Anhydrous pill ingestion: A new cause of esophageal obstruction
2
CASE REPORT esophagus, obstruction, cause; obstruction, esophagus, cause Anhydrous Pill Ingestion: A New Cause of Esophageal Obstruction We report the case of a patient who presented with complaints of abdominal discomfort and recurrent vomiting after ingestion of an anhydrous protein pill. Esophagoscopy revealed the presence of a pill much larger than initially ingested. The pill was removed through the endoscope. This is the first re- port of esophageal obstruction from anhydrous pill ingestion. [Roach J, Mar- tyak T, Benjamin G: Anhydrous pill ingestion: A new cause of esophageal obstruction. Ann Emerg Med August 1987;16:913-914.] INTRODUCTION Adherence of a drug product to esophageal mucosa is a significant cause of esophageal injury.l,¢ The majority of patients with pill-induced esophageal injury have no history of esophageal disease. 3 We recently evaluated a patient with dysphagia to solids and liquids, anorexia, and recurrent vomiting over a 48-hour period after swallowing a pill. CASE REPORT A 20-year-old man, previously in excellent health, presented complaining of abdominal discomfort and persistent vomiting. Three days earlier, the pa- tient began taking chewable protein tablets because of a health food fad. Because of his dislike for the taste of the pill, he swallowed one without chewing it. Ten to fifteen seconds after swallowing he experienced epigastric pain followed by vomiting of all ingested material. During the next three days his symptoms of pain and vomiting became progressively worse and he presented to our emergency service. His medical history was unremarkable for pyrosis, reflux, or dysphagia. The cardiopulmonary exam was normal and there was no stridor or wheez- ing. Respirations were 16, and temperature was 36.3 C. There was mild orthostasis by pulse, increasing from 54 supine (with a blood pressure of 120/70 mm Hg) to 108 on standing (with a blood pressure of 130/90 mm Hg), and slight tenderness to deep palpation in the epigastric region. Bowel sounds were active, and there was no rebound or rigidity. Because of concerns about foreign body obstruction, esophagoscopy was done, revealing a large pill lodged at the esophagogastric junction. The pill was markedly enlarged from that initially ingested and was spongy in texture. It was removed through the endoscope and fragmented into several pieces unsuitable for measurement. The esophageal mucosa appeared mildly irritated after removal without gross evidence of masses or Schatki's ring. A follow-up barium swallow was sched- uled, but the patient was lost to follow-up. The protein pills are 90% anhydrous protein N x 6.25 (N is Avogadro's Number or the number of molecules in one mole, and is equal to 6.02 x 1023/g mole}, 4.5% moisture, 4% mineral ash, and 1.5% stabilizer and flavors (exact composition unknown). The package label notes that the pills are "chewable" but contains no warning about swallowing them whole. DISCUSSION Improper ingestion of pills is a significant factor in esophageal pill reten- tion. 3 The symptoms of dysphagia, odynophagia, and retrosternal chest pain are strongly suggestive of esophageal impaction. 4 Additional symptoms may include anorexia, abdominal pain, and volume depletion, as were seen in this James~Roach, MD* Thomas Martyak, MDI Georges Benjamin, MD, FACP1- Washington, DC From the Department of Medicine* and Emergency Medicine Service,t Walter Reed Army Medical Center, Washington, DC. Received for publication June 16, 1986. Revision received November 24, 1986. Accepted for publication January 28, 1987. The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the Department of the Army. Address for reprints: James Roach, MD, Department of Medicine, Walter Reed Army Medical Center, Washington, DC 20307-5001. 16:8 August 1987 Annals of Emergency Medicine 913/129
-
Upload
james-roach -
Category
Documents
-
view
213 -
download
1
Transcript of Anhydrous pill ingestion: A new cause of esophageal obstruction

CASE REPORT esophagus, obstruction, cause; obstruction, esophagus, cause
Anhydrous Pill Ingestion: A New Cause of Esophageal Obstruction
We report the case of a patient who presented with complaints of abdominal discomfort and recurrent vomiting after ingestion of an anhydrous protein pill. Esophagoscopy revealed the presence of a pill much larger than initially ingested. The pill was removed through the endoscope. This is the first re- port of esophageal obstruction from anhydrous pill ingestion. [Roach J, Mar- tyak T, Benjamin G: Anhydrous pill ingestion: A new cause of esophageal obstruction. Ann Emerg Med August 1987;16:913-914.]
INTRODUCTION Adherence of a drug product to esophageal mucosa is a significant cause of
esophageal injury.l,¢ The majority of patients with pill-induced esophageal injury have no history of esophageal disease. 3
We recently evaluated a patient with dysphagia to solids and liquids, anorexia, and recurrent vomiting over a 48-hour period after swallowing a pill.
CASE REPORT A 20-year-old man, previously in excellent health, presented complaining
of abdominal discomfort and persistent vomiting. Three days earlier, the pa- tient began taking chewable protein tablets because of a health food fad. Because of his dislike for the taste of the pill, he swallowed one without chewing it. Ten to fifteen seconds after swallowing he experienced epigastric pain followed by vomiting of all ingested material. During the next three days his symptoms of pain and vomiting became progressively worse and he presented to our emergency service. His medical history was unremarkable for pyrosis, reflux, or dysphagia.
The cardiopulmonary exam was normal and there was no stridor or wheez- ing. Respirations were 16, and temperature was 36.3 C. There was mild orthostasis by pulse, increasing from 54 supine (with a blood pressure of 120/70 m m Hg) to 108 on standing (with a blood pressure of 130/90 m m Hg), and slight tenderness to deep palpation in the epigastric region. Bowel sounds were active, and there was no rebound or rigidity. Because of concerns about foreign body obstruction, esophagoscopy was done, revealing a large pill lodged at the esophagogastric junction. The pill was markedly enlarged from that initially ingested and was spongy in texture. It was removed through the endoscope and fragmented into several pieces unsuitable for measurement. The esophageal mucosa appeared mildly irritated after removal without gross evidence of masses or Schatki's ring. A follow-up barium swallow was sched- uled, but the patient was lost to follow-up.
The protein pills are 90% anhydrous protein N x 6.25 (N is Avogadro's Number or the number of molecules in one mole, and is equal to 6.02 x 1023/g mole}, 4.5% moisture, 4% mineral ash, and 1.5% stabilizer and flavors (exact composition unknown). The package label notes that the pills are "chewable" but contains no warning about swallowing them whole.
DISCUSSION Improper ingestion of pills is a significant factor in esophageal pill reten-
tion. 3 The symptoms of dysphagia, odynophagia, and retrosternal chest pain are strongly suggestive of esophageal impaction. 4 Additional symptoms may include anorexia, abdominal pain, and volume depletion, as were seen in this
James~Roach, MD* Thomas Martyak, MDI Georges Benjamin, MD, FACP1- Washington, DC
From the Department of Medicine* and Emergency Medicine Service,t Walter Reed Army Medical Center, Washington, DC.
Received for publication June 16, 1986. Revision received November 24, 1986. Accepted for publication January 28, 1987.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the Department of the Army.
Address for reprints: James Roach, MD, Department of Medicine, Walter Reed Army Medical Center, Washington, DC 20307-5001.
16:8 August 1987 Annals of Emergency Medicine 913/129

ANHYDROUS PILL INGESTION Roach, Martyak & Benjamin
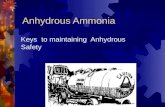
case. Despi te the genera l ly ben ign nature of medication ingestion, many complications, including esophageal impaction, can occur (Figure).
Un l ike mos t cases of esophageal impaction, pill-induced impaction and injury usually is not associated with esophageal disease, 3 and some reten- tion of pills in the esophagus is a com- m o n occurrence in hea l thy individ- uals. 5 Normally, structural or moti l i ty abnormali t ies of the esophagus such as str icture, Schatzki 's ring, esoph- ageal tumors, hiatial hernia, extrinsic compression, and esophagitis increase the risk of esophageal obs t ruc t ion . 4 Composition is another important fac- tor with pills, especially if they be- come sticky after swallowing or are of a caustic composition.
This case demonstrates the first re- port of an anhydrous pill ingestion re- sult ing in esophageal obstruction. In our patient prolonged esophageal con-
FIGURE. Esophageal compl ica t ions of pil l ingest ions
tact occurred, wi th swell ing of the tablet and eventual obstruction. The anhydrous nature of this tablet makes this a particularly likely event.
SUMMARY This case demonstrates one poten-
tial complication of improper medica- t ion ingestion. Many pills may stick to the esophageal mucosa even if it is normal; in the case of anhydrous pills, swe l l i ng can occur and r e s u l t in esophageal obstruction.
REFERENCES i. Marvola M, Rajaniemi M, Marttila E, et al: Effect of dosage form and formulation factor on the adherence of drugs to the esophagus, l Pharm Sci 1983;72:I034-1036.
2. Hughes R: Drug induced esophageal injury. Br Med J 1979;2:132.
Ulceration
Perforation
Hemorrhage
Desiccation
Burns
Obstruction (mechanical/edema)
Esophagitis
Stricture
3. Kikendall JW, Friedman AC, Oyewole MA, et al: Pill-induced esophageal injury -- Case re- ports and review of the medical literature. Dig Dis and Sci 1983;28:174-182.
4. Nandi E Ong GB: Foreign body in the oesophagus. Review of 2394 cases. Br J Surg 1978;65:5-9.
5. Evans KT, Roberts GM: Where do all the tab- lets go? Lancet 1976;2:1237-1239.
130/914 Annals of Emergency Medicine 16:8 August 1987