
Anita Chiu, MD Long Island College Hospital June 12, · PDF fileundergoing appendectomy for...
42
Management of Appendicitis Anita Chiu, MD Long Island College Hospital June 12, 2009
Transcript of Anita Chiu, MD Long Island College Hospital June 12, · PDF fileundergoing appendectomy for...
Management of Appendicitis
Anita Chiu, MDLong Island College HospitalJune 12, 2009,
C P t tiCase Presentationxx-year-old male presenting with a x-day history of abdominal pain associated with nausea, vomiting, decreased appetite, fever and chills on mm/dd/yyyyPain began in epigastrium and migrated to right lower quadrantIncreased in intensity but improved 2 days prior to y p y padmission
PMHx: nonePSHx: noneBirth History: noneImmunizations: up to dateParents separated with joint custody
C P t tiCase PresentationVitals:
Temp 101.5°F BP 104/54 HR 108 RR 20Physical Exam:y
Gen: thin male, anxious, in mild distressHEENT: NC/ATLungs: CTA B/LCVS: RRRAbdomen: soft, RLQ tenderness (+Murphy’s) with palpable 6cm mass, nondistended, +Rovsing’s, +obturator, +rebound tendernesstendernessGU: normal scrotum, testes descended bilaterally, no inguinal hernias
C P t tiCase Presentation
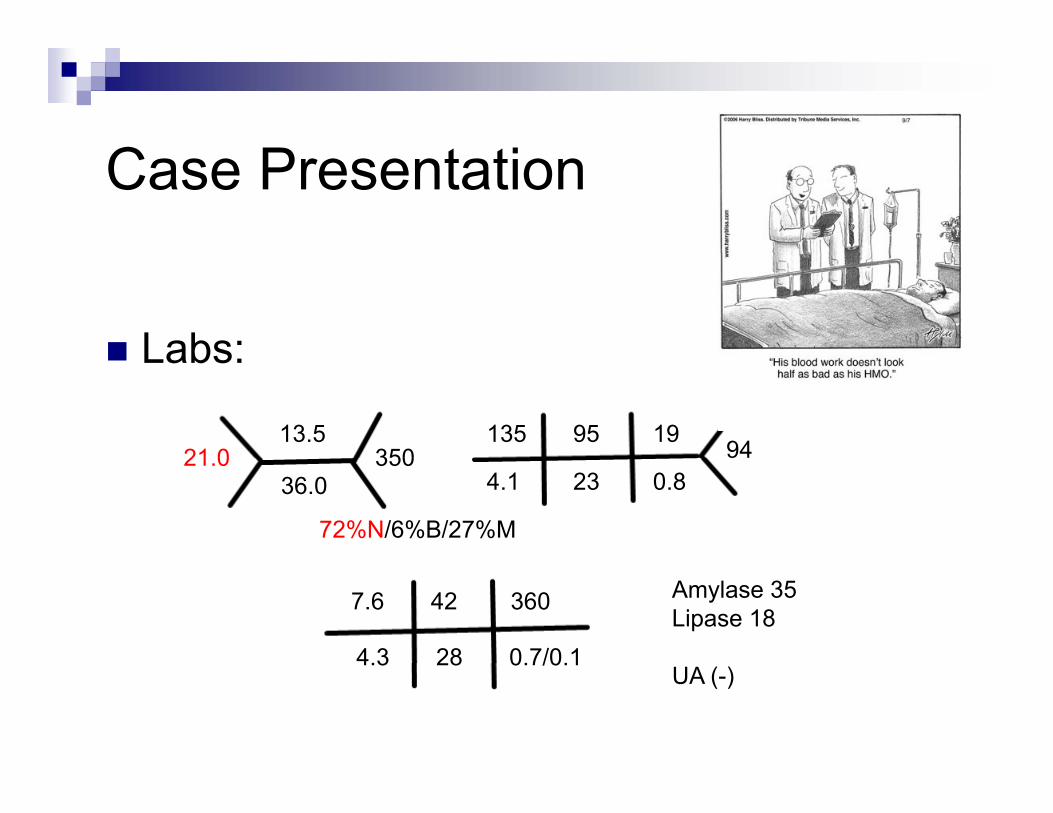
Labs:Labs:
21 013.5
350135 95 19
9421.036.0
350
72%N/6%B/27%M
4.1 23 0.89
7.6 42 360
4.3 28 0.7/0.1
Amylase 35Lipase 18
4.3 28 0.7/0.1UA (-)
C P t tiCase Presentation
Diagnosis of perforated appendicitis with appendicolith and phlegmon madeR it ti ith IVF tibi tiResuscitation with IVF, antibioticsTaken to OR
RLQ incisionRLQ incisionUnable to remove appendix or appendicolithOpen drainage of pusp g pDrain placedSkin left partially open with staples
C P t tiCase Presentation
Post-op course:POD#0: fever, WBC 13.6POD#1: +N/V/D feverPOD#1: +N/V/D, feverPOD#2: fever, diarrhea,distended abdomenPOD#3: fever, abdomen tense, WBC 21POD#4 f fl t bl d BM 1POD#4: fever, +flatus, bloody BMx1POD#5: afebrile, abx changed based on C/S, increased abdominal distensionPOD#6: +diarrhea, C.diff+ -> started on flagyl, JP pulledPOD#7: fever, WBC 22 -> repeat CT scan
C P t tiCase Presentation
C P t tiCase Presentation
POD#8: fever, parenteral nutrition started, IR drainage of RLQ collection (30cc hematoma) with pigtail left in placePOD#9: feverPOD#9: feverPOD#10: WBC 24, staples d/c’d with 10cc pus drainedPOD#11: diarrhea improving, wound draining purulent fluidPOD#12: afebrile, WBC 12POD#13: IR drain d/c’d patient d/c’d home on poPOD#13: IR drain d/c d, patient d/c d home on po antibiotics
AppendicitisAppendicitis
Hi tHistory
1736: first appendectomy credited to Claudius Amyand (St. George’s Hospital, London) on an 11 yo boy with scrotal hernia and fecal fistulascrotal hernia and fecal fistula1824: Louyer-Villermay presented 2 autopsy cases in Paris emphasizing importance of appendicitis1827 F i M li fi t t t t t1827: Francois Melier first to suggest antemortem recogniton of condition but discounted1839: Bright & Addision described symptoms and identified RLQ1886: Fitz coined “appendicitis” in landmark paper
Hi tHistory
Initial surgical therapy designed to drain RLQ abscesses that occurred secondary to perforation1848: Hancock performed first surgical treatment for1848: Hancock performed first surgical treatment for appendicitis with abscess (open drainage without appendectomy)1883: first elective appendectomy in Canada1883: first elective appendectomy in Canada1886: Krönlein – first published account of appendectomy for appendicitis1889: McBurney – landmark paper describing early1889: McBurney landmark paper describing early laparotomy for treatment of appendicitis1894: McBurney’s paper describing his famous incision1982: Semm first successful laparoscopic1982: Semm – first successful laparoscopic appendectomy
I idIncidence
Lifetime rate of appendectomy –12% men, 25% women; approx. 7% of all people undergoing appendectomy for acute appendicitisundergoing appendectomy for acute appendicitis
Rate of appendectomy for appendicitis is constant at 10 per 10,000 patients/yearco sta t at 0 pe 0,000 pat e ts/yeaMost frequently seen in patients in 2nd through 4th decades of life (mean age 31.3, median 22)M:F 1.2 to 1.3:1Misdiagnosis rate 15.3%
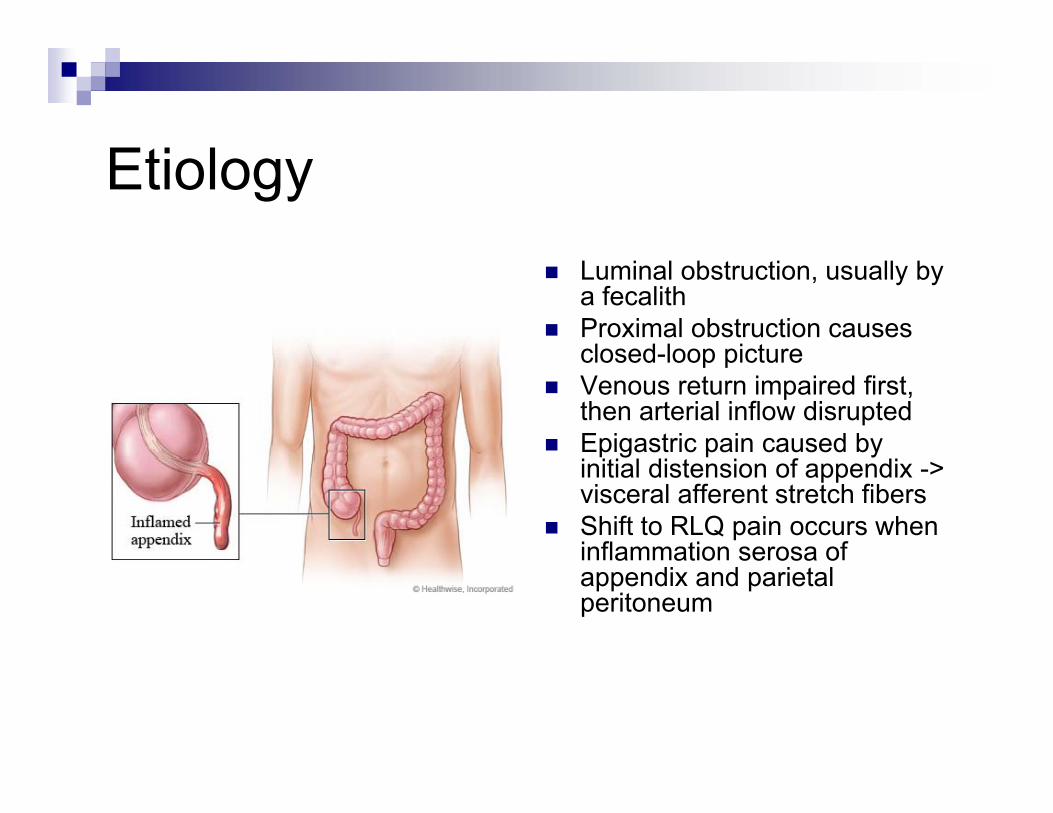
Eti lEtiologyLuminal obstruction, usually by a fecalithProximal obstruction causes closed-loop pictureclosed-loop pictureVenous return impaired first, then arterial inflow disruptedEpigastric pain caused by initial distension of appendix -> visceral afferent stretch fibersShift to RLQ pain occurs when inflammation serosa of a at o se osa oappendix and parietal peritoneum
B t i lBacteriology
Normal appendix similar to that of normal colonnormal colonPrincipal organisms Escherichia coli andEscherichia coli and Bacteroides fragilisFacultative, anaerobic and mycobacteria may be present
A tibi tiAntibiotics
Nonperforated: 24 to 48 hoursPerforated: 7 to 10 daysPerforated: 7 to 10 daysIV antibiotics are usually given until:
WBC lWBC normalAfebrile x 24 hours
P t tiPresentationSymptoms:
AnorexiaAbdominal pain
Signs:Determined by anatomic position of inflamed appendixVi l i i i ll h dVomiting
ObstipationDiarrhea (in children)
Vital signs minimally changed unless complication has already occurredSupine with right thigh drawn p g gupMcBurney’s sign – anterior appendixRebound tendernessRebound tendernessRovsing’s sign, psoas sign, obturator sign
Di iDiagnosis
CBCMild leukocytosis (10,000 to 18,000 mm3) with mild PMN’s
Graded compression sonographyGraded compression sonographyBlind ending, nonperistaltic bowel loop coming off cecum -> noncompressible appendix ≥ 6mm in AP dimensionSensitivity 55 to 96% specificity 85 to 98%Sensitivity 55 to 96%, specificity 85 to 98%
CT scanInflamed, dilated appendix (>5mm), thickened wall, “dirty fat,” target signtarget sign
OR
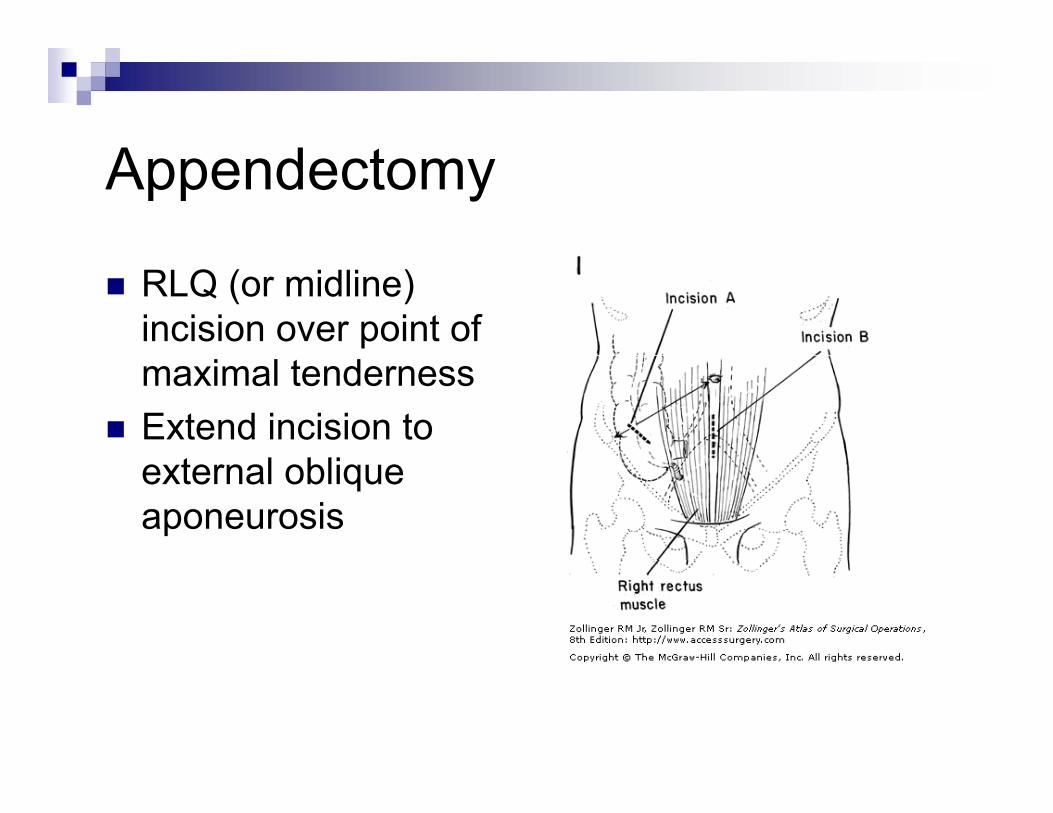
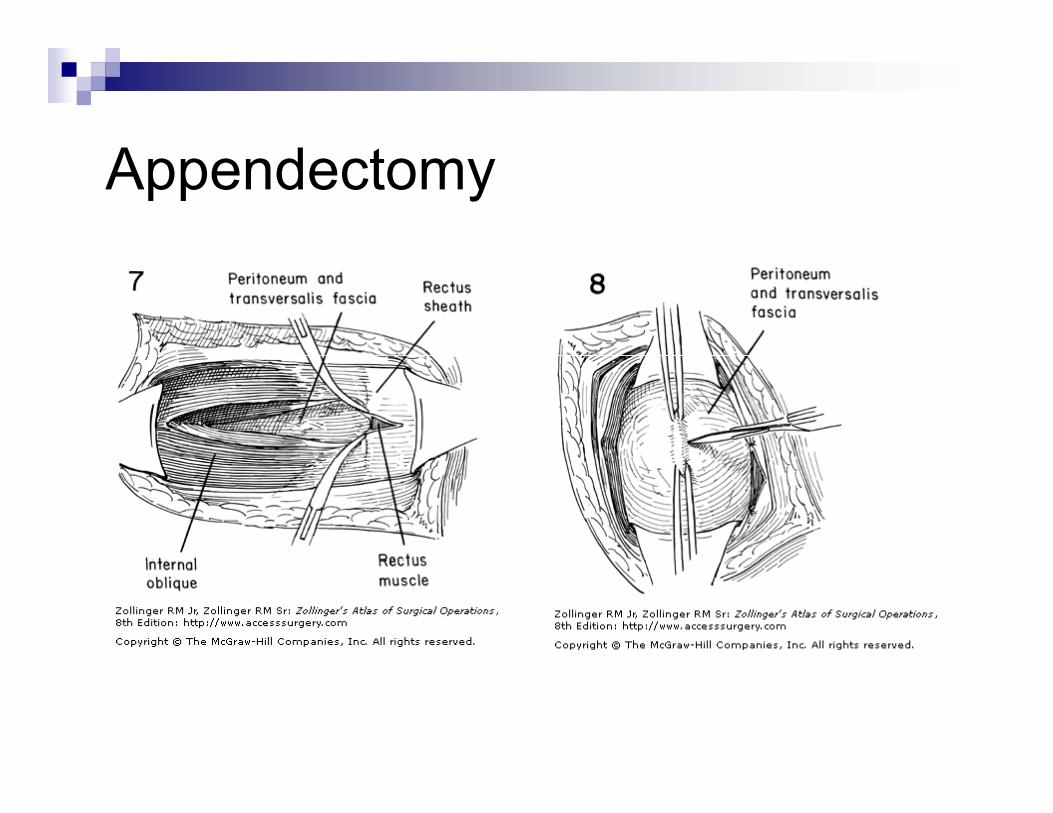
A d tAppendectomy
RLQ (or midline) incision over point of maximal tendernessExtend incision to
t l bliexternal oblique aponeurosis
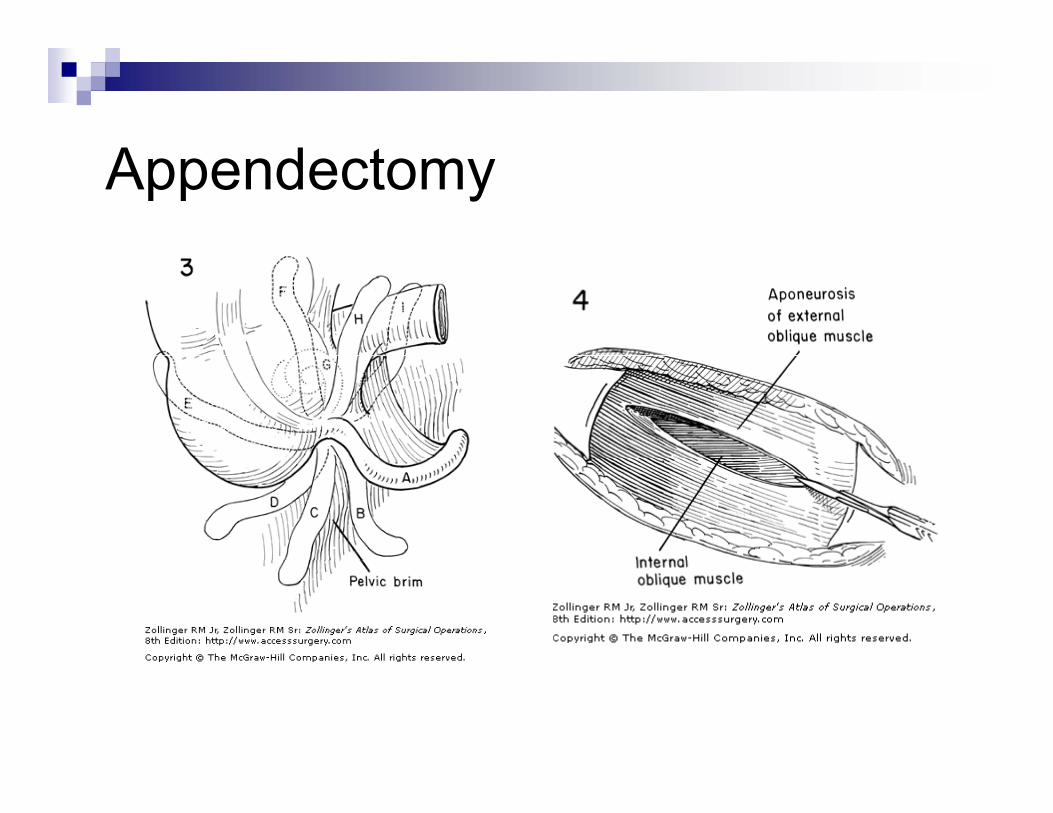
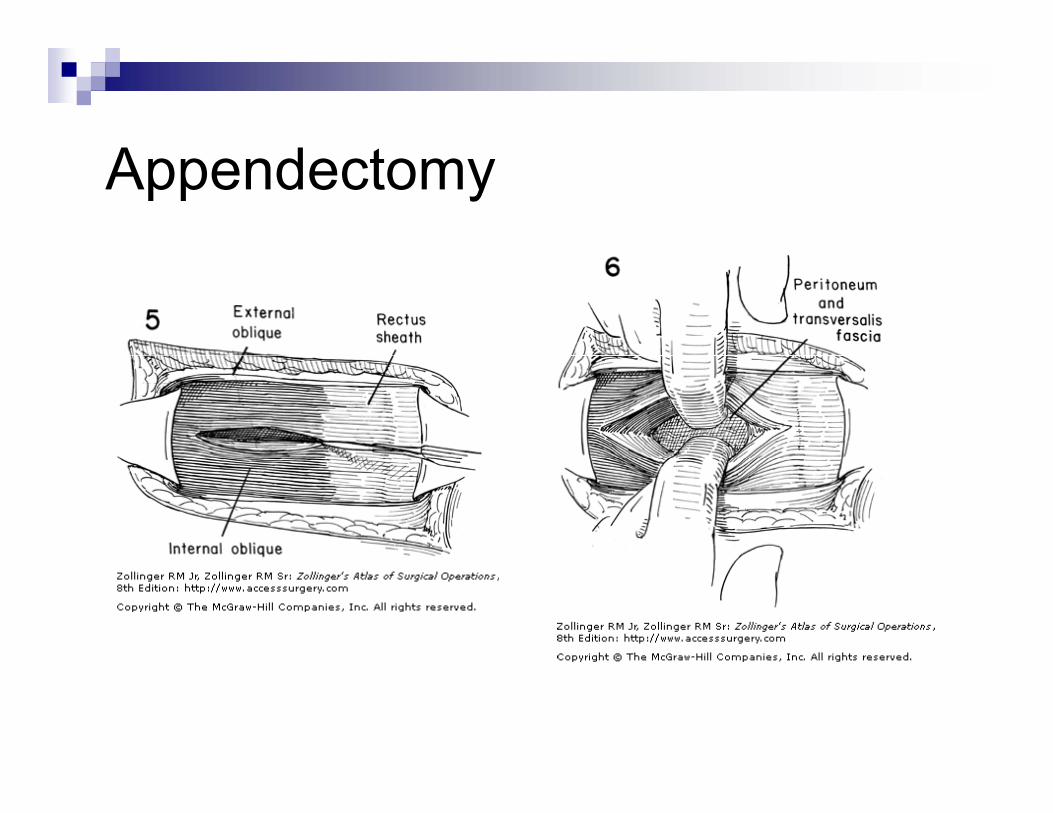
A d tAppendectomy
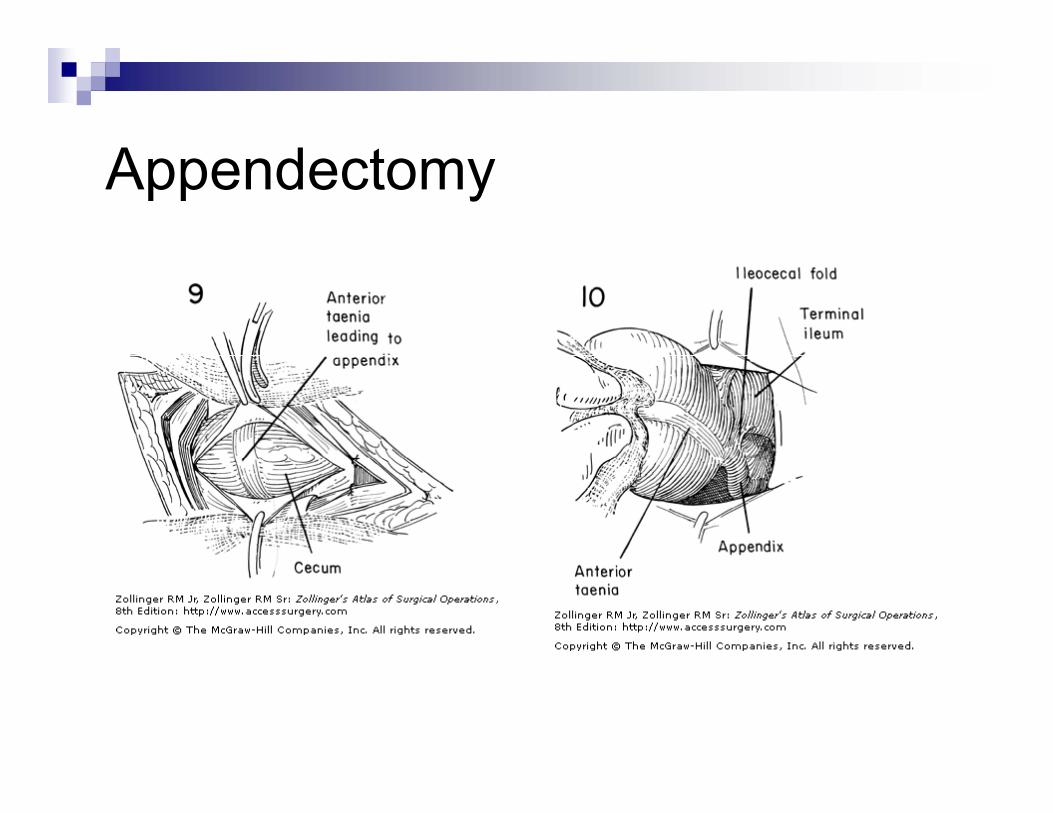
A d tAppendectomy
A d tAppendectomy
A d tAppendectomy
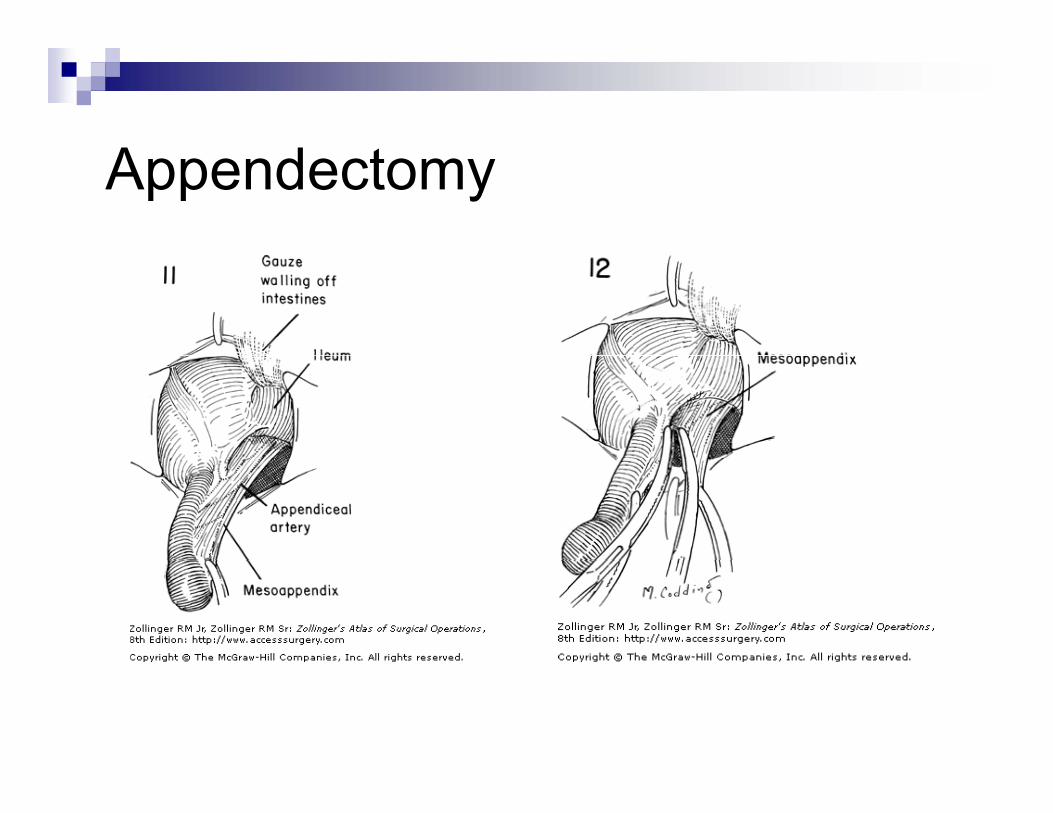
A d tAppendectomy
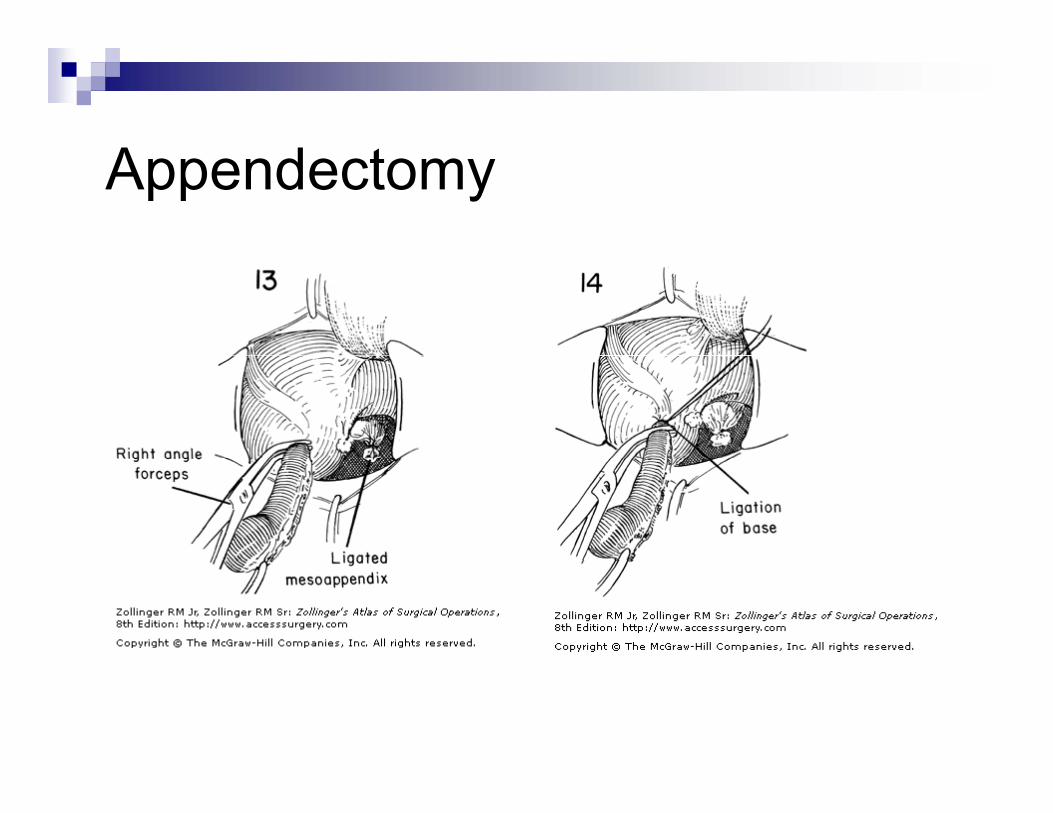
A d tAppendectomy
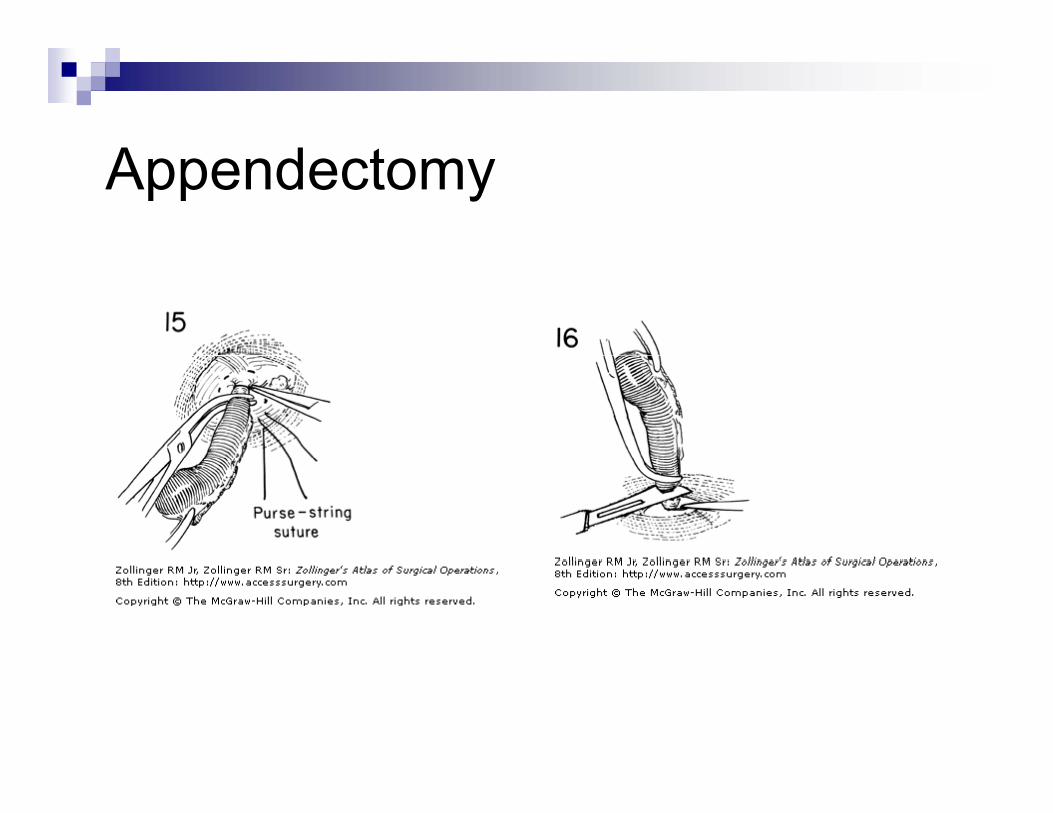
A d tAppendectomy
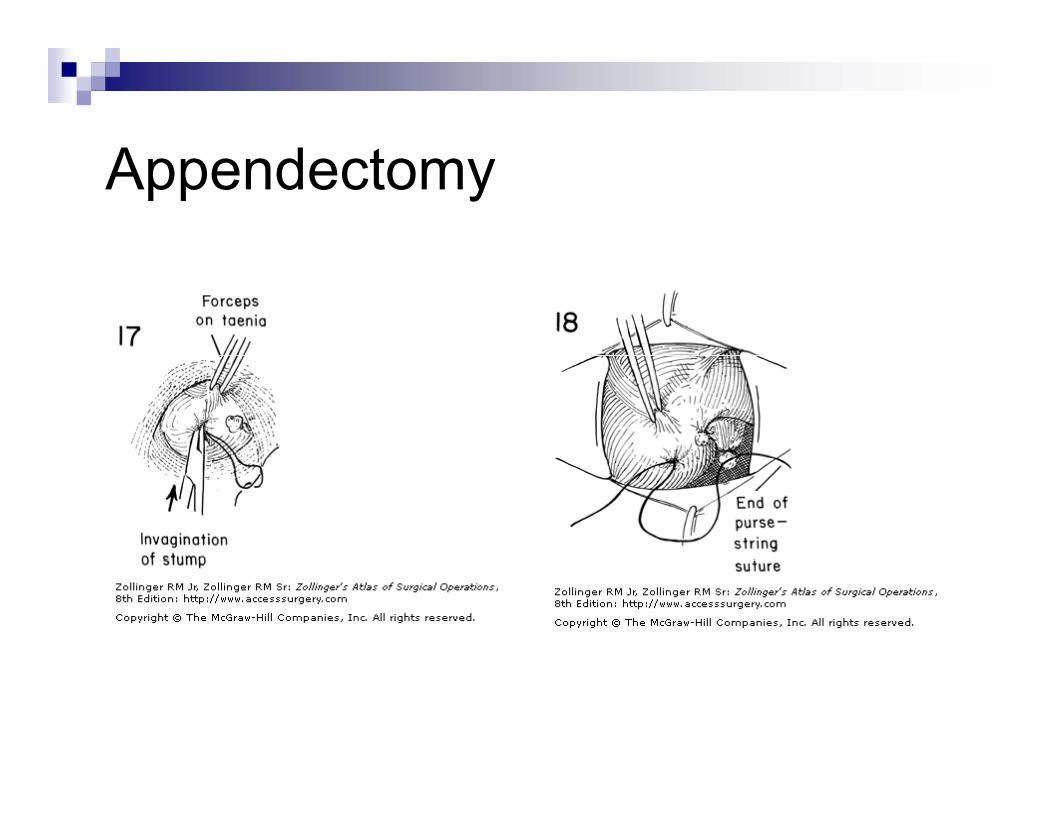
A d tAppendectomy
A d tAppendectomy
IrrigateLayered closureLayered closure
Peritoneum + transversalis with running or interrupted absorbableinterrupted absorbableInternal oblique – interruptedExternal oblique – interrupedExternal oblique – interrupedSkin, subcutaneous
I i iIncisions
McBurney’s – oblique incision 1/3 distance from ASIS to umbilicus1/3 distance from ASIS to umbilicusAdapt incision to point of maximal tendernessParallel to fibers of external obliqueParallel to fibers of external oblique
Rocky-Davis – straight transverse incision through the skin muscle splittingthrough the skin, muscle splitting
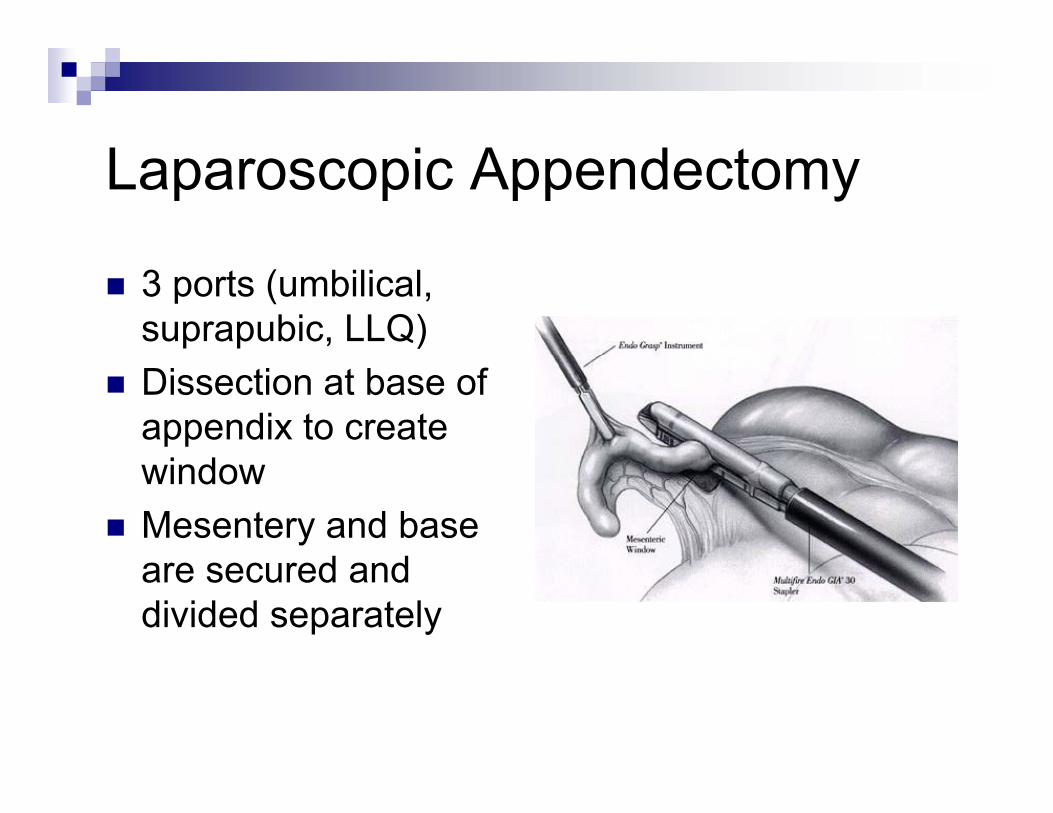
L i A d tLaparoscopic Appendectomy
3 ports (umbilical, suprapubic, LLQ)Dissection at base of appendix to create
i dwindowMesentery and base
d dare secured and divided separately
A di iti i ChildAppendicitis in Children
<5 years: negative appendectomy rate 25%P f ti t 45%Perforation rate 45% Tsao et al (2008) suggest that diagnosis with CTthat diagnosis with CT scan vs H&P alone is more statistically accurate and may guide initialand may guide initial management
“Nurse, he said, it’s an appendix!”
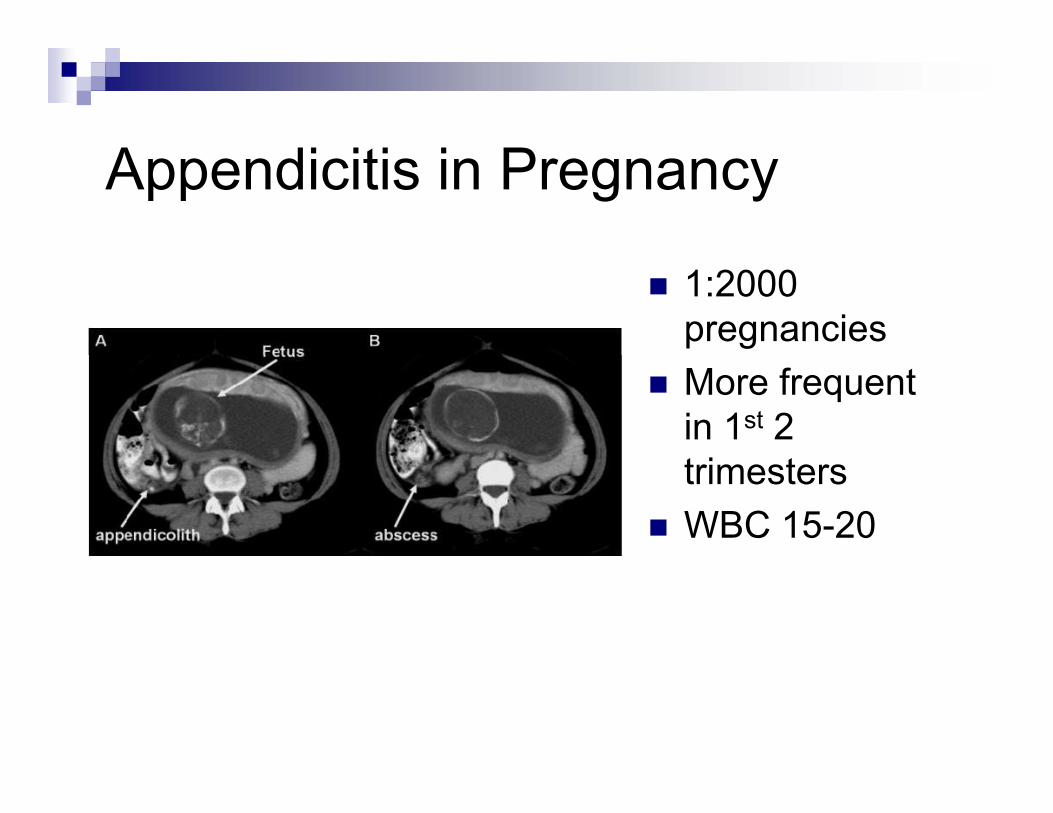
A di iti i PAppendicitis in Pregnancy
1:2000 pregnanciesMore frequent in 1st 2 t i ttrimestersWBC 15-20
A di l R tAppendiceal Rupture
Rate of perforated appendicitis 25.8%
5 (45%) 65 (51%)<5 (45%), >65 (51%)T> 39°F (102°C)WBC > 18 000 mm3WBC > 18,000 mm3
Ill-defined mass 2-6%Majority – contained j y(localized rebound tenderness)
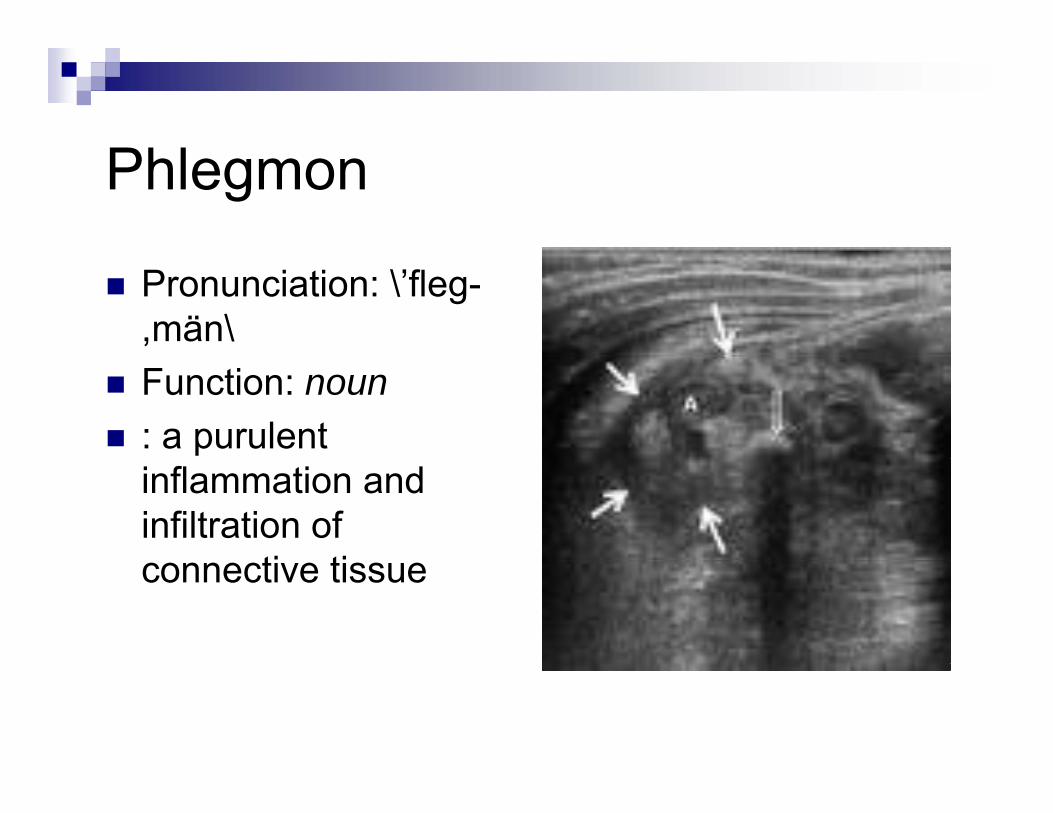
PhlPhlegmon
Pronunciation: \’fleg-,män\Function: noun: a purulent inflammation and infiltration of
ti ticonnective tissue
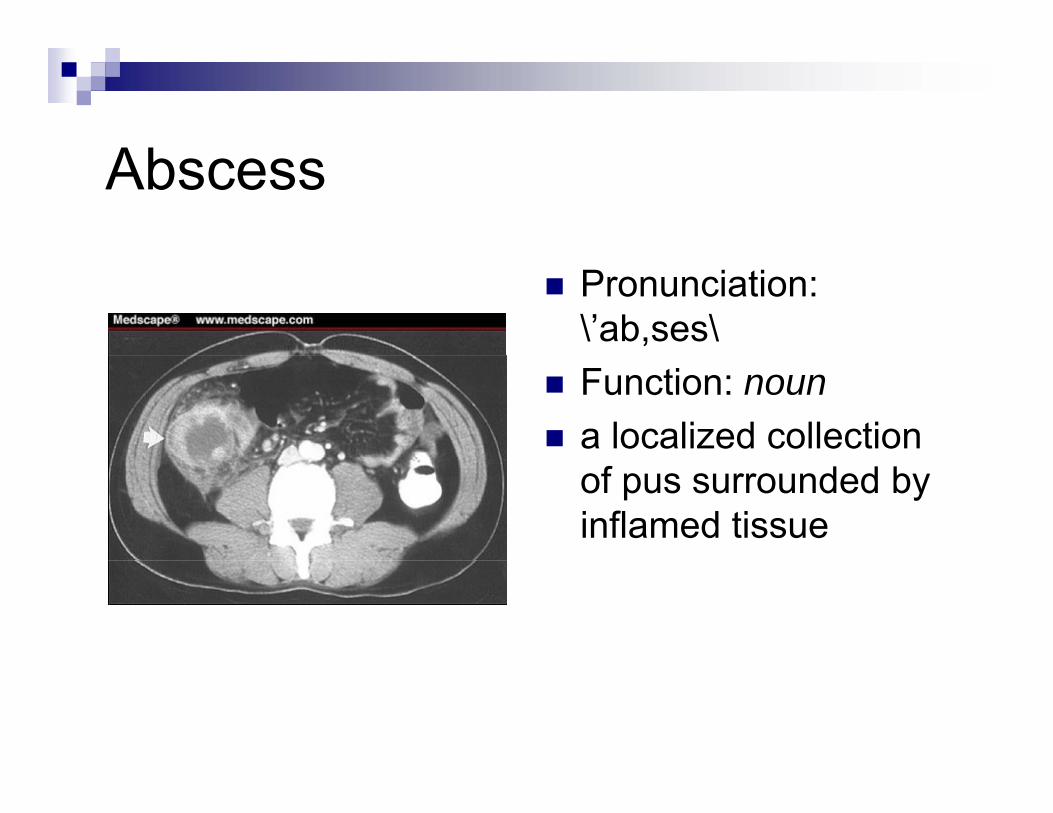
AbAbscess
Pronunciation: \’ab,ses\Function: nouna localized collection of pus surrounded by inflamed tissue
Complicated Appendicitis inComplicated Appendicitis in Children
Roach et al (2007) – retrospective review of all children undergoing appendectomy over 5 year period1,106 children -> 360 had perforation -> 92 with abscess , por phlegmon60/92 underwent appendectomy32/92 underwent drainage and/or abx with delayed32/92 underwent drainage and/or abx with delayed appendectomy2nd group had longer prodrome, higher WBC, same LOS but lower complication rate requiring readmission (0% vs p q g (10%)Conclude that in children presenting with prolonged symptoms and discrete appendiceal abscess or y p ppphlegmon, drainage and delayed appendectomy should be the treatment of choice
Nonoperative management vs p gimmediate appendectomy in perforated appendicitisperforated appendicitis
Multicenter case-control study (2007)1998 to 2003Data suggest that nonoperativeData suggest that nonoperative management should be prospectively evaluated in children with perforatedevaluated in children with perforated appendicitis presenting with a history of pain > 5 dayspain > 5 days
P f t d di iti i hildPerforated appendicitis in children
Whyte et al (2008) sought early identifiers of failure of nonoperative management in perforated appendicitis to help in surgical decision making58 patients had CT-proven perforated appendicitis -> treated nonoperatively36/58 (62%) responded( ) p22/58 (38%) failedDetermined that 3 parameters identify patients who fail
Persistence of fever after 24 hours of treatmentPersistence of fever after 24 hours of treatmentBandemia on admissionMultisector involvement on CT scan

Failure of conservativeFailure of conservative management
Aprahamian et al (2007) concluded that lack of an abscess and presence of an pappendicolith predict failure of nonoperative managementp g
I t l A d tInterval Appendectomy
Ein (2005) demonstrated that the presence of an appendicolith was associated with a 72% rate of recurrent appendicitis (vs 26% with no appendicolith)recurrent appendicitis (vs 26% with no appendicolith)N = 96 pediatric patients (16 months to 17 years), 1980 to 2003All t t d ith IV t i l tibi ti f 5 t 21 dAll were treated with IV triple antibiotics for 5 to 21 days for ruptured appendix with inflammatory mass or abscessAuthors conclude that patients with appendicolith should have an interval appendectomy
O t ti t i t l d tOutpatient interval appendectomy
Whyte et al (2008) – retrospective observational study (2/03 to 1/07)37 children who had successful nonoperative treatment37 children who had successful nonoperative treatment of CT-documented perforated appendicitisInterval appendectomy offered and recommended when f lith i l dfecalith involved31/37 requested IA24/31 underwent LIA21/24 (88%) were discharged on DOA
R fReferencesJaffe Bernard M, Berger David H, "Chapter 29. The Appendix" (Chapter). Brunicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE, Schwartz SI: Schwartz's Principles of Surgery, 8th Edition: http://www.accesssurgery.com/content.aspx?aID=15019. Whyte Christine, Tran Eric, et al, “Outpatient interval appendectomy after perforated appendicitis,” Journal of Pediatric Surgery (2008) 43, 1970-1972.Whyte Christine, Levin Terry, et al, “Early decisions in perforated appendicitis in children: lessons from a study of nonoperative management,” Journal of Pediatric Surgery (2008) 43, 1459-1463.Keckler Scott, Tsao Kuojen, et al, “Resource utilization and outcomes from percutaneous drainage and interval appendectomy for perforated of appendicitis with abscess,” Journal of Pediatric Surgery (2008) 43, 977-980.T K t l “M t f di t i t di iti i th t d t hi ” JTsao K, et al, “Management of pediatric acute appendicitis in the computed tomographic era,” J Surg Res. 2008 Jun 15; 147 (2):221-4.Aprahamian C, et al,” Failure in the nonoperative management of pediatric ruptured appendicitis: predictors and consequences,” J Pediat Surg. 2007 Jun; 42(6): 934-8.Ein, S, et al,” Nonoperative management of pediatric ruptured appendix with inflammatory mass or abscess: presence of an appendicolith predicts recurrent appendicitis ” Journal of Pediatricabscess: presence of an appendicolith predicts recurrent appendicitis, Journal of Pediatric Surgery (2005) 40, 1612-1615.Roach Jonathan, et al, “Complicated appendicitis in children: a clear role for drainage and delayed appendectomy,” The American Journal of Surgery 194 (2007) 769-773.Meeks Derek & Kao Lillian, “Controversies in Appendicitis,” Surgical Infections. Vol 9 No 6, 2008.
Th E dThe End





![Clinical Study Laparoscopic-Assisted Single-Port ...Appendicitis is the most common cause of acute abdom-inaldiseaseinchildren[ ]. Despite several advantages of laparoscopic appendectomy](https://static.fdocuments.net/doc/165x107/60c5d0c53cc0b00b80379732/clinical-study-laparoscopic-assisted-single-port-appendicitis-is-the-most-common.jpg)



![The current management of acute uncomplicated appendicitishub.hku.hk/bitstream/10722/251485/1/content.pdf · of acute uncomplicated appendicitis with promising re-sults [6–8]. Appendectomy,](https://static.fdocuments.net/doc/165x107/5c9dec6588c993d8368bb27a/the-current-management-of-acute-uncomplicated-of-acute-uncomplicated-appendicitis.jpg)







