ANTENATAL DIAGNOSIS OF ADRENOCORTICAL HYPERPLASIA
1
732 newborn infant indeed resembles patients with Wilson’s disease in having a high level of copper in the liver and a diminished ability to synthesise caeruloplasmin. With the metal stopcocks further potential hazards were residual dried blood, and a white turbidity which was thought to be due to silicone grease. In view of these results, replacement of metal stopcocks for exchange transfusions by disposable plastic stopcocks or exchange-transfusion sets is advocated. Children’s Medical Research Foundation, Royal Alexandra Hospital for Children, Sydney, New South Wales 2050. JEANETTE BLOMFIELD. ANTENATAL DIAGNOSIS OF ADRENOCORTICAL HYPERPLASIA SiR,-Jeffcoate el aLl have suggested that it is justifiable to examine the amniotic fluid before term for 17-oxosteroid and pregnanetriol content in the hope of achieving early detection of adrenocortical hyperplasia in the foetus of a mother who has already given birth to an affected child. Apart from the drawbacks associated with the sampling procedure, the results obtained would now appear to be inconclusive,2 and there are distinct advantages if the diagnosis can be made from analysis of pregnancy urine. It has been our contention for some years that adrenocortical hyperplasia in the foetus is likely to cause increased excretion of oestrogens during preg- nancy, just as foetal adrenocortical hypoplasia entails a very low oestrogen excretion.3 The opportunity to test this hypo- thesis has only recently arisen, and the results in the first case are so striking that they seem worthy of mention. A woman, aged 30 years, had had two previous pregnancies. The first child was a virilised girl, and congenital adreno- cortical hyperplasia due to 21-hydroxylase deficiency was diagnosed in the neonatal period. A second girl was entirely normal. Urine specimens were collected during the third pregnancy, which ended with delivery in the 37th week of gestation of a second affected child weighing 4-1 kg.-again a virilised girl, with an enlarged clitoris with the opening of the urogenital sinus at its base. On the 9th day of life the 24-hour urinary steroid excretion was as follows: 17-oxosteroids 2-8 mg., 17-hydroxycorticosteroids (Few) 5-8 mg., Porter-Silber chromogens 0-65 mg., pregnanetriol (gas-liquid chromato- graphy, upper limit of normal in the laboratory 0-1 mg. per 24 hours) 0-63 mg., and 11-oxopregnanetriol 0-29 mg. At the age of 1 month the hydrocortisone secretion during stimula- tion with corticotrophin was 5-02 mg. per 24 hours, or 20-1 per sq. m. per 24 hours. The mother’s oestriol excretion at 26, 29, and 34 weeks of gestation is shown in the accompanying figure, in which it is compared with the normal values established in the same laboratory 4: all the values, 26,500 ug., 32,400 ug., and 58,870 ug. per 24 hours, respectively, were clearly higher than the upper limit of the normal range. Dr. Mary Coyle’s normal values for oestrone and cestradiol-17B excretion in pregnancy are to be published elsewhere.5 In this pregnancy, the oestrone-excretion values at 26, 29, and 34 weeks, com- pared with the corresponding values for pregnancy associated with a normal foetus weighing more than 2-95 kg. at term, were (normals ±S.D. in parentheses) 532 (730 ±360), 1930 (700 ±410), and 1746 (610 ±440), fLg. per 24 hours, respec- tively. The oestradiol-17p excretion values were (normals ±S.D. in parentheses) 601 (200±100), 420 (180±90), and 1137 (220 90), ug. per 24 hours, respectively. These results strongly suggest that the diagnosis of con- 1. Jeffcoate, T. N. A., Fliegner, J. R. H., Russell, S. H., Davis, J. C., Wade, A. P. Lancet, 1965, ii, 553. 2. Merkatz, I. R., New, M. I. Excerpta med. int. Congr. Ser. 1968, 157, 175. 3. Cathro, D. M., Coyle, M. G. ibid. 1967, 132, 688. 4. Coyle, M. G., Brown, J. B. J. Obstet. Gynœc. Br. Commonw. 1963, 70, 226. 5. Cathro, D. M. in Pædiatric Endocrinology (edited by D. Hubble); p. 218. Oxford, 1969. (Eestriol excretion of mother of foetus with adrenal hyperplasia. Asterisks represent values given in text. genital adrenocortical hyperplasia may be made before birth by the standard urinary oestriol assay, which is widely available. Several cases will be required to prove the point but, in the meantime, it is suggested that the urine of mothers at risk should be routinely assayed for oestriol. I.N.S.E.R.M., Unite de Recherches, D. METHVEN CATHRO Hopital Debrousse, Lyon 5e, France. JEAN BERTRAND. Department of Obstetrics and Gynaecology, University of Dundee, Scotland. MARY G. COYLE. DISINFECTION OF VENTILATORS BY ULTRASONIC NEBULISATION SIR,-It was a pleasure to read the article by Dr. Judd and his colleagues. 1 We have also been investigating various methods of decontaminating inhalation therapy equipment; and we have arrived at essentially the same conclusions as Judd et al. We further believe this approach, utilising ultrasonic nebulisa- tion of hydrogen peroxide, has broader medical application for disinfection. We must disagree with the conclusions of Dr. Spencer and his group. 2 It has been theoretically determined that the particle size generated by ultrasonic nebulisers bears the following relationship to surface tension, density, and operating frequency: D cz yl/a . 1 . 1 D "(1/.. pI I.. F2/. where: D=particle diameter, y=surface tension, p=density, F= operating frequency. On the basis of these relationships, we question whether the appreciable difference of the particle size developed by the L.K.B. nebuliser and by the DeVilbiss and Monaghan units reported by Spencer is not actually due to different methods of measurement. The most important physical factors determining nebulisa- tion-rate for a given nebuliser are viscosity and vapour pressure. Tests conducted here have indicated that the DeVilbiss ultra- sonic nebuliser (contrary to Dr. Spencer’s findings) can nebulise 1. Judd, P. A., Tomlin, P. J., Whitby, J. L., Inglis, T. C. M., Robinson, J. S. Lancet, 1968, ii, 1019. 2. Spencer, G., Ridley, M., Eykyn, S., Achong, J. ibid. p. 1144.
Transcript of ANTENATAL DIAGNOSIS OF ADRENOCORTICAL HYPERPLASIA

732
newborn infant indeed resembles patients with Wilson’sdisease in having a high level of copper in the liver and adiminished ability to synthesise caeruloplasmin. With the metalstopcocks further potential hazards were residual dried blood,and a white turbidity which was thought to be due to siliconegrease.
In view of these results, replacement of metal stopcocks forexchange transfusions by disposable plastic stopcocks or
exchange-transfusion sets is advocated.Children’s Medical Research Foundation,Royal Alexandra Hospital for Children,
Sydney, New South Wales 2050. JEANETTE BLOMFIELD.
ANTENATAL DIAGNOSIS OF ADRENOCORTICAL
HYPERPLASIA
SiR,-Jeffcoate el aLl have suggested that it is justifiable toexamine the amniotic fluid before term for 17-oxosteroid andpregnanetriol content in the hope of achieving early detectionof adrenocortical hyperplasia in the foetus of a mother whohas already given birth to an affected child. Apart from thedrawbacks associated with the sampling procedure, the resultsobtained would now appear to be inconclusive,2 and thereare distinct advantages if the diagnosis can be made fromanalysis of pregnancy urine. It has been our contention forsome years that adrenocortical hyperplasia in the foetus is
likely to cause increased excretion of oestrogens during preg-nancy, just as foetal adrenocortical hypoplasia entails a verylow oestrogen excretion.3 The opportunity to test this hypo-thesis has only recently arisen, and the results in the firstcase are so striking that they seem worthy of mention.A woman, aged 30 years, had had two previous pregnancies.
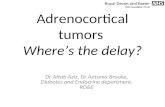
The first child was a virilised girl, and congenital adreno-cortical hyperplasia due to 21-hydroxylase deficiency wasdiagnosed in the neonatal period. A second girl was entirelynormal. Urine specimens were collected during the thirdpregnancy, which ended with delivery in the 37th week ofgestation of a second affected child weighing 4-1 kg.-again avirilised girl, with an enlarged clitoris with the opening of theurogenital sinus at its base. On the 9th day of life the 24-hoururinary steroid excretion was as follows: 17-oxosteroids 2-8mg., 17-hydroxycorticosteroids (Few) 5-8 mg., Porter-Silberchromogens 0-65 mg., pregnanetriol (gas-liquid chromato-graphy, upper limit of normal in the laboratory 0-1 mg. per24 hours) 0-63 mg., and 11-oxopregnanetriol 0-29 mg. At theage of 1 month the hydrocortisone secretion during stimula-tion with corticotrophin was 5-02 mg. per 24 hours, or 20-1per sq. m. per 24 hours.The mother’s oestriol excretion at 26, 29, and 34 weeks of
gestation is shown in the accompanying figure, in which it iscompared with the normal values established in the same
laboratory 4: all the values, 26,500 ug., 32,400 ug., and
58,870 ug. per 24 hours, respectively, were clearly higher thanthe upper limit of the normal range. Dr. Mary Coyle’snormal values for oestrone and cestradiol-17B excretion in
pregnancy are to be published elsewhere.5 In this pregnancy,the oestrone-excretion values at 26, 29, and 34 weeks, com-pared with the corresponding values for pregnancy associatedwith a normal foetus weighing more than 2-95 kg. at term,were (normals ±S.D. in parentheses) 532 (730 ±360), 1930
(700 ±410), and 1746 (610 ±440), fLg. per 24 hours, respec-tively. The oestradiol-17p excretion values were (normals±S.D. in parentheses) 601 (200±100), 420 (180±90), and1137 (220 90), ug. per 24 hours, respectively.These results strongly suggest that the diagnosis of con-
1. Jeffcoate, T. N. A., Fliegner, J. R. H., Russell, S. H., Davis, J. C.,Wade, A. P. Lancet, 1965, ii, 553.
2. Merkatz, I. R., New, M. I. Excerpta med. int. Congr. Ser. 1968, 157,175.
3. Cathro, D. M., Coyle, M. G. ibid. 1967, 132, 688.4. Coyle, M. G., Brown, J. B. J. Obstet. Gynœc. Br. Commonw. 1963, 70,
226.5. Cathro, D. M. in Pædiatric Endocrinology (edited by D. Hubble);
p. 218. Oxford, 1969.
(Eestriol excretion of mother of foetus with adrenal hyperplasia.Asterisks represent values given in text.
genital adrenocortical hyperplasia may be made before birthby the standard urinary oestriol assay, which is widely available.Several cases will be required to prove the point but, in themeantime, it is suggested that the urine of mothers at riskshould be routinely assayed for oestriol.
I.N.S.E.R.M., Unite de Recherches, D. METHVEN CATHRO
Hopital Debrousse, Lyon 5e, France. JEAN BERTRAND.Department of Obstetrics and Gynaecology,
University of Dundee, Scotland. MARY G. COYLE.
DISINFECTION OF VENTILATORS
BY ULTRASONIC NEBULISATION
SIR,-It was a pleasure to read the article by Dr. Judd andhis colleagues. 1 We have also been investigating variousmethods of decontaminating inhalation therapy equipment; andwe have arrived at essentially the same conclusions as Judd et al.We further believe this approach, utilising ultrasonic nebulisa-tion of hydrogen peroxide, has broader medical application fordisinfection.We must disagree with the conclusions of Dr. Spencer and
his group. 2 It has been theoretically determined that the
particle size generated by ultrasonic nebulisers bears the
following relationship to surface tension, density, and operatingfrequency:
D cz yl/a . 1 . 1D "(1/.. pI I.. F2/.where: D=particle diameter, y=surface tension, p=density, F=
operating frequency.On the basis of these relationships, we question whether theappreciable difference of the particle size developed by theL.K.B. nebuliser and by the DeVilbiss and Monaghan unitsreported by Spencer is not actually due to different methods ofmeasurement.
The most important physical factors determining nebulisa-tion-rate for a given nebuliser are viscosity and vapour pressure.Tests conducted here have indicated that the DeVilbiss ultra-sonic nebuliser (contrary to Dr. Spencer’s findings) can nebulise1. Judd, P. A., Tomlin, P. J., Whitby, J. L., Inglis, T. C. M., Robinson,
J. S. Lancet, 1968, ii, 1019.2. Spencer, G., Ridley, M., Eykyn, S., Achong, J. ibid. p. 1144.