
Ankylosing Spondylitis. Case 52 yo wm c 25 yr hx of AS. Recurrent iritis and persistent bilateral...
38
Ankylosing Spondylitis
-
Upload
clarissa-gibbs -
Category
Documents
-
view
215 -
download
0
Transcript of Ankylosing Spondylitis. Case 52 yo wm c 25 yr hx of AS. Recurrent iritis and persistent bilateral...
Ankylosing SpondylitisAnkylosing Spondylitis
CaseCase
52 yo wm c 25 yr hx of AS. Recurrent iritis and persistent bilateral knee synovitis treated with indomethacin and local steroid injections.
52 yo wm c 25 yr hx of AS. Recurrent iritis and persistent bilateral knee synovitis treated with indomethacin and local steroid injections.
In 2006 increasing knee pain with failure of cortisone injections led to consideration of TKR. Low grade fever by hx, weight loss, anemia, malaise and an increase of creatinine to 2.0 led to dc of indocin.
On Clinoril or Diclofenac creatinine 1.8. Chronic kidney stones. Sed rate 120; CRP 18. SPEP IgM lambda monoclonal spike
0.2 gm/dl ;Ig G 2500 ; IgA and IgM normal. Bone marrow normal. Upper and lower endoscopies negative.
In 2006 increasing knee pain with failure of cortisone injections led to consideration of TKR. Low grade fever by hx, weight loss, anemia, malaise and an increase of creatinine to 2.0 led to dc of indocin.
On Clinoril or Diclofenac creatinine 1.8. Chronic kidney stones. Sed rate 120; CRP 18. SPEP IgM lambda monoclonal spike
0.2 gm/dl ;Ig G 2500 ; IgA and IgM normal. Bone marrow normal. Upper and lower endoscopies negative.
Lab hgb 9.4 , wbc 9900, plt 792,000 sed 112;
crp 18.1; urinalysis hematuria, no protein. Renal consult saw and found an negative ANA, but a positive ANCA with PR3 of 97 (20). Nephrologist thought he saw one red cell cast.
Lung and ENT CT’s and eval neg for Wegener’s. Kidney biopsy showed no glomerulonephritis, very minimal interstitial inflammation.
Lab hgb 9.4 , wbc 9900, plt 792,000 sed 112;
crp 18.1; urinalysis hematuria, no protein. Renal consult saw and found an negative ANA, but a positive ANCA with PR3 of 97 (20). Nephrologist thought he saw one red cell cast.
Lung and ENT CT’s and eval neg for Wegener’s. Kidney biopsy showed no glomerulonephritis, very minimal interstitial inflammation.
Attempted right TKR, but surgeon closed the procedure thinking tissues looked infected. Extensive evaluation of the knee tissues and for SBE for infection were negative.
Attempted right TKR, but surgeon closed the procedure thinking tissues looked infected. Extensive evaluation of the knee tissues and for SBE for infection were negative.
Temporal artery biopsy was negative. PPD neg pt was started on Enbrel and left off an NSAID. Three weeks later ESR was 50; crp 3, pt had gained 5 lbs had continued neck pain. Scheduled for TKR again.
Temporal artery biopsy was negative. PPD neg pt was started on Enbrel and left off an NSAID. Three weeks later ESR was 50; crp 3, pt had gained 5 lbs had continued neck pain. Scheduled for TKR again.
1. False positive PR3
2. Perioperative use of antiinflammatories and immunosuppressants.
3. Effects of above meds on bone fusion surgeries.
1. False positive PR3
2. Perioperative use of antiinflammatories and immunosuppressants.
3. Effects of above meds on bone fusion surgeries.
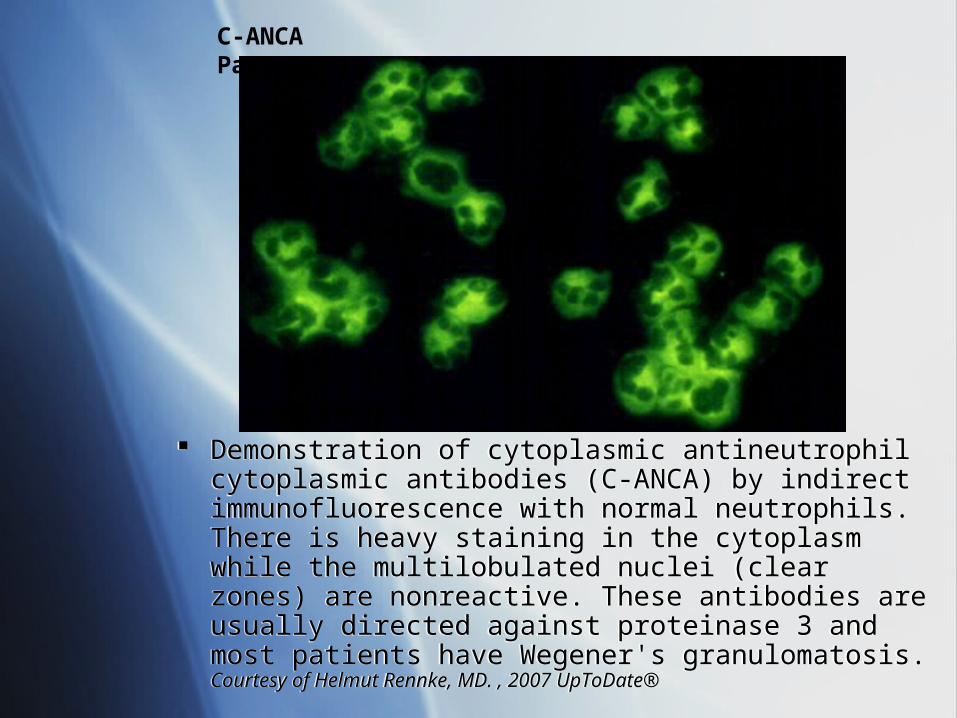
Demonstration of cytoplasmic antineutrophil cytoplasmic antibodies (C-ANCA) by indirect immunofluorescence with normal neutrophils. There is heavy staining in the cytoplasm while the multilobulated nuclei (clear zones) are nonreactive. These antibodies are usually directed against proteinase 3 and most patients have Wegener's granulomatosis. Courtesy of Helmut Rennke, MD. , 2007 UpToDate®
Demonstration of cytoplasmic antineutrophil cytoplasmic antibodies (C-ANCA) by indirect immunofluorescence with normal neutrophils. There is heavy staining in the cytoplasm while the multilobulated nuclei (clear zones) are nonreactive. These antibodies are usually directed against proteinase 3 and most patients have Wegener's granulomatosis. Courtesy of Helmut Rennke, MD. , 2007 UpToDate®
C-ANCA Pattern
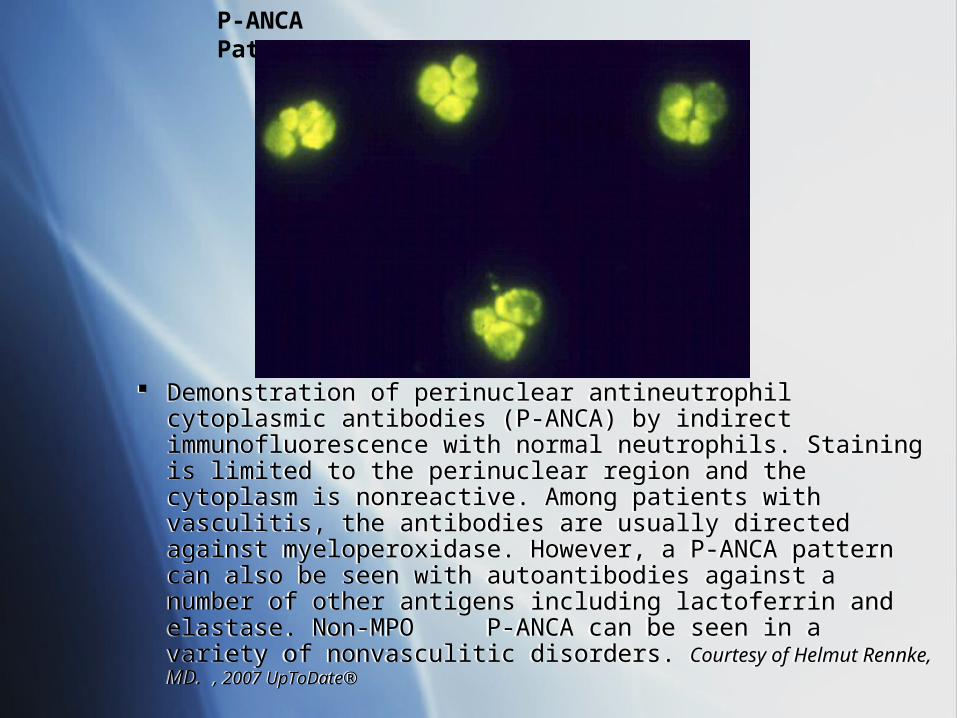
Demonstration of perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) by indirect immunofluorescence with normal neutrophils. Staining is limited to the perinuclear region and the cytoplasm is nonreactive. Among patients with vasculitis, the antibodies are usually directed against myeloperoxidase. However, a P-ANCA pattern can also be seen with autoantibodies against a number of other antigens including lactoferrin and elastase. Non-MPO P-ANCA can be seen in a variety of nonvasculitic disorders. Courtesy of Helmut Rennke, MD. , 2007 UpToDate®
Demonstration of perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) by indirect immunofluorescence with normal neutrophils. Staining is limited to the perinuclear region and the cytoplasm is nonreactive. Among patients with vasculitis, the antibodies are usually directed against myeloperoxidase. However, a P-ANCA pattern can also be seen with autoantibodies against a number of other antigens including lactoferrin and elastase. Non-MPO P-ANCA can be seen in a variety of nonvasculitic disorders. Courtesy of Helmut Rennke, MD. , 2007 UpToDate®
P-ANCA Pattern
PR3PR3
Subacute bacterial endocarditis with positive cytoplasmic antineutrophil cytoplasmic antibodies and anti-proteinase 3 antibodies.
AU Choi HK; Lamprecht P; Niles JL; Gross WL;
Merkel PA SO Arthritis Rheum 2000 Jan;43(1):226-31.
Subacute bacterial endocarditis with positive cytoplasmic antineutrophil cytoplasmic antibodies and anti-proteinase 3 antibodies.
AU Choi HK; Lamprecht P; Niles JL; Gross WL;
Merkel PA SO Arthritis Rheum 2000 Jan;43(1):226-31.
OBJECTIVE: To report a potentially important limitation of antineutrophil cytoplasmic antibody (ANCA) testing: positive results in patients with subacute bacterial endocarditis (SBE).
METHODS: We describe 3 patients with SBE who presented with features mimicking ANCA-associated vasculitis (AAV) and positive findings on tests for cytoplasmic ANCA (cANCA) by indirect immunofluorescence and for anti-proteinase 3 (anti-PR3)antibodies by antigen-specific enzyme-linked immunosorbent assay (ELISA).
OBJECTIVE: To report a potentially important limitation of antineutrophil cytoplasmic antibody (ANCA) testing: positive results in patients with subacute bacterial endocarditis (SBE).
METHODS: We describe 3 patients with SBE who presented with features mimicking ANCA-associated vasculitis (AAV) and positive findings on tests for cytoplasmic ANCA (cANCA) by indirect immunofluorescence and for anti-proteinase 3 (anti-PR3)antibodies by antigen-specific enzyme-linked immunosorbent assay (ELISA).
RESULTS: We are now aware of a total of 7 cases of SBE with positive cANCA and anti-PR3 antibodies. We are not aware of any cases of SBE associated with antimyeloperoxidase/perinuclear ANCA.
Clinical manifestations mimicking AAV included glomerulonephritis, purpura, epistaxis, or sinus symptoms in 6 of the patients.
Streptococcal species were identified in 5 patients, and cardiac valvular abnormalities were demonstrated in 6.
All patients except 1, who died of a complication of SBE, recovered with antibiotic therapy.
RESULTS: We are now aware of a total of 7 cases of SBE with positive cANCA and anti-PR3 antibodies. We are not aware of any cases of SBE associated with antimyeloperoxidase/perinuclear ANCA.
Clinical manifestations mimicking AAV included glomerulonephritis, purpura, epistaxis, or sinus symptoms in 6 of the patients.
Streptococcal species were identified in 5 patients, and cardiac valvular abnormalities were demonstrated in 6.
All patients except 1, who died of a complication of SBE, recovered with antibiotic therapy.
CONCLUSION: Findings of tests for anti-PR3/cANCA antibodies may be positive in patients with SBE.
When encountering ANCA positivity in patients suspected of having systemic vasculitis, physicians should take appropriate steps to rule out infectious diseases, including SBE, before committing the patient to long-term, aggressive immunosuppressive therapy.
CONCLUSION: Findings of tests for anti-PR3/cANCA antibodies may be positive in patients with SBE.
When encountering ANCA positivity in patients suspected of having systemic vasculitis, physicians should take appropriate steps to rule out infectious diseases, including SBE, before committing the patient to long-term, aggressive immunosuppressive therapy.
PR3PR3
Antineutrophil cytoplasmic antibodies reacting with human neutrophil elastase as a diagnostic marker for cocaine-induced midline destructive lesions but not autoimmune vasculitis.
AU Wiesner O; Russell KA; Lee AS; Jenne DE;
Trimarchi M; Gregorini G; Specks U Arthritis Rheum 2004 Sep;50(9):2954-65.
Antineutrophil cytoplasmic antibodies reacting with human neutrophil elastase as a diagnostic marker for cocaine-induced midline destructive lesions but not autoimmune vasculitis.
AU Wiesner O; Russell KA; Lee AS; Jenne DE;
Trimarchi M; Gregorini G; Specks U Arthritis Rheum 2004 Sep;50(9):2954-65.
OBJECTIVE: Human neutrophil elastase (HNE) and proteinase 3 (PR3) are structurally and functionally related. PR3 is the prominent target antigen for antineutrophil cytoplasmic antibodies (ANCAs) in Wegener's granulomatosis (WG). Reported frequencies of HNE ANCAs in WG and other autoimmune diseases range from 0% to 20%.
OBJECTIVE: Human neutrophil elastase (HNE) and proteinase 3 (PR3) are structurally and functionally related. PR3 is the prominent target antigen for antineutrophil cytoplasmic antibodies (ANCAs) in Wegener's granulomatosis (WG). Reported frequencies of HNE ANCAs in WG and other autoimmune diseases range from 0% to 20%.
HNE ANCA reactivity in 25 patients with CIMDL was characterized and compared with that in a control cohort of 604 consecutive patients (64 with WG, 14 with microscopic polyangiitis [MPA], and 526 others) and 45 healthy volunteers
HNE ANCA reactivity in 25 patients with CIMDL was characterized and compared with that in a control cohort of 604 consecutive patients (64 with WG, 14 with microscopic polyangiitis [MPA], and 526 others) and 45 healthy volunteers
Among patients with CIMDL, HNE ANCAs were detectable by 1 assay in 84%, by 2 assays in 68%, and by all 3 assays in 36%. Fifty-seven percent of HNE ANCA-positive CIMDL sera were also PR3 ANCA-positive by at least 1 assay.
Among patients with CIMDL, HNE ANCAs were detectable by 1 assay in 84%, by 2 assays in 68%, and by all 3 assays in 36%. Fifty-seven percent of HNE ANCA-positive CIMDL sera were also PR3 ANCA-positive by at least 1 assay.
In contrast, only 8 (1.3%) of 604 control sera reacted with HNE in at least 1 assay, 3 (0.5%) reacted in 2 assays, and only 1 serum sample (0.16%) reacted in all 3 assays.
Sera obtained from patients with WG or MPA were universally HNE ANCA-negative, as were sera obtained from healthy controls. CONCLUSION: Optimal sensitivity for HNE ANCA requires multimodality testing.
In contrast, only 8 (1.3%) of 604 control sera reacted with HNE in at least 1 assay, 3 (0.5%) reacted in 2 assays, and only 1 serum sample (0.16%) reacted in all 3 assays.
Sera obtained from patients with WG or MPA were universally HNE ANCA-negative, as were sera obtained from healthy controls. CONCLUSION: Optimal sensitivity for HNE ANCA requires multimodality testing.
PR3PR3
Clinical interpretation of antineutrophil cytoplasmic antibodies: parvovirus B19 infection as a pitfall.
AU Hermann J; Demel U; Stunzner D;
Daghofer E; Tilz G; Graninger W SO Ann Rheum Dis 2005 Apr;64(4):641-3.
Epub 2004 Oct 14.
Clinical interpretation of antineutrophil cytoplasmic antibodies: parvovirus B19 infection as a pitfall.
AU Hermann J; Demel U; Stunzner D;
Daghofer E; Tilz G; Graninger W SO Ann Rheum Dis 2005 Apr;64(4):641-3.
Epub 2004 Oct 14.
OBJECTIVE: To investigate whether positive ANCA test results may be a common feature of acute parvovirus B19 infection.
METHODS: Sera were analysed from 1242 patients from a rheumatology outpatient clinic for reactivity with parvovirus B19 and EBV antibodies. They were tested for the presence of PR3-ANCA and MPO-ANCA
OBJECTIVE: To investigate whether positive ANCA test results may be a common feature of acute parvovirus B19 infection.
METHODS: Sera were analysed from 1242 patients from a rheumatology outpatient clinic for reactivity with parvovirus B19 and EBV antibodies. They were tested for the presence of PR3-ANCA and MPO-ANCA
ANCA were found in 10% (5/50) of the sera positive for IgM antibodies to parvovirus and in 3/51 sera containing IgM antibodies to EBV.
Three of six patients with arthritis and concomitant parvovirus infection were found positive for PR3-ANCA and two were found positive for MPO-ANCA. All six patients tested negative for ANCA after six months of follow up.
ANCA were found in 10% (5/50) of the sera positive for IgM antibodies to parvovirus and in 3/51 sera containing IgM antibodies to EBV.
Three of six patients with arthritis and concomitant parvovirus infection were found positive for PR3-ANCA and two were found positive for MPO-ANCA. All six patients tested negative for ANCA after six months of follow up.
CONCLUSIONS: PR3-ANCA and MPO-ANCA may occur transiently in patients with acute B19 infection or infectious mononucleosis, highlighting the importance of repeated antibody tests in oligosymptomatic clinical conditions in which systemic autoimmune disease is suspected.
Department of Medicine, Johns Hopkins University Vasculitis Center, 1830 E. Monument Street, Suite 7500, Baltimore, MD 21205, USA.
CONCLUSIONS: PR3-ANCA and MPO-ANCA may occur transiently in patients with acute B19 infection or infectious mononucleosis, highlighting the importance of repeated antibody tests in oligosymptomatic clinical conditions in which systemic autoimmune disease is suspected.
Department of Medicine, Johns Hopkins University Vasculitis Center, 1830 E. Monument Street, Suite 7500, Baltimore, MD 21205, USA.
PR3PR3
Prevalence of antineutrophil cytoplasmic antibodies in patients with various pulmonary diseases or multiorgan dysfunction.
The Henry Dunant Hospital, Athens, Greece.
OBJECTIVE: To determine the prevalence of antineutrophil cytoplasmic antibodies (ANCA) in patients with diseases that may mimic systemic vasculitides, such as severe multiorgan dysfunction (MOD) and parenchymal pulmonary disorders.
Prevalence of antineutrophil cytoplasmic antibodies in patients with various pulmonary diseases or multiorgan dysfunction.
The Henry Dunant Hospital, Athens, Greece.
OBJECTIVE: To determine the prevalence of antineutrophil cytoplasmic antibodies (ANCA) in patients with diseases that may mimic systemic vasculitides, such as severe multiorgan dysfunction (MOD) and parenchymal pulmonary disorders.
METHODS: We conducted a prospective study of patients with MOD admitted to the medical intensive care unit and patients with various lung diseases seen at the outpatient pulmonary clinic of a tertiary care hospital. Patients with a documented diagnosis of Wegener's granulomatosis (WG) served as positive controls.
RESULTS: Ninety-nine patients with MOD, 29 outpatients with various lung disorders, and 18 patients with WG were included in the study. ANCA were detected by IIF alone in 16% (15/96) of patients with nonvasculitic MOD and 17% (5/29) of outpatients with various pulmonary disorders. The majority of the positive IIF specimens from each group displayed an atypical IIF pattern (73% and 80%, respectively). Only 1 specimen from patients with nonvasculitic disorders was positive for anti-MPO
METHODS: We conducted a prospective study of patients with MOD admitted to the medical intensive care unit and patients with various lung diseases seen at the outpatient pulmonary clinic of a tertiary care hospital. Patients with a documented diagnosis of Wegener's granulomatosis (WG) served as positive controls.
RESULTS: Ninety-nine patients with MOD, 29 outpatients with various lung disorders, and 18 patients with WG were included in the study. ANCA were detected by IIF alone in 16% (15/96) of patients with nonvasculitic MOD and 17% (5/29) of outpatients with various pulmonary disorders. The majority of the positive IIF specimens from each group displayed an atypical IIF pattern (73% and 80%, respectively). Only 1 specimen from patients with nonvasculitic disorders was positive for anti-MPO
CONCLUSION: Detection of ANCA by the combination of IIF and antigen-specific assays for proteinase 3 and myeloperoxidase in diseases that mimic systemic vasculitides is highly specific for WG, microscopic polyangiitis, and Churg-Strauss syndrome.
CONCLUSION: Detection of ANCA by the combination of IIF and antigen-specific assays for proteinase 3 and myeloperoxidase in diseases that mimic systemic vasculitides is highly specific for WG, microscopic polyangiitis, and Churg-Strauss syndrome.
Periop Management-UpToDate®Periop Management-UpToDate®
Only limited data have been published to guide perioperative management. A randomized trial in orthopedic patients found no increased rate of infection in patients who continued weekly methotrexate compared with those who discontinued methotrexate two weeks before surgery [89]. There are no available human data regarding other DMARDs in the perioperative period. Many DMARDs are renally excreted, and thus impaired kidney function can lead to buildup of DMARDs or their metabolites; this may lead to bone marrow suppression.
Only limited data have been published to guide perioperative management. A randomized trial in orthopedic patients found no increased rate of infection in patients who continued weekly methotrexate compared with those who discontinued methotrexate two weeks before surgery [89]. There are no available human data regarding other DMARDs in the perioperative period. Many DMARDs are renally excreted, and thus impaired kidney function can lead to buildup of DMARDs or their metabolites; this may lead to bone marrow suppression.
We recommend that in patients with normal renal function, methotrexate can be continued in the perioperative period. In patients with renal insufficiency, methotrexate should be held for two weeks. Sulfasalazine and azathioprine should be held for a week prior to surgery and resumed after surgery. Leflunamide should be held for two weeks before surgery and resumed after surgery. Hydroxychloroquine has few potential side effects and can be continued without interruption, if the patient can take oral medications. The biologic response modifiers should be stopped one to two weeks prior to surgery and resumed one to two weeks after surgery.
UpToDate®
We recommend that in patients with normal renal function, methotrexate can be continued in the perioperative period. In patients with renal insufficiency, methotrexate should be held for two weeks. Sulfasalazine and azathioprine should be held for a week prior to surgery and resumed after surgery. Leflunamide should be held for two weeks before surgery and resumed after surgery. Hydroxychloroquine has few potential side effects and can be continued without interruption, if the patient can take oral medications. The biologic response modifiers should be stopped one to two weeks prior to surgery and resumed one to two weeks after surgery.
UpToDate®
High dose nonsteroidal anti-inflammatory drugs compromise spinal fusion.
Acute Pain Service, Baystate Medical Center and Tufts University School of Medicine, 759 Chestnut Street, Springfield, Massachusetts 01199, USA. [email protected]
The goal of this retrospective study was to assess the incidence of non-union following the perioperative administration of ketorolac, celecoxib, or rofecoxib. METHODS: We retrospectively analyzed the data of 434 patients receiving perioperative ketorolac [20-240 mg day(-1)], celecoxib [200-600 mg day(-1)], rofecoxib [50 mg day(-1)], or no NSAIDs in the five days following spinal fusion surgery.
High dose nonsteroidal anti-inflammatory drugs compromise spinal fusion.
Acute Pain Service, Baystate Medical Center and Tufts University School of Medicine, 759 Chestnut Street, Springfield, Massachusetts 01199, USA. [email protected]
The goal of this retrospective study was to assess the incidence of non-union following the perioperative administration of ketorolac, celecoxib, or rofecoxib. METHODS: We retrospectively analyzed the data of 434 patients receiving perioperative ketorolac [20-240 mg day(-1)], celecoxib [200-600 mg day(-1)], rofecoxib [50 mg day(-1)], or no NSAIDs in the five days following spinal fusion surgery.
RESULTS: There were no significant differences in the incidence of non-union among the groups that received no NSAIDs (11/130; 8.5%), celecoxib 5/60; 8.3%), or rofecoxib (9/124; 7.3%).
In contrast, 23/120 of patients (19.2%) that received ketorolac had a higher incidence (P < 0.001) of non-union compared to non-NSAID users. However, only 3/50 patients (6%) receiving low-dose ketorolac [< or = 110 mg day(-1)] resulted in non-union which was not significantly different from non-NSAID users.
Patients administered higher doses of ketorolac [120-240 mg day(-1)] resulted in a higher incidence (P < 0.0001) of non-union (20/70; 29%) compared to non-NSAID users.
RESULTS: There were no significant differences in the incidence of non-union among the groups that received no NSAIDs (11/130; 8.5%), celecoxib 5/60; 8.3%), or rofecoxib (9/124; 7.3%).
In contrast, 23/120 of patients (19.2%) that received ketorolac had a higher incidence (P < 0.001) of non-union compared to non-NSAID users. However, only 3/50 patients (6%) receiving low-dose ketorolac [< or = 110 mg day(-1)] resulted in non-union which was not significantly different from non-NSAID users.
Patients administered higher doses of ketorolac [120-240 mg day(-1)] resulted in a higher incidence (P < 0.0001) of non-union (20/70; 29%) compared to non-NSAID users.
CONCLUSIONS: This study revealed that the short-term perioperative administration of celecoxib, rofecoxib, or low-dose ketorolac [< or = 110 mg day(-1)] had no significant deleterious effect on non-union.
In contrast, higher doses of ketorolac [120-240 mg day (-1)], history of smoking, and two level vertebral fusions resulted in a significant increase in the incidence of non-union following spinal fusion surgery.
CONCLUSIONS: This study revealed that the short-term perioperative administration of celecoxib, rofecoxib, or low-dose ketorolac [< or = 110 mg day(-1)] had no significant deleterious effect on non-union.
In contrast, higher doses of ketorolac [120-240 mg day (-1)], history of smoking, and two level vertebral fusions resulted in a significant increase in the incidence of non-union following spinal fusion surgery.
The effect of cyclooxygenase-2 inhibition on analgesia and spinal fusion.
Baystate Medical Center and Tufts University School of Medicine, 759 Chestnut Street, Springfield, MA 01199, USA. [email protected]
METHODS: Eighty patients who were scheduled to undergo spinal fusion received either celecoxib or placebo one hour before the induction of anesthesia and every twelve hours after surgery for the first five postoperative days.
The effect of cyclooxygenase-2 inhibition on analgesia and spinal fusion.
Baystate Medical Center and Tufts University School of Medicine, 759 Chestnut Street, Springfield, MA 01199, USA. [email protected]
METHODS: Eighty patients who were scheduled to undergo spinal fusion received either celecoxib or placebo one hour before the induction of anesthesia and every twelve hours after surgery for the first five postoperative days.
RESULTS: There were no differences in demographic data or blood loss between the two groups. Pain scores were lower in the celecoxib group at one, four, eight, sixteen, and twenty hours postoperatively. There were no differences between the two groups with regard to the pain scores at twelve and twenty-four hours postoperatively.
CONCLUSIONS: The perioperative administration of celecoxib resulted in a significant reduction in postoperative pain and opioid use following spinal fusion surgery. In addition, the short-term administration of this COX-2-specific non-steroidal anti-inflammatory drug had no apparent effect on the rate of nonunion at the time of the one-year follow-up.
RESULTS: There were no differences in demographic data or blood loss between the two groups. Pain scores were lower in the celecoxib group at one, four, eight, sixteen, and twenty hours postoperatively. There were no differences between the two groups with regard to the pain scores at twelve and twenty-four hours postoperatively.
CONCLUSIONS: The perioperative administration of celecoxib resulted in a significant reduction in postoperative pain and opioid use following spinal fusion surgery. In addition, the short-term administration of this COX-2-specific non-steroidal anti-inflammatory drug had no apparent effect on the rate of nonunion at the time of the one-year follow-up.
Time-dependent inhibitory effects of indomethacin on spinal fusion.
Department of Orthopaedic Surgery, Barnes-Jewish Hospital at Washington University, St. Louis, Missouri 63110, USA. [email protected]
METHODS: Seventy New Zealand White rabbits underwent posterior intertransverse process arthrodesis at L5-L6 with use of iliac autograft. Rabbits randomly received indomethacin (10 mg/kg orally) starting at two weeks after surgery (twenty-four animals), indomethacin starting at four weeks postoperatively (twenty-three), or saline starting at two weeks postoperatively (twenty-three) (the control group).
Time-dependent inhibitory effects of indomethacin on spinal fusion.
Department of Orthopaedic Surgery, Barnes-Jewish Hospital at Washington University, St. Louis, Missouri 63110, USA. [email protected]
METHODS: Seventy New Zealand White rabbits underwent posterior intertransverse process arthrodesis at L5-L6 with use of iliac autograft. Rabbits randomly received indomethacin (10 mg/kg orally) starting at two weeks after surgery (twenty-four animals), indomethacin starting at four weeks postoperatively (twenty-three), or saline starting at two weeks postoperatively (twenty-three) (the control group).
RESULTS: Sixty-five percent (fifteen) of the twenty-three spines in the control group and 48% (eleven) of the twenty-three in the four-week group fused. However, only 21% (five) of the twenty-four spines in the two-week group fused. The difference between the two-week and control groups was significant (p < 0.002), as was the difference between the two and four-week groups (p = 0.05).
CONCLUSIONS: The earlier that indomethacin was resumed postoperatively, the greater was its negative effect on fusion. Indomethacin appears to play a significant inhibitory role in the early phase of healing. Initiating indomethacin treatment in the latter phase of healing does not appear to significantly affect fusion rates, although there was a nonsignificant trend toward inhibition.
RESULTS: Sixty-five percent (fifteen) of the twenty-three spines in the control group and 48% (eleven) of the twenty-three in the four-week group fused. However, only 21% (five) of the twenty-four spines in the two-week group fused. The difference between the two-week and control groups was significant (p < 0.002), as was the difference between the two and four-week groups (p = 0.05).
CONCLUSIONS: The earlier that indomethacin was resumed postoperatively, the greater was its negative effect on fusion. Indomethacin appears to play a significant inhibitory role in the early phase of healing. Initiating indomethacin treatment in the latter phase of healing does not appear to significantly affect fusion rates, although there was a nonsignificant trend toward inhibition.
Infectious and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy.
Department of Orthopaedic Surgery, Marshfield Clinic, WI 54449, USA. [email protected]
METHODS: Patients with rheumatoid arthritis undergoing elective foot and ankle surgery over a 12-month period were prospectively followed for the development of complications in the postoperative period. All patients continued their antirheumatic medication schedule unaltered in the perioperative period
Patients were then stratified into two groups based on the use of immunomodulation via TNF-alpha inhibition (group 1) versus patients who did not receive TNF-alpha inhibition therapy (group 2). Groups 1 and 2 were followed and compared for the development of infectious/healing complications.
Infectious and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy.
Department of Orthopaedic Surgery, Marshfield Clinic, WI 54449, USA. [email protected]
METHODS: Patients with rheumatoid arthritis undergoing elective foot and ankle surgery over a 12-month period were prospectively followed for the development of complications in the postoperative period. All patients continued their antirheumatic medication schedule unaltered in the perioperative period
Patients were then stratified into two groups based on the use of immunomodulation via TNF-alpha inhibition (group 1) versus patients who did not receive TNF-alpha inhibition therapy (group 2). Groups 1 and 2 were followed and compared for the development of infectious/healing complications.
RESULTS: Thirty-one patients were enrolled in the study. Group 1 (n = 16) and group 2 (n = 15) patients were comparable for sex distribution, number of orthopaedic procedures performed, and use of steroids, methotrexate, leflunamide, and nonsteroidal anti-inflammatory drugs. Group 1 contained six times the number of smokers in group 2. At mean follow-up of 10.6 months (group 1) and 9.7 months (group 2), healing or infectious complications were similar in both groups. However, when total complications (healing + infection) were analyzed, group 1 (TNF-alpha inhibition, "higher risk") patients demonstrated a lower complication rate (p = .033).
CONCLUSIONS: The data suggest that in patients with rheumatoid arthritis undergoing elective foot and ankle surgery, the use of TNF-alpha inhibition agents may be safely undertaken in the perioperative period without increasing the risk of healing or infectious complications.
RESULTS: Thirty-one patients were enrolled in the study. Group 1 (n = 16) and group 2 (n = 15) patients were comparable for sex distribution, number of orthopaedic procedures performed, and use of steroids, methotrexate, leflunamide, and nonsteroidal anti-inflammatory drugs. Group 1 contained six times the number of smokers in group 2. At mean follow-up of 10.6 months (group 1) and 9.7 months (group 2), healing or infectious complications were similar in both groups. However, when total complications (healing + infection) were analyzed, group 1 (TNF-alpha inhibition, "higher risk") patients demonstrated a lower complication rate (p = .033).
CONCLUSIONS: The data suggest that in patients with rheumatoid arthritis undergoing elective foot and ankle surgery, the use of TNF-alpha inhibition agents may be safely undertaken in the perioperative period without increasing the risk of healing or infectious complications.
Methotrexate and early postoperative complications in patients with rheumatoid arthritis undergoing elective orthopaedic surgery.
Wrightington Hospital NHS Trust, Hall Lane, Appley Bridge, Wigan WN6 9EP, UK.
OBJECTIVES: To determine whether continued methotrexate treatment increases the risk of postoperative infections or of surgical complications in patients with rheumatoid arthritis (RA) within one year of elective orthopaedic surgery. DESIGN: A prospective randomized study of postoperative infection or surgical complications occurring within one year of surgery in patients with RA who underwent elective orthopaedic surgery.
SUBJECTS: 388 patients with RA who were to undergo elective orthopaedic surgery. Patients who were receiving methotrexate were randomly allocated to groups who either continued methotrexate (group A) or who discontinued methotrexate from two weeks before surgery until two weeks after surgery (group B). Their complication rates were compared with complications occurring in 228 patients with RA (group C) who were not receiving methotrexate and who also underwent elective orthopaedic surgery.
Methotrexate and early postoperative complications in patients with rheumatoid arthritis undergoing elective orthopaedic surgery.
Wrightington Hospital NHS Trust, Hall Lane, Appley Bridge, Wigan WN6 9EP, UK.
OBJECTIVES: To determine whether continued methotrexate treatment increases the risk of postoperative infections or of surgical complications in patients with rheumatoid arthritis (RA) within one year of elective orthopaedic surgery. DESIGN: A prospective randomized study of postoperative infection or surgical complications occurring within one year of surgery in patients with RA who underwent elective orthopaedic surgery.
SUBJECTS: 388 patients with RA who were to undergo elective orthopaedic surgery. Patients who were receiving methotrexate were randomly allocated to groups who either continued methotrexate (group A) or who discontinued methotrexate from two weeks before surgery until two weeks after surgery (group B). Their complication rates were compared with complications occurring in 228 patients with RA (group C) who were not receiving methotrexate and who also underwent elective orthopaedic surgery.
RESULTS: Signs of infection or surgical complications occurred in two of 88 procedures in group A (2%), 11 of 72 procedures in group B (15%), and 24 of 228 (10.5%) procedures in group C. The surgical complication or infection frequency in group A was less than that in either group B (p<0.003) or group C (p=0.026).
At six weeks after surgery there were no flares in group A, six flares in group B (8%), and six flares in group C (2.6%). Logistic regression analysis of the overall surgical complication rate in all the patients with RA studied showed that methotrexate, whether continued or discontinued before surgery, did not increase the early complication rate in the patients with RA who underwent elective orthopaedic surgery.
CONCLUSION: Continuation of methotrexate treatment does not increase the risk of either infections or of surgical complications occurring in patients with RA within one year of elective orthopaedic surgery. Thus methotrexate treatment should not be stopped in patients whose disease is controlled by the drug before elective orthopaedic surgery.
RESULTS: Signs of infection or surgical complications occurred in two of 88 procedures in group A (2%), 11 of 72 procedures in group B (15%), and 24 of 228 (10.5%) procedures in group C. The surgical complication or infection frequency in group A was less than that in either group B (p<0.003) or group C (p=0.026).
At six weeks after surgery there were no flares in group A, six flares in group B (8%), and six flares in group C (2.6%). Logistic regression analysis of the overall surgical complication rate in all the patients with RA studied showed that methotrexate, whether continued or discontinued before surgery, did not increase the early complication rate in the patients with RA who underwent elective orthopaedic surgery.
CONCLUSION: Continuation of methotrexate treatment does not increase the risk of either infections or of surgical complications occurring in patients with RA within one year of elective orthopaedic surgery. Thus methotrexate treatment should not be stopped in patients whose disease is controlled by the drug before elective orthopaedic surgery.


















