Antenatal Care in Poor Countries MCH in Developing Countries January 2009 Stephen Gloyd.
53
Antenatal Care in Poor Countries MCH in Developing Countries January 2009 Stephen Gloyd
-
date post
21-Dec-2015 -
Category
Documents
-
view
217 -
download
0
Transcript of Antenatal Care in Poor Countries MCH in Developing Countries January 2009 Stephen Gloyd.

Antenatal Care in Poor Countries
MCH in Developing CountriesJanuary 2009
Stephen Gloyd

Antenatal Care 2
Antenatal Care Initiatives
MAKING PREGNANCY SAFER (WHO) Reduce maternal mortality 75% by 2015 SAFE MOTHERHOOD INITIATIVE (WHO-1988)“Four Pillars” Family planning Prenatal care Clean birth Essential obstetric services at referral level
(including availability of transport)
And…Improvement of womens' status

Antenatal Care 3
IMPORTANCE OF ANTENATAL CARE
reduce high perinatal risk reduce high maternal risk (50x) major point of access to health care for
women

Antenatal Care 4
Access to antenatal care
Physical access Time and/or distance to facility Economic costs & barriers Cultural and social factors Quality of care

Antenatal Care 5
Trends in Antenatal care 1990-2000

Antenatal Care 6
Estimates of the proportion of pregnant women who received some antenatal care (1996)

Antenatal Care 7
Number of visits to ANC by region

Antenatal Care 8

Antenatal Care 9

Antenatal Care 10

Antenatal Care 11
Antenatal care and delivery

Antenatal Care 12
Timing of ANC visits (most in 1st trimester except Africa)

Antenatal Care 13
Estimates of the proportion of deliveries attended by skilled personnel (1996)

Antenatal Care 14
Prenatal care vs attended birth and post partum care

Antenatal Care 15
Components of prenatal care:
Health education Screening Diagnosis and treatment Referral
Screening/Dxo Identify women at high risko Intervene to prevent development of problemso Dx and Rx pre-existing medical conditionso Dx and Rx complications of pregnancy

Antenatal Care 16
Perinatal Morbidity and Mortality
LBW Birth trauma, obstructed labor Infection
amnionitis herpes gonorrhea syphilis streptococcus HIV Tetanus
Abruptio Placenta Congenital malformations "other" (30%)

Antenatal Care 17
Maternal Morbidity and Mortality
(Five main causes) Hemorrhage Sepsis Eclampsia Obstructed Labor Abortion Note: Mortality reduction requires secondary
and tertiary care

Antenatal Care 18
Other Causes of Maternal Morbidity and Mortality
Hypertension Diabetes Heart Disease Hepatitis Anemia Malaria Tuberculosis STDOverall Morbidity: 3-12% of all pregnancies
(up to 37% in India)

Antenatal Care 19
Poor outcomes: 3465 birth registries
in 30 hospitals of Cote d’Ivoire (1997)
Condition Rate per 1000Normal 760
Stillbirth 44
Neonatal death 6
LBW < 2500g < 2000g <1500g
190 52 17
Eclampsia 2
Fetal disproportion 13
Fetal distress 15
Hemorrhage 22
Maternal deaths 2
Others 12
Operative delivery 36

Antenatal Care 20
Prevalence of low birth weight globally

Antenatal Care 21

Antenatal Care 22
Sexually transmitted infections (STI) among pregnant women in Mozambique

Antenatal Care 23
Preventability
Overall Infant Deaths - 33% preventable (Nairobi)
Syphilis: 100% preventable 10% stillbirths 20% Infant Mortality 20% Congenital Syphilis
Other causes: % preventable not clear

Antenatal Care 24
Risk Approach
Identification of high risk factors Predictive (Previous fetal loss) Contribution (Grand multipara, young or old) Causation (syphilis, HIV, maternal
malnutrition)

Antenatal Care 25
Risk Approach
Not an effective ANC strategy because: Complications cannot be predicted—all pregnant women
are at risk for developing complications
Risk factors are usually not direct cause of complications
Many “low risk” women develop complications
Have false sense of security
Do not know how to recognize/respond to problems
Most “high risk” women give birth without complications
Thus, an inefficient use of scarce resources

Antenatal Care 26
WHO working group on prenatal care 1994
PNC should be individualized Part of overall, functional system Midwife usually most appropriate Include empowerment
WHO Antenatal Care Randomized Trial(Villar et al 2001)
Manual for the Implementation of the New Model

Antenatal Care 27
Current state of Prenatal Care 2008
Too many interventions Poor quality of care for interventions that work Need to focus on a FEW interventions based on
epidemiology
Interventions that are cheap and effective pMTCT (HIV screening and prophylaxis)
Malaria IPT (Intermittent Preventive Therapy)
Syphilis screening and Rx Iron therapy Tetanus immunization Family planning Nutritional supplementation

Antenatal Care 28
Other interventions that need more study
STD identification and treatment Routine anti parasite drugs Waiting houses Diabetes screening (depends on prevalence) Management and treatment of HTN

Antenatal Care 29
HIV in pregnancy
Prevention of HIV transmission (pMTCT) Opt-in vs opt out Single dose Niverapine vs AZT vs HAART Efficiency of treatment
Care for HIV positive mother during pregnancy Special nutritional needs Social needs, stigma
HAART in pregnancy Toxicity (NVP, AZT) Patient flow and adherence

Antenatal Care 30
Prevention of Mother to Child Transmission of HIV (pMTCT)
Short term ARVs reduce transmission by > 50% AZT vs Nevirapine Cost-effectiveness based on prevalence Effectiveness depends on adequate follow up of women
HIV+ to counseling Links between prenatal care and hospital
Implementation Not necessary to wait until everything is in place Important to involve PLWAs Community consultation critical Counselors need training Mothers need support and follow up (including psychosocial) Works best in conjunction with HAART

Prevention and Control of Malaria during Pregnancy

Antenatal Care 32
Effects of Malaria on Pregnant Women
All pregnant women in malaria-endemic areas are at risk
Parasites attack and destroy red blood cells
Malaria causes up to 15% of anemia in pregnancy
Can cause severe anemia
In Africa, anemia due to malaria causes up to 10,000 maternal deaths per year

Antenatal Care 33
Malaria Prevention and Treatment during Pregnancy
Focused antenatal care (ANC) with health education about malaria
Use of insecticide-treated nets (ITNs)
Intermittent preventive treatment (IPT)
Case management of women with symptoms and signs of malaria

Antenatal Care 34
Active Syphilis Infection in Pregnancy
Adverse outcome in 50-70% of infected pregnancies In sub-Saharan Africa, prenatal syphilis positivity
varies between 4-16% (average ~ 9%) In Zambia & Malawi, 26-42% of stillbirths attributable
to prenatal syphilis 8% of IMR due to syphilis Screening is effective & inexpensive
Basic Screening Test (RPR) costs US$0.25-0.35, takes 15-20 minutes
Treatment: 3 doses (1 per week) of Benzathine Penicillin at US$1.00 per dose
Estimated screening of women in ANC in Africa - 38% Obstacles: cost, organization of services Missed opportunities for screening >1 million
Antenatal Care 35
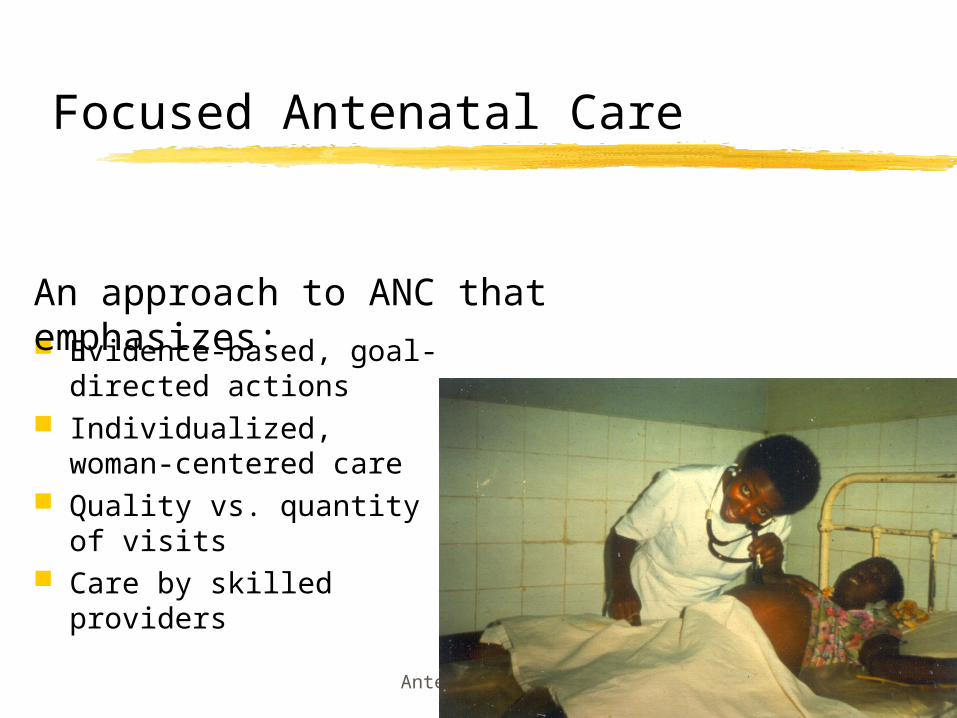
Focused Antenatal Care
Evidence-based, goal-directed actions
Individualized, woman-centered care
Quality vs. quantity of visits
Care by skilled providers
An approach to ANC that emphasizes:

Antenatal Care 36
Goal of Focused Antenatal Care
To promote maternal and newborn health and survival through:
Early detection and treatment of problems and complications
Prevention of complications and disease
Birth preparedness and complication readiness
Health promotion

Antenatal Care 37
No Longer Recommended
Numerous, routine visits Burden to women and healthcare system
Routine measurements and examinations: Maternal height and weight Ankle edema Fetal position before 36 weeks
Care based on risk assessment

Antenatal Care 38

Antenatal Care 39
Focused Antenatal Care Services (cont’d.)
Care by a skilled provider who:
Has formal training and experience
Has knowledge, skills, and qualifications to deliver safe, effective maternal and newborn healthcare
Practices in home, hospital, health center
May be a midwife, nurse, doctor, clinical officer, etc

Antenatal Care 40
Focused Antenatal Care Services (cont’d.)
Individualized, woman-centered care based on each woman’s:
Specific needs and concerns
Circumstances
History, physical examination, testing
Available resources

Antenatal Care 41
Focused Antenatal Care Services (cont’d.)
Quality vs. quantity of ANC visits: WHO multi-center study
Number of visits reduced without affecting outcome for mother or baby
Recommendations Content and quality vs. number of visits Goal-oriented care Minimum of four visits

Antenatal Care 42
Activities within PNC
Minimum of 4 visits (see table)
Individualized delivery plan depending on risk profile
One PNC visit at referral hospital
Health promotion (to individual and community)
Emergency transport

Antenatal Care 43
First visit: By 16 weeks or when woman first thinks she is pregnant
Second visit: At 24–28 weeks or at least once in second trimester
Third visit: At 32 weeks
Fourth visit: At 36 weeks
Other visits: If complication occurs, followup or referral is needed, woman wants to see provider, or provider changes frequency based on findings (history, exam, testing) or local policy
Scheduling and Timing of ANC Visits

Antenatal Care 44
Basic components of the WHO antenatal care program (1994)

Antenatal Care 45

Antenatal Care 46
Problems with interventions (general):
Utilization is variable
Gestation at first visit (after sixth month)
Variable epidemiology of risk factors (Malaria, eclampsia, Anemia, pelvic size)
Cultural barriers identification of pregnancy, taboosreluctance to use family planning
Limitations of referral and transport
Sensitivity and specificity of risk factors

Antenatal Care 47
Inadequate health systems
Emergency obstetric care (EOC) requires - Surgical facilities Anesthesia Blood transfusion Manual delivery tools (VE, forceps) Medical treatment (HTN, Sepsis, shock) Family Planning

Antenatal Care 48
Safe childbirth care

Antenatal Care 49

Antenatal Care 50
Impact of Traditional Birth Attendant training in Rural Mozambique (1)
MOH established a TBA program in
Goals: reduce maternal and infant mortality & improve utilization of primary health care
Over 8 years MOH trained >300 TBAs - supported by quarterly supervision, basic equipment, and annual refresher courses
Surveys showed TBAs improved their knowledge of obstetric emergencies and skills in how to manage them
An evaluation was planned to assess whether the program had met its initial goals (1995)

Antenatal Care 51
Impact of Traditional Birth Attendant training in Rural Mozambique (2)
A retrospective cohort study
Comparison of maternal and newborn outcomes in
40 communities where TBAs had been trained
27 communities where TBAs had not yet been trained.
In each community –respondents interviewed in 30 households closest to the trained TBA (or center of the community with no trained TBA) with pregnancies in the past 3 years
Principal outcomes utilization of TBA or health facility services (delivery and ANC)
outcome of pregnancy for mother and child
utilization of other primary health care services
Antenatal Care 52
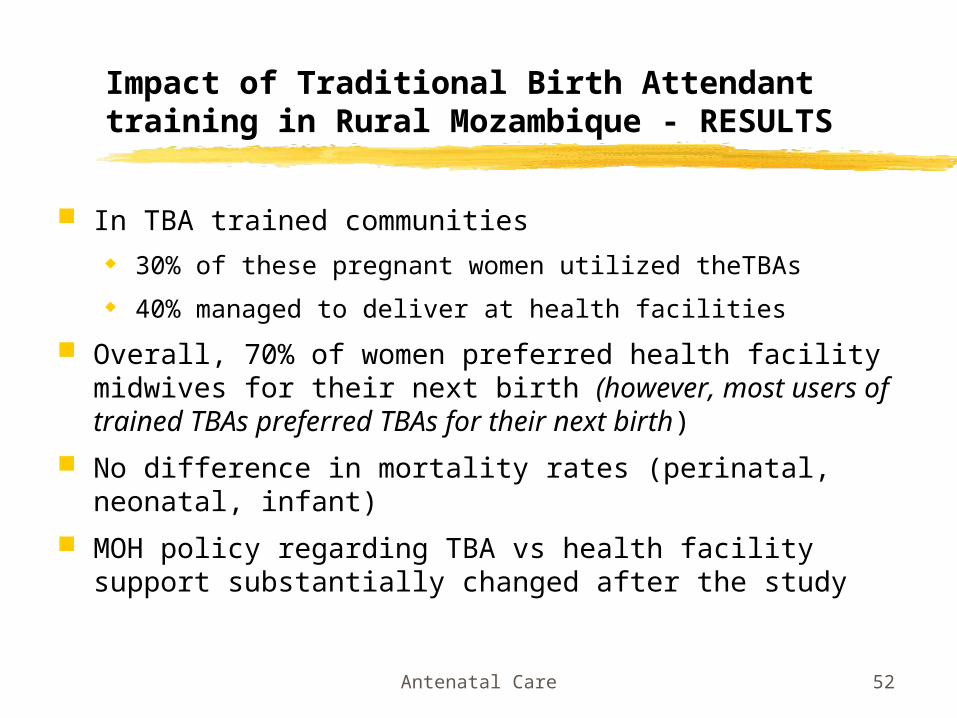
Impact of Traditional Birth Attendant training in Rural Mozambique - RESULTS
In TBA trained communities 30% of these pregnant women utilized theTBAs
40% managed to deliver at health facilities
Overall, 70% of women preferred health facility midwives for their next birth (however, most users of trained TBAs preferred TBAs for their next birth)
No difference in mortality rates (perinatal, neonatal, infant)
MOH policy regarding TBA vs health facility support substantially changed after the study

Antenatal Care 53
Some operational issues – prenatal and birth care
Malaria in pregnancy (done by Paula Brentlinger?)
pMTCT (prevention of mother to child transmission of HIV
Antenatal syphilis screening in Mozambique
Traditional birth attendant training