
Andrew Triebwasser Department of Anesthesiology October, 2014.
42
The preoperative fast: where we’ve been; where we are Andrew Triebwasser Department of Anesthesiology October, 2014
-
Upload
julius-tucker -
Category
Documents
-
view
218 -
download
1
Transcript of Andrew Triebwasser Department of Anesthesiology October, 2014.

The preoperative fast:where we’ve been; where we
are
Andrew TriebwasserDepartment of Anesthesiology
October, 2014

pulmonary aspiration of gastric contents a longstanding & central concern in anesthesia
may have been causative in first anesthetic mortality (Hannah Greener 1848)
tri-modal clinical scenarios◦ (near) drowning◦ airway obstruction◦ pneumonitis w/variable severity
Historical context of preoperative fasting (I)

Winternitz - acid pneumonitis (1920) Hall (JAMA) 15 cases in parturients (1940) Mendelson: pneumonitis in rabbits worsened
w/lower pH, higher volume, solid particles *
Mendelson’s syndrome: aspiration ≥ 25 ml (0.4 ml/kg) with pH ≤ 2.5 **
*Am J Obst Gynec 1946;52:191** Shirley (unpublished) 1954 (rhesus)
Historical context of preoperative fasting (II)

Pulmonary aspiration of gastric contents – an overview
gastric contents
capable of damage
regurgitation of these gastric
contents
significant pulmonary aspiration
Pulmonary aspiration of gastric contents – early measures
gastric contents
capable of damage
regurgitation of these gastric
contents
significant pulmonary aspiration
1960’s →“modern techniques” please refer to the archived PowerPoint on Sellick and RSI
forced emesis
balloon tipped esophageal blockers

ingestion and gastric secretions
gastric emptying
Focus: gastric contents
“nulla per os” after midnight (or 8º fast) had become accepted standard by 1950’s

problems associated
with prolonged
fasting
need for an empty
stomach
“while it is desirable that there be no solid matter in the stomach when chloroform is administered, it will be found very salutary to give a cup of tea or beef-tea about 2 hours previously” (1883)
Joseph Lister
as late as 1948, Digby Leigh recommended 1º fast after clears
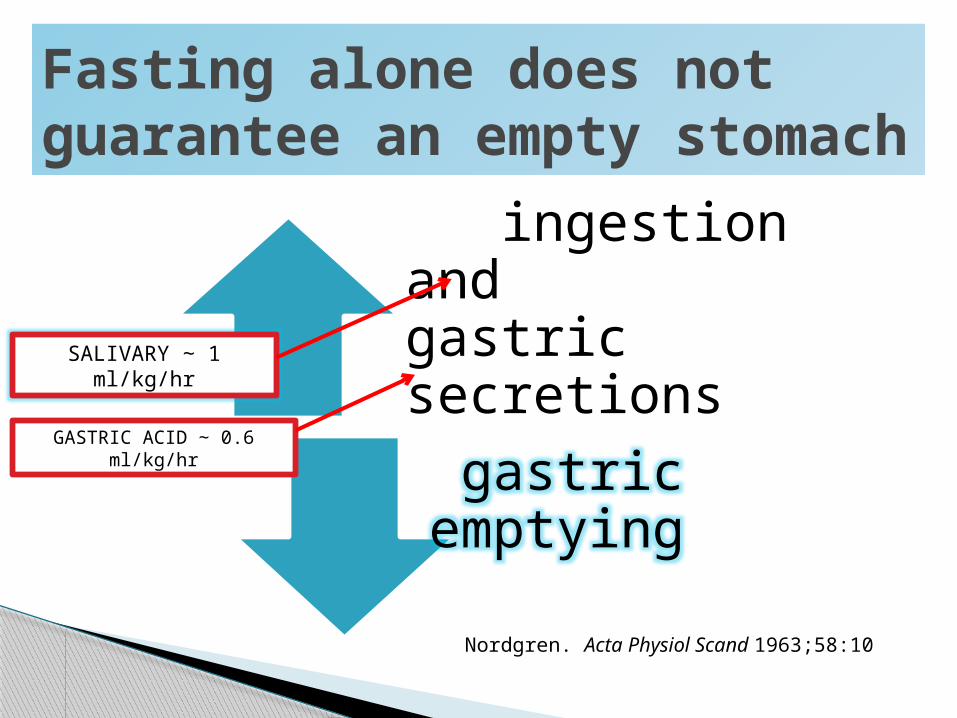
ingestion and gastric secretions
gastric emptying
Fasting alone does not guarantee an empty stomach
SALIVARY ∼ 1 ml/kg/hr
GASTRIC ACID ∼ 0.6 ml/kg/hr
Nordgren. Acta Physiol Scand 1963;58:10
Flash forward/flash backward
intense and rigorous fasting protocols $$$$ invested in the pharmacological
manipulation of gastric volume and pH aspiration risk too low* to provide
meaningful endpoints, so we are left with surrogate endpoints to assess risk
Narberth, Pa 1987
* Warner MA. Anesthesiology 1999;90:66 (1985-97 Mayo Clinic):~ 2:10,000 elective anesthetics with virtually no morbidity (↑↑ emergent)

The problem with “gastric contents” as a sine qua non risk factor for aspiration
quantification based on direct instillation “at-risk” parameters under question * no evidence from RCT, cohort or case-
control studies that link GFV & aspiration 30-60% of pts “at-risk” yet very rare
event
Schreiner MS. Anesth Analg 1998;87-754
* James (1984): critical pH 1.8 (rats) Raidoo (1988): 0.4 ml/kg & pH 1.0 minimal effect (rhesus monkeys)
I cannot forecast to you the action of Russia. It is a riddle wrapped in a mystery inside an enigma.
-Winston Churchillradio broadcast October, 1939
(widely misquoted)
gastric contents

Reassessing “NPO after midnight” in 1980’s (I)
hypovolemia/hypotension hypoglycemia (or need for IV dextrose) irritability (for adults → lack of caffeine) difficult compliance / dissatisfaction delays or cancellations
IS THE PREOPERATIVE FAST BENIGN?

Reassessing “NPO after midnight” in 1980’s (II)
this would be bad
DOES FASTING LEAD TO REDUCED GASTRIC VOLUME?
Reassessing “NPO after midnight” in 1980’s (III)
what about this??
CANCEL
?
DOES FASTING LEAD TO REDUCED GASTRIC VOLUME?

historical (why did we stop?) physiological benefit to patient RCT’s
Basis for liberalizing preoperative clear fluids

ingestion & gastric secretions
gastric emptying
Gastric contents

William Beaumont
gastric physiologist who determined that liquids emptied from stomach in under an hour and also demonstrated the effects of emotion on gastric emptying
A real flashback - 1833

GOOD REFERENCE Splinter et al. Anes Analg 1999:89:80
Gastric emptying
protein > CHO > lipids
simple liquids < 1º, longer if ↑ osm, ↑ cal, non-neutral pH
complex meals may take 9º, simple ones under 3º

Remember: digestion is dependent on the state in the stomach
liquid in stomach liquid and solid (curds) phases in stomach

historical (why did we stop?) physiological benefit to patient RCT’s
Basis for liberalizing preoperative clear fluids in the late 1980’s

the only way to “liberalize” fasting guidelines which have unknown morbidity and unclear benefit is to at least “prove” that this would not adversely affect “aspiration risk” through surrogate endpoints of gastric volume and pH
Liberalizing clear fluids: RCT’s → the paradox
another paradox

slew of RCT’s in 1980’s some w/multiple variables & Mendelson still central endpoint
Liberalizing clear fluids: RCT’s → the paradox (II)
STUDY NPO (hr) VOLUME GFV (ml/kg) *
MaltbyAnesth Analg 1986;65:1112
(had ranitidine group)
2.5 study14.4 control
150 ml water 17.6 ml (adults)26.7 ml
Splinter Can J Anaesth 1989;36:55
14.5 control2.5 study 3 ml/kg AJ
0.43±0.460.24±0.31 **
SandharAnesthesiology 1989 71:327
8.6 control2-3 study
5 ml/kg 0.250.34
MeakinBr J Anaesth 1987;59:678
(had multiple variables)
2-4 study2-4 studyfasted
orange drinkdrink + biscuit
0.390.460.25** significantly different from
control* gastric fluid pH consistently < 2.5 in both groups

“wild” - revised instructions for study group without any confounding interventions
measurement of usual surrogate endpoints power sufficient for “no difference” linear analog scoring of several
experience-based parameters

Gastric fluid analysis (CHOP)
STUDY (clears) (53)
CONTROL (NPO) (68)
p
Gastric fluid volume(GFV) (ml/kg)
0.44 ± 0.51 0.57 ± 0.51 0.12
GFV > 0.4 ml/kg (%)
48 58 0.77
H+ mean (pH) 0.015±.008 (1.81) 0.017±.01 (1.77) 0.47
Gastric pH ≤ 2.5 (%)
97 92 0.57
Gastric pH ≤ 2.5 and GFV 0.4 ml/kg (%)
46 48 0.86
Schreiner et al. Anesthesiology 1990;72:593

Clear benefits to clear fluids:questionnaire results CHOP study
A ease of compliance
B temperament
C overall experience
p < 0.001
p < 0.001
p < 0.01
Schreiner et al. Anesthesiology 1990;72:593

revised NPO 2.6 ± 0.7º vs. 13.5 ± 3.1º clears do not ↑ Mendelson risk factors and
with appropriate power might show ↓ clears associated with ↑ satisfaction
a major institution well known for conservatism
IMPACT
what about infants? what about (others) excluded from study *
CHOP: questions not asked
*ASA III-IVknown risk factors that ↓ gastric emptyingknown risk factors ↑ acid production

INGESTED MATERIAL MINIMUM FASTING PERIOD
clear liquids 2 hours
breast milk 4 hours
infant formula/non-human milk 6 hours
light meal (toast & clears) 6 hours
prophylactic pharmacologic agents to reduce aspiration risk NOT recommended

PROBABLY ENOUGH TIME: breast milk complete emptying by 3º *
* Sethi AK. Anaesthesia 1999;54:51
PURPOSE
enhance quality efficiency anesthetic care stimulate evaluation individual practices reduce severity complications related to
pulmonary aspiration of gastric contents
Anesthesiology 1999;90:896
10 years well spent
cost effective use peri-op preventive medication
increased patient satisfaction avoidance delays and cancellations ↓ risk dehydration/hypoglycemia prolonged
fast minimize perioperative morbidity
Anesthesiology 1999;90:896
enhance quality and efficiency of care …..

meta-analysis of RCT with clears 2-4 hours◦ adults: highly supportive (A) ↑ pH and ↓ GFV ◦ peds: highly supportive (A) for pH; equivocal GFV (C)◦ no evidence (D) supporting risk emesis/aspiration
consultants strongly agree on clears 2-4 hours and agree on all other aspects of guidelines
Anesthesiology 2011;114:495
no change NPO guidelines
category B2 evidence that co-morbidities may be associated with ↑ risk pulmonary aspiration◦ GERD◦ dysphagia or other disorders GI motility◦ potential difficult airway◦ metabolic disorders such as diabetesAnesthesiology
2011;114:495
preoperative assessment – experts strongly agree it should be performed, but only class D evidence it changes outcome

NPO guidelines are only a part of the continuum of patient evaluation and preparation….aspiration risk factors need to be assessed on an individualized basis and anesthetic plan proceed accordingly
Putting NPO guidelines in context
14 yo arrives in HU chewing gum
Real life clinical scenario (I)
your plan???

ingestion & gastric secretions
gastric emptying
Gastric contents & gum
Poulton TJ. Pediatric Anesthesia 2012;22:288
overall, may transiently ↑ volume, but not acidity
both gastric emptying and LES sphincter relaxation may be ↑, but probably not clinically so
SALIVARY may increase 4-5 fold over first 15
minutes
if it is prohibited, exercise your right to cancel or delay the full 6 hours
compromise and wait 2 hours no delay but make sure it gets spit out
Gum chewing during pre-anesthetic fast: how to proceed
QUESTION: if chewed gum is swallowed, is cancellation indicated?
equally reasonable options?

6 yo fell off monkey bars 4º ago while eating ice cream cone. Supracondylar fracture with possible vascular compromise. If surgeon amenable, any benefit in delaying 2º?
what if the patient was scheduled for the next AM with appropriate NPO time? LMA OK?
what if at that time the patient showed up in the HU without an IV? how proceed?
Real life clinical scenario (II)

GI motility and emptying may be adversely affected by stress (SNS), pain, opioids
affected by severity injury (femur > wrist) * ↑ gastric aspirates if injury w/in 2º eating **
◦ hunger not reliable indicator adequate emptying future directions – US measurement ??
◦ (residual volume, liquid vs. solid) ***
Gastric contents post trauma
*Olsson GL. Acta Anaesthesiol Scand 1982;26:417**Bricker SRW. Anaesthesia 1989;44:721
*** Van de Putte. Br J Anaesth 2014;10:1093
14 month old hypospadias scheduled for 2 PM arrives – has had nothing by mouth since 7 PM the previous evening – it is now 1 PM and OR is on schedule (child is cranky)
Real life clinical scenario (III)
DO YOU:do nothing?insist on clear fluids w/delay?clear fluids w/out delay?start IV in HU and hydrate?

concept of “enhanced recovery after surgery” oral CHO solution 2º pre-op ↓ anxiety/hunger,
post-op improved pain scores, ↓ complications clear advantages to pre-op oral hydration w/
optimal solutions needing further study *
future direction?
Anesth Analg 2014;118:1163
* Nakamura.Anesth Analg 2014;118:1268

THE FARTHER BACKWARD YOU CAN LOOK, THE FARTHER FORWARD YOU ARE LIKELY TO SEE


















