ANGIOTENSIN CONVERTING ENZYME INHIBITOR HARISHT
17
INHIBITORS BY. A.Harish Kumar Amit Dadarya Gupta ANGIOTENSIN CONVERTING ENZYME
-
Upload
anna-university-chennai -
Category
Technology
-
view
141 -
download
0
Transcript of ANGIOTENSIN CONVERTING ENZYME INHIBITOR HARISHT
INHIBITORS
BY.
A.Harish Kumar
Amit Dadarya Gupta
ANGIOTENSIN CONVERTING
ENZYME
INTRODUCTION
ANGIOTENSIN-CONVERTING ENZYME (ACE) is a dipeptidyl peptidase transmembranebound enzyme.
A soluble form of ACE in plasma is derived from the plasma membrane-bound formby proteolytic cleavage of its COOH-terminal domain.
There are two distinct isoforms of ACE: somatic and testicular. They are transcribedfrom a single gene at different initiation sites.
The somatic form of ACE is a large protein (150 –180 kDa) that has two identicalcatalytic domains and a cytoplasmic tail. It is synthesized by the vascular endo-theliumand by several epithelial and neural cell types.
The testicular form of ACE is a 100- to 110-kDa protein that has a single catalyticdomain corresponding to the COOH terminal domain of somatic ACE and is only foundin developing spermatids and mature sperm where it may play a role in fertilization.
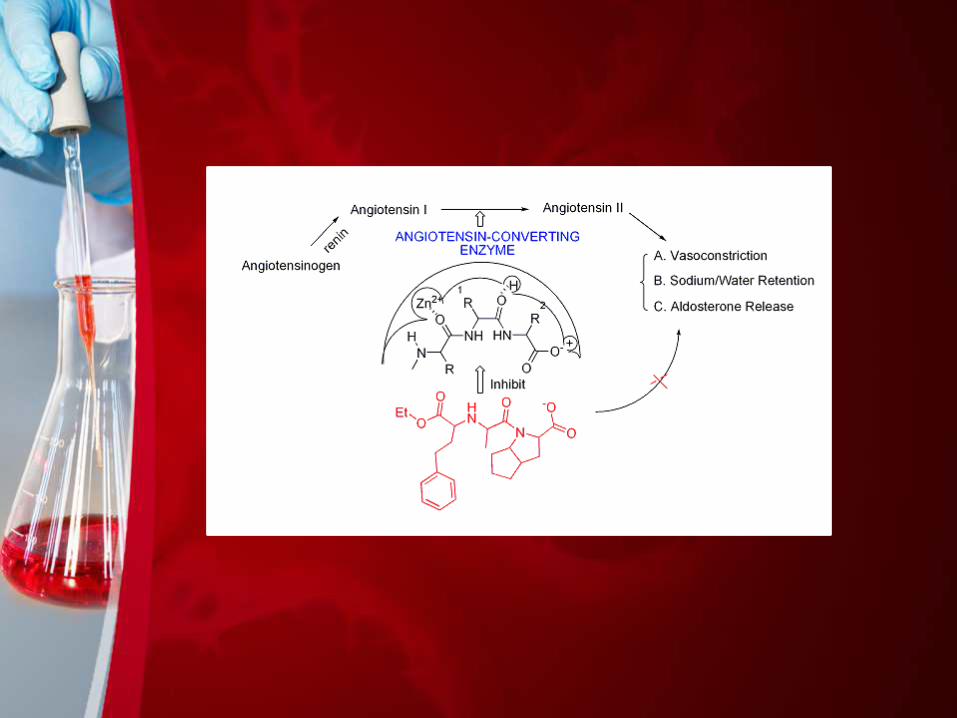
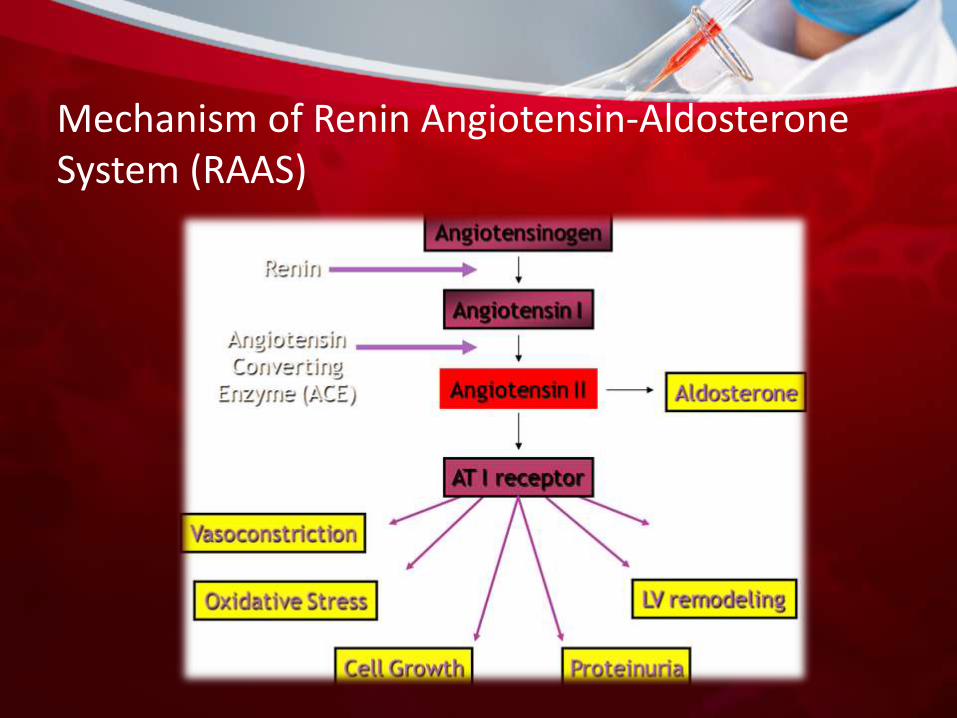
Mechanism of Renin Angiotensin-AldosteroneSystem (RAAS)
ANGIOTENSINOGEN
ANGIOTENSIN I
ANGIOTENSIN II
ANGIOTENSIN III
Renin
ACE
Aminopeptidase
Non-ACE
(eg. Chymasein heart)
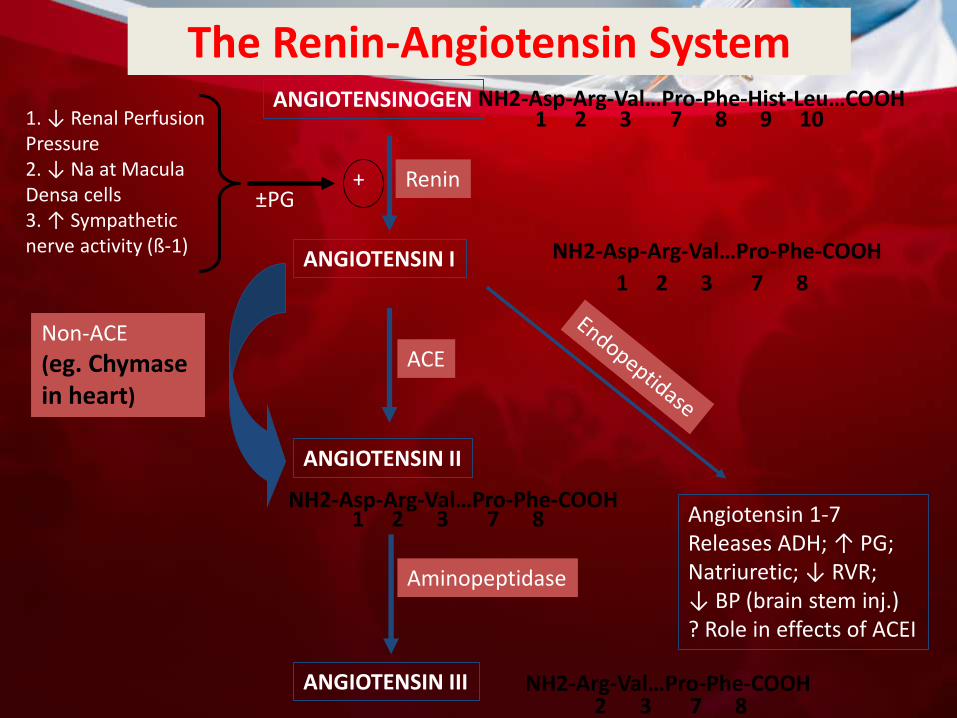
Angiotensin 1-7Releases ADH; ↑ PG;Natriuretic; ↓ RVR; ↓ BP (brain stem inj.)? Role in effects of ACEI
1 2 3 7 8 9 10
NH2-Asp-Arg-Val…Pro-Phe-COOH
1 2 3 7 8
NH2-Asp-Arg-Val…Pro-Phe-COOH1 2 3 7 8
NH2-Arg-Val…Pro-Phe-COOH2 3 7 8
NH2-Asp-Arg-Val…Pro-Phe-Hist-Leu…COOH
+
1. ↓ Renal PerfusionPressure2. ↓ Na at Macula Densa cells3. ↑ Sympathetic nerve activity (ß-1)
±PG
The Renin-Angiotensin System
MECHANISM ACE inhibitor amplified the effects of bradykinin in vessels thatlacked measurable ACE activity
ACE inhibitors also directly activate the bradykinin B1 receptor,acting at the Zn-binding pentameric consensus sequence HEXXH ofthe B1 receptor
A motif that is present in the active center of ACE but absentfrom the B2 receptor
ACE inhibitors also induce phosphorylation of the ACEintracellular tail (Ser1270) via CK2, resulting in outside-in signalingthat enhances expression of ACE and cyclooxy-genase-2
The effect of the ACE inhibitor on COX-2 is due to thetranscription factor activator prot-ein-1(AP-1). This results inincreased release of prostacyclin and prostaglandin E2 by theendothelial cells that is independent of local accumulation ofkinins
Competitive inhibition of ACE reduces generation of angiotensin II and consequently reduces the release of aldosterone .

Generic Trade Name
Benazepril Lotensin (Novartis)
Captopril Capoten (Bristol-Myers Squibb)
Enalapril Vasotec (Merck)
Fosinopril Monopril (Bristol-Myers Squibb)
Lisinopril Prinivil (Merck), Zestril (Zeneca)
Moexipril Univasc (Schwarz Pharmaceuticals)
Perindopril Aceon (Solvay Pharmaceuticals)
Quinapril Accupril (Pfizer)
Ramipril Altace (Monarch Pharmaceuticals)
Trandolapril Mavik (Knoll Pharmaceuticals)
EXAMPLES OF ACEI
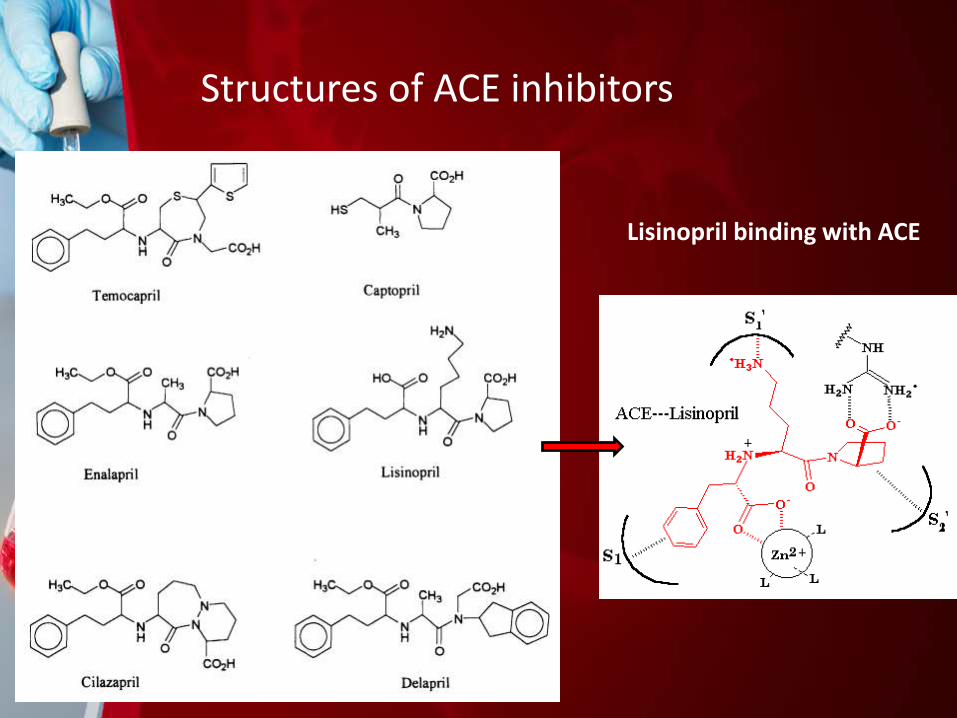
Structures of ACE inhibitors
Lisinopril binding with ACE
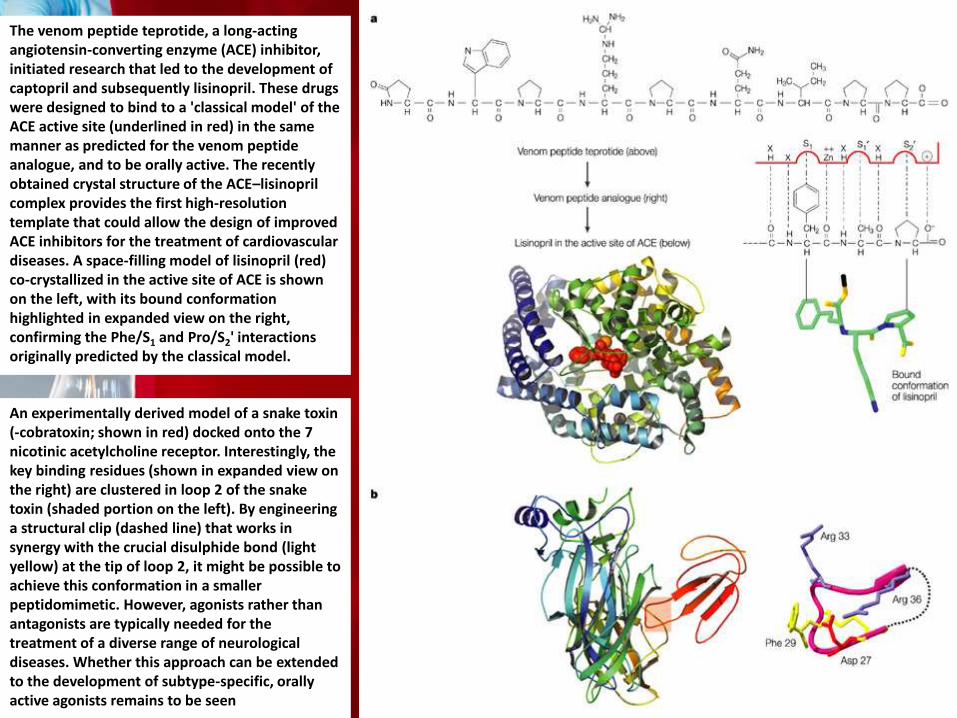
The venom peptide teprotide, a long-acting angiotensin-converting enzyme (ACE) inhibitor, initiated research that led to the development of captopril and subsequently lisinopril. These drugs were designed to bind to a 'classical model' of the ACE active site (underlined in red) in the same manner as predicted for the venom peptide analogue, and to be orally active. The recently obtained crystal structure of the ACE–lisinoprilcomplex provides the first high-resolution template that could allow the design of improved ACE inhibitors for the treatment of cardiovascular diseases. A space-filling model of lisinopril (red) co-crystallized in the active site of ACE is shown on the left, with its bound conformation highlighted in expanded view on the right, confirming the Phe/S1 and Pro/S2' interactions originally predicted by the classical model.
An experimentally derived model of a snake toxin (-cobratoxin; shown in red) docked onto the 7 nicotinic acetylcholine receptor. Interestingly, the key binding residues (shown in expanded view on the right) are clustered in loop 2 of the snake toxin (shaded portion on the left). By engineering a structural clip (dashed line) that works in synergy with the crucial disulphide bond (light yellow) at the tip of loop 2, it might be possible to achieve this conformation in a smaller peptidomimetic. However, agonists rather than antagonists are typically needed for the treatment of a diverse range of neurological diseases. Whether this approach can be extended to the development of subtype-specific, orally active agonists remains to be seen
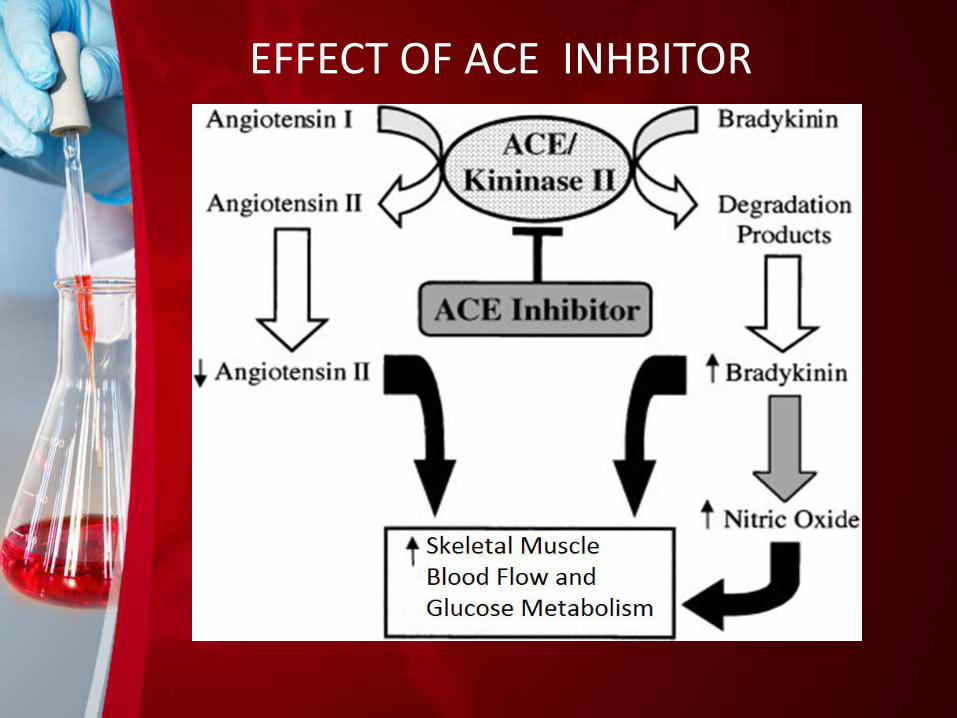
EFFECT OF ACE INHBITOR
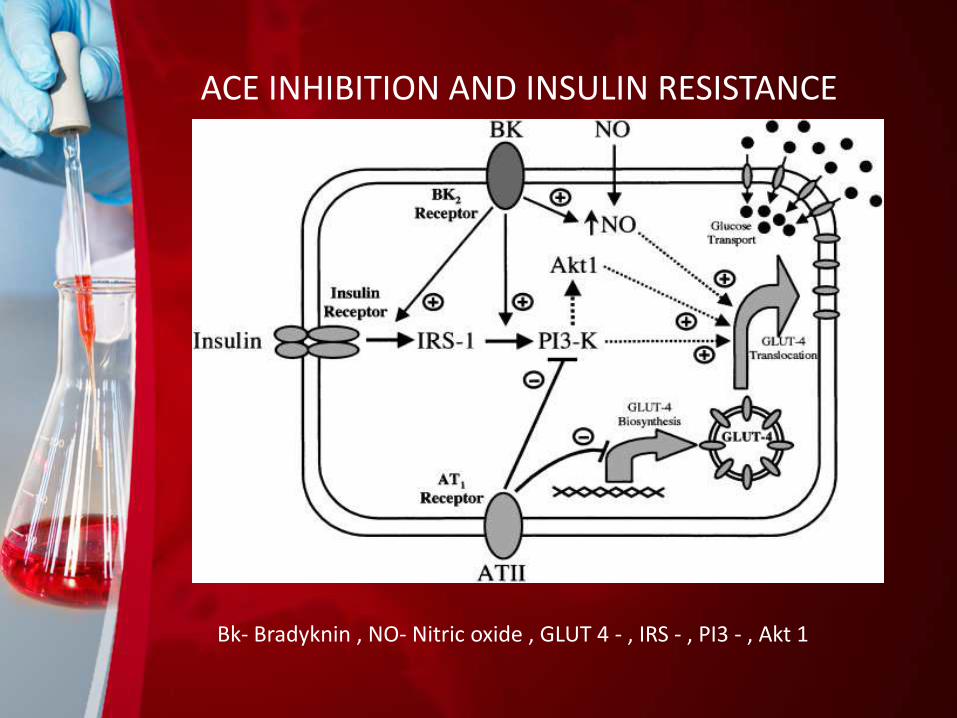
ACE INHIBITION AND INSULIN RESISTANCE
Bk- Bradyknin , NO- Nitric oxide , GLUT 4 - , IRS - , PI3 - , Akt 1
PHARMACOKINETICS OF ACE INHIBITORS
• Some are primany eliminated by kidney.
• Others are eliminated in bile and feces.
• Useful in selection of patients – Reduced Kidney Function Or Liver Function.
• Except CAPTORIL (capoten) and LISINOPRIL (prinivil, zestril) all other are inactive.
CONDITIONS FOR ACE INHIBITORS USAGE
• Stroke.
• Hypertension.
• Antihypertensive.
• Reverse left ventricular hypertrophy and vascular disease.
• Prevent remodeling after myocardial infarction.
• Slow progression of heart failure.
• Slow progression of renal disease (diabetes, microal buminuria).
• Prevent diabetes.
• Prevent cancer and slow the aging process.
Uses of ACE inhibitors
• Treatment of hypertension .
• Treatment of heart failure .
• Secondary prevention after myocardial infarction .
• Diabetic nephropathy in insulin dependent diabetes .
Side effects of ace inhibitors
•Dizziness•Headache •Drowsiness•Diarrhea•Low blood pressure•Weakness •Cough dry•Rash•Many cause birth defects•Swelling of tissues
References:-
Hecker M, Blaukat A, Bara AT, Mu¨ ller-Esterl W, and Busse R. ACE inhibitorpotentiation of bradykinin-induced venoconstriction. Br J Phar-macol 121: 1475–1481,1997.
Ignjatovic T, Tan F, Brovkovych V, Skidgel RA, and Erdo¨ s EG. Activation of bradykininB1 receptor by ACE inhibitors. Int Immunophar-macol 2: 1787–1793, 2002.
Peng H, Carretero OA, Vuljaj N, Liao T-D, Motivala A, Peterson EL,and Rhaleb N-E.Angiot -ensin-converting enzyme inhibitors: a new mech-anism of action.
Young ME, Leighton B. 1998. Evidence for altered sensitivity of the nitric oxide/cGMPsignalling cascade in insulin-resistant skeletal muscle. Biochem J 329:73–79.
Roberts CK, Barnard RJ, Scheck SH, Balon TW. 1997. Exercise-stimulated glucosetransport in skeletal muscle is nitric oxide dependent. Am J Physiol Endocrinol Metab273:E220–E225.
Cartee GD, Douen AG, Ramlal T, Klip A, Holloszy JO. 1991. Stimulation of glucosetransport in skeletal muscle by hypoxia. J Appl Physiol 70:1593–1600.