
Annual Report and Accounts - NHS Lothian · nhs lothian annual report and accounts for the year...
106
Annual Report and Accounts Year ended 31 st March 2017
Transcript of Annual Report and Accounts - NHS Lothian · nhs lothian annual report and accounts for the year...

Annual Report and Accounts
Year ended 31st
March 2017

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
2
INDEX PAGE
Annual Report 3
Section A: The Performance Report
Overview
Performance Analysis
3 3
14
Section B: The Accountability Report
Corporate Governance Report - Directors report - Statement of Health Board Members’ Responsibilities in
respect of Accounts - Statement of Chief Executive’s Responsibilities as the
Accountable Officer of the Health Board - The Governance Statement
Remuneration and Staff Report
Parliamentary Accountability Report
25 25 25
27
30 31 40 53
Independent Auditor’s Report 54
Accounts’ Primary Financial Statements 57
Notes to the Accounts 62
Accounts Direction 105
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
3
ANNUAL REPORT SECTION A: THE PERFORMANCE REPORT
1. Overview
a) Statement from the Chief Executive on the Performance of the NHS Board 2016/17 was an exciting and challenging year for NHS Lothian. There have been many examples of improvements and achievements by NHS Lothian, services and teams, and individuals in the year. Improvements and achievements by NHS Lothian, services and teams, and individuals in the year. These have all been achieved while continuing to provide our broad range of services and managing immediate financial pressures. The opening section of Section 2 – Performance Analysis provides a summary of those achievements. Over the past year a significant number of key property developments have moved forward. The £48 million Phase One redevelopment of the Royal Edinburgh Hospital campus is completed, with patients moving into their new accommodation from June 2017. Within our acute hospitals we delivered expanded critical care and a new £3.75m renal and transplant high dependency unit at the Royal Infirmary of Edinburgh, and at St John’s Hospital in Livingston we are investing £3.35m in increased theatre capacity for ophthalmology and hand surgery. Construction of the new £150 million Royal Hospital for Sick Children and Department of Clinical Neurosciences has continued over the last year; handover of the building is planned for Autumn 2017 with services moving in by Spring 2018. In May 2016 construction started on the £28 million Bundle Programme which will see health and council partnership centres built as revenue funded projects through HUB South-East Ltd in Firrhill and North West Edinburgh, Blackburn, West Lothian. These will be opening by the end of 2017. New GP premises in Ratho and Leith Walk, and upgrades in Loanhead and Prestonpans, are all underway. Construction works have commenced for the new East Lothian Community Hospital; the facility has a phased handover programme with full occupation planned for 2021. Acknowledging the need to continue to invest in our facilities, the Board is planning significant developments for the re-provision of the Princess Alexandra Eye Pavilion, the Edinburgh Cancer Centre and Phase 2 of the Royal Edinburgh Hospital. The ever-present challenges within the health system will always require us to pursue continuous improvement. There are Local Delivery Plan standards which NHS Lothian is not meeting, and an example of this is waiting times where performance deteriorated during the year. The Board had previously decided to stop using the independent sector for largely financial reasons. In response to this situation, trajectories were developed based on detailed Demand, Capacity, Activity and Queue work, with regular review to evaluate performance. Towards the end of the year the Board agreed to invest £6m in the use of the independent sector to help improve access waiting times for out-patients until the end of March 2017, recognising this was using non-recurring money and did not offer a sustainable solution. Robust oversight and governance arrangements have been further focused to measure the positive impact of this additional capacity. Further clinically lead work has been deployed to support improved communication with waiting patients and improved triage to minimise the clinical impact of additional waiting time on patients. This triage work is currently being tested in Gastro-Intestinal services, and any effective models arising from this will be rolled out across other specialties. I would like to acknowledge the hard work of all of the Board’s staff, and thank them for all their efforts which allow us to continue to provide safe, effective, person-centred care. Developing Organisational Culture and Leadership Over the past 5 years we have undertaken a lot of work to develop the organisation’s culture, and a recent internal audit report acknowledged the significant progress that has been made in this regard, after following up on the actions

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
4
raised in two Scottish Government commissioned reviews into waiting times management and organisational culture. You can find all internal audit reports on the Board’s website. http://www.nhslothian.scot.nhs.uk/OurOrganisation/KeyDocuments/Audits/Pages/default.aspx The development of the organisational culture has been supported through the delivery of training and development. In June 2014, NHS Lothian selected CMP Resolutions to work in partnership and develop the way the organisation responds to and manages conflict between staff. Broadly the aims were to recruit and train mediators, support the establishment of a mediation service and build the skills of a cadre of managers to manage conflict better at source. We have now trained 4 cohorts and have 26 mediators trained in two-party mediation and of those 9 mediators who can undertake group mediation. In 2016 the Mediation Service was contacted about 27 possible mediations of which 20 allocated and 15 went to joint mediation. There have also been 3 group mediations this year. Additionally the Mediation Co-ordinator resolved a number of referrals through coaching conversations. In addition to offering mediation as a way to provide an alternative approach to conflict and dispute resolution, NHS Lothian engaged CMP Resolution to deliver training to managers to develop skills to have more robust conversations in line with our Values into Action. Workshops have been provided with participation from a wide range of people. In 2016/17 the training was rolled out as part of the University Hospitals and Support Services Development Programme for senior managers with 90 managers participating. In my 2015/16 statement I reported that I have also introduced a revised way of working amongst my corporate management team with a smaller core group of three directors working with me to take collective responsibility for transforming the performance of the whole system, applying particular focus to quality, cost and performance. During 2016/17 we have taken the next steps to further develop our culture and leadership model. The fundamental challenge facing the leadership team is how to address the fact that the growth in demand is outstripping the growth in resources (human, financial and estate). There is also a more complex organisational landscape with the emergence of integration joint boards (“IJB”) and the new roles of IJB Chief Officers. There was a need to reconcile these new roles and the traditional functional roles of Board directors, and to consider how best to support the delivery of my principal accountabilities (as Chief Executive) for quality, whole system performance and financial balance. This means that we need to deliver genuinely transformed models of service delivery – encouraging supported self care, prevention, alternatives to secondary care in the community, primary and social care and new ways of delivering secondary and tertiary care. We need to embrace technology, innovation and experimentation and we need to have the capacity and capability to take giant leaps as well as small steps of change. There is a risk that the executive team and other senior leaders can have all of their time consumed by attending to immediate operational pressures. This can also include having to respond to the impact that deteriorating performance can have on people being able to receive care in a timely manner and the Board’s ability to achieve recurring financial balance. This brings with it the associated risk of deterioration of safety and quality. We need to ensure that the Corporate Management Team has the capacity and capability to provide the leadership that is required to achieve the Board’s Vision and Mission. The Corporate Management Team needs to drive forward transformation, innovation and experimentation alongside the necessary work to deliver current operational performance requirements. We have made changes to the leadership structure which should to free up my role as the Chief Executive to focus principally on strategic transformational change and also to have a stronger leadership role in the East of Scotland region. We will develop a culture that promotes enabled, clinically-led, distributed leadership, empowered to experiment and innovate. On 1 April 2016 Dr Simon Watson took up a new role of the Board’s Chief Quality Officer, to lead the work to create an enhanced whole organisation approach to quality assurance and improvement, and to make quality the focus of how we carry out our activities. The recently established Quality Management System (The QMS) is the means to turn this aspiration into reality. The QMS approach begins by understanding and describing the systems underpinning core, day-to-day processes and pathways. We then deploy our analytical service to extract the data underpinning these pathways to understand the causes and consequences of unwarranted variation. By training, enabling and empowering front line teams to

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
5
manage quality, tests of change to continuously improve performance are then undertaken. These will be supported by patient-level costing systems, which will enable us to understand the cost savings associated with reduction in unwarranted variation and waste. This is a big change to the way we work and we have spent the last year prototyping our Quality Management infrastructure to be tested in key services. Training staff from front line teams, supported by our middle and senior level managers, has been a high priority. Through our Quality Academy, we have run four courses in Planning for Quality for middle and senior managers. By the middle of 2017, over 150 leaders will have graduated as Fellows of the Academy. This is matched by a similar number of fellows from our Quality Improvement skills course, which has been designed for front line staff undertaking quality improvement projects. These courses have been formally evaluated, with lessons learned driving improvement. The fellows of the Academy are key to driving our priority clinical quality programmes in both primary and secondary care. The programmes currently focus on improving outcomes in mental health, stroke disease, cancer and more recently outpatient endoscopy and hip fracture, in addition to supporting the new Primary Care Quality Clusters. Although the QMS is in its infancy, we have already developed an effective delivery model and are seeing significant, sustained improvements and a very high level of staff engagement. In January 2017, Jim Crombie took up a new role of Deputy Chief Executive. The Deputy Chief Executive will focus on operational delivery and performance across NHS Lothian. The Deputy Chief Executive’s key priorities will be patient access to services, and the interface between the areas of primary, social, and secondary care. The Directors of each of the four Health & Social Care Partnerships in Lothian (who are also the Chief Officers of the IJBs) shall continue to report to myself however they will also be accountable to the Deputy Chief Executive for operational performance. The Board has delegated a large element of its functions and services to four integration joint boards, and 2016/17 was the first full year where the integration joint boards were responsible for those “integration functions”. They are focussed on improving the health and wellbeing outcomes of the population of their local authority area. The NHS Lothian Organisational Development team in collaboration with colleagues from the four local authorities (City of Edinburgh, East Lothian, Midlothian and West Lothian) has taken forward supporting activities for the new health & social care leaders and their teams. They delivered a brief leadership development intervention for leaders of health & social care integration, Playing to your Strengths, which was designed to complement existing development programmes in each organisation and enable leaders to take stock of their own leadership in a new and changing context. 115 people have taken part in this, drawn from all four health & social care partnerships, the acute sector, social care, GPs, and leaders from the voluntary sector. Additionally internal and external coaches have provided 230 coaching sessions, and evaluation has shown that these have been considered to be valued and effective. With the aim of developing a person-centred team-working culture and which supports the vision, values and strategic plan of each of the four integration joint boards, the Organisational Development team has commissioned external consultants to co-produce a toolkit. This initiative will specifically support newly formed integrated health & social care teams and existing integrated teams wishing to review how they are developing in a changing environment. A core module will enable teams to look at culture, vision and values with additional modules designed around the needs of teams. There will be a range of resources which can be used by teams, individual team members and team leaders to address a particular need and be capable of being used without the need for external facilitation support. The toolkit will be rolled out during 2017/18. Looking Ahead The Board approved six Corporate Objectives for 2017/18 on 6 April 2017. They have been developed to support the achievement of the Scottish Government’s Vision for NHS Scotland and the Board’s Mission, and also reflects NHS Lothian’s Our Values in Action. The detailed actions within the Corporate Objectives address the main areas of focus and action as outlined in the Scottish Government’s Health & Social Care Delivery Plan (December 2016) and the NHS Lothian 2017/18 Local Delivery Plan. The objectives also reflect key strategic planning activities, financial and workforce plans and include reference to the requirements outlined by the Scottish Government relating to integration performance measures (unplanned admissions, occupied bed days for unscheduled care, A&E performance, delayed discharges, end of life care and balance of spend across institutional and community services). Our Vision
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
6
By 2020 everyone is able to live longer healthier lives at home, or in a homely setting and, that we will have a healthcare system where:
We have integrated health and social care
There is a focus on prevention, anticipation and supported self-management
When hospital treatment is required, and cannot be provided in a community setting, day case treatment will be the norm
Whatever the setting, care will be provided to the highest standards of quality and safety, with the person at the centre of all decisions supported through House of Care and Realistic Healthcare approaches
There will be a focus on ensuring that people get back into their home or community environment as soon as appropriate, with minimal risk of re-admission Our Mission
improving the health of the population,
improving the quality of healthcare and
achieving value and financial sustainability. Better health, better care, better value Our Values
Care and Compassion
Dignity and Respect
Quality
Teamwork
Openness, Honesty and Responsibility Our Objectives
1. Protect and Improve the Health of Our Population 2. Improve patient pathways and shift the balance of care. 3. Improve Quality, Safety and Experience Across the Organisation. 4. Support the Engagement and Development of Our Staff through Leadership and Behaviours 5. Achieve Greater Financial Sustainability and Value. 6. To work with partner boards to develop a Regional Health & Social Care Delivery Plan for the East of
Scotland. We will work in collaboration with our four Health & Social Care Partnerships to deliver our objectives and move us closer to achieving our Vision. The above Corporate Objectives have been disseminated throughout the organisation to inform personal objective-setting and to help individuals understand how they do and can contribute to the delivery of the objectives of the wider organisation. I shall ensure that each director is clear as to which aspects of the Corporate Objectives they are responsible for, and that there are agreed performance measures and timelines in place. It should be noted that the 2017/18 Local Delivery Plan already sets out in considerable detail the actions that will be taken to deliver our objectives and measures of success. The Board and its committees shall routinely receive reports on aspects of performance related to the corporate objectives. Additionally the Board shall receive a report on the progress made on all of the Corporate Objectives in October 2017 and April 2018. In addition to the Corporate Objectives and the Local Delivery Plan for 2017/18, the Board has discussed the Scottish Government’s Health and Social Care Delivery Plan, and the suggested approach to Regional Planning therein. I have been appointed as the lead Chief Executive for the East of Scotland region, with a seat on the National Delivery Board for the Health and Social Care Delivery Plan. I shall ensure that we continue to work closely with partner boards from the East of Scotland (Fife, Borders, Tayside and Forth Valley) to produce a Regional Delivery Plan which is due to be submitted to the Scottish Government in
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
7
September 2017. The sections of the Regional Delivery Plan are Context, Prevention, Integrated Services, Workforce, Finance and Acute Services.
b) History, Purpose and Activities of the NHS Board Lothian Health Board (the “Board”) was established in 1974 under the National Health Service (Scotland) Act 1972, and is commonly referred to as “Lothian NHS Board”. The National Health Service (Scotland) Act 1978, other law, and Government directions determine the Board’s constitution, duties and functions. Health Boards carry out functions on behalf of Scottish Ministers, and are required to follow any regulations or directions that may be made.
The Board is responsible for the healthcare services for the residents of four local authority areas (City of Edinburgh, East Lothian, Midlothian and West Lothian). The National Records of Scotland projections for 2010 to 2025 show a 15% increase in total Lothian population from 836,711 to 965,007. The Board also provides a wide range of specialist services for people from across Scotland, including liver and kidney transplantation, neo-natal intensive care, cancer services and complex surgery. Further information on the Board, including its history and details of its services and locations can be found on the Board’s website:
www.nhslothian.scot.nhs.uk/Our Organisation
Integration of Health & Social Care Services
During 2015/16 a new integration joint board (IJB) was established in each of the four local authority areas within the NHS Lothian boundary, under the terms of the Public Bodies (Joint Working) (Scotland) Act 2014. The IJBs are distinct legal entities separate from the NHS Board and the relevant local authority. The NHS Board and the relevant local authority for the local authority area have delegated some of their functions to them, and 2016/17 was the first year that the IJBs were responsible for those “integration functions”. Each IJB is wholly responsible for carrying out those functions, and does so by preparing a strategic plan and then directing the NHS Board and the relevant local authority as to how those functions are to be carried out. The IJB will be required to have regard to the national health & wellbeing outcomes, the integration delivery principles and the needs of localities within the local authority area.
This was a fundamental change as to the governance of the “integration functions”. The law required the NHS
Board and the relevant local authority to delegate certain functions to the extent that they are provided to people who are at least 18 years old, namely adult social care, and all adult community health care and specific adult hospital services relating to unscheduled care. The relevant services are:
• Social Work Functions: Residential Care – Older People, Extra Care Housing and Sheltered Housing (Housing Support provided), Intermediate Care, Supported Housing-Learning Disability, Rehabilitation-Mental Health, Day Services and Local Area Coordination-LD; Older People; Mental Health, Care at Home services and enablement–all client groups, Rapid Response, Telecare, Respite services-all client groups, Quality assurance and Contracts, Assessment and Care Management-including OT services, Specialist Services-Sensory Impairment, Drugs and Alcohol.
• Hospital services: (includes associated services – e.g. allied health professionals) A&E, general medicine, geriatric medicine, rehabilitation medicine, respiratory medicine, psychiatry of learning disability, palliative care, hospital services provided by GPs, mental health services provided in a hospital with exception of forensic mental health services, and services relating to an addiction or dependence on any substance.
• Community Health Services: District nursing, services relating to an addiction or dependence on any substance, services provided by allied health professionals, public dental service, primary medical services (GP), general dental services, ophthalmic services, pharmaceutical services, out-of-hours primary medical services, community geriatric medicine, palliative care, mental health services, continence services, kidney dialysis, and services to promote public health.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
8
The NHS Board took the option to delegate further functions. An example of this is the provision of the following services to people who are under 18 years of age:
▪ Primary Medical Services and General Medical Services (including GP Pharmaceutical services)
▪ General Dental Services, Public Dental Services and the Edinburgh Dental Institute
▪ General Ophthalmic Services
▪ General Pharmaceutical Services
▪ Out of Hours Primary Medical Services
▪ Learning Disabilities The NHS Board continues to directly carry out all its functions which have not been delegated to IJBs. Within the NHS Board’s website there is a page with further information on health & social care integration, and links to the websites of the IJBs. You can access this through the link below: http://www.nhslothian.scot.nhs.uk/community
c) The Key Issues and Risks that could affect the NHS Board in delivering its objectives
The Board agreed that a Strategic Plan should be developed in order to implement the Strategic Clinical Framework which it previously agreed in May 2013. The Board’s Strategic Planning Committee led the development of the Strategic Plan 2014-2024 (“Our Health, Our Care, Our Future”), which set out in detail the challenges that the Board faces, under four broad headings, namely:
Demography, inequalities and ill health
Multimorbidity
Health service demand
Tighter finances
The Board’s website contains all the information relating to the Strategic Plan and you can find this at the link below: http://www.nhslothian.scot.nhs.uk/OurOrganisation/OurHealthOurCareOurFuture/Pages/default.aspx The fundamental challenges identified within Our Health, Our Care, Our Future have not changed and they are live issues. The population is growing, and the population is ageing with an increasing number of frail individuals with complex needs. It follows that there is an increased demand for NHS services which will drive up expenditure.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
9
Table 1: Population Growth in Lothian
There were 9,386 births and 7,774 deaths of people resident in Lothian in 2015. Although Lothian continues to have a rising population, it has the lowest overall fertility rate in Scotland. However, the fertility rate among 35-39 year olds and 40-44 year olds is among the highest in the country.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
10
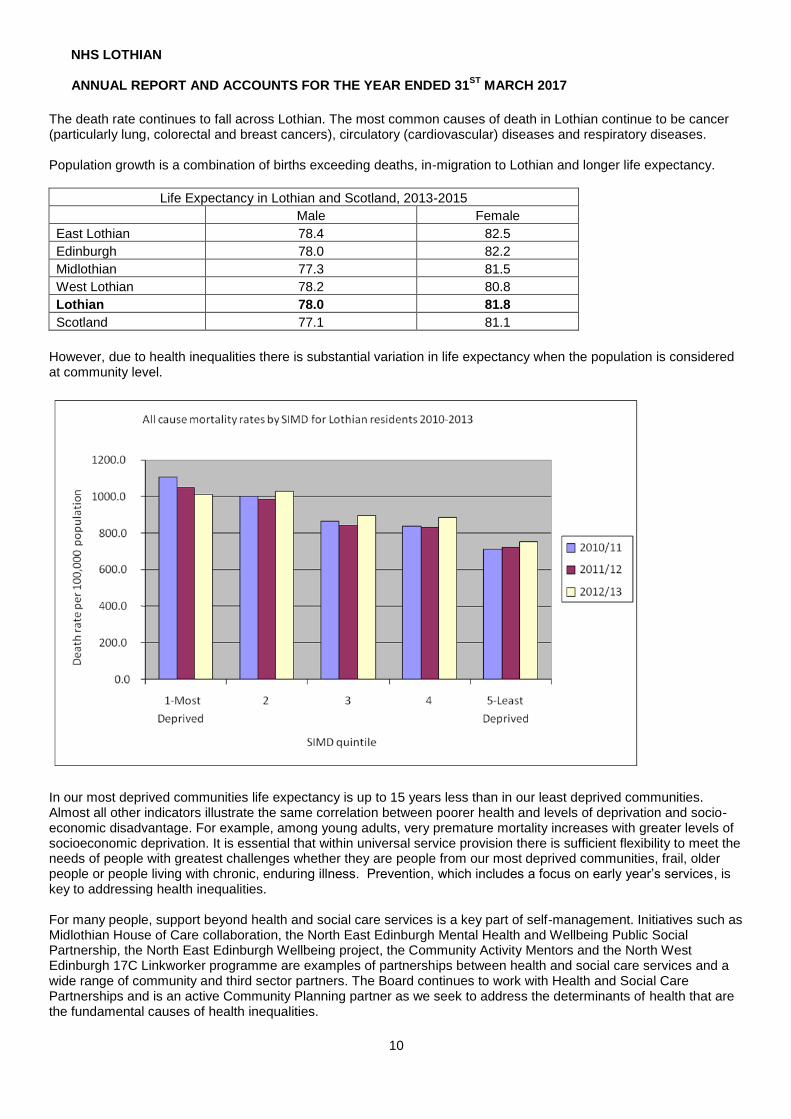
The death rate continues to fall across Lothian. The most common causes of death in Lothian continue to be cancer (particularly lung, colorectal and breast cancers), circulatory (cardiovascular) diseases and respiratory diseases. Population growth is a combination of births exceeding deaths, in-migration to Lothian and longer life expectancy.
Life Expectancy in Lothian and Scotland, 2013-2015
Male Female
East Lothian 78.4 82.5
Edinburgh 78.0 82.2
Midlothian 77.3 81.5
West Lothian 78.2 80.8
Lothian 78.0 81.8
Scotland 77.1 81.1
However, due to health inequalities there is substantial variation in life expectancy when the population is considered at community level.
In our most deprived communities life expectancy is up to 15 years less than in our least deprived communities. Almost all other indicators illustrate the same correlation between poorer health and levels of deprivation and socio-economic disadvantage. For example, among young adults, very premature mortality increases with greater levels of socioeconomic deprivation. It is essential that within universal service provision there is sufficient flexibility to meet the needs of people with greatest challenges whether they are people from our most deprived communities, frail, older people or people living with chronic, enduring illness. Prevention, which includes a focus on early year’s services, is key to addressing health inequalities. For many people, support beyond health and social care services is a key part of self-management. Initiatives such as Midlothian House of Care collaboration, the North East Edinburgh Mental Health and Wellbeing Public Social Partnership, the North East Edinburgh Wellbeing project, the Community Activity Mentors and the North West Edinburgh 17C Linkworker programme are examples of partnerships between health and social care services and a wide range of community and third sector partners. The Board continues to work with Health and Social Care Partnerships and is an active Community Planning partner as we seek to address the determinants of health that are the fundamental causes of health inequalities.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
11
However the integration joint boards and the NHS Board continue to tackle the issues relating to prevention, inequalities and an ageing population in a very challenging financial climate.
Audit Scotland published NHS in Scotland 2016 in October 2016 which set out in detail the financial challenges in NHS Scotland. That report included the following remarks: “NHS funding is not keeping pace with increasing demand and the needs of an ageing population. NHS boards are facing an extremely challenging financial position and many had to use short-term measures to break even. NHS boards are facing increasing costs each year, for example drug costs increased by ten per cent, allowing for inflation, between 2012/13 and 2014/15. NHS boards will need to make unprecedented levels of savings in 2016/17 and there is a risk that some will not be able to achieve financial balance.” “Despite the significant financial challenges facing NHS boards, there have been improvements in some areas, for example in reducing the overall number of bed days from delayed discharges. However, boards are struggling to meet the majority of key national standards and the balance of care, in terms of spending, is still not changing. It is difficult balancing the demand for hospital care, alongside providing more care in the community. Boards need to ensure they maintain high-quality hospitals, while investing in more community-based facilities.” “The NHS is going through a period of major reform. A number of wide-ranging strategies propose significant change, including the National Clinical Strategy, integration of health and social care services and a new GP contract. These need to be underpinned by a clear plan for change. Some progress is being made in developing new models of care, but this has yet to translate to widespread change in local areas and major health inequalities remain.”
The Board’s Corporate Risk Register had the following risks at the end of 2016/17:-
1. The scale or quality of the Board’s services is reduced in the future due to failure to respond to the financial
challenge (“Very High”) 2. Achieving the 4-hour emergency care target (“Very High”) 3. Achieving the delayed discharge targets at 2 weeks (“Very High”) 4. General Practice Sustainability (“Very High”) 5. Patient Experience - Management of complaints and feedback (“Very High”) 6. Patient Safety - Delivery of four Scottish Patient Safety Programme work streams (“High”) 7. Achievement of the national waiting times targets (“High”) 8. Healthcare Associated Infection (risk scoring = “High”) 9. Medical workforce sustainability (“High”) 10. Facilities – Fit for Purpose (“High”) 11. Health & Safety - Management of violence and aggression (“High”) 12. Roadway/ traffic management (“High”) 13. Nursing Workforce – Safe Staffing Levels (“Medium”)
Comparing the above risks to the position at the end of 2015/16, the risk for “patient experience – management of complaints” has increased from “high” to “very high”. However the “Healthcare Associated Infection” risk has been lowered from “very high” to “high”, and “nursing workforce” has been lowered from “high” to “medium”. All others have remained the same. A proportion of the Board’s property has been procured through Private Finance Initiative/ Public Private Partnership contracts. It is recognised that these contracts have a key role in the management of key service and financial risks. During 2016/17 the Director of Finance broadened the role of a group which was overseeing the Royal Infirmary of Edinburgh contract. The Commercial PFI Group now oversees all such contracts so as to provide greater assurance on this subject, monitor performance against the contracts and to look for opportunities for improvement. The Director of Finance chairs the Group and its membership includes representatives from finance, estates and capital planning. The four integration joint boards each have their own risk management system and risk register. However the Board’s risks have been and are being reviewed to recognise the role of the integration joint boards, and that some risks are now shared with them.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
12
d) Performance Summary The Performance Analysis section (Section 2) below sets out some detailed information on the Board’s performance in the year. This Performance Summary has been prepared to summarise some key messages. Throughout 2016/17 the Board has delivered the following services to its population:
Primary & Community Care
Primary care is the first point of consultation with the patient, and for most people contact with the NHS begins and ends in primary & community care. The Board engages independent contractors to provide primary and community health services. As at 4 May 2017 within the Lothian area there were 123 general medical practices with 1,020 general practitioners. There were 182 dental practices with 555 dentists. There were 114 optician premises with 292 opticians. There were also 184 pharmacy premises.
Secondary Care
Patients will enter secondary or acute care when they need a specific clinical intervention, with ISD reporting that the Board sees approximately 670,000 outpatients, 65,000 patients as day cases, 25,000 elective (scheduled) inpatients and 80,000 emergency (unscheduled) inpatients annually.
Secondary Care - Unscheduled The performance on unscheduled care is dependent on the flow of patients throughout the health & social care system. The work on addressing capacity, patient pathways (including primary care and social care), delayed discharges and the integration process more generally is critical in this respect.
Within Lothian during 2016/17 there were 269,057 attendances at Accident & Emergency, which national figures show is the second highest level of activity within a Board area in Scotland, with Greater Glasgow & Clyde being the highest. NHS Lothian Accident & Emergency activity accounted for 16.6% of all such activity in Scotland. The Board’s performance during 2016/17 on seeing patients within 4 hours ranged from 93.2% - 97.1% except for December and January where there was a decline to 92.5% and 92.8% respectively - as a result of increased activity due to winter and in part due to higher volumes of very elderly and frail patients. However, January’s performance was over 4 percentage points better than as at the same time last year. The performance in March 2017 had improved to 95.7%.
Secondary Care - Scheduled The Board has a legal requirement (under the Patients Rights (Scotland) Act 2011) that once planned inpatient and day case treatment has been agreed with the patient, the patient must receive that treatment within 12 weeks. The Board’s performance on the treatment time guarantee (“TTG”) has deteriorated. However the level of investment that is required to sustain (and improve) this level of performance is prohibitive (in light of us moving out of financial balance). The charts below demonstrate the Board’s comparative performance against NHS Scotland for the five quarters to 31 March 2017 for Treatment Time Guarantee and as at Quarter End over the same period for Outpatients respectively:

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
13
Treatment Time Guarantee Performance - patients seen within 12 weeks
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Jan-Mar 16 Apr-Jun 16 Jul-Sep 16 Oct-Dec 16 Jan-Mar 17
NHS Lothian NHS Scotland Target (min)
Outpatient Performance – patients waiting 12 weeks or less
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
As at 31st Mar 16 As at 30th Jun 16 As at 30th Sep 16 As at 31st Dec 16 As at 31st Mar 17
NHS Lothian NHS Scotland Target (min)
Finance
The Board has met its financial targets for 2016/17.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
14
2. Performance Analysis
2A – Improvements and Achievements in 2016/17
Person-Centred and Efficient
The new Robert Fergusson National Brain Injury Unit started caring for patients in its new fit-for-purpose facilities in February 2017. The unit is part of Phase 1 of the £48m re-development of the Royal Edinburgh Campus.
The West Lothian Community Palliative Care Team won the ‘Innovation’ award at the Marie Curie Peacock awards. The service provides specialist palliative care services for people with any advanced, progressive and incurable illness, and their families. Additionally, Libby Milton, who is based at the Marie Curie Hospice, Edinburgh won the ‘Nurse Leadership’ category. She has played a key role over the last 18 months in leading the expansion of the community services as part of the hospice redesign initiative.
Four individuals and three healthcare teams from NHS Lothian were selected as finalists at the Scottish Healthcare Awards 2016, and there were two NHS Lothian winners. Orla Duncan, a psychosocial nurse practitioner at Royal Hospital for Sick Children won the Unsung Hero Award in recognition for her unwavering dedication to improving the lives of her patients and their families. The Patient Experience and Anticipatory Care Plan Team (PACT) won the Innovation Award. Following a successful two year pilot, the team has reduced hospital admissions within their population by 30%, and delivered a significant economic benefit: for every £1 invested in PACT, the service has been able to return a saving of £6.
Fiona Haston, a Clinical Nurse Specialist at the Western General Hospital was awarded the British Empire Medal in the New Year’s Honours List for her outstanding contribution to service improvement work.
The Outpatient Modernisation Team and the NHS Lothian webmasters have re-designed the REFHELP website. REFHELP’s aim is to help GPs and other clinicians make the best possible patient referrals within the Lothian health system, by providing up-to-date information on all services which accept referrals. The site has information to inform the referring practitioner which patients would benefit from a referral, and how to make a good referral to the service. The site has the potential for further development so that it can also support public health initiatives and programmes.
The Flow Centre was launched on 4th July 2016. It is a centralised service to support the flow of patients across all adult acute sites in NHS Lothian. The Centre works with GPs, health & social care partnerships and acute hospital staff to create clear admission pathways and, where possible, avoid admission altogether. The aim is to ensure the patient is seen at the right time, in the right place, by the right person. The Centre also co-ordinates transport for all patient transport and discharges across Lothian, including out of area patients, thereby ensuring a seamless service from admission to discharge.
The Medical Physics team has instigated a series of patient education days within the osteoporosis service. Nine events took place in 2016, with a further ten booked for 2017; each event has been attended by approximately twenty people. This has facilitated a significant reduction in the osteoporosis patient pathway, with patients now being assessed by a multi-disciplinary team and treated within 2-3 weeks. This is a significant improvement on a pathway which previously took 2-3 months to complete.
Safe and Equitable
Within West Lothian, the uptake of childhood immunisations is higher than the Scotland average at all ages when an immunisation is due.
In response to an outbreak of measles in Edinburgh in October 2016, NHS Lothian set up Measles, Mumps & Rubella vaccination clinics, and 1,003 people received vaccination.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
15
The Healthcare Environment Inspectorate carried out an unannounced inspection of St John’s Hospital in August 2016. They published a very positive report in October 2016 which had no requirements or recommendations.
For all of NHS Lothian there has been a sustained reduction in the rate of incidences of Clostridium-difficile (“C-Diff) infections in patients aged 65 years and over. NHS Lothian’s annual overall rate of C-Diff infection is, for the first time within the Local Delivery Plan standards. Over the course of the year the Western General Hospital has significantly improved its performance on infection control, with rates for C-Diff and staphylococcus aureus bacteraemia (“SaB”).
At the Royal Infirmary of Edinburgh there have been significant reductions in length of stay in the general medical wards, supported by the introduction of a new consultant / medical model. This has included the trialling of a complex discharge co-ordinator who works in partnership with the Discharge Hub. This is reducing the length of stay for patients whose discharge from hospital has been delayed, as well as the number of delayed discharges within medical wards.
Following an invited Review carried out by the Royal College of Paediatrics and Child Health in the first half of 2016, the Board established a Paediatric Programme Board which was chaired by a non- executive Board member, and had extensive clinical representation. We have now made significant progress in implementing all the College’s recommendations and specifically, the recommended workforce model for the St John’s Hospital Children’s Ward.
A programme of work was undertaken to reduce the vacancy rate in the number of health visitors in Edinburgh, and this has reduced the rate from 25% to 10%. A plan is in place to manage the remaining vacancies and reach the required staffing level to deliver a new health visitor pathway.
Effective and Timely
The Royal College of Psychiatrists accredited the Regional Eating Disorders Unit, which is based at the Royal Edinburgh Hospital. The review team was especially impressed with the feedback from frontline staff and service users which highlighted good care, the high morale of staff with regular supervision and supportive structures.
In May 2016 the maternity unit at St John’s Hospital achieved full Baby Friendly accreditation from UNICEF. The award is a wonderful celebration of all the hard work that the team has put in over the years supporting mums whether breastfeeding or formula feeding to build strong relationships with their baby.
In July 2016, a pioneering robotic surgery service for patients with prostate cancer was introduced at the Cancer Centre at the Western General Hospital.
The Mental Health Information Station celebrated its first anniversary in October 2016, after welcoming over 1,000 visitors in its first 12 months. The Mental Health Information Station is available every Thursday from 11am until 3pm and offers a one-stop-shop providing support, information and sign posting for anyone affected by mental health and wellbeing issues. Patient feedback has been excellent, with respondents highlighting the way the service has helped them make sense of the plethora of therapeutic and self-management options available to them.
Allied Health Professionals have been involved in work to support and empower musculoskeletal patients towards more successful self management of their conditions. This has delivered a saving of over 1,000 outpatient appointments in the first year. A single telephone number has been introduced for musculoskeletal, physiotherapy, podiatry and orthotics, which has significantly reduced the number of appointments where the patient did not attend. The improvement work has led to a reduction in the number of requests for lumbar MRI, quicker first appointment times for patients with back pain, and an improvement in the rapid escalation for patients who require a surgical intervention.
There is a standard that 95% of patients are to wait no longer than 4 hours from arrival to admission, discharge or transfer for A&E treatment. NHS Lothian has put in place a rolling programme of improvement work which has led to generally improved performance, albeit that the standard is not consistently met. In July 2016 NHS Lothian achieved its highest level of performance ever (97%).
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
16
The Royal Hospital for Sick Children and Department of Clinical Neurosciences project has won the GO Sustainable Procurement Award at the National GO Excellence in Public Procurement Awards 2017/18. These awards showcased the very best in the UK’s public procurement community and the project has been recognised for its collaborative working to deliver employment opportunities, training and development for the people of Lothian, investment in local and Scottish businesses, environmental schemes and charity projects in the local community. - www.goawards.co.uk
There have also been some notable achievements for NHS Lothian in its capacity as an employer:
NHS Lothian continues to work in partnership with the Prince’s Trust on our Get into Healthcare Programmes. These have recruited into both facilities and clinical roles. A total of 24 young people through the programme in 2016/17, with 17 securing permanent posts with NHS Lothian. The current cohort has 7 young people who have been placed within Theatres.
NHS Lothian’s Employability & Work placement team continues to work in partnership with the City of Edinburgh Council, Edinburgh College and Intowork to deliver Edinburgh Project SEARCH, which is an employability programme for young people (Interns) aged 16-24 with a recognised disability who want to move into employment. The programme is run within the Western General Hospital and in its first year 2015/2016 - all 10 young persons completing the programme, secured permanent employment within NHS Lothian. For 2016/17, the second cohort consists of 12 interns, 4 of whom have already secured employment within NHS Lothian and 8 are entering their final placements of the programme whilst being supported to search and apply for jobs. The team are currently preparing for the intake of the third cohort during 2017/18.
In March 2017, NHS Lothian were runners up in the national Family Friendly Working Scotland (FFWS) (the Carers Scotland best for carers and elders care). The 2017 awards received almost triple the number of entries compared to last year, demonstrating the increased importance Scottish Employers place on flexible and family friend working. NHS Lothian was also awarded the Established level of the ‘Carer Positive’ Award (which is the middle of 3 levels) for recognising and respecting that many employees combine their paid work with additional caring responsibilities at home. This award is presented to employers in Scotland who have a working environment where carers are valued and supported. The work included two minute digital clips from two managers and two carers as well as from the Chief Executive, roadshows and promotional posters and fliers across all sites. We continue to endorse the importance of supporting staff who juggle a paid caring role with an unpaid one recognising that this can help reduce levels of stress, reduce sickness absence, lower recruitment and training costs and increase staff morale and productivity levels.
2B Performance against Key Non-Financial Targets
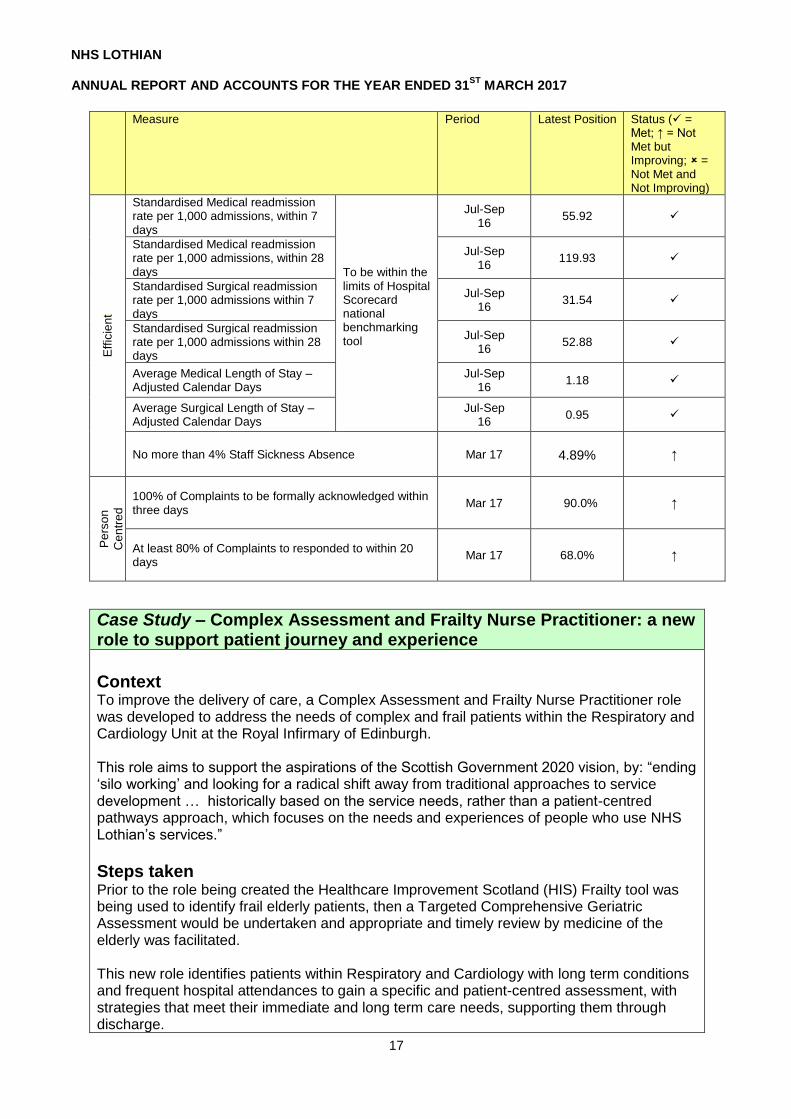
The Board monitors its performance against a range of quality and performance measures, some of which are set nationally. The Board receives a Quality & Performance Improvement Report at every meeting and this includes more detailed information. NHS Lothian publishes its Board papers on its website here: http://www.nhslothian.scot.nhs.uk/OurOrganisation The performance measures in this section use national and local data sources to present the 2016/17 performance. Please note much of the data is taken from live systems and can be updated. Accordingly they may be revised in the future. The performance measures are shown under the six Domains of Quality derived from the Institute of Medicine; – Person Centred, Efficient, Safe, Equitable, Effective and Timely.
Person Centred and Efficient
The Board closely monitors the quality of the care it provides and the outcomes for its patients. When we compare its performance to other NHS Boards, NHS Lothian meets expectations on readmissions and length of stay. However we do need to continue our improvement in how we manage complaints.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
17
Measure Period Latest Position Status ( = Met; ↑ = Not Met but Improving; = Not Met and Not Improving)
Eff
icie
nt
Standardised Medical readmission rate per 1,000 admissions, within 7 days
To be within the limits of Hospital Scorecard national benchmarking tool
Jul-Sep 16
55.92
Standardised Medical readmission rate per 1,000 admissions, within 28 days
Jul-Sep 16
119.93
Standardised Surgical readmission rate per 1,000 admissions within 7 days
Jul-Sep 16
31.54
Standardised Surgical readmission rate per 1,000 admissions within 28 days
Jul-Sep 16
52.88
Average Medical Length of Stay – Adjusted Calendar Days
Jul-Sep 16
1.18
Average Surgical Length of Stay – Adjusted Calendar Days
Jul-Sep 16
0.95
No more than 4% Staff Sickness Absence Mar 17
4.89%
↑
Pe
rso
n
Cen
tre
d
100% of Complaints to be formally acknowledged within three days
Mar 17 90.0% ↑
At least 80% of Complaints to responded to within 20 days
Mar 17 68.0% ↑
Case Study – Complex Assessment and Frailty Nurse Practitioner: a new role to support patient journey and experience
Context To improve the delivery of care, a Complex Assessment and Frailty Nurse Practitioner role was developed to address the needs of complex and frail patients within the Respiratory and Cardiology Unit at the Royal Infirmary of Edinburgh. This role aims to support the aspirations of the Scottish Government 2020 vision, by: “ending ‘silo working’ and looking for a radical shift away from traditional approaches to service development … historically based on the service needs, rather than a patient-centred pathways approach, which focuses on the needs and experiences of people who use NHS Lothian’s services.”
Steps taken Prior to the role being created the Healthcare Improvement Scotland (HIS) Frailty tool was being used to identify frail elderly patients, then a Targeted Comprehensive Geriatric Assessment would be undertaken and appropriate and timely review by medicine of the elderly was facilitated. This new role identifies patients within Respiratory and Cardiology with long term conditions and frequent hospital attendances to gain a specific and patient-centred assessment, with strategies that meet their immediate and long term care needs, supporting them through discharge.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
18
Case Study – Complex Assessment and Frailty Nurse Practitioner: a new role to support patient journey and experience The primary objective of this work was to assess the effectiveness of a novel role to:
reduce length of stay
prioritise care needs
promote use of frailty identification in the acute setting
work more effectively across specialties and services - thus providing quality-enhanced patient experience. This was undertaken by the post-holder:-
Building a more thorough patient profile and strong relationship with the individual;
Spending more quality time with individuals and their carers promoting patient-centred care through discussion, including realistic goal setting and sharing of pertinent information, to enhance communication between all services and individuals involved in a patient’s discharge and ongoing care;
Tailored discharge, for example a patient with no next of kin (Length of Stay 82 days) was assisted to source a plumber to do repair work and helped with their shopping on the day of discharge and settling in at home;
Facilitating complex and psychological assessment working alongside Elderly Care, Assessment Teams and Psychological Medicine;
Anticipatory Care Planning by hospital team. A robust service has thereby developed through engagement, support and close liaison with multiple specialties.
Outcomes Frail and complex patients are identified much earlier in their journey, with the median length of stay for all patients reducing from four to three days. All patients are screened and the post-holder will engage with appropriate patients within the clinical setting. Most of the patients in respiratory are frail but the frail non complex patients also receive input from the new role in terms of ensuring care packages are in place in the community and looking for boarding/downstream options. The post-holder has also assisted patients to resolve social issues and with support for their relatives in the community. Improvements have contributed to a reduction in length of stay for respiratory patients and for cardiology patients lengths of stay were kept to a median of 2 days.
Median Length of Stay 2014 2015 2016
Respiratory Ward 204 & 204 Annexe
3.9 days
2.5 days (Post commenced June 2015)
2.7 days
Cardiology Ward 103
1.8 days
2.0 days 2.0 days (Post commenced June 2016)
Cardio-Thoracic Surgery Ward 102
(Post commenced October 2016)
There is also evidence of reduced hospital attendance for example for one patient of 283 days in 2014/15 to one day in 2016. This patient only presented to A&E in 2016 and was settled and sent back into the community as per their care plan - and even today has not represented. By chance the role-holder met the patient again in their new setting and they were coping much better – in contrast to their previous setting which could not cope with

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
19
Case Study – Complex Assessment and Frailty Nurse Practitioner: a new role to support patient journey and experience them. These improvements were achieved by addressing complex physical and psychological needs through anticipatory care planning and post-discharge support. Feedback has shown an enhanced experience, with expertise, planning and effective and realistic outcomes.
Safe and Equitable The positive progress shown last year in the management of Healthcare Associated Infections for both CDI (clostridium difficile infections) and SAB (staphylococcus aureus bacteraemia (including MRSA)) has continued with the former now meeting the national target and doing so alongside HSMR (hospital standardised mortality), falls with harm and antenatal booking. Performance on cardiac arrest rates in hospitals and on supporting those stopping smoking are being looked upon to improve. Measure Period Latest Position Status ( =
Met; ↑ = Not Met but Improving; = Not Met and Not Improving)
Sa
fe
Median Rate of Cardiac Arrest to be no more than 0.95 per 1,000 discharges
Median to Mar 17
1.76
NHS Boards' rate of CDI (clostridium difficile infections) in patients aged 15 and over is 0.32 cases or less per 1,000 total occupied bed days.
Mar 17 0.27
NHS Boards' rate of SAB (staphylococcus aureus bacteraemia (including MRSA)) cases are 0.24 or less per 1,000 acute occupied bed days.
Mar 17 0.30
Hospital Standardised Mortality Ratio to be within limits of Hospital Scorecard national benchmarking tool as well as less than 1
Sep 16 0.87
Median Rate of Falls with harm per 1,000 occupied bed days to be no more than 0.31
Median to Mar 17
0.18
Eq
uitab
le
At least 80% of pregnant women in each Scottish Index of Multiple Deprivation quintile will have booked for antenatal care by the 12th week of gestation
Feb 17 84.7%
Sustain and embed successful smoking quits, at 12 weeks post quit, in the 40% Scottish Index of Multiple Deprivation areas, with a target of 404 this quarter
Dec 16
203
Case Study – A physical activity programme culturally adapted for South Asian women
Context Scotland has high rates of type 2 diabetes and it is well understood that South Asian ethnic groups have substantially higher rates of diabetes 1. Edinburgh Health and Social Care Partnership funds Fit for Health - a 12 week physical activity programme for people with long term conditions, delivered by Edinburgh Leisure. Through partnership working with communities, including Nari Kallyan Shangho (NKS), we recognised Fit for Health presented barriers to participation for South Asian women.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
20
Case Study – A physical activity programme culturally adapted for South Asian women
Steps taken We collaborated with the University of Edinburgh to culturally adapt physical activity interventions that meet the needs of South Asian women. Next, we delivered the programme in the NKS community to improve engagement and carried out an evaluation to identify ways of improving participation in physical activity in this particular community. The aim of this project was - through partnership working with health, leisure, the third sector and academia - to culturally adapt a physical activity programme to meet the needs of South Asian women and improve their health outcomes, specifically to:
Deliver a 12-week physical activity programme for South Asian women with diabetes
Evaluate the impact of Fit for Health on health outcomes
Tackle health inequalities and identify an alternative model of care to improve diabetes outcomes.
Outcomes Feedback from women who participated in the programme was positive. The key reasons for wanting to participate in this physical activity programme were that it was hosted in their local community centre, it was for women only and there was no cost attached. The main barrier for their participation in physical activity was ‘lack of opportunities within the community’ (80%). A post-programme questionnaire and walking test were repeated after 12 weeks. The results of the walk test demonstrated a 23% improvement in the distance walked over 6 minutes. Feedback showed that the physical activity programme was valued by the participants and of clear benefit to their health and wellbeing.
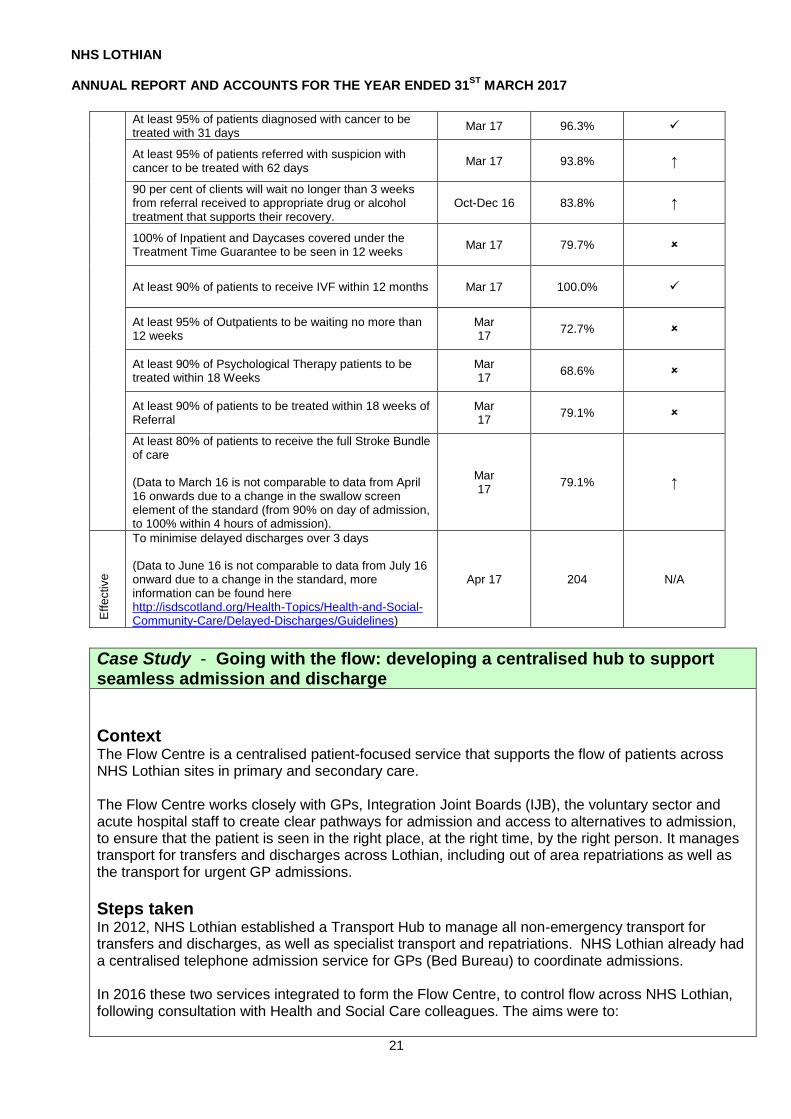
Effective and Timely
As highlighted earlier in the accounts and despite the best efforts of staff, patients are still waiting longer than they ought in NHS Lothian with the expected standards met in four of 13 measures considered. Progress however was made in improving the position in many areas despite use of the independent sector being limited through financial constraints. Although it did not meet the national target Stroke made significant progress and met a local target for March 2017 of 75%.
Measure Period Latest Position Status ( =
Met; ↑ = Not Met but Improving; = Not Met and Not Improving)
Tim
ely
At least 95%, with an ambition of 98%, of unscheduled care patients to be admitted, treated or discharged within 4 hours
Mar 17 95.7%
Sustain and embed alcohol brief interventions in 3 priority settings (primary care, A&E, antenatal) and broaden delivery in wider settings (at least 9,757 overall, 80% being in priority settings)
Mar 17 22,291
At least 90% of Child and Adolescent Mental Health Patients to be treated within 18 weeks of referral
Mar 17 51.4%
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
21
At least 95% of patients diagnosed with cancer to be treated with 31 days
Mar 17 96.3%
At least 95% of patients referred with suspicion with cancer to be treated with 62 days
Mar 17 93.8% ↑
90 per cent of clients will wait no longer than 3 weeks from referral received to appropriate drug or alcohol treatment that supports their recovery.
Oct-Dec 16 83.8% ↑
100% of Inpatient and Daycases covered under the Treatment Time Guarantee to be seen in 12 weeks
Mar 17 79.7%
At least 90% of patients to receive IVF within 12 months Mar 17 100.0%
At least 95% of Outpatients to be waiting no more than 12 weeks
Mar 17
72.7%
At least 90% of Psychological Therapy patients to be treated within 18 Weeks
Mar 17
68.6%
At least 90% of patients to be treated within 18 weeks of Referral
Mar 17
79.1%
At least 80% of patients to receive the full Stroke Bundle of care (Data to March 16 is not comparable to data from April 16 onwards due to a change in the swallow screen element of the standard (from 90% on day of admission, to 100% within 4 hours of admission).
Mar 17
79.1% ↑
Eff
ective
To minimise delayed discharges over 3 days (Data to June 16 is not comparable to data from July 16 onward due to a change in the standard, more information can be found here http://isdscotland.org/Health-Topics/Health-and-Social-Community-Care/Delayed-Discharges/Guidelines)
Apr 17 204 N/A
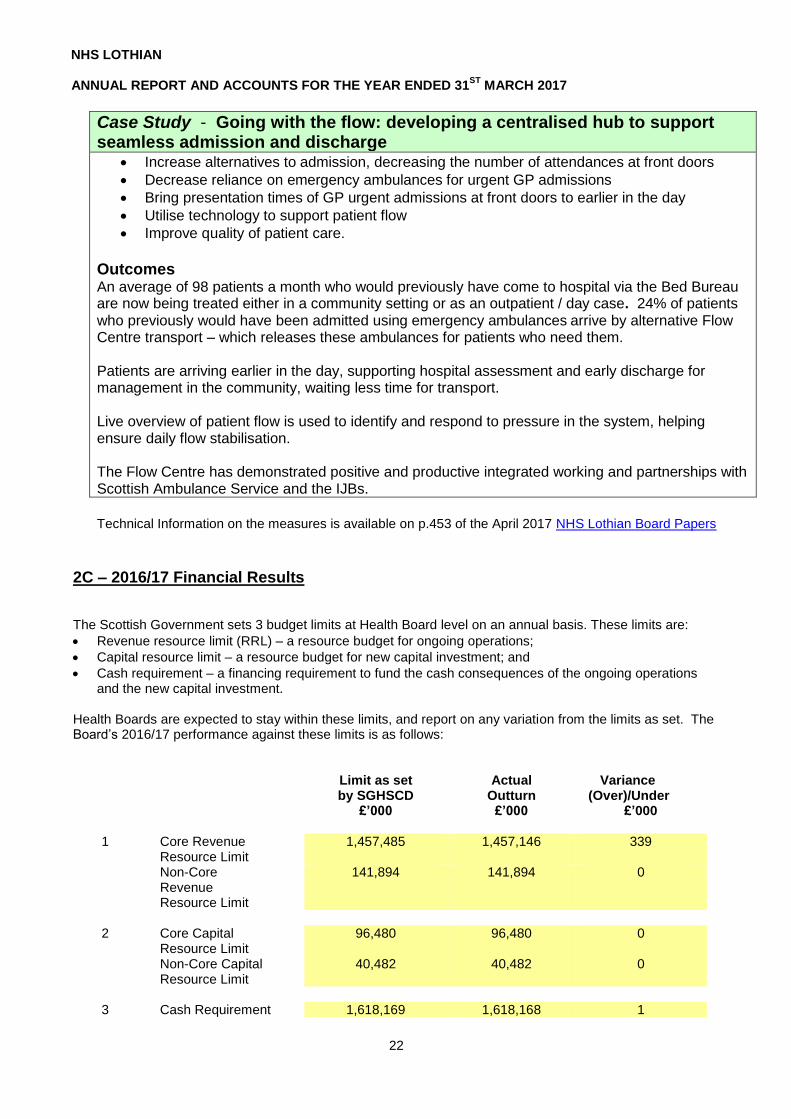
Case Study - Going with the flow: developing a centralised hub to support seamless admission and discharge
Context The Flow Centre is a centralised patient-focused service that supports the flow of patients across NHS Lothian sites in primary and secondary care. The Flow Centre works closely with GPs, Integration Joint Boards (IJB), the voluntary sector and acute hospital staff to create clear pathways for admission and access to alternatives to admission, to ensure that the patient is seen in the right place, at the right time, by the right person. It manages transport for transfers and discharges across Lothian, including out of area repatriations as well as the transport for urgent GP admissions.
Steps taken In 2012, NHS Lothian established a Transport Hub to manage all non-emergency transport for transfers and discharges, as well as specialist transport and repatriations. NHS Lothian already had a centralised telephone admission service for GPs (Bed Bureau) to coordinate admissions. In 2016 these two services integrated to form the Flow Centre, to control flow across NHS Lothian, following consultation with Health and Social Care colleagues. The aims were to:
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
22
Case Study - Going with the flow: developing a centralised hub to support seamless admission and discharge
Increase alternatives to admission, decreasing the number of attendances at front doors
Decrease reliance on emergency ambulances for urgent GP admissions
Bring presentation times of GP urgent admissions at front doors to earlier in the day
Utilise technology to support patient flow
Improve quality of patient care.
Outcomes An average of 98 patients a month who would previously have come to hospital via the Bed Bureau are now being treated either in a community setting or as an outpatient / day case. 24% of patients who previously would have been admitted using emergency ambulances arrive by alternative Flow Centre transport – which releases these ambulances for patients who need them. Patients are arriving earlier in the day, supporting hospital assessment and early discharge for management in the community, waiting less time for transport. Live overview of patient flow is used to identify and respond to pressure in the system, helping ensure daily flow stabilisation. The Flow Centre has demonstrated positive and productive integrated working and partnerships with Scottish Ambulance Service and the IJBs.
Technical Information on the measures is available on p.453 of the April 2017 NHS Lothian Board Papers
2C – 2016/17 Financial Results The Scottish Government sets 3 budget limits at Health Board level on an annual basis. These limits are:
Revenue resource limit (RRL) – a resource budget for ongoing operations;
Capital resource limit – a resource budget for new capital investment; and
Cash requirement – a financing requirement to fund the cash consequences of the ongoing operations and the new capital investment.
Health Boards are expected to stay within these limits, and report on any variation from the limits as set. The Board’s 2016/17 performance against these limits is as follows:
Limit as set by SGHSCD
Actual Outturn
Variance (Over)/Under
£’000 £’000 £’000
1 Core Revenue Resource Limit
1,457,485 1,457,146 339
Non-Core Revenue Resource Limit
141,894 141,894 0
2 Core Capital
Resource Limit 96,480 96,480 0
Non-Core Capital Resource Limit
40,482 40,482 0
3 Cash Requirement 1,618,169 1,618,168 1

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
23
Memorandum of In Year Outturn Brought forward surplus from previous financial year
349
Deficit against in year total Revenue Resource Limit
(10)
Net Savings against RRL 339
The Board has therefore operated within the Scottish Government’s financial limits in 2016/17.
The notes to the accounts provide further detail on the Board’s income and expenditure during the year. The NHS Scotland Unified Board Accounts Manual 2016/17 requires additional information on certain amounts in the financial statements to be disclosed in the Performance Analysis section of the Performance Report, and this is provided below.
Details of NHS Lothian's Net Operating Costs and RRL outturn are set out in Notes 2 to 8 to the Accounts. The Board’s Revenue and Capital Resource limits have been split between two component elements. Core revenue and capital have a cash or near-cash impact on the Board’s net expenditure. Non cash revenue and capital elements of net expenditure such as impairments, provisions and depreciation on assets have a non-core impact.
Demand led income and expenditure in respect of Family Health Services (including Dental, Ophthalmic and Pharmacy services) is not included in RRL and net expenditure is deducted from the Statement of Consolidated Comprehensive Net Expenditure in measuring performance against the Board’s revenue resource limit. This is set out in the Resource Outturn Statement on page 58. At 31 March 2017 NHS Lothian carried a provision for bad debts of £2.75m (31 March 2016 £1.85m). Details of the movement on the provision are contained in Note 13 to the Accounts. Provision for Clinical and Medical Negligence at 31 March 2017 amounted to £92.8m (31 March 2016 £39.2m). Most of the provisions are recoverable under the NHS Clinical Negligence and Other Risks Insurance Scheme (CNORIS).
2D - Payment Policy
The Scottish Government’s Health & Social Care Directorate (SGHSCD) is committed to supporting business by paying bills more quickly, aiming to pay all undisputed invoices within 10 working days. The Board calculates this by comparing the date that payment was made, to the date that it received the invoice. In 2016/17 the average number of days the Board took to pay an invoice was 11 days (2015/16 – 11 days).
2016/17 2015/16
% of Invoices by Value, paid within 30 days 94% 93%
% of Invoices by Value, paid within 10 days 85% 83%
% of Invoices by Volume, paid within 30 days 93% 93%
% of Invoices by Volume, paid within 10 days 84% 82%
No payments were made under Late Payment of Commercial Debts (interest) Act 1998 in 2016/17 (2015/16 - Nil).
2E - Pension Liabilities
The accounting policy note for pensions is provided in Note 1 and disclosure of the costs is shown within Note 24 and the remuneration report.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
24
2F - Sustainability and Environmental Reporting The Climate Change (Scotland) Act 2009 set outs measures adopted by the Scottish Government to reduce emissions in Scotland by at least 80% by 2050. Lothian NHS Board submitted the required annual report for 2015/16 to the Sustainable Scotland Network detailing compliance with the climate change duties imposed by the Act. The information returned by the Board is compiled into a national analysis report, published annually and superseding the prior requirement for public bodies to publish individual sustainability reports.
Further information on the Act, along with copies of prior year national reports, can be found at the following resource:
http://www.keepscotlandbeautiful.org/sustainability-climate-change/sustainable-scotland-network/climate-change-reporting/
2G- Events after the end of the reporting period
There have been no events after the end of the reporting period.
Tim Davison, Chief Executive and Accountable Officer , 21 June 2017

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
25
SECTION B: THE ACCOUNTABILITY REPORT
B1 Corporate Governance Report
(A) The Directors’ Report
Date of Issue The Board presents this report and the audited accounts for the year ended 31 March 2017. The Board approved these accounts on 21 June 2017 for submission to the Scottish Government.
Appointment of the Board’s External Auditors The Public Finance and Accountability (Scotland) Act 2000 places personal responsibility on the Auditor General for Scotland to decide who is to undertake the audit of each health body in Scotland. The Auditor General appointed Scott-Moncrieff to under the audit of Lothian NHS Board for the five-year period from 2016/17 to 2020/21. The general duties of the auditors of health bodies, including their statutory duties, are set out in the Code of Audit Practice issued by Audit Scotland and approved by the Auditor General.
Remuneration for Non-Audit Work The remuneration of the auditors is disclosed in note 3 to the accounts. During the year 2016/17 the Board’s external auditors received no fees in relation to non-audit work.
Board Membership The Cabinet Secretary (Health & Wellbeing) appoints all NHS Board members. The Board is made up of executive and non-executive members. The members are collectively responsible for the governance of the organisation, and the Board is accountable to the Scottish Government. The Board discharges its governance role through regular Board meetings and the work of its committees. You can find the Board’s Standing Orders and other key governance policies on the Board’s website at: http://www.nhslothian.scot.nhs.uk/OurOrganisation/KeyDocuments/Standing Orders
As at 31 March 2017 the Board had 5 executive Board members and 20 non-executive Board members. The Board’s non-executive members include nominees from key stakeholders, and lay members who have applied through a public appointment process. Members are selected on the basis of their position as stakeholders or the particular expertise which enables them to contribute to the decision making process at a strategic level. Table 1 below sets out who held the position of Board members at any time during 2016/17.
Table 1: Individuals who were Board Members at any time during the period from 1 April 2016 to 31 March 2017
Name Position
Brian Houston Non-executive, Chair
Tim Davison Chief Executive
Jim Crombie Acting Chief Executive (from 22 August 2016 to 4 January 2017)
Dr David Farquharson Medical Director (until 31 January 2017)
Professor Alex McMahon Director of Nursing, Midwifery & Allied Health Professionals (from 1 July 2016)
Susan Goldsmith Director of Finance
Professor Alison McCallum Director of Public Health & Health Policy
Dr Tracey Gillies Medical Director (from 1 February 2017)
Shulah Allan MBE Non-executive, Vice-Chair
Michael Ash Non-executive

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
26
Name Position
Kay Blair Non-executive
Cllr Donald Grant Non-executive (East Lothian Council)
Cllr Ricky Henderson Non-executive (City of Edinburgh Council)
Prof Moira Whyte Non-executive (University of Edinburgh)
Cllr Catherine Johnstone Non-executive (Midlothian Council)
Peter Johnston Non-executive
Alex Joyce Non-executive (Employee Director)
Julie McDowell Non-executive
Alison Meiklejohn Non-executive (Area Clinical Forum) (until 31 August 2016)
Fiona Ireland Non-executive (Area Clinical Forum) (from 1 September 2016)
Alison Mitchell Non-executive
Cllr Frank Toner Non-executive (West Lothian Council) (until 24 May 2016)
Cllr Harry Cartmill Non-executive (West Lothian Council) (from 1 June 2016)
George Walker Non-executive (until 31 January 2016)
Dr Richard Williams Non-executive (GP Representative)
John Oates Non-executive
Carolyn Hirst Non-executive
Martin Hill Non-executive
Lynsay Williams Non-executive
Peter Murray Non-executive
The following changes to the Board membership occurred after 31 March 2017:
Julie McDowell’s term of office ended on 31 May 2017
Peter Johnston’s term of office ended on 31 May 2017
Donald Grant’s term of office ended on 30 April 2017 Scottish Ministers appoint local authority councillors onto the NHS Board on the condition that they continue to serve as a councillor and maintain the nomination and support of the local authority. Their nomination is only for the life of the Council, which ends when there is an election. The Scottish local authority elections were held on 4 May 2017. Consequently Councillors Ricky Henderson, Catherine Johnstone and Harry Cartmill ceased being their local authority’s nomination to the Board after midnight on 3 May.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
27
The Statement of the Health Board Members’ Responsibilities in respect of the Accounts
Under the National Health Service (Scotland) Act 1978, the Health Board is required to prepare accounts in accordance with the directions of Scottish Ministers which require that those accounts give a true and fair view of the state of affairs of the Health Board as at 31 March 2017 and of its operating costs for the year then ended. In preparing these accounts the Directors are required to:
Apply on a consistent basis the accounting policies and standards approved for the NHS Scotland by Scottish Ministers.
Make judgements and estimates that are reasonable and prudent.
State where applicable accounting standards, as set out in the Financial Reporting Manual (FReM), have not been followed where the effect of the departure is material.
Prepare the accounts on the going concern basis unless it is inappropriate to presume that the Board will continue to operate.
The Health Board members are responsible for ensuring that proper accounting records are maintained which disclose with reasonable accuracy at any time the financial position of the Board and enable them to ensure that the accounts comply with the National Health Service (Scotland) Act 1978 and the requirements of Scottish Ministers. They are also responsible for safeguarding the assets of the Board and hence taking reasonable steps for the prevention of fraud and other irregularities. The NHS Board members confirm they have discharged the above responsibilities during the financial year and in preparing the accounts.
Board Members’ and Senior Managers’ Interests
All Board members are subject to the Ethical Standards in Public Life (Scotland) Act 2002. The members are required to maintain their entry on the Board’s Register of Interests, and this can be found on the Board’s website at: http://www.nhslothian.scot.nhs.uk/OurOrganisation/BoardCommittees/LothianNHSBoard/BoardMembers Details of any interests of Board members and other senior staff and senior managers in contracts or potential contracts with the Health Board as required by IAS 24 are disclosed in Note 27. Some Board members are also voting members of the integration joint boards and some of the Board’s employees are non-voting members. The integration joint boards and their members are also subject to the Ethical Standards in Public Life (Scotland) Act 2002, and each will maintain its own Register of Interests. There is a page on the NHS Lothian website which provides information on health & social care integration and a link to the websites of the integration joint boards. http://www.nhslothian.scot.nhs.uk/Community/Pages/default.aspx All Board members are also trustees of charitable funds that the Board holds. The Trustees govern the charitable funds distinctly from the Board’s exchequer funds. Lothian Health Board Endowment Fund (commonly known as the Edinburgh & Lothian Health Foundation) is a charity registered with the Office of the Scottish Charity Regulator under number SCO07342. The Board is required to consolidate the financial statements of Lothian Health Board Endowment Fund within the Board’s Annual Accounts. Note 29 details how these consolidated Financial Statements have been calculated. The Board members are also members of Board committees. The Board approves all of the appointments to committees. Figure 1 below identifies the key governance committees and their remits.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
28
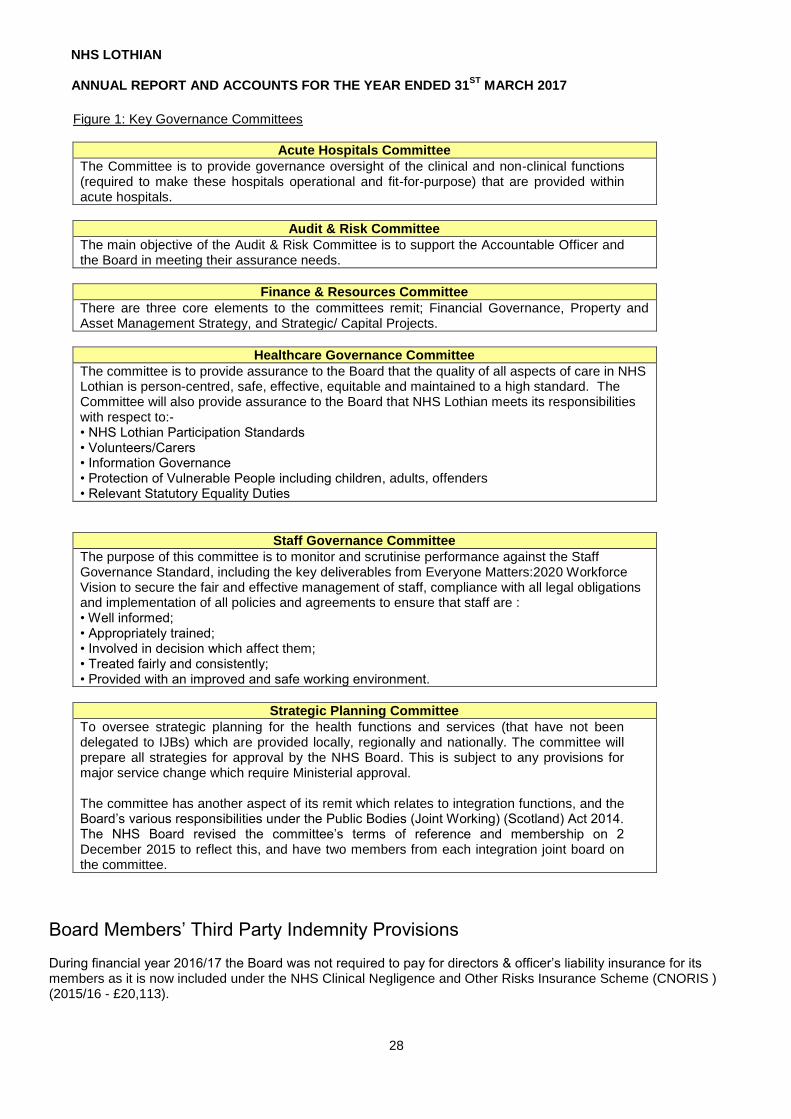
Figure 1: Key Governance Committees
Acute Hospitals Committee
The Committee is to provide governance oversight of the clinical and non-clinical functions (required to make these hospitals operational and fit-for-purpose) that are provided within acute hospitals.
Audit & Risk Committee
The main objective of the Audit & Risk Committee is to support the Accountable Officer and the Board in meeting their assurance needs.
Finance & Resources Committee
There are three core elements to the committees remit; Financial Governance, Property and Asset Management Strategy, and Strategic/ Capital Projects.
Healthcare Governance Committee
The committee is to provide assurance to the Board that the quality of all aspects of care in NHS Lothian is person-centred, safe, effective, equitable and maintained to a high standard. The Committee will also provide assurance to the Board that NHS Lothian meets its responsibilities with respect to:- • NHS Lothian Participation Standards • Volunteers/Carers • Information Governance • Protection of Vulnerable People including children, adults, offenders • Relevant Statutory Equality Duties
Staff Governance Committee
The purpose of this committee is to monitor and scrutinise performance against the Staff Governance Standard, including the key deliverables from Everyone Matters:2020 Workforce Vision to secure the fair and effective management of staff, compliance with all legal obligations and implementation of all policies and agreements to ensure that staff are : • Well informed; • Appropriately trained; • Involved in decision which affect them; • Treated fairly and consistently; • Provided with an improved and safe working environment.
Strategic Planning Committee
To oversee strategic planning for the health functions and services (that have not been delegated to IJBs) which are provided locally, regionally and nationally. The committee will prepare all strategies for approval by the NHS Board. This is subject to any provisions for major service change which require Ministerial approval. The committee has another aspect of its remit which relates to integration functions, and the Board’s various responsibilities under the Public Bodies (Joint Working) (Scotland) Act 2014. The NHS Board revised the committee’s terms of reference and membership on 2 December 2015 to reflect this, and have two members from each integration joint board on the committee.
Board Members’ Third Party Indemnity Provisions During financial year 2016/17 the Board was not required to pay for directors & officer’s liability insurance for its members as it is now included under the NHS Clinical Negligence and Other Risks Insurance Scheme (CNORIS ) (2015/16 - £20,113).

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
29
Public Services Reform (Scotland) Act 2010 This Act requires the Board to publish information on expenditure and certain other matters as soon as is reasonably practicable after the end of each financial year. The relevant information on expenditure greater than £25,000, overseas travel, consultancy and public relations expenditure is disclosed under the Board’s website at: http://www.nhslothian.scot.nhs.uk/OurOrganisation/KeyDocuments/Pages/Financial.aspx
Personal Data Related Incidents reported to the Information Commissioner During 2016/17, the Board (two incidents) and another individual (two incidents) reported four incidents to the Information Commissioner’s Office for review. The Board has referred one of those four incidents to Police Scotland, and Police Scotland is considering the matter. The Information Commissioner’s Office has ruled that the Board has acted appropriately in relation to all incidents and therefore they have been closed down.
Disclosure of Information to Auditors The Board members who held office at the date of approval of this report confirm that so far as they are aware, there is no relevant audit information of which the Board’s auditors are unaware; and each Board member has taken all the steps that they ought reasonably to have taken as a Board member to make themselves aware of any relevant audit information, and to establish that the Board’s auditors are aware of that information.
Financial Instruments Information in respect of the financial risk management objectives and policies of the Board and the exposure of the Board to price risk, credit risk, liquidity risk and cash flow risk is disclosed in note 26.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
30
(B) The Statement of the Chief Executive’s Responsibilities as the Accountable Officer of the Health Board
Under Section 15 of the Public Finance and Accountability (Scotland) Act, 2000, the Principal Accountable Officer (PAO) of the Scottish Government has appointed me as the Accountable Officer of the Board.
This designation carries with it responsibility for:
the propriety and regularity of financial transactions under my control
the economical, efficient and effective use of resources placed at the Board’s disposal; and
safeguarding the assets of the Board.
In preparing the accounts I am required to comply with the requirements of the Government’s Financial Reporting Manual (FReM) and in particular to:
observe the accounts direction issued by Scottish Ministers including the relevant accounting and disclosure requirements and apply suitable accounting policies on a consistent basis
make judgements and estimates on a reasonable basis
state whether applicable accounting standards as set out in the FReM have been followed and disclose and explain any material departures; and
prepare the accounts on a going concern basis.
I confirm that the Annual Report and Accounts as a whole are fair, balanced and reasonable. I am responsible for ensuring proper records are maintained and that the Accounts are prepared under the principles and in the format directed by Scottish Ministers. To the best of my knowledge and belief, I have properly discharged my responsibilities as Accountable Officer as intimated in the Departmental Accountable Officers’ letter to me of the 28 April 2012.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
31
(C) The Governance Statement
As Accountable Officer, I have responsibility for maintaining an adequate and effective system of internal control that supports the achievement of Lothian NHS Board (“the Board”) policies and promotes achievement of the Board’s aims and objectives, including those set by Scottish Ministers. I am also responsible for safeguarding the public funds and assets assigned to the Board. In accordance with IAS 27 – Separate Financial Statements, these financial statements consolidate the Lothian Health Board Endowment Fund (SC007342). This statement includes any relevant disclosure in respect of these Endowment Accounts
Purpose of System of Internal Control
The system of internal control is based on an ongoing process designed to identify and mitigate the principal risks facing the organisation. The system aims to evaluate the nature and extent of those risks and to manage them efficiently, effectively and economically, and is designed to manage rather than eliminate the risk of failure to achieve the Board’s policies, aims and objectives. As such it can only provide reasonable and not absolute assurance. The process is consistent with the Scottish Public Finance Manual (“SPFM”) and supplementary NHS guidance, and has been in place for the year up to the date of the approval of the annual report and accounts. The Scottish Ministers issues the SPFM to provide guidance to the Scottish Government and other relevant bodies on the proper handling and reporting of public funds, and it can be accessed via the following link:
http://www.gov.scot/Topics/Government/Finance/spfm/Intro
Governance Framework The Performance Report (pages 3 - 24) describes the organisation, the Board’s approach to setting strategic direction and corporate objectives, and how outcomes are established. It also explains how the governance arrangements for health and social care functions have been fundamentally revised as a result of the implementation of the Public Bodies (Joint Working) (Scotland) Act 2014, and the creation of four integration joint boards in Lothian. The Board approved a Corporate Communications Strategy (and associated action plan) in June 2014, with the aim to continuously improve its arrangements for engagement with all stakeholders. The Public Involvement Manager within the Communication and Public affairs team provides advice and support to services and departments to ensure that public are kept well informed and consulted on issues affecting health and care services. The Board approved an Involving People Framework 2014-2017 in June 2014, which has taken into account the principles and propositions within the Board’s Strategic Plan. 2016/17 was the first year that the integration joint boards were fully responsible for the carrying out of their delegated “integration functions”. The integration joint boards are responsible for their own systems of governance and within the NHS Board’s website there is a page with further information on health & social care integration, and links to the websites of the IJBs. You can access this through the following link: http://www.nhslothian.scot.nhs.uk/community The Directors’ Report (at pages 25 - 29) provides further information on the Board and its committees. Throughout 2016/17 the Board’s governance framework has continued to develop in response to the integration agenda. Measures that have been taken include:
The Board has continued to refresh its membership appointments to integration joint boards.
The Board agreed a forward programme of development sessions for 2017, with one of two overarching questions for each session seeking to clarify what the role of the Board is for the subject matter, in light of functions being delegated.
The Board has reviewed its Standing Orders to align it with current regulations, and this included removing material that related to the now dissolved community health (and care) partnerships.
The Board has reviewed both its Standing Financial Instructions and its Scheme of Delegation so that financial authority may be delegated to local authority employees. This facilitates integrated management teams and integrated working at an operational level.
The Healthcare Governance Committee held a workshop which led to revised terms of reference, and each integration joint board having one voting member on the committee.
The Area Clinical Forum has revised its constitution to address engagement with integration joint boards, with a standing invitation to the professional lead for clinical and care governance of each integration joint board.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
32
The Finance & Resources Committee has held a workshop to consider the specific financial governance and management issues which integration presents.
The chairs of the audit & risk committees of the Board and the integration joint board have met and developed a set of principles to underpin their working relationships.
The Staff Governance Committee has reviewed its terms of reference to clarify its role with regard to assurance and scrutiny. The Committee has subsequently given specific consideration to the oversight of integration functions and its relationship with integration joint boards, and shall be communicating with the chairs of the integration joint boards on this subject.
In addition to the developments of the governance framework, the Board is specifically considering integration in the context of its forward planning (e.g. Local Delivery Plan, financial planning and budget setting, corporate objectives, Lothian hospitals plan) and its approach to risk management (see below). The Scottish Government issues circulars and there is an internal process to distribute those to the relevant directors. Some of this material is pertinent to the design of the system of corporate governance and is fed into the process of continuous review. The complete suite of circulars can be found on the NHS Scotland website: http://www.scot.nhs.uk/publications/ The Corporate Management Team has reviewed this process during 2016/17 to ensure it remains fit for purpose following the changes resulting from the integration agenda. This review has led to the introduction of a 6-monthly report to the Corporate Management Team to provide assurance that appropriate action is being taken. The Board routinely receives the minutes of committee meetings with accompanying summaries from the committee chairs, and as a Board member, I am routinely informed of the output of their activities. The Board also routinely receives the minutes of integration joint board meetings for information. The chairs of Board committees meet monthly with the Board Chairman, and this provides an additional opportunity for the chairs to discuss any governance matters of common interest. The Scottish Workforce and Governance Committee defined the role and remit of a NHS Board Whistleblowing Champion and the Board has appointed one of its non-executive members to that role. The Board reviewed its Whistleblowing Policy during 2017 and it is one of many human resources (“HR”) policies which are available on the Board’s HR Online intranet site. HR Online provides access to all human resources policies and procedures, and associated flow charts, tools & templates, and Frequently Asked Questions to support the understanding and effective implementation of policies. HR Online also has an HR Enquiry facility where a query regarding any HR issue can be emailed and a response will be provided. The Board routinely uses the internal bulletin, the Team Brief, to communicate when any new HR policy has been agreed. Additionally there is an NHSScotland Confidential Alert Line, which an independent whistleblowing charity runs, to provide a safe space for NHS employees to raise concerns. Management have raised awareness of the Confidential Alert Line through an internal communications exercise, which included placing posters on staff notice boards throughout NHS Lothian. The Board does enhance its governance framework in response to significant issues and risks. The Board had commissioned the Royal College of Paediatrics and Child Health to undertake an independent review of medical paediatric inpatient services in Lothian. The Board considered the resultant report and proposals in June 2016 and established a Paediatric Programme Board which was chaired by a non-executive Board member and reporting to the Acute Hospitals Committee, to take forward the report’s wider recommendations. Following a meeting with the Scottish Public Services Ombudsman (“SPSO”) in August 2016, the Board has developed a local action plan to take forward a number of improvements. As part of this improvement work the Board has decided to appoint a non-executive Board member as its “Complaints Champion”. The Complaints Champion will oversee the implementation of the action plan and chair a local group which includes the Chairman, the Nurse Director, the Medical Directors and the Head of Patient Experience in its membership. A new model complaints handling procedure for NHSScotland was established on 1 April 2017. In conjunction with the above action plan and the new model complaints handling procedure a Complaints Improvement Project Board has been established to oversee 4 sub-projects:
NHS Lothian complaints handling procedure
SPSO complaints processes
Support to NHS Lothian from the SPSO Learning & Improvement Unit

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
33
Learning from Complaints, Concerns, Comments and Compliments The Healthcare Governance Committee has oversight of this work and the subject is a regular agenda item. A revised reporting template has been introduced to support this oversight. Assurance for this works sits with the Healthcare Governance, where this is regular agenda item and a revised reporting template has been developed to monitor oversight of this work. The Healthcare Governance Committee agreed in March 2017 that it accepted moderate assurance that an improvement programme that has been put in place to mitigate the risks in this area. The Committee has asked for an update on this subject at every second meeting shall next consider it in July 2017. During 2016/17 the Board has transferred the responsibility for detailed performance oversight to the relevant Board committee, whilst the Board continues to receive a high level overall performance report. This allows the committees to consider performance management in detail and in the context of all the factors that are pertinent to carrying out the associated functions and services. Additionally with the committees carrying out the detailed scrutiny this creates an opportunity for the Board to have more time for strategic matters. The quality of reports and information to the Board and its committees has a bearing on the effectiveness of the system of corporate governance and the system of quality management. During 2016/17 there has been further development in this area. The Board and its committees have started to use standard levels of assurance (Significant, Moderate, Limited, None) within the reports they receive. The aim of this is to ensure all reports are properly focused and lead to clear conclusions. The use of standard levels provides a common language which helps committees to efficiently communicate with each other and the Board. These levels are now used by the committees to conclude how their assurance needs have been met, as well as to assess the adequacy of improvement plans in relation to performance and the management of corporate risk. The assurance levels which the committees agree are reflected in the Board’s Corporate Risk Register as well as the Board’s routine Quality and Performance Improvement report. Additionally during the year the Board considered a draft strategy entitled Better Information, Better Decisions, Better Care, which set out a proposed way forward to ensure that decision-makers have the information they need. The Board agreed that further consultation with stakeholders should proceed, and that its Strategic Planning Committee shall oversee this work.
The Board members have also participated in two exercises at the start of 2016 to inform the review of the collective performance of the Board;
1. NHSScotland Board Diagnostic Tool 2015/16, and 2. The Board members completed an iMatter questionnaire to produce a team report. You can find out more
about iMatter at: http://www.staffgovernance.scot.nhs.uk/monitoring-employee-experience/imatter/
The vast majority of responses to the questions in the Board diagnostic tool were positive, however the members did identify some opportunities for development and improvement. The members ranked the domains in terms of the level of development required and “Engaging with Stakeholders” was judged to require the most development, whilst “Board Leadership” was judged to require the least development. With regard to engaging with stakeholders, during 2016/17 as has been set out above, the Board has taken forward several measures and developed an improvement programme to attend to the various issues relating to complaints and patient experience. The Board has also revised its template for all Board and committee reports by re-titling a section to “Duty to Inform, Engage, and Consult People who use our services”, and there is supplementary guidance available on the Board’s intranet. The purpose of this change is to promote greater visibility and consideration of this subject as part of the normal conduct of all business. The Board agreed a forward schedule of Board development sessions for 2017 in December 2016. These sessions are designed to give greater focus on the development of the Board and how it functions, rather than being used as briefing sessions. One of these sessions is focussed on patient and public experience.
Process to Review Adequacy and Effectiveness As Accountable Officer I am responsible for reviewing the effectiveness of the system of internal control. The following processes have been established to inform my review of the effectiveness of the system of internal control.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
34
During 2016/17 the executive Board members and other senior managers met formally and informally on a monthly basis as the Corporate Management Team, which I (or the Acting Chief Executive) chaired, to discuss and progress the delivery of the Board’s business.
My direct reports have provided me with certificates of assurance which have been informed by reviews of their systems of internal control, as required by the Scottish Public Finance Manual. The work of the Board’s committees also supports my role as Accountable Officer. This Governance Statement has been informed by the annual reports of the Audit & Risk Committee, Staff Governance Committee, Healthcare Governance Committee, Information Governance Assurance Board (which reports into the Healthcare Governance Committee), Acute Hospitals Committee and the Finance & Resources Committee. The Audit & Risk Committee has governance oversight of system of risk management system, and that committee receives a report on risk management at every meeting. Other committees have responsibility for oversight of specific categories of risk which relate to their remit. The work of all committees includes oversight of compliance with the law and regulatory activity which is relevant to their remits. The Board’s committees use a common template to prepare their annual reports, which has been developed during 2016/17 in order to provide a more explicit report on the assurance they are providing. The committees have confirmed through their annual reports that they have operated in line with their terms of reference in 2016/17, and have or are in the process of reviewing their effectiveness. The committees have also confirmed that they are satisfied that where there are any areas of control weakness, these have been properly acknowledged and have been reflected into the Board’s risk management processes.
My review is also informed by the work of the Board’s internal auditors and external auditors. I routinely attend the Audit & Risk Committee where all audit reports are considered. The Risk Management Steering Group also receives all internal audit reports. The Chief Internal Auditor has provided the following audit opinion in her 2016/17 annual report: Overall, Internal Audit’s work indicates that NHS Lothian has a framework of controls in place that provides reasonable assurance regarding the effective and efficient achievement of the organisation’s objectives and the management of key risks. Proper arrangements are in place, in the areas Internal Audit has reviewed, to promote value for money and secure regularity and propriety in the administration and operation of the organisation. Risk Assessment
The Board has reviewed the corporate risk register and an associated briefing at six of its seven meetings in 2016/17. The standard format for Board and committee papers requires consideration of the relevant risks. Board papers are available on the Board’s website at:
http://www.nhslothian.scot.nhs.uk/OurOrganisation/BoardCommittees/LothianNHSBoard/BoardPapers/Pages/default.aspx
Executive managers are responsible for managing risk. As the Accountable Officer, I am required to ensure that risks are identified, that their significance is assessed and that appropriate remedial action is taken to reduce risk exposure, or eliminate it where possible. I have delegated the executive responsibility for the system of risk management to the Medical Director who is supported by an Associate Director for Quality Improvement & Safety.
The Board published a Risk Management Policy and Operational Procedure in June 2012. The Board also has an Adverse Event Policy and Procedure which the Healthcare Governance Committee approved in March 2014. The Risk Management Policy sets out the responsibility for managing risk at different levels in the organisation, and is clear that all employees have a role to play in managing risk in the organisation and that risk should be managed at the most devolved point in the organisation. The Board has a risk management system with modules on risk management and adverse event management, which supports an organisation-wide approach to risk management. There are also structures and systems in place to manage key risks on a topic basis, e.g. health & safety, patient safety, business continuity management, emergency planning and infection control.
As part of the system of risk management, I chair a monthly Risk Management Steering Group. The role of the Group is to provide a leadership role and develop, review and oversee the implementation of NHS Lothian’s Risk Management Policy and Procedure. The Risk Management Steering Group includes directors, senior managers and others involved in the management of risk. The annual report on risk management has informed this statement.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
35
The Audit & Risk Committee received the 2016/17 Risk Management Annual Report on 19 June 2017, and the key points are summarised below.
With regard to the system of Risk Management, the focus of 2016-17 has been to embed NHS Lothian’s two sets of policies and procedures: the Adverse Event Policy and Procedure (March 2014) and the Risk Management Policy and Procedure (June 2012), set within the context of enhancing NHS Lothian’s safety culture to support improvement. Based on learning and feedback from the service, both policies have been reviewed and are in draft format for completion.
The Healthcare Governance Committee in January 2017 accepted significant assurance on the systems in place to manage and learn from adverse events. Actions taken to improve the processes for managing and learning from adverse events in Lothian, which included:-
The focus has been on improving reliability of processes so that learning is identified in a
more timely fashion There is evidence of process improvement by a reduction in the backlog of reviews and
reduction in time to complete reviews. The May 2017 data showed that the median of significant adverse events reported and closed were both 45 per month and if sustained, no further backlog would build up. This data is reviewed weekly and actions taken to support the service should a backlog start to build up, supported by the Datix Dashboards which provide real time data on management of adverse events.
There has been a considerable body of work undertaken in 2016/17 to develop the system of risk management:
Management have reviewed operational risk registers, and these are routinely reported through management structures
The review and completion of the University Hospitals Services risk register has taken place, and it has been aligned to corporate objectives. This will be used to inform management and the Acute Hospitals Committee, aligned with the Board’s Quality & Performance Improvement Report
Management have reviewed the Health & Social Care Partnerships (“HSCP”) risk registers. This has included harmonising the content where appropriate to reflect risks that are HSCP specific, and those that are common across the system.
There has been active engagement with the Integration Joint Boards/ risk process, including development of the risk registers informed by H&SCP operational risks and a mapping of the flow of risks across H&SCPs, NHS Lothian and IJBs. This is to develop a shared understanding of risk profiles across the system.
Management are working with internal auditors of both NHS Lothian and the IJBs to develop an effective and efficient audit process which will inform the risk management system and audit priorities.
NHS Lothian’s Corporate Risk Register is being reviewed within the context of IJBs. The initial focus is on the risks relating to delayed discharges and GP Sustainability.
Internal audit reviewed the system of risk management in 2016-17 and concluded that the systems of control were adequate, and they did not identify any weakness in controls, apart from one minor point.
The Performance Report (at page 3) sets out the risks on the Board’s corporate risk register at the end of 2016/17. The priorities for management of adverse events for 2017/18 are as follows:-
Sustained process improvement for management of significant adverse events
Maximise mechanisms for learning and feedback to services from individual and themes from reviews
Preparing for the Duty of Candour legislation by mapping and modelling into current adverse event reviews process against the requirements of this legislation due to be introduced in 2018.
The priorities for risk management for 2017/18 are as follows:-

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
36
Continue to embed and improve engagement with risk management processes, with a particular focus on demonstrating how risk management informs priorities and decision making at both corporate and operational levels
Refresh the corporate and operational risk registers to improve clarity of expression of risks, controls and actions to maximise effectiveness of the process
Further develop and test processes for management of risk in partnership with the H&SCPs to ensure optimum management of risk across the whole system including the Integration Joint Boards.
Disclosures
Review of Disclosures made in the 2015/16 Governance Statement The Board continues to hold equipment that cannot be encrypted without breaching the Medicines and Healthcare Products Regulatory Agency licence, and some out of date equipment that cannot be encrypted. There will always be some equipment that cannot be encrypted but the organisation has no alternative to use. The Board’s Caldicott Guardian has a process which requires departments to notify her of any exceptional use of unencrypted equipment. Local departments are required to take appropriate action to minimise any risk. The Board’s standard for transfers of sensitive personal data between departments is that they be carried out securely on IT systems, and measures have been put in place for this to be observed across the organisation. Some fax machines are retained for business continuity reasons. Some departments have had to continue using fax machines to receive sensitive personal data from external organisations. There are planned IT developments, both local and national, which will eventually eliminate the use of fax and hard copy. In the meantime the Caldicott Guardian has a procedure to ensure any exceptions to the standard are clearly documented and risk assessed, with local departments responsible for managing the residual risk. The Information Commissioner’s Office (“ICO”) conducted a consensual audit in February 2016 after reflection on several historic incidents within NHS Lothian relating to personal data. The audit focussed on three areas; training and awareness, records management (manual and electronic) and subject access requests. The ICO published its report on 27 May 2016 which made an assessment of “limited assurance” and issued recommendations in each of these areas. Management implemented an action plan to attend to the recommendations and the issues in the report. The ICO provided a follow-up report in January 2017 which was a positive report recognising a considerable amount of work and improvement. The Information Governance Assurance Board shall oversee the small number of issues from the original report which remain to be addressed. Throughout 2016/17 the Board and the Healthcare Governance Committee have exercised oversight of healthcare associated infection. The Board approved the arrangements for performance reporting and action plans for Clostridium Difficile (C-diff) infection and Staphylococcus Bacteraemia (SAB). The Healthcare Governance Committee received a report on 9th May 2017 which confirmed that the Board has not achieved the Local Delivery Plan standards for SAB with performance at same level as previous year. C-diff infection however has improved significantly and the Local Delivery Plan target has been exceeded. Management have developed robust action plans to continue to improve the Board’s performance for SAB. The key issue for SAB is addressing soft tissue infections and invasive device related infections. To maintain C-Diff performance the key issue remains prudent prescribing and reducing the use of high risk antibiotics. Management have standard infection prevention and control policies which are in line with national guidance and subject to clinical audits, but acknowledge that sustainably delivering targets for healthcare associated infection is a continuing challenge. The Healthcare Governance Committee has agreed that it shall receive progress reports on healthcare associated infection at every second meeting throughout 2017/18 and it will monitor the improvement plan. The Board is required (by regulation) to publish a pharmaceutical care services plan, which is a summary of the pharmaceutical services provided in the area of the Board together with an analysis by the Board of where it believes there is a lack of adequate provision of pharmaceutical services. The Board also has to monitor its plan annually to reflect changes in service provision. During 2015/16 aspects of pharmaceutical care need were fed into the development of the joint strategic needs assessments for integration joint boards. The Board's pharmaceutical care plan is in final draft stage and going through its governance processes. This plan will run for three years from 1 April 2017 and be reviewed annually. If an annual review identified a need for a significant and material change to the plan then this will be brought to the Board’s attention.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
37
NHS Scotland Counter Fraud Services are still undertaking a major case involving a former employee, which covers offences carried out in previous years. Managing delivery of financial balance has been extremely challenging during 2016/17, and the key issues and risks have been discussed in the overview section of the Performance Report (at pages 3 – 24). Both the Finance and Resources Committee and the Board have received regular updates, and had the opportunity to discuss performance and actions to address the position. Board and Committee members have also considered detail in relation to the level of non-recurring support utilised to achieve balance. Regular performance meetings have been held throughout the year to consider management action and progress against Financial Recovery Plans. The Efficiency and Productivity Group has reviewed its terms of reference to consider the sustainability and value programme and plans to oversee a wider range of improvement programmes to support the financial position. The Board did achieve its financial targets for 2016/17. This was achieved with significant reliance on non-recurring resources. The Board agreed its Local Delivery Plan on 5 April, 2017, and this reflected that there remains a gap from financial balance of £22.4m in the 2017/18 Financial Plan. The Scottish Government had indicated that it will be applying a 7.5% efficiency saving requirement to the total level of funding for the Outcomes Framework in 2016/17, recognising the increased flexibility Boards have been given to determine locally how they achieve defined outcomes. The 2015/16 Governance Statement reflected that the Board had factored in an assumed reduction of 7.5% into its financial plan however the actual reduction was £629k greater (total reduction = £2.5m). This reduction is built into the 2017/18 Financial Plan and service management are attempting to mitigate its impact on the level and quality of patient care. Management have taken further steps to ensure that business cases, and the services that they affect, are designed in a manner where the revenue consequences are affordable. New fit-for-purpose healthcare premises are designed and built to higher standards than existing buildings in the estate, so they will often generate some additional revenue consequences. Management have introduced three key changes to the business case development process to mitigate this risk. The revised Scottish Capital Investment Manual requires the Board to follow a process which starts with a focus on the required design of services, which in turn will determine what the Board’s asset management strategy. The asset management strategy sets out how the Board will improve the state of its assets and supporting the needs of the service strategies. The effect of this is that the starting point for early options appraisals should not be larger buildings, unless there is a clear service justification. The Board’s Standing Financial Instructions state that the Board shall follow the Scottish Capital Investment Manual.
Secondly the Facilities Directorate has been directly tasked with delivering new ways of working which will improve productivity and efficiency and absorb the additional costs within their area of control arising from the development of new premises, or reconfiguration of the existing estate.
The Finance & Resources Committee has also requested that business cases should include a holistic assessment of service developments, shared services, and other initiatives which may demonstrate overall resource savings arising from the proposed asset investment. This is embedded within a prioritisation process currently being agreed across health and social care, and is in addition to reviewing the costs arising directly from the creation of new assets. The Finance & Resources Committee has previously highlighted that there are significant risks relating to the issue of improving efficiency & productivity, and the vulnerability of achieving financial balance due to its reliance on the successful delivery of efficiency schemes. There are growing opportunities for efficiency & productivity arising from the Board’s maturing quality agenda, as well as national Sustainability & Value projects. The Comm ittee shall continue to oversee this issue in the context of the delivery of the 2017/18 Financial Plan. Management have successfully resolved a previously disclosed issue relating to the invoicing processes with staff agencies, through a file transfer solution. However there is still continuing dialogue with a company to improve the recharging functionality within the Staff Bank software so as to improve the financial information available to local management teams. Management previously identified the need to update the information asset register for the Royal Edinburgh Hospital & Associated Services (“REAS”), and following from that the information risk assessment for that area. Management have updated the REAS Information Governance and Public Records Action Plan to include these actions. More generally NHS Lothian has prepared its Information Asset Register for the whole organisation, and this is subject to continuous review.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
38
Management have provided regular reports to the Healthcare Governance Committee on the action plan to improve the management of adverse events, particularly with respect to the backlogs in adverse events within acute hospitals and those relating to suicide. Healthcare Improvement Scotland has removed NHS Lothian from the risk register relating to suicide management. The Healthcare Governance Committee agreed in January 2017 that it had a significant level of assurance with regard to the management of adverse events. Although there had been moderate improvement in the number of patients delayed in Lothian leading up to April 2016, this performance was not sustained throughout 2016/17 financial year. This raises concern about the performance and the negative impact it has on individual patients and the systemic problems it creates within hospitals. From April 2016 the integration joint boards have been responsible for the planning and performance of the health functions relating to delayed discharges and all IJBs have developed delayed discharge improvement trajectories. These trajectories facilitate dialogue between Health Board and IJB colleagues as to the planning and delivery of services. The Chief Officers of the integration joint boards report via the Deputy Chief Executive to the Scottish Government on the delivery of key targets which include delayed discharges and actions in response to performance. There are a number of multidisciplinary fora with representation from senior management, health & social care partnerships and hospitals where delayed discharge performance is routinely reviewed and improvement actions explored and agreed; Healthcare Governance Committee, the Cost Quality & Performance Group meetings, the Corporate Management Team, and weekly teleconferences. The Healthcare Governance Committee received moderate assurance with regard to their being improved oversight of delayed discharges and enhanced joint working. However it was acknowledged that due to the significant increase in delays there was an ongoing risk associated with achieving the desired level of performance, and the Committee has concerns with regard to the negative impact this has on patient experience and outcomes from care. The Committee has limited assurance that improvement plans are in place to mitigate the risk. The Committee has requested that management present improvement plans at its July 2017 meeting. The Scottish Government set out the performance objectives for integration joint boards in January 2017. This included six performance measures which the Scottish Government shall monitor nationally, and one of those is delayed discharges. It is anticipated that these measures will form the basis for much of the improvement work within integration joint boards over the coming years. As at March 2017 there were 153 delays in Lothian above the agreed trajectory. The chief officers have provided the Deputy Chief Executive with initial trajectories for 2017/18 for each local authority area, as part of the measures to improve performance in 2017/18.
There is an increasing level of risk of the Board not being able to deliver upon its various performance measures, particularly the “effective” and “timely” measures that are linked to the Board’s operational capacity. The Performance Report within these annual accounts describes the key issues and risks that the Board faces, namely:
Demography, inequalities and ill health
Multimorbidity
Health service demand
Tighter finances In particular this impacts on the delivery of the treatment time guarantee and the outpatient waiting times, both in terms of the number of patients waiting longer than 12 weeks and the increasing length of those waits. The previous decision to stop using the independent sector to provide operational capacity, in light of financial constraints set out in the Board’s Financial Plan, does increase the challenge in minimising the difference between core capacity and service demand. The Board is supporting Demand, Capacity, Activity and Queue analysis at a specialty level. This takes account of opportunities for improvements and efficiencies to develop new performance trajectories. Those trajectories provide a baseline for performance monitoring. There is also an outpatient improvement programme and a theatre improvement programme, both of which have detailed work streams with the aims to reduce demand, optimise capacity and support technological solutions to reduce patient attendance in secondary care. Additionally the Medical Director is supporting a clinically led risk assessment framework to help identify and reduce risk for patients waiting for long periods for their new outpatient appointment.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
39
New Disclosures for 2016/17 The Facilities directorate has followed the Board’s procedure to register its information assets, however it has not carried out the associated risk assessments for those assets. Management shall carry out a formal review of the requirements in the first quarter of 2017/18 and any required actions will be taken thereafter. Some diagnostic tests rely on scarce expertise to undertake and require the secure transfer of identifiable or disclosive data to university laboratories or small scientific enterprises (often health service or university spin offs) in the UK and overseas. Individual exceptions to standard practice are put in place to ensure that essential clinical need for care is met. The Caldicott Guardian then scrutinises the evidence, tissue and information governance. Thereafter agreed data sharing and processing agreements are put in place as appropriate, and standard operating procedures for transfer of data and clinical material are agreed.
A third party contractor had a data breach which in turn compromised the security of data relating to some of the Board’s employees. All of the affected employees have been informed and provided with appropriate advice on what action to take. There are ongoing discussions with the company at a national level with regard to service provision and improving the system of control. The Board has started to prepare for the General Data Protection Regulation. The Regulation introduces a number of new requirements, including an accountability principle, which requires organisations to be able to demonstrate that they comply with the principles of the Regulation. The new arrangements need to be put in place before UK legislation has been passed, in order to be operational by the Regulation’s compliance date of 25 May 2018. The Information Commissioner’s guidance shall inform this work. During the year an external case note review of the Lothian Perinatal Community Service was completed. This indicated poor and inconsistent compliance with record-keeping standards, which has the potential to adversely affect patient care. Management are taking action to address the issues that have been raised. The Healthcare Governance Committee agreed in March 2017 that it had limited assurance with regard to the improvement plans to address the risks associated with GP workforce sustainability. The Committee considered plans in May 2017, which although well received, did not provide further assurance that there will be an improvement. Consequently the Committee has asked for a further update in July 2017. The Board currently does not currently have a long-term sustainable financial plan. One of the Board’s Corporate Objectives for 2017/18 is to “Achieve Greater Financial Sustainability and Value”, and one of the agreed actions is to develop a 3-year financial plan. This financial plan is to set out plans for investment and reform to ensure the best use of available resources and return NHS Lothian to recurring balance. The Finance & Resources Committee has approved initial agreements for the replacement of the Eye Pavilion and bridging projects for the Cancer Centre which address significant capacity and physical environment issues. In the absence of Scottish Government funding being available for these, Committee members have raised concerns about the Board’s ability to address these issues and the impact on the patient environment. Management shall develop contingency plans to provide an alternative response to the issues in the event that funding is not made available for the business cases.
The Care Inspectorate and Healthcare Improvement Scotland (HIS) carried out a joint inspection of older people’s services in health and social work across Edinburgh from October to December 2016. The City of Edinburgh Health & Social Care Partnership was measured against 10 quality indicators to establish if the health and social care services in Edinburgh worked together to provide good outcomes for older people and their unpaid carers. The findings of the report highlighted a number of specific areas for improvement related around delivery of key processes including the number of assessments and adult protection referrals. There were 17 recommendations in the report and several key issues that need improvement.
The management of the City of Edinburgh Health & Social Care Partnership have developed a full service improvement plan which has 90 actions which cover all this matters raised in the report. Many of the actions had commenced before the inspection was carried out. A representative group shall meet monthly and oversee the improvement plan. A process has been put in place to ensure managers provide progress reports on the action plan for the group’s meetings.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
40
REMUNERATION AND STAFF REPORT
1. Board Members’ and Senior Employees’ Remuneration
Information disclosed in this report relates to the remuneration of Board Members and senior managers who directly report to the Chief Executive. Other disclosures in these accounts provide details of the interests of Board Members and senior managers, and information about related party transactions.
Board Members and senior managers are remunerated in accordance with approved national pay rates. All posts at this level are subject to rigorous job evaluation arrangements and the pay scales applied reflect the outcomes of these processes. All extant policy guidance issued by Scottish Government Health & Social Care Directorate (SGHSCD) has been appropriately applied and agreed by the Remuneration Committee. Determination of individual salary placement on appointment is guided by the terms of circulars Health Department Letter (HDL) (2006)23 and HDL (2006)59 as amended by subsequent directives issued by SGHSCD.
All senior manager posts have been evaluated using the HAY methodology through the National Evaluation Committee. NHS Lothian Executive Board Members are appointed and graded within the new Executive Cohort in accordance with HDL (2006)23. Other senior managers, other than those in transitional grades as determined by NHS Management Executive Letter (MEL) (2000)25, are appointed and graded to a new Senior Manager cohort in compliance with HDL (2006)59. Managers within transitional grades have been re-evaluated to grades within Agenda for Change pay-scales.
In accordance with the Financial Reporting Manual (FReM) and the Companies Act, 2013-14 was the first year that publication of the “pension benefits” was required. This calculation aims to bring public bodies in line with other industries in disclosing an assessed cumulative pension benefit for a standard 20 year period, which is the estimated life span following retirement.
Details of Board Members’ remuneration are disclosed in notes 2a – 2e of the remuneration report and have been subject to audit.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
41
REMUNERATION REPORT (AUDITED)
2(a). Board Members’ and Senior Employees’ Remuneration – 2016/17
Gross Salary (Bands
of £5,000)
Benefits in kind (£’000)
Total Earnings in Year
(Bands of £5,000)
Pension Benefits (£’000)
Total Remuneration
(Bands of £5,000)
Remuneration of: Executive Members
Mr Tim Davison, Chief Executive note 1
175-180 - 175-180 48.8 225-230
Mrs Susan Goldsmith, Director of Finance 135-140 - 135-140 16 150-155
Dr David Farquharson, Medical Director (Until 31/03/2017) note 2
200-205 - 200-205 16 220-225
Miss Tracey Gillies, Medical Director (From 01/02/2017) note 3
25-30
- 25-30 102.1 125-130
Professor Alison McCallum, Director of Public Health and Health Policy
120-125 - 120-125 22.6 145-150
Professor Alex McMahon, Nurse Director (From 20/06/2016) note 4
100-105 - 100-105 23 23-130
Non Executive Members
Mr Brian Houston, Chairman 40-45 - 40-45 - 40-45
Cllr Donald Grant, East Lothian Council 5-10 - 5-10 - 5-10
Cllr Ricky Henderson, City of Edinburgh Council 5-10 - 5-10 - 5-10
Cllr Catherine Johnston, Midlothian Council 5-10 - 5-10 - 5-10
Cllr Harry Cartmill, West Lothian Council (From 01/06/2016)note 5 5-10 - 5-10 - 5-10
Mr Peter Johnston note 6 15-20 - 15-20 - 15-20
Mrs Julie McDowell (until 31/05/17) note 7 25-30 - 25-30 - 25-30
Dr Richard Williams note 8
130-135 - 130-135 54.6 185-190
Mrs Shulah Allan, Public Partnership Forum Chair and Vice Chair 15-20 - 15-20 - 15-20
Mr Michael Ash note 9 15-20 - 15-20 - 15-20
Mrs Alison Mitchell 15-20 - 15-20 - 15-20
Mr John Oates 5-10 - 5-10 - 5-10
Mrs Lynsay Williams 5-10 - 5-10 - 5-10
Mr Peter Murray 5-10 - 5-10 - 5-10
Mr Martin Hill note 10 10-15 - 10-15 - 10-15
Mrs Carolyn Hirst 5-10 - 5-10 - 5-10
Mrs Kay Blair 15-20 - 15-20 - 15-20
Professor Moira Whyte, The University of Edinburgh note 11
5-10 - 5-10 - 5-10
Ms Fiona Ireland (From 01/09/2016) note 12
0-5 - 0-5 - 0-5
Mr Alex Joyce, Employee Director note 13
50-55 - 5-10 8 50-55
Cllr Frank Toner, West Lothian Council (Until 24/05/2016) note 14 0-5 - 0-5 - 0-5
Mr George Walker (Until 31/01/2017) note 15 20-25 - 20-25 - 20-25
Mrs Alison Meiklejohn, Chair of Lothian Area Clinical Forum (until 31/08/2016)
note 16 60-65 - 60-65 8.1 65-70
Other Senior Employees
Mr Jim Crombie, Deputy Chief Executive (From 26/01/2017) note 17 135-140 4 135-140 37.9 180-185
Simon Watson, Chief Quality Officer (From 04/04/2016) 135-140 - 135-140 179 315-320
Mr James Forrest, Chief Officer, West Lothian Integration Joint Board
note 18 45-50 1.1 50-55 7.3 55-60
Mr David Small, Chief Officer, East Lothian Integration Joint Board note 19
50-55 - 50-55 18.2 65-70
Eibhlin McHugh, Chief Officer, Midlothian Integration Joint Board note 20
75-80 - 75-80 - 75-80
Rob McCulloch-Graham, Chief Officer, Edinburgh Integration Joint Board
note 21
50-55 - 50-55 - 50-55
Mrs Janis Butler, Interim Director of Human Resources 95-100 - 95-100 73.5 165-170
5.1 587.4
There were no Performance related bonus payable for 2016-17.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
42
Notes to Remuneration Table 2(a)
1. Tim Davison exited the pension scheme on 31/03/2014 and the Pension Benefits figures above are in line with this change.
2. David Farquharson exited the pension scheme on 31/03/2012 and the Pension Benefits figures above are in line with this change.
3. The Pension Benefit figure for Tracey Gillies includes contributions from her previous employer. Her annualised salary figure would be £160,904.04.
4. The salary figure for Alex McMahon relates to his position as acting Nurse Director until 20/06/2016 and substantive post thereafter.
5. The annualised salary figure for Harry Cartmill would be £8,169. 6. Peter Johnston received £8,169 as Vice Chair of the Midlothian IJB. 7. Julie McDowell's remuneration includes £1,940.72 as Vice Chair of West Lothian IJB until 22/06/2016 and
£8,008 as arrears of pay for her role as Vice Chair of the West lothian IJB. The annualised salary for the IJB duties would be £8,169.
8. Richard William’s salary includes £125,524.06 for non-board duties. 9. Michael Ash's remuneration includes £1,869 as Vice Chair of the East Lothian IJB. The annualised salary
figure for the IJB position would be £8,169. 10. Martin Hill's remuneration includes £6,308.28 as Vice Chair of the West Lothian IJB from 23/06/2016. The
annualised sary figure for this position would be £8,169. 11. Moira Whyte is an employee of The University of Edinburgh and her Non Executive Allowance is charged
to NHS Lothian. 12. Fiona Ireland has withheld the consent to disclose the salary and pension contributions for her non-board
duties. The annualised salary figure for her non-executive position would be £8,169. 13. The salary figure for Alex Joyce includes £41,898.75 for non board duties. 14. The annualised salary figure for Frank Toner would be £8,169. 15. George Walker's remuneration includes £6,807.50 as Chair of the Edinburgh IJB until 31/01/2017. The
annualised salary for all his positions would be £24,507. 16. The salary figure for Alison Meiklejohn includes £58,217.04 for non-board duties. 17. The salary figure for Jim Crombie includes the salaries as Chief Officer until 10/07/2016, Acting Chief
Executive until 25/01/2017 and Deputy Chief Executive from 26/01/2017. 18. The above cost is the 50% NHS Lothian’s share of the salary, the other 50% for James Forrest are
charged to West Lothian Council. This salary is in relation to their role as Chief Officer of the IJB and is disclosed IJB accounts.
19. The above cost is the 50% NHS Lothian’s share of the salary, the other 50% of the costs for David Small are charged to East Lothian Council. This salary is in relation to their role as Chief Officer of the IJB and is disclosed IJB accounts.
20. The above cost is the 50% NHS Lothian’s share of the salary, which is charged to us by Midlothian Council as Eibhlin McHugh is an employee of Midlothian Council. This salary is in relation to their role as Chief Officer of the IJB and is disclosed IJB accounts.
21. The above cost is the 50% NHS Lothian’s share of the salary, which is charged to us by The City of Edinburgh Council as Rob McCulloch-Graham is an employee of The City of Edinburgh Council. This salary is in relation to their role as Chief Officer of the IJB and is disclosed IJB accounts.
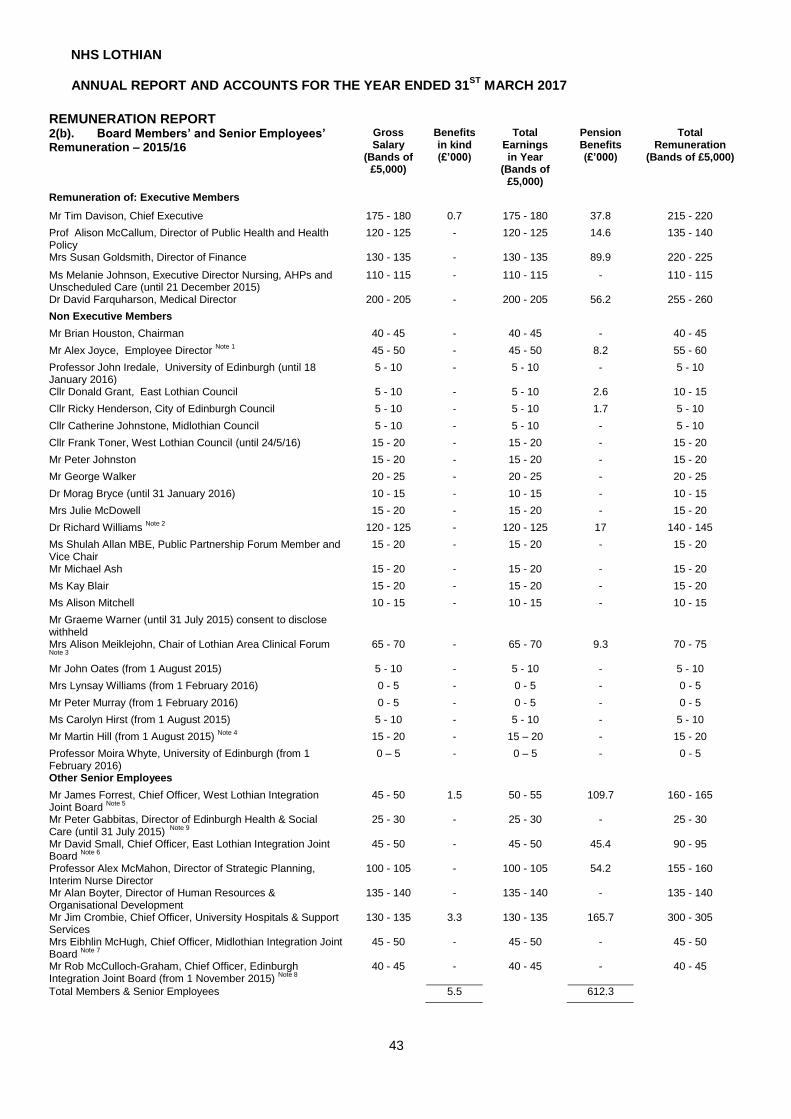
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
43
REMUNERATION REPORT 2(b). Board Members’ and Senior Employees’ Remuneration – 2015/16
Gross Salary
(Bands of £5,000)
Benefits in kind (£’000)
Total Earnings in Year
(Bands of £5,000)
Pension Benefits (£’000)
Total Remuneration
(Bands of £5,000)
Remuneration of: Executive Members
Mr Tim Davison, Chief Executive 175 - 180 0.7 175 - 180 37.8 215 - 220
Prof Alison McCallum, Director of Public Health and Health Policy
120 - 125 - 120 - 125 14.6 135 - 140
Mrs Susan Goldsmith, Director of Finance 130 - 135 - 130 - 135 89.9 220 - 225
Ms Melanie Johnson, Executive Director Nursing, AHPs and Unscheduled Care (until 21 December 2015)
110 - 115 - 110 - 115 - 110 - 115
Dr David Farquharson, Medical Director 200 - 205 - 200 - 205 56.2 255 - 260
Non Executive Members
Mr Brian Houston, Chairman 40 - 45 - 40 - 45 - 40 - 45
Mr Alex Joyce, Employee Director Note 1
45 - 50 - 45 - 50 8.2 55 - 60
Professor John Iredale, University of Edinburgh (until 18 January 2016)
5 - 10 - 5 - 10 - 5 - 10
Cllr Donald Grant, East Lothian Council 5 - 10 - 5 - 10 2.6 10 - 15
Cllr Ricky Henderson, City of Edinburgh Council 5 - 10 - 5 - 10 1.7 5 - 10
Cllr Catherine Johnstone, Midlothian Council 5 - 10 - 5 - 10 - 5 - 10
Cllr Frank Toner, West Lothian Council (until 24/5/16) 15 - 20 - 15 - 20 - 15 - 20
Mr Peter Johnston 15 - 20 - 15 - 20 - 15 - 20
Mr George Walker 20 - 25 - 20 - 25 - 20 - 25
Dr Morag Bryce (until 31 January 2016) 10 - 15 - 10 - 15 - 10 - 15
Mrs Julie McDowell 15 - 20 - 15 - 20 - 15 - 20
Dr Richard Williams Note 2
120 - 125 - 120 - 125 17 140 - 145
Ms Shulah Allan MBE, Public Partnership Forum Member and Vice Chair
15 - 20 - 15 - 20 - 15 - 20
Mr Michael Ash 15 - 20 - 15 - 20 - 15 - 20
Ms Kay Blair 15 - 20 - 15 - 20 - 15 - 20
Ms Alison Mitchell 10 - 15 - 10 - 15 - 10 - 15
Mr Graeme Warner (until 31 July 2015) consent to disclose withheld
Mrs Alison Meiklejohn, Chair of Lothian Area Clinical Forum Note 3
65 - 70 - 65 - 70 9.3 70 - 75
Mr John Oates (from 1 August 2015) 5 - 10 - 5 - 10 - 5 - 10
Mrs Lynsay Williams (from 1 February 2016) 0 - 5 - 0 - 5 - 0 - 5
Mr Peter Murray (from 1 February 2016) 0 - 5 - 0 - 5 - 0 - 5
Ms Carolyn Hirst (from 1 August 2015) 5 - 10 - 5 - 10 - 5 - 10
Mr Martin Hill (from 1 August 2015) Note 4
15 - 20 - 15 – 20 - 15 - 20
Professor Moira Whyte, University of Edinburgh (from 1 February 2016)
0 – 5 - 0 – 5 - 0 - 5
Other Senior Employees
Mr James Forrest, Chief Officer, West Lothian Integration Joint Board
Note 5
45 - 50 1.5 50 - 55 109.7 160 - 165
Mr Peter Gabbitas, Director of Edinburgh Health & Social Care (until 31 July 2015)
Note 9 25 - 30 - 25 - 30 - 25 - 30
Mr David Small, Chief Officer, East Lothian Integration Joint Board
Note 6
45 - 50 - 45 - 50 45.4 90 - 95
Professor Alex McMahon, Director of Strategic Planning, Interim Nurse Director
100 - 105 - 100 - 105 54.2 155 - 160
Mr Alan Boyter, Director of Human Resources & Organisational Development
135 - 140 - 135 - 140 - 135 - 140
Mr Jim Crombie, Chief Officer, University Hospitals & Support Services
130 - 135 3.3 130 - 135 165.7 300 - 305
Mrs Eibhlin McHugh, Chief Officer, Midlothian Integration Joint Board
Note 7
45 - 50 - 45 - 50 - 45 - 50
Mr Rob McCulloch-Graham, Chief Officer, Edinburgh Integration Joint Board (from 1 November 2015)
Note 8 40 - 45 - 40 - 45 - 40 - 45
Total Members & Senior Employees 5.5 612.3

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
44
Notes to Remuneration Tables 2(b) 1. Alex Joyce’s salary includes £41,000 in respect of non-board duties. 2. Richard Williams’s salary includes £115,000 in respect of non-board duties. 3. Alison Meiklejohn’s salary includes £58,000 in respect of non- board duties 4. Martin Hill’s salary includes £11,000 in respect of non-board duties. 5. 50% of the costs for James Forrest are charged to West Lothian Council. The above figures therefore show
NHS Lothian’s share. 6. 50% of the costs for David Small are charged to East Lothian Council. The above figures therefore show NHS
Lothian’s share. 7. Eibhlin McHugh is an employee of Midlothian Council and 50% of her salary is charged to NHS Lothian. The
above figures therefore show NHS Lothian’s share. 8. Rob McCulloch-Graham is an employee of City of Edinburgh Council and 50% of his salary is charged to NHS
Lothian. The above figures therefore show NHS Lothian’s share. 9. 50% of the costs for Peter Gabbitas were charged to City of Edinburgh Council. The above figures therefore
show NHS Lothian’s share.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
45
2(c) Cash Equivalent Transfer Value (CETV) of deferred pension rights 2016/2017
Total accrued
pension at age 60 at 31
March (Bands of
£5,000)
Real increase in pension
at age 60
(Bands of £2,500)
Total accrued lump sum at age 60 at 31
March (Bands of
£5,000)
Real increase in lump sum
at age 60
(Bands of £2,500)
Cash Equivalent
Transfer Value (CETV) at 31 March 2016
£’000
Cash Equivalent
TransferValue (CETV) at 31 March 2015
£’000
Real increase in CETV in
year £’000
Pension Values: Executive Members
Mr Tim Davison, Chief Executive note 1
70-75 0-2.5 220-225 5-7.5 1497 1580 84
Mrs Susan Goldsmith, Director of Finance 40-45 0-2.5 125-130 2.5-5 888 947 39
Dr David Farquharson, Medical Director (Until 31/03/2017) note 2
110-115 0-2.5 335-340 5-7.5 2422 2417 -4
Miss Tracey Gillies, Medical Director (From 01/02/2017) note 3
50-55 2.5-5 135-140 5-7.5 808 901 94
Professor Alison McCallum, Director of Public Health and Health policy
45-50 0-2.5 135-140 5-7.5 947 1012 47
Alex Mcmahon, Nurse Director (From 20/06/2016) 15-20 0-2.5 50-55 2.5-5 294 333 25
Pension Values: Non Executive Members
Dr Richard Williams note 4 + 5
60-65 2.5-5 180-185 7.5-10 - - -
Mr Alex Joyce note 4
20-25 0-2.5 60-65 0-2.5 427 450 19
Mrs Alison Meiklejohn (until 31/08/2016) note 4
25-30 0-2.5 85-90 0-2.5 562 592 23
Pension Values: Other Senior Employees
Mr Jim Crombie, Deputy Chief Executive (From 26/01/2017) 40-45 2.5-5 125-130 7.5-10 810 884 54
Mrs Janis Butler, Interim Director of Human Resources 35-40 2.5-5 95-100 5-7.5 508 572 64
Mr James Forrest, Chief Officer, West Lothian Integration Joint Board 50-55 0-2.5 155-160 0-2.5 1090 1137 33
Mr David Small, Chief Officer, East Lothian Integration Joint Board 40-45 0-2.5 120-125 5-7.5 810 871 47
Mr Simon Watson, Chief Quality Officer (From 04/04/2016) 30-35 7.5-10 85-90 20-22.5 358 499 141
The real discount rate used to evaluate CETV has been as advised by the UK Government Actuaries Department. Unless also subject to an employment contract with the Board, non executive members have no deferred pension rights under the NHS Superannuation Scheme for Scotland. Such members are therefore not included in the schedule of CETV transfer values above.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
46
Notes to Pension Table 2(c)
1. Tim Davison exited the pension scheme on 31/03/2014 and the figures above are as per the prior year. 2. David Farquharson exited the pension scheme on 31/03/2012 and the figures above are as per the prior
year. 3. Pension Contributions and Real Increases for Tracey Gillies include contributions from her previous
employer. 4. Pension Contributions for Richard Williams, Alex Joyce and Alison Meklejohn relate to their substantive
posts. 5. SPPA cannot provide CETV calculations for Richard Williams because he has reached the age limit for
transfers. 6. Fiona Ireland has withheld the consent to disclose the pension contributions for her non-board duties. 7. Ricky Henderson and Donald Grant had been erronuosly enrolled on the pension scheme. Their position
has been rectified during the year and for this reason they are no longer disclosed.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
47
2(d) Cash Equivalent Transfer Value (CETV) of deferred pension rights 2015/16
Total accrued pension at
age 60 at 31 March
(Bands of £5,000)
Real increase in pension
at age 60
(Bands of £2,500)
Total accrued lump sum at age 60 at 31
March (Bands of
£5,000)
Real increase in lump sum
at age 60
(Bands of £2,500)
Cash Equivalent
Transfer Value (CETV) at 31 March 2016
£’000
Cash Equivalent
TransferValue (CETV) at 31 March 2015
£’000
Real increase in CETV in
year £’000
Pension Values: Executive Members
Mr Tim Davison, Chief Executive 70 – 75 0.0 – 2.5 215 – 220 2.5 – 5.0 1,458 1,386 72
Prof Alison McCallum, Director of Public Health and Health Policy 40 – 45 0.0 – 2.5 125 – 130 2.5 – 5.0 924 869 37
Mrs Susan Goldsmith, Director of Finance 40 – 45 2.5 – 5.0 120 – 125 12.5 – 15.0 866 743 103
Ms Melanie Johnson, Executive Director Nursing, AHPs and Unscheduled Care (until 21 December 2015)
35 – 40 0 115 – 120 0 805 981 0
Dr David Farquharson, Medical Director 105 – 110 0.0 – 2.5 325 – 330 5.0 – 7.5 2,389 2,381 8
Pension Values: Non Executive Members
Mr Alex Joyce, Employee Director 20 – 25 0.0 – 2.5 60 – 65 0.0 – 2.5 417 395 19 Mrs Alison Meiklejohn, Chair of Lothian Area Clinical Forum 25 – 30 0.0 – 2.5 80 – 85 0.0 – 2.5 546 517 22
Dr Richard Williams 50 – 55 0 – 2.5 150 – 155 2.5 – 5 1,171 1,102 51
Cllr Donald Grant 0 - 5 0 – 2.5 0 0 9 7 3
Cllr Ricky Henderson 0 – 5 0.0 – 2.5 0 0 6 5 1
Pension Values: Other Senior Employees
Professor Alex McMahon, Director of Strategic Planning, Interim Nurse Director
15 – 20 2.5 – 5.0 45 – 50 7.5 – 10.0 285 224 47
Mr James Forrest, Chief Officer, West Lothian Integration Joint Board 50 – 55 5.0 – 7.5 150 – 155 15.0 – 17.5 1,065 926 125
Mr Peter Gabbitas, Director of Edinburgh Health & Social Care (until 31 July 2015)
15 – 20 0 55 – 60 0 391 993 0
Mr David Small, Chief Officer, East Lothian Integration Joint Board 35 – 40 2.5 – 5.0 115 – 120 7.5 – 10.0 789 717 58
Mr Jim Crombie, Chief Officer, University Hospitals & Support Services 40 – 45 7.5 – 10.0 120 – 125 22.5 – 25.0 789 614 157
Mr Alan Boyter, Director of Human Resources & Organisational Development
45 – 50 0 140 – 145 0 958 1,142 0
703
The real discount rate used to evaluate CETV has been as advised by the UK Government Actuaries Department. Unless also subject to an employment contract with the Board, non executive members have no deferred pension rights under the NHS Superannuation Scheme for Scotland. Such members are therefore not included in the schedule of CETV transfer values above.
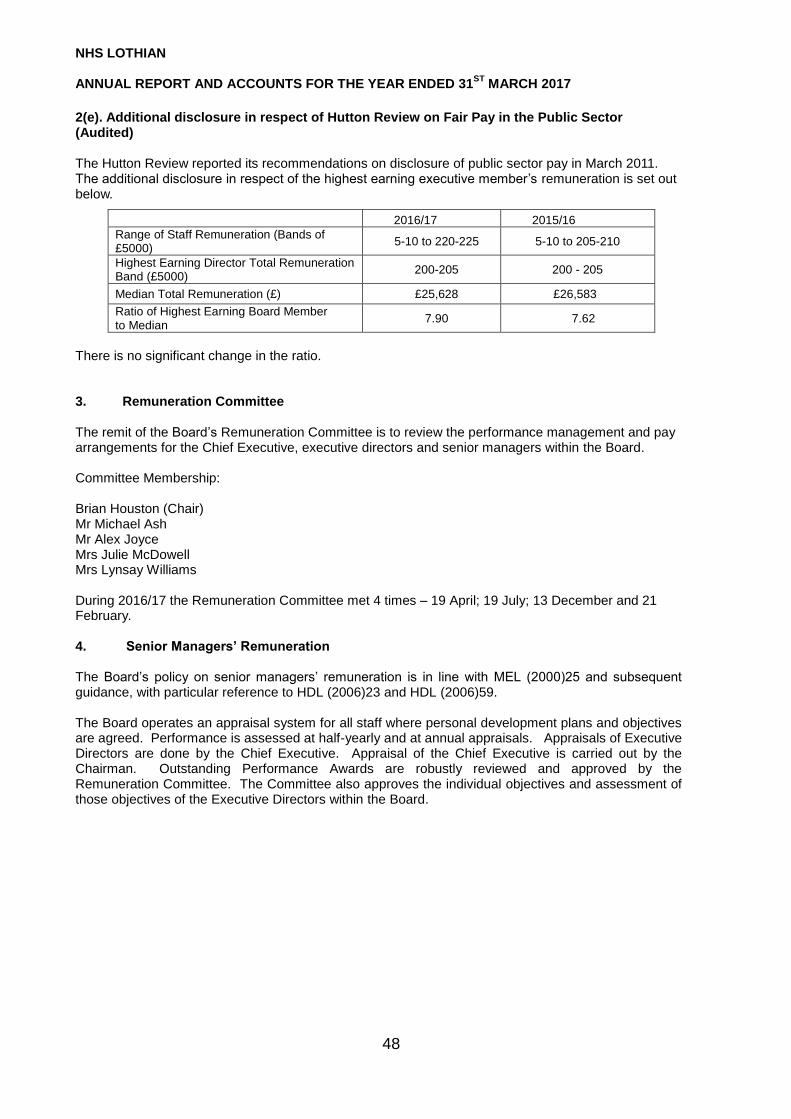
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
48
2(e). Additional disclosure in respect of Hutton Review on Fair Pay in the Public Sector (Audited) The Hutton Review reported its recommendations on disclosure of public sector pay in March 2011. The additional disclosure in respect of the highest earning executive member’s remuneration is set out below.
2016/17 2015/16
Range of Staff Remuneration (Bands of £5000)
5-10 to 220-225 5-10 to 205-210
Highest Earning Director Total Remuneration Band (£5000)
200-205 200 - 205
Median Total Remuneration (£) £25,628 £26,583
Ratio of Highest Earning Board Member to Median
7.90 7.62
There is no significant change in the ratio.
3. Remuneration Committee The remit of the Board’s Remuneration Committee is to review the performance management and pay arrangements for the Chief Executive, executive directors and senior managers within the Board. Committee Membership: Brian Houston (Chair) Mr Michael Ash Mr Alex Joyce Mrs Julie McDowell Mrs Lynsay Williams During 2016/17 the Remuneration Committee met 4 times – 19 April; 19 July; 13 December and 21 February. 4. Senior Managers’ Remuneration The Board’s policy on senior managers’ remuneration is in line with MEL (2000)25 and subsequent guidance, with particular reference to HDL (2006)23 and HDL (2006)59. The Board operates an appraisal system for all staff where personal development plans and objectives are agreed. Performance is assessed at half-yearly and at annual appraisals. Appraisals of Executive Directors are done by the Chief Executive. Appraisal of the Chief Executive is carried out by the Chairman. Outstanding Performance Awards are robustly reviewed and approved by the Remuneration Committee. The Committee also approves the individual objectives and assessment of those objectives of the Executive Directors within the Board.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
49
STAFF REPORT 1a) HIGHER PAID EMPLOYEES’ REMUNERATION
Other employees, not being directors or senior employees, whose remuneration fell within the following ranges:
Clinical Staff Other Staff 2017
Number 2016
Number 2017
Number 2016
Number
£50,001 to £60,000 559 435 62 61 £60,001 to £70,000 264 228 27 32 £70,001 to £80,000 177 132 16 20 £80,001 to £90,000 169 153 16 12 £90,001 to £100,000 149 129 10 9 £100,001 to £110,000 185 140 4 3 £110,001 to £120,000 110 100 2 2 £120,001 to £130,000 106 88 1 1 £130,001 to £140,000 91 72 1 0 £140,001 to £150,000 70 61 0 0 £150,001 to £160,000 55 51 0 1 £160,001 to £170,000 28 26 0 0 £170,001 to £180,000 16 10 0 0 £180,001 to £190,000 14 8 0 0 £190,001 to £200,000 5 3 0 0 £200,001 and above 6 7 0 0
Clinicians’ remuneration includes only that which arises from their NHS Lothian work.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
50
1.(b) STAFF NUMBERS AND COSTS
Executive Board
Members
Non Executive Members
Permanent Staff
Inward Secondees
Other Staff Outward
Secondees 2017 Total
2016 Total
STAFF COSTS £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000
Salaries & Wages 776 285 750,342 0 0 (2,501) 748,902 720,932 Social security costs 101 16 73,779 0 0 0 73,896 57,822 NHS scheme employers’ costs 54 0 97,282 0 0 0 97,336 94,549 Inward Secondees 0 0 0 346 0 0 346 578 Agency & recharged Univ. Staff 0 0 0 0 19,141 0 19,141 26,743
931 301 921,403 346 19,141 (2,501) 939,621 900,624 Compensation for loss of office
1,901
1,901
739
Pensions to former Board members 0
TOTAL 931 301 923,304 346 19,141 (2,501) 941,522 901,363
Included in the total staff costs above were costs of staff engaged directly on capital projects, charged to capital expenditure of:
92
0 STAFF NUMBERS
Whole time equivalent (WTE) 5 9 20,574 6 211 (43) 20,762 21,145
Included in the total staff numbers above were staff engaged directly on capital projects, charged to capital expenditure of: 3 0 Included in the total staff above were disabled staff of: 286 281 Included in the total staff numbers above were Special Advisers of: 0 0
Note: Staff pension benefits are provided through the NHS Superannuation Scheme for Scotland. Details of the scheme are in note 24

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
51
1c) Staff Composition
2017 2016
Male Female
Prefer not to say
Total Male Female Prefer not to
say Total
Executive Directors 2 3 0 5 2 2 0 4
Non-Executive Directors and Employee Director
9 10 0 19 12 8 0 20
Senior Employees 47 40 0 87 55 42 0 97
Other 5,990 22,453 0 28,443 5,919 20,978 0 26,897
Total Headcount 6,048 22,506 0 28,554 5,988 21,030 0 27,018
1d) Sickness Absence
2017 2016
Sickness Absence Rate
4.89% 5.02%
1e) Staff Policies The Board is fully aware of their obligations around disability. Our application process allows disabled candidates to request any adjustments or assistance that they may be required at the time of interview and then if successful in the work place to allow them to undertake their role. If subsequently during the course of their employment, a member of staff becomes disabled, appropriate adjustments, following Occupational Health advice, would be made to allow them to remain in the workforce. An Annual Report is also prepared for the Staff Governance Committee by protected characteristics which includes disability and the trends and actions required are highlighted. NHS Lothian is also participating in the National Management Training Scheme for disabled candidates and currently two Management Trainees with a disability are working within NHS Lothian. Whilst there are no specific policies relating to disability, all of our policies and procedures recognise our roles and responsibilities around disability.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
52
2a) Exit Packages
Exit Packages - Current Year
2017
Exit Package cost band Number of Compulsory
Number of other
departures agreed
Total number of exit
packages by cost band
< £10,000 0 2 2
£10,000 - £25,000 0 8 8
£25,000 - £50,000 0 8 8
£50,000 - £100,000 0 0 0
£100,000 - £150,000 0 0 0
£150,000 - £200,000 0 0 0
>£200,000 0 0 0
Total number of exit Packages by type
0 18 18
Total Resource Cost (£’000) 0 442 442
Exit Packages –Prior Year
2016
Exit Package cost band Number of Compulsory
Number of other departures
agreed
Total number of exit packages by
cost band
< £10,000 0 17 17
£10,000 - £25,000 0 7 7
£25,000 - £50,000 0 12 12
£50,000 - £100,000 0 8 8
£100,000 - £150,000 0 1 1
£150,000 - £200,000 0 0 0
>£200,000 0 0 0
Total number of exit Packages by type
0 45 45
Total Resource Cost (£’000) 0 1,231 1,231
……………………… …………………….…………… Chief Executive and Accountable Officer
21 June 2017
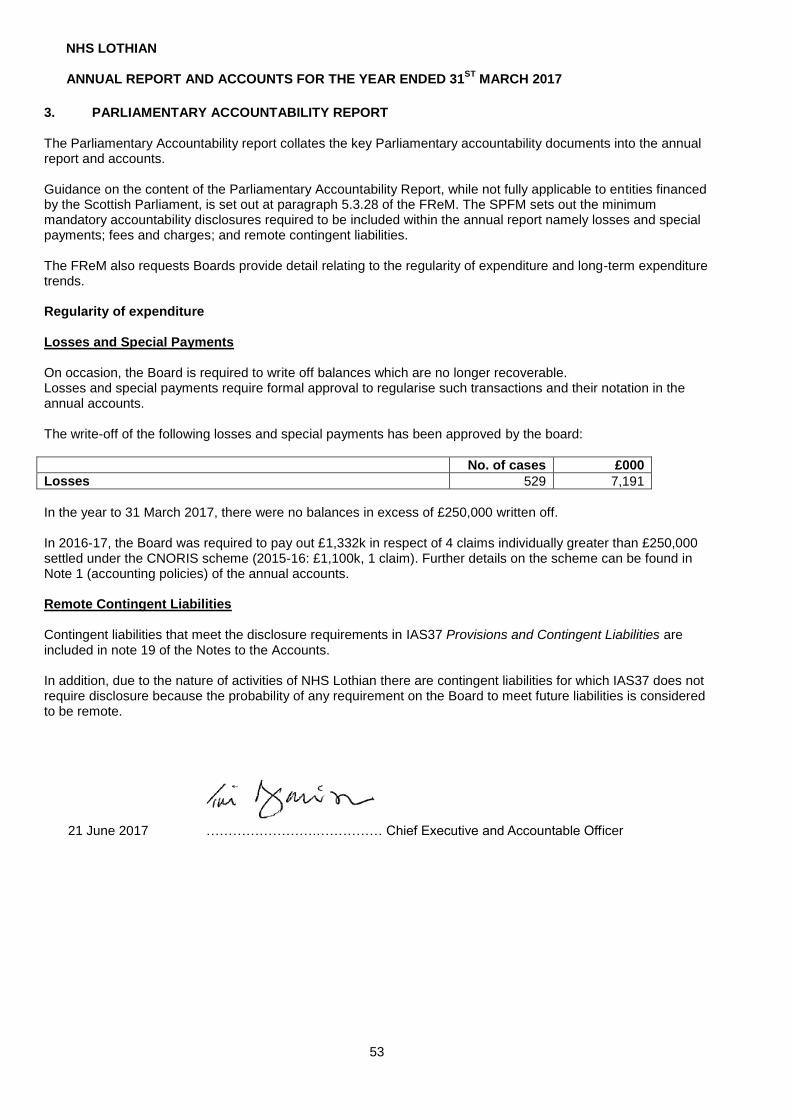
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
53
3. PARLIAMENTARY ACCOUNTABILITY REPORT The Parliamentary Accountability report collates the key Parliamentary accountability documents into the annual report and accounts. Guidance on the content of the Parliamentary Accountability Report, while not fully applicable to entities financed by the Scottish Parliament, is set out at paragraph 5.3.28 of the FReM. The SPFM sets out the minimum mandatory accountability disclosures required to be included within the annual report namely losses and special payments; fees and charges; and remote contingent liabilities. The FReM also requests Boards provide detail relating to the regularity of expenditure and long-term expenditure trends. Regularity of expenditure Losses and Special Payments On occasion, the Board is required to write off balances which are no longer recoverable. Losses and special payments require formal approval to regularise such transactions and their notation in the annual accounts. The write-off of the following losses and special payments has been approved by the board:
No. of cases £000
Losses 529 7,191
In the year to 31 March 2017, there were no balances in excess of £250,000 written off. In 2016-17, the Board was required to pay out £1,332k in respect of 4 claims individually greater than £250,000 settled under the CNORIS scheme (2015-16: £1,100k, 1 claim). Further details on the scheme can be found in Note 1 (accounting policies) of the annual accounts. Remote Contingent Liabilities Contingent liabilities that meet the disclosure requirements in IAS37 Provisions and Contingent Liabilities are included in note 19 of the Notes to the Accounts. In addition, due to the nature of activities of NHS Lothian there are contingent liabilities for which IAS37 does not require disclosure because the probability of any requirement on the Board to meet future liabilities is considered to be remote.
21 June 2017 …………………….…………… Chief Executive and Accountable Officer
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
54
Independent auditor’s report to the members of Lothian Health Board, the Auditor General for Scotland
and the Scottish Parliament
This report is made solely to the parties to whom it is addressed in accordance with the Public Finance and
Accountability (Scotland) Act 2000 and for no other purpose. In accordance with paragraph 120 of the Code of
Audit Practice approved by the Auditor General for Scotland, we do not undertake to have responsibilities to
members or officers, in their individual capacities, or to third parties.
Report on the audit of the financial statements
Opinion on financial statements
We have audited the financial statements in the annual report and accounts of Lothian Health Board and its
group for the year ended 31 March 2017 under the National Health Service (Scotland) Act 1978. The financial
statements comprise the Statement of Consolidated Comprehensive Net Expenditure, the Consolidated Balance
Sheet, the Statement of Consolidated Cash Flow, the Statement of Consolidated Changes in Taxpayers’ Equity
and notes to the financial statements, including a summary of significant accounting policies. The financial
reporting framework that has been applied in their preparation is applicable law and International Financial
Reporting Standards (IFRSs) as adopted by the European Union, and as interpreted and adapted by the 2016/17
Government Financial Reporting Manual (the 2016/17 FReM).
In our opinion the accompanying financial statements:
give a true and fair view in accordance with the National Health Service (Scotland) Act 1978 and
directions made thereunder by the Scottish Ministers of the state of affairs of the board and its group as
at 31 March 2017 and of the net expenditure for the year then ended;
have been properly prepared in accordance with IFRSs as adopted by the European Union, as
interpreted and adapted by the 2016/17 FReM; and
have been prepared in accordance with the requirements of the National Health Service (Scotland) Act
1978 and directions made thereunder by the Scottish Ministers.
Basis of opinion
We conducted our audit in accordance with applicable law and International Standards on Auditing in the UK and
Ireland (ISAs (UK&I)). Our responsibilities under those standards are further described in the Auditor’s
Responsibilities for the Audit of the Financial Statements section of our report. We are independent of the board
and its group in accordance with the ethical requirements that are relevant to our audit of the financial statements
in the UK including the Financial Reporting Council’s Ethical Standards for Auditors, and we have fulfilled our
other ethical responsibilities in accordance with these requirements. We believe that the audit evidence we have
obtained is sufficient and appropriate to provide a basis for our opinion.
Responsibilities of the Accountable Officer for the financial statements
As explained more fully in the Statement of the Chief Executive's Responsibilities as the Accountable Officer of
the Health Board, the Accountable Officer is responsible for the preparation of financial statements that give a
true and fair view in accordance with the financial reporting framework, and for such internal control as the
Accountable Officer determines is necessary to enable the preparation of financial statements that are free from
material misstatement, whether due to fraud or error.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
55
Auditor’s responsibilities for the audit of the financial statements
Our responsibility is to audit and express an opinion on the financial statements in accordance with applicable
legal requirements and ISAs (UK&I) as required by the Code of Audit Practice approved by the Auditor General
for Scotland. Those standards require us to comply with the Financial Reporting Council’s Ethical Standards for
Auditors. An audit involves obtaining evidence about the amounts and disclosures in the financial statements
sufficient to give reasonable assurance that the financial statements are free from material misstatement,
whether caused by fraud or error. This includes an assessment of: whether the accounting policies are
appropriate to the circumstances of the board and its group and have been consistently applied and adequately
disclosed; the reasonableness of significant accounting estimates made by the Accountable Officer; and the
overall presentation of the financial statements.
Our objectives are to achieve reasonable assurance about whether the financial statements as a whole are free
from material misstatement, whether due to fraud or error, and to issue an auditor’s report that includes our
opinion. Reasonable assurance is a high level of assurance, but is not a guarantee that an audit conducted in
accordance with ISAs (UK&I) will always detect a material misstatement when it exists. Misstatements can arise
from fraud or error and are considered material if, individually or in the aggregate, they could reasonably be
expected to influence the economic decisions of users taken on the basis of these financial statements.
Other information in the annual report and accounts
The Accountable Officer is responsible for the other information in the annual report and accounts. The other
information comprises the information other than the financial statements and our auditor’s report thereon. Our
opinion on the financial statements does not cover the other information and we do not express any form of
assurance conclusion thereon except on matters prescribed by the Auditor General for Scotland to the extent
explicitly stated later in this report.
In connection with our audit of the financial statements in accordance with ISAs (UK&I), our responsibility is to
read all the financial and non-financial information in the annual report and accounts to identify material
inconsistencies with the audited financial statements and to identify any information that is apparently materially
incorrect based on, or materially inconsistent with, the knowledge acquired by us in the course of performing the
audit. If we become aware of any apparent material misstatements or inconsistencies we consider the
implications for our report.
Report on regularity of expenditure and income
Opinion on regularity
In our opinion in all material respects the expenditure and income in the financial statements were incurred or
applied in accordance with any applicable enactments and guidance issued by the Scottish Ministers.
Responsibilities for regularity
The Accountable Officer is responsible for ensuring the regularity of expenditure and income. We are
responsible for expressing an opinion on the regularity of expenditure and income in accordance with the Public
Finance and Accountability (Scotland) Act 2000.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
56
Report on other requirements
Opinions on other prescribed matters
We are required by the Auditor General for Scotland to express an opinion on the following matters.
In our opinion, the auditable part of the Remuneration and Staff Report has been properly prepared in
accordance with the National Health Service (Scotland) Act 1978 and directions made thereunder by the Scottish
Ministers.
In our opinion, based on the work undertaken in the course of the audit
the information given in the Performance Report for the financial year for which the financial statements
are prepared is consistent with the financial statements and that report has been prepared in
accordance with the National Health Service (Scotland) Act 1978 and directions made thereunder by
the Scottish Ministers; and
the information given in the Governance Statement for the financial year for which the financial
statements are prepared is consistent with the financial statements and that report has been prepared
in accordance with the National Health Service (Scotland) Act 1978 and directions made thereunder by
the Scottish Ministers.
Matters on which we are required to report by exception
We are required by the Auditor General for Scotland to report to you if, in our opinion:
adequate accounting records have not been kept; or
the financial statements and the auditable part of the Remuneration and Staff Report are not in
agreement with the accounting records; or
we have not received all the information and explanations we require for our audit; or
there has been a failure to achieve a prescribed financial objective.
We have nothing to report in respect of these matters.
Chris Brown (for and on behalf of Scott-Moncrieff)
Exchange Place 3
Edinburgh
EH3 8BL
29 June 2017

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
57
STATEMENT OF CONSOLIDATED COMPREHENSIVE NET EXPENDITURE FOR THE YEAR ENDED 31 MARCH 2017
2015 - 16
£’000 Note £’000 £’000
Clinical Services Costs
1,424,071 Hospital and Community 4 2,418,458
(255,471) Less: Hospital and Community Income 8 (1,122,613)
1,168,600 1,295,845
377,281 Family Health 5 391,119
(11,943) Less: Family Health Income 8 (13,095)
365,338 378,024
1,533,938 Total Clinical Services Costs 1,673,869
9,014 Administration Costs 6 7,038
43,133 Other Non Clinical Services 7 87,813
(34,188) Less: Other Operating Income 8 (96,226)
8,945 (8,413)
0 Joint Ventures accounted for on an equity basis (1,845)
1,551,897 Net Expenditure 1,670,649
OTHER COMPREHENSIVE NET EXPENDITURE
(20,375) Net gain on revaluation of Property Plant and Equipment SOCTE 7,508
1,531,522 Total Comprehensive Expenditure 1,678,157
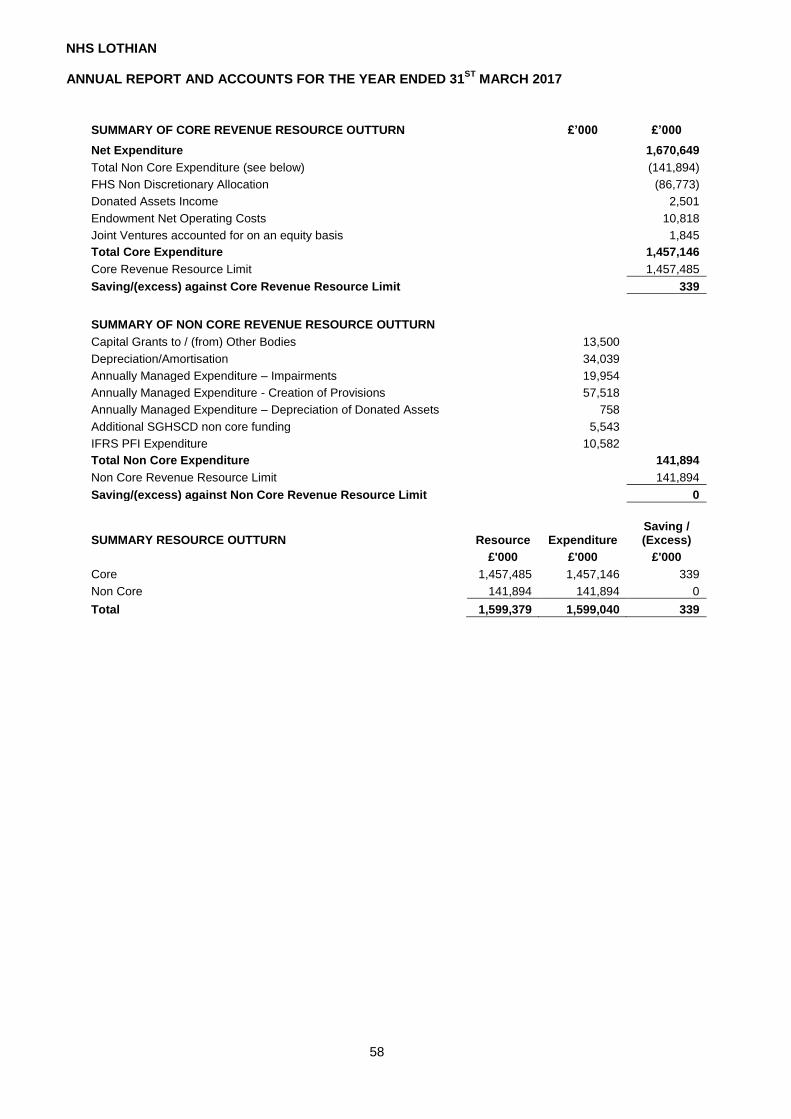
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
58
SUMMARY OF CORE REVENUE RESOURCE OUTTURN £’000 £’000
Net Expenditure 1,670,649
Total Non Core Expenditure (see below) (141,894)
FHS Non Discretionary Allocation (86,773)
Donated Assets Income 2,501
Endowment Net Operating Costs 10,818
Joint Ventures accounted for on an equity basis 1,845
Total Core Expenditure 1,457,146
Core Revenue Resource Limit 1,457,485
Saving/(excess) against Core Revenue Resource Limit 339
SUMMARY OF NON CORE REVENUE RESOURCE OUTTURN
Capital Grants to / (from) Other Bodies 13,500
Depreciation/Amortisation 34,039
Annually Managed Expenditure – Impairments 19,954
Annually Managed Expenditure - Creation of Provisions 57,518
Annually Managed Expenditure – Depreciation of Donated Assets 758
Additional SGHSCD non core funding 5,543
IFRS PFI Expenditure 10,582
Total Non Core Expenditure 141,894
Non Core Revenue Resource Limit 141,894
Saving/(excess) against Non Core Revenue Resource Limit 0
SUMMARY RESOURCE OUTTURN Resource Expenditure Saving / (Excess)
£'000 £'000 £'000
Core 1,457,485 1,457,146 339
Non Core 141,894 141,894 0
Total 1,599,379 1,599,040 339

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
59
CONSOLIDATED BALANCE SHEET FOR THE YEAR ENDED 31 MARCH 2017
Consolidated 2016
Board 2016
Consolidated 2017
Board 2017
£’000 £’000 Note £’000 £’000
Non-current assets:
891,465 891,465 Property, plant and equipment 11d 959,017 959,017
1,862 1,862 Intangible assets 10 868 868
Financial assets:
67,167 1,555 Available for sale financial assets 14 76,378 2,110
0 0 NHS Share of Joint Venture 1,845 0
32,881 32,881 Trade and other receivables 13 44,608 44,608
993,375 927,763 Total non-current assets 1,082,716 1,006,603
Current Assets:
16,078 16,078 Inventories 12 17,450 17,450
85,123 85,050 Trade and other receivables 13 115,718 115,119
2,953 696 Cash and cash equivalents 15 15,308 12,860
104,154 101,824 Total current assets 148,476 145,429
1,097,529 1,029,587 Total assets 1,231,192 1,152,032
Current liabilities
(24,411) (24,411) Provisions 17 (75,069) (75,069)
Financial liabilities:
(205,464) (201,255) Trade and other payables 16 (216,520) (213,531)
(229,875) (225,666) Total current liabilities (291,589) (288,600)
867,654 803,921 Non-current assets plus/(less) net current assets/(liabilities)
939,603 863,432
Non-current liabilities
(94,946) (94,946) Provisions 17 (145,896) (145,896)
Financial liabilities:
(284,420) (284,044) Trade and other payables 16 (377,572) (377,421)
(379,366) (378,990) Total non-current liabilities (523,468) (523,317)
488,288 424,931 Assets less liabilities
416,135 340,115
Taxpayers' Equity
222,506 222,506 General fund SOCTE 152,686 152,686
202,425 202,425 Revaluation reserve SOCTE 187,429 187,429
0 0 Joint Venture reserves SOCTE 1,845 0
63,357 0 Fund held on Trust SOCTE 74,175 0
488,288 424,931 Total taxpayers' equity
416,135 340,115
The Notes to the Accounts, numbered 1 to 29, form an integral part of these Accounts. The Accountable Officer authorised these financial statements for issue on 21st June 2017 ……………………………………………. Director of Finance 21 June 2017
……………………………………………. Chief Executive 21 June 2017
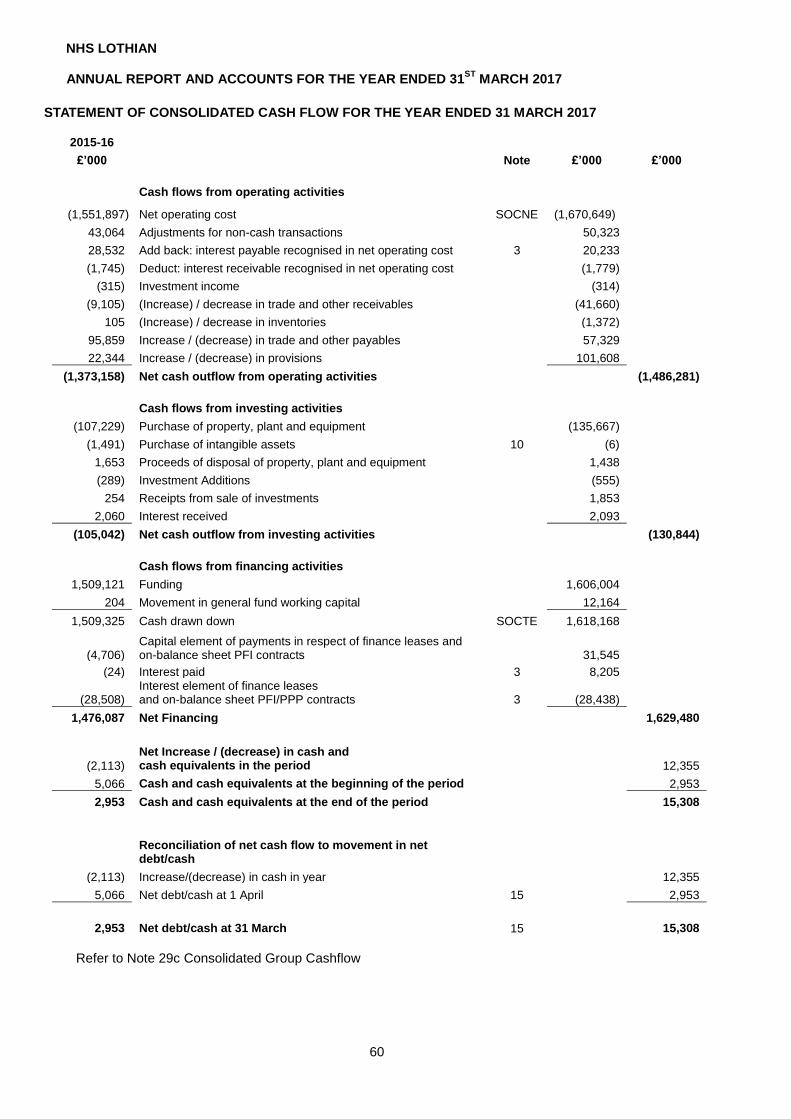
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
60
STATEMENT OF CONSOLIDATED CASH FLOW FOR THE YEAR ENDED 31 MARCH 2017 2015-16
£’000 Note £’000 £’000
Cash flows from operating activities
(1,551,897) Net operating cost SOCNE (1,670,649)
43,064 Adjustments for non-cash transactions 50,323
28,532 Add back: interest payable recognised in net operating cost 3 20,233
(1,745) Deduct: interest receivable recognised in net operating cost (1,779)
(315) Investment income (314)
(9,105) (Increase) / decrease in trade and other receivables (41,660)
105 (Increase) / decrease in inventories (1,372)
95,859 Increase / (decrease) in trade and other payables 57,329
22,344 Increase / (decrease) in provisions 101,608
(1,373,158) Net cash outflow from operating activities (1,486,281)
Cash flows from investing activities
(107,229) Purchase of property, plant and equipment (135,667)
(1,491) Purchase of intangible assets 10 (6)
1,653 Proceeds of disposal of property, plant and equipment 1,438
(289) Investment Additions (555)
254 Receipts from sale of investments 1,853
2,060 Interest received 2,093
(105,042) Net cash outflow from investing activities (130,844)
Cash flows from financing activities
1,509,121 Funding 1,606,004
204 Movement in general fund working capital 12,164
1,509,325 Cash drawn down SOCTE 1,618,168
(4,706) Capital element of payments in respect of finance leases and on-balance sheet PFI contracts 31,545
(24) Interest paid 3 8,205
(28,508) Interest element of finance leases and on-balance sheet PFI/PPP contracts 3 (28,438)
1,476,087 Net Financing 1,629,480
(2,113)
Net Increase / (decrease) in cash and cash equivalents in the period 12,355
5,066 Cash and cash equivalents at the beginning of the period 2,953
2,953 Cash and cash equivalents at the end of the period 15,308
Reconciliation of net cash flow to movement in net debt/cash
(2,113) Increase/(decrease) in cash in year 12,355
5,066 Net debt/cash at 1 April 15 2,953
2,953 Net debt/cash at 31 March 15 15,308
Refer to Note 29c Consolidated Group Cashflow

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
61
STATEMENT OF CONSOLIDATED CHANGES IN TAXPAYERS’ EQUITY FOR YEAR ENDED 31 MARCH 2017
Note General
Fund Revaluation
Reserve
Joint
Venture Reserves
Funds held in Trust
Total Reserves
£’000 £’000 £’000 £’000 £’000
Balance at 31 March 2016 222,506 202,425 0
63,357 488,288
Balance at 1 April 2016
222,506 202,425
0 63,357 488,288
Changes in taxpayers' equity for 2016/17
Net gain/(loss) on revaluation/indexation of property, plant and equipment
11 0 (35,737)
0 0 (35,737)
Impairment of property, plant and equipment 11 0 (43) 0
0 (43)
Revaluation & impairments taken to operating costs 0 28,272 0
0 28,272
Transfers between reserves 7,488 (7,488) 0
0 0
Net operating cost for the year (1,683,312) 0 1,845
10,818 (1,670,649)
Total recognised income and expense for 2016/17
(1,675,824) (14,996)
1,845 10,818 (1,678,157)
Funding:
Drawn down CFS
1,618,168 0
0 0 1,618,168
Movement in General Fund (Creditor) / Debtor
(12,164) 0
0 0 (12,164)
Balance at 31 March 2017 BS
152,686 187,429
1,845 74,175 416,135
Balance at 31 March 2015 249,926 201,926 0
70,488 522,340
Balance at 1 April 2015 249,926 201,926 0
70,488 522,340
Changes in taxpayers’ equity for 2015/16
Net gain/(loss) on revaluation/indexation of property, plant and equipment
11 0 20,375
0 0 20,375
Impairment of property, plant and equipment 11
0 (13,574)
0 0 (13,574)
Revaluation & impairments taken to operating costs 3
0 766
0 0 766
Transfers between reserves 7,147 (7,147) 0
0 0
Transfer of non current assets from other bodies (9) 79 0
0 70
Other non current asset transfer 1,087 0 0
0 1,087 Net operating cost for the year
(1,544,766) 0
0 (7,131) (1,551,897)
Total recognised income and expense for 2015/16
(1,536,541) 499
0 (7,131) (1,543,173)
Funding:
Drawn down
1,509,325 0
0 0 1,509,325
Movement in General Fund (Creditor) / Debtor
(204) 0
0 0 (204)
Balance at 31 March 2016 BS
222,506 202,425
0 63,357 488,288
The Notes to the Accounts numbered 1 to 29 form an integral part of these Accounts

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
62
NOTES TO THE ACCOUNTS FOR YEAR ENDED 31 MARCH 2017 NOTE 1 ACCOUNTING POLICIES
1. Authority In accordance with the accounts direction issued by Scottish Ministers under section 19(4) of the Public
Finance and Accountability (Scotland) Act 2000 appended, these Accounts have been prepared in accordance with the Government Financial Reporting Manual (FReM) issued by HM Treasury, which follows International Financial Reporting Standards as adopted by the European Union (IFRS as adopted by the EU), IFRIC Interpretations and the Companies Act 2006 to the extent that they are meaningful and appropriate to the public sector. They have been applied consistently in dealing with items considered material in relation to the accounts. The preparation of financial statements in conformity with IFRS requires the use of certain critical accounting estimates. It also requires management to exercise its judgement in the process of applying the accounting policies. (a) Standards, amendments and interpretations effective in 2016-17 There are no new standards, amendments or interpretations effective for the first time this year that have had a material effect on the financial statements. (b) Standards, amendments and interpretation early adopted this year There are no new standards, amendments or interpretations early adopted in 2016-17. (c) Standards, amendments and interpretations issued in the current year but not yet effective. The following standards, amendments and interpretations were issued in the current year but are not yet effective and have not been applied:
IFRS 9 Financial Instruments. The standard is expected to be applied, through Government Financial Reporting Manual interpretation, in 2018/19. Application of the standard is not expected to have a material effect on the financial statements.
IFRS 15 Revenue from Contracts with Customers. The standard is expected to be applied, through Government Financial Reporting Manual interpretation, in 2018/19. Application of the standard is not expected to have a material effect on the financial statements.
IFRS 16 Leases. The standard is expected to be applied, subject to EU adoption and consultation and through Government Financial Reporting Manual interpretation, in 2019/20. The standard represents a significant change in lessee accounting by largely removing the distinction between operating and finance leases and introducing a single lessee accounting model. The lessor accounting model is significantly unchanged. Application of the standard is subject to ongoing analysis and review by HM Treasury and the other Relevant Authorities. A cross government Technical Working Group has been formed to assist with the assessment. The possible impact on the financial statements from applying this standard cannot yet be reasonably estimated.
2. Basis of Consolidation Consolidation In accordance with IAS 27 – Separate Financial Statements, the Financial Statements consolidate the Lothian Health Board Endowment Fund operating under the name of the Edinburgh & Lothian’s Health Foundation. NHS Endowment Funds were established by the NHS (Scotland) Act 1978. The legal framework under which charities operate in Scotland is the Charities and Trustee Investment (Scotland) Act 2005. Under the 1978 Act Endowment Trustees are also members of the NHS Board. The Board members (who are also Trustees) are appointed by Scottish Ministers.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
63
The Edinburgh & Lothian Health Foundation is a Registered Charity with the Office of the Charity Regulator of Scotland (OSCR) and is required to prepare and submit Audited Financial Statements to OSCR on an annual basis. The basis of consolidation used is Merger Accounting. Any intragroup transactions between the Board and the Endowment Fund have been eliminated on consolidation. Note 29 to the Annual Accounts, details how these consolidated Financial Statements have been calculated. The integration of health and social care services under the terms of the Public Bodies (Joint Working) (Scotland) Act 2014 and associated secondary legislation impacts on Health Board disclosure requirements in the annual accounts. In accordance with IAS 28 – Investments in Associates and Joint Arrangements, the primary financial statements have been amended for the additional disclosure required to accurately reflect the interest of IJBs using the equity method of accounting. IJBs will act as principal in their own right. The Board’s contributions and subsequent expenditure in delivering services are treated as distinct and separate from the commissioning income that will be received. Note 29 to the Annual Accounts, details how these consolidated Financial Statements have been calculated.
3. Going Concern
The accounts are prepared on the going concern basis, which provides that the entity will continue in operational existence for the foreseeable future.
4. Accounting Convention The Accounts are prepared on a historical cost basis, as modified by the revaluation of property, plant and
equipment, intangible assets, inventories, available-for-sale financial assets and financial assets and liabilities (including derivative instruments) at fair value.
5. Funding Most of the expenditure of the Health Board as Commissioner is met from funds advanced by the Scottish
Government within an approved revenue resource limit. Cash drawn down to fund expenditure within this approved revenue resource limit is credited to the general fund.
All other income receivable by the Board that is not classed as funding is recognised in the year in which it is receivable.
Where income is received for a specific activity which is to be delivered in the following financial year, that
income is deferred. Income from the sale of non-current assets is recognised only when all material conditions of sale have
been met, and is measured as the sums due under the sale contract. Non-discretionary funding out with the RRL is allocated to match actual expenditure incurred for the
provision of specific pharmaceutical, dental or ophthalmic services identified by the Scottish Government. Non-discretionary expenditure is disclosed in the accounts and deducted from operating costs charged against the RRL in the Statement of Resource Outturn.
Funding for the acquisition of capital assets received from the Scottish Government is credited to the
general fund when cash is drawn down. Expenditure on goods and services is recognised when, and to the extent that they have been received,
and is measured at the fair value of those goods and services. Expenditure is recognised in the Statement
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
64
of Comprehensive Net Expenditure except where it results in the creation of a non-current asset such as property, plant and equipment.
6. Property, plant and equipment The treatment of capital assets in the accounts (capitalisation, valuation, depreciation, particulars
concerning donated assets) is in accordance with the NHS Capital Accounting Manual. Title to properties included in the accounts is held by Scottish Ministers.
6.1 Recognition Property, Plant and Equipment is capitalised where: it is held for use in delivering services or for administrative purposes; it is probable that future economic benefits will flow to, or service potential be provided to, the Board; it is expected to be used for more than one financial year; and the cost of the item can be measured reliably. All assets falling into the following categories are capitalised:
1) Property, plant and equipment assets which are capable of being used for a period which could exceed one year, and have a cost equal to or greater than £5,000.
2) In cases where a new hospital would face an exceptional write off of items of equipment costing individually less than £5,000, the Board has the option to capitalise initial revenue equipment costs with a standard life of 10 years.
3) Assets of lesser value may be capitalised where they form part of a group of similar assets
purchased at approximately the same time and cost over £20,000 in total, or where they are part of the initial costs of equipping a new development and total over £20,000.
6.2 Measurement Valuation: All property, plant and equipment assets are measured initially at cost, representing the costs directly attributable to acquiring or constructing the asset and bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management. All assets that are not held for their service potential (i.e. investment properties and assets held for sale), including operational assets which are surplus to requirements where there are no restrictions on disposal which would prevent access to the market, are measured subsequently at fair value as follows: Specialised NHS Land, buildings, equipment, installations and fittings are stated at depreciated replacement cost, as a proxy for fair value as specified in the FReM.
Non specialised land and buildings, such as offices, are stated at fair value.
Valuations of all land and building assets are reassessed by valuers under a 5-year programme of professional valuations and adjusted in intervening years to take account of movements in prices since the latest valuation. The valuations are carried out in accordance with the Royal Institution of Chartered Surveyors (RICS) Appraisal and Valuation Manual insofar as these terms are consistent with the agreed requirements of the Scottish Government.
Non specialised equipment, installations and fittings are valued at fair value. Boards value such assets using the most appropriate valuation methodology available (for example, appropriate indices). A depreciated historical cost basis as a proxy for fair value in respect of such assets which have short useful lives or low values (or both).
Assets under construction are held at cost until operational. Thereafer they are valued as above according to the asset categories. These are also subject to impairment review.
To meet the underlying objectives established by the Scottish Government the following accepted variations of the RICS Appraisal and Valuation Manual have been required:

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
65
Specialised operational assets are valued on a modified replacement cost basis to take account of modern substitute building materials and locality factors only.
Operational assets which are in use delivering front line services or back office functions, and surplus assets with restrictions on their disposal, are valued at current value in existing use. Assets have been assessed as surplus where there is no clear plan to bring the asset back into future use as an operational asset.
Subsequent expenditure:
Subsequent expenditure is capitalised into an asset’s carrying value when it is probable the future economic benefits associated with the item will flow to the Board and the cost can be measured reliably. Where subsequent expenditure does not meet these criteria the expenditure is charged to the Statement of Comprehensive Net Expenditure. If part of an asset is replaced, then the part it replaces is de-recognised, regardless of whether or not it has been depreciated separately.
Revaluations and Impairment:
Increases in asset values arising from revaluations are recognised in the revaluation reserve, except where, and to the extent that, they reverse an impairment previously recognised in the Statement of Comprehensive Net Expenditure, in which case they are recognised as income. Movements on revaluation are considered for individual assets rather than groups or land/buildings together.
Permanent decreases in asset values and impairments are charged gross to the Statement of Comprehensive Net Expenditure. Any related balance on the revaluation reserve is transferred to the General Fund. Gains and losses on revaluation are reported in the Statement of Comprehensive Net Expenditure. 6.3 Depreciation Items of Property, Plant and Equipment are depreciated to their estimated residual value over their remaining useful economic lives in a manner consistent with the consumption of economic or service delivery benefits.
Depreciation is charged on each main class of tangible asset as follows:
1) Freehold land is considered to have an infinite life and is not depreciated.
2) Assets in the course of construction and residual interests in off-balance sheet PFI contract assets are not depreciated until the asset is brought into use or reverts to the Board, respectively.
3) Property, Plant and Equipment which has been reclassified as ‘Held for Sale’ ceases to be
depreciated upon the reclassification. 4) Buildings, installations and fittings are depreciated on current value over the estimated
remaining life of the asset, as advised by the appointed valuer. They are assessed in the context of the maximum useful lives for building elements.
5) Equipment is depreciated over the estimated life of the asset. 6) Property, plant and equipment held under finance leases are depreciated over the shorter of
the lease term and the estimated useful life.
Depreciation is charged on a straight line basis. The following asset lives have been used:

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
66
Asset Category/Component Useful Life Building – Structural 5 – 75 years* Building – Engineering and External Plant 15 – 35 years Medical Equipment 3 –15 years Vehicles 7 years Furniture 10 years Office & IT Equipment 5 – 8 years *The useful life of building – structural is based on independent valuers recommendations.
7. Intangible Assets
7.1 Recognition Intangible assets are non-monetary assets without physical substance which are capable of being sold
separately from the rest of the Board’s business or which arise from contractual or other legal rights. They are recognised only where it is probable that future economic benefits will flow to, or service potential be provided to, the Board and where the cost of the asset can be measured reliably.
Intangible assets that meet the recognition criteria are capitalised when they are capable of being used in a Board’s activities for more than one year and they have a cost of at least £5,000.
The main classes of intangible assets recognised are:
Internally generated intangible assets: Internally generated goodwill, brands, mastheads, publishing titles, customer lists and similar items are not
capitalised as intangible assets. Expenditure on research is not capitalised. Expenditure on development is capitalised only where all of the following can be demonstrated:
the project is technically feasible to the point of completion and will result in an intangible asset for sale or use;
the Board intends to complete the asset and sell or use it;
the Board has the ability to sell or use the asset;
how the intangible asset will generate probable future economic or service delivery benefits e.g. the presence of a market for it or its output, or where it is to be used for internal use, the usefulness of the asset;
adequate financial, technical and other resources are available to the Board to complete the development and sell or use the asset; and
the Board can measure reliably the expenses attributable to the asset during development. Expenditure so deferred is limited to the value of future benefits.
Software:
Software which is integral to the operation of hardware e.g. an operating system, is capitalised as part of the relevant item of property, plant and equipment. Software which is not integral to
the operation of hardware e.g. application software, is capitalised as an intangible asset. Software licences:
Purchased computer software licences are capitalised as intangible assets where expenditure of at least £5,000 is incurred.
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
67
Carbon Emissions (Intangible Assets): A cap and trade scheme gives rise to an asset for allowances held and a liability for the obligation to deliver allowances equal to emissions that have been made. Intangible Assets, such as EU Greenhouse Gas Emission Allowances intended to be held for use on a continuing basis whether allocated by government or purchased are classified as intangible assets. Allowances that are issued for less than their fair value are measured initially at their fair value. When allowances are issued for less than their fair value, the difference between the amount paid and fair value is revaluation and charged to the general fund. The general fund is charged with the same proportion of the amount of the revaluation, which the amount of the grant bears to the acquisition cost of the asset. A provision is recognised for the obligation to deliver allowances equal to emissions that have been made. It is measured at the best estimate of the expenditure required to settle the present obligation at the balance sheet date. This will usually be the present market price of the number of allowances required to cover emissions made up to the balance sheet date. Websites: Websites are capitalised only when it is probable that future economic benefits will flow to, or service potential be provided to, the Board; where the cost of the asset can be measured reliably, and where the cost is at least £5,000.
7.2 Measurement
Valuation
Intangible assets are recognised initially at cost, comprising all directly attributable costs needed to create, produce and prepare the asset to the point that it is capable of operating in the manner intended by management.
Subsequently intangible assets that are not held for their service potential (i.e. assets held for sale),
including operational assets which are surplus to requirements where there are no restrictions on disposal which would prevent access to the market, are measured at fair value. Where an active (homogeneous) market exists, intangible assets are carried at fair value. Where no active market exists, the intangible asset is revalued, using indices or some suitable model, to the lower of depreciated replacement cost and value in use where the asset is income generating. Where there is no value in use, the intangible asset is valued using depreciated replacement cost. These measures are a proxy for fair value.
Revaluation and impairment
Increases in asset values arising from revaluations are recognised in the revaluation reserve, except where, and to the extent that, they reverse an impairment previously recognised in the Statement of Comprehensive Net Expenditure, in which case they are recognised in income.
Permanent decreases in asset values and impairments are charged gross to the Statement of
Comprehensive Net Expenditure. Any related balance on the revaluation reserve is transferred to the General Fund.
Temporary decreases in asset values or impairments are charged to the revaluation reserve to the extent
that there is an available balance for the asset concerned, and thereafter are charged to the Statement of Comprehensive Net Expenditure.
Intangible assets held for sale are reclassified to ‘non-current assets held for sale’ measured at the lower
of their carrying amount or ‘fair value less costs to sell’. Operational assets which are in use delivering front line services or back office functions, and surplus
assets with restrictions on their disposal, are valued at current value in existing use. Assets have been assessed as surplus where there is no clear plan to bring the asset back into future use as an operational asset.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
68
7.3 Amortisation
Intangible assets are amortised to their estimated residual value over their remaining useful economic lives in a manner consistent with the consumption of economic or service delivery benefits.
Amortisation is charged to the Statement of Comprehensive Net Expenditure on each main class of intangible asset as follows:
1) Internally generated intangible assets. Amortised on a systematic basis over the period
expected to benefit from the project. 2) Software. Amortised over their expected useful life. 3) Software licences. Amortised over the shorter term of the licence and their useful economic
lives.
4) Other intangible assets. Amortised over their expected useful life. 5) Intangible assets which has been reclassified as ‘Held for Sale’ ceases to be amortised upon
the reclassification.
Amortisation is charged on a straight line basis. The following asset lives have been used: Asset Category/Component Useful Life Application Software 4 years
8. Non-current assets held for sale
Non-current assets intended for disposal are reclassified as ‘Held for Sale’ once all of the following criteria are met:
the asset is available for immediate sale in its present condition subject only to terms which are usual and customary for such sales;
the sale must be highly probable i.e.:
management are committed to a plan to sell the asset; an active programme has begun to find a buyer and complete the sale; the asset is being actively marketed at a reasonable price; the sale is expected to be completed within 12 months of the date of classification as ‘Held for
Sale’; and the actions needed to complete the plan indicate it is unlikely that the plan will be dropped or
significant changes made to it.
Following reclassification, the assets are measured at the lower of their existing carrying amount and their ‘fair value less costs to sell’. Depreciation ceases to be charged and the assets are not revalued, except where the ‘fair value less costs to sell’ falls below the carrying amount. Assets are de-recognised when all material sale contract conditions have been met. Property, plant and equipment which is to be scrapped or demolished does not qualify for recognition as ‘Held for Sale’ and instead is retained as an operational asset and the asset’s economic life is adjusted. The asset is de-recognised when scrapping or demolition occurs.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
69
9. Donated Assets
Non-current assets that are donated or purchased using donated funds are included in the Balance Sheet initially at the current full replacement cost of the asset. The accounting treatment, including the method of valuation, follows the rules in the NHS Capital Accounting Manual.
10. Sale of Property, plant and equipment, intangible assets and non-current assets held for sale Disposal of non-current assets is accounted for as a reduction to the value of assets equal to the net book
value of the assets disposed. When set against any sales proceeds, the resulting gain or loss on disposal will be recorded in the Statement of Comprehensive Net Expenditure. Non-current assets held for sale will include assets transferred from other categories and will reflect any resultant changes in valuation.
11. Leasing Finance leases Where substantially all risks and rewards of ownership of a leased asset are borne by the Board, the asset
is recorded as Property, Plant and Equipment and a corresponding liability is recorded. Assets held under finance leases are valued at their fair values and are depreciated over the remaining period of the lease in accordance with IFRS.
The asset and liability are recognised at the inception of the lease, and are de-recognised when the liability
is discharged, cancelled or expires. The minimum lease payments (annual rental less operating costs e.g. maintenance and contingent rental) are apportioned between the repayment of the outstanding liability and a finance charge. The annual finance charge is allocated to each period during the lease term so as to produce a constant periodic rate of interest on the remaining balance of the liability using either the implicit interest rate or another relevant basis of estimation such as the sum of the digits method. Finance charges are recorded as interest payable in the Statement of Comprehensive Net Expenditure. Contingent rental and operating costs are charged as expenses in the periods in which they are incurred.
Operating leases Other leases are regarded as operating leases and the rentals are charged to expenditure on a straight-
line basis over the term of the lease. Operating lease incentives received are added to the lease rentals and charged to expenditure over the life of the lease.
Leases of land and buildings Where a lease is for land and buildings, the land component is separated from the building component and
the classification for each is assessed separately. Leased land is treated as an operating lease unless title to the land is expected to transfer.
12. Impairment of non-financial assets
Assets that are subject to depreciation and amortisation are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount may not be recoverable. An impairment loss is recognised for the amount by which the asset’s carrying amount exceeds its recoverable amount. The recoverable amount is the higher of an asset’s fair value less costs to sell and value in use. Where an asset is not held for the purpose of generating cash flows, value in use is assumed to equal the cost of replacing the service potential provided by the asset, unless there has been a reduction in service potential. For the purposes of assessing impairment, assets are grouped at the lowest levels for which there are separately identifiable cash flows (cash-generating units). Non-financial assets that suffer an impairment are reviewed for possible reversal of the impairment. Impairment losses charged to the Statement Of Comprehensive Net Expenditure are deducted from future operating costs to the extent that they are identified as being reversed in subsequent revaluations.
13. General Fund Receivables and Payables
Where the Health Board has a positive net cash book balance at the year end, a corresponding creditor is created and the general fund debited with the same amount to indicate that this cash is repayable to the SGHSCD. Where the Health Board has a net overdrawn cash position at the year end, a corresponding

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
70
debtor is created and the general fund credited with the same amount to indicate that additional cash is to be drawn down from the SGHSCD.
14. Inventories Inventories are valued at the lower of cost and net realisable value. Taking into account the high turnover
of NHS inventories, the use of average purchase price is deemed to represent current cost. Work in progress is valued at the cost of the direct materials plus the conversion costs and other costs incurred to bring the goods up to their present location, condition and degree of completion.
15. Losses and Special Payments Operating expenditure includes certain losses which would have been made good through insurance cover
had the NHS not been bearing its own risks. Had the NHS provided insurance cover, the insurance premiums would have been included as normal revenue expenditure.
16. Employee Benefits Short-term Employee Benefits
Salaries, wages and employment-related payments are recognised in the year in which the service is received from employees. The cost of annual leave and flexible working time entitlement earned but not taken by employees at the end of the year is recognised in the financial statements to the extent that employees are permitted to carry-forward leave into the following year. Pension Costs
The Board participates in NHS Superannuation Schemes for Scotland providing pension benefits. Contributions are credited to the Exchequer and are deemed to be invested in a portfolio of Government Securities. The Board is unable to identify its share of the underlying notional assets and liabilities of the scheme on a consistent and reasonable basis and therefore accounts for the scheme as if it were a defined contribution scheme, as required by IAS 19 ‘Employee Benefits’. As a result, the amount charged to the Statement of Comprehensive Net Expenditure represents the Board’s employer contributions payable to the scheme in respect of the year. The contributions deducted from employees are reflected in the gross salaries charged and are similarly remitted to Exchequer. The pension cost is assessed every four years by the Government Actuary and determines the rate of contributions required. The most recent actuarial valuation is published by the Scottish Public Pensions Agency and is available on their website.
Additional pension liabilities arising from early retirements are not funded by the scheme except where the
retirement is due to ill-health. The full amount of the liability for the additional costs is charged to the Statement of Comprehensive Net Expenditure at the time the Board commits itself to the retirement, regardless of the method of payment.
17. Clinical and Medical Negligence Costs Employing health bodies in Scotland are responsible for meeting medical negligence costs up to a
threshold per claim. Costs above this threshold are reimbursed to Boards from a central fund held as part of the Clinical Negligence and Other Risks Indemnity Scheme (CNORIS) by the Scottish Government.
NHS Lothian provide for all claims notified to the NHS Central Legal Office according to the value of the claim and the probability of settlement. Claims assessed as ‘Category 3’ are deemed most likely and provided for in full, those in ‘Category 2’ as 50% of the claim and those in ‘category 1’ as nil. The balance of the value of claims not provided for is disclosed as a contingent liability. This procedure is intended to estimate the amount considered to be the liability in respect of any claims outstanding and which will be recoverable from the Clinical Negligence and Other Risks Indemnity Scheme in the event of payment by an individual health body. The corresponding recovery in respect of amounts provided for is recorded as a debtor and that in respect of amounts disclosed as contingent liabilities are disclosed as contingent assets. NHS Lothian also provides for its liability from participating in the scheme. The Participation in CNORIS provision recognises the Board’s respective share of the total liability of NHS Scotland as advised by the Scottish Government and based on information prepared by NHS Boards and the Central Legal Office.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
71
The movement in the provisions between financial years is matched by a corresponding adjustment in AME provision and is classified as non-core expenditure.
18. Related Party Transactions Material related party transactions are disclosed in the note 27 in line with the requirements of IAS 24.
Transactions with other NHS bodies for the commissioning of health care are summarised in Note 4.
19. Value Added Tax
Most of the activities of the Board are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of non-current assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
20. PFI/HUB/NPD Schemes
Transactions financed as revenue transactions through the Private Finance Initiative or alternative initiatives such as HUB or the Non Profit Distributing Model (NPD) are accounted for in accordance with the HM Treasury application of IFRIC 12, Service Concession Arrangements, outlined in the FReM.
Transactions which meet the IFRIC 12 definition of a service concession, as interpreted in HM Treasury’s FReM, are accounted for as ‘on-balance sheet’ by the Board. The underlying assets are recognised as Property, Plant and Equipment and Intangible Assets at their fair value. An equivalent liability is recognised in accordance with IAS 17. Where it is not possible to separate the finance element from the service element of unitary payment streams this has been estimated from information provided by the operator and the fair values of the underlying assets. Assets are subsequently revalued in accordance with the treatment specified for their applicable asset categories.
The annual contract payments are apportioned between the repayment of the liability, a finance cost and the charges for services. The finance cost is calculated using the implicit interest rate for the scheme.
The service charge and the finance cost interest element are charged in the Statement of Comprehensive Net Expenditure.
21. Provisions The Board provides for legal or constructive obligations that are of uncertain timing or amount at the
balance sheet date on the basis of the best estimate of the expenditure required to settle the obligation. Where the effect of the time value of money is significant, the estimated cash flows are discounted using the discount rate prescribed by HM Treasury.
22. Contingencies Contingent assets (that is, assets arising from past events whose existence will only be confirmed by one
or more future events not wholly within the Board’s control) are not recognised as assets, but are disclosed in note 19 where an inflow of economic benefits is probable.
Contingent liabilities are not recognised, but are disclosed in note 19, unless the probability of a transfer of economic benefits is remote. Contingent liabilities are defined as:
possible obligations arising from past events whose existence will be confirmed only by the occurrence of one or more uncertain future events not wholly within the entity’s control; or
present obligations arising from past events but for which it is not probable that a transfer of economic benefits will arise or for which the amount of the obligation cannot be measured with sufficient reliability.
23. Corresponding Amounts
Corresponding amounts are shown for the primary statements and notes to the financial statements.
Where the corresponding amounts are not directly comparable with the amount to be shown in respect of

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
72
the current financial year, IAS 1 ‘Presentation of Financial Statements’, requires that they should be
adjusted and the basis for adjustment disclosed in a note to the financial statements. 24. Financial Instruments
Financial assets Classification The Board classifies its financial assets in the following categories: at fair value through profit or loss, loans and receivables, and available for sale. The classification depends on the purpose for which the financial assets were acquired. Management determines the classification of its financial assets at initial recognition. (a) Financial assets at fair value through profit or loss Financial assets at fair value through profit or loss comprise derivatives. Assets in this category are classified as current assets. The Board does not trade in derivatives and does not apply hedge accounting. (b) Loans and receivables Loans and receivables are non-derivative financial assets with fixed or determinable payments that are not quoted in an active market. They are included in current assets, except for maturities greater than 12 months after the balance sheet date. These are classified as non-current assets. Loans and receivables comprise trade and other receivables and cash at bank and in hand in the balance sheet. (c) Available-for-sale financial assets Available-for-sale financial assets are non-derivatives that are either designated in this category or not classified in any of the other categories. They are included in non-current assets unless management intends to dispose of the investment within 12 months of the balance sheet date. Available for sale financial assets comprise investments.
Recognition and measurement Financial assets are recognised when the Board becomes party to the contractual provisions of the financial instrument. Financial assets are derecognised when the rights to receive cash flows from the asset have expired or have been transferred and the Board has transferred substantially all risks and rewards of ownership. (a) Financial assets at fair value through profit or loss Financial assets carried at fair value through profit or loss are initially recognised at fair value, and transaction costs are expensed in the Statement of Comprehensive Net Expenditure. Financial assets carried at fair value through profit or loss are subsequently measured at fair value. Gains or losses arising from changes in the fair value are presented in the Statement of Comprehensive Net Expenditure. (b) Loans and receivables Loans and receivables are recognised initially at fair value and subsequently measured at amortised cost using the effective interest method, less provision for impairment. A provision for impairment of loans and receivables is established when there is objective evidence that the Board will not be able to collect all amounts due according to the original terms of the receivables. Significant financial difficulties of the debtor, probability that the debtor will enter bankruptcy or financial reorganisation, and default or delinquency in payments (more than 30 days overdue) are considered indicators that the loan and receivable is impaired. The amount of the provision is the difference between the asset’s carrying amount and the present value of estimated future cash flows, discounted at the original effective interest rate. The carrying amount of the asset is reduced through the use of an allowance account, and the amount of the loss is recognised in the Statement of Comprehensive Net Expenditure. When a loan or receivable is
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
73
uncollectible, it is written off against the allowance account. Subsequent recoveries of amounts previously written off are credited in the Statement of Comprehensive Net Expenditure. (c) Available-for-sale financial assets Available-for-sale financial assets are initially recognised and subsequently carried at fair value. Changes in the fair value of financial assets classified as available for sale are recognised in equity in other reserves. When financial assets classified as available for sale are sold or impaired, the accumulated fair value adjustments recognised in equity are included in the Statement of Comprehensive Net Expenditure. Dividends on available-for-sale equity instruments are recognised in the Statement of Comprehensive Net Expenditure when the Board’s right to receive payments is established. Investments in equity instruments that do not have a quoted market price in an active market and whose fair value cannot be reliably measured are measured at cost less impairment. The Board assesses at each balance sheet date whether there is objective evidence that a financial asset or a group of financial assets is impaired. In the case of equity securities classified as available for sale, a significant or prolonged decline in the fair value of the security below its cost is considered as an indicator that the securities are impaired. If any such evidence exists for available-for-sale financial assets, the cumulative loss – measured as the difference between the acquisition cost and the current fair value, less any impairment loss on that financial asset previously recognised in profit or loss – is removed from equity and recognised in the Statement of Comprehensive Net Expenditure. Impairment losses recognised in the Statement of Comprehensive Net Expenditure on equity instruments are not reversed through the income statement.
Financial Liabilities Classification The Board classifies its financial liabilities in the following categories: at fair value through profit or loss, and other financial liabilities. The classification depends on the purpose for which the financial liabilities were issued. Management determines the classification of its financial liabilities at initial recognition. (a) Financial liabilities at fair value through profit or loss Financial liabilities at fair value through profit or loss comprise derivatives. Liabilities in this category are classified as current liabilities. The NHS Board does not trade in derivatives and does not apply hedge accounting. (b) Other financial liabilities Other financial liabilities are included in current liabilities, except for maturities greater than 12 months after the balance sheet date. These are classified as non-current liabilities. The NHS Board’s other financial liabilities comprise trade and other payables in the balance sheet. Recognition and measurement Financial liabilities are recognised when the NHS Board Scotland becomes party to the contractual provisions of the financial instrument. A financial liability is removed from the balance sheet when it is extinguished, that is when the obligation is discharged, cancelled or expired. (a) Financial liabilities at fair value through profit or loss Financial liabilities carried at fair value through profit or loss are initially recognised at fair value, and transaction costs are expensed in the income statement. Financial liabilities carried at fair value through profit or loss are subsequently measured at fair value. Gains or losses arising from changes in the fair value are presented in the Statement of Comprehensive Net Expenditure. (b) Other financial liabilities

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
74
Other financial liabilities are recognised initially at fair value and subsequently measured at amortised cost using the effective interest method.
25. Segmental reporting
Operating segments are reported in a manner consistent with the internal reporting provided to the chief operating decision-maker, who is responsible for allocating resources and assessing performance of the operating segments. Operating segments do not relate to the analysis of expenditure shown in notes 4 to 7 for Hospital & Community, Family Health and Other Service and Administration Costs, the basis of which relates to Scottish Government funding streams and the classification of which varies depending on Scottish Government reporting requirements. The segmental information for NHS Lothian is detailed in Note 28.
26. Cash and cash equivalents Cash and cash equivalents includes cash in hand, deposits held at call with banks, cash balances held
with the Government Banking Service, balances held in commercial banks and other short-term highly liquid investments with original maturities of three months or less, and bank overdrafts. Bank overdrafts are shown within borrowings in current liabilities on the balance sheet. Where the Government Banking Service is using Citi and Royal Bank of Scotland Group to provide the banking services, funds held in these accounts should not be classed as commercial bank balances.
The NHS Lothian Accounts include the consolidation of The Edinburgh & Lothian Health Foundation
(ELHF). The Foundation investments are categorised as level 1 in accordance with IFRS 13 and are denominated in pounds sterling.
27. Foreign exchange The functional and presentational currencies of the Board are sterling. A transaction which is denominated in a foreign currency is translated into the functional currency at the
spot exchange rate on the date of the transaction. Where the Board has assets or liabilities denominated in a foreign currency at the balance sheet date:
monetary items (other than financial instruments measured at ‘fair value through income and expenditure’) are translated at the spot exchange rate on 31 March;
non-monetary assets and liabilities measured at historical cost are translated using the spot exchange rate at the date of the transaction; and
non-monetary assets and liabilities measured at fair value are translated using the spot exchange rate at the date the fair value was determined.
Exchange gains or losses on monetary items (arising on settlement of the transaction or on re-translation at the balance sheet date) are recognised in income or expenditure in the period in which they arise.
Exchange gains or losses on non-monetary assets and liabilities are recognised in the same manner as
other gains and losses on these items. 28. Key sources of judgement and estimation uncertainty
Estimates and judgements are continually evaluated and are based on historical experience and other factors, including expectations of future events that are believed to be reasonable under the circumstances. The Board makes estimates and assumptions concerning the future. The resulting accounting estimates will, by definition, seldom equal the related actual results. The Board makes judgements in applying accounting policies.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
75
2. STAFF COSTS
Total staff costs for the year to 31 March 2017 were £941.5m (2016: £901.4m). Further detail and analysis of staff costs can be found in the Remuneration and Staff Report, forming part of the Accountability Report.
3. OTHER OPERATING COSTS
2015-16
£’000 Expenditure Not Paid In Cash Note £’000
34,457 Depreciation on Purchased Assets 11a 34,812
1,797 Amortisation 10 1,000
750 Depreciation on Donated Assets 11b 758
0 Impairments on PPE charged to SOCNE 11a 43
3,225 Net revaluation on PPE charged to SOCNE 11a 28,229
(2,459) Reversal of impairments on PPE charged to SOCNE 11a 0
(126) Loss/(Profit) on disposal of property, plant and equipment 312
(1,023) Funding of Donated assets (2,501)
1,078 Transfer of assets 0
0 IJB joint venture share 29a (1,845)
151 Other non cash 24
37,850 Total Expenditure Not Paid In Cash 60,832
Interest Payable
28,508 PFI Finance Lease charges allocated in year 23 28,438
24 Unwinding of Discount (8,205)
28,532 Total 20,233
Statutory Audit
388 External auditor's remuneration and expenses 297
4. HOSPITAL AND COMMUNITY HEALTH SERVICES
2015-16
£’000 BY PROVIDER £’000
1,334,497 Treatment in Board area of NHS Scotland Patients 1,437,904
9,135 Other NHS Scotland Bodies 9,583
1,863 Health Bodies outside Scotland 1,274
12,192 Private sector 9,578
Community Care
46,871 Resource Transfer 73,599
0 Contribution of Health Board to Integration Joint Board 868,663
15,975 Payments made to Voluntary Bodies and Charities 14,464
1,420,533 Total NHS Scotland Patients 2,415,065
3,538 Treatment of UK residents based outside Scotland 3,393
1,424,071 Total Hospital & Community Health Service SOCNE 2,418,458

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
76
5. FAMILY HEALTH SERVICE EXPENDITURE
2015-16 Unified Budget
Non Disc TOTAL
£’000 £’000 £’000 £’000
124,762 Primary Medical Services 128,695 0 128,695
174,718 Pharmaceutical Services 157,178 24,469 181,647
62,323 General Dental Services 6,187 58,268 64,455
15,478 General Ophthalmic Services 407 15,915 16,322
377,281 Total SOCNE 292,467 98,652 391,119
6. ADMINISTRATION COSTS
2015-16
£’000 Note £’000
1,108 Board members' remuneration Note 2 (a) 1,232
448 Administration of Board Meetings and Committees 382
751 Corporate Governance and Statutory Reporting 684
5,013 Health Planning, Commissioning and Performance Reporting 3,196
424 Treasury Management and Financial Planning 477
628 Public Relations 543
642 Other 524
9,014 Total administration costs SOCNE 7,038
7. OTHER NON CLINICAL SERVICES
2015-16
£’000 Note £’000
65 Nurse Teaching 61
14,957 Compensation payments – Clinical 58,436
980 Compensation payments - Other 1,694
1,608 Pension enhancement & redundancy 3,704
126 Patients' Travel Attending Hospitals 160
1,796 Health Promotion 1,660
4,295 Public Health 5,125
182 Public Health Medicine Trainees 196
70 Emergency Planning 113
440 Shared Services 448
0 Profit on disposal of non-current assets 312
9,048 Endowment expenditure 3,483
9,566 Other 12,421
43,133 Total Other Non Clinical Services SOCNE 87,813

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
77
8. OPERATING INCOME
2015-16
£’000 HCH Income Note £’000
NHSScotland Bodies
1,382 SGHSCD 1,102
228,126 Boards 229,593
5,758 NHS Non-Scottish Bodies 4,754
Non NHS
2,571 Private Patients 2,590
3,153 Compensation Income 1,874 14,481
0 Other HCH Income Income for services commissioned by Integration Joint Board
14,037 868,663
255,471 Total HCH Income SOCNE 1,122,613
FHS Income
344 Unified 1,216
Non Discretionary
11,592 General Dental Services 11,871
7 General Ophthalmic Services 8
11,943 Total FHS Income SOCNE 13,095
Other Operating Income
14,405 Contributions in respect of Clinical/medical negligence claims 59,296
126 Profit on disposal of non current assets 0
1,023 Donated Asset Additions 2,501
586 Shared Services 616
1,618 Endowment income 14,002
16,430 Other 19,811
34,188 Total Other Operating Income SOCNE 96,226
301,602 Total Income 1,231,934
Restated
228,126 Of the above, the amount derived from NHS bodies is 229,593

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
78
9. CAPITAL EXPENDITURE
2015-16
£’000 EXPENDITURE Note £’000
1,491 Acquisition of Intangible Assets 10 6
107,789 Acquisition of Property, plant and equipment 11a 138,356
951 Donated Asset Additions 11b 2,477
290 Hub enabling expenditure 555
110,521 Gross Capital Expenditure 141,394
INCOME
8 Net book value of disposal of Property, plant and equipment 11a 1,907
0 Net book value of disposal of Donated Assets 11b 24
1,615 Value of disposal of Non-Current Assets held for sale 11c 0
1,023 Donated Asset Capital income 8 2,501
2,646 Capital Income 4,432
107,875 Net Capital Expenditure 136,962
SUMMARY OF CAPITAL RESOURCE OUTTURN
The summary outturn against core and non-core allocations of capital expenditure was as follows: Core
Non Core Total
107,875 Net capital expenditure as above 96,480 40,482 136,962
107,875 Capital Resource Limit 96,480 40,482 136,962
0 Saving/(excess) against Capital Resource Limit 0 0 0

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
79
10. INTANGIBLE ASSETS – BOARD AND CONSOLIDATED
Software Licences
Total
Note £’000 £’000 Cost or Valuation: As at 1 April 2016 20,623 20,623 Additions 9 6 6 Disposals (666) (666)
As at 31 March 2017 19,963 19,963
Amortisation As at 1 April 2016 18,761 18,761 Provided during the year 3 1,000 1,000 Disposals (666) (666)
At 31 March 2017 19,095 19,095
Net Book Value at 1 April 2016 1,862 1,862
Net Book Value at 31 March 2017 B S 868 868
PRIOR YEAR – CONSOLIDATED
Software Licences Total
Note £’000 £’000 Cost or Valuation: As at 1 April 2015 19,132 19,132 Additions 9 1,491 1,491
As at 31 March 2016 20,623 20,623
Amortisation As at 1 April 2015 16,964 16,964 Provided during the year 3 1,797 1,797
At 31 March 2016 18,761 18,761
Net Book Value at 31 March 2015 2,168 2,168
Net Book Value at 31 March 2016 B S 1,862 1,862

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
80
11(a) PROPERTY, PLANT AND EQUIPMENT (Purchased Assets) – BOARD AND CONSOLIDATED
Note
Land (including
under buildings)
Buildings (excluding dwellings) Dwellings
Transport Equipment
Plant & Machinery
Information Technology
Furniture & Fittings
Assets Under
Construction Total £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 Cost or valuation At 1 April 2016 59,841 665,802 1,912 361 134,029 27,551 2,257 141,827 1,033,580 Additions 9 536 0 0 0 15,965 1,212 0 120,643 138,356 Completions 0 53,196 0 0 410 0 0 (53,606) 0 Transfers 4,645 (4,645) 0 0 0 0 0 0 0 Revaluation (6,148) (54,173) 40 0 0 0 0 0 (60,281) Impairment Charge 0 0 0 0 (48) 0 0 0 (48) Disposals 9 (315) 0 (892) (75) (19,709) (541) 0 0 (21,532)
At 31 March 2017 58,559 660,180 1,060 286 130,647 28,222 2,257 208,864 1,090,075
Depreciation At 1 April 2016 0 40,308 57 361 90,745 22,853 1,636 0 155,960 Provided during the year 3 0 21,914 76 0 10,514 2,181 127 0 34,812 Revaluation 0 (31,044) (26) 0 0 0 0 0 (31,070) Impairment Charge 0 0 0 0 (5) 0 0 0 (5) Disposals 9 0 0 (43) (75) (18,966) (541) 0 0 (19,625)
At 31 March 2017 0 31,178 64 286 82,288 24,493 1,763 0 140,072
Net book value at 1 April 2016 59,841 625,494 1,855 0 43,284 4,698 621 141,827 877,620
Net book value at 31 March 2017 11d 58,559 629,002 996 0 48,359 3,729 494 208,864 950,003
Open Market Value of Land, buildings and Dwellings Included Above
11d 8,500 0 0
Asset financing: Owned 58,559 377,434 996 0 48,357 3,729 494 208,864 698,433 Finance leased 0 4,580 0 0 2 0 0 0 4,582 On-balance sheet PFI contracts 0 246,988 0 0 0 0 0 0 246,988
Net Book Value at 31 March 2017 11d 58,559 629,002 996 0 48,359 3,729 494 208,864 950,003
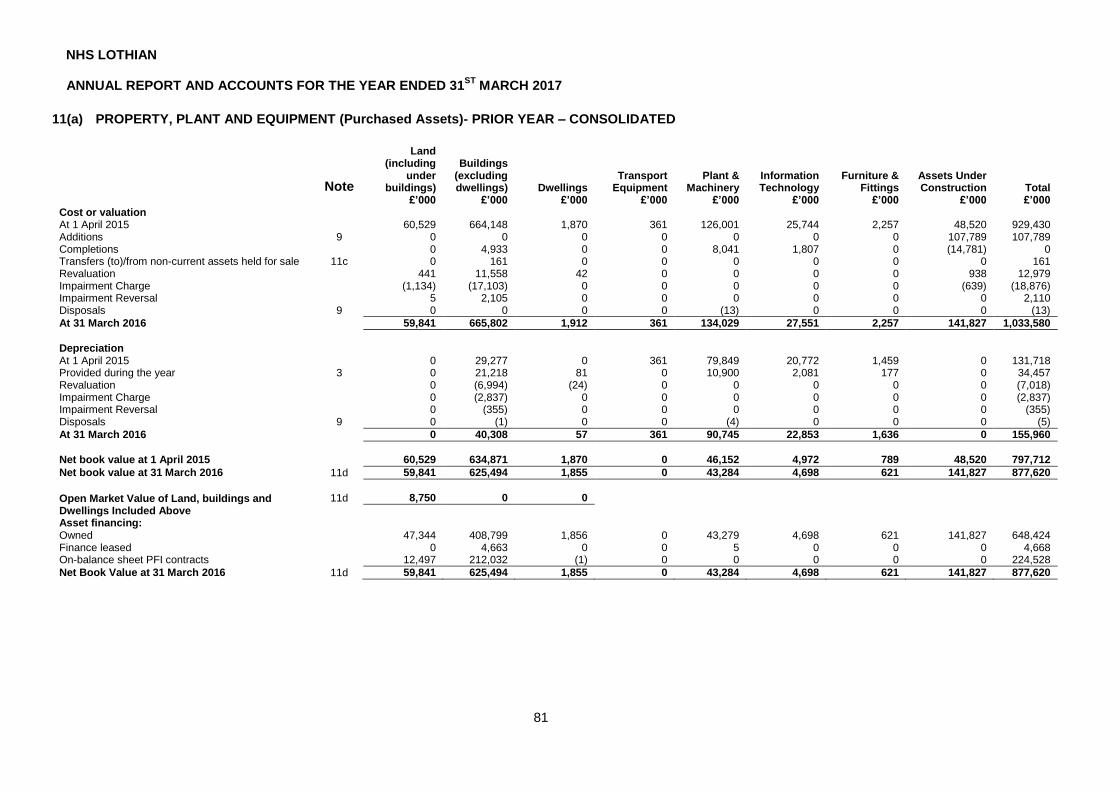
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
81
11(a) PROPERTY, PLANT AND EQUIPMENT (Purchased Assets)- PRIOR YEAR – CONSOLIDATED
Note
Land (including
under buildings)
Buildings (excluding dwellings) Dwellings
Transport Equipment
Plant & Machinery
Information Technology
Furniture & Fittings
Assets Under Construction Total
£’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 Cost or valuation At 1 April 2015 60,529 664,148 1,870 361 126,001 25,744 2,257 48,520 929,430 Additions 9 0 0 0 0 0 0 0 107,789 107,789 Completions 0 4,933 0 0 8,041 1,807 0 (14,781) 0 Transfers (to)/from non-current assets held for sale 11c 0 161 0 0 0 0 0 0 161 Revaluation 441 11,558 42 0 0 0 0 938 12,979 Impairment Charge (1,134) (17,103) 0 0 0 0 0 (639) (18,876) Impairment Reversal 5 2,105 0 0 0 0 0 0 2,110 Disposals 9 0 0 0 0 (13) 0 0 0 (13)
At 31 March 2016 59,841 665,802 1,912 361 134,029 27,551 2,257 141,827 1,033,580
Depreciation At 1 April 2015 0 29,277 0 361 79,849 20,772 1,459 0 131,718 Provided during the year 3 0 21,218 81 0 10,900 2,081 177 0 34,457 Revaluation 0 (6,994) (24) 0 0 0 0 0 (7,018) Impairment Charge 0 (2,837) 0 0 0 0 0 0 (2,837) Impairment Reversal 0 (355) 0 0 0 0 0 0 (355) Disposals 9 0 (1) 0 0 (4) 0 0 0 (5)
At 31 March 2016 0 40,308 57 361 90,745 22,853 1,636 0 155,960
Net book value at 1 April 2015 60,529 634,871 1,870 0 46,152 4,972 789 48,520 797,712
Net book value at 31 March 2016 11d 59,841 625,494 1,855 0 43,284 4,698 621 141,827 877,620
Open Market Value of Land, buildings and Dwellings Included Above
11d 8,750 0 0
Asset financing: Owned 47,344 408,799 1,856 0 43,279 4,698 621 141,827 648,424 Finance leased 0 4,663 0 0 5 0 0 0 4,668 On-balance sheet PFI contracts 12,497 212,032 (1) 0 0 0 0 0 224,528
Net Book Value at 31 March 2016 11d 59,841 625,494 1,855 0 43,284 4,698 621 141,827 877,620

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
82
11(b) PROPERTY, PLANT AND EQUIPMENT (Donated Assets) – CONSOLIDATED
Note
Land (land holdings and land
underlying buildings)
Buildings (excluding dwellings) Dwellings
Transport Equipment
Plant & Machinery
Information Technology
Furniture & Fittings
Assets Under Construction Total
£’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 Cost or valuation At 1 April 2016 45 12,998 0 146 4,103 5 0 657 17,954 Additions 9 0 0 0 0 244 0 0 2,233 2,477 Completions 0 135 0 0 0 0 0 (135) 0 Revaluation (45) (7,701) 0 0 0 0 0 0 (7,746) Disposals 0 0 0 (30) (1,015) 0 0 0 (1,045)
At 31 March 2017 0 5,432 0 116 3,332 5 0 2,755 11,640
Depreciation At 1 April 2016 0 1,160 0 82 2,863 4 0 0 4,109 Provided during the year 0 421 0 10 326 1 0 0 758 Revaluation 0 (1,220) 0 0 0 0 0 0 (1,220) Disposals 0 0 0 (30) (991) 0 0 0 (1,021)
At 31 March 2017 0 361 0 62 2,198 5 0 0 2,626
Net book value at 1 April 2016 45 11,838 0 64 1,240 1 0 657 13,845
Net book value at 31 March 2017 11d 0 5,071 0 54 1,134 0 0 2,755 9,014
Open Market Value of Land in Land and Dwellings Included Above
0 0
Asset financing: Owned 0 5,071 0 54 1,134 0 0 2,755 9,014
Net Book Value at 31 March 2017 11d 0 5,071 0 54 1,134 0 0 2,755 9,014

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
83
11(b) PROPERTY, PLANT AND EQUIPMENT (Donated Assets)- PRIOR YEAR – CONSOLIDATED
Note
Land (land holdings and land
underlying buildings)
Buildings (excluding dwellings) Dwellings
Transport Equipment
Plant & Machinery
Information Technology
Furniture & Fittings
Assets Under Construction Total
£’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 Cost or valuation At 1 April 2015 45 12,398 0 75 3,796 5 0 294 16,613 Additions 9 0 0 0 0 0 0 0 951 951 Completions 0 210 0 71 307 0 0 (588) 0 Revaluation 0 390 0 0 0 0 0 0 390
At 31 March 2016 45 12,998 0 146 4,103 5 0 657 17,954
Depreciation At 1 April 2015 0 737 0 75 2,532 3 0 0 3,347 Provided during the year 0 411 0 7 331 1 0 0 750 Revaluation 0 12 0 0 0 0 0 0 12
At 31 March 2016 0 1,160 0 82 2,863 4 0 0 4,109
Net book value at 1 April 2015 45 11,661 0 0 1,264 2 0 294 13,266
Net book value at 31 March 2016 11d 45 11,838 0 64 1,240 1 0 657 13,845
Open Market Value of Land in Land and Dwellings Included Above
0 0
Asset financing: Owned 45 11,838 0 64 1,240 1 0 657 13,845
Net Book Value at 31 March 2016 11d 45 11,838 0 64 1,240 1 0 657 13,845

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
84
11(c) NON CURRENT ASSETS HELD FOR SALE – CONSOLIDATED
2016 £'000 Note £'000
1,776 At 1 April 2016 0
(161) Transfers (to)/from property, plant and equipment 0 (1,615) Disposals of non-current assets held for sale 0
0 As at 31 March 2017 0
No property assets are currently classified in the Balance Sheet as held for sale.
11(d) PROPERTY, PLANT AND EQUIPMENT DISCLOSURES - CONSOLIDATED
2016
£’000 Net book value of Property, plant and equipment at 31 March Note £’000
877,620 Purchased 11a 950,003
13,845 Donated 11b 9,014
891,465 Total B S 959,017
8,750 Net book value related to land valued at open market value at 31 March 8,500
Total value of assets held under:
4,668 Finance Leases 11a 4,582
224,528 PFI and PPP Contracts 11a 246,988
229,196 251,570 Total depreciation charged in respect of assets held under:
266 Finance leases 262
5,561 PFI and PPP contracts 5,963
5,827 6,225
In line with the Board’s revaluation policy a sample was revalued by an independent valuer, GVA at 31 March 2017 on the basis of fair value (market value or depreciated replacement cost where appropriate). The values were computed in accordance with the Royal Institute of Chartered Surveyors Statement of Asset Valuation Practice and Guidance notes, subject to the special accounting practices of the NHS. The net impact was an increase in value of £35.780m (2015/16 increase of £6.801m) which was credited to revaluation reserve. Impairment of £28.272m (2015/16 £0.766m) was charged to the Statement of Comprehensive Net Expenditure and Summary of Resource Outturn. The net impact was an increase in value of £35,780k of which was £7,508k was credited to the revaluation reserve.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
85
12. INVENTORIES – BOARD & CONSOLIDATED
2016
£’000 Note
16,078 Raw Materials and Consumables B S 17,450
16,078 Total Inventories 17,450
13. TRADE AND OTHER RECEIVABLES
Consolidated 2016
Board 2016
Consolidated Board
£’000 £’000 Note £’000 £’000
Receivables due within one year
NHS Scotland
191 191 SGHSCD 70 70
17,332 17,332 Boards 14,279 14,279
17,523 17,523 Total NHS Scotland Receivables 14,349 14,349
568 568 NHS Non-Scottish Bodies 212 212
4,903 4,903 VAT recoverable 1,677 1,677
32,712 32,712 Prepayments 21,847 21,847
9,983 9,983 Accrued income 17,983 17,983
13,170 13,097 Other Receivables 9,828 9,229
4,711 4,711 Reimbursement of provisions 17a 47,479 47,479
1,553 1,553 Other Public Sector Bodies 2,343 2,343
85,123 85,050 Total Receivables due within one year B S 115,718 115,119
Receivables due after more than one year
490 490 Prepayments 694 694
6 6 Other Receivables 5 5
32,385 32,385 Reimbursement of Provisions 17a 43,909 43,909
32,881 32,881 Total Receivables due after more than one year B S 44,608 44,608
118,004 117,931 TOTAL RECEIVABLES 160,326 159,727
1,853 1,853 The total receivables figure above includes a provision for bad debts of : 2,747 2,747
Movements on the provision for impairment of receivables are as follows:
Consolidated 2016
Board 2016
Consolidated Board
£’000 £’000 £’000 £’000
354 354 At 1 April 1,853 1,853
1,771 1,771 Provision for receivables impairment 2,831 2,831
(1) (1) Receivables written off during the year as uncollectable (275) (275)
(271) (271) Unused amounts reversed (1,662) (1,662)
1,853 1,853 At 31 March 2,747 2,747

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
86
13. TRADE AND OTHER RECEIVABLES (continued)
The receivables assessed as individually impaired were mainly English, Welsh and Irish NHS Trusts/ Health Authorities, other Health Bodies, overseas patients, research companies and private individuals and it was assessed that not all of the receivable balance may be recovered. Receivables that are less than three months past their due date are not considered impaired. As at 31 March 2017, receivables with a carrying value of £8.7m (2016: £11.8m) were past their due date but not impaired. The ageing of receivables which are past due but not impaired is as follows:
Consolidated 2016
Board 2016
Consolidated Board
£’000 £’000 £’000 £’000
7,198 7,198 Up to 3 months past due 4,429 4,429
1,466 1,466 3 to 6 months past due 1,692 1,692
3,174 3,174 Over 6 months past due 2,588 2,588
11,838 11,838 Total at 31 March 8,709 8,709
The receivables assessed as past due but not impaired were mainly NHS Scotland Health Boards, Local Authorities and Universities and there is no history of default from these customers recently. Concentration of credit risk is limited due to the customer base being large and unrelated/government bodies. Due to this, management believe that there is no future credit risk provision required in excess of the normal provision for doubtful receivables. The credit quality of receivables that are neither past due nor impaired is assessed by reference to external credit ratings where available. Where no external credit rating is available, historical information about counterparty default rates is used. Trade receivables that are neither past due nor impaired are shown by their credit risk below.
Consolidated 2016
Board 2016
Consolidated Board
£’000 £’000 £’000 £’000
29,128 29,128 Existing customers with no defaults in the past 39,330 39,330
29,128 29,128 Total neither past due or impaired 39,330 39,330
The maximum exposure to credit risk is the fair value of each class of receivable. The NHS Board does not hold any collateral as security. The carrying amount of receivables are denominated in Pounds. All non-current receivables are due within 6 years (2015-16: 6 years) from the balance sheet date. The carrying amount of short term receivables approximates their fair value. The fair value of long term other receivables is £44.6m (2015-16: £32.8m). The effective interest rate on non-current other receivables is Nil% (2015-16: Nil%). Pension liabilities are discounted at Nil% (2015-16: Nil%).

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
87
14. AVAILABLE FOR SALE FINANCIAL ASSETS
Consolidated
2016
Board
2016
Consolidated
Board
£’000 £’000 Note £’000 £’000
16,653 0 UK equities & investment trusts 17,817 0
28,842 0 Non UK equities & investment trusts 36,305 0
8,362 0 Fixed Interest securities 9,008 0
13,310 1,555 Other 13,248 2,110
67,167 1,555 TOTAL BS 76,378 2,110
72,346 1,266 At 1 April 67,167 1,555
10,143 289 Additions 11,164 555
(10,107) 0 Disposals (12,462) 0
(5,215) 0 Revaluation (deficit)/surplus transferred to equity 10,509 0
67,167 1,555 At 31 March 76,378 2,110
0 0 Current BS 0 0
67,167 1,555 Non-current BS 76,378 2,110
67,167 1,555 At 31 March 76,378 2,110
Other Financial Assets available for sale comprise:
33 Loans to Hub South East Scotland Limited 33
33 33
The Edinburgh & Lothian Health Foundation (ELHF) has a pooled investment portfolio with NHS Lanarkshire which is managed by independent investment managers, Schroders. These investments are categorised as level 1 in accordance with IFRS13. Only the ELHF share of the investments is recorded within the Foundations’ Financial Statements and is included within the consolidated Board statements. At year end 2016/17 there were investments of £63,121k and cash awaiting investment £27k. The NHS Lanarkshire share was 6.31% of the total portfolio managed by Casenove (Schroders). ELHF also holds investment properties of £11,120k these are solely owned by ELHF. The investments in the shares of Hub South East Scotland Limited are unlisted and are denominated in UK pounds sterling. These investments are categorised as level 2 in accordance with IFRS13 and are valued at cost less impairment. The loan to Hub South East Scotland Limited is also denominated in UK pounds sterling. The Board owns 11.11% of the share capital of Hub South East Scotland Limited and holds its shares alongside 9 public and private sector partners, including the Scottish Futures Trust, a company controlled by Scottish Ministers. The Board has made a loan of £33k to Hub South East Scotland Limited, and also advanced a further £267k to its public sector partners, to enable them to finance the initial working capital requirements of Hub South East Scotland Limited. NHS Lothian is entitled to recover the full economic cost of activity in support of Hub South East Scotland and has no requirement to under-write any reported trading losses of these companies. The carrying value of the investment is cost less impairment as there is no active market for the equity investment in Hub South East Scotland Limited.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
88
15. CASH AND CASH EQUIVALENTS
At 01/04/16
Cash Flow
At 31/03/17
Note £’000 £’000 £’000
Government Banking Service account balance 623 12,132 12,755 Cash at bank and in hand 73 32 105 Endowments 2,257 191 2,448
Total cash – balance sheet BS 2,953 12,355 15,308
Prior Year
At 01/04/15
Cash Flow
At 31/03/16
£’000 £’000 £’000
Government Banking Service account balance 354 269 623 Cash at bank and in hand 138 (65) 73 Endowment cash 4,574 (2,317) 2,257
Total cash – balance sheet 5,066 (2,113) 2,953
Cash at bank is with major UK banks. The credit risk associated with cash at bank is considered to be low.
16. TRADE AND OTHER PAYABLES
Consolidated
2016
Board
2016
Consolidated
Board
£’000 £’000 Note £’000 £’000
Payables due within one year
NHS Scotland
1,079 1,079 SGHSCD 1,065 1,065
7,123 7,123 Boards 5,599 5,599
8,202 8,202 Total NHS Scotland Payables 6,664 6,664
6,036 6,036 NHS Non-Scottish Bodies 2,296 2,296
696 696 General Fund Payable 12,860 12,860
24,762 24,762 FHS Practitioners 27,443 27,443
17,771 17,346 Trade Payables 548 548
67,330 63,546 Accruals 86,414 83,425
19,666 19,666 Deferred Income 19,003 19,003
4 4 Net obligations under Finance Leases 22 0 0
5,320 5,320 Net obligations under PPP/PFI Contracts 6,990 6,990
16,438 16,438 Income tax and social security 18,590 18,590
12,806 12,806 Superannuation 13,139 13,139
278 278 Other Public Sector Bodies (33) (33)
2,246 2,246 Other payables 1,573 1,573
11,036 11,036 Employee Benefits 11,256 11,256
5,822 5,822 Pay and Conditions Accrual 2,037 2,037
7,051 7,051 Capital Accruals 7,740 7,740
205,464 201,255 Total Payables due within one year B S 216,520 213,531
Payables due after more than one year
6,031 6,031 Net obligations under PPP/PFI Contracts due within 1-2 years 7,413 7,413
23,435 23,435 Net obligations under PPP/PFI Contracts due after 2 years but within 5 years 28,533 28,533
151,583 151,583 Net obligations under PPP/PFI Contracts due after 5 years 174,982 174,982
376 0 Accruals 151 0
102,995 102,995 NPDs 166,493 166,493
284,420 284,044 Total Payables due after more than one year B S 377,572 377,421
489,884 485,299 TOTAL PAYABLES 594,092 590,952

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
89
16. TRADE AND OTHER PAYABLES (continued)
Consolidated 2016
Board 2016
Consolidated Board
£’000 £’000 £’000 £’000
Borrowings included above comprise:
4 4 Finance Leases 0 0
186,369 186,369 PFI Contracts 217,918 217,918
186,373 186,373 217,918 217,918
The carrying amount and fair value of the non-current borrowings are as follows:
Carrying amount
181,049 181,049 PFI Contracts 210,928 210,928
181,049 181,049 210,928 210,928
Fair value
0 0 Finance Leases 204,875 204,875
181,049 181,049 PFI Contracts 173,350 173,350
181,049 181,049 378,225 378,225
The carrying amount of short term payables approximates to their fair value and is demonminated in Pounds.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
90
17. PROVISIONS – CONSOLIDATED
2016 Pensions &
similar obligations
Clinical & Medical
Negligence
Participation in CNORIS
Other Total
£'000 £’000 £’000 £’000 £’000 £’000
97,013 At 1 April 2016 21,789 39,192 57,526 850 119,357
33,803 Arising during the year 3,913 65,626 45,630 1,398 116,567
(5,909) Utilised during the year (1,676) (3,831) 0 (434) (5,941)
24 Unwinding of discount 4 (8,209) 0 0 (8,205)
(5,574) Reversed unutilised (528) 0 0 (285) (813)
119,357 At 31 March 2017 23,502 92,778 103,156 1,529 220,965
The amounts shown above are stated gross and the amount of any expected reimbursements are separately disclosed as receivables in Note 13. Other provisions include an amount of £1,529k for non medical CNORIS. Analysis of expected timing of discounted cash flows:
2016 Pensions &
similar obligations
Clinical & Medical
Negligence
Participation in CNORIS
Other Total
£'000 £’000 £’000 £’000 £’000 £’000
24,411 Payable within one year 1,672 47,317 24,611 1,469 75,069
64,406 Payable between 2 -5 years 21,830 33,198 53,657 60 108,745
3,416 Payable between 6 – 10 years 0 1,539 2,570 0 4,109
27,124 Thereafter 0 10,724 22,318 0 33,042
119,357 At 31 March 2017 23,502 92,778 103,156 1,529 220,965
Pensions and similar obligations The board meets the additional cost of benefits beyond the normal National Health Service Superannuation Scheme for Scotland benefits in respect of employees who retire early by paying the required amounts annually to the National Health Service Superannuation Scheme for Scotland over the period between early departure and normal retirement date. The Board provides for this in full when the early retirement programme becomes binding by establishing a provision for the expected share of payments over the remaining lives of the former employees, discounted by the Treasury discount rate of 0.24% (2015/16: 1.37%). The Board expects expenditure to be charged to this provision for a period of up to 30 years. Clinical & Medical Negligence The Board holds a provision to meet the costs of all outstanding and potential clinical and medical negligence claims. All legal claims notified to the Board are processed by the Scottish NHS Central Legal Office who will decide upon risk liability and likely outcome of each case. The provision contains sums for settlement awards, legal expenses and third party costs. Clinical and medical negligence cases lodged can be extremely complex. It is expected that expenditure will be charged to this provision for up to 10 years. The amounts disclosed are stated gross and the amount of any expected reimbursements from the Clinical Negligence and Other Risks Insurance Scheme (CNORIS) is shown separately as receivables in Note 13 to the accounts. Reimbursements yet to be received are included in current and long term trade receivables.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
91
17a) CLINICAL NEGLIGENCE AND OTHER RISKS INDEMNITY SCHEME (CNORIS)
2016 2017
£’000 Note £’000
40,042 Provision recognising individual claims against the NHS Board as at 31 March
17 94,307
(37,096) Associated CNORIS receivable at 31 March 13 (91,388) 57,526 Provision recognising the NHS Board’ liability from participating in the scheme at 31 March 17 103,156
60,472 Net Total Provision relating to CNORIS at 31 March 106,075
The Clinical Negligence and Other Risks Scheme (CNORIS) has been in operation since 2000. Participation in the scheme is mandatory for all NHS boards in Scotland. The scheme allows for risk pooling of legal claims in relation to clinical negligence and other risks and works in a similar manner to an insurance scheme. CNORIS has an agreed threshold of £25k and any claims with a value less than this are met directly from within boards’ own budgets. Participants e.g. NHS boards contribute to the CNORIS pool each financial year at a pre-agreed contribution rate based on the risks associated with their individual NHS board. If a claim is settled the board will be reimbursed by the scheme for the value of the settlement, less a £25k “excess” fee. The scheme allows for the risk associated with any large or late in the financial year legal claims to be managed and reduces the level of volatility that individual boards are exposed to. When a legal claim is made against an individual board, the board will assess whether a provision or contingent liability for that legal claim is required. If a provision is required then the board will also create an associated receivable recognising reimbursement from the scheme if the legal claim settles. The provision and associated receivable are shown in the first two lines above. The receivable has been netted off against the provision to reflect reimbursement from the scheme. As a result of participation in the scheme, boards should also recognise that they will be required to make contributions to the scheme in future years. Therefore a second provision that recognises the board’s share of the total CNORIS liability of NHSScotland has been made and this is reflected in third line above. Therefore there are two related but distinct provisions required as a result of participation in the scheme. Both of these provisions as well as the associated receivable have been shown in the note above to aid the reader’s understanding of CNORIS. Further information on the scheme can be found at: http://www.clo.scot.nhs.uk/our-services/cnoris.aspx

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
92
18. MOVEMENT ON WORKING CAPITAL
2016 Opening
Balances Closing
Balances Net
Movement
£’000 Note £’000 £’000 £’000
INVENTORIES
105 Balance Sheet 12 16,078 17,450
105 Net Decrease/(Increase) (1,372)
TRADE AND OTHER RECEIVABLES
1,598 Due within one year 13 85,050 115,119
(10,647) Due after more than one year 13 32,881 44,608
117,931 159,727
96 Less: Property, Plant & equipment included in above (116) (297)
117,815 159,430
(8,953) Net Decrease/(Increase) (41,615)
TRADE AND OTHER PAYABLES
12,714 Due within one year 16 201,255 213,531
79,705 Due after more than one year 16 284,044 377,421 (560) Less: Property, Plant & Equipment (Capital) included
in above (7,051) (9,740)
(204) Less: General Fund Creditor included in above 16 (696) (12,860)
4,706 Less: Lease and PFI Creditors included in above 16 (186,373) (217,918)
291,179 350,434
96,361 Net (Decrease)/Increase 59,255
PROVISIONS
22,344 Due within one year 17 119,357 220,965
22,344 Net (Decrease)/Increase 101,608
109,857 NET MOVEMENT Decrease/(Increase) 117,876
19. CONTINGENT LIABILITIES/ASSETS – CONSOLIDATED The following contingent liabilities have not been provided for in the Accounts:
2016
£’000 £’000
78,395 Clinical and medical compensation payments 69,822
755 Other 423
79,150 70,245 The following contingent assets have not been provided for in the Accounts:
2016
£’000 £’000 (76,891) Clinical and medical negligence contingent assets (68,685)
In the normal course of business, medical incidents may have occurred but may not yet be reported to the Board and so cannot be quantified with sufficient degree of certainty to allow an assessment to be made as to whether or not provision is required. Accordingly no provision has been reported in these Accounts.
Other non-quantifiable contingent liabilities So far as the members are aware, the Board has not entered into any guarantee arrangement, indemnity nor provided any letter of comfort which would give rise to a contingent liability within the meaning of IAS 37.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
93
20. EVENTS AFTER THE REPORTING PERIOD There were no Post Balance Sheet date events having a material effect on the accounts. 21. COMMITMENTS – CONSOLIDATED (a) Capital Commitments The Board have the following capital commitments which have not been provided for in the accounts:
2016
£’000 Contracted £’000
1 Royal Hospital for Sick Children/DCN enablement 1,448
12 Aseptic Pharmacy Modernisation 25
2,756 REH Phase 1 67
3,557 Microbiology Automation 3,212
0 Ward 20 1,445
0 Medical Equipment 348
0 BLM 474
557 Other Commitments 1,297
6,883 8,316
Authorised but not Contracted
32,999 Royal Hospital for Sick Children and DCN project (Hub) 33,206
1,125 Endoscopy Decon Unit WGH 2,491
18 Aseptic Pharmacy Modernisation 1,114
3,893 REH Phase 1 1,749
1,784 Partnership Centre Bundle 10,544
1,735 Prestonpans 358
1,480 Islay Unit 24
0 Office Property Rationalisation 1,229
0 Anti Ligature 2,802
0 MRI Scanner 1,718
0 Demolition and Site Enabling 3,106
592 Other 1,809
43,626 Total 60,150
(b) Other financial commitments The Board has no other financial commitments (c) Financial Guarantees, Indemnities and Letters of Comfort The Board has not entered into any quantifiable guarantee, or indemnity or letter of comfort arrangement which would require evaluation under IAS 39.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
94
22. LEASES – CONSOLIDATED Total future minimum lease payments under operating and finance leases are given in the table below for the each of the following periods.
2016
£'000 Operating Leases £'000
Buildings
2,434 Not later than one year 3,610
2,434 Later than one year but not later than two years 3,067
7,302 Later than two but not later than five years 9,107
17,672 Later than five years 21,006
Other
2,194 Not later than one year 2,129
1,840 Later than one year but no later than two years 1,174
460 Between two and five years (inclusive) 1,117
Amounts charged to Operating Costs in year were:
5,426 Hire of equipment (including vehicles) 5,445
6,289 Other operating leases 6,002
11,715 11,447
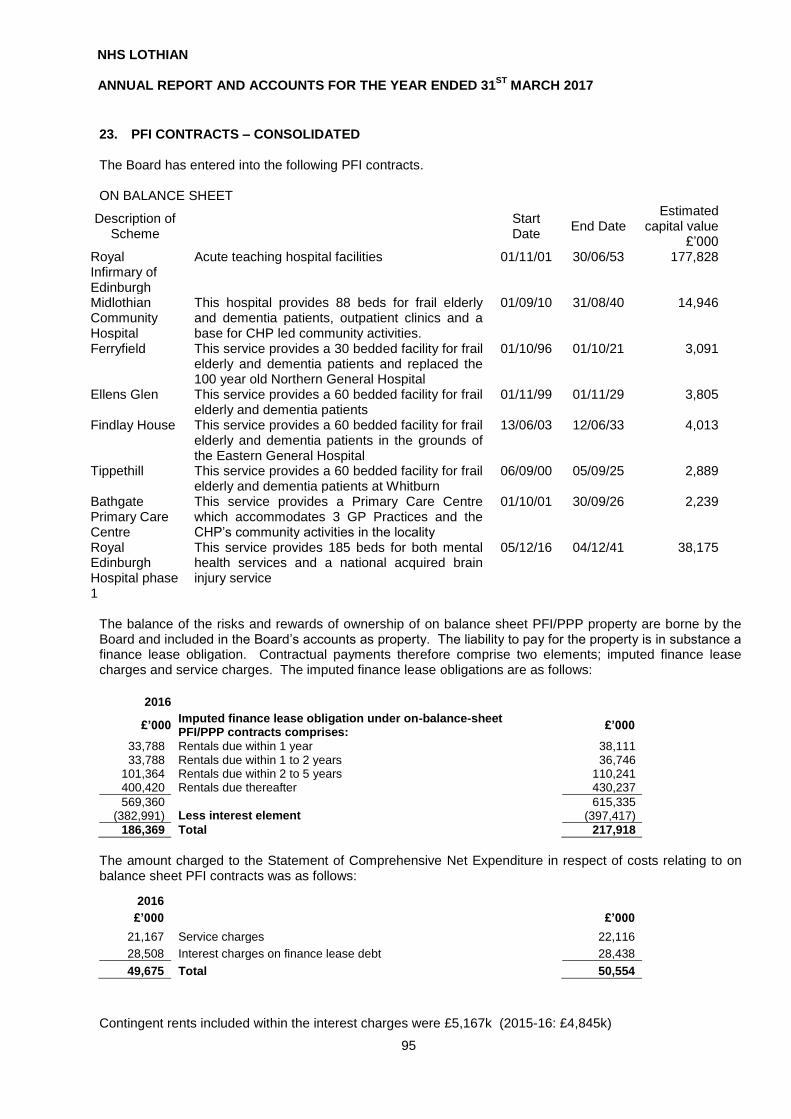
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
95
23. PFI CONTRACTS – CONSOLIDATED The Board has entered into the following PFI contracts. ON BALANCE SHEET
Description of Scheme
Start Date
End Date Estimated
capital value £’000
Royal Infirmary of Edinburgh
Acute teaching hospital facilities 01/11/01 30/06/53 177,828
Midlothian Community Hospital
This hospital provides 88 beds for frail elderly and dementia patients, outpatient clinics and a base for CHP led community activities.
01/09/10 31/08/40 14,946
Ferryfield This service provides a 30 bedded facility for frail elderly and dementia patients and replaced the 100 year old Northern General Hospital
01/10/96 01/10/21 3,091
Ellens Glen This service provides a 60 bedded facility for frail elderly and dementia patients
01/11/99 01/11/29 3,805
Findlay House This service provides a 60 bedded facility for frail elderly and dementia patients in the grounds of the Eastern General Hospital
13/06/03 12/06/33 4,013
Tippethill This service provides a 60 bedded facility for frail elderly and dementia patients at Whitburn
06/09/00 05/09/25 2,889
Bathgate Primary Care Centre
This service provides a Primary Care Centre which accommodates 3 GP Practices and the CHP’s community activities in the locality
01/10/01 30/09/26 2,239
Royal Edinburgh Hospital phase 1
This service provides 185 beds for both mental health services and a national acquired brain injury service
05/12/16 04/12/41 38,175
The balance of the risks and rewards of ownership of on balance sheet PFI/PPP property are borne by the Board and included in the Board’s accounts as property. The liability to pay for the property is in substance a finance lease obligation. Contractual payments therefore comprise two elements; imputed finance lease charges and service charges. The imputed finance lease obligations are as follows:
2016
£’000 Imputed finance lease obligation under on-balance-sheet PFI/PPP contracts comprises:
£’000
33,788 Rentals due within 1 year 38,111 33,788 Rentals due within 1 to 2 years 36,746
101,364 Rentals due within 2 to 5 years 110,241 400,420 Rentals due thereafter 430,237
569,360 615,335 (382,991) Less interest element (397,417)
186,369 Total 217,918
The amount charged to the Statement of Comprehensive Net Expenditure in respect of costs relating to on balance sheet PFI contracts was as follows:
2016
£’000 £’000
21,167 Service charges 22,116
28,508 Interest charges on finance lease debt 28,438
49,675 Total 50,554
Contingent rents included within the interest charges were £5,167k (2015-16: £4,845k)
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
96
24. PENSION COSTS The NHS Board participates in the NHS Superannuation Scheme (Scotland). The scheme is an unfunded statutory public service pension scheme with benefits underwritten by the UK Government. The scheme is financed by payments from employers and from those current employees who are members of the scheme and paying contributions at progressively higher marginal rates based on pensionable pay, as specified in the regulations. The rate of employer contributions is set with reference to a funding valuation undertaken by the scheme actuary. The last four-yearly valuation was undertaken as at 31 March 2012. The next valuation will be as at 31 March 2016 and this will set contribution rates from 1 April 2019. The NHS board has no liability for other employers obligations to the multi-employer scheme. As the scheme is unfunded there can be no deficit or surplus to distribute on the wind-up of the scheme or withdrawal from the scheme. The scheme is an unfunded multi-employer defined benefit scheme. It is accepted that the scheme can be treated for accounting purposes as a defined contribution scheme in circumstances where the NHS board is unable to identify its share of the underlying assets and liabilities of the scheme. The employer contribution of £97.3m were payable to SPPA (2015/16 £94.5m) at the rate of 14.9% (2015/16 14.9%) of pensionable pay for the period from 1 April 2016. While the employee rate applied is a variable it will provide an actuarial yield of 9.8% of pensionable pay. At the last valuation a shortfall of £1.4 billion was identified in the notional fund which will be repaid by a supplementary rate of 2.6% of employers pension contributions for fifteen years from 1 April 2015. This contribution is included in the 14.9% employers contribution rate. The NHS board level of participation in the scheme is 13% based on the proportion of employer contributions paid in 2015 -16. Description of schemes
The new NHS Pension Scheme (Scotland) 2015
From 1 April 2015 the NHS Pension Scheme (Scotland) 2015 was introduced. This scheme is a Career Average Re-valued Earnings (CARE) scheme. Members will accrue 1/54 of their pay as pension for each year they are a member of the scheme. The accrued pension is re-valued each year at an above inflation rate to maintain its buying power. This is currently 1.5% above increases to the Consumer Prices Index (CPI). This continues until the member leaves the scheme or retires. In 2015-16 members paid tiered contribution rates ranging from 5.2% to 14.7% of pensionable earnings. The normal retirement age is the same as the State Pension age. Members can take their benefits earlier but there will be a deduction for early payment. The NHS Superannuation Scheme (Scotland) This scheme closed to new joiners on 31 March 2015 but any benefits earned in either NHS 1995 or NHS 2008 sections are protected and will be paid at the section’s normal pension age using final pensionable pay when members leave or retire. Some members who were close to retirement when the NHS 2015 scheme launched will continue to earn benefits in their current section. This may affect members who were paying into the scheme on 1 April 2012 and were within 10 years of their normal retirement age. Some members who were close to retirement but did not qualify for full protection will remain in their current section beyond 1 April 2015 and join the 2015 scheme at a later date. All other members automatically joined the NHS 2015 scheme on 1 April 2015. Further information is available on the Scottish Public Pensions Agency (SPPA) web site at www.sppa.gov.uk

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
97
2016 2017
£'000 £'000
94,549 Pension cost charge for the year 97,336
21,789 Provisions/Liabilities/Pre-payments included in the Balance Sheet 23,502
25. PRIOR YEAR ADJUSTMENTS
There were no Prior year adjustments
26. FINANCIAL INSTRUMENTS – Consolidated
2016 AT 31 MARCH 2017 Loans and
Receivables Available for
sale Total
£’000 Note £’000 £’000 £’000
Assets per balance sheet 67,167 Investments 14 0 76,378 76,378 25,280 Trade and other receivables excluding
prepayments, reimbursements of provisions and VAT recoverable.
13
30,371 0 30,371
2,953 Cash and cash equivalents 15 15,308 0 15,308
95,400 45,679 76,378 122,057
2016 Other
Financial Liabilities
Total
£’000 Note £’000 £’000
Liabilities per balance sheet 4 Finance lease liabilities 16 0 0
186,369 PFI Liabilities 16 217,918 217,918
143,404
Trade and other payables excluding statutory liabilities (VAT and income tax and social security)
152,285 152,285
329,777 370,203 370,203
FINANCIAL INSTRUMENTS – Board
2016 AT 31 MARCH 2017 Loans and
Receivables Available for
sale Total
£’000 Note £’000 £’000 £’000
Assets per balance sheet 1,555 Investments 14 0 2,110 2,110
25,207 Trade and other receivables excluding prepayments, reimbursements of provisions and VAT recoverable.
29,772 0 29,772
696 Cash and cash equivalents 15 12,860 0 12,860
27,458 42,632 2,110 44,742
2016
Other Financial Liabilities
Total
Note £’000 £’000
Liabilities per balance sheet 4 Finance lease liabilities 16 0 0
186,369 PFI Liabilities 16 217,918 217,918 138,819 Trade and other payables excluding
statutory liabilities (VAT and income tax and social security)
149,145 149,145
325,192 367,063 367,063

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
98
26 (b) Financial Risk Factors
Exposure to Risk
The NHS Board's activities expose it to a variety of financial risks:
Credit risk - the possibility that other parties might fail to pay amounts due
Liquidity risk - the possibility that the NHS Board might not have funds available to meet its commitments to make payments
Market risk - the possibility that financial loss might arise as a result of changes in such measures as interest rates, stock market movements of foreign exchange rates.
Because of the largely non-trading nature of its activities and the way in which government departments are financed, the NHS Board is not exposed to the degree of financial risk faced by business entities. The Board provides written principles for overall risk management, as well as written policies covering: i) Credit Risk Credit risk arises from cash and cash equivalents, deposits with banks and other institutions, as well as credit exposures to customers, including outstanding receivables and committed transactions. For banks and other institutions, only independently rated parties with a minimum rating of 'A' are accepted. Customers are assessed, taking into account their financial position, past experience and other factors, with individual credit limits being set in accordance with internal ratings in accordance with parameters set by the NHS Board. The utilisation of credit limits is regularly monitored. No credit limits were exceeded during the reporting period and no losses are expected from non-performance by any counterparties in relation to deposits. ii) Liquidity Risk The Scottish Parliament makes provision for the use of resources by the NHS Board for revenue and capital purposes in a Budget Act for each financial year. Resources and accruing resources may be used only for the purposes specified and up to the amounts specified in the Budget Act. The Act also specifies an overall cash authorisation to operate for the financial year. The NHS Board is not therefore exposed to significant liquidity risks. The table below analyses the financial liabilities into relevant maturity groupings based on the remaining period at the balance sheet to contractual maturity date. The amounts disclosed in the table are the contractual undiscounted cash flows.
iii) Market Risk The NHS Board has no powers to borrow or invest surplus funds. Financial assets and liabilities are generated by day-to-day operational activities and are not held to manage the risks facing the NHS Board in undertaking its activities. Cash flow and fair value interest risk The NHS Board has no significant interest bearing assets or liabilities and as such income and expenditure cash flows are substantially independent of changes in market interest rates. Foreign Currency Risk The NHS Board is not exposed to foreign exchange rates except through occasional ad-hoc settlement of purchase liabilities denominated in non sterling currencies. The Foundation holds non Sterling equities and bonds and is therefore exposed to foreign currency risk.
Less than 1
year
Between 1 and 2 years
Between 2 and 5 years
Over 5 years
TOTAL
PFI Liabilities 6,990 7,413 28,533 174,982 217,918
Trade and other payables excluding statutory liabilities 7,585 7,585
At 31 March 2017 (£’000) 14,575 7,413 28,533 174,982 225,503
At 31 March 2016 (£’000) 31,655 6,031 23,435 151,583 212,704
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
99
Price risk The NHS Board is not exposed to equity security price risk. The Foundation holds equities and bonds and is therefore exposed to equity price risk. This risk is managed by the investment managers.
26 (c) Fair Value Estimation The fair value of financial instruments that are not traded in an active market is determined using valuation techniques based on future projected cash flows. The carrying value less impairment provision of trade receivables and payables are assumed to approximate their fair value. The fair value of financial liabilities for disclosure purposes is estimated by discounting the future contractual cash flows at the current HM Treasury interest rate that is available for similar financial instruments 26 (d) Derivative Financial Instruments And Forward Currency Exchange Contracts At 31 March 2017 there were no principal amounts outstanding in respect of forward currency exchange contracts and there were no amounts credited or charged to the Statement of Consolidated Comprehensive Net Expenditure in respect of gains or losses on such contracts in the year ended 31 March 2017. 27. RELATED PARTY TRANSACTIONS
(a) By virtue of their membership of the Board, executive and non-executive members are Trustees of the Lothian NHS Endowment Fund, which is a registered Scottish Charity and which expends donations for any NHS purpose and in accordance with the donor of the funds. During 2016/17 the funds spent a total of £4.05m (2015/16: £5.52m), in support and in addition to, NHS funded supplies and services, including capital projects. NHS Lothian had a trading balance due from the Lothian NHS Endowment Fund of £385,170 as at 31 March 2017 (31 March 2016: £480,498).
(b) Mr George Walker was a non-executive member of NHS Lothian until 31 January 2017 and is a director of Waverley Care. In 2016/17, NHS Lothian’s made payments to Waverley Care in relation to mental health service provision that amounted to £484,000 (2015/16: £213,744).
(c) Mr Harry Cartmill is a non-executive member of NHS Lothian and is a director of West Lothian Leisure. In 2016/17, NHS Lothian’s made payments to West Lothian Leisure in relation to health service provision that amounted to £108,104 (2015/16: £107,884).
(d) The Board enters into transactions with other Scottish Government and United Kingdom Government agencies and publicly funded bodies (such as Councils and educational institutions) in the ordinary course of its operations. These transactions take place at arms length. Scottish Ministers issue instructions and guidance on special transactions between publicly funded bodies in areas such as property transfers and joint venture investments.
(e) During 2015/16 a new integration joint board (IJB) was established in each of the four local authority areas within the NHS Lothian boundary, under the terms of the Public Bodies (Joint Working) (Scotland) Act 2014. The IJBs are distinct legal entities the NHS Board and the relevant local authority. The NHS Board and the relevant local authority have delegated some of their functions to these IJBs, and each IJB is wholly responsible for carrying out those functions. The new arrangements for health and social care came fully into effect on 1 April 2016. The Health Board has incurred costs of £868,663k for its contribution to the IJB.

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
100
28. SEGMENT INFORMATION The net operating costs of the Board are analysed on the basis of Individual Business Units reported to the Board for performance management purposes. The acute specialist hospital services are reported under the University Hospital Support Services. East Lothian, Mid Lothian, West Lothian and City of Edinburgh Partnership Business Units are responsible for delivery of Family and Community health services and include Child and Adult Mental Health, Learning Disabilities and acute adult and child mental health services at the Royal Edinburgh Hospital . Corporate Department budgets include the non-clinical support services performed to support the Board’s core operations and Strategic Budgets represent the Board’s commissioning of services, and central overhead costs of the Board. As responsibilities for care shift from the acute sector the segmental analysis and comparatives will reflect these changes. The segments that have been used to report performance management this year are as follows:
University Hospital Support Services East Lothian; Mid Lothian; West Lothian and City of Edinburgh Partnership Business Unit Corporate and Strategic Departments
Edinburgh Integration Joint Boards (IJB) Endowments Assets and liabilities are not reported as part of performance management arrangements so this information is not provided.
Univ Hospitals Support
Services
Partnership Business
Units
Corporate Edinburgh IJB
Endowments Total
£’000 £’000 £’000 £’000 £’000 £’000
Net operating cost 2016/17
901,546 648,511 133,255 (1,845) (10,818) 1,670,649
Net operating cost 2015/16 – Restated
874,755
598,719
71,292
0
7,131
1,551,897

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
101
29. LINKED STATEMENT OF CONSOLIDATED COMPREHENSIVE NET EXPENDITURE (a) Group SOCNE Integrated Joint Board (Joint venture)
Group
2016 Board Endowments
Intra Group adjustment
Edinburgh West East Mid Consolidated
£’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000
Clinical Services Costs
1,424,071 Hospital and Community 2,418,757 0 (299) 0 0 0 0 2,418,458
(255,471) Hospital and Community Income (1,122,613) 0 0
0
0
0
0 (1,122,613)
1,168,600 1,296,144 0 (299) 0 0 0 0 1,295,845
377,281 Family Health 391,119 0 0 0 0 0 0 391,119
(11,943) Family Health Income (13,095) 0 0 0 0 0 0 (13,095)
1,533,938 Total Clinical Services Costs 1,674,168 0 (299) 0 0 0 0 1,673,869
9,014 Administration Costs 7,038 0 0 0 0 0 0 7,038
9,014 7,038 0 0 0 0 0 0 7,038
43,133 Other Non Clinical Services 84,330 3,993 (510) 0 0 0 0 87,813
(34,188) Other Operating Income (82,224) (14,811) 809 0 0 0 0 (96,226)
Joint ventures accounted for on an equity basis 0 0 0
(1,845)
0
0
0 (1,845)
1,551,897 Net Expenditure 1,683,312 (10,818) 0 (1,845) 0 0 0 1,670,649
The intercompany adjustments relate to removal of intercompany rental income to endowments from NHS Lothian £299k, and removal of grants to NHS Lothian £809k. Gains from Foundation investments of £10,117k have been recognised in the Endowment ‘Other Non clinical services’ line above. The £1,845k relates to the NHS Lothian share of £3,690k reserves held by Edinburgh IJB as per 31st March 2017.
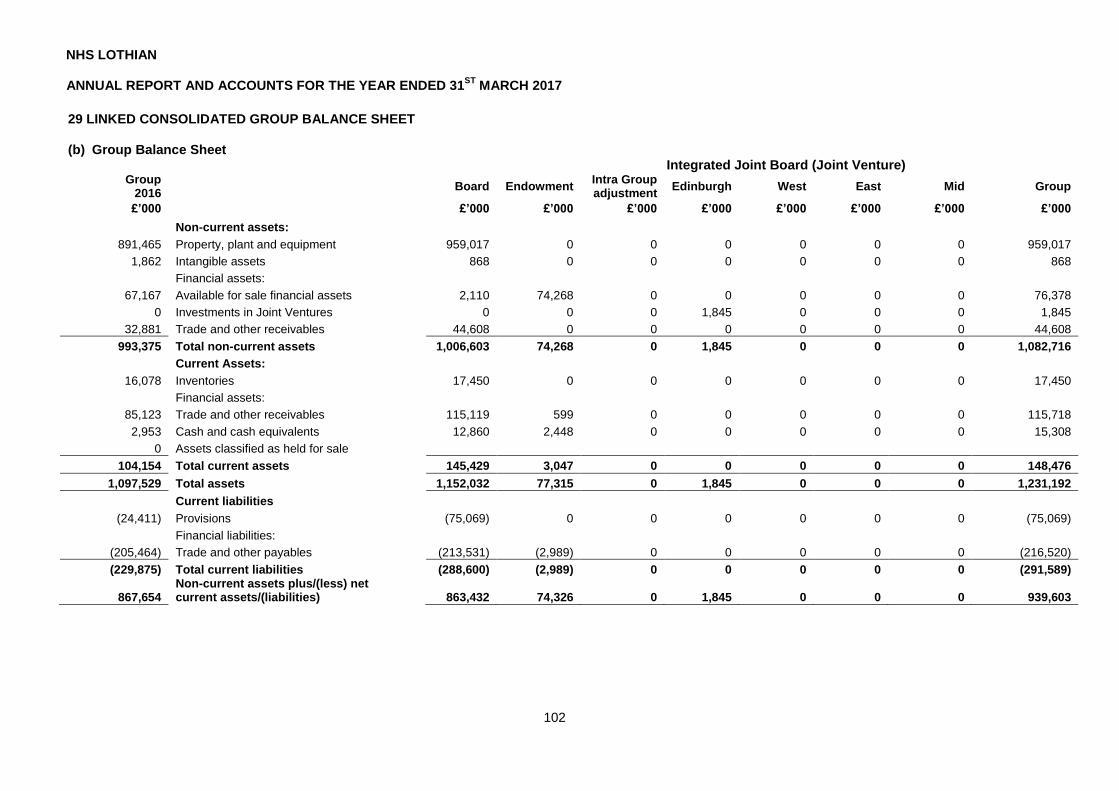
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
102
29 LINKED CONSOLIDATED GROUP BALANCE SHEET (b) Group Balance Sheet
Integrated Joint Board (Joint Venture) Group
2016
Board Endowment
Intra Group adjustment
Edinburgh West East Mid Group
£’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000 £’000
Non-current assets:
891,465 Property, plant and equipment 959,017 0 0 0 0 0 0 959,017
1,862 Intangible assets 868 0 0 0 0 0 0 868
Financial assets:
67,167 Available for sale financial assets 2,110 74,268 0 0 0 0 0 76,378
0 Investments in Joint Ventures 0 0 0 1,845 0 0 0 1,845
32,881 Trade and other receivables 44,608 0 0 0 0 0 0 44,608
993,375 Total non-current assets 1,006,603 74,268 0 1,845 0 0 0 1,082,716
Current Assets:
16,078 Inventories 17,450 0 0 0 0 0 0 17,450
Financial assets:
85,123 Trade and other receivables 115,119 599 0 0 0 0 0 115,718
2,953 Cash and cash equivalents 12,860 2,448 0 0 0 0 0 15,308
0 Assets classified as held for sale
104,154 Total current assets 145,429 3,047 0 0 0 0 0 148,476
1,097,529 Total assets 1,152,032 77,315 0 1,845 0 0 0 1,231,192
Current liabilities
(24,411) Provisions (75,069) 0 0 0 0 0 0 (75,069)
Financial liabilities:
(205,464) Trade and other payables (213,531) (2,989) 0 0 0 0 0 (216,520)
(229,875) Total current liabilities (288,600) (2,989) 0 0 0 0 0 (291,589)
867,654 Non-current assets plus/(less) net current assets/(liabilities) 863,432 74,326 0
1,845
0
0
0 939,603

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
103
Non-current liabilities
(94,946) Provisions (145,896) 0 0 0 0 0 0 (145,896)
Financial liabilities:
(284,420) Trade and other payables (377,421) (151) 0 0 0 0 0 (377,572)
(379,366) Total non-current liabilities (523,317) (151) 0 0 0 0 0 (523,468)
488,288 Assets less liabilities 340,115 74,175 0 1,845 0 0 0 416,135
Taxpayers' Equity
222,506 General fund 152,686 0 0 0 0 0 0 152,686
202,425 Revaluation reserve 187,429 0 0 0 0 0 0 187,429
0 Joint venture reserves 0 0 0 1,845 0 0 0 1,845
63,357 Funds held on Trust 0 74,175 0 0 0 0 0 74,175
488,288 Total taxpayers' equity 340,115 74,175 0 1,845 0 0 0 416,135
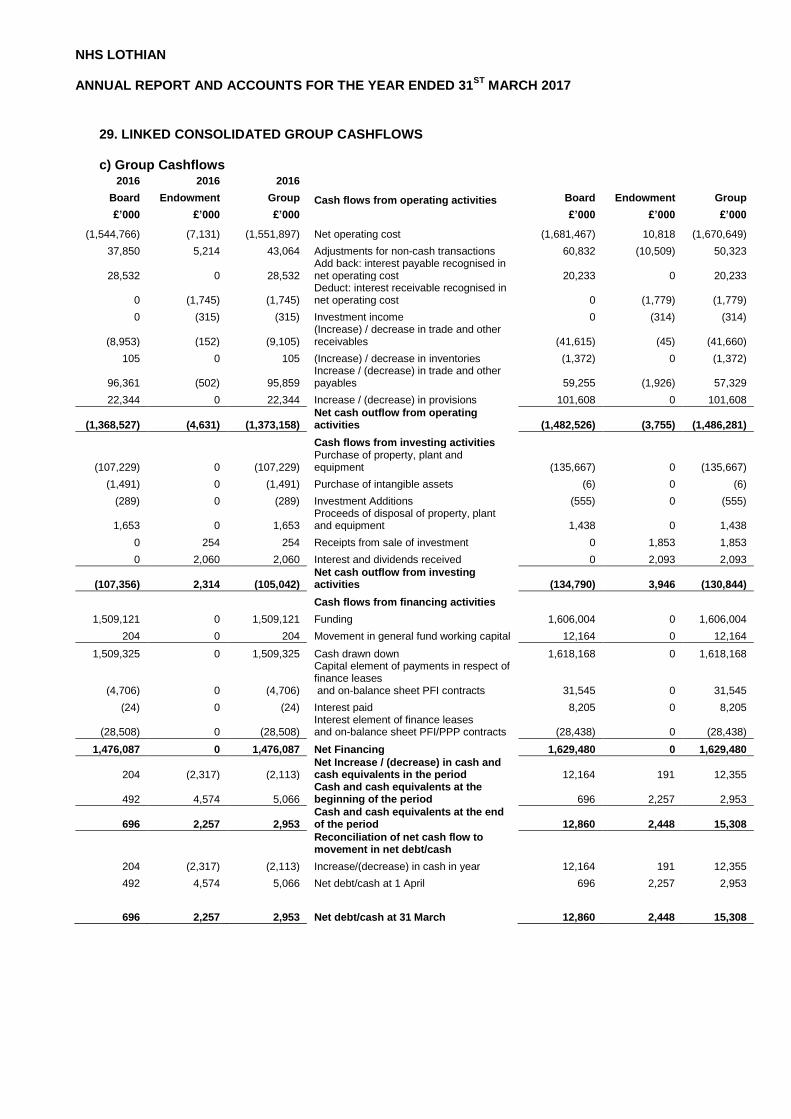
NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
29. LINKED CONSOLIDATED GROUP CASHFLOWS c) Group Cashflows
2016 2016 2016
Board Endowment Group Cash flows from operating activities Board Endowment Group
£’000 £’000 £’000 £’000 £’000 £’000
(1,544,766) (7,131) (1,551,897) Net operating cost (1,681,467) 10,818 (1,670,649)
37,850 5,214 43,064 Adjustments for non-cash transactions 60,832 (10,509) 50,323
28,532 0 28,532 Add back: interest payable recognised in net operating cost 20,233 0 20,233
0 (1,745) (1,745) Deduct: interest receivable recognised in net operating cost 0 (1,779) (1,779)
0 (315) (315) Investment income 0 (314) (314)
(8,953) (152) (9,105) (Increase) / decrease in trade and other receivables (41,615) (45) (41,660)
105 0 105 (Increase) / decrease in inventories (1,372) 0 (1,372)
96,361 (502) 95,859 Increase / (decrease) in trade and other payables 59,255 (1,926) 57,329
22,344 0 22,344 Increase / (decrease) in provisions 101,608 0 101,608
(1,368,527) (4,631) (1,373,158) Net cash outflow from operating activities (1,482,526) (3,755) (1,486,281)
Cash flows from investing activities
(107,229) 0 (107,229) Purchase of property, plant and equipment (135,667) 0 (135,667)
(1,491) 0 (1,491) Purchase of intangible assets (6) 0 (6)
(289) 0 (289) Investment Additions (555) 0 (555)
1,653 0 1,653 Proceeds of disposal of property, plant and equipment 1,438 0 1,438
0 254 254 Receipts from sale of investment 0 1,853 1,853
0 2,060 2,060 Interest and dividends received 0 2,093 2,093
(107,356) 2,314 (105,042) Net cash outflow from investing activities (134,790) 3,946 (130,844)
Cash flows from financing activities
1,509,121 0 1,509,121 Funding 1,606,004 0 1,606,004
204 0 204 Movement in general fund working capital 12,164 0 12,164
1,509,325 0 1,509,325 Cash drawn down 1,618,168 0 1,618,168
(4,706) 0 (4,706)
Capital element of payments in respect of finance leases and on-balance sheet PFI contracts 31,545 0 31,545
(24) 0 (24) Interest paid 8,205 0 8,205
(28,508) 0 (28,508) Interest element of finance leases and on-balance sheet PFI/PPP contracts (28,438) 0 (28,438)
1,476,087 0 1,476,087 Net Financing 1,629,480 0 1,629,480
204 (2,317) (2,113) Net Increase / (decrease) in cash and cash equivalents in the period 12,164 191 12,355
492 4,574 5,066 Cash and cash equivalents at the beginning of the period 696 2,257 2,953
696 2,257 2,953 Cash and cash equivalents at the end of the period 12,860 2,448 15,308
Reconciliation of net cash flow to movement in net debt/cash
204 (2,317) (2,113) Increase/(decrease) in cash in year 12,164 191 12,355
492 4,574 5,066 Net debt/cash at 1 April 696 2,257 2,953
696 2,257 2,953 Net debt/cash at 31 March 12,860 2,448 15,308

NHS LOTHIAN ANNUAL REPORT AND ACCOUNTS FOR THE YEAR ENDED 31
ST MARCH 2017
105



















