Anemia of Chronic Disease - GrG · Italian Journal of Medicine 2007. Definition The WHO definition...
63
Journal Club-18 Gennaio 2008 Anemia of Anemia of Chronic Disease Chronic Disease Piera Barbisoni
Transcript of Anemia of Chronic Disease - GrG · Italian Journal of Medicine 2007. Definition The WHO definition...
Journal Club-18 Gennaio 2008
Anemia ofAnemia of Chronic DiseaseChronic DiseasePiera Barbisoni

Anemia in the elderly is associated with increased mortality and hospitalization, worst quality of life and overall health/functional status, cardiovascular and pulmonary diseases, renal impairment, cognitive impairment, falls, disabilityand frailty.
Medical and Functional Consequences of Anemia in the Elderly. Balducci, JAGS, 2003 Anemia of Chronic Disease. Weiss et Goodnough, NEJM, 2005 Anemia in the elderly: A Public Health Crisis in Hematology. Guralnik et al. Hematology, 2005Epidemiology of anemia in the elderly. Nardi et al. Ital J Medicine, 2007Chronic Anemia and Fatigue in Elderly Patients: Results of s Randomized, Double-Blind, Placebo-Controlled, Crossover Exploratory Study with Epoietin Alfa. Agnihotri et al. JAGS 2007
Definition
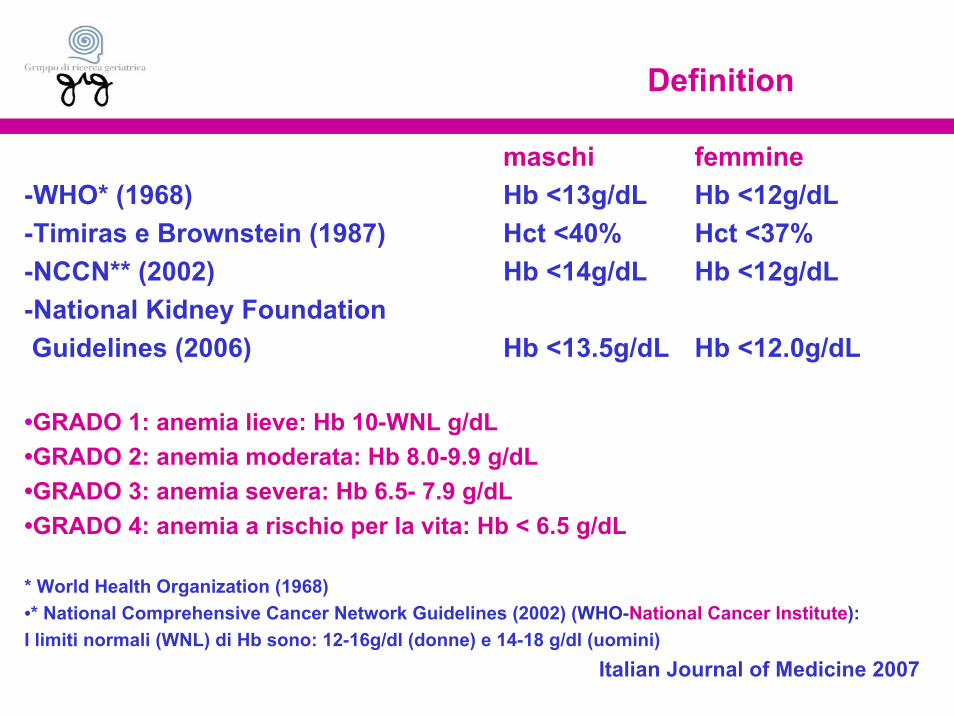
maschi femmine-WHO* (1968) Hb <13g/dL Hb <12g/dL -Timiras e Brownstein (1987) Hct <40% Hct <37% -NCCN** (2002) Hb <14g/dL Hb <12g/dL -National Kidney Foundation Guidelines (2006) Hb <13.5g/dL Hb <12.0g/dL
•GRADO 1: anemia lieve: Hb 10-WNL g/dL •GRADO 2: anemia moderata: Hb 8.0-9.9 g/dL•GRADO 3: anemia severa: Hb 6.5- 7.9 g/dL•GRADO 4: anemia a rischio per la vita: Hb < 6.5 g/dL
* World Health Organization (1968)•* National Comprehensive Cancer Network Guidelines (2002) (WHO-National Cancer Institute):I limiti normali (WNL) di Hb sono: 12-16g/dl (donne) e 14-18 g/dl (uomini)
Italian Journal of Medicine 2007
Definition
The WHO definition of anemia (Hb <13g/dL in men and Hb <12 g/dL in women) is the most frequently (although not universally) used criteria.
This definition in elderly patients may be “too restrictive”, expecially in the light of recent data.
Italian Journal of Medicine 2007

Looking at the Relationship Between Hemoglobin Concentration and Prevalent Mobility Difficulty in Older Women. Shouldthe Criteria Currently Used to Define Anemia in Older People be Reevaluated?
Chaves et al, JAGS 2002

Definition
Findings from the Women’s Health and Aging Study I and II (WHAS I, II) in 633 disabled community-dwelling women aged 70 to 80 have shown that:• women with Hb between 13.0 and 14.0 g/dl consistently obteined the best results in performance based tests of mobility function;• those with Hb less than 12.0 g/dl achieved the worst results; • and those with Hb between 12.0 and 13.0 g/dl (low-normal Hb concentrations) performed intermediately.
……….Hb 12.0 g/dl might be a suboptimal cutoff for defining anemia in older women.
Definition
Women’s Health and Aging Study I (WHAS I)In 686 community-dwelling women aged 65 and older with moderate to severe self reported disability, Hb levels progressively lower than 11 g/dl were associated with increasingly higher risks for all-cause 5-year mortality than levels of 12.0 g/dl, whereas Hb levels of 13.0 and 14.0 g/dl were associated with a lower risk of death.
…considerations should be given to refining the current definition of anemia inelderly.
… Hb levels higher than what is currently recommended might offer clinical advantage.

The Definition of Anemia in Older PersonsIzaks GJ et al, JAMA 1999
The study of 755 subjects >85 years of age showed that a Hb <13g/dl in males and <12g/dl infemales was associated with an increasedrelative risk of mortality of 1.6 in males (95% CI 1.2-2.1) and 2.3 in females (95% CI 1.6-3.3).
Disorders such as malignancy, peptic ulcer, and infection were more common in the anemic patients. However, the mortality risk in elderly anemic patients without obvious clinical disease was also increased to more than twice that of nonanemic patients.

In conclusion:
The mortality risk was increased in older persons with anemia if anemia was defined by the WHO criteria (the WHO criteria are appropriate for older persons).
Anemia in older patients is due to the disease and not aging, and that further investigation is warranted if an older person’s Hb is below normal, even if no clinical disease is immediately apparent.
Prevalence
The studies of prevalence of anemia amongthe elderly are notable for their extreme diversity(variability in the patient populations studied,countries in which the research was conducted,range of simple sizes, definition of anemia used,quality of the research and setting of care).
Italian Journal of Medicine 2007
Prevalence
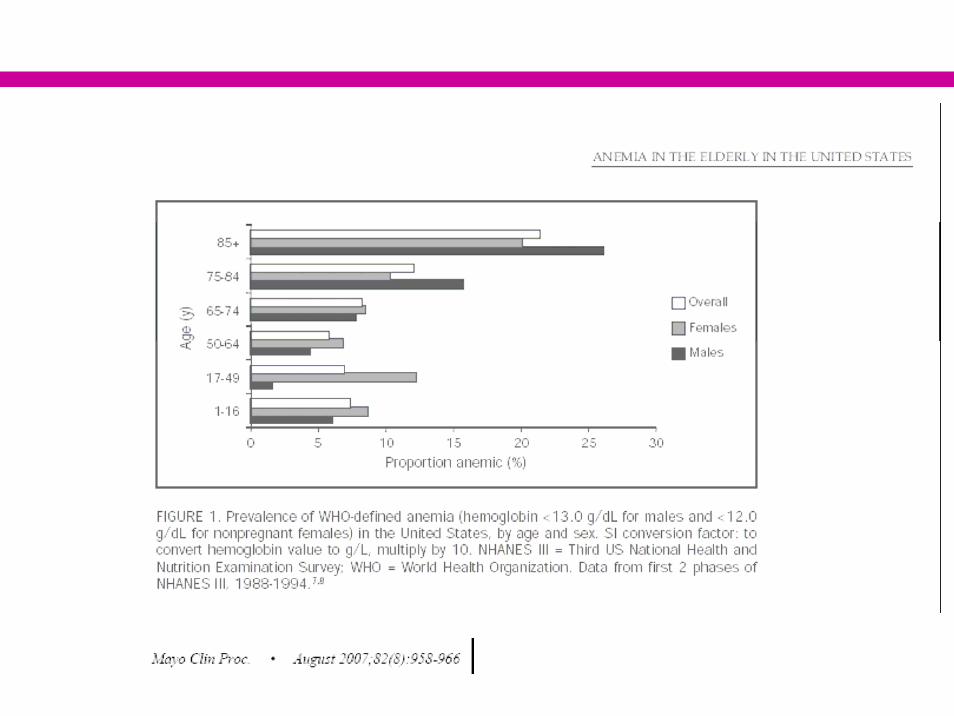
Anemia is an increasingly common medical disorder in the elderly, affecting approximately13% of people aged 70 and older.
The prevalence of anemia increases with ageand this increase starts at the age of 65 and rises sharply after 80.
Am J Med 2004
Prevalence
In addition to age, sex is a factor that has been shown to influence the prevalence of anemia in theelderly.
Anemia is generally more common in men than women perhaps because the Hb levels used to defineanemia are tipically higher for men (42.8% 70-74y; 59.5% >85y)
JAGS 2003
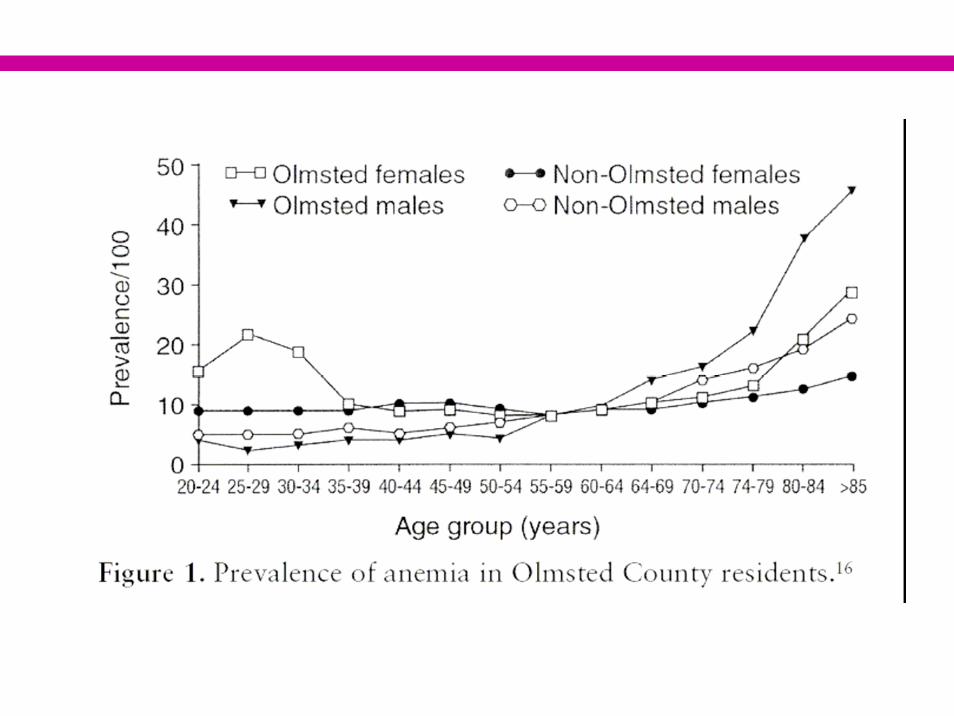
Before age 55, the prevalence of anemia is lowerin men than in women (3% in men vs 6% in women aged50-54). After this age, the trend is reversed (prevalenceat 65y is 21% in men and 16% in women) (higher prevalence of underlying diseases in men).
(Olmsted County Study Minnesota, JAGS 2003)
Prevalence

Prevalence
Using the WHO definition of anemia, 11% of menand 10.2% of women (>65y) were anemic according tothe NHANES III data set (Third US National Health an NutritionExamination Survey).
Hematology, 2005
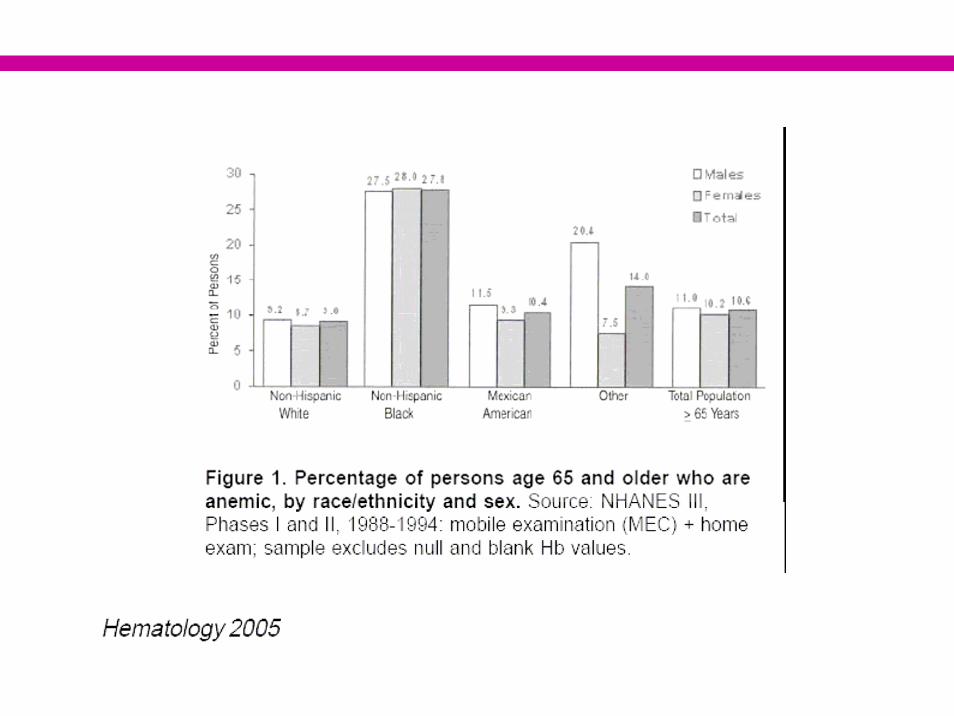

Although the prevalence of anemia is greater inwomen than men aged <75, by age 75 male prevalence surpasses female prevalence by about 5 percentage points, a disparity that continues into upper age brackets (Third US National Health an Nutrition Examination Survey).
Hematology, 2005
Prevalence

Prevalence
The general prevalence of anemia in thepopulation aged 65 and older varies greatly dependingon residential status.
The prevalence is lower in community residents(2.9%-34% in men and 3.3%-25% in women) than inpatients admitted to acute hospital wards or long-termcare facilities (17.7%-61% in men and 8.4%-41% inwomen) (these patients are sicker than the general elderly population).
Italian Journal of Medicine 2007
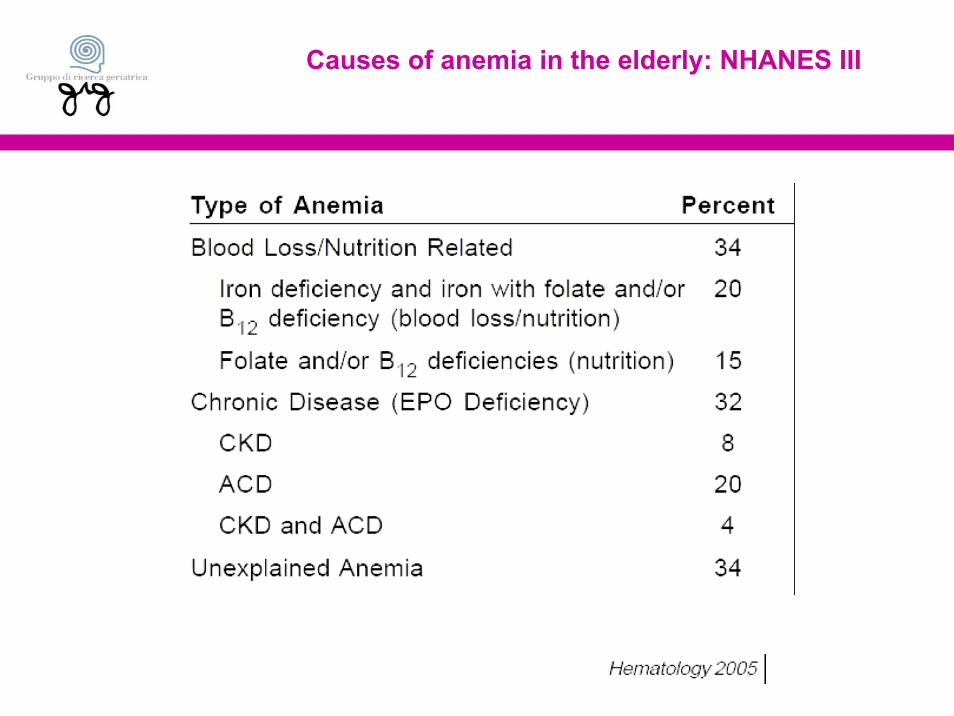
Causes of anemia in the elderly: NHANES III

Causes


Anemia of Chronic Disease
Anemia of chronic disease is the second most common anemia worldwide (iron deficiency) but it is the most common in elderly patients and in acute hospitalwards or long-term care facilities .
It occurs in patients with acute or chronic immune activation. The condition has thus been termed “anemia of chronic inflammation”.
It was initially thought to be associated primarily with chronic disorders, infectious, inflammatory diseases, or cancer. NEJM 2005

Anemia of Chronic Disease
However, other observations have shown that this anemia can be seen in a variety of conditions, including severe trauma, heart disease, diabetes mellitus, and in those with acute or chronic immune activation.
→The severity of anemia generally correlates with the severity of the underlying disease.
NEJM 2005

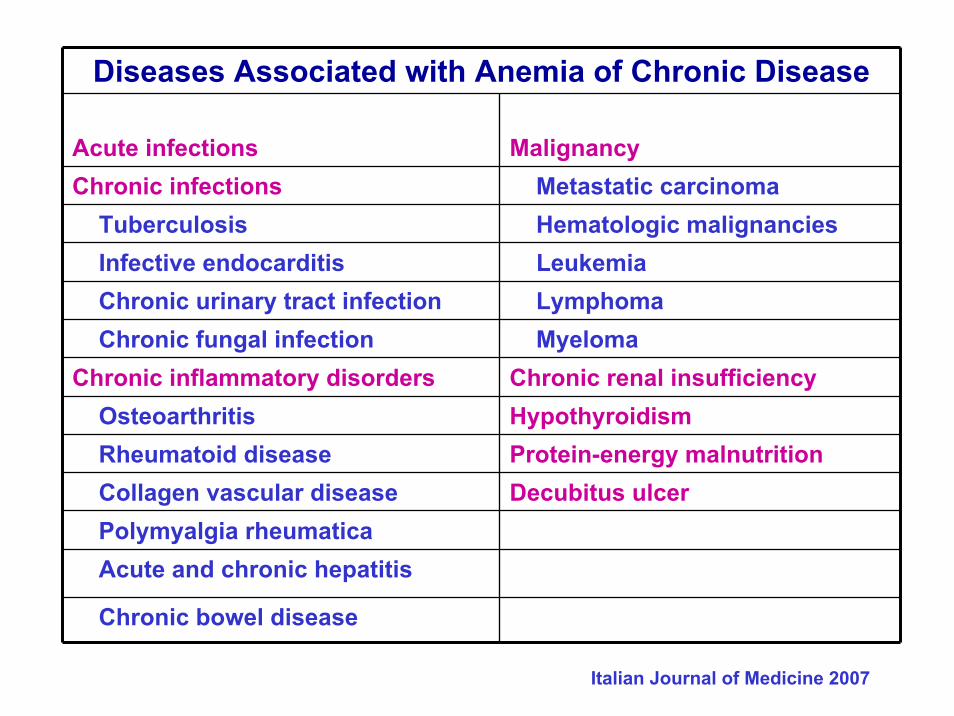
Diseases Associated with Anemia of Chronic Disease
Acute infections MalignancyChronic infections Metastatic carcinoma
Tuberculosis Hematologic malignancies Infective endocarditis LeukemiaChronic urinary tract infection LymphomaChronic fungal infection Myeloma
Chronic inflammatory disorders Chronic renal insufficiencyOsteoarthritis HypothyroidismRheumatoid disease Protein-energy malnutritionCollagen vascular disease Decubitus ulcerPolymyalgia rheumaticaAcute and chronic hepatitis
Chronic bowel disease
Italian Journal of Medicine 2007

Pathophysiology
Aging itself is unlikely to be a direct cause of anemia, especially because data have shown that hemoglobin levels do not change significantly in healthy olders individuals aged between 60 and 98.
Nevertheless, experimental and clinical data have suggested that aging is associated with a progressivereduction in hematopoietic reserve, which makes older individuals more susceptible to developing anemiaduring hematopoietic stress.
JAGS, 2003

Pathophysiology
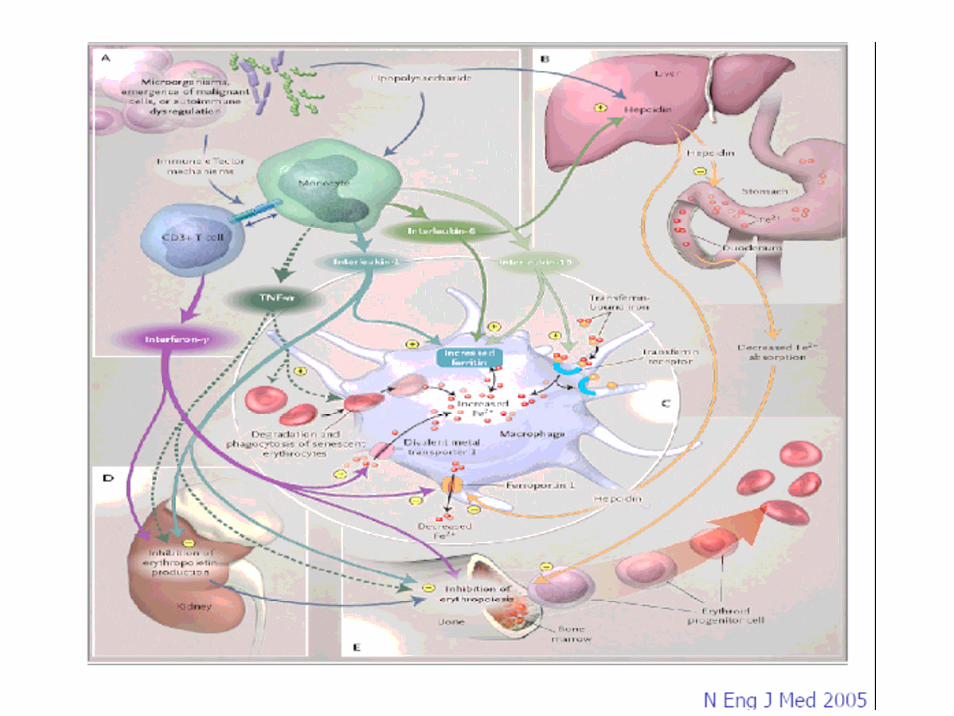
• L’attivazione del sistema immunitario da parte dei linfociti T e dei macrofagi in risposta ad uno stimolo infettivo, infiammatorio o neoplastico, determina la liberazione delle citochine -INFγ, IL-1, IL-6 e TNFα-responsabili dell’anemia.
Pathophysiological mechanism features are:
NEJM 2005
Pathophysiology
1) Impaired erythropoiesisproliferation and differentiation of erythroid precursors are impaired (inhibitory effects of cytokines) → inability of the morphologically normal marrow to increase erythropoirsis in response to anemia → anemia, decreased reticulocyte count
2) dysregulation of iron homeostasis ↑ iron storage within the RES with subsequent limitation of the availability of iron for erythroid progenitor cells (hypoferremia, hyperferritinemia) ↓ iron intestinal absorption by ↑ liver production hepcidin (hypoferremia)↑ iron uptake and inhibition of iron recirculation fromerythrophagocytosis in macrophages (hypoferremia)
Pathophysiology
3) Decreased in Erythropoietin (EPO) production (by citokines) and reduced biologic activity of EPO in response to anemic hypoxia that lead to inhibition of erythropoiesis (decreased levels of circulating EPO, anemia)
4) decreased lifespan of red blood cellsincreased erythrophagocytosis during inflammation leads to a decreased erythrocyte half-life (↓10-15%)

Pathophysiology: anemia and renal insufficiency
Anemia of renal insufficiency is primarily due to a deficiency of endogenous erithropoietin, and it has been suggested that it develops when the glomerular filtration rate falls below 50% of the normal range. It has also been suggested that a shortened red blood cell lifespan and suppressed red blood cell production aggravate the mechanism underlying this form of anemia.
NEJM 2005

Laboratory Evaluation
Anemia of chronic disease is hypoproliferative normochromic, normocytic anemia (MCV between 80 and 100 fL) of variable severity.
Many patients have mild anemia (Hb level: 10-11g/dl). However, more severe anemia (Hb level < 8g/dl) occurs in 20% of cases.
NEJM 2005
Laboratory Evaluation
The absolute reticulocyte count is frequently low (reticulocyte production is impaired and not enough to compensate for the decreased red blood cell county).
Low iron serum level is a necessary condition for diagnosis (cytokines ↓ iron concentration and limited availability of iron for erythroid cell). → An important aspect of ACD is the inability of the patient to mobilize and use iron effectively.
NEJM 2005

Laboratory Evaluation
In both CDA and iron deficiency anemia, the serum concentration of iron and transferrin saturation are reduced, reflecting absolute iron deficiency in iron deficiency anemia and hypoferremia due to acquisition of iron by RES in anemia of chronic disease with decreased levels of serum iron.
In iron deficiency anemia, transferrin saturation may be even low because serum concentrations of transferrin(the iron transporter) are increased, whereas transferrin levels remain normal or decreased in anemia of chronic disease.
NEJM 2005

Laboratory Evaluation
The soluble transferrin receptor is normal (↑ in iron deficiency anemia).
The serum level of ferritin is normal or increased (>100μg/L) marker of iron storage; reflecting ↑ storage and retention of iron within the RES and ↑ ferritin levels due to immune activation). (30 μg/L cutoff – ferritin is ↓ in iron-deficiency anemia).
NEJM 2005


The soluble transferrin receptor (s-TfR) is a truncated fragment of the membrane receptor that is increased in iron deficiency, when the availability of iron for erythropoiesis is low.
→Negli stati ferro carenziali ha una sensibilità maggiore rispetto ad altri parametri di laboratorio.
In contrast, levels of soluble trasferrin receptors in anemia of chronic disease are not significantly different from normal, because transferrin-receptor expression is negatively affected by inflammatory citokines.
NEJM 2005
Laboratory Evaluation

The ratio of the concentration of soluble transferrin receptors to the log of the ferritin level (s-TfR/log ferritina) may also be helpful:
A ratio <1 (low) suggests anemia of chronic disease
A ratio >2 (high) suggests absolute iron deficiency coexisting with anemia of chronic disease (reale fabbisogno di ferro).
NEJM 2005
Laboratory Evaluation


Treatment
The rationale for the treatment of anemia of chronic disease is based on two principles.
1) Anemia can be generally deleterious in itself, requiring a compensatory increase in cardiac output in order to maintain systemic oxygen delivery;
NEJM 2005

Treatment
2) Anemia is associated with a poorer prognosis in a variety of conditions. Thus, moderate anemia warrants correction, expecially in patients older than 65y of age, those with additional risk factors (coronary artery disease, pulmonary disease, chronic kidney disease), or a combination of these factors.
In patients with renal failure who are receiving dialysis and in patients with cancer who are undergoing chemotherapy, correction of anemia up to hemoglobin levels of 12g/dl is associated with an improvement in the quality of life.
NEJM 2005

Treatment Options
Treatment Options
When possible, treatment of the underlying disease is the therapeutic approach of choice for anemia of chronic disease.
In cases in which treating the underlying disease is not feasible, alternative strategies are necessary.
NEJM 2005

Treatment: Transfusion (NEJM 2005)
Blood trasfusions are widely used as a rapid and effective therapeutic intervention. Trasfusions are particularly helpful in the context of either severe anemia(Hb <8.0g/dl) or life-threating anemia (Hb <6.5g/dl).
Blood trasfusion therapy has been associated with increased survival rates in anemic patients with myocardial infarction, but trasfusion itself has also been associated with multiorgan failure and increased mortalityin patients who are in critical care. Whether blood trasfusions modulate the immune system, causing clinically relevant adverse effects, remains undetermined.
Treatment: Transfusion (NEJM 2005)
It is important to note that existing guidelines for the management of anemia of chronic disease in patients with cancer or chronic kidney disease do not recommend long term blood transfusion therapy in their management algorithms because of the risks associated with long-term transfusion, such as iron overload and sensitization to HLA antigens that may occur in patients before renal transplantation.

Treatment: Iron Therapy (NEJM 2005)
Iron therapy for patients with anemia of chronic disease is controversial.
Iron is an essential nutrient for proliferating microorganism, and the sequestration of iron from microorganism or tumor cells into the RES is believed to be a potentially effective defense strategy to inhibit the growth of pathogens.
In addition, iron therapy in a setting of long-term immune activation promotes the formation of highly toxic hydroxyl radicals that can cause tissue damage and endothelial dysfunction and increase risk of acute cardiovascular events.

Treatment: Iron Therapy (NEJM 2005)
• On the other hand, iron therapy may confer benefit:Absolute iron deficiency accompanying the anemia of
chronic disease (these patients should receive supplemental iron therapy);
Functional iron deficiency that develops under conditions of intense erythropoiesis during therapy with erythropoietic agents. Parenteral iron has been demonstrated to enhance rates of response to therapy with erytropoietic agents in patients with cancer who are undergoing chemotherapy and in patients undergoing dialysis.

Treatment: Iron Therapy (NEJM 2005)
To achieve and maintain the target Hb levels with erythropoietin, sufficient body iron stores are required. Supplemental iron should be administered, as needed, to maintain a transferrin saturation of >20%, and a serum ferritin level of >100 ng/ml.
However, iron therapy is currently not recommended for patients with anemia of chronic disease who have a high or normal ferritin level (above 100ng/ml), owing to possible adverse outcomes in this setting.

Treatment: Erythropoietic Agents (NEJM 2005)
The therapeutic effect involves counteracting the antiproliferative effects of cytokines, along with the stimulation of iron uptake and heme biosynthesis in erythroid progenitor cells.
Erythropoietic agents for patients with anemia of chronic disease are currently approved for use by patients with cancer who are undergoing chemotherapy, patients with chronic kidney disease, and patients with HIV infection who are undergoing myelosuppressive therapy.

Treatment: Erythropoietic Agents (NEJM 2005)
The percentage of patients with anemia of chronic disease who respond to therapy with erythropoietic agents is 25% in myelodysplastic syndromes, 80% in multiple myeloma, and up to 95% in chronic kidney disease.
• Three erythropoietic agents are currently available:epoietin alfa, epoietin beta, and darbepoietin alfa which differ in terms of their pharmacologic compounding modifications, receptor-binding affinity, and serum half life.
Treatment: Erythropoietic Agents (NEJM 2005)
• Current findings indicate that for patients receiving erythropoietic agents, target Hb levels should be 11 to 12g/dl. Overcorrection of anemiato normal Hb levels and insufficient treatmenthave each been associated with unfavorable clinical course.
• Before the initiation of therapy with an erythropoietin agent, iron deficiency should be rouled out.
Treatment: Erythropoietic Agents (NEJM 2005)
• For monitoring the response to erythropoietic agents,Hb levels should be determined after four weeks oftherapy and at intervals of two to four weeks thereafter. If the Hb level increases by less 1 g/dl, theiron status should be reevaluated and iron supplementation considered.
• The dose of erythropoietic agents should be adjustedonce the Hb concentration reaches 12g/dl.
• If no response is achieved after eight weeks ofoptimal dosage in the absence of iron deficiency, apatient is considered nonresponsive to erythopoietic agents.
Treatment: Erythropoietic Agents (NEJM 2005)
• EPO is given in a starting dose of 100 to 150 U/Kgsubcutaneously three times weekly along with supplemental oral iron.
• However, most clinicians use 30.000-40.000 U of EPO given once a week, a single dose which is numerically equivalent to a dose of 140 to 190 U/Kgthree times per week for a 70 Kg person. This dose can be increased to 60.000 U if there is no response(ie, Hb rise <1g/dl) at four weeks.
• Darbepoetin is a newer formulation of erythropoietin which has a longer in vivo half-life than erythropoietin (500 μg every 2-3 weeks).
Treatment: Erythropoietic Agents (NEJM 2005)
Although the positive short-term effects of therapy with erythropoietic agents on the correction of anemia and avoidance of blood transfusions are well documented, few data are available on possible effects on the course of underlying disease.
Erythropoietic recetors are found on several malignant cell lines, including mammary, ovarian, uterine, prostate, hepatocellular, and renal carcinomas. A recent study (Lancet 2003) investigating the effect of therapy with epoietin on the clinical course of patients with metastatic breast carcinoma was discontinued because of a trend toward higher mortality among patients receiving the drug.

Conclusioni
1. Anemia in the elderly is an extremely commonproblem that is associated with increased mortality and poorer health-related quality of life.
2. It may represent a sign of serious underlying disease and may be itself a cause of dysfunctionof multiple organ systems from chronic hypoxiemia.
3. Future research is needed to define the optimal Hb levels for health, to refine diagnostic testing to sort out the etiology of the unexplained anemias, and to evaluate rigorously therapies designed to augment erythropoiesis.

Prevalenza di anemia in anziani spedalizzati
Femmine Maschi Totale
N=2086 N=1294 N=3380
Anemia 464 (22,2) 215 (16,6) 679 (20,1)

EORTC Guidelines for the use of Erythropoetic Proteins in Anemic Patients with Cancer (Eur J Cancer 2007)
•Il trattamento con Eritropoietina va intrapreso per valori diHb compresi tra 9 e 11 g/dl in base ai sintomi correlati, avendo come obiettivo il raggiungimento di valori di 12-13 g/dl o un miglioramento della sintomatologia.
•La dose raccomandata è di 30.000/40.000 UI settimanali (per eritropoietina beta e alfa) o 500 μg ogni 2-3 settimane (darbepoietina).
•La risposta alla terapia migliora se viene eseguita una integrazione di ferro ev. Alcuni autori raccomandano di mantenere la saturazione della transferrina > il 20% e laferritina >100 ng/ml.
•L’unico fattore predittivo di risposta sembra essere un basso valore di eritropoietina sierica all’esordio.