Anorectal Malformation- Ayat5

of 48
-
Upload
paulhaddon-muetebi -
Category
Documents
-
view
135 -
download
2
Transcript of Anorectal Malformation- Ayat5
Anorectal malformationsBy Matovu Paul & Ntambi Rogers Moderator Dr. Sekabira
Headlines
Anal Anatomy Embryology of the imperforate anus Definition Incidence Classification Approach Prognosis Photos!!
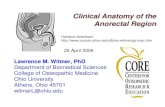
Anal Anatomy
Anorectal malformationsThe cloacaSeparated into:(which is a common chamber into the hindgut and allantois)
The bladder
post-allantoic gut (rectum) Proctadeum (epiplastic bud)
Downward growth of a septum
Fusion during the 3rd month of intrauterine lifewhen there is imperfect fusion imperforate anus
The spectrum of anorectal malformations ranges from simple anal stenosis to the persistence of a cloaca; incidence ranges from 1 in 4000 to 5000 live births and is slightly more common in boys. The most common defect is an imperforate anus with a fistula between the distal colon and the urethra in boys or the vestibule of the vagina in girls.
By 6 weeks of gestation, the urorectal septum moves caudally to divide the cloaca into the anterior urogenital sinus and posterior anorectal canal. Failure of this septum to form results in a fistula between the bowel and urinary tract (in boys) or the vagina (in girls). Complete or partial failure of the anal membrane to resorb results in an anal membrane or stenosis. The perineum also contributes to development of the external anal opening and genitalia by formation of cloacal folds, which extend from the anterior genital tubercle to the anus.
CON`T
The perineal body is formed by fusion of the cloacal folds between the anal and urogenital membranes. Breakdown of the cloacal membrane anywhere along its course results in the external anal opening being anterior to the external sphincter (i.e., anteriorly displaced anus).
Imperforate anus
Includes agenesis and atresia of the rectum and anus Etiology: unknown Incidence: 1 in 4,500 SEX: 60% male
Imperforate anusLow abnormalitiesTermination of bowel below the pelvic floor Easy to Dx Simple to ttt Outlook is good 1)Covered anus 2)Ectopic anus 3)Stenosed anus 4)Membranous stenosis
High abnormalitiesTermination of bowel above the pelvic floor Often have a fistula into the urinary tract with deficient pelvic floor Difficult to ttt 1)Anorectal agenesis 2)Rectal atresia 3)cloaca
Low abnormalities
1)Covered anusAnal canal covered by a bar of skin with a track running forwards to the perineal raphe. This track is called Bucket Handle midline Raphe fistula.
2)Ectopic anusAnus situated anteriorly in , it opens in perineum in , it opens in vulva(more commonly)>> (rare)
vulval ectopic anus
or vagina
3)Stenosed anusi.e. microscopic anus There is a minute opening that can be seen if examined carefuly
4)Membranous stenosis
Rare Anus is
normally sited covered with a thin membrane that bulges with retained meconium
High abnormalitiesCould be associated with:a fistulas connection between the blind rectal stump and the bladder or other pelvic structures abnormalitie
1)Anorectal agenesis
Rare Blind rectal pouch lies just above the pelvic floor In anterior aspect attached to the bladder & often there is a rectovesical fistula or rectourethral fistula (manifested by passage of gas or meconium in the urine) or perineal fistula In fistula to the posterior fornix >> rectovestibular (or rectovaginal) low RVF easy to correct postop. Function is good high RVF difficult to correct postop function is poor
2)Rectal atresia
Rare Anal canal is normal but ends blindly at the level of pelvic floor & the rectum also ends blindly above the pelvic floor without a fistulas opening.
3)cloaca
Occurs only in Bowel, urinary & genital tracts all open into a common wide cavity Commonly associated with other developmental abnormalities e.g. tracheoesophagial fistula
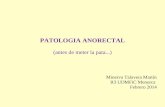
Approach
History >>> the systems involved Examination >>> DDx Investigation >>> Dx Management
History
Failure to pass meconium within the 1st 24 hours of life. Patients with anterior ectopic anus may present in childhood or in adulthood. These patients have lifelong histories of constipation and painful defecation and usually have required laxatives or enemas for management.
ExaminationInspection alone is sufficient for management plan in 90% of patients. ?High LowBucket handle defect Gas/meconium from perineum Perineal fistula if skin bridge between vestibule and fistula. Anterior ectopic anus i.e. normal sized anus surrounded by normal muscle. Urine free of meconium(NB average of 20 hrs for meconium to appear in urine).
Flat bottom Short sacrum Little muscle contraction Meconium per urethra Rectovestibular fistula if within mucosal margin of the vestibule. Sphincter located close to the scrotum or bifid scrotum often associated with a Prostatic Fistula. Cloacae are often missed if urethral opening is not identified in female with a recto-vaginal fistula. Furthermore, cloacae often have small openings and may be a cause of referral for ambiguous genitalia.
Differential Diagnosis of Conditions That May Be Associated with Failure to Pass Meconium in the Newborn
Hirschsprung's disease >>Tight anus, empty rectum, transition zone Meconium plug syndrome >> Meconium plugs Meconium ileus >> Abdominal distention at birth, cystic fibrosis Anorectal malformation >> Absent anus, tight anus or fistula Small left colon syndrome >>Transition zone* at splenic flexure Hypoganglionosis >> Transition zone* Neuronal intestinal dysplasia type A >>Transition zone*, mucosal inflammation Neuronal intestinal dysplasia type B >> Megacolon Megacystis-microcolon-intestinal hypoperistalsis syndrome >> Microcolon, megacystis
*--Transition zone (from small- to large-diameter bowel) refers to radiographic visualization on contrast study.
InvestigationVery Important to:1. Exclude other anomalies!! 2.Determine whether abnormality is high or low!!
1. Exclude other anomalies!!Anal atresia may occur as a part of the VACTERL group of anomalies V Vertebral body segmentation defect A Anal atresia C Cardiovascular (PDA, VSD) TE Tracheo esophagial fistula R unilateral Renal agenesis L Limb anomaly (radial ray hypoplasia)
So, very careful examination of the baby must be made to exclude these anomalies
Associated abnormality "V" Vertebral Abnormality (butterfly vertebrae, hemi-vertebrae) "C" Cardiac, Heart Abnormality Cardiac ECHO (VSD, ASD, PDA)
Investigation Spinal ultrasound, Spinal x-ray Cardiac ECHO
"R" Renal, Kidney abnormality (solitary Renal ultrasound, Voiding cystokidney, horse shoe kidney) urethra-gram (VCUG) "TE" tracheoesophogeal abnormality (TEF) "L" Limb deformity Physical examination Physical examination, x-rays
2.Determine whether abnormality is high or low!!1)Invertogram:with a metal button or a coin strapped to the site of the anus or a metal bougie inserted into the blind anal canal Infant is held upside down for 3-4 minutes Then radiograph in the inverted lateral position ( both the greater trochanters should be on the same line) The gas in the rectum will rise to the top indicates the distance between the site of the metal indicator and the blind end of the rectum >>> if the distance > 2.5 cm, the abnormality is high!! if the rectum ends above the PC line (pubococcygeal line = from the symphysis pubis to the last vertebra), the abnormality is Low & vise versa or according to ischeal line (between ant.-sup. Iliac spines). When to be done? Although it is a useful method, sometimes vitiated by a plug of meconium in the rectum causing an apparent gap far in excess of that actually present. So, it may be necessary to wait until the baby is 24 hrs old before rectal gas appears
Metal button
PC line
gas in the rectum
2)Urine culture:Presence of meconium Presence of proteus or pseudomonas usually signifies that a fistula is present
3)US:To evaluate the lesion type
4)MRI:If we suspected complex malformation
5)Micturating cystourethrogram:By injecting a dye in the urethra
Treatment of Low abnormalities:1)Covered anus: The track should be opened by scissors Followed by routine dilatation of the anus 2)Ectopic anus: Plastic cut-back operation 3)Stenosed anus: Regular dilatation
Treatment of High abnormalities:Very difficult problem & each case must be considered on its merits The possibilities are: Two-stage operation: 1st stage laparotomy Division of rectourethral fistula Transverse colostomy 2nd stage rectal pull-through operation One-stage operation: laparotomy Division of fistula pull-through operation Division of fistula & rectal pull-down operation through the perinum ( know rarely used)
Cont. Treatment of High abnormalities:
The new technique is post-sagittal rectoplasty (PSARP) colostomy only ( for cloaca)
Pull-through operation
Lower bowel is mobilized New passage is created through the pelvic floor by passing a pair of curved forceps & through it, keeping close to the urethra, to the site of the future anus. This is dilated by Hegars dilator so that the bowel can be pulled down and its mucosa stitched to the skin of the newly formed anus. Daily dilatation will be required for at least 3 mo. after the operation and it may be necessary for years.
PSARPPublished by Dr. Albeto Pea >> It is assumed that theinnervation to the sphincter mechanism is paired and meets in the midline. The PSARP dissection is along the midline providing excellent exposure with minimal trauma to nerves and musculature.
It involves: Stimulation of muscles to demonstrate the midline and sphincter Posterior sagittal incision - length depends on severity of abnormality and required extent of dissection Rectum identified. Abdominal approach may be required in addition in 10% of males and 40% of cloacae Rectum dissected Separation from genitourinary tract Repositioning the neoanus within the sphincteric mechanism
Position for PSARP
Incision in PSARP
Posterior sagittal repair of a rectovestibular fistula .
PrognosisIn high % of cases, imperforate anus is associated with other congenital abnormalities especially of the urinary organs & nearly 50% of deaths in cases of imperforate anus are due to other malformations
IN a Summary
1 opening >>> Cloaca 2 openings >>> anorectal agenesis with rectovaginal fistula 3 openings >>> ectopic anus, stenosed anus, membranous anus, rectal atresia or even normal anus!!! The most important investigation is the invertogram It is very important to rule out other anomalies The best & the newest operation is PSARP
Cloaca
Anorectal agenesis and rectovestibular fistula.
Anourethral fistula
imperforate anus and a rectoperineal fistula .
imperforate anus and a bucket-handle malformation
Covered anus
Thank you!!
References:
Bailey & Loves short practice of surgery (24th edition) The management of ARM course companion Cinncinatti childrens hospital medical center (2007) University of Michigan, Section of Pediatric Surgery Clinical picture from Emedicine website & Cinncinatti CHMC.