage)
Etiologies
Sleep disturbances
Lack of Exercise
Microtrauma
Emotional State
Viral infection
Chemical Imbalance (GH, Serotonin)
Autoimmune(RA)

Nutrition for the Childbearing Years
A women’s nutritional status before and during pregnancy and during lactation helps determine the outcome of her pregnancy and the long term health of herself and her child.
Maternal nutrition during pregnancy & lactation influence:
development of braincomposition and size of the
bodyinfant’s metabolic competence
to handle nutrientsmother’s future health
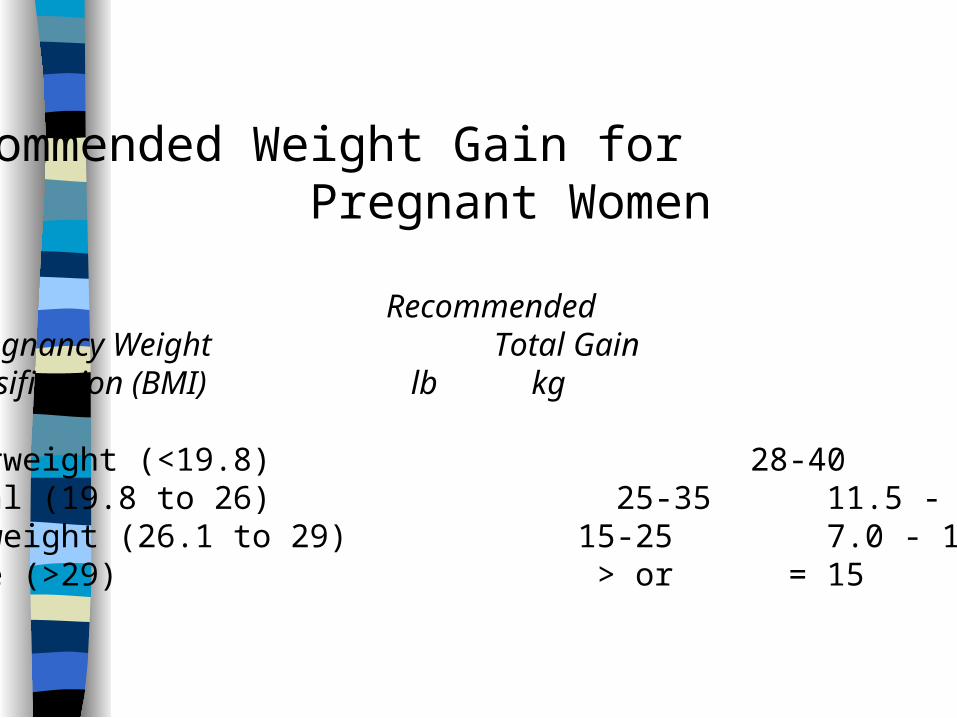
Recommended Weight Gain for Pregnant Women
RecommendedPrepregnancy Weight Total Gain classification (BMI) lb kg
Underweight (<19.8) 28-40 12.5 - 18Normal (19.8 to 26) 25-35 11.5 - 16Overweight (26.1 to 29) 15-25 7.0 - 11.5Obese (>29) > or = 15 > or = 7
Energy Requirements
1st trimester 96 k cal/day (2115)
2nd trimester 265 k cal/day (2275)
3rd trimester 430 k cal/day (2356)
Macronutrients & Micronutrients
The quality of the maternal diet is as
important as its quantity.
ProteinRequirements= 60 g/day
20% increase over nonpregnant level
Greatest concerns are low levels of:•iron•calcium•zinc•folic acid
IronIron deficiency anemia is a serious condition during pregnancy. It is
associated with preterm delivery and increased maternal mortality.
RDA pregnant (30 mg)non pregnant (15 mg)
• rapid expansion of maternal blood volume
•deposition of iron in fetal tissues
Heme Iron•found in food of animal origin•absorbed at a rate of 15 -30%
Non-Heme Iron•found in food of plant origin•absorbed at a rate of 5%
Vegetarian
Avoidance of red meat but consumption of fish and/or chicken
lacto - ovo: no meat consumption but intake of dairy products
vegans: no consumption of food of animal origin.
(Macrobiotic diet included)
Foods High in Calcium(Recommended Intake 1, 000 mg/day)
Milk & Dairy Products Calcium (mg)yogurt, plain, nonfat (1 cup) 452yogurt, fruit flavored, low fat (1 cup) 345chocolate milkshake (1 cup) 256skim milk (1 cup) 302whole milk (1 cup) 285cheddar cheese (1 oz) 204American cheese (1 oz) 174ice cream, soft serve (1 cup) 206ice cream, hard serve (1 cup) 170cottage cheese (1 cup) 154
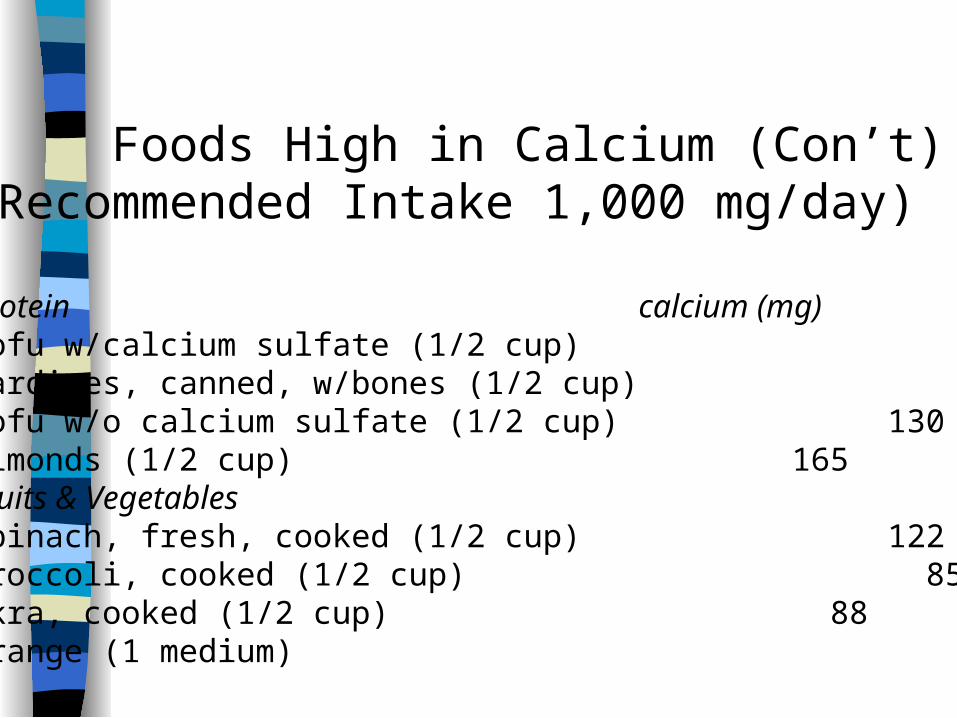
Foods High in Calcium (Con’t)(Recommended Intake 1,000 mg/day)
Protein calcium (mg)tofu w/calcium sulfate (1/2 cup) 434sardines, canned, w/bones (1/2 cup) 428tofu w/o calcium sulfate (1/2 cup) 130almonds (1/2 cup) 165Fruits & Vegetablesspinach, fresh, cooked (1/2 cup) 122broccoli, cooked (1/2 cup) 85okra, cooked (1/2 cup) 88orange (1 medium) 54
ZINC
crucial for tissue growth deficiency can cause poor fetal growth deficiency common because Zinc is
found in the same foods as Iron & Calcium
RDA pregnant 20 mg
non pregnant 15 mg

Plant Sources of Zinc
wheat germnuts
dried beans
Folic Acid
most important vitamin during pregnancy
all cell divisionDNA synthesis
Recommended Daily Allowances
adults 230 mgchildbearing years 400 mg
pregnancy 800 mg
Folic Acid
5-10 mg fruitsvegetablescheesemilkeggs
100-150 mg liverorange juicespinach
DeficiencyNeural tube defects in the fetus
megaloblastic anemia in mother
Vitamin A
excess is teratogenicretinol
Beta Carotene is not
Smoking Highest % of Low Birth Weight Babies
#1 obese smokers who gained
< or = 15 lbs
#2 normal weight smokers who gained
< or = 25 lbs
Hellerstedt, Hines, Story,
Altm & Edwards (1997)
Caffiene
does cross the placentabreast milkhalf life higher in pregnancy -
11 hoursinfants (100 hrs)
Pregnancy Test
Urine• HCG: hormone called human chronic Gonadotropin
• 26 -36 days after last menstrual period
• 8 -10 days after conception
A positive result usually indicates pregnancy. Only two-thirds of women with ectopic pregnancies will have positive pregnancy tests.Positive results also occur in :
(a) choriocarcinoma(b) hydatidiform mole(c) testicular tumors(d) chorioepithelioma(e) chorioadenoma destruens(f) conditions w/a high ESR such as
acute salpingitis(g) cancer of lung, stomach, colon, pancreas,
and breast

Interfering Factors
1.False-negative tests and falsely low levels of HCG may be due to a dilute urine (low specific gravity) or a specimen obtained too early in pregnancy.
2. False-positive tests are associated with(a) proteinuria(b) hematuria(c ) presence of excess pituitary
gonadotropin (HLH) as in menopausal women
(d) drugs1. Anticonvulsants2. Antiparkinsons3. Hypnotics4. Tranquilizers
Obstetric Sonogram Confirming pregnancy facilitating amniocentesis determine fetal age multiple pregnancy fetal development is normal fetal viability localizing placenta masses postmature pregnancy
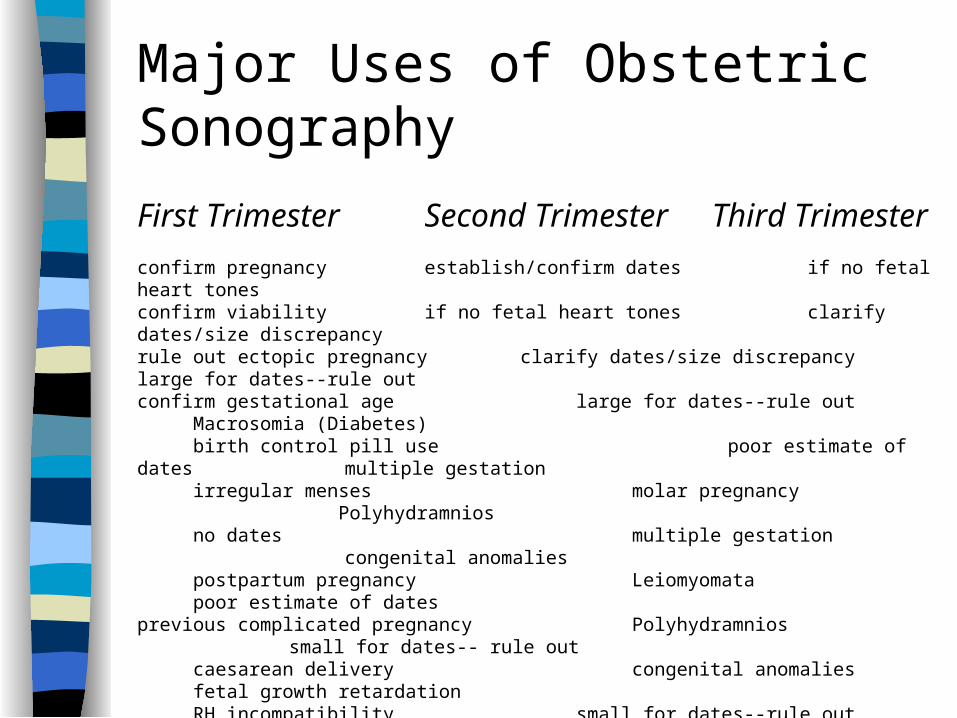
Major Uses of Obstetric Sonography
First Trimester Second Trimester Third Trimester
confirm pregnancy establish/confirm dates if no fetal heart tonesconfirm viability if no fetal heart tones clarify dates/size discrepancyrule out ectopic pregnancy clarify dates/size discrepancy large for dates--rule outconfirm gestational age large for dates--rule out Macrosomia (Diabetes) birth control pill use poor estimate of dates multiple gestation irregular menses molar pregnancy Polyhydramnios no dates multiple gestation congenital anomalies postpartum pregnancy Leiomyomata poor estimate of datesprevious complicated pregnancy Polyhydramnios small for dates-- rule out caesarean delivery congenital anomalies fetal growth retardation RH incompatibility small for dates--rule out Oligohydramnios diabetes mellitus poor estimate of dates congenital anomalies fetal growth retardation fetal growth retardation poor estimate of dates
congenital anomalies Oligohydramnios
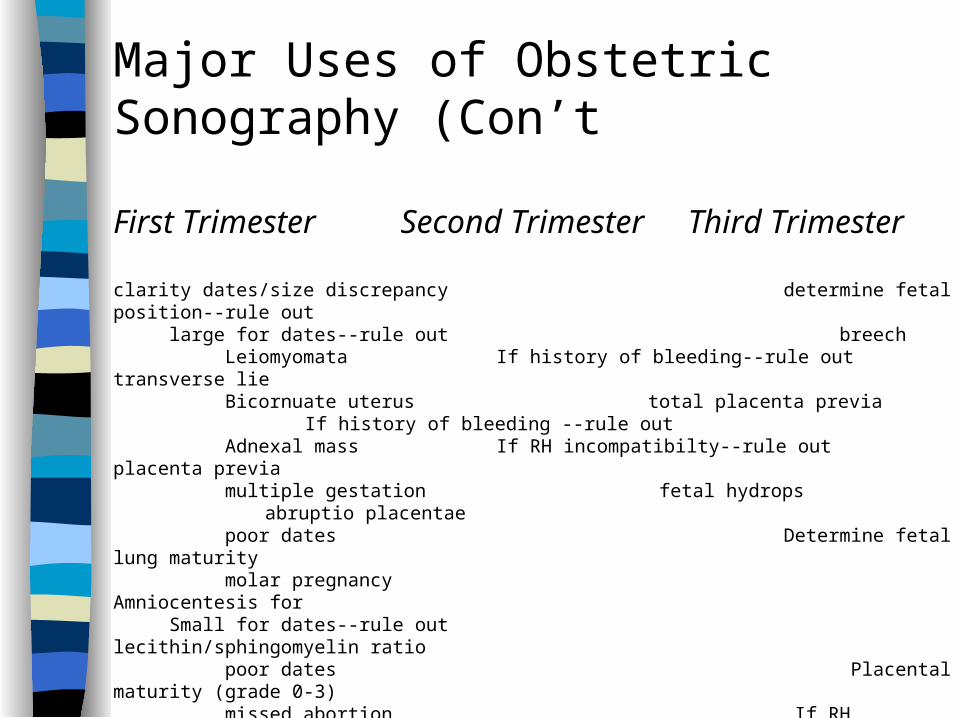
Major Uses of Obstetric Sonography (Con’t
First Trimester Second Trimester Third Trimester
clarity dates/size discrepancy determine fetal position--rule out large for dates--rule out breech Leiomyomata If history of bleeding--rule out transverse lie Bicornuate uterus total placenta previa If history of bleeding --rule out Adnexal mass If RH incompatibilty--rule out placenta previa multiple gestation fetal hydrops abruptio placentae poor dates Determine fetal lung maturity molar pregnancy Amniocentesis for Small for dates--rule out lecithin/sphingomyelin ratio poor dates Placental maturity (grade 0-3) missed abortion If RH incompatibility--rule out blighted ovum fetal hydrops
RUBELLA ANTIBODY TEST
Induce IgG IgM antibody formation infection in 1st trimester associated with
congenital abnormalities, miscarriage or stillbirth Elisa Test (enzyme immunoassay or enzyme linked immunoassay)

TESTS DONE TO PREDICT NORMAL FETAL OUTCOME AND IDENTIFY FETUS AT RISK
FOR INTRAUTERINE ASPHYXIA
Name of Test & Normal Values
Breast Stimulation Test (BST)Normal values: reactive; negativeImplies that placental support is adequate and that the fetus is probably able to tolerate the stress of labor should it begin within a week. There should be a low risk of intrauterine death due to hypoxia.
Reason for Performing Test
After 26 weeks’ gestation, the nipples are stimulated to release oxytocin that causes uterine contractions similar to labor contractions.
1
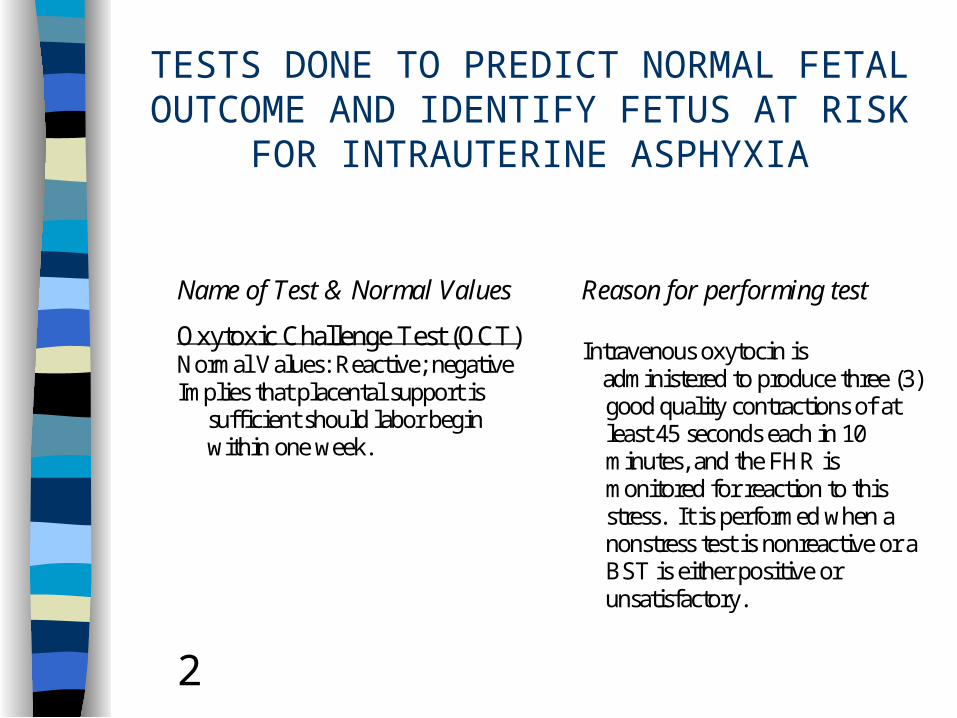
TESTS DONE TO PREDICT NORMAL FETAL OUTCOME AND IDENTIFY FETUS AT RISK
FOR INTRAUTERINE ASPHYXIA
Name of Test & Normal Values
Oxytoxic Challenge Test (OCT)Normal Values: Reactive; negativeImplies that placental support is sufficient should labor begin within one week.
Reason for performing test
Intravenous oxytocin is administered to produce three (3) good quality contractions of at least 45 seconds each in 10 minutes, and the FHR is monitored for reaction to this stress. It is performed when a nonstress test is nonreactive or a BST is either positive or unsatisfactory.
2

TESTS DONE TO PREDICT NORMAL FETAL OUTCOME AND IDENTIFY FETUS AT RISK
FOR INTRAUTERINE ASPHYXIA
Name of Test & Normal Values
Acoustic StimulationNormal Values: Reactive
Reason for performing test
Using an electronic fetal monitor and sound source on the maternal abdomen, an evaluation of fetal movement in response to stimulation is done.
Nonstress testNormal Values: Reactive; at least two (2) episodes of fetal movement associated with a rise in FHRProvides a baseline status & implies an intact CNS and autonomic N-S that are not being affected by intrauterine hypoxia
It determines fetus’ ability to respond to environment by an increase in FHR associated with movement where not under the stress of labor.
3
Amniocentesis
hematologic disorders fetal infections
inborn errors of metabolism sex linked disorders
identification of chromosomal abnormalities neural tube defects such as:
-anencephaly -encephalocele -spina bifida
-myelomeningocele
estimation of fetal age wellbeing of fetus
pulmonary maturity
HIGH-RISK PARENTS WHO SHOULD BE OFFERED PRENATAL DIAGNOSIS
1. Women of advanced maternal age (35 or over). 90% fall in this category; at risk for children with chromosome abnormality, especially trisomy 21 (at age 35 to 40, the risk for Down’s is 1% to 3%; at age 40 to 45, there is a 4% to 12% risk; and over age 45, the risk is 12% or greater.2. Women who have previously borne a trisomic child, or clients who previously had a child with any kind of chromosome abnormality.3. Parents of previous child with spina bifida or anencephaly or family history of neural tube disorders.4. Couples in which either parent is a known carrier of a
balanced translocation chromosome for Down syndrome.
HIGH-RISK PARENTS WHO SHOULD BE OFFEREDPRENATAL DIAGNOSIS (CON’T)
5. Couples, of which both partners are carriers for a diagnosable metabolic or structural autosomal recessive disorder. Presently, over 70 inherited metabolic disorders can be diagnosed by amniotic fluid analysis.6. Couples, of which either partner or a previous child is affected with a diagnosable metabolic or structural dominant disorder.7. Women who are presumed carriers of a serious x-linked disorder.8. Couples and families whose medical history reveals mental retardation, ambiguous genitalia, parental exposure to environmental agents (drugs, irradiation, infections).9. Couples and families whose medical history reveals multiple miscarriage or stillbirths, infertility.10. Anxiety about potential offspring.
CLINICAL IMPLICATIONS
1. Elevated level of alpha-fetoprotein is an indicator of possible neural tube defects.2. Creatinine levels are reduced in prematurity.3. Increased and decreased total volume of amniotic fluid is associated with certain developmental arrests.4. Increased bilirubin levels are associated with impending fetal death.5. Color changes of fluid are associated with fetal distress and other disorders.6. Sickle cell anemia and thalassemia can be detected by examination of fibroblast DNA obtained by amniocentesis.
CLINICAL IMPLICATIONS (Con’t)
7. X-linked disorders are not routinely diagnosable in utero. However, because they affect only males, the sex of the fetus may be determined in a woman who is a carrier of a deleterous x-linked gene, as in hemophilia or Duchenne’s muscular dystrophy.8. Cystic fibrosis.9. The presence of some of the over 100 detectable metabolic disorders.10. For disorders in which an abnormal protein is not expressed in amniotic fluid cells, other test procedures are necessary, such as DNA restriction endonuclease analysis.
HERPES
Natrum Mutriaticum (Chloride of Sodium)
Pica
Calcarea Carbonica (Carbonate of lime)
Nitricun Acidum (Nitric Acid)
LACTATION:
The greatest physiologicalstress of the
life cycle
Fatty acid composition of human milk is influenced by the
maternal diet.
Fatty acids are responsible for nerve & brain development
in the infant.
• Protein Requirements = Pregnancy (60 g/day)• Iron Requirements drop (15 mg/day)• Mineral content of Milk (Ca 2+, Mg 2+, K +2, Na 2+ ) are not affected by maternal diet• Vitamin Content is dependent on maternal dietary intake. (esp. B6, thiamine, folic acid)• Weight loss is experienced by 80% lactating women• Aerobic exercise does not affect breast milk volume or composition
BEST-ODDS NURSING DIET
Increase the caloric intake to about 500 calories per day over the pregregnancy requirements.
Increase calcium requirement to five servings per day.
Reduce protein intake to three servings per day Drink at least eight glasses of fluids (milk, water,
broths or soups, and juices); take more during hot weather and if perspiring a lot.
Splurge occasionally.
Lactation
Protein requirements: 60g/day Iron: 15 mg/day Mineral content of milk not affected by maternal
diet Vitamin content is dependent on maternal
dietary intake Weight loss experienced by 80% lactating
women Aerobic activity does not affect breast milk
volume or composition
Benefits of physical fitness
Good muscle tone Sense of well-being
Sense of body control Best physical shape for labor and delivery
Reduced anxiety an dfrustration
Improved sleep
Weight control Body fat deposition to a minimum
Improve chances for easier labor
Improved self image
Treatment Protocol
Manipulation: decrease 2nd tri, inc. 3rd tri Massage(caution in severe edema-
toxemia) Heat/ice (no modalities) Foot reflexology/cranial sacral Peppermint, ginger, papaya Meridian stimulation
Stress Injury to Bone: Interactive model
Mechanical factor
Hormonal Influence
Nutritional environment
Genetic Predisposition
Definition of Stress Injury
Stress injury to a bone occurs on a continuum, ranging from normal bone remodeling/repair to frank cortical fractures. Terms such as bone strain and stress reaction are used to reflect this progression of bone injury toward a frank cortical stress fracture, which is defined as a partial or complete fracture of a bone resulting from its inability to withstand nonviolent stress that is applied in a rhythmic, repeated, sub threshold manner
Bone Biology overview

Extrinsic Mechanical Factors
Acute change in training regimen– Duration, intensity, frequency)
Footwear age Fitness level: early fatigue of muscles Running Surface/terrain
– Uneven: hills, roads– Hard/soft
Intrinsic Mechanical Factors
Tibial Bone width– Large compression and
tension forces – The external forces
exceed the tibia’s intrinsic resistance strength
– Narrow mediolateral tibial width have less resistance to these forces(area moment of inertia)
Foot Structure– Pes cavus(high arch)
absorbs less stress and transmits greater force to the tibia and femur
– Pes Planus(flexible, low arch) absorbs greater metatarsal force
Hormonal Factors
Delayed Menarche Hypothalamic hypoestrogenic Amenorrhea Ovulatory Disturbances Oral Contraceptive Pills Testosterone
Nutritional Factors
Low Calcium Intake
Vitamin D Genetics
Inadequate Calories
Anorexia Nervosa
Common Sites for Fractures
Pubic Ramus Femoral Neck Femoral Shaft
Patella Tibia Medial Malleolus
Tarsal Navicular
Fifth Metatarsal
Sacrum

Topics in Women’s Health
Chiropractors are ‘Port of Entry’Women account for nearly twice as many outpatient visits as menNIA, office of research on Women’s Health 1990’sNCCAM: National Center for Complementary and Alternative medicine(COGME) Fifth Report on Women and Medicine The Council on Graduate Medical Education

What is Port of Entry Care
Provide evaluation of comprehensive health needs and coordinate care
Involves integrated, accessible health services that addresses most of an individual’s needs, regardless of problem type or organ system
PCP’s are assumed to be competent in initial evaluation of all problems with which patients present.

What are the needs?
POE’s: internists, general practitioners– Pap smear– Preventative tests– Evaluation of symptoms, DDX, ROF, Refer• Chiropractors:
• Preventative tests• Evaluation of symptoms, DDX, ROF, Refer• Port of Entry for non-allopathic therapy
Women’s Education
Mass media: print, television, radio– One study: 90% women reported the media as
main source of information about mammography• How do they report in compared to :
• Medical journal articles• Women’s greatest health risks• Most commonly expressed health concerns
http://www.nlm.nih.gov/medlineplus/womenshealth.html
Resources
http://www.cdc.gov/women/index.htm
http://womenshealth.gov/topics.cfmwww.shirleys-wellness-cafe.com/women.htm
http://www.healthy.net/www.cogme.gov/rpt5_4.htm

Paradigm shift
Historical, medical research has been based on the 70-kg man. Efforts to acknowledge the biological differences.
Women’s participation in the medical profession has risen dramatically. Female Osteopathic physicans increased 36% between 1989-1992. The trend has been on a continuous rise.
Demand by consumers and policy makers for increased attention to women’s health issues.